73
“DANGEROUS TRIAD OF OBESITY, DIABETES & HYPERTENSION” - IS SURGERY THE SINGLE ANSWER? DR SREEJOY PATNAIK
| Date post: | 14-Jul-2015 |
| Category: |
Healthcare |
| Upload: | shanti-memorial-hospital-pvtltd |
| View: | 315 times |
| Download: | 0 times |

“DANGEROUS TRIAD OF OBESITY, DIABETES &
HYPERTENSION”- IS SURGERY
THE SINGLE ANSWER?
DR SREEJOY PATNAIK

Bariatric & Metabolic Surgery Dept.Bariatric & Metabolic Surgery Dept.Shanti Memorial Hospital Pvt Ltd.Shanti Memorial Hospital Pvt Ltd.
DR SREEJOY PATNAIKLIFE MEMBER OSSI,IFSO,SAGES
www.obesityinindia.com, www.shantimemorialhospital.com
Obesity EpidemicObesity Epidemic
• World epidemic - 1.7 billion people
• BMI >35 & >40 showing rapid growth
• Rise in obesity > rise in comorbidities
• Comorbidities > 2.5 million deaths per year
• Morbid obesity - reduction in lifespan
Buchwald et al. Jama 2004Buchwald et al. Jama 2004

Obesity EpidemicObesity Epidemic
• T/t :
• Diet therapy alone is ineffective in long term .
• Currently, there are no effective pharmaceutical agents to treat obesity, especially morbid obesity
North American Association for the North American Association for the Study of Obesity. NIH 2000Study of Obesity. NIH 2000
Obesity in India
• Morbid obesity - 10% of the country's population.
• Unhealthy, processed food has become much more accessible in global food markets.
• Indians are genetically susceptible to weight accumulation especially around the waist.
• A SNP (single nucleotide polymorphism) GENE named rs12970134 to be mostly associated with waist circumference

AETIOLOGY :MULTIFACTORIAL COMPLEX DISEASE
GENETIC
LACK OF PHYSICAL ACTIVITY& MEDICAL REASONS
LIFESTYLE CAUSES
• Calculated as follows: Weight(kg)/Height(m2)
• Mortality lowest = BMI < 25kg/m2
• Mortality highest = BMI > 40kg/m2
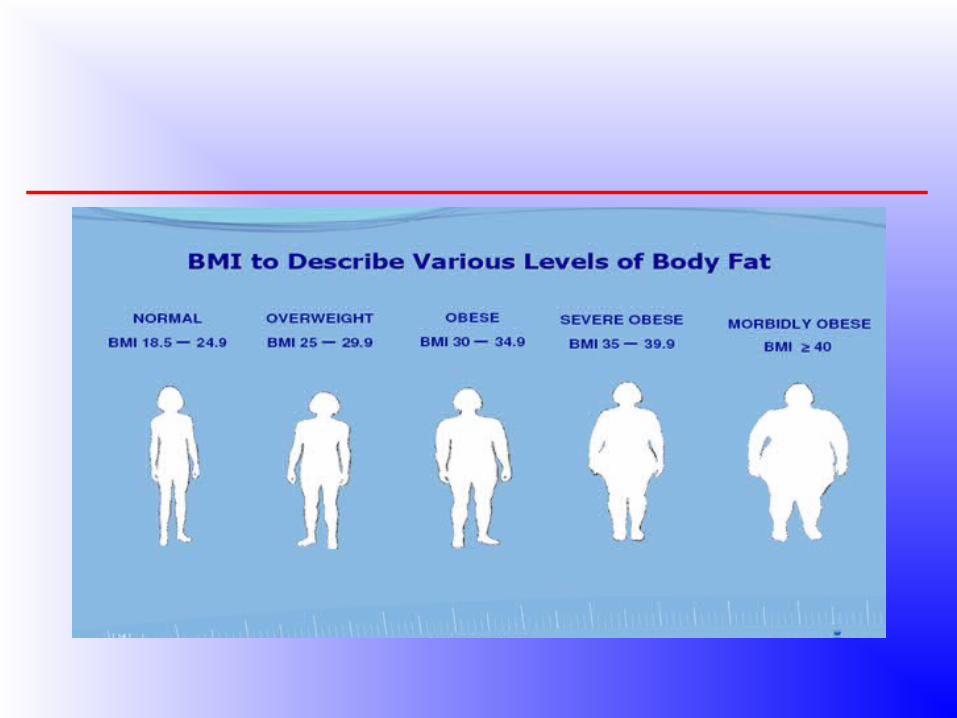
Definition of Obesity Definition of Obesity according to BMIaccording to BMI
BMIBMI
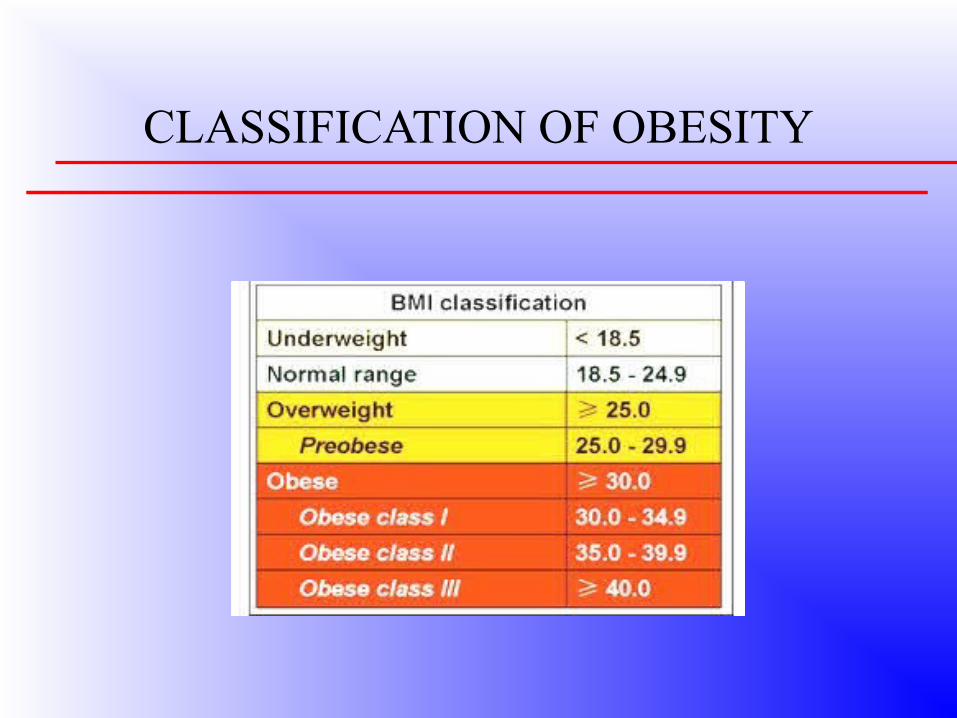
CLASSIFICATION OF OBESITY
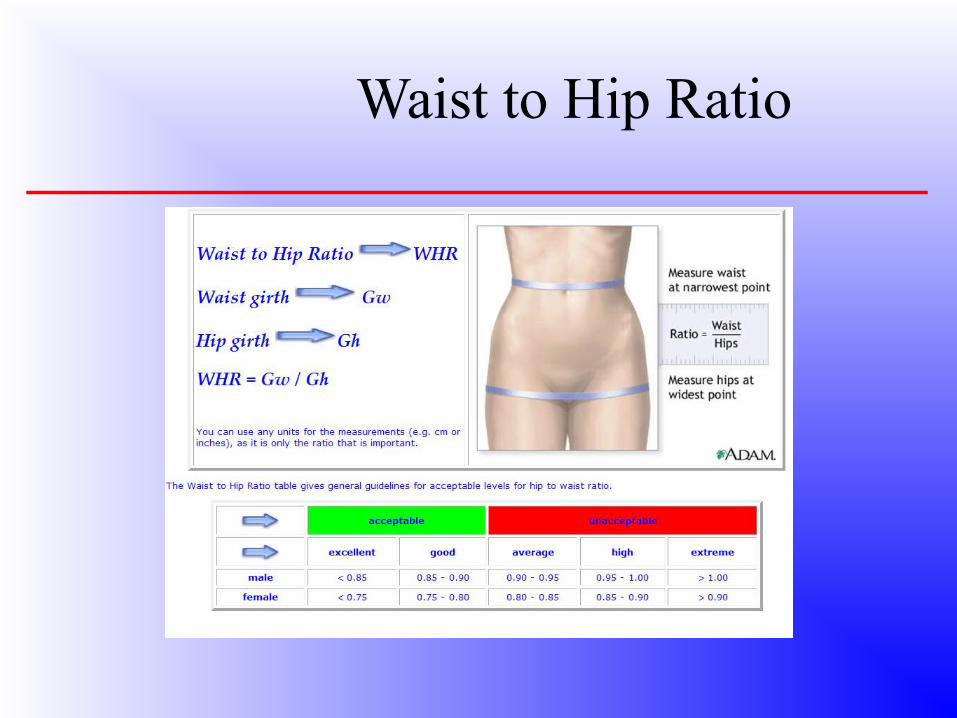
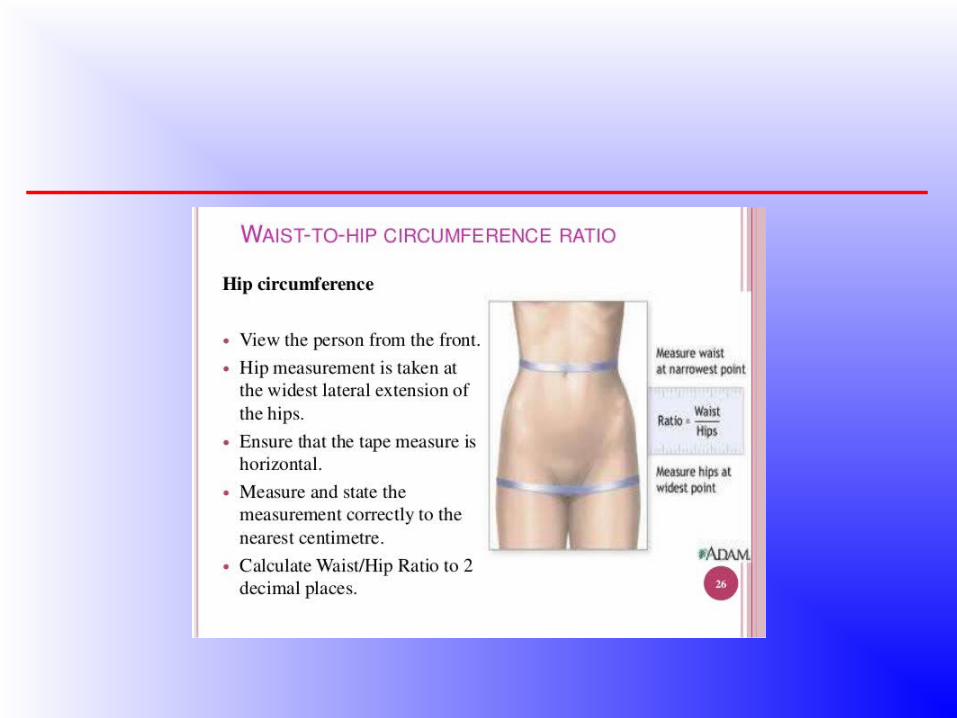
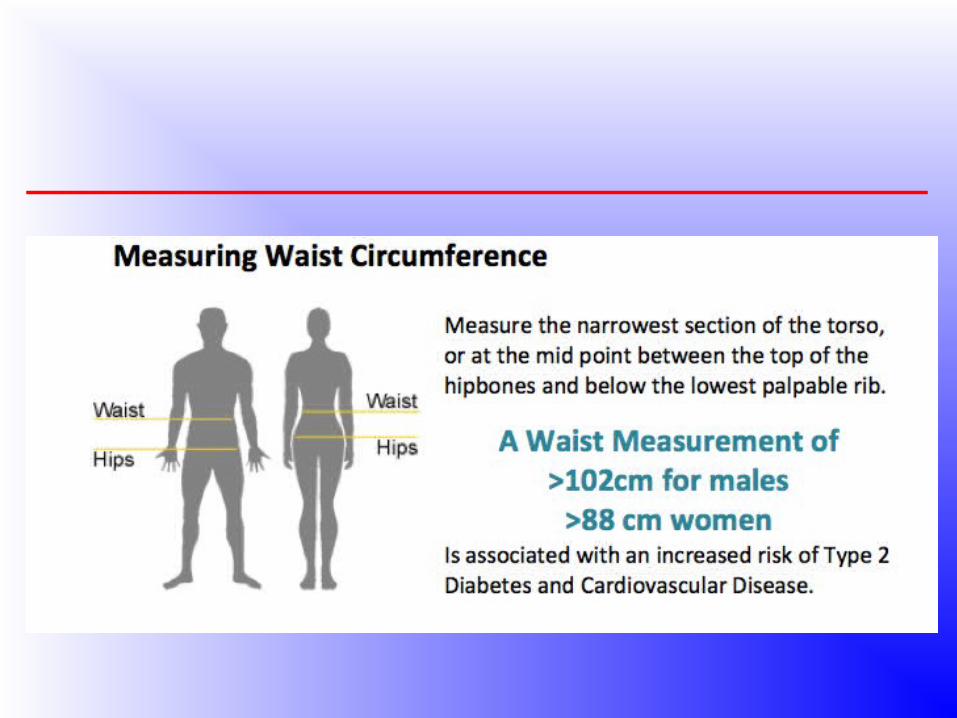
Waist to Hip Ratio


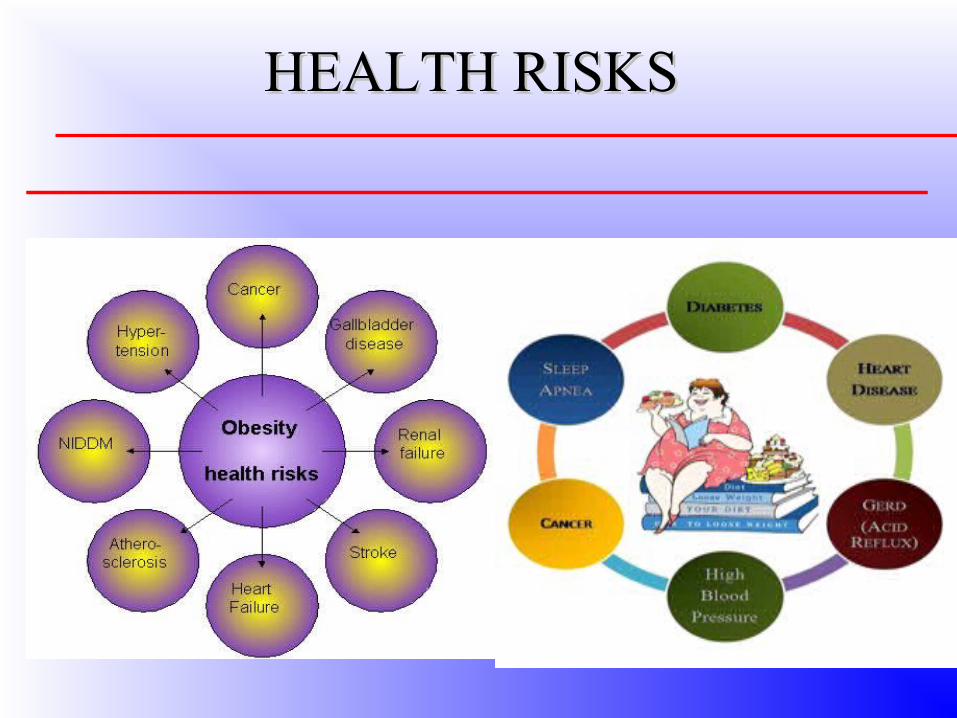
Negative Effects of Obesity
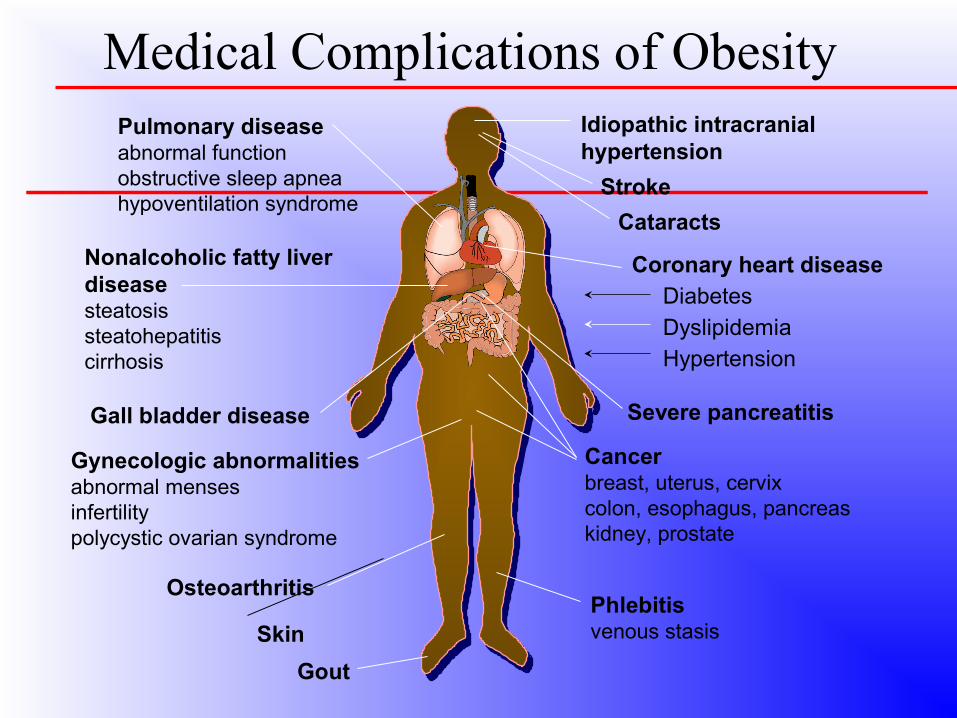
Pulmonary diseaseabnormal functionobstructive sleep apneahypoventilation syndrome
Nonalcoholic fatty liver diseasesteatosissteatohepatitiscirrhosis
Coronary heart disease Diabetes Dyslipidemia Hypertension
Gynecologic abnormalitiesabnormal mensesinfertilitypolycystic ovarian syndrome
Osteoarthritis
Skin
Gall bladder disease
Cancerbreast, uterus, cervixcolon, esophagus, pancreaskidney, prostate
Phlebitisvenous stasis
Gout
Medical Complications of ObesityIdiopathic intracranial hypertension
Stroke
Cataracts
Severe pancreatitis

Metabolic Syndrome or Syndrome X
THE DANGEROUS TRIAD
Abdominal obesity
Hyperinsulinemia
High fasting plasma glucose
Impaired glucose tolerance
Hypertriglyceridemia
Low HDL-cholesterol
Hypertension
TREATMENT OF OBESITY
1.DIET
2.EXERCISE
3.BEHAVIOURAL/LIFESTYLE MODIFICATION
4.MEDICAL / DRUGS
5. SURGERY
Medical Treatment of Obesity
Diet – low in calories, fat and carbohydrates (1200 cal/ day)
Exercise– 40 minutes 5 times per week
Behavior Modification – eat 3 sensible meals per day, avoid snacking
Drugs/Prescription medications-Stimulants/appetite suppressants
– Antidepressants (Meridia®)
– Reduce fat absorption (Orlistat)

Disadvantages of medical treatment:
Most patients (95-97%) regain weight that was lost within 2-5 years following diet or drug treatment
The average amount of weight loss is relatively small – 10-20 Kgs
Drug therapy may be associated with severe complications
Disadvantages of medical treatment:
Most insurance companies do not cover costs
• Very difficult to maintain these programs in the long term
• “Yo-Yo” effect leads to significant weight fluctuations
Surgical Treatment of Obesity
• Surgeons who specialize in treating obesity or the Dangerous Triad are known as Bariatric or a Metabolic surgeon.
• Bariatric surgery leads to significant and long lasting irreversible weight-loss alongwith resolution of comorbidities in severely obese patients
Bariatric and Metabolic Surgery
• Bariatric Surgery - from the Greek “baros” meaning “weight”, is synonymous with weight loss surgery.
• Metabolic surgery - be defined as “a set of GI operations used with the intent to treat diabetes ("diabetes surgery") and metabolic syndrome. (X- syndrome )”.
Indications for SurgeryIndications for SurgeryNIH Guidelines
BMI > 35 WITH 1 OR MORE COMORBID CONDITIONS (DM / HTN )
BMI > 40 WITHOUT ANY COMORBID CONDITIONS
PREVIOUSLY FAILED WEIGHT LOSS ATTEMPTS ( e.g, non-surgical interventions, diet control, behavioral modifications, exercise )
Indications for SurgeryIndications for Surgery
• Age > 18 or < 65• Failure of diet > 6 months• Obesity history > 5 years • Low risk for surgery• No endocrinological disease• Psychologically sound
NIH Consensus Conference NIH Consensus Conference Ann Intern Med 1991Ann Intern Med 1991
Goals of Surgery
• Effective: Loss > 50% of Excess Weight
• Low operative morbidity & mortality
• Well tolerated
• No long term complications
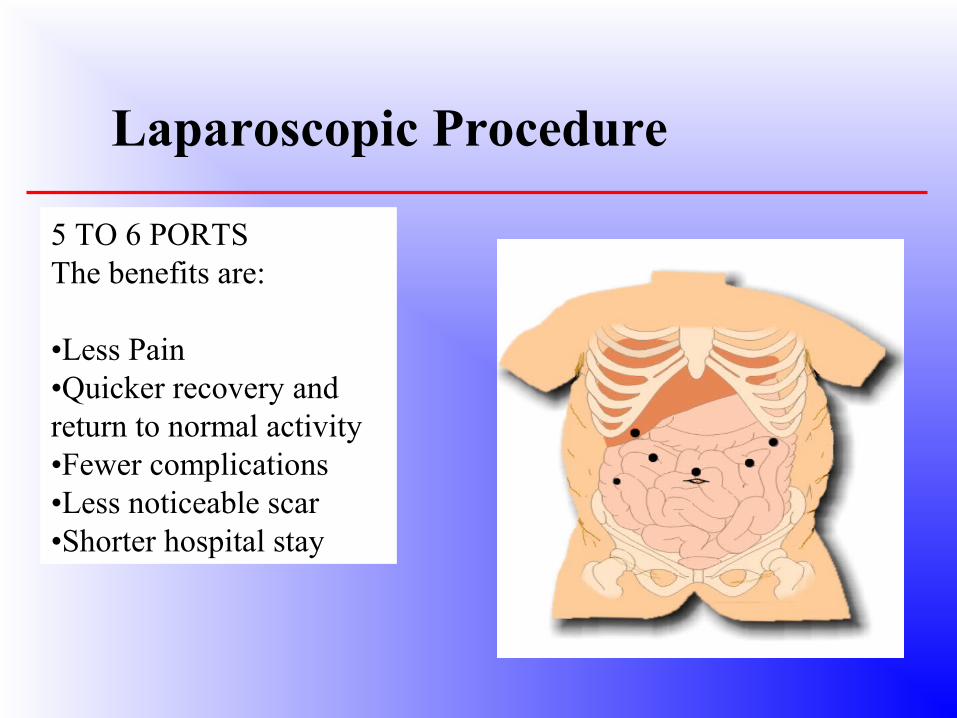
5 TO 6 PORTSThe benefits are:
•Less Pain•Quicker recovery and return to normal activity•Fewer complications•Less noticeable scar•Shorter hospital stay
Laparoscopic Procedure
Surgical ProceduresSurgical Procedures
• 1.RESTRICTIVE PROCEDURESES
• Restrictive surgeries shrink the size of the stomach which reduces the amount of food it can hold. This makes you feel full when eating much sooner than you did before surgery
–Gastric Banding–Sleeve Gastrectomy–-Gastric Plication
2. MALABSORPTIVE PROCEDURES
Malabsorptive surgeries rearrange and/or remove part your digestive system which then limits the amount of calories and nutrients that your body can absorb.
–Biliopancreatic Diversion• Scopinaro• Duodenal-Switch BPD
3. HYBRID PROCEDURES
– When surgery combines both restrictive and malabsorptive component, it is known as a “combination” procedure.
– Roux-en-Y Gastric Bypass / Banded– -Mini Gastric Bypass
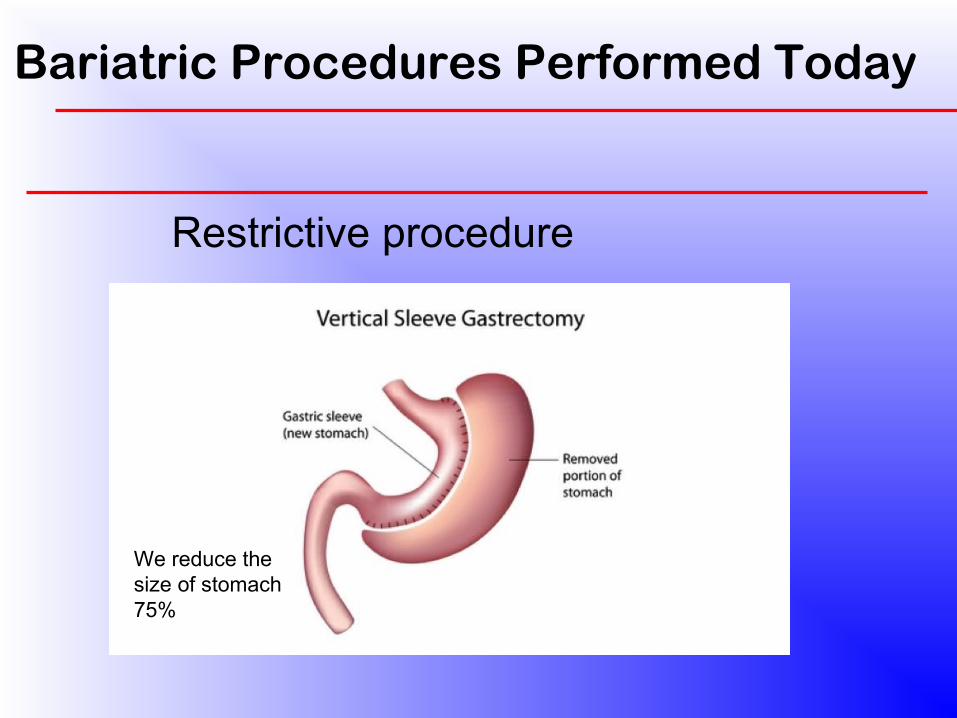
Bariatric Procedures Performed Today
Restrictive procedure
We reduce the size of stomach 75%

How does a sleeve work?One of the mechanisms involved in weight loss observed after the LSG is the dramatic reduction of the capacity of the stomach.
Ghrelin An orexigenic (appetite-stimulating) peptide hormone mainly produced in the fundus of the stomach, is supposed to be involved in the mechanisms regulating hunger .

MALABSORPTIVE PROCEEDUREBilio-pancreatic diversion
Scopinaro SG with DS
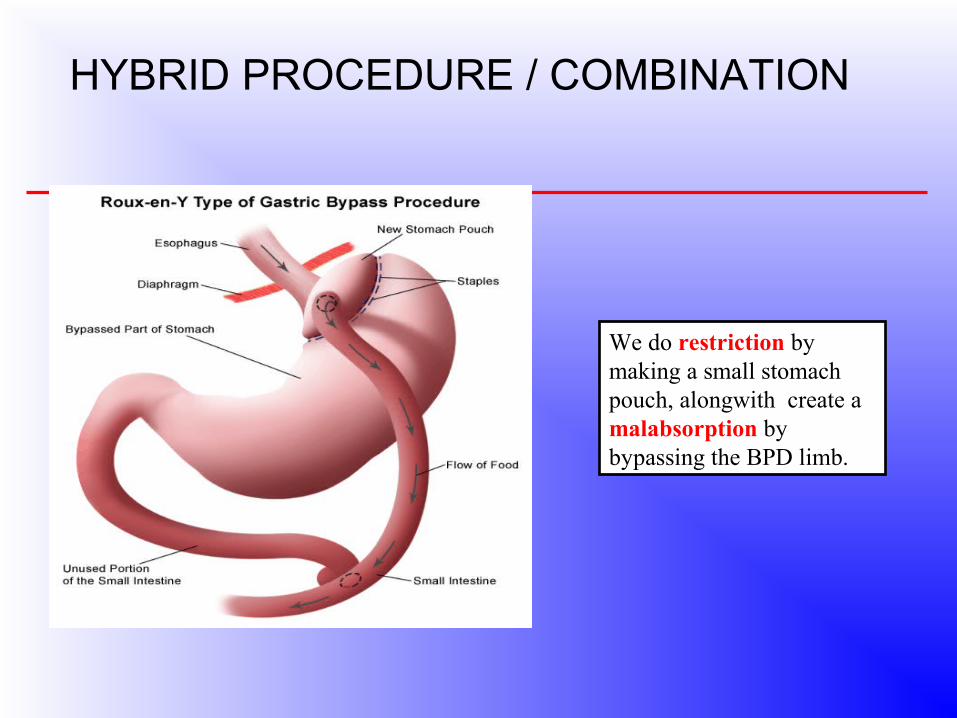
HYBRID PROCEDURE / COMBINATION
We do restriction by making a small stomach pouch, alongwith create a malabsorption by bypassing the BPD limb.
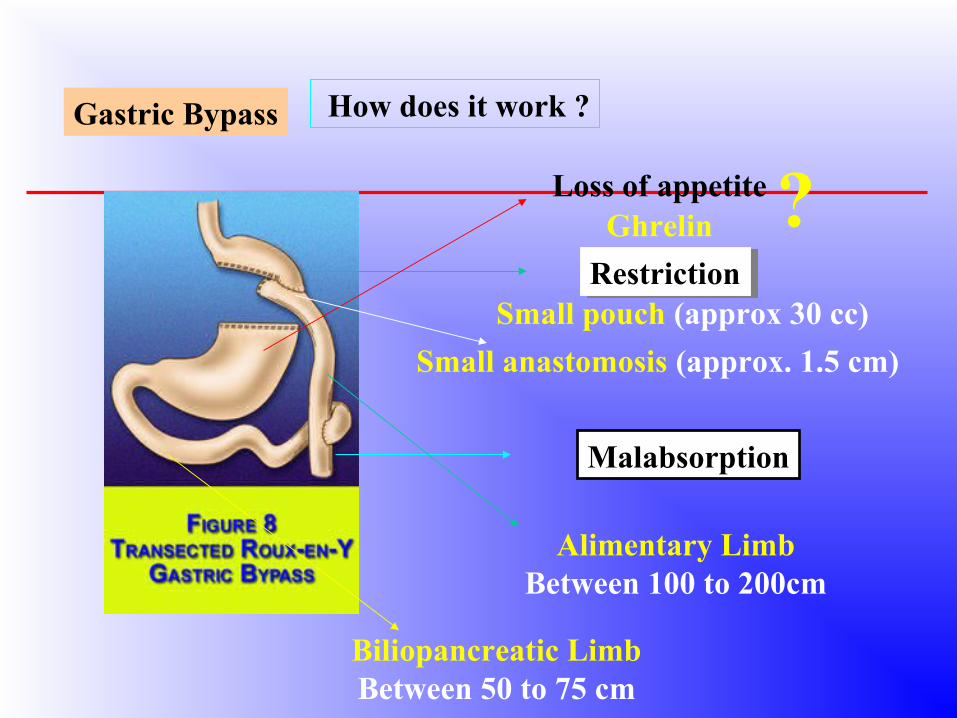
RestrictionRestriction
Malabsorption
Gastric Bypass
Loss of appetite ?Small pouch (approx 30 cc)
Small anastomosis (approx. 1.5 cm)
How does it work ?
Alimentary LimbBetween 100 to 200cm
Biliopancreatic LimbBetween 50 to 75 cm
Ghrelin
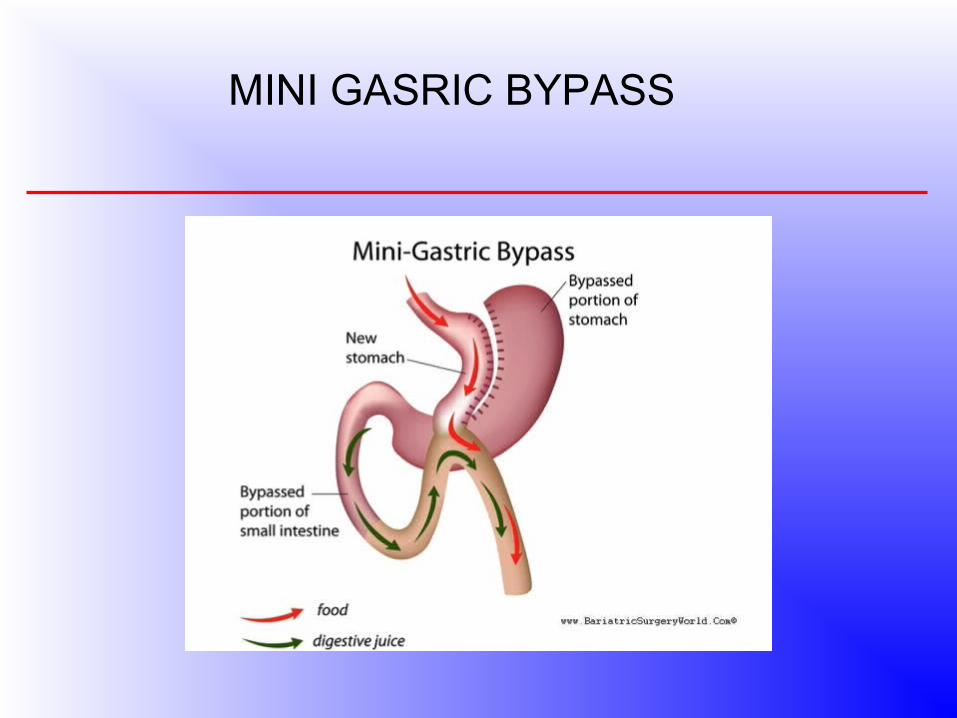
MINI GASRIC BYPASS

OPERATION THEATRE LAY OUT
POST OP ICU LAY OUT
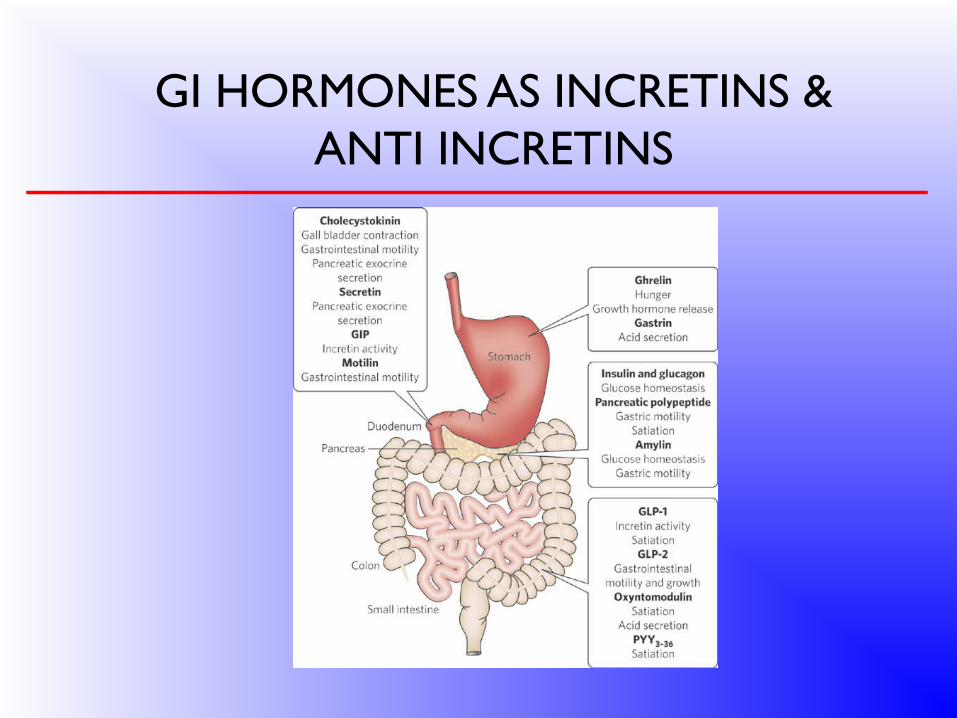
GI HORMONES AS INCRETINS & ANTI INCRETINS
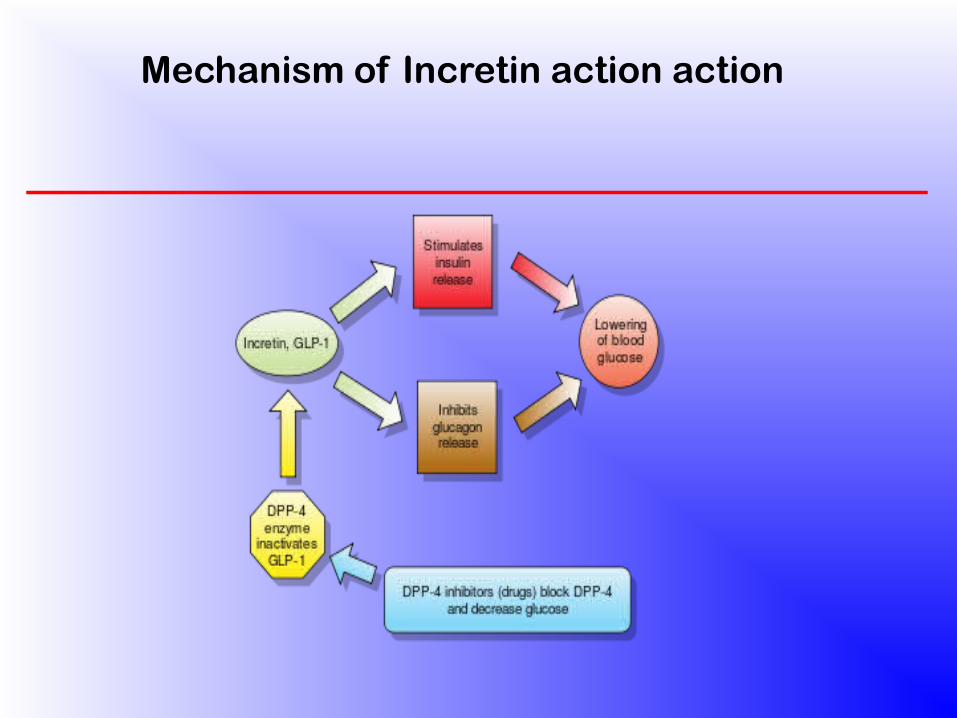
Mechanism of Incretin action action
PROPOSED THEORIES FOR IMPROVED GLYCAEMIA
(A) RAPID HINDGUT DELIVERY HYPOTHESIS
• Rapid delivery of ingested nutrients to lower bowel due to intestinal bypass leads to stimulation of L cells , ( distal i leum & colon ) which in turn results in increased secretion of incretin hormones & improved glucose homoeostasis.
•Proximal nutrient related signals that are transmitted from the duodenum to the distal bowel by neural pathways leads to increased Incretin secretion.
PROPOSED T(B) FOREGUT HYPOTHESIS HEORIES FOR IMPROVED
GLYCAEMIA
•The proximal small intestine (foregut / BPD limb ) is excluded resulting in reduction in secretion of Anti – incretin factors ( diabetogenic hormones) in response to absence of nutrients in the fore gut.
•This leads to improved glycaemia. &•Decreased Intestinal Glucagon synthesis
.
Benefits of Weight Loss Surgery
Significant weight loss• Lower cholesterol – D-30• Lower blood pressure• Improvement of Type II diabetes –D-1
• Improvement of cardiovascular health• Relief of sleep apnea• Relief of digestive problems –GERD• Decreased joint pain• Improved mobility
• Improved self image•
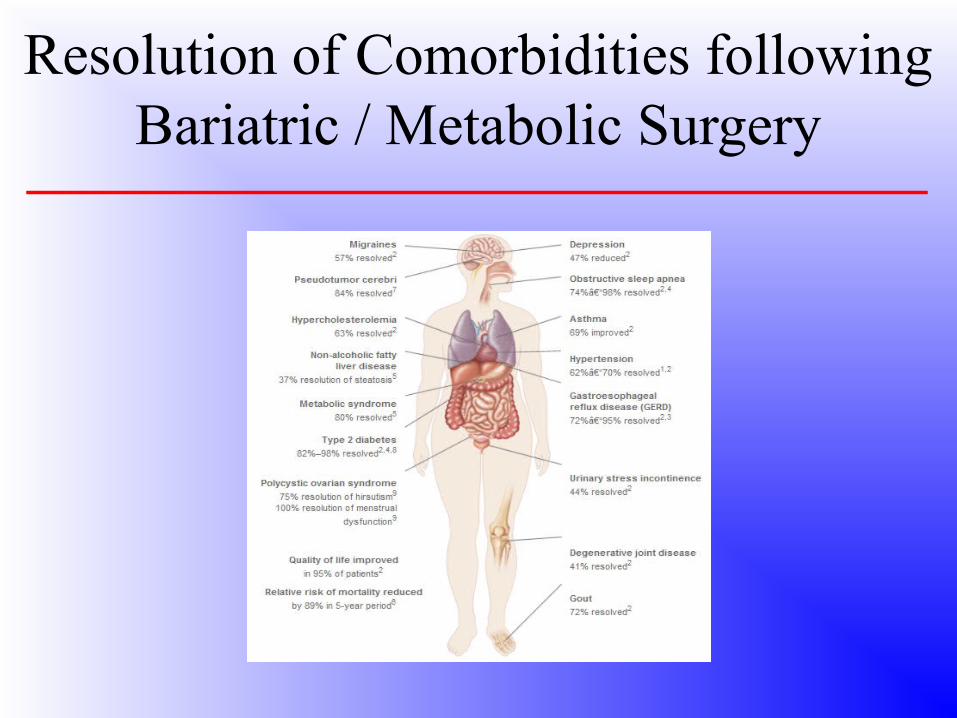
Resolution of Comorbidities following Bariatric / Metabolic Surgery
MY ExperienceS iN Bariatric Surgery
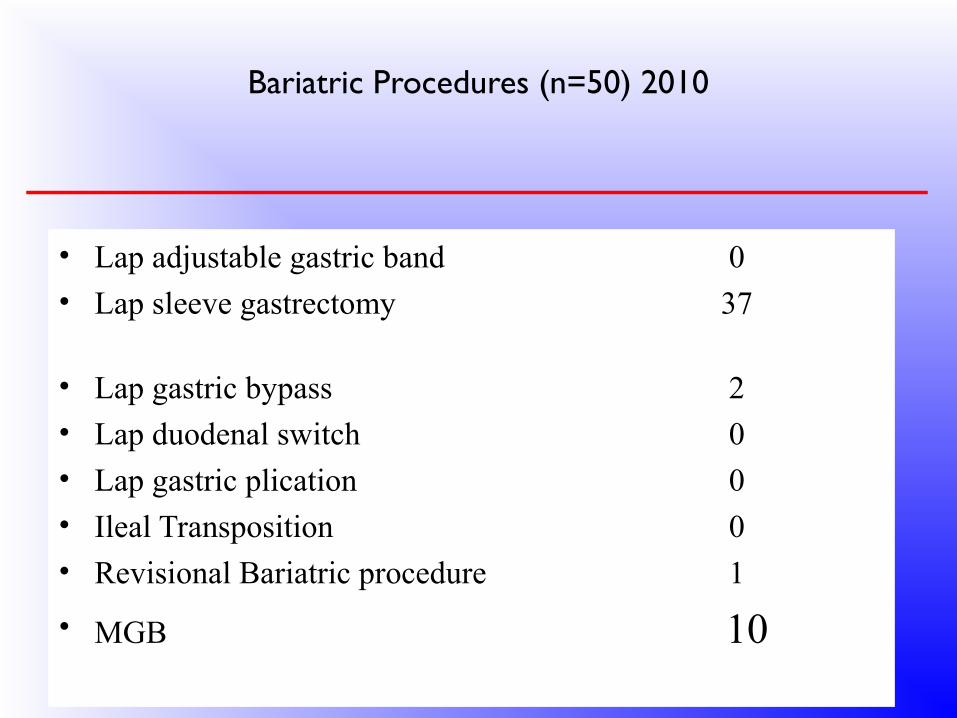
Bariatric Procedures (n=50) 2010
• Lap adjustable gastric band 0• Lap sleeve gastrectomy 37
• Lap gastric bypass 2• Lap duodenal switch 0
• Lap gastric plication 0• Ileal Transposition 0• Revisional Bariatric procedure 1
• MGB 10

OUR SUCCESSFUL PATIENTS
SANJAYAge: 34BW: 158 kgBMI: 56HTN: (+)DM: (+)ASTHMA: (+)OA: (+)Hypothyroidism: (+)
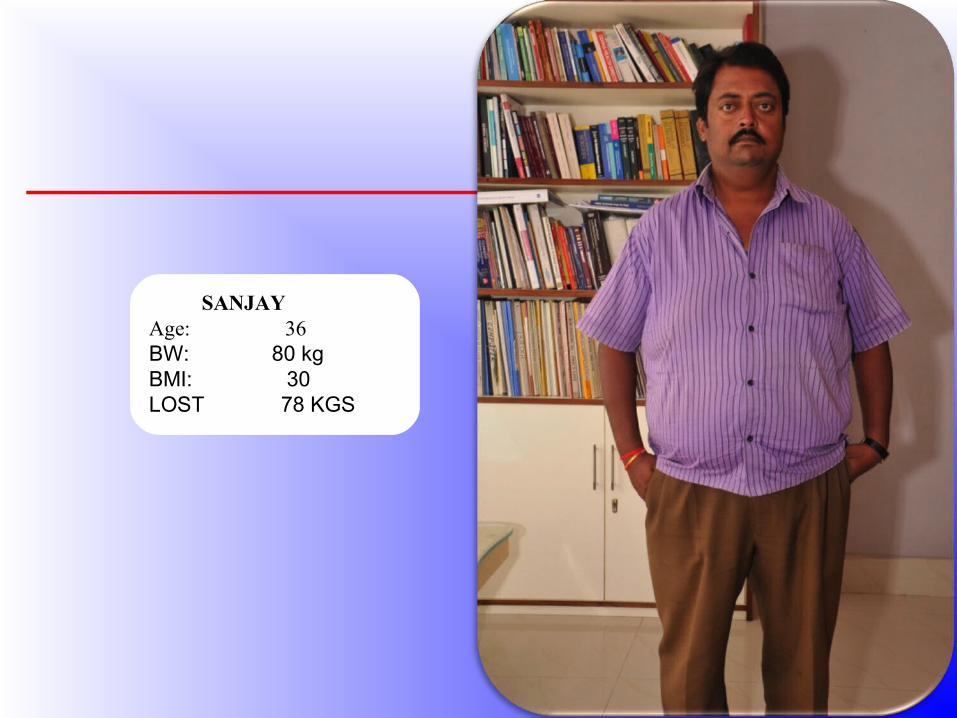
SANJAYAge: 36BW: 80 kgBMI: 30LOST 78 KGS

RAGHAV Age: 22BW: 135 kgBMI: 44.5 HTN: (+)DM: (+)

Age: 25BW: 72 kgBMI: 23.5LOST 63 KGS

SANTOSHAge: 57BW: 105 kgBMI: 46HTN: (+)DM: (+)OA: (+)Hypothyroidism: (+)
SANTOSH Age: 60Body Weight: 60 kgBMI: 25LOST 35 KGS
SUDATTAAge: 31BW: 100 kgBMI: 37HTN +PCOD +
SUDATTAAge: 32BW: 50kgBMI: 23LOST 50 KGS

APARAJITAAge: 29BW: 96 kgBMI: 36OA: (+)PCOD +
APARAJITAAge: 29BW: 60 kgBMI: 26LOST 36 KGS
HAPPY AFTER MARRIAGE


UMABALLAVAge: 50BW: 111 kgBMI: 39HTN: (+)DM: (+)ASTHMA: (+)OA: (+)Hypothyroidism: (+)Hyperlipidmia: (+)
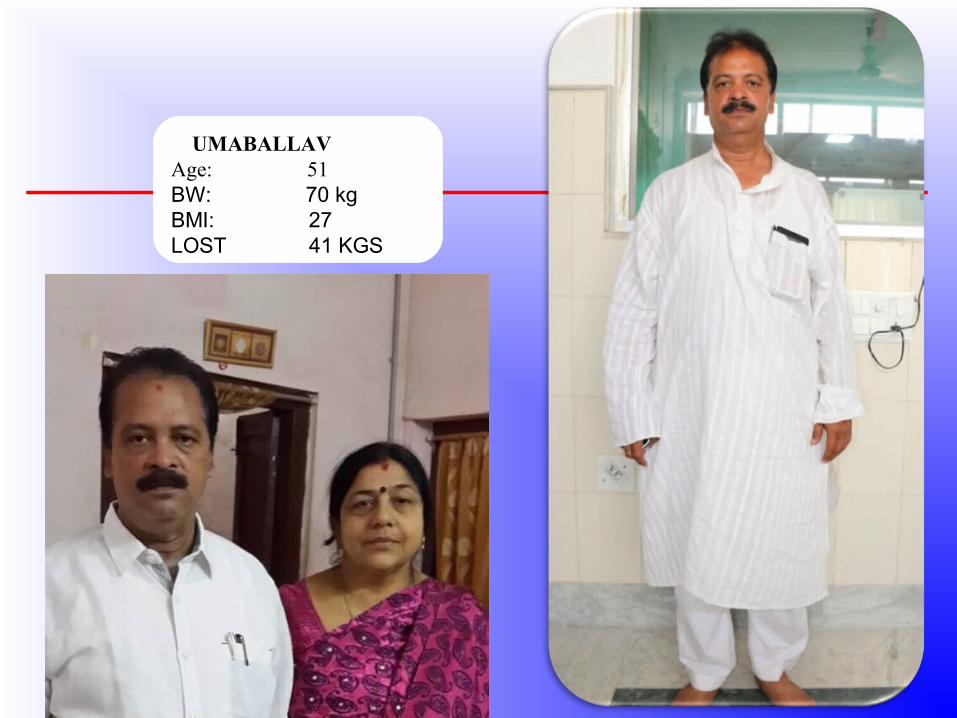
UMABALLAVAge: 51BW: 70 kgBMI: 27LOST 41 KGS

KISHANLALAge: 56BW: 107 kgBMI: 36.5HTN: (+)DM: (+)ASTHMA: (+)OA: (+)Hypothyroidism: (+)Hyperlipidmia: (+)

KISHANLALAge: 56BW: 76 kgBMI: 24.5LOST 31 KGS

MAHUAAge: 32BW: 108 kgBMI: 42Hypothyroidism: (+)Hyperlipidaemia: (+)

MAHUAAge: 32BW: 60 kgBMI: 27LOST 48 KGS

COMPLICATIONS (n=50)
• 1.Leak – 1 case,P.O day 15, GE junction > closed abscess, Halitosis.
• Endoscopic Septotomy , NGT feeding- 6 wks.
• 2.GE stenosis – late – after 1 yr.
• Managed conservatively with balloon dalatation.
• 3. Weight regain – after 2yrs – SG > MGB
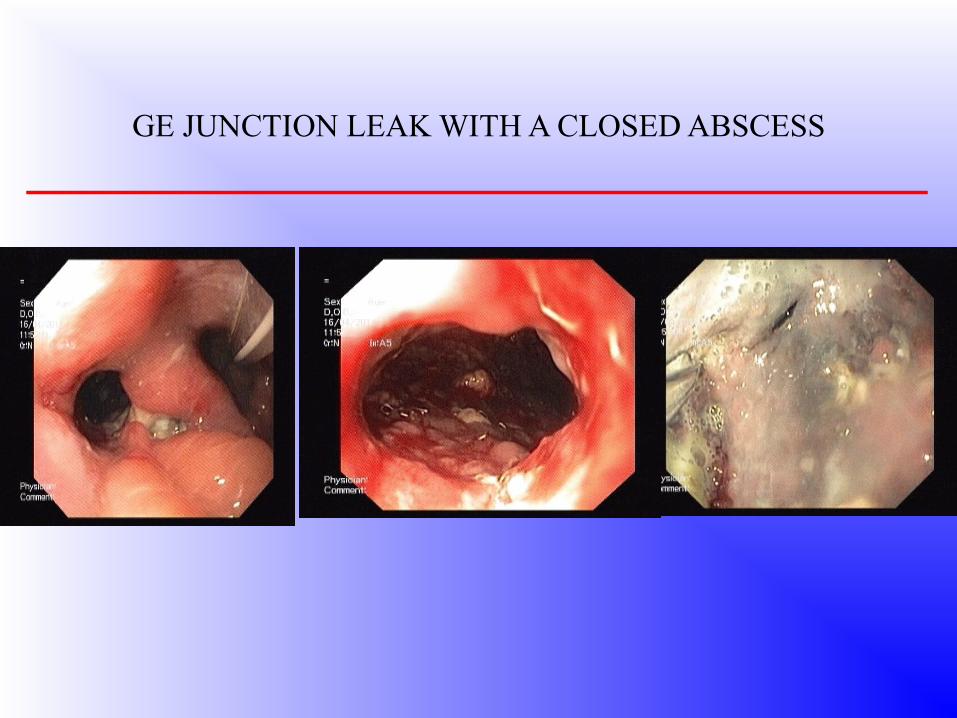
GE JUNCTION LEAK WITH A CLOSED ABSCESS

2nd Endoscopy
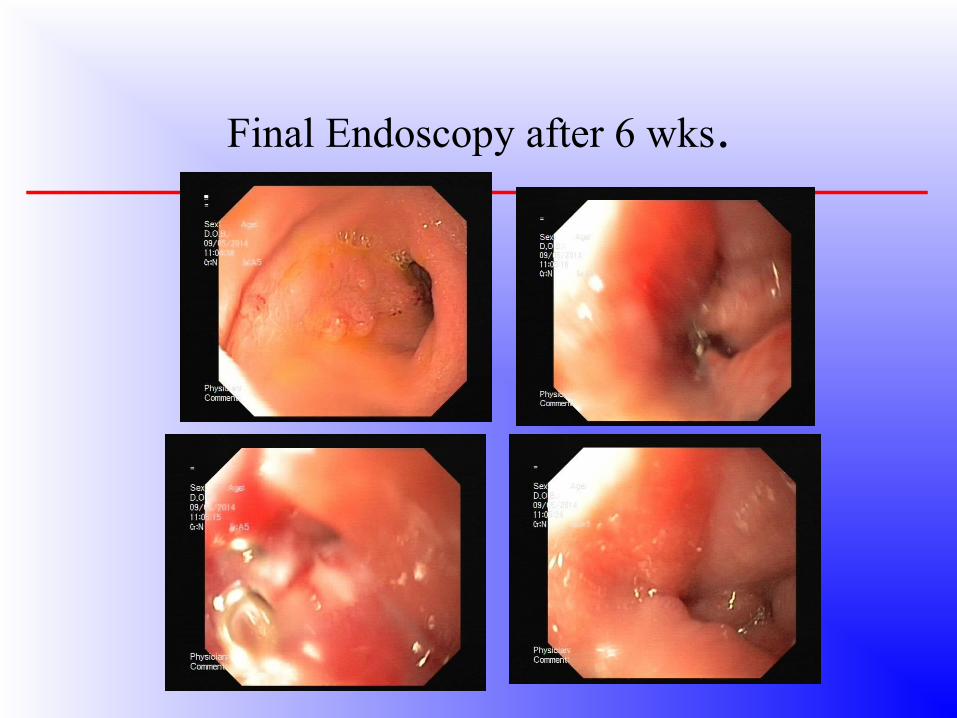
Final Endoscopy after 6 wks.
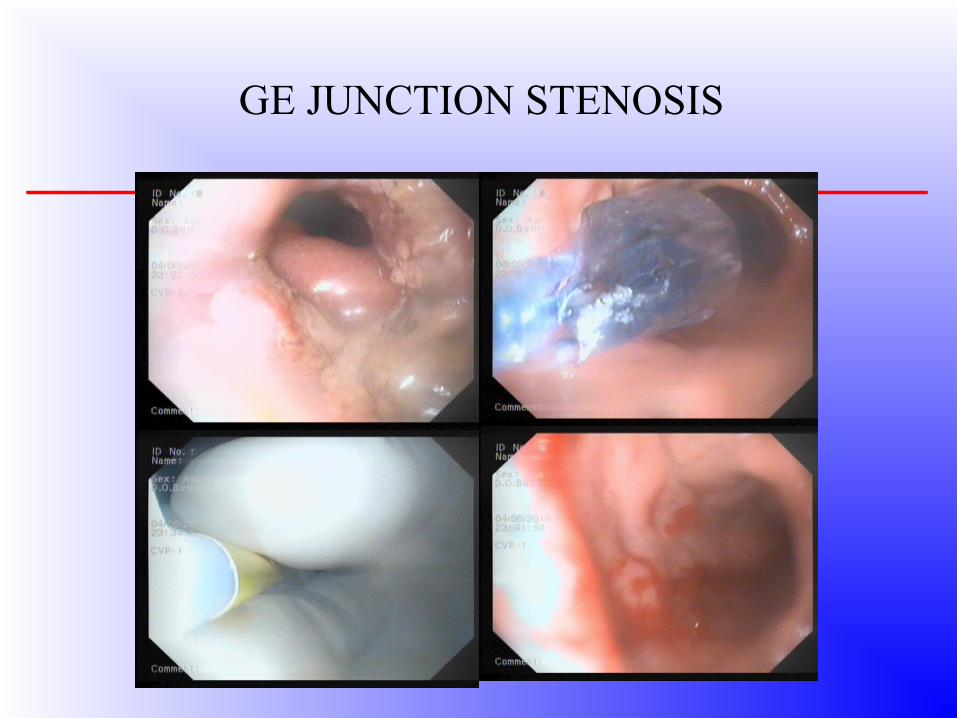
GE JUNCTION STENOSIS

ConclusionIn Bariatric Surgery
Everything is BIG!!!
Patient Risks
Expectations.
Multidisciplinary team Multidisciplinary team And ProgramAnd Program

THE XXXTH ANNUAL CONFERENCE OF ASI ODISHA
CHAPTER 2015
• DATE – 6-8 TH FEBRUARY 2015 • PLEASE BLOCK YOUR DATES
• 6TH - 3D LAP. WORKSHOP- 1ST TIME IN E.Z• 7 & 8TH – CONFERENCE
• VENUE- B.P.F,TV INSTITUTE, CUTTACK
• PLEASE REGISTER AT THE EARLIEST.

FOR YOUR PATIENT HEARING