EVIDENCE-BASED CHILD HEALTH: A COCHRANE REVIEW JOURNAL Evid.-Based Child Health 2: 943–964 (2007) Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/ebch.172 Overview of Reviews The Cochrane Library and trachoma: an overview of reviews Elizabeth Sumamo, 1 * Paul Emerson, 2 Krystal Harvey 3 and Matthew Burton 4 1 Alberta Research Centre for Child Health Evidence, University of Alberta, Edmonton, Alberta, Canada 2 The Carter Center, Emory University, Atlanta, Georgia, USA 3 Cochrane Child Health Field, University of Alberta, Edmonton, Alberta, Canada 4 Department of Infectious & Tropical Diseases, London School of Hygiene & Tropical Medicine, London, UK Abstract Background: Trachoma is the leading infectious cause of blindness worldwide. Active trachoma is caused by the bacterium Chlamydia trachomatis. Recurrent infection over many years may lead to scarring of the conjunctiva, entropion, trachomatous trichiasis and corneal opacity. Objective: To summarize Cochrane reviews that assess the effect of SAFE strategy (surgery, antibiotics, face washing and environmental change) for trachoma in developing countries. Methods: The Cochrane Database of Systematic Reviews was searched for any intervention to prevent or treat trachoma. Data was extracted in duplicate and analyzed. Main Results: There were four systematic reviews addressing trachoma, all of which met the inclusion criteria. There was some evidence that the prevalence of active trachoma was reduced by the use of antibiotics. At three months, six of nine trials found a significant reduction in relative risk of active trachoma in the intervention groups. At 12 months, only three of six studies found a significant reduction. Oral azithromycin performed better than topical tetracycline at clearing infection at three months, but not at resolving clinical signs. There is evidence that face washing in combination with topical tetracycline antibiotics can reduce the prevalence of severe trachoma compared to face washing alone. Insecticide spray as a fly control measure significantly reduced trachoma and health education may be effective in reducing active trachoma. Full thickness incision of the tarsal plate was found to be the most successful type of surgery for trichiasis. Tarsal rotation surgery was also found to be more effective than non-surgical techniques for minor trichiasis. This surgery was equally effective when performed by appropriate trained ophthalmic nurses and ophthalmologists and also when conducted in a health centre or village setting. Authors’ Conclusions: There are no clinical trials of the full SAFE strategy for trachoma control on blindness prevention, or on reducing active trachoma, or ocular Chlamydia trachomatis infection. However, there is some evidence that separately supports each of the components of SAFE: surgery, antibiotics, facial cleanliness, and environmental improvements. Programmatically, continued delivery of the full SAFE strategy is warranted and can be expected to have a positive impact on the control of blinding trachoma. Editors’ note: Overviews of reviews, compiling evidence from multiple Cochrane reviews into one accessible and usable document, are a regular feature of this journal. Our aim for each overview is to focus on the treatment question, ‘which treatment should I use for this condition?’ It is our hope that the overview of reviews will serve as a ‘friendly front end’ to The Cochrane Library, allowing the reader a quick overview (and an exhaustive list) of Cochrane reviews relevant to the clinical decision at hand. *Correspondence to: Elizabeth Sumamo, 9416-Aberhart Centre One, University of Alberta, Edmonton, AB T6G 2J3, Canada. E-mail: [email protected]Copyright 2007 John Wiley & Sons, Ltd.
Transcript
EVIDENCE-BASED CHILD HEALTH: A COCHRANE REVIEW JOURNALEvid.-Based Child Health 2: 943–964 (2007)Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/ebch.172
Overview of Reviews
The Cochrane Library and trachoma: an overview ofreviewsElizabeth Sumamo,1* Paul Emerson,2 Krystal Harvey3 and Matthew Burton4
1Alberta Research Centre for Child Health Evidence, University of Alberta, Edmonton, Alberta, Canada2The Carter Center, Emory University, Atlanta, Georgia, USA3Cochrane Child Health Field, University of Alberta, Edmonton, Alberta, Canada4Department of Infectious & Tropical Diseases, London School of Hygiene & Tropical Medicine, London, UK
Abstract
Background: Trachoma is the leading infectious cause of blindness worldwide. Active trachoma is caused bythe bacterium Chlamydia trachomatis. Recurrent infection over many years may lead to scarring of theconjunctiva, entropion, trachomatous trichiasis and corneal opacity.
Objective: To summarize Cochrane reviews that assess the effect of SAFE strategy (surgery, antibiotics, facewashing and environmental change) for trachoma in developing countries.
Methods: The Cochrane Database of Systematic Reviews was searched for any intervention to prevent ortreat trachoma. Data was extracted in duplicate and analyzed.
Main Results: There were four systematic reviews addressing trachoma, all of which met the inclusioncriteria. There was some evidence that the prevalence of active trachoma was reduced by the use ofantibiotics. At three months, six of nine trials found a significant reduction in relative risk of active trachomain the intervention groups. At 12 months, only three of six studies found a significant reduction. Oralazithromycin performed better than topical tetracycline at clearing infection at three months, but not atresolving clinical signs. There is evidence that face washing in combination with topical tetracyclineantibiotics can reduce the prevalence of severe trachoma compared to face washing alone. Insecticide spray asa fly control measure significantly reduced trachoma and health education may be effective in reducing activetrachoma.
Full thickness incision of the tarsal plate was found to be the most successful type of surgery for trichiasis.Tarsal rotation surgery was also found to be more effective than non-surgical techniques for minor trichiasis.This surgery was equally effective when performed by appropriate trained ophthalmic nurses andophthalmologists and also when conducted in a health centre or village setting.
Authors’ Conclusions: There are no clinical trials of the full SAFE strategy for trachoma control onblindness prevention, or on reducing active trachoma, or ocular Chlamydia trachomatis infection. However,there is some evidence that separately supports each of the components of SAFE: surgery, antibiotics, facialcleanliness, and environmental improvements. Programmatically, continued delivery of the full SAFE strategyis warranted and can be expected to have a positive impact on the control of blinding trachoma.
Editors’ note: Overviews of reviews, compiling evidence from multiple Cochrane reviews into one accessibleand usable document, are a regular feature of this journal. Our aim for each overview is to focus on the treatmentquestion, ‘which treatment should I use for this condition?’ It is our hope that the overview of reviews will serveas a ‘friendly front end’ to The Cochrane Library, allowing the reader a quick overview (and an exhaustive list)of Cochrane reviews relevant to the clinical decision at hand.
*Correspondence to: Elizabeth Sumamo, 9416-Aberhart Centre One, University of Alberta, Edmonton, AB T6G 2J3, Canada. E-mail:
Trachoma is the leading infectious cause of blind-ness worldwide. Recurrent infection by the bacteriumChlamydia trachomatis produces a chronic keratocon-junctivitis (inflammation affecting both the conjunc-tiva and cornea) referred to as Active Trachoma. Theinfection is spread from person to person by fingersand clothes used to wipe away eye discharge. It is alsotransmitted through fly-eye contact (1). The repeatedcycle of infection and inflammation causes the innersurface of the upper eyelid to scar. Progressive scarringresults in distortion and shortening of the inside of theeyelid. As the lid margin turns inward (entropion) itcauses the eyelashes to also turn inwards and touch thesurface of the eye, a condition known as trachomatoustrichiasis. This condition can damage the cornea bydirect trauma and secondary bacterial infection unlesscorrected surgically, by rotating the lid margin andlashes away from the eye. Without surgical correc-tion, blinding corneal opacification can develop (2).Although trachoma is easily controlled, blindness fromtrachoma is essentially irreversible.
The World Health Organization (WHO) lists thenational trachoma prevalence estimates for 52 endemiccountries (http://globalatlas.who.int/globalatlas): appr-oximately 460 million people are at risk for blind-ing trachoma; 63 million have active trachoma; and9.5 million have unoperated trichiasis. It has also beenestimated that trachoma is responsible for 3.6% ofglobal blindness (approximately 1.3 million people)making it the world’s leading cause of preventableblindness (3).
Description of the interventions
WHO has adopted an integrated control strategyto prevent blindness from trachoma and to controltrachoma transmission. The strategy has the name‘SAFE’ and consists of: Surgery to correct trachoma-tous trichiasis; Antibiotics to treat active infectionsand reduce the community reservoir of infection; andFacial cleanliness and Environmental change to sup-press transmission by modifying factors that favour it(4,5).
How the interventions might work
Surgery is usually the first component of the SAFEstrategy to be implemented, as it can stop cornealdamage from progressing, and hence prevent blindnessin those at immediate risk, before irreversible cornealopacification has occurred (6). Epilation (plucking theeyelashes) and eyelid taping (forcing eyelashes backto the correct position and holding them with stickingplaster) can be used in lieu of surgery, although thelong-term efficacy of these interventions in preventingblindness is not certain. The most common surgicalprocedures are bilamellar tarsal rotation (full thickness
incision through the eyelid), posterior lamellar tarsalrotation (incision only through the scarred tarsal plateand conjunctiva) and tarsal advance and rotation(incision in the tarsal plate and rotation of the terminalportion, in which the upper part of the tarsus isseparated from the anterior lamellar and advanced) (6).All of the surgical procedures reverse the in-turnedlashes characteristic of trachomatous trichiasis so thatthey are returned to their original, outward-pointingposition.
For treatment with antibiotics, the WHO currentlyrecommends either: (a) 1% tetracycline eye ointmenttwice a day for six weeks applied topically on the innersurface of the lower eyelid, or (b) a single oral doseof azithromycin (1000 mg for an adult and 20 mg/kgfor children) (7). Antibiotics effectively treat currentinfections and are used for both individual treatmentand in mass drug administration (without individualdiagnoses) in hyperendemic communities to reduce thecommunity reservoir of ocular Chlamydia trachoma-tis. Mass drug administration is recommended in acommunity where the prevalence of the characteristicsigns of follicular trachoma (Grade TF in the Sim-plified WHO Grading System, (8)) exceeds 10% inchildren aged 1–9 years (7).
Washing the face removes potentially infectiousocular and nasal discharge from those with currentinfections who are shedding Chlamydia trachomatis,preventing contamination of fomites and reducinghand-eye transmission. Washing away the bacteriamay also play a role in reducing self-reinfection.Children with clean faces have also been observed tohave a reduced frequency of fly-eye contact with thetrachoma vector, Musca sorbens (9). This is importantin the reduction of both acquisition and transmissionof infection as flies that contact the eyes of childrenwho are shedding Chlamydia trachomatis can carrythe bacteria to the eyes of those who are not infected.The increase of clean faces is where the F and E ofthe SAFE strategy come together. Facial cleanlinessis implemented as hygiene promotion in its broadersense including personal grooming, use of soap, notsharing towels, and frequent washing of clothes andbed sheets, and this is facilitated and enhanced bythe provision of water and sanitation – which arethe primary Environmental changes that form the Ecomponent of SAFE.
Other environmental interventions that aim to con-trol eye-seeking flies and address other trachoma riskfactors include: water provision; reducing environmen-tal contamination with human faeces; promotion oflatrine use; moving animals away from domestic resi-dences; village cleaning with the promotion of refusedumps; and fly control with insecticides (2,10,11,12).
Some studies looked at infection with C. trachoma-tis in addition to active trachoma as an outcome. Therelationship between infection (as compared to clin-ical signs) and trichiasis and blindness is yet to be
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 945
established, but it is likely that the control of infec-tion in addition to reduction in clinical signs will beof long-term benefit.
Why it is important that we do this review
The brunt of the burden of blinding trachoma isborne by the most impoverished populations in theworld, populations whose poverty comes hand-in-handwith the unhygienic overcrowded living conditions andpoor access to water and sanitation, which are asso-ciated with trachoma. The economic impact of thedisability caused by trichiasis and blindness on thosewho are already poor contributes to keeping them inthe cycle of poverty. Trachoma has disappeared fromEurope, North America and individual countries with-out specific or large-scale control programs. It hasalso been demonstrated that it is possible to con-trol trachoma using the SAFE strategy in even themost disadvantaged parts of the world such as South-ern Sudan (13). The global elimination of blindingtrachoma should be possible, and it is necessary toinvestigate the efficacy of the interventions that aimto do so.
Objectives
To summarize Cochrane reviews related to the WHO’sSAFE Strategy, evaluating the effectiveness of inter-ventions to control active trachoma and to surgicallycorrect established trachomatous trichiasis.
Methods
Search Strategy
The Cochrane Database of Systematic Reviews wassearched for all systematic reviews examining anyintervention for the treatment of trachoma. The term‘trachoma’ was entered and restricted to record title,abstract or keyword. Four reviews were found, oneof which was being updated, and all of which wereincluded in this overview of reviews.
Selection of reviews
Each of the reviews retrieved assessed one of the fourcomponents of the WHO’s SAFE strategy to preventtrachoma; surgery, antibiotics, facial cleanliness andenvironmental changes (2,6,12,14). The characteristicsof the reviews can be found in Table I. All includedrandomized trials. While the focus of some of thesereviews was active trachoma and infection in children,adults were included in this analysis since mostinterventions to control trachoma are aimed at thecommunity and all the surgery trials were conducted inadults. Subjects in the trials of surgery and trichiasisrecurrence were graded as having major (more thanfive lashes touching the eye) or minor trichiasis (one
to five lashes touching the eye), or as having defectivelid closure.
Data extraction and management
Two authors, Elizabeth Sumamo (primary) and KrystalHarvey, were responsible for the extraction of outcomedata from the four reviews. Tables were created tocapture the statistical measures of interest; relativerisk (RR), risk difference (RD) and control group risk.Three community level trials adjusted for clusteringwithin their published statistics; however the RR andRD presented in this review was calculated at theindividual level without adjusting for clustering in theincluded tables (1,15,16). Any difficulties encounteredduring data extraction were discussed between bothauthors and all statistical issues were resolved withthe assistance of a biostatistician.
Assessment of quality of evidence
All reviews stated that the quality was assessedaccording to the methods set out in Section 6 ofthe Cochrane Handbook for Systematic Reviews ofInterventions using the Cochrane Eyes and VisionGroup Review Development Guidelines.
Data synthesis
The data were extracted from the four systematicreviews and displayed in Tables II, III, IV and V. Onereview had an analysis portion from which RR, RDand control group risk could be directly taken (2). Inthe other three reviews, not all the statistical numberswere expressed in this way. In one study, only oddsratios (OR) were reported and there was insufficientinformation available to calculate RR, RD and controlgroup risk (17). Besides this one instance, uniformreporting across all of the reviews was possible.
Involvement of authors
The team of authors for this overview of reviewsincluded Elizabeth Sumamo and Krystal Harvey whoextracted the data and participated in writing. MatthewBurton and Paul Emerson reviewed the data, edited thedocument and were the main authors for all sections.
Results
Four systematic reviews of 27 studies that examinedinterventions for trachoma control were found withinthe Cochrane Database of Systematic Reviews. Fouradditional recent studies were included due to theirhigh relevance and because they will be includedin future updates of included systematic reviews(16,18,19,20). The details of the individual studiesare found in Tables II, III, IV and V. The interven-tions to control active disease included topical and
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
946 E. Sumamo et al.
Tab
leI.
Cha
ract
eris
tics
ofin
clud
edre
view
s
Tit
leA
utho
rsD
ate
last
upda
ted
Po
pula
tio
nIn
terv
enti
on
Co
mpa
riso
nsO
utco
mes
Ant
ibio
tics
for
trac
hom
a(2
)M
abey
DFr
aser
-Hur
tN
Pow
ellC
Feb
2005
Adu
ltsan
dch
ildre
n•
Topi
cala
ndor
alan
tibio
tics
atan
ydo
seor
frequ
ency
•To
pica
ladm
inist
ratio
nof
antib
iotic
sat
any
dose
orfr
eque
ncy
•Pl
aceb
oor
notr
eatm
ent
•O
rala
dmin
istra
tion
ofan
yan
tibio
tican
dan
ydo
seor
freq
uenc
y
Prim
ary
-A
ctiv
etr
acho
ma
Seco
ndar
y-
Posit
ive
test
for
Chla
myd
iatra
chom
atis
infe
ctio
n-
Adv
erse
side
effe
cts
Face
was
hing
prom
otio
nfo
rpr
even
ting
activ
etr
acho
ma
(14)
Ejer
eH
Alh
assa
nM
BRa
biu
M
Mar
2004
1–
14ye
ars
•Fa
cew
ashi
ngpr
omot
ion
•Fa
cew
ashi
ngpr
omot
ion
and
mas
san
tibio
tictr
eatm
ent
•N
oin
terv
entio
n
•M
ass
antib
iotic
trea
tmen
tal
one
Prim
ary
-A
ctiv
etr
acho
ma
Seco
ndar
y-
Part
icip
ants
with
uncl
ean
face
s-
Seve
retr
acho
ma
Envi
ronm
enta
lsa
nita
ryin
terv
entio
nsfo
rpr
even
ting
activ
etr
acho
ma
(12)
Rabi
uM
Alh
assa
nM
Ejer
eH
Feb
2005
Adu
ltsan
dch
ildre
n•
Fly
cont
rol
•W
ater
prov
ision
•H
ealth
educ
atio
n
•N
oin
terv
entio
nPr
imar
y-
Act
ive
trac
hom
a
Seco
ndar
y-
Fly
dens
ity-
Latr
ine
utiliz
atio
n-
Wat
erut
ilizat
ion
-A
dver
seef
fect
s
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 947
Inte
rven
tions
for
trac
hom
atr
ichi
asis
(6)
Yor
ston
DM
abey
DH
att
SBu
rton
M
Mar
2006
Adu
lts•
Bila
mel
lar
tars
alro
tatio
n
•Bi
lam
ella
rta
rsal
rota
tion
•Ta
rsal
adva
nce
and
rota
tion
•Ev
ersio
nsp
lintin
g•
Tars
alad
vanc
e•
Tars
algr
oovi
ng•
Elec
trol
ysis,
cryo
ther
apy
orbi
lam
ella
rta
rsal
rota
tion
•Bi
lam
ella
rta
rsal
rota
tion
•Ta
rsal
adva
nce
and
rota
tion
•Ep
ilatio
n(m
anua
lrem
oval
ofey
elas
hes
•Po
ster
ior
lam
ella
rta
rsal
rota
tion,
tetr
acyc
line
and
azith
rom
ycin
•Pr
ovid
ing
surg
ery
inpa
rtic
ipan
ts’o
wn
villa
ge•
Surg
ery
byno
n-op
htha
lmol
ogist
inte
grat
edey
eca
rew
orke
rs
•Po
ster
ior
lam
ella
rta
rsal
rota
tion
•N
oco
ntro
lgro
up,
part
icip
ants
rand
omiz
edto
one
ofth
ree
oper
atio
ns
•N
oco
ntro
lgro
up,
part
icip
ants
rand
omiz
edto
one
offiv
eop
erat
ions
•Ta
rsal
adva
nce
and
rota
tion
•Ta
rsal
adva
nce
with
bucc
alm
ucos
alm
embr
ane
graf
t•
Dou
ble-
sided
stic
king
plas
ter
•Po
ster
ior
lam
ella
rta
rsal
rota
tion
and
tetr
acyc
line
•Pr
ovid
ing
surg
ery
inne
ares
the
alth
cent
re•
Surg
ery
byop
htha
lmol
ogist
s
Prim
ary
-Re
curr
ence
oftr
ichi
asis
Seco
ndar
y-
Visu
alac
uity
-A
ccep
tanc
eof
trea
tmen
t
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
948 E. Sumamo et al.
Tab
leII
.Act
ive
Tra
chom
a(T
For
TI)
Aut
hor/
year
Inte
rven
tio
nan
dco
mpa
riso
nN
o.s
ubje
cts
Co
ntro
lgr
oup
risk
[bas
elin
eri
sk]
Ris
kdi
ffere
nce
(95%
CI)
Rel
ativ
eri
sk(9
5%C
I)C
om
men
ts
Ant
ibio
tics
stud
ies
Ora
lant
ibio
tics
vers
usco
ntro
lgro
upD
arou
gar
1980
b(2
5)Tr
eatm
ent:
oral
doxy
cycl
ine,
one
dose
per
mon
thfo
r12
mon
ths
Com
paris
on:v
itam
inpi
lls1
dose
per
mon
thfo
r12
mon
ths
3m
o.91 12
mo.
91
72.3
%
70.2
%
0.00
(−0.
18,0
.19)
−0.1
6,(−
0.35
,0.0
4)
1.01
(0.7
8,1.
29)
0.78
(0.5
6,1.
08)
Hou
seho
ldtr
eatm
ent
Daw
son
1969
i(26
)Tr
eatm
ent:
oral
trisu
lfapy
rimid
ines
3da
ilydu
ring
3co
nsec
utiv
ew
eeks
Com
paris
on:l
acto
se-p
lace
bo3
daily
for
3co
nsec
utiv
ew
eeks
12m
o.36
83.3
%−0
.50
(−0.
78,−
0.22
)0.
40(0
.20,
0.79
)O
nly
activ
etr
acho
ma
case
str
eate
d
Daw
son
1969
ii(2
6)Tr
eatm
ent:
oral
trisu
lfapy
rimid
ines
3da
ilydu
ring
3co
nsec
utiv
ew
eeks
Com
paris
on:l
acto
se-p
lace
bo3
daily
for
3co
nsec
utiv
ew
eeks
3m
o.29
7.1%
0.00
(−0
.19,
0.18
)0.
93(0
.06,
13.5
4)O
nly
activ
etr
acho
ma
case
str
eate
d
Fost
er19
66(4
2)Tr
eatm
ent:
oral
sulp
ham
etho
xypy
ridaz
ine
once
daily
for
5co
nsec
utiv
eda
ysev
ery
wee
kfo
r3
wee
ksC
ompa
rison
:no
trea
tmen
t
3m
o.21
9
12m
o.21
9
82.2
%
63.6
%
−0.0
5(−
0.16
,0.0
5)
0.08
(−0.
04,0
.20)
0.93
(0.8
2,1.
07)
1.12
(0.9
3,1.
35)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Hos
hiw
ara
1973
(27)
Trea
tmen
t:or
aldo
xycy
clin
eon
ceda
ilyfo
r5
cons
ecut
ive
days
ever
yw
eek
upto
28do
ses
in40
days
Com
paris
on:p
lace
boon
ceda
ilyfo
r5
cons
ecut
ive
days
ever
yw
eek
upto
28do
ses
in40
days
3m
o.10
381
.5%
−0.2
4(−
0.42
,−0.
07)
0.70
(0.5
3,0.
92)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Shuk
la19
66(4
3)Tr
eatm
ent
1:to
pica
lsul
phaf
uraz
ole
+su
lpha
dim
etho
xine
twic
eda
ilyfo
r5
cons
ecut
ive
days
ever
ym
onth
for
5m
onth
s/bi
-wee
kly
for
5m
onth
sT
reat
men
t2:
sulp
hadi
met
hoxi
nebi
wee
kly
orw
eekl
ydo
sefo
r5
mon
ths
Com
paris
on:n
otr
eatm
ent
3m
o.12
5
12m
o.12
5
85.7
%
83.3
%
−0.2
2(−
0.37
,−0.
07)
−0.4
0(−
0.55
,−0.
24)
0.74
(0.6
1,0.
91)
0.52
(0.3
9,0.
69)
Onl
yac
tive
trac
hom
aca
ses
trea
ted.
Tre
atm
ents
wer
epo
oled
and
com
pare
dw
ithco
ntro
lO
nly
activ
etr
acho
ma
case
str
eate
d.T
reat
men
tsw
ere
pool
edan
dco
mpa
red
with
cont
rol
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 949
To
pica
lant
ibio
tic
vers
usco
ntro
lgro
upA
ttia
h19
73(4
4)Tr
eatm
ent1
:top
ical
tetr
acyc
line
deriv
ativ
eon
ceev
ery
scho
olda
yfo
r11
wee
ksTr
eatm
ent2
:top
ical
terr
amyc
inon
ceev
ery
scho
olda
yfo
r11
wee
ksC
ompa
rison
:no
trea
tmen
t
3m
o.22
876
.3%
−0.2
1(−
0.33
,−0
.09)
0.72
(0.6
0,0.
88)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Dar
ouga
rTr
eatm
ent:
topi
cal
oxyt
etra
cycl
ine
twic
eda
ilyfo
r7
cons
ecut
ive
days
ever
ym
onth
for
12m
onth
sC
ompa
rison
:vita
min
pills
1do
sepe
rm
onth
for
12m
onth
s
3m
o.85 12
mo.
85
72.3
%
70.2
%
0.04
(−0.
15,0
.23)
−0.2
0(−
0.41
,0.0
0)
1.05
(0.8
2,1.
35)
0.71
(0.4
9,1.
03)
Hou
seho
ldtr
eatm
ent
Fost
er19
66(4
2)Tr
eatm
ent:
topi
calt
etra
cycl
ine
3tim
esda
ilyon
5co
nsec
utiv
eda
ysev
ery
wee
kfo
r6
wee
ksC
ompa
rison
:no
trea
tmen
t
3m
o.21
3
12m
o.21
3
82.2
%
63.6
%
−0.0
8(−
0.19
,−0
.03)
−0.0
2(−
0.15
,0.1
1)
0.91
(0.7
9,1.
04)
0.96
(0.7
8,1.
19)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Peac
h19
86(2
2)Tr
eatm
ent:
topi
calo
ilyte
trac
yclin
eda
ilyfo
r5
days
once
am
onth
for
3m
onth
sC
ompa
rison
:no
trea
tmen
t
3m
o.64
178
.1%
−0.0
9(−
0.15
,−0
.02)
0.89
(0.8
1,0.
98)
Com
mun
ity-w
ide
trea
tmen
t
Shuk
la19
66(4
3)Tr
eatm
ent1
:top
ical
sulp
hafu
razo
le+
oral
sulp
hadi
met
hoxi
netw
ice
daily
for
5co
nsec
utiv
eda
ysev
ery
mon
thfo
r5
mon
ths/
bi-w
eekl
yfo
r5
mon
ths
Tre
atm
ent2
:top
ical
sulp
hafu
razo
letw
ice
daily
for
5co
nsec
utiv
eda
ysev
ery
mon
thfo
r5
mon
ths
Com
paris
on:n
otr
eatm
ent
3m
o.10
4
12m
o.10
4
85.7
%
83.3
%
−0.3
9(−
0.55
,−0
.23)
−0.2
7(−
0.44
,−0
.10)
0.55
(0.4
1,0.
73)
0.68
(0.5
2,0.
88)
Tre
atm
ents
wer
epo
oled
and
com
pare
dw
ithco
ntro
l
Woo
lridg
e19
67(4
5)Tr
eatm
ent:
topi
calt
etra
cycl
ine
twic
eda
ilyfo
r6
cons
ecut
ive
days
per
wee
kfo
r6
wee
ksC
ompa
rison
:no
trea
tmen
t
3m
o.32
2
12m
o.32
2
85.8
%
83.3
%
−0.1
7(−
0.26
,−0
.08)
−0.1
0(−
0.19
,−0
.01)
0.80
(0.7
1,0.
90)
0.89
(0.7
9.0.
99)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Ora
lvs
topi
cala
ntib
ioti
cBo
wm
an20
00(2
4)Tr
eatm
ent:
oral
azith
rom
ycin
(sin
gle
dose
,20
mg/
kg)
Com
paris
on:u
nsup
ervi
sed
6w
eek
cour
seof
topi
cal
tetr
acyc
line
twic
eda
ily
10w
k.29
1
6m
o.29
5
53.2
%
27.0
%
−0.1
7(−
0.28
,−0
.06)
−0.1
5(−
0.24
,−0
.06)
0.65
(0.4
8,0.
86)
0.46
(0.2
8,0.
76)
Onl
yac
tive
trac
hom
aca
ses
trea
ted.
RRan
dRD
are
base
don
per
prot
ocol
anal
ysis;
thos
eth
atm
issed
follo
wup
are
not
incl
uded
(con
tinue
dov
erle
af)
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
950 E. Sumamo et al.
Tab
leII
.(Co
ntin
ued)
Aut
hor/
year
Inte
rven
tio
nan
dco
mpa
riso
nN
o.s
ubje
cts
Co
ntro
lgr
oup
risk
[bas
elin
eri
sk]
Ris
kdi
ffere
nce
(95%
CI)
Rel
ativ
eri
sk(9
5%C
I)C
om
men
ts
Dar
ouga
r19
80b
(25)
Trea
tmen
t:or
aldo
xycy
clin
eon
edo
sepe
rm
onth
for
12m
onth
sC
ompa
rison
:top
ical
oxyt
etra
cycl
ine
twic
eda
ilyfo
r7
cons
ecut
ive
days
ever
ym
onth
for
12m
onth
s
3m
o.82 12
mo.
82
76.3
%
50.0
%
−0.0
4(−
0.22
,0.1
5)
0.05
(−0.
17,0
.26)
0.95
(0.7
5,1.
23)
1.09
(0.7
2,1.
66)
Hou
seho
ldtr
eatm
ent
Daw
son
1997
(28)
Trea
tmen
t1:
oral
azith
rom
ycin
(1do
seof
20m
g/kg
)T
reat
men
t2:
oral
azith
rom
ycin
(1do
se/w
eek
for
3w
eeks
)T
reat
men
t3:
oral
azith
rom
ycin
1do
seev
ery
4w
eeks
for
6do
ses)
Com
paris
on:t
opic
alox
ytet
/pol
ymyx
in+
oral
plac
ebo
once
daily
for
5co
nsec
utiv
eda
ysev
ery
28da
ysfo
r6
times
2m
o.16
0
1yr
.15
9
66.7
%
57.1
%
1D
ose
0.05
(−0.
15,0
.25)
3D
oses
−0.0
9(−
0.30
,0.1
2)
6D
oses
−0.0
3(−
0.23
,0.1
8)
Pool
edtr
eatm
ent
arm −0.0
2(−
0.19
,0.1
4)
1D
ose
−0.0
8(−
0.30
,0.1
3)
3D
oses
−0.1
4(−
0.35
,0.0
8)
6D
oses
0.04
(−0.
17,0
.26)
Pool
edtr
eatm
ent
arm −0.0
6(−
0.23
,0.1
2)
1D
ose
1.08
(0.8
1,1.
44)
3D
oses
0.86
(0.6
1,1.
21)
6D
oses
0.96
(0.7
0,1.
32)
Pool
edtr
eatm
ent
arm
0.97
(0.7
5,1.
24)
1D
ose
0.85
(0.5
6,1.
29)
3D
oses
0.76
(0.4
9,1.
19)
6D
oses
1.08
(0.7
5,1.
54)
Pool
edtr
eatm
ent
arm
0.90
(0.6
5,1.
23)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Fost
er19
66(4
2)Tr
eatm
ent
1:or
alsu
lpha
met
hoxy
pyrid
azin
eon
ceda
ilyfo
r5
cons
ecut
ive
days
ever
yw
eek
for
3w
eeks
Trea
tmen
t2:
topi
calt
etra
cycl
ine
3tim
esda
ilyon
5co
nsec
utiv
eda
ysev
ery
wee
kfo
r6
wee
ksC
ompa
rison
:no
trea
tmen
t
3m
o.21
8
12m
o.21
8
74.5
%
61.3
%
0.02
(−0.
09,0
.14)
0.10
(−0.
02,0
.23)
1.03
(0.8
9,1.
20)
1.16
(0.9
6,1.
41)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Scha
chte
r19
99i(
21)
Trea
tmen
t:or
alaz
ithro
myc
inon
cea
wee
kfo
r3
wee
ks(a
dults
1g,c
hild
ren
20m
g/kg
)C
ompa
rison
:oxy
tetr
acyc
line
once
daily
for
6w
eeks
3m
o.18
25
12m
o.19
41
25.7
%
19.6
%
−0.1
2(−
0.16
,−0
.09)
−0.0
5(−
0.08
,−0
.02)
0.52
(0.4
3,0.
64)
0.74
(0.6
1,0.
90)
Com
mun
ity-
wid
etr
eatm
ent.
Cou
ntry
:Egy
pt
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 951
Scha
chte
r19
99ii
(21)
Tre
atm
ent:
oral
azith
rom
ycin
once
aw
eek
for
3w
eeks
(adu
lts1
g,ch
ildre
n20
mg/
kg)
Com
paris
on:o
xyte
trac
yclin
eon
ceda
ilyfo
r6
wee
ks
3m
o.16
0012
mo.
1197
6.1%
15.7
%
−0.0
1(−
0.04
,0.0
1)
−0.0
7(−
0.11
,−0
.03)
0.76
(0.5
0,1.
15)
0.55
(0.4
0,0.
75)
Com
mun
ity-w
ide
trea
tmen
t.C
ount
ry:T
heG
ambi
a
Scha
chte
r19
99iii
(21)
Tre
atm
ent:
oral
azith
rom
ycin
once
aw
eek
for
3w
eeks
(adu
lts1
g,ch
ildre
n20
mg/
kg)
Com
paris
on:o
xyte
trac
yclin
eon
ceda
ilyfo
r6
wee
ks
3m
o.25
7712
mo.
2276
19.2
%
20.6
%
0.03
(0.0
0,0.
06)
0.04
(0.0
1,0.
07)
1.16
(1.0
0,1.
36)
1.19
(1.0
2,1.
40)
Com
mun
ity-w
ide
trea
tmen
t.C
ount
ry:T
anza
nia
Shuk
la19
66(4
3)Tr
eatm
ent:
oral
sulp
hadi
met
hoxi
nebi
wee
kly
orw
eekl
ydo
sefo
r5
mon
ths
Com
paris
on:s
ulph
afur
azol
etw
ice
daily
for
5co
nsec
utiv
eda
ysev
ery
mon
thfo
r5
mon
ths
3m
o.12
5
12m
o.14
5
85.7
%
56.5
%
−0.2
2(−
0.37
,−0
.07)
−0.1
3(−
0.29
,0.0
3)
0.74
(0.6
1,0.
91)
0.77
(0.5
5,1.
07)
Tre
atm
ents
wer
epo
oled
and
com
pare
dw
ithco
ntro
l
Tabb
ara
1996
(46)
Trea
tmen
t:or
alaz
ithro
myc
in(2
0m
g/kg
)C
ompa
rison
:top
ical
tetr
acyc
line
twic
eda
ilyfo
r5
cons
ecut
ive
days
per
wee
kov
er6
wee
ks
3m
o.64 6
mo.
56
37.5
%
34.6
%
0.09
(−0.
15,0
.33)
0.02
(−0.
23,0
.27)
1.25
(0.7
0,2.
23)
1.06
(0.5
2,2.
15)
Onl
yac
tive
trac
hom
aca
ses
trea
ted
Fac
ew
ashi
ngan
dhe
alth
educ
atio
nF
ace
was
hing
stud
ies
Peac
h19
87(2
2)Tr
eatm
ent
1:Te
trac
yclin
eey
edr
ops
daily
for
one
wee
kev
ery
mon
thfo
r3
mon
ths
Tre
atm
ent
2:Ey
ew
ashi
ngda
ilyfo
r3
mon
ths
Tre
atm
ent
3:Te
trac
yclin
eey
edr
ops
plus
eye
was
hing
Com
paris
on:N
otr
eatm
ent
3m
o.11
4375
.8%
Eye
drop
s−0
.09
(−0.
16,−
0.01
)
Eye
was
hing
0.02
(−0.
06,0
.10)
Eye
drop
s+
eye
was
hing
−0.0
7(−
0.15
,0.0
1)
Eye
drop
s0.
88(0
.79,
0.98
)
Eye
was
hing
1.02
(0.9
3,1.
13)
Eye
drop
s+
eye
was
hing
0.91
(0.8
2,1.
01)
No
met
a-an
alys
isco
nduc
ted
astr
ials
diffe
red
inse
vera
lre
spec
ts.
All
part
icip
ants
lost
tofo
llow
upas
sum
edto
have
follic
les
atth
een
dof
the
stud
yan
din
tent
ion
totr
eat
prin
cipl
ew
asap
plie
din
the
anal
ysis
ofre
sults
.W
est1
995
(17)
Trea
tmen
t:Fa
cew
ashi
ngpr
omot
ion
com
bine
dw
ithm
ass
tetr
acyc
line
oint
men
tC
ompa
rison
:Mas
ste
trac
yclin
eoi
ntm
ento
nly.
12m
o.14
17Pa
ir1
60%
Pair
250
%Pa
ir3
65%
Tet
racy
clin
eoi
ntm
ent
was
adm
inist
ered
topi
cally
once
daily
for
30da
ys.R
elat
ive
risk
and
risk
diffe
renc
esap
prox
imat
edfro
mpe
rcen
tage
s.D
iffer
ence
sar
eno
tst
atist
ical
lysig
nific
ant.
How
ever
,aut
hors
dono
tre
port
the
RRan
dRD
valu
es.
OR:
0.81
(0.4
2,1.
59)
(con
tinue
dov
erle
af)
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
952 E. Sumamo et al.
Tab
leII
.(Co
ntin
ued)
Aut
hor/
year
Inte
rven
tio
nan
dco
mpa
riso
nN
o.s
ubje
cts
Co
ntro
lgr
oup
risk
[bas
elin
eri
sk]
Ris
kdi
ffere
nce
(95%
CI)
Rel
ativ
eri
sk(9
5%C
I)C
om
men
ts
Hea
lth
Edu
cati
on
Resn
ikof
f199
5(2
3)Tr
eatm
ent:
Hea
lthed
ucat
ion
one
wee
kpe
rm
onth
for
6m
onth
s.C
ompa
rison
:No
heal
thed
ucat
ion
6m
o.18
107.
1%−0
.03
(−0.
06,0
.00)
0.59
(0.3
4,1.
04)
Com
paris
ons
wer
eon
lydo
nebe
twee
non
evi
llage
and
the
cont
rolv
illage
.Ed
war
ds20
06(1
8)Tr
eatm
ent:
Com
mun
ities
targ
eted
byN
GO
san
dSA
FEst
rate
gy(s
urge
ry,a
ntib
iotic
s,fa
cew
ashi
ng,a
nden
viro
nmen
tal
impr
ovem
ents
)w
hich
rece
ived
radi
obr
oadc
asts
and
may
have
rece
ived
vide
osc
reen
ings
.C
ompa
rison
:Com
mun
ities
rece
ived
radi
obr
oadc
asts
only
12m
o.18
4266
.7%
−0.0
4(−
0.09
,0.0
1)0.
94(0
.87,
1.01
)
Env
iro
nmen
tals
tudi
esF
lyco
ntro
lint
erve
ntio
nsEm
erso
n19
99(1
5)Tr
eatm
ent:
spra
yw
ith0.
175%
volu
me
tovo
lum
ede
ltam
ethr
inup
to20
mou
tsid
eea
chvi
llage
.T
wic
ew
eekl
yin
the
wet
seas
onan
don
cew
eekl
yin
the
dry
seas
onfo
r3
mon
ths.
Com
paris
on-
No
inse
ctic
ide
spra
y.
3m
o.11
3415
.7%
−0.1
0(−
0.10
,−0
.09)
∗0.
39(0
.27,
0.56
)∗Bo
thEm
erso
n19
99an
dEm
erso
n20
04as
sess
inse
ctic
ide
spra
ybu
tno
met
a-an
alys
isco
nduc
ted
beca
use
ofsig
nific
ant
clin
ical
hete
roge
neity
.Em
erso
n20
04(1
)Tr
eatm
ent:
Spra
yw
ithw
ater
solu
ble
perm
ethr
info
r6
mon
ths.
Com
paris
on:N
oin
terv
entio
n
6m
o.48
506.
2%−0
.04
(−0.
04,
−0.0
3)∗
0.44
(0.3
3,0.
59)∗
Wes
t200
6(1
6)In
terv
entio
n:A
llm
embe
rsof
inte
rven
tion
balo
ziw
ere
give
na
singl
edo
seof
azith
rom
ycin
and
then
hous
ehol
dsan
dsu
rrou
ndin
gar
eas
wer
esp
raye
dw
ithin
sect
icid
e(1
0%pe
rmet
hrin
inw
ater
)th
roug
hout
the
year
.C
ompa
rison
:All
mem
bers
ofco
ntro
lbal
oziw
ere
give
na
singl
edo
seof
azith
rom
ycin
.
6m
o.22
9
12m
o.20
6
33%
44%
−0.1
3(−
0.25
,−0
.02)
∗
−0.0
1(−
0.15
,0.
13)∗
0.60
(0.3
7,0.
96)∗
0.97
(0.7
0,1.
34)∗
Obs
erva
tions
wer
eon
child
ren
aged
<8
year
s.O
bser
vatio
nsw
ere
onch
ildre
nag
ed<
8ye
ars.
Lat
rine
pro
visi
on
Emer
son
2004
(1)
Trea
tmen
t:La
trin
epr
ovisi
onC
ompa
rison
:No
inte
rven
tion
6m
o.28
366.
2%−1
.21
(1.2
2,−1
.20)
∗0.
72(0
.53,
0.96
)∗A
naly
sisw
asby
clus
ter,
and
not
indi
vidu
aln
=7
inea
chgr
oup.
∗ The
RRan
dRD
isca
lcul
ated
inth
isre
view
atth
ein
divi
dual
leve
lwith
out
adju
stin
gfo
rcl
uste
ring.
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 953
Only those with severetrachoma at baseline wereincluded
West 1995 (17) Treatment: Face washingpromotion combined withmass tetracycline ointmentComparison: Masstetracycline ointment only.Tetracycline ointment wasadministered topically oncedaily for 30 days.
12 mo.1417(totalnum-ber ofpartici-pantsin trial)
Informationnotavailable
This paper only presentsodds ratios for theintervention villages
Severe trachoma: 0.62 (0.40,0.97)
Any trachoma: 0.81 (0.42,1.59)
Schachter 1999i(21)
Treatment: oral azithromycinonce a week for 3 weeks(adults 1 g, children20 mg/kg)Comparison: oxytetracyclineonce daily for 6 weeks
12 mo.1938 4.6% 0.01 (0.00, 0.03) 1.37 (0.91,
2.07)Community-wide treatment.Country: Egypt
Schachter 1999ii(21)
Treatment: oral azithromycinonce a week for 3 weeks(adults 1 g, children20 mg/kg)Comparison: oxytetracyclineonce daily for 6 weeks
12 mo.1197 7.1% 0.00 (−0.02, 0.01) 0.83 (0.40,
1.70)Community-wide treatment.Country: The Gambia
Schachter 1999iii(21)
Treatment: oral azithromycinonce a week for 3 weeks(adults 1 g, children20 mg/kg)Comparison: oxytetracyclineonce daily for 6 weeks
12 mo.2213 8.4% 0.03 (0.01, 0.04) 1.74 (1.17,
2.58)Community-wide treatment.Country: Tanzania
oral antibiotics at any dose or frequency, face wash-ing promotion with or without antibiotic treatment, flycontrol, and health education. Interventions for trichi-asis included bilamellar tarsal rotation, tarsal advanceand rotation, eversion splinting, tarsal advance, tarsal
grooving, electrolysis, cryotherapy, epilation, posteriorlamellar tarsal rotation, tetracycline and azithromycinat surgery, providing surgery in participants’ own vil-lage, and surgery by non-ophthalmologist integratedeye care workers.
Table IV. Chlamydia trachomatis infection
Author/year
Intervention andcomparison No. subjects
Control grouprisk Risk difference
Relative risk(95% CI) Comments
Antibiotic versus controlDarougar 1980b(25)
Treatment 1: topicaloxytetracycline twice daily for7 consecutive days everymonth for 12 monthsTreatment 2: oraldoxycycline one dose permonth for 12 monthsComparison: vitamin pills 1dose per month for12 months
Treatment: oral doxycyclineonce daily for 5 consecutivedays every week up to 28doses in 40 daysComparison: placebo oncedaily for 5 consecutive daysevery week up to 28 doses in40 days
3 mo.103 53.7% −0.05 (−0.24,
0.15)0.81 (0.63, 1.04)
Oral versus topical antibioticDawson 1997(28)
Treatment 1: oralazithromycin (1 dose of20 mg/kg)Treatment 2: oralazithromycin (1 dose/weekfor 3 weeks)Treatment 3: oralazithromycin 1 dose every4 weeks for 6 doses)Comparison: topicaloxytet/polymyxin + oralplacebo once daily for 5consecutive days every28 days for 6 times
3 mo.160
12 mo.138
7.3%
15.2%
−0.03 (−0.12,0.06)
−0.08 (−0.22,0.05)
0.57 (0.14, 2.30)
0.44 (0.15, 1.29)
Schachter 1999i(21)
Treatment: oral azithromycinonce a week for 3 weeks(adults 1g, children 20 mg/kg)Comparison: oxytetracyclineonce daily for 6 weeks
3 mo.1782
12 mo.1914
4.5%
6.2%
−0.04 (−0.05,−0.02)
−0.03 (−0.05,−0.01)
0.22 (0.11, 0.44)
0.48 (0.31, 0.74)
Community-widetreatment
Schachter 1999ii(21)
Treatment: oral azithromycinonce a week for 3 weeks(adults 1 g, children20 mg/kg)Comparison: oxytetracyclineonce daily for 6 weeks
3 mo.1453
12 mo.1126
13.6%
13.5%
−0.07 (−0.10,−0.04)
−0.05 (−0.09,−0.01)
0.51 (0.37, 0.70)
0.62 (0.44, 0.87)
Community-widetreatment
Schachter 1999iii(21)
Treatment: oral azithromycinonce a week for 3 weeks(adults 1 g, children20 mg/kg)Comparison: oxytetracyclineonce daily for 6 weeks
3 mo.2538
12 mo.2236
6.2%
8.0%
−0.02 (−0.04,0.00)
0.00 (−0.02, 0.02)
0.68 (0.49, 0.95)
1.01 (0.76, 1.35)
Community-widetreatment
Darougar 1980b(25)
Treatment 1: topicaloxytetracycline twice daily for7 consecutive days everymonth for 12 monthsTreatment 2: doxycyclineone dose per month for12 monthsComparison: vitamin pills 1dose per month for12 months
3 mo.82
12 mo.82
2.6%
2.6%
0.13 (0.01, 0.25)
−0.03 (−0.05,0.00)
6.05 (0.78, 46.95)
2.59 (0.28, 23.88)
Active Trachoma
Antibiotics and active trachoma
One review examined the antibiotic arm of theSAFE strategy by measuring the effects of antibi-otic treatment on both active trachoma and Chlamy-dia trachomatis infection of the conjunctiva (defined
as a positive nucleic acid amplification test resultfrom an ocular swab) (2). There were 15 includedtrials that randomized 8,678 participants and lookedfor the presence of active trachoma at either threeor 12 months after starting treatment. The reviewdivided the analysis of studies into those who receivedany antibiotics (topical or oral) versus placebo/no
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 955
treatment and those who received oral versus topi-cal antibiotics. Trial participants were usually residentin areas where trachoma is endemic, but were froma number of different countries and resided in vari-ous locations, including villages and boarding schools.One set of studies randomized entire communitiesrather than individuals to the intervention (21). TheWHO currently recommends either topical tetracyclineor oral azithromycin for individual and mass treatmentof trachoma, although the studies have used variousantibiotic treatment regimens.
(A) Antibiotics versus placebo/no treatment Summary statisticscould not be performed in studies where oral andtopical antibiotics were compared with placebo or withno treatment due to the degree of heterogeneity.
(I) Active trachoma at three monthsWhen measuring the effect of treatment with antibi-
otics on active trachoma at three months, the pointestimates were consistent with the antibiotics havingan effect with a risk reduction. The results were asfollows:
(a) any antibiotic(i) RR < 1 in six trials (P < 0.05)
(ii) RR < 1 in two trials (non significant(n.s.))
(iii) RR > 1 in one trial (n.s.)(b) oral antibiotics
(i) RR < 1 in three trials (P < 0.05)(ii) RR < 1 in two trials (n.s.)
(iii) RR > 1 in one trial (n.s.)(c) topical antibiotics
(i) RR < 1 in four trials (P < 0.05)(ii) RR < 1 in one trial (n.s.)
(iii) RR > 1 in one trial (n.s.)(II) Active trachoma at 12 months
The relative risks of study participants exhibitingactive trachoma at 12 months after treatment withantibiotic were consistent with there being no effect ofantibiotics at 12 months. The results are as follows:
(a) any antibiotic(i) RR < 1 in three trials (P < 0.05)
(ii) RR > 1 in three trials (n.s.)(b) oral antibiotics
(iii) RR < 1 in one trial (P < 0.05)(iv) RR < 1 in one trial (n.s.)(v) RR > 1 in one trial (n.s.)
(c) topical antibiotics(vi) RR < 1 in two trials (P < 0.05)
(vii) RR < 1 in two trials (n.s.)
(B) Oral antibiotics versus topical antibiotics When azithromy-cin or other oral antibiotics were compared withtopical tetracycline or other topical antibiotics, thedata suggest that oral antibiotics are neither morenor less effective than topical antibiotic treatment inreducing the prevalence of active trachoma after threeor 12 months.
When oral azithromycin versus topical tetracyclinewere compared, the point estimates of relative risk ofactive trachoma at three months were as follows:
(i) RR < 1 in two trials (P < 0.05)(ii) RR < 1 in two trials (n.s.)
(iii) RR > 1 in two trials (n.s.)
When other oral and topical antibiotics were com-pared, the relative risks of active trachoma at threemonths were as follows:
(i) RR < 1 in one trial (P < 0.05)(ii) RR < 1 in one trial (n.s.)
(iii) RR > 1 in one trial (n.s.)
When oral azithromycin versus topical tetracyclinewere compared, the point estimates of relative risk ofactive trachoma at 12 months were as follows:
(i) RR < 1 in two trials (P < 0.05)(ii) RR < 1 in one trial (n.s.)
(iii) RR > 1 in one trial (n.s.)
When other oral and topical antibiotics were com-pared, the relative risks of active trachoma at 12 mon-ths were as follows:
(i) RR < 1 in one trial (n.s.)(ii) RR > 1 in two trials (n.s.)
All of the trials were of poor to moderate qualityand intention to treat analysis was not performed inmost of them.
Face washing and active trachoma
There were only two trials included in the face wash-ing review. They employed different interventions andmeasured different outcome measures and therefore,meta-analysis was deemed inappropriate.
Face washing promotion combined with mass tetracycline ointmentversus mass tetracycline ointment only In the one studythat included this comparison, three pairs of villageswere recruited and one of each pair randomly assignedto tetracycline eye ointment only, with the otherassigned to combined intervention of tetracycline eyeointment plus a community-based behaviour changeprogram to promote face washing (17). All pre-schoolchildren in all villages were screened for clinicalsigns of trachoma at baseline and after 12 months. Inone pair of villages at 12 months, the prevalence ofactive trachoma (WHO grade TF) was lower in thevillage that received the combination of face washingand antibiotics (55%) than the village that receivedantibiotics alone (60%). In a second pair, the sametrend occurred and lower levels of active trachomawere found in the combination village (40%) than theantibiotic alone village (50%). In the third village, inwhich there had been poor uptake of the behaviourchange program, statistically similar levels of activetrachoma were seen in the combination village (70%)
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
956 E. Sumamo et al.
Tab
leV
.Rec
urre
nce
oftr
acho
ma
tric
hias
is
Aut
hor/
year
Inte
rven
tio
nan
dco
mpa
riso
nN
o.
subj
ects
Co
ntro
lgr
oup
risk
[tri
chia
sis
atfo
llow
-up]
Ris
kdi
ffere
nce
Rel
ativ
eri
sk(9
5%C
I)C
om
men
ts
Surg
ery
tech
niqu
eA
dam
u20
02(2
9)1)
Bila
mel
lar
Tars
alRo
tatio
n(B
TR)
2)Ta
rsot
omy
(Tra
nsve
rse
Tars
otom
yan
dlid
mar
gin
Rota
tion
=TT
R)
3m
o.15
3pa
tient
s(2
56ey
es)
Min
ortr
ichi
asis
4.9%
Maj
ortr
ichi
asis
16.0
%
Min
ortr
ichi
asis
(TTR
asco
ntro
l)0.
06(−
0.07
,0.1
8)
Maj
ortr
ichi
asis
(TTR
asco
ntro
l)−0
.06
(−0.
16,0
.05)
Min
ortr
ichi
asis
(TTR
asco
ntro
l)2.
12(0
.38,
11.9
)
Maj
ortr
ichi
asis
(TTR
asco
ntro
l)0.
65(0
.29,
1.44
)Re
ache
r19
90(3
0)In
terv
entio
n:M
ean
follo
wup
per
grou
p7.
4to
8.8
mo.
Bila
mel
lar
tars
alro
tatio
n(B
TR)
Con
trol
s:1)
76ey
es1)
88.6
%1)
−0.3
1(−
0.52
,−0.
11)
1)0.
35(0
.17,
0.75
)
1)Ta
rsal
groo
ving
(TG
)2)
Tars
alad
vanc
ean
dro
tatio
n(T
AR)
3)Ev
ersio
nsp
lintin
g(E
S)4)
Tars
alad
vanc
e(T
A)
2)65
eyes
3)65
eyes
4)82
eyes
2)54
.2%
3)70
.8%
4)73
.2%
2)−0
.21
(−0.
45,0
.02)
3)−0
.37
(−0.
60,−
0.14
)
4)−0
.37
(−0.
56,−
0.17
)
2)0.
53(0
.27,
1.06
)
3)0.
32(0
.15,
0.68
)
4)0.
32(0
.15,
0.66
)Re
ache
r19
92(3
1)M
inor
Tric
hias
isTr
ial
9m
o.fo
llow
-up
1)Bi
lam
ella
rta
rsal
rota
tion
2)El
ectr
olys
is3)
Cry
othe
rapy
166
eyes
62.3
%−0
.51
(−0.
63,−
0.38
)0.
19(0
.09,
0.40
)M
inor
Tric
hias
is
Maj
orTr
ichi
asis
Tria
l9
or21
mo.
afte
rfo
llow
-up
1)Bi
lam
ella
rta
rsal
rota
tion
2)Ta
rsal
adva
nce
and
rota
tion
199
eyes
45.5
%−0
.27
(−0.
40,−
0.15
)0.
40(0
.25.
0.64
)M
ajor
Tric
hias
is
No
n-o
pera
tive
trea
tmen
tG
raz
1999
(32)
1)St
icki
ngpl
aste
r12
wee
ks2)
Stic
king
plas
ter
8w
eeks
and
epila
tion
4w
eeks
3)Ep
ilatio
non
ly
12w
eeks
3910
0%12
wee
kspl
aste
rvs
.Ep
ilatio
n−0
.71
(−0.
92,−
0.51
)
12w
eeks
plas
ter
vs.E
pila
tion
0.29
(0.1
5,0.
56)
100%
Cov
erag
e
Ant
ibio
tic
trea
tmen
tBu
rton
2005
(33)
1)U
nila
mel
lar
surg
ery
acco
mpa
nied
byun
supe
rvise
dte
trac
yclin
eey
eoi
ntm
ent
twic
ea
day
for
2w
eeks
asw
ella
ssin
gle
dose
azith
rom
ycin
toth
epa
tient
atsu
rger
yan
dsix
mon
ths.
Fam
ilym
embe
rsw
ere
also
trea
ted
with
azith
rom
ycin
atbo
thoc
casio
ns.
6m
o.41
0
12m
o.42
6
26.1
%
41.4
%
0.11
(0.0
2,0.
20)
0.00
(−0.
10,0
.09)
1.43
(1.0
7,1.
91)
0.99
(0.7
9,1.
25)
Med
ian
ages
ofth
egr
oups
are
57.3
and
57.2
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 957
2)U
nila
mel
lar
surg
ery
and
unsu
perv
ised
tetr
acyc
line
eye
oint
men
ttw
ice
ada
yfo
r2
wee
ksW
est
2006
(19)
1)Tr
ichi
asis
surg
ery
follo
wed
byW
hen
recu
rren
cew
asde
tect
edor
at12
mo.
1gof
oral
azith
rom
ycin
for
the
patie
ntor
singl
e-do
seaz
ithro
myc
in(2
0m
g/kg
upto
1g)
for
the
patie
ntan
dal
lhou
seho
ldm
embe
rs2)
Tric
hias
issu
rger
yfo
llow
edby
twic
epe
rda
yto
pica
ltet
racy
clin
efo
rsix
wee
ks
1406
6.8%
−0.0
3(−
0.06
,−0.
01)
0.53
(0.3
3,0.
85)
Mea
nag
esw
ere
50(h
ouse
hold
azith
rom
ycin
),48
.5(p
atie
nton
lyaz
ithro
myc
in),
and
48(t
etra
cycl
ine)
Zha
ng20
06(2
0)1)
Bila
mel
lar
tars
alro
tatio
nsu
rger
yan
da
singl
edo
seof
azith
rom
ycin
imm
edia
tely
afte
rsu
rger
y2)
Bila
mel
lar
tars
alro
tatio
nsu
rger
yan
dpl
aceb
oad
min
ister
edaf
ter
surg
ery
∗A
llpa
tient
sw
ithac
tive
trac
hom
aor
infla
mm
ator
ytr
acho
ma
rece
ived
tetr
acyc
line
oint
men
tat
base
line
and
follo
wup
.
6m
o.11
112
mo.
114
27.6
%
28.1
%
−0.0
1(−
0.18
,0.1
5)
0.02
(−0.
15,0
.18)
0.96
(0.5
2,1.
77)
1.06
(0.6
0,1.
89)
81.7
%of
popu
latio
nw
asag
ed>
40ye
ars.
Sur
gery
sett
ing
Bow
man
2000
(34)
1)Su
rger
yin
villa
ge2)
Surg
ery
inhe
alth
cent
re3
mo.
896.
3%0.
03(−
0.09
,0.1
4)1.
40(0
.29,
6.83
)M
edia
nag
ew
as53
and
56ye
ars
Cov
erag
ew
as66
%in
the
villa
gean
d44
%in
the
heal
thca
rece
ntre
s.P
erso
nnel
perf
orm
ing
surg
ery
Ale
may
ehu
2004
(35)
1)Bi
lam
ella
rta
rsal
rota
tion
carr
ied
out
byin
tegr
ated
eye
wor
ker
2)Bi
lam
ella
rta
rsal
rota
tion
3m
o.73
1
6m
o.
12.1
%−0
.03
(−0.
07,0
.02)
0.78
(0.5
1,1.
18)
3.2%
ofth
epo
pula
tion
wer
ech
ildre
nyo
unge
rth
an15
year
s.ca
rrie
dou
tby
At
sixm
onth
s,au
thor
sdi
dno
tre
port
spec
ific
recu
rren
cera
tes.
Aut
hors
repo
rted
nost
atist
ical
opht
halm
olog
istdi
ffere
nce
inre
curr
ence
betw
een
the
2ty
pes
ofsu
rgeo
ns.
(con
trol
)
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
958 E. Sumamo et al.
and in the antibiotics alone village (65%). There wasan overall reduction in the odds of trachoma (WHOgrade TF) in the combined combination villages thanin the antibiotics alone villages, but this effect was notstatistically significant: OR: 0.81 (0.42, 1.59).
Tetracycline eye drops plus eye washing, eye drops alone, eyewashing alone versus no treatment Another study assessedthe efficacy of tetracycline drops alone, eye washingalone as well as their use in combination in reducingtrachoma infection (22). The relative risks of folliclesbeing seen at three months for each interventioncompared to controls were as follows:
The results suggested no statistically significantbenefit from tetracycline eye drops and eye washing,or eye washing alone compared to no intervention. Amodest benefit from eye drops alone compared to nointervention was reported.
Health education and active trachoma
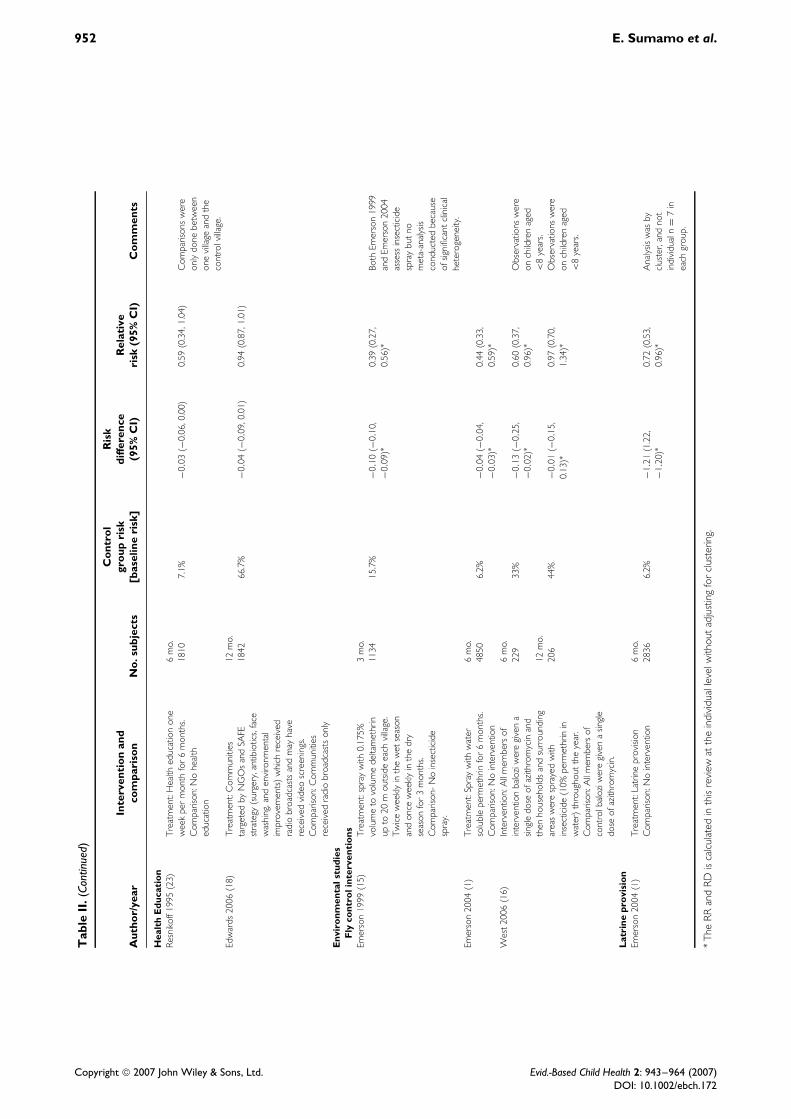
Two studies measured active trachoma after a healtheducation intervention was delivered. One study founda significant decrease in relative risk associated withhealth education when compared to no education (23).The intervention included weekly information regard-ing personal and family hygiene and household sani-tation. Another study compared the rate of active tra-choma in communities targeted by non-governmentalorganizations (NGOs) and the SAFE strategy thatreceived radio broadcasts and video screenings againstcommunities who were not targeted by NGOs and whoonly received radio broadcasts (18). No significant dif-ferences in the rate of active trachoma at one year wereobserved between communities targeted by the SAFEstrategy and those who were not, but a small signifi-cant reduction was observed at the one year follow upcompared to the baseline survey (18).
Environmental factors
Three trials assessed the environmental arm of theSAFE Strategy (1,15,16). Emerson et al. 2004 lookedat the effect of insecticide spray and latrine provisionwhilst Emerson et al. 1999 and West et al. assessedinsecticide spray only. Meta-analysis was inappropri-ate due to significant heterogeneity between trials.
Insecticide spray versus no intervention on active trachomaAt three months one study, in which two pairs ofvillages were recruited and one of each pair randomlyassigned to insecticide spray whilst the other was acontrol, found there to be a prevalence of 6.2% in theintervention villages compared to 15.7% in the controlvillages (15). The relative risk of active trachoma at
three months was 0.39 (0.27, 0.56) suggesting thatinsecticide spray significantly reduced the magnitudeof active trachoma. In a second study, in which therewere seven pairs of insecticide spray and controlvillages, clinical signs of active trachoma (WHOgrade TF) were 55.8% lower in the interventionclusters compared to the control (1). The relative riskwas 0.44 (0.33, 0.59) at six months, indicating thatcommunity-wide insecticide spray also significantlyreduced the magnitude of active trachoma in thisstudy. A third study found a significant reduction (RR:0.60 (0.37, 0.96)) in active trachoma in children at sixmonths when insecticide spray was used on controlneighbourhoods rather than villages (16). When thisdifference was analysed by neighbourhood, however,a non-significant reduction was observed. There wereno significant differences in active trachoma betweenintervention and control groups at one year in thisstudy.
Latrine provision versus no intervention on active trachoma Theone study that looked at latrine provision found a29.5% reduction of active trachoma at six months(WHO grades TF and TI combined) in the clustersthat received latrines compared to the controls (1). Therelative risk was 0.72 (0.53, 0.96) when analysed atthe individual level, although the confidence intervalincluded 1.0 when analysed at the community level.
Severe trachoma (WHO grade TI)
Five trials captured data on the prevalence of severetrachoma (WHO grade TI). Detailed statistics fromthese studies are found in Table III. One trial used aface washing intervention while the others used antibi-otics (17,21,24). In the face washing trial the overallprevalence of severe trachoma was lower in childrenfrom the village from each of the three pairs that hadreceived a combination of face washing and antibi-otics (8%) than the villages that had received antibioticalone (14%) at 12 months. This difference was foundto be statistically significant: OR: 0.62 (0.40, 0.97).In the other studies the efficacy of oral azithromycinwas compared to that of tetracycline in three differentcountries, Egypt, The Gambia and Tanzania (21,24).One study found a significant effect of azithromycinover tetracycline at six months, whilst another studyfound no difference between azithromycin and tetra-cycline at 12 months (21,24).
Ocular infection with Chlamydia trachomatis
Antibiotics versus placebo or no treatment
When looking at C. trachomatis infection at threemonths, the point estimates in all four trials suggesteda reduced risk in the antibiotic group (2,25,26,27).However, none found a significant difference betweenthe pooled antibiotic and control groups (2). Onlyone trial reported outcomes at 12 months and found asignificantly reduced risk in the antibiotic group (25).
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 959
Oral antibiotics versus topical antibiotics
There were five trials assessing oral versus topi-cal antibiotics on C. trachomatis infection. At threemonths, a significant reduction in relative risk wasfound in three of the four trials that comparedazithromycin to a topical antibiotic whilst the fourthshowed a non-significant reduction (21,28). At 12months, there was a significant reduction in two tri-als, Dawson et al. found some reduction and Schachteret al. showed some increase (21,28). The fifth trialcompared oral doxycycline with topical oxytetracy-cline and found a non-significant increase at both threeand 12 months (25).
Process indicators
Active and severe trachoma and evidence of infectionwith Chlamydia trachomatis are the endpoints of mosttrials and have been discussed above. However, thereviews also assessed process indicators (clean facesand fly-eye contact) that are not in the tables and arereported in the narrative below.
Clean faces
In the only face-washing study that addressed thisoutcome, the percentage of children with clean facesincreased in both the combination face washing plusantibiotic villages and the antibiotic alone villages, incomparison to the controls (17). The effect was greaterin the face washing plus antibiotic combination vil-lages compared to the antibiotic alone villages: facewashing and antibiotic combination; 18% at baseline;to 33% at six months; and 35% at 12 months, com-pared to the antibiotic alone group: 19% at baseline;30% at six months; and 26% at 12 months. The dif-ference between the groups was statistically significant(P < 0.05).
Fly-eye contact
Two studies measured frequencies of fly-eye contact asa process indicator (1,15). The first study reported thatfly-eye contact by the trachoma vector, Musca sorbens,was decreased by 96% with the community-widespraying of deltamethrin in comparison to controls.The second study reported a reduction in fly-eyecontact by Musca sorbens of 88% with community-wide insecticide spraying with permethrin, and a30% reduction in villages that had received latrineprovision compared to controls. All three reductionswere statistically significant (P < 0.05).
Trichiasis surgery
The antibiotic, face washing and environmental com-ponents of the SAFE strategy are used to con-trol Chlamydia trachomatis transmission. The surgerycomponent aims to correct trachomatous trichiasis,which occurs as a result of repeated cycles of infec-tion and resolution of ocular Chlamydia infection; is
not, in itself, caused by current active trachoma. Theprimary outcome of surgery trials is usually the rateof recurrence of trichiasis after surgery. See Table Vfor results from the surgery trials.
Surgery techniques
In one study, there was no significant difference in therecurrence rate at three months between the bilamellartarsal rotation and transverse tarsotomy and lid marginrotation (similar to Trabut method) (29). In anotherstudy, bilamellar tarsal rotation was no more effectivethan tarsal advance and rotation RR: 0.53 (0.27,1.06), tarsal grooving RR: 0.35 (0.17, 0.75), eversionsplinting RR: 0.32 (0.15, 0.68) or tarsal advance RR:0.32 (0.15, 0.66) (30). In a third study, however,bilamellar tarsal rotation was more effective in treatingthose with minor trichiasis (one to five lashes touchingthe eye) than destroying the lashes by cryotherapy orelectrolysis RR: 0.19 (0.09, 0.40) (31). In those withmajor trichiasis (six or more lashes touching the eye),bilamellar tarsal rotation was more effective than tarsaladvance and rotation RR: 0.40 (0.25, 0.64). Therewas insufficient enrolment to assess these outcomesin those with defective lid-closure.
Non-operative treatment of trichiasis
At three months, one study found that using stickingtape alone was significantly more effective than epila-tion alone RR: 0.29 (0.15, 0.56) (32). The differencebetween epilation alone and sticking tape followedby epilation was not statistically significant (P = 0.5).The authors reported good clinical status as: no lashestouching the eyeball, complete lid closure, no con-junctival hyperaemia and no unplanned treatment nec-essary during follow up.
Post-operative antibiotic treatment
Three trials have examined the effect of post-operativeazithromycin on the recurrence of trichiasis (19,20,33).Two of these were published subsequent to the lastupdate of the surgery review (20,19). One trial foundno difference in trichiasis recurrence rates betweenpatients who had received post operative azithromycin(41.2%) and those who did not (41.4%) when assessedat 12 months (33). Another trial found no differencein the cumulative incident trichiasis recurrence ratesbetween the azithromycin treated group (29.8%) andthe placebo group (28.1%) at 12 months (20). Addi-tional sub-set analysis suggested that there may besome benefit from azithromycin for individuals whohad major trichiasis. The third and largest study con-cluded that a single dose of azithromycin was asso-ciated with a 33% reduction in trichiasis recurrence,compared with a 6-week regimen of topical tetracy-cline (19).
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
960 E. Sumamo et al.
Surgery setting
One study that assessed people with major trichiasisfound that there were similar success rates (no recur-rence) between patients randomized to village-basedsurgery (91%) and health centre-based surgery (94%)at three months (34). In another study, the trichia-sis recurrence rates among patients who had surgeriesconducted by an ophthalmologist was 12.7%, com-pared to 9.9% among patients operated by an inte-grated eye care worker at three months (35). Thedifference was small and did not achieve statisticalsignificance, OR: 1.32 (0.83, 2.11). At six months,the difference between recurrence rates was again notstatistically significant.
Visual acuity as a surgical outcome
There were four trials in the surgery review thatassessed visual acuity following surgical and non-operative interventions. One trial reported that trichia-sis surgery improved vision but the degree of improve-ment was not quantified; however it was not statisti-cally significant (29). Another study found a statisti-cally significant improvement of about half a line ofSnellen Visual Acuity (P < 0.0001) following surgeryfor major trichiasis, but not those with minor trichia-sis (31). A third study reports an overall improvementin visual acuity of 0.14 LogMAR units 12 monthsafter surgery (P < 0.0001), however the data were notreported by randomization groups (33). Follow-up datawere not presented in the fourth study (35).
Uptake of surgical intervention
The uptake of intervention was only recorded in threestudies. One study reports that 38 participants refusedrandom allocation, with the refusal rate greater in thedefective lid closure group (31). Another study did notrecord attendance for treatment but mentions that therewere compliance issues (32). The third study statesthat surgical uptake was higher for those randomizedto village-based surgery (66%) than those who wererandomized to the health centre-based surgery (44%)(34).
Quality of life following surgery
Burton et al. examined quality of life after surgery,although this was not analyzed by randomizationgroup (33). Among all study participants, 77% reportedan improvement in vision and 94% felt more comfortin the operated eye.
Economic evaluation of surgery
Journey time and cost of travel was significantly lessfor clusters randomized to community-based surgerythan for those randomized to health centre-basedsurgery (34).
Adverse events related to surgery
Four studies reported on adverse events. No detailswere given but one study stated that lid-notchingand pyogenic granuloma were more common in thebilamellar than the posterior lamellar tarsal rotationoperations (29). The second study reported one caseof over-correction following bilamellar rotation andgranulomas in two lids (30). The third study reportedtwo cases of over-correction following bilamellartarsal rotations but none in the tarsal advance androtation group (31). The fourth study reported thatpatients found epilation to be less comfortable thansticking tape (P = 0.002) among those with unilateraltrichiasis (32).
Discussion
Trichiasis surgery
The authors of the Cochrane review on interventionsfor trachomatous trichiasis concluded that the mostsuccessful operation type involves full thickness inci-sion of the tarsal plate. Two main procedures arecurrently in use in most trachoma endemic settings:the bilamellar tarsal rotation and the unilamellar tarsalrotation. No convincing evidence was found that oneprocedure is better than the other, although the unil-amellar technique varied between studies. For minortrichiasis there is evidence that tarsal rotation surgeryis more effective than non-surgical techniques includ-ing cryotherapy and electrolysis. For mild trichiasis,however, epilation is commonly performed and hasnever been formally compared to surgery.
The review found good evidence that tarsal rotationsurgery can be performed equally well by appropri-ately trained ophthalmic nurses and ophthalmologists.This is of great programmatic importance as in mosttrachoma endemic countries the number of ophthal-mologists is very limited and the backlog of trichiasissurgery far exceeds what could be delivered by thesephysicians alone. The review also found evidence thatsurgery performed at community (village) level hadequivalent outcomes to that performed at a health cen-tre. However, the uptake was higher for village-basedsurgery, which is an important observation as in manyendemic regions the uptake of surgery is low.
The three studies investigating whether post-opera-tive azithromycin treatment improves surgical out-come have provided mixed results. Two were pub-lished after the last update of the review (19,20).Two studies found no convincing evidence thatazithromycin reduces trichiasis recurrence (20,33).The third and largest study did find a significant reduc-tion in trichiasis recurrence with azithromycin (16).This may have been because the study was conductedin a region where C. trachomatis infection is hyper-endemic. However, no difference in the prevalence ofchlamydial infection was demonstrated between thetreatment groups, leaving open the question of how
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 961
the antibiotic affected the outcome. The additionalantibiotic treatment of family members did not conferany extra benefit. Overall, it is difficult to reach anydefinite conclusions about the effect of azithromycinon trichiasis recurrence, particularly in an operational(rather than research) setting.
Antibiotics
The authors of the review of Antibiotics for Trachomafound only limited evidence that antibiotics reduce theprevalence of active trachoma. There were two maintypes of study. The first was a very heterogeneousgroup of trials of antibiotics versus placebo, in which,overall, the results are consistent with a modestbeneficial effect on active trachoma at three monthsbut not at one year of follow-up. However, most ofthese studies targeted treatment to individuals withsigns of active disease. Therefore, the full potential ofany antibiotic on controlling trachoma has probablynever been tested in a placebo-controlled trial, as theimpact of treatment in these studies is likely to havebeen greatly undermined by reinfection from untreatedmembers of the community.
The second group of studies compared oral with top-ical antibiotics. The authors of the review concludedthat there was no evidence of a difference in the resultsbetween topical and oral antibiotic treatment. We agreewith this conclusion with respect to clinically activedisease, but differ in our interpretation with respectto C. trachomatis infection. We consider that the evi-dence supports the view that oral azithromycin is moreeffective at clearing infection than topical treatment.However, the clinical significance of this finding iscurrently unclear because in these and other studiesthe inflammatory disease persists. One possible expla-nation for this disparity is that the resolution of theclinical signs of active trachoma has been found tolag behind the resolution of infection (36).
Face washing
The authors of the Cochrane review on the promo-tion of face washing for prevention of active trachomaconclude that from the available data there is some evi-dence that face washing, when combined with topicaltetracycline eye ointment, can be effective in reducingsevere trachoma. They additionally conclude that thecurrent evidence does not support a beneficial effectof face washing alone, or in combination with topi-cal tetracycline eye ointment, in reducing the preva-lence of active trachoma (14). Since the review waswritten there have been no additional clinical trials,although clean face, which has a variety of defini-tions, has been included in many observational studiesand cross-sectional surveys since the publication of theoriginal Tanzania ‘clean face’ study (17). The evidencefrom these studies has been summarized in a numberof traditional reviews (10,11,37). In the absence of astandardized definition of ‘clean face’ and without an
agreed-upon methodology of when and how it shouldit measured (the frequency of the components usuallyused to define a clean face such as food or dust on theface and the presence of ocular and nasal discharge arestrongly dependent on the time of day, season and ageof the child) it is difficult to interpret the findings ofthe risk factor studies. The difficulty in interpretation isexacerbated by the fact that two of the components ofan unclean face (ocular and nasal discharge) may be aresult of active trachoma. All of this notwithstanding,the results of the original trial on severe trachoma, andthe observational studies are considered to be sufficientto warrant the continued inclusion of behaviour changecommunication and promotion of personal groomingto promote clean face as one of the pillars of the SAFEstrategy (17).
Environmental change
The authors of the Cochrane review on the E com-ponent of SAFE conclude that there is evidence thatinsecticide spray as a fly control measure reduces tra-choma significantly, that latrine provision as a fly con-trol measure has not demonstrated significant trachomareduction, and that health education may be effectivein reducing trachoma. The authors note that there isa dearth of data to determine the effectiveness of allaspects of environmental sanitation in the control oftrachoma. Given the shortage of data available in thereview (shown again in Table II) and the heterogeneityof study design, a meta-analysis was not conducted. Inthe absence of any well-conducted intervention trials,there was no reference to the role of water provisionin trachoma control in the review, despite access towater being one of the major areas of implementationfor control programs.
Since the publication of the Cochrane review, twonew studies have been conducted that contributeadditional data (16,18). Edwards et al. examined theimpact of health education through radio broadcastsalone (control), radio plus routine non-governmentalorganization (NGO) program activities (standard), andradio plus NGO activities plus video (18). There wasa small and statistically significant reduction in theprevalence of clinical signs of trachoma in all thecommunities in the study, but no difference betweenthe three arms. The study lacked a true control armin which there had been no trachoma intervention,so the observed reduction in prevalence cannot beascribed with certainty to the health education. Westet al. examined the effect of insecticide spray forfly control after mass antibiotic treatment in an areaof central Tanzania hyperendemic for trachoma (16).The insecticide spray successfully and effectivelycontrolled eye-seeking flies, although there was nostatistically significant effect on either clinical signsof trachoma or prevalence of ocular swabs positivefor C. trachomatis at six or 12 months.
The Cochrane review references a number of tra-ditional reviews of the literature on the F and E
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
962 E. Sumamo et al.
components of SAFE (10,11,38,39). Mabey et al.(1992), Mabey et al. (2003), and Kuper et al. alsoinclude useful discussion on the F and E compo-nents (37,40,41). These non-systematic reviews focusmainly on the numerous observational studies on tra-choma. Although it should be noted that trachoma hasdisappeared from Europe and North America, and nowfrom parts of the Middle East, as a result of improvedliving conditions and not as a result of programs basedon antibiotic distribution or surgery, the interventionsfor F and E currently being adopted in endemic areashave not been rigorously tested. Of note, there havebeen no clinical trials of improving access to water, useof latrines, hygiene promotion, trachoma health edu-cation, village cleaning, or moving domestic animalsaway from living quarters, all of which are currentlybeing used as trachoma control measures in one ormore countries.
Conclusions
Implications for practice
The control of blinding trachoma is based on theWHO endorsed integrated SAFE strategy. Whilst it isnot possible to state that there are sufficient rigorousclinical trial data to support or refute the use ofthe SAFE strategy for blindness prevention throughtrachoma control in its entirety, there is some goodevidence for each of the separate components.
There is a reasonably good evidence base to guidepractice in the surgical management of trachomatoustrichiasis. Surgery should involve a full thickness inci-sion and rotation of the terminal portion of the tarsus.Surgery can be safely and effectively performed byappropriately trained ophthalmic nurses. Results canbe equally good for surgery performed at the com-munity level, which can significantly improve uptakeof this intervention. Results of the post-operative useof azithromycin are mixed. Given the frequent con-junctival bacterial infection in people with trichiasis,it is appropriate to use some form of post-operativeantibiotic.
The evidence for antibiotics in trachoma control isconsistent with a modest risk reduction in clinicallyactive trachoma at three months post treatment, butnot at twelve months. The data suggest that oralantibiotics have a greater effect on C. trachomatisinfection than topical treatment at three months andpossibly one year. They appear to have an equivalenteffect on clinically active trachoma. The impact ofmass community–wide treatment may be much greaterthan treatment targeted at individuals with disease.However, this has not been formally assessed bya randomized placebo-controlled trial. It should benoted that the studies of mass azithromycin treatmentused three doses as opposed to the current WHOrecommendation of a single annual dose (21). Whetherthese regimens are equally effective is unknown. In
practice, the current recommendation that trachomabe treated with either topical tetracycline or oralazithromycin is unaffected by this review. There are,however, major gaps in the evidence on which tobase recommendations for the targeting, frequency andduration of antibiotic treatment.
For the F and E components, there is evidence thatface washing in conjunction with antibiotics has aneffect on severe trachoma, and that fly control withinsecticide spray reduces active trachoma. In terms ofprocess, face washing can increase the prevalence ofclean face and latrine promotion can reduce the fre-quency of fly-eye contact. Operationally, the inclusionof activities that support face washing and fly controlare warranted. These include hygiene promotion, waterprovision, fly spraying, latrine promotion and villagecleaning.
Implications for research
Each of the components of the SAFE strategy has beentested in isolation, but the impact of the full strategy onblindness prevention has never been tested. It wouldnow be ethically improper, however, to conduct a lon-gitudinal study of the impact of SAFE in comparisonto controls who were screened, but not included inimplementation activities. Fortunately, rigorous impactassessments of existing implementation programs, inwhich there are good quality baseline and follow-updata, coupled with monitoring data giving an insightto the intensity of the interventions delivered, shouldbe adequate. The A, F and E components of the SAFEstrategy share a common objective of contributing to areduction in transmission of the disease. Clinical trialshave usually tested just one of these components at atime, yet it could be anticipated that there is a syn-ergistic effect between them. Clinical trials that aredesigned to test the hypothesis that there is a syner-gistic effect of these three components of SAFE suchthat the effect of antibiotic is enhanced by face wash-ing and environmental improvements (and visa versa)should be conducted. For the individual components ofSAFE, a number of less complex operational researchstudies would enhance the delivery of programs.
Trichiasis surgery
The optimal management of minor trichiasis (one tofive lashes touching the eye) is uncertain. Currentlyboth early surgery and epilation are practiced. How-ever, it is unknown whether these are equally effec-tive. A randomized controlled trial of these alternativeswould be of programmatic value.
Recurrent trichiasis remains a significant problemwhich limits the effectiveness of surgery in preventingblindness. There is a need to assess simple approachesto improve the long-term outcomes. For example,absorbable sutures may be superior to the currentlyused silk. The outcome of surgery varies significantlybetween surgeons. Therefore, realistic strategies toaudit results and improve quality are necessary.
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
The Cochrane Library and trachoma: an overview of reviews 963
The uptake of surgery is often disappointingly lowparticularly among women who have a disproportion-ate burden of disease. The barriers to surgery probablyvary and need to be assessed in different regions.Strategies designed to overcome these, especially forwomen in rural areas, need to be tested.
Antibiotics
Mass antibiotic distribution programs are being setup in many trachoma endemic countries. For ethicalreasons, it is now unlikely that there will ever bea trial that investigates the effectiveness of massantibiotic against a placebo as there is a consensus thatthe current alternatives (oral azithromycin and topicaltetracycline) probably have some effect. However,there is a pressing need for evidence to help optimizetheir use. It remains uncertain who should be giventreatment, how often and for how long. Comparativetrials of different distribution strategies are needed.Given that the signs of clinically active trachoma canpersist long after the infection has been cleared byantibiotics, there is potentially a role for a simplepoint of care test for the infection to determinewhether a community needs an ongoing treatmentprogram.
Facial cleanliness
The combination of available trial and observationaldata is considered sufficient to warrant the continua-tion of hygiene promotion and face washing in tra-choma control programs. However a repeat of theoriginal face washing trial that included as processindicators azithromycin treatment and face washing,and that had both clinical and microbiological out-put, would be extremely useful. The current defi-nitions of clean face include ocular and nasal dis-charge, which are correlated with both the effectof face washing and the absence of disease. Thispotential impediment to interpretation will have to beaddressed in the study design and selected outcomeindicators.
Environmental improvements
Whilst there is evidence that insecticide spray for eye-seeking flies reduces active trachoma, other simple andsustainable strategies to control flies have not beentested. There is a need for large randomized controlledtrials of the effectiveness of latrines, village cleaning,and moving animals away from domestic residencesfor trachoma control. The effect of water provisionalone, or in combination with other routine trachomaprogram interventions, on the prevalence of trachomahas not been formally tested.
Declarations of Interest
None.
References
1. Emerson PM, Lindsay SW, Alexander N, Bah M, Dibba SM,Faal HB. Role of flies and provision of latrines in trachomacontrol: cluster randomized controlled trial. Lancet. 2004;363(9415): 1093–8.
2. Mabey D, Fraser-Hurt N, Powell C. Antibiotics for trachoma.Cochrane Database of Systematic Reviews 2005, Issue 2. Art. No.:CD001860. DOI: 10.1002/14651858.CD001860.pub2.
3. Resnikoff S, Pascolini D, Etay’ale D, Kocur I, Pararajasegaram R,Gopal P, et al. Global data on visual impairment in the year 2002.Bull World Health Organ. 2004; 82: 844–51.
4. WHO Programme for the Prevention of Blindness andDeafness. Future Approaches to Trachoma Control. Report of aGlobal Scientific Meeting. Geneva, 17–20 June 1996. Geneva:WHO; 1997; Ordering code: WHO/PBL/9656. Available from:http://whqlibdoc.who.int/hq/1996/WHO PBL 96.56.pdf.
5. WHO. Global elimination of blinding trachoma. World HealthAssembly Resolution WHA 51.11. Geneva: WHO; 1998; Availablefrom: http://www.who.int/ncd/vision2020 actionplan/documents/WHA51.11.pdf.
6. Yorston D, Mabey D, Hatt S, Burton M. Interventions for tra-choma trichiasis. Cochrane Database of Systematic Reviews 2006,Issue 3. Art. No.: CD004008. DOI: 10.1002/14651858.CD004008.pub2.
7. Solomon AW, Zondervan M, Kuper H, Buchan JC, Mabey DCW,Foster A. Trachoma Control: a guide for program managers.Geneva: WHO; London: London School of Hygiene & TropicalMedicine; New York: International Trachoma Initiative; 2006;Available from: http://www.who.int/blindness/publications/tcm%20who pbd get 06 1.pdf.
8. Thylefors B, Dawson CR, Jones BR, West SK, Taylor HR. Asimple system for the assessment of trachoma and itscomplications. Bull World Health Organ. 1987; 65: 477–83.
9. Emerson PM, Bailey RB, Mahdi OS, Walraven GEL, Lind-say SW. Transmission ecology of the fly Musca sorbens, a putativevector of trachoma. Trans R Soc Trop Med Hyg. 2000; 94(1):28–32.
10. Pruss A, Mariotti S. Preventing trachoma through environmentalsanitation: a review of the evidence base. Bull World Health Organ.2000; 78: 258–66.
11. Emerson PM. Review of the evidence base for the ‘F’ and ‘E’components of the SAFE strategy for trachoma control. Trop MedInt Health. 2000; 5: 515–27.
12. Rabiu M, Alhassan M, Ejere H. Environmental sanitary inter-ventions for preventing active trachoma. Cochrane Database ofSystematic Reviews 2005, Issue 2. Art. No.: CD004003. DOI:10.1002/14651858.CD004003.pub2.
13. Ngondi J, Onsarigo A, Matthews F, Reacher M, Brayne C,Baba S, et al. Effect of 3 years of SAFE (surgery, antibiotics,facials cleanliness, and environmental change) strategy fortrachoma control in southern Sudan: a cross-sectional study.Lancet. 2006; 368: 589–95.
14. Ejere H, Alhassan MB, Rabiu M. Face washing promotionfor preventing active trachoma. Cochrane Database of Sys-tematic Reviews 2004, Issue 3. Art. No.: CD003659. DOI:10.1002/14651858.CD003659.pub2.
15. Emerson PM, Lindsay SW, Walraven GEL, Faal H, Bøgh C,Lowe K, et al. Effect of fly control on trachoma and diarrhea.Lancet. 1999; 353(9162): 1401–3.
16. West SK, Emerson PM, Mkocha H, McHiwa W, Munoz B,Bailey R, et al. Intensive insecticide spraying for fly control aftermass antibiotic treatment for trachoma in a hyperendemic setting:a randomised trial. Lancet. 2006; 368: 596–600.
17. West S, Munoz B, Lynch M, Kayongoya A, Chilangwa Z, MmbagaBB, et al. Impact of face-washing on trachoma in Kongwa,Tanzania. Lancet. 1995; 345: 155–8.
18. Edwards T, Cumberland P, Hailu G, Todd J. Impact of healtheducation on active trachoma in hyperendemic rural communitiesin Ethiopia. Ophthalmology. 2006; 113(4): 548–55.
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172
964 E. Sumamo et al.
19. West SK, West ES, Alemayehu W, Melese M, Munoz B, Imeru A,et al. Single-dose azithromycin prevents trichiasis recurrence fol-lowing surgery. Arch Ophthalmol. 2006; 124: 309–14.
20. Zhang H, Kandel RP, Atakari HK, Dean D. Impact of oralazithromycin on recurrence of trachomatous trichiasis in Nepalover 1 year. Br J Ophthalmol. 2006; 90: 943–8.
21. Schachter J, West SK, Mabey D, Dawson CR, Bobo L, Bailey R,et al. Azithromycin in control of trachoma. Lancet. 1999; 354:630–5.
22. Peach H, Piper S, Devanesen D, et al. Northern TerritoryTrachoma and Eye Health Committee’s randomized controlled trialof the effect of eye drops and eye washing on follicular trachomaamong Aboriginal children. Report of the Northern TerritoryTrachoma Control and Eye Health Committee Incorporated. 1987;1–33.
23. Resnikoff S, Peyramaure F, Bagayogo CO, Huguet P. Healtheducation and antibiotic therapy in trachoma control. Rev Int TrachPathol Ocul Trop Subtrop Sante Publique. 1995; 72: 89–98.
24. Bowman RJC, Sillah A, van Dehn C, Goode VM, Mugit MM,Johnson GJ, et al. Operational comparison of single-doseazithromycin and topical tetracycline for trachoma. InvestOphthalmol Vis Sci. 2000; 41(13): 4074–9.
25. Darougar S, Jones BR, Viswalingam N, Poirier RH, Allami J,Houshmand A, et al. Family-based suppressive intermittenttherapy of hyperendemic trachoma with topical oxytetracycline ororal doxycycline. Br J Ophthalmol. 1980; 64(4): 291–5.
26. Dawson CR, Hanna L, Wood TR, Coleman V, Briones OC,Jawetz E. Controlled trials with trisulfapyrimidines in thetreatment of chronic trachoma. J Infect Dis. 1969; 119(6): 581–90.
27. Hoshiwara I, Ostler HB, Hanna L, Cignetti F, Coleman VR,Jawetz E. Doxycycline treatment of chronic trachoma. JAMA.1973; 224(2): 220–3.
28. Dawson CR, Schachter J, Sallam S, Sheta A, Rubinstein RA,Washton H. A comparison of oral azithromycin with topicaloxytetracycline/polymyxin for the treatment of trachoma inchildren. Clin Infect Dis. 1997; 24: 363–8.
29. Adamu Y, Alemayehu W. A randomized clinical trial of thesuccess rates of bilamellar tarsal rotation and tarsotomy for uppereyelid trachomatous trichiasis. Ethiop Med J. 2002; 40: 107–14.
30. Reacher MH, Huber MJE, Canagaratnam R, Alghassany A. Atrial of surgery for trichiasis of the upper lid from trachoma. Br JOphthalmol. 1990; 74: 109–13.
31. Reacher MH, Munoz B, Alghassany A, Daar AS, Elbualy M,Taylor HR. A controlled trial of surgery for trachomatous trichiasisof the upper lid. Arch Ophthalmol. 1992; 110: 667–74.
32. Graz B, Xu JM, Yao ZS, Han SR, Kok A. Trachoma: cantrichiasis be treated with sticking-plaster? A randomized clinicaltrial in China. Trop Med Int Health. 1999; 4(3): 222–8.
33. Burton MJ, Kinteh F, Jallow O, Sillah A, Bah M, Faye M, et al.A randomised controlled trial of azithromycin following surgeryfor trachoma trichiasis in the Gambia. Br J Ophthalmol. 2005; 89:1282–8.
34. Bowman RJ, Soma OS, Alexander N, Milligan P, Rowley J,Faal H, et al. Should trichiasis surgery be offered in the village?A community randomised trial of village vs. health centre-basedsurgery. Trop Med Int Health. 2000; 5(8): 528–33.
35. Alemayehu W, Melase M, Bejiga A, Worku A, Kebede W,Fantaye D. Surgery for trichiasis by ophthalmologists versusintegrated eye workers: a randomized trial. Ophthalmology. 2004;111(3): 578–84.
36. Bailey R, Duong T, Carpenter R, Whittle H, Mabey D. Theduration of human ocular Chlamydia trachomatis is age dependant.Epidemiol Infect. 1999; 123: 479–86.
37. Kuper H, Solomon AW, Buchan J, Zondervan M, Foster A,Mabey D. A critical review of the SAFE strategy for the preventionof blinding trachoma. Lancet Infect Dis. 2003; 3(6): 372–81.
38. Esrey SA, Potash JB, Roberts L. Shiff C. Effects of improvedwater supply and sanitation on ascariasis, diarrhoea, dracunculiasis,hookworm infection, schistosomiasis, and trachoma. Bull WorldHealth Organ. 1991; 69(5): 609–21.
39. Prost A, Negrel AD. Water, trachoma and conjunctivitis. BullWorld Health Organ. 1989; 67(1): 9–18.
40. Mabey DC, Bailey RL, Ward ME, Whittle HC. A longitudinalstudy of trachoma in a Gambian village: implications concerningthe pathogenesis of chlamydial infection. Epidemiol Infect. 1992;108(2): 343–51.
42. Foster SO, Powers DK, Thygeson P. Trachoma therapy: acontrolled study. Am J Ophthalmol. 1966; 61(3): 451–5.
43. Shukla BR, Nema HV, Mathur JS, Nath K. Gantrisin andmadribon in trachoma. Br J Ophthalmol. 1966; 50(4): 218–21.
44. Attiah MA, el Kohly AM. Clinical assessment of the comparativeeffect of terramycin and GS 2989 in the mass treatment oftrachoma. Rev Int Trach. 1973; 50(3): 11–20.
45. Woolridge RL, Cheng KH, Chang IH, Yang CY, Hsu TC, GraystonJT. Failure of trachoma treatment with ophthalmic antibiotics andsystemic sulfonamides used alone or in combination with trachomavaccine. Am J Ophthalmol. 1967; 63(5 Suppl): 1577–86.
46. Tabbara KF, El-Asrar AMA, Al-Omar O, Choudhury AH, Al-Faisal Z. Single-dose azithromycin in the treatment of trachoma: arandomized, controlled study. Ophthalmology. 1996; 103: 842–6.
Copyright 2007 John Wiley & Sons, Ltd. Evid.-Based Child Health 2: 943–964 (2007)DOI: 10.1002/ebch.172