33
The Democratisation of Information Dr. Gareth Goodier Chief Executive Melbourne Health 21 October 2015
| Date post: | 12-Apr-2017 |
| Category: |
Healthcare |
| Upload: | health-informatics-new-zealand |
| View: | 190 times |
| Download: | 9 times |

The Democratisation of Information
Dr. Gareth GoodierChief ExecutiveMelbourne Health
21 October 2015

• Serving more than 1 million Victorians
• Victoria’s first public hospital
• Provides local and tertiary/ quaternary academic health services
• Largest mental health service in Melbourne
• Services over 1.2 million Melburnians
• Opened in 2013• Joint venture with the
University of Melbourne• World-class institute in
infection and immunity
Royal Park Campus
City Campus

“The goal is to turn data into information, and information into insight.”
– Carly Fiorina (Former CEO and Chair Hewlett, Packard)
AnalyticsTools External:
Informationfor strategic
development and externaladvocacy
Internal:Insights to
inform operational and clinical decisions
• Embed analytics within decision making processes
• Drive behavioural change
• Improved outcomes for patients
• Improved resource utilisation• Faster response to challenges and opportunities
• Track Strategic Plan and Business Plan
• Benchmark with peer organisations
• Improved strength in negotiation with funding bodies
Data
DataDATA
DATAdata
Data
Data
Information is power
How do clinicians want information? Electronic Accessible Intuitive Graphical Real-time Reliable Comprehensive
“The most valuable commodity I know of is
information” – Gordon Gecko (Wall
Street)

The Business Intelligence Maturity Model
Several sources of
truth
Centralised information
Advanced Analytics
Information: • We have
consistent and accessible information across RMH
• Ongoing work with Consultant Attribution data accuracy
Insight:• We are
developing and acting on insights including:− Emergency − Length of Stay− Patient
Incidents− DNA rates
We are
here
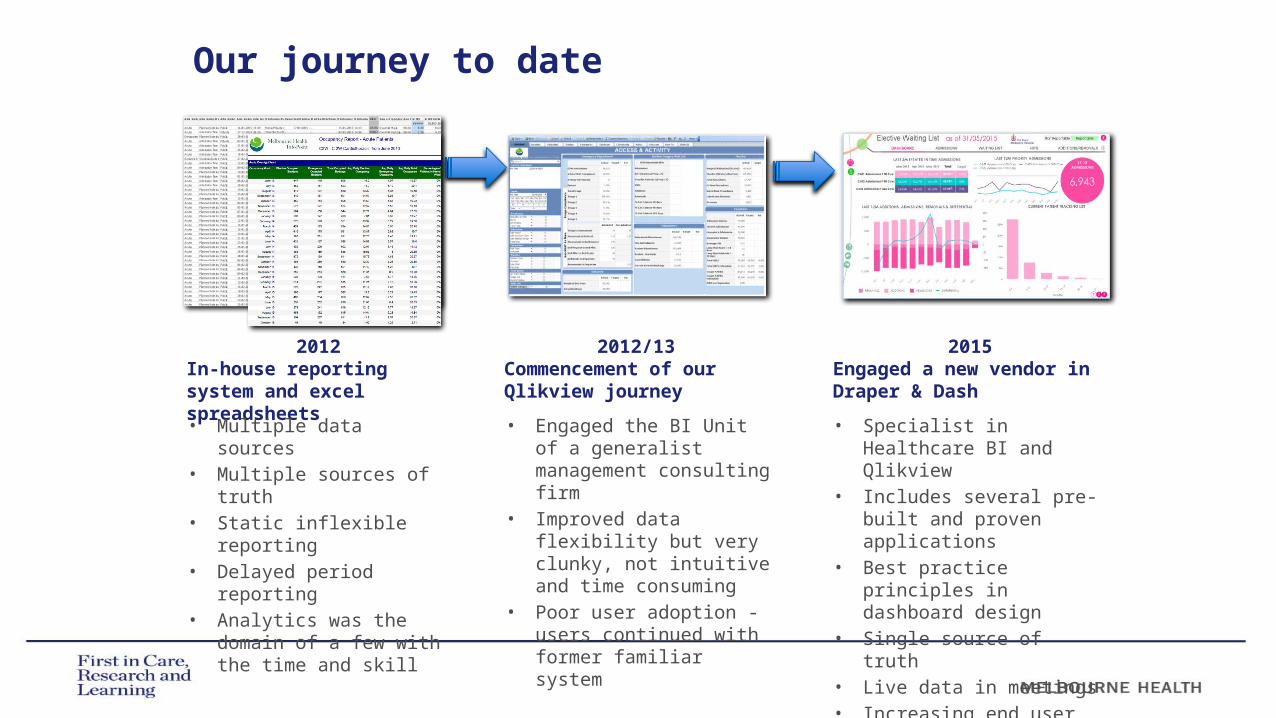
Our journey to date
2015Engaged a new vendor in Draper & Dash
2012/13Commencement of our Qlikview journey
2012In-house reporting system and excel spreadsheets
Admission Care TypeAdmission MethodAdmission Account GroupAdmission DateAdmission TimeDischarge MethodExpected DischargeMedical DischargeDischarge DateDischarge TimeDRG Same DayGender Age BandWIES WIES Estimation##### 18,012.36
Acute Planned AdmissionPublic 14-01-2015 13:49 Home/Private residence/accommodation17/01/2015 : - 15-01-2015 14:13 Q61B-RED BLOOD CELL DISDERS -CSCCOvernightMale 90-94 0.38 0.63Acute Admission from ED (VEMD only)Private 27-12-2014 20:39 Transfer to other hospital- - 07-01-2015 14:36 B70B-STROKE & OTH CEREB DIS +SCCOvernightFemale 90-94 1.36 4.29Designated Rehabilitation UnitPlanned AdmissionPublic 20-03-2015 15:55 Home/Private residence/accommodation- - 31-03-2015 08:42 Z60Z-REHABILITATIONOvernightFemale 85-89 0.00 0.00Acute Admission from ED (VEMD only)Private 03-01-2015 18:26 Home/Private residence/accommodation- - 08-01-2015 15:52 E62A-RESPIRATRY INFECTN/INFLAMM+CCCOvernightMale 80-84 1.64 1.71Acute Admission from ED (VEMD only)Public 31-01-2015 18:59 Home/Private residence/accommodation- - 01-02-2015 08:30 F66B-CORONARY ATHEROSCLEROSIS -CSCCOvernightMale 85-89 0.46 0.52Acute Admission from ED (VEMD only)Public 25-02-2015 15:11 Transfer to other hospital- - 27-02-2015 12:52 L67B-OTH KIDNY & URNRY TRCT DX-CSCCOvernightMale 90-94 0.62 0.62Acute Admission from ED (VEMD only)Public 18-02-2015 23:36 Statistical Separation- - 27-02-2015 16:01 F12B-IMPLANT/REPLCE PM,TOT SYS -CCCOvernightFemale 85-89 2.88 2.21Geriatric Evaluation & ManagementStatistical AdmissionPublic 27-02-2015 16:02 Home/Private residence/accommodation- - 17-03-2015 10:26 F76B-ARRHY, CARD & COND DISDR -CSCCOvernightFemale 85-89 0.00 0.00Acute Admission from ED (VEMD only)Public 12-02-2015 20:01 Home/Private residence/accommodation16/02/2015 : 15/02/2015 : 15-02-2015 12:29 L63A-KDNY & UNRY TRCT INF +CSCCOvernightMale 75-79 1.22 0.74Acute Admission from ED (VEMD only)Public 09-02-2015 13:50 Home/Private residence/accommodation- - 10-02-2015 16:50 E74C-INTERSTITIAL LUNG DIS -CCOvernightMale 90-94 0.77 0.54Acute Planned AdmissionPublic 19-02-2015 06:27 Home/Private residence/accommodation- 19/02/2015 : 19-02-2015 14:00 B05Z-CARPAL TUNNEL RELEASESame DayFemale 70-74 0.39 0.46Acute Admission from ED (VEMD only)Public 01-01-2015 18:36 Home/Private residence/accommodation- - 06-01-2015 15:36 E65B-CHRNIC OBSTRCT AIRWAY DIS -CCCOvernightFemale 70-74 1.07 0.83Acute Admission from ED (VEMD only)Public 08-02-2015 20:20 Home/Private residence/accommodation- - 12-02-2015 15:16 L63A-KDNY & UNRY TRCT INF +CSCCOvernightFemale 75-79 1.22 0.95Acute Admission from ED (VEMD only)Public 28-02-2015 17:58 Home/Private residence/accommodation01/03/2015 : - 01-03-2015 13:40 T63B-VIRAL ILLNESS -CCOvernightFemale 75-79 0.55 0.54Acute Planned AdmissionPublic 19-01-2015 13:41 Home/Private residence/accommodation- - 21-01-2015 09:13 F65B-PERIPHERAL VASCULAR DSRD -CSCCOvernightMale 75-79 0.77 1.23Acute Planned AdmissionPublic 25-02-2015 07:00 Home/Private residence/accommodation- - 27-02-2015 11:46 E42B-BRONCHOSCOPY -CCCOvernightMale 80-84 1.68 1.21Acute Admission from ED (VEMD only)Public 15-01-2015 20:25 Aged care residential facility19/01/2015 : - 16-01-2015 15:24 F76A-ARRHY, CARD & COND DISDR +CSCCOvernightFemale 90-94 1.26 0.54Acute Planned AdmissionPublic 03-01-2015 06:00 Home/Private residence/accommodation- - 03-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 05-01-2015 06:00 Home/Private residence/accommodation- - 05-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 07-01-2015 06:00 Home/Private residence/accommodation- - 07-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 09-01-2015 06:00 Home/Private residence/accommodation- - 09-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 12-01-2015 06:00 Home/Private residence/accommodation- - 12-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 14-01-2015 06:00 Home/Private residence/accommodation- - 14-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 16-01-2015 06:00 Home/Private residence/accommodation- - 16-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 19-01-2015 06:00 Home/Private residence/accommodation- - 19-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 21-01-2015 06:00 Home/Private residence/accommodation- - 21-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 23-01-2015 06:00 Home/Private residence/accommodation- - 23-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 26-01-2015 06:00 Home/Private residence/accommodation- - 26-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 28-01-2015 06:00 Aged care residential facility- - 28-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 30-01-2015 06:00 Aged care residential facility- - 30-01-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 02-02-2015 06:00 Home/Private residence/accommodation- - 02-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 04-02-2015 06:00 Home/Private residence/accommodation- - 04-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 06-02-2015 06:00 Home/Private residence/accommodation- - 06-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 09-02-2015 06:00 Home/Private residence/accommodation- - 09-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 11-02-2015 06:00 Home/Private residence/accommodation- - 11-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 13-02-2015 06:00 Home/Private residence/accommodation- - 13-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 16-02-2015 06:00 Home/Private residence/accommodation- - 16-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 18-02-2015 06:00 Home/Private residence/accommodation- - 18-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 20-02-2015 06:00 Home/Private residence/accommodation- - 20-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 23-02-2015 06:00 Home/Private residence/accommodation- - 23-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11Acute Planned AdmissionPublic 25-02-2015 06:00 Home/Private residence/accommodation- - 25-02-2015 11:00 L61Z-HAEMODIALYSISSame DayMale 70-74 0.11 0.11
• Multiple data sources• Multiple sources of
truth• Static inflexible
reporting• Delayed period
reporting • Analytics was the
domain of a few with the time and skill
• Engaged the BI Unit of a generalist management consulting firm
• Improved data flexibility but very clunky, not intuitive and time consuming
• Poor user adoption - users continued with former familiar system
• Specialist in Healthcare BI and Qlikview
• Includes several pre-built and proven applications
• Best practice principles in dashboard design
• Single source of truth• Live data in meetings • Increasing end user
adoption

The Democratisation of Information
“IT IS NOT JUST ABOUT PROVIDING BETTER INFORMATION. IT IS THE DEMOCRATISATION OF INFORMATION, LEADING TO CULTURE AND BEHAVIOUR CHANGE”

A new approach to reporting
“You can have data without information, but you cannot have information without
data” - Daniel Keys Moran
“Few people will appreciate the
music if I just show them the notes.
Most of us need to hear it”
- Hans Rosling

Performance at a glanceEmergency Department Visibility
Emergency Department

Targeted audience requirementsOutpatients
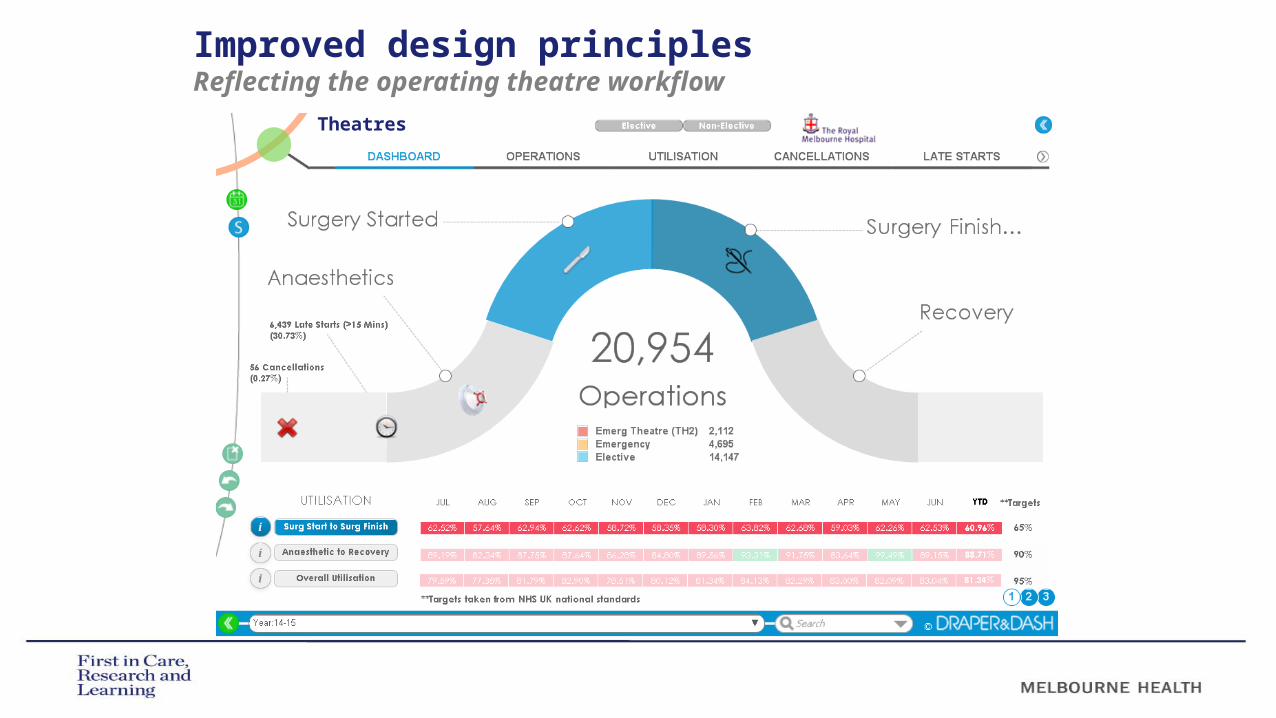
Improved design principlesReflecting the operating theatre workflow
Theatres
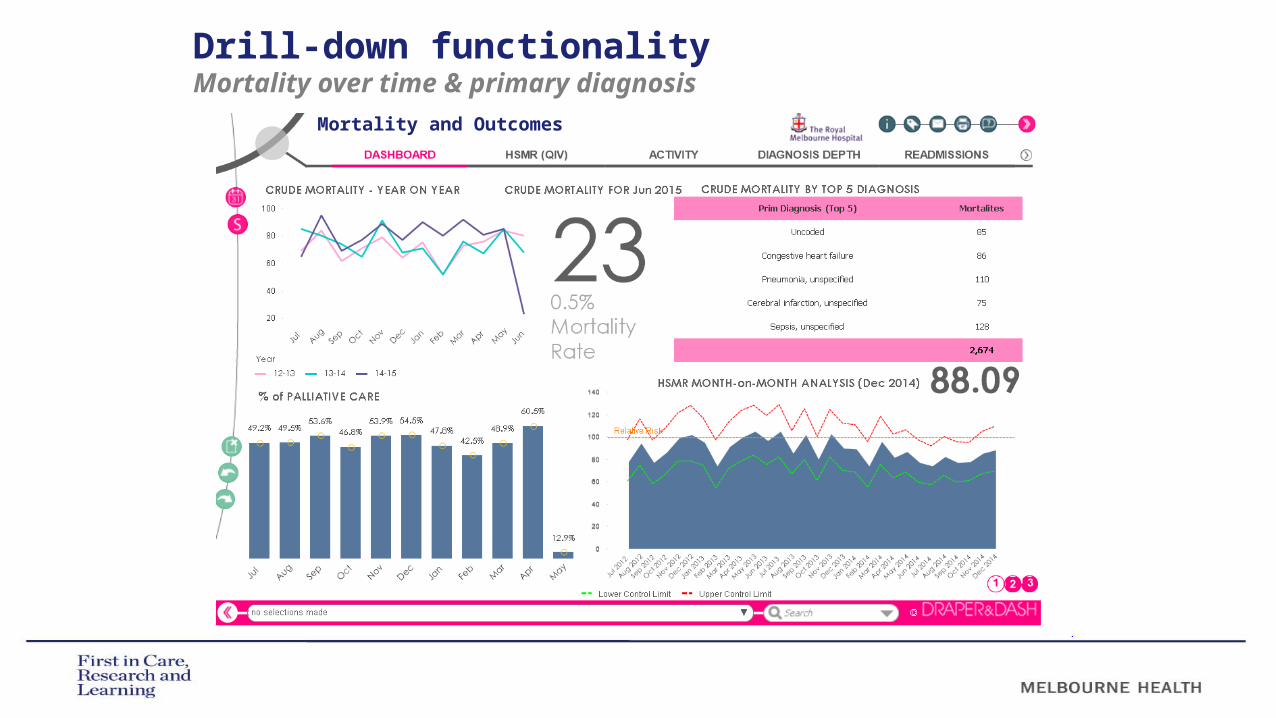
Drill-down functionalityMortality over time & primary diagnosis
Mortality and Outcomes

Focussed on key challengesUnderstanding readmissions
Readmissions

Driving user adoption
• Measuring and monitoring usage since re-launch in April 2015
• Uptake continues to be supported by:− Launch and
promotional activities
− Education− Scorecard
reporting− Cultural change

The data is wrong
DENIAL
It does not apply to me
ANGER
I will get the correct data
But we are special
BARGAINING
There is nothing I can do about it
DEPRESSION
Acceptance and action
RESOLUTION
Adapted from Elisabeth Kübler-Ross 5 stage model
The 5 stages of data grief

Relentless focus on variation
•“IN THE LAST 30 YEARS, RESEARCH HAS DEMONSTRATED THAT:1) quality can be measured, 2) that quality varies enormously, 3) that where you go for care affects its quality far more than who
you are, and4) that improving quality of care, while possible, is difficult and
painful”.– Brook, McGlynn & Shekelle (2000)
•EVIDENCE SUGGESTS THAT THERE IS, AT BEST, A TWO TO THREE FOLD VARIANCE IN CLINICAL BEHAVIOUR/TREATMENT PRACTICE ACROSS MEDICINE
•WHERE THERE IS POOR CLINICAL EVIDENCE (E.G. ADHD) THE VARIATION CAN INCREASE TO MORE THAN A TWENTY FOLD DIFFERENCE
“If all variation were bad, solutions would be easy. The difficulty is in reducing the bad variation, which reflects the limits of professional knowledge and failures in its application, while preserving the good
variation that makes care patient centered”
- AJ Mulley (BMJ, 2010)

“The most expensive item in the hospital is the
Doctor’s pen”
Variation – at what cost?

International variation
Foreign body left in during procedure in adults,
2011
Average length of stay for acute myocardial infarction (AMI), 2011
Different rates of
mortality from
cancer in people <75yrs
Source: OECD Health Statistics 2013

The power of transparency
Case Examples
“However beautiful the strategy, one should occasionally look at the
results” -
Winston Churchill

Case Example 1: Improving patient safety - FallsIdentifying contributing factors
11am
3pm 9p
m
Understanding falls incidents by: • Ward• Outcome• Time• Patient level
details• Age• Location• Time• Activity
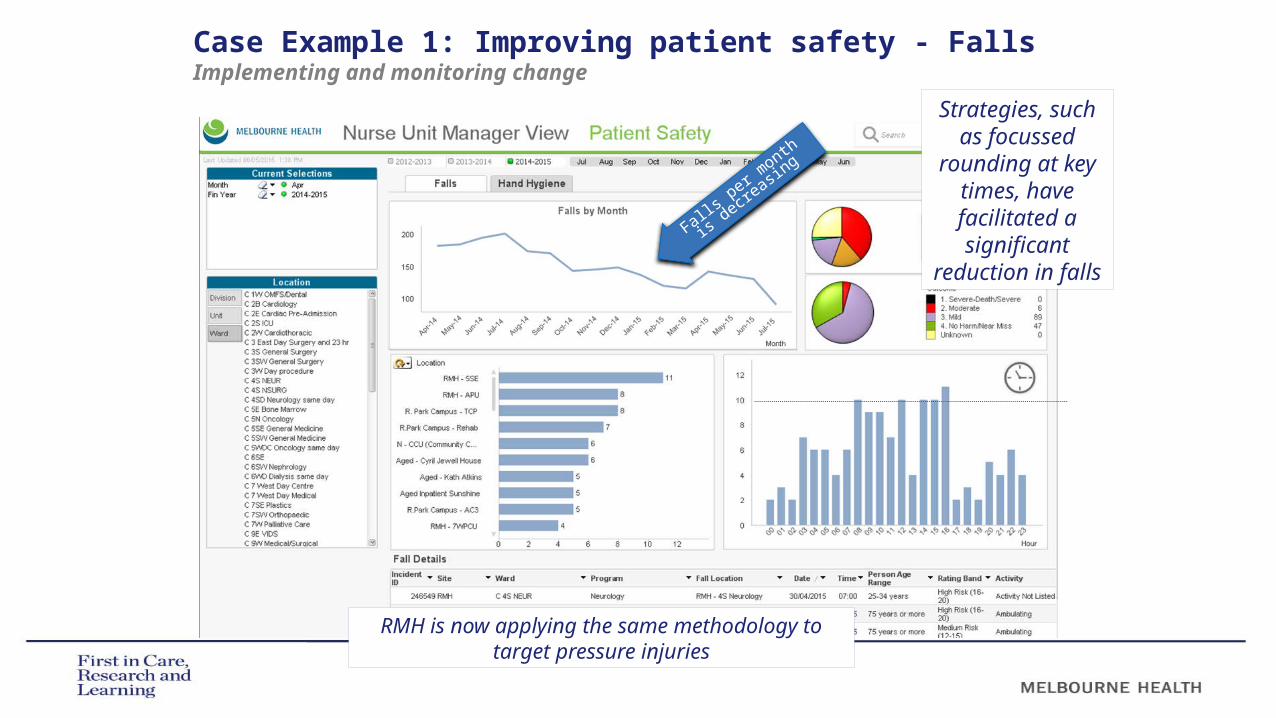
Case Example 1: Improving patient safety - FallsImplementing and monitoring change
Strategies, such as
focussed rounding at key times,
have facilitated a significant
reduction in falls
RMH is now applying the same methodology to target pressure injuries
Falls p
er mon
th is
decreas
ing
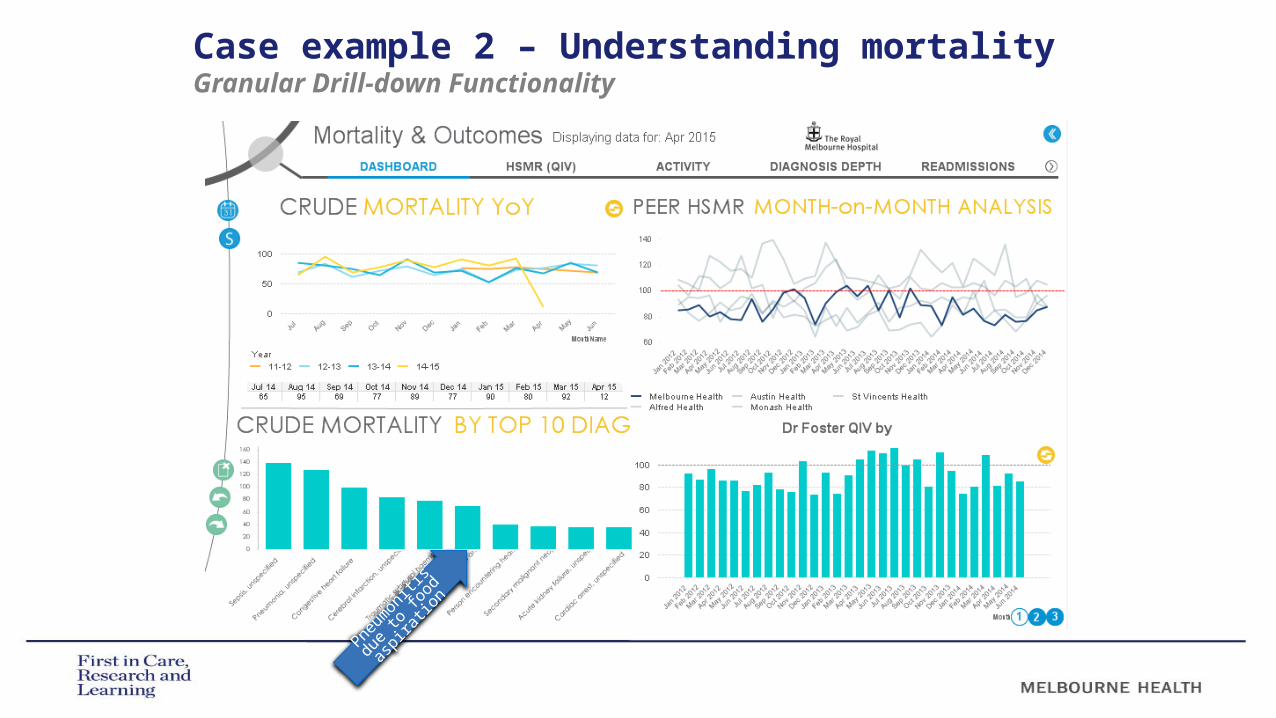
Pneu
moniti
s due
to foo
d
aspir
ation
Case example 2 – Understanding mortality Granular Drill-down Functionality
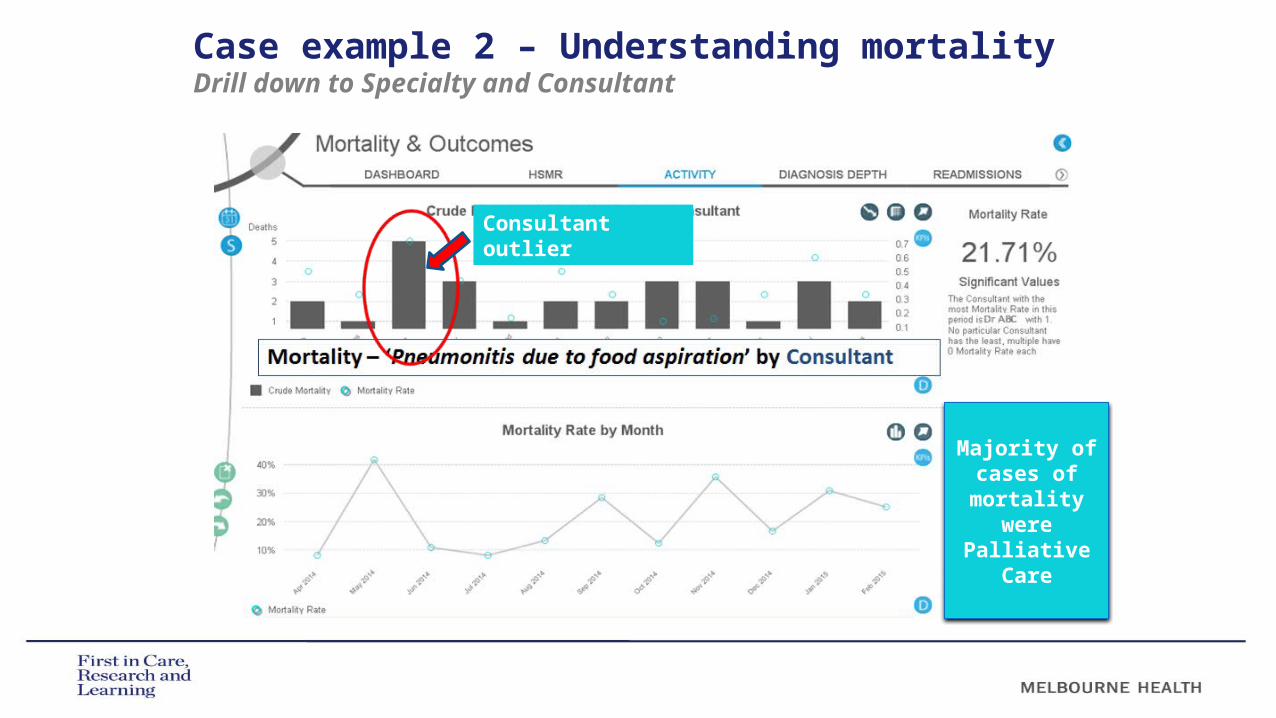
Case example 2 – Understanding mortality Drill down to Specialty and Consultant
Consultant outlier
Majority of cases of
mortality were
Palliative Care
Audit of 60 cases of mortality from aspiration pneumonia
More than half (32/60) were admitted from 23 different nursing homes with aspiration pneumonia
Speech Pathologist and Physician worked with nursing homes to improve management of patients with dysphagia:
– dysphagia management guidelines– e-learning package– expert advice– advance care planning for patients with chronic
dysphagia
Case example 2 – Understanding mortality Using data for improvement

RMH HAS HAD SIGNIFICANT SUCCESS WITH SHORT STAY SURGICAL MODELS OF CARE THAT BOTH REDUCE LENGTH OF STAY AND REDUCE COMPLICATIONS
OUR EMERGENCY GENERAL SURGERY MODEL HAS DELIVERED REDUCED LOS, REDUCED COMPLICATIONS, A REDUCTION IN CONVERSION TO SURGERY AND A STATISTICALLY SIGNIFICANT REDUCTION IN MORTALITY (SHAKERIAN ET AL, WJS, 2015; SHAKERIAN ET AL, BJS ACCEPTED FOR PUBLICATION AUGUST 2015)
ARE THERE OPPORTUNITIES TO MAKE SIMILAR IMPROVEMENT TO LOS AND OUTCOMES IN THE ELECTIVE PATIENT COHORT?
Benchmarking surgical LOS with
British Association of Day Surgery
(BADS)
Case Example 3: Improving resource utilisationIn-depth analysis and benchmarking

Case Example 3: Improving resource utilisationIn-depth analysis and benchmarking
1. Filte
r data
using apps 2. E
xport for in
depth analysis

Case Example 3: Improving resource utilisationIn-depth analysis and benchmarking
BADS
BADS Target%Day Case
RMHDC %
Cases Below BADS
Target
Net Financial Outcome Modelling
Breast SurgeryExcision/biopsy of breast tissue ± localisation 95% 53.10% 24 58,894$ Simple Mastectomy (inc axillary node biopsy) 15% 0.00% 5 23,395-$
Breast Surgery Total 29 35,499$
CardiologyElective cardioversion 95% 66.30% 25 89,391$
Implantation of cardiac pacemaker 50% 0.00% 105 153,873$ Cardiology Total 130 243,264$
ENT/Head and NeckFESS Endoscopic uncinectomy, anterior and posterior 50% 6.70% 5 8,933$
Intranasal antrostomy inc luding endoscopic 80% 0.00% 2 3,573$ Biopsy / Sampling of cervical lymph nodes 40% 0.00% 1 5,229$
Enucleation of cyst of jaw 95% 80.00% 1 2,141$ Exc ision of submandibular gland 30% 0.00% 1 7,103$
ENT/Head and Neck Total 10 26,979$
General SurgeryExcision biopsy of lymph node for diagnosis (cervical, 40% 0.00% 2 8,299$
Inc ision and drainage of perianal abscess 90% 34.10% 9 3,318$ Laparoscopic repair of hiatus hernia with anti-reflux 40% 0.00% 1 2,101$
Pilonidal sinus surgery - laying open or suture/skin graft 45% 38.50% 20 5,514$ Primary repair of femoral hernia 90% 0.00% 1 1,611$ Primary repair of inguinal hernia 95% 29.40% 12 15,677$
Repair of other abdominal hernia 85% 0.00% 1 1,611$ General Surgery Total 46 38,131$
OphthalmologyDacryocystorhinostomy inc insertion of tube 90% 40.00% 3 5,332$
Surgical trabeculectomy or other penetraating 95% 0.00% 1 1,290$ Ophthalmology Total 4 6,622$
OralSurgical removal of impacted / buried tooth / teeth 95% 9.00% 11 19,935$
T&OArthroscopy of knee including menisectomy, meniscal 95% 0.00% 1 425$
Neurolysis and transposition of peripheral nerve e.g 95% 0.00% 3 3,509-$ Repair of hand or wrist tendon 90% 29.10% 34 66,463$
T&O Total 38 63,380$
RMH TOTAL 268 433,810$
Royal Melbourne Hospital
Indicators
COMPARING RMH SHORT STAY SURGERY EPISODES WITH BADS BENCHMARKS
IDENTIFIED COHORTS WITH LONGER LOS
FINANCIAL OUTCOME MODELLING IDENTIFIED A SAVINGS OPPORTUNITY OF $433K IF RMH ALIGNED AREAS OF LONGER LOS WITH WITH BADS TARGETS
WORK PROGRESSING IN CARDIOLOGY AND GENERAL SURGERY TO REVIEW CURRENT MODELS AND THE APPLICABILITY OF BADS MODELS OF CARE FOR LOCAL IMPLEMENTATION AT RMH
Implan
tation
of
pacemak
er.
BADS suggest
50% day
case.
RMH curre
ntly 0%

Lessons learned
CULTURE ‘DEMOCRATISATION OF INFORMATION’ LEADING TO
CULTURE AND BEHAVIOUR CHANGE
ACTIVELY PROMOTE DATA TRANSPARENCY
STAFF ENGAGEMENT IS IMPORTANT
““Opportunities multiply as they are seized” - Sun Tzu

Lessons learned
OPERATIONAL A BUSINESS INTELLIGENCE PROGRAM REQUIRES BOTH TECHNICAL
AND CLINICAL EXPERTISE TO DEVELOP AND DELIVER
INVEST IN BUSINESS INTELLIGENCE TOOL THAT IS GRAPHICAL AND INTUITIVE
TAKE PRAGMATIC APPROACH TO DATA ACCURACY – IT TENDS TO IMPROVE WITH TRANSPARENCY AND EXPOSURE
PROMOTE AND MEASURE END USER ADOPTION
A CHANGE MANAGEMENT APPROACH IS ESSENTIAL – THE EMBEDDING OF ANALYTICS INTO ORGANISATIONAL DECISION MAKING IS BOTH A TECHNICAL AND A CULTURAL JOURNEY
CONSULTANT ATTRIBUTION
PATIENT LEVEL COSTING BY SUB-CATEGORY (I.E. PHARMACY AND THEATRE MINS)
EXTERNAL BENCHMARKING
““Opportunities multiply as they are seized” - Sun Tzu

What can a data driven hospital achieve?
HIGH QUALITYRMH HAS A LOW STANDARDISED MORTALITY
RATE (HSMR 80; AUGUST 2015)
REDUCED LENGTH OF STAY• RMH has an 86% Relative Stay Index compared
with all major Australian hospitals.
REDUCED COST • RMH is $600 lower cost per funding unit (WIES)
than the closest peer hospital; • The National Health Performance Authority
(NHPA) reported the RMH is the “LOWEST” cost tertiary hospital in Australia.
“The price of light is less than the cost of darkness” - Arthur C. Nielsen

Our next steps…
MOBILE APPLICATIONS“MOBILE IS THE FUTURE OF EVERYTHING” –
FORBES
MOBILE APPLICATIONS FOR SENIOR DOCTORS EARLY 2016
GRANULAR LEVEL BENCHMARKING• Combine benchmarking data with drill down
functionality
KEY IN DEPTH ANALYTICS PROJECTS • Linking clinical costings with patient outcomes
in Orthopaedics• Understanding and monitoring readmissions
“Hiding within those mounds of data is knowledge that could change the
life of a patient, or change the world”
- Atul Butte

















