31
The Dept. OB/GY of the first hospi The Dept. OB/GY of the first hospi tal of Xi’an Jiao Tong university tal of Xi’an Jiao Tong university Cervical carcinoma
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | norma-glenn |
| View: | 216 times |
| Download: | 0 times |

The Dept. OB/GY of the first hospital of Xi’aThe Dept. OB/GY of the first hospital of Xi’an Jiao Tong university n Jiao Tong university
Cervical carcinoma
Etiology
• Sexual activity• HPV infection-16,18 types.• Tobacco use• Oral contraceptive pill• Herpes simplex infection• High-risk men• etc
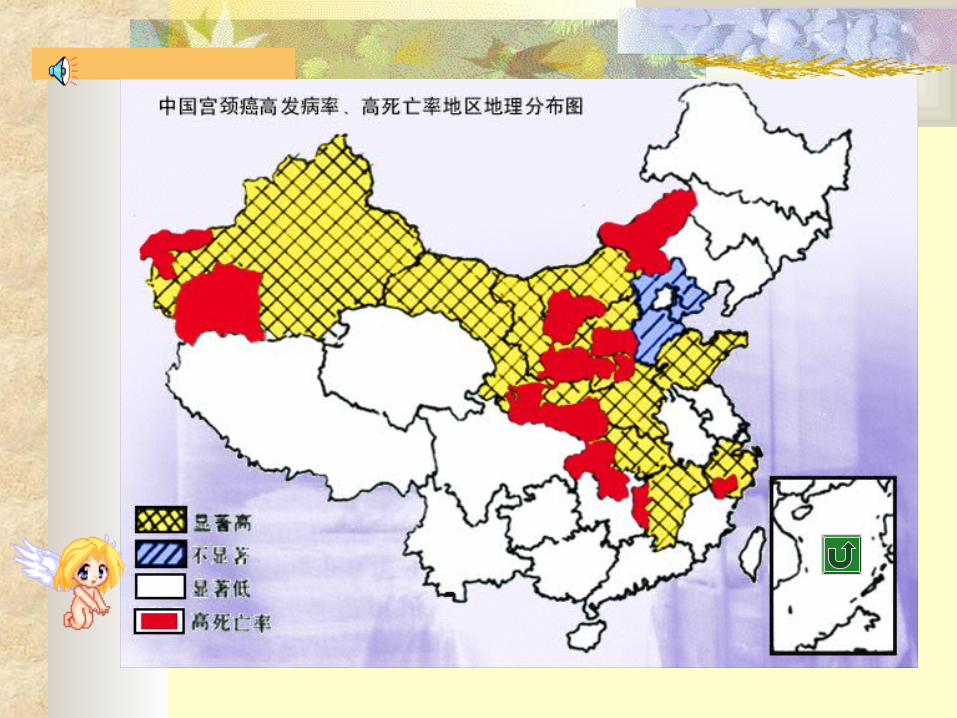

General considerations Dichotomy of its incidence in developed
and developing countries Average age at diagnosis 51 years Model of a “controllable ” cancer 5-year survival for stage I >91%, stage IIA,
stage IIIA, IV are 83%, 45%, 14%

Tran
sformation
zon
e
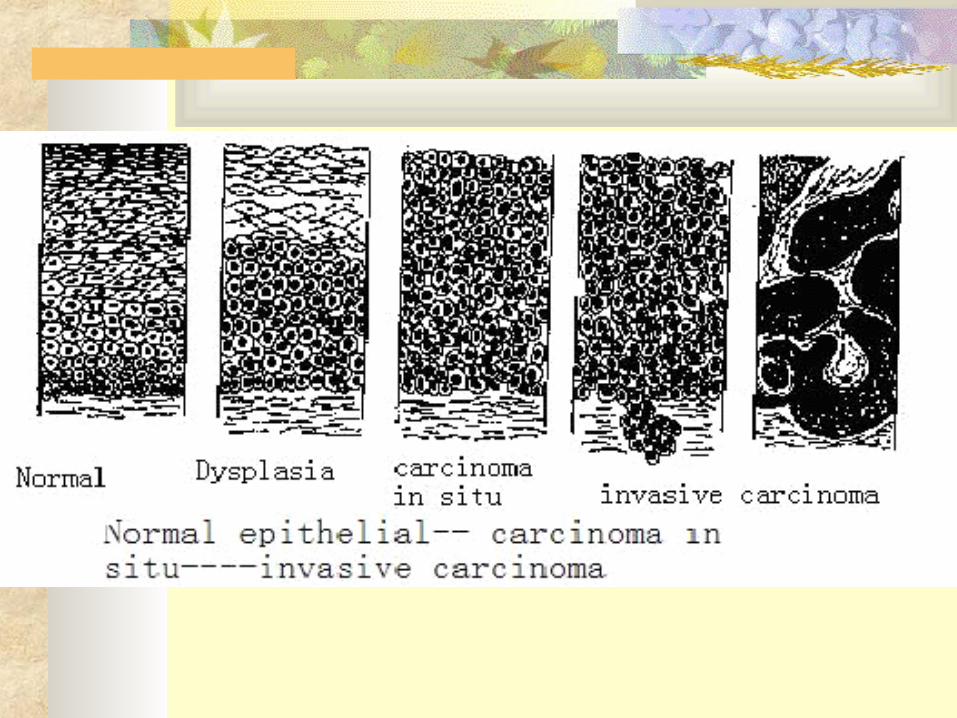

Pathology Squamous carcinoma: 80-95% Adenocarcinoma: 15% Adenosquamous carcinoma: 3-5%

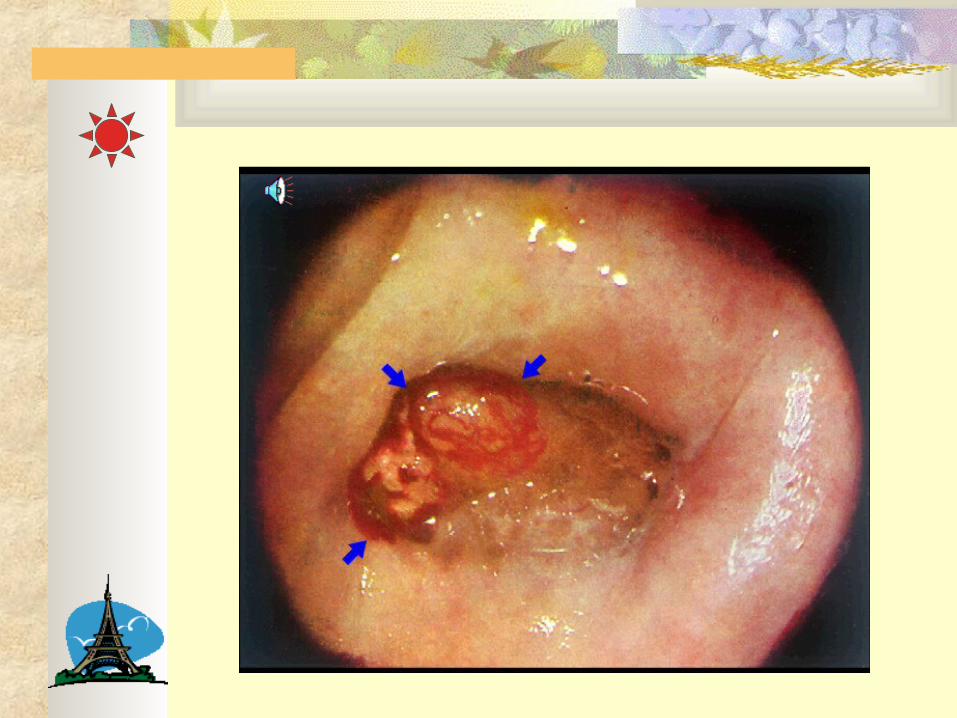
Ectophytic growthendophytic growthUlcerating growthEndocervial growth
Gross p
athology
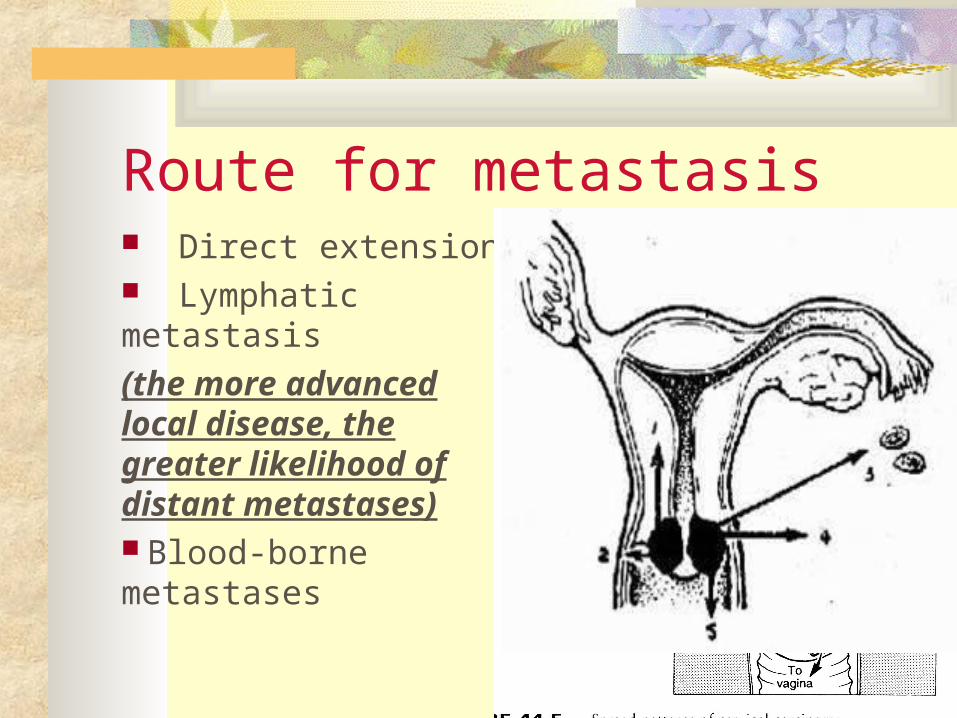
Route for metastasis Direct extension Lymphatic metastasis
(the more advanced local disease, the greater likelihood of distant metastases) Blood-borne metastases

Clinical FIGO StagingStage I I Strictly confined to cervix
IA. Microscopically diagnosed preclinical lesion, stromal invasion with depth <5.0 mm and width < 7.0mm.
IA1 Stromal invasion no greater than 3.0 mm and no wider than 7.0 mm
IA2 Stromal invasion > 3 mm and < 5 mm, horizontal invasion < 7 mm
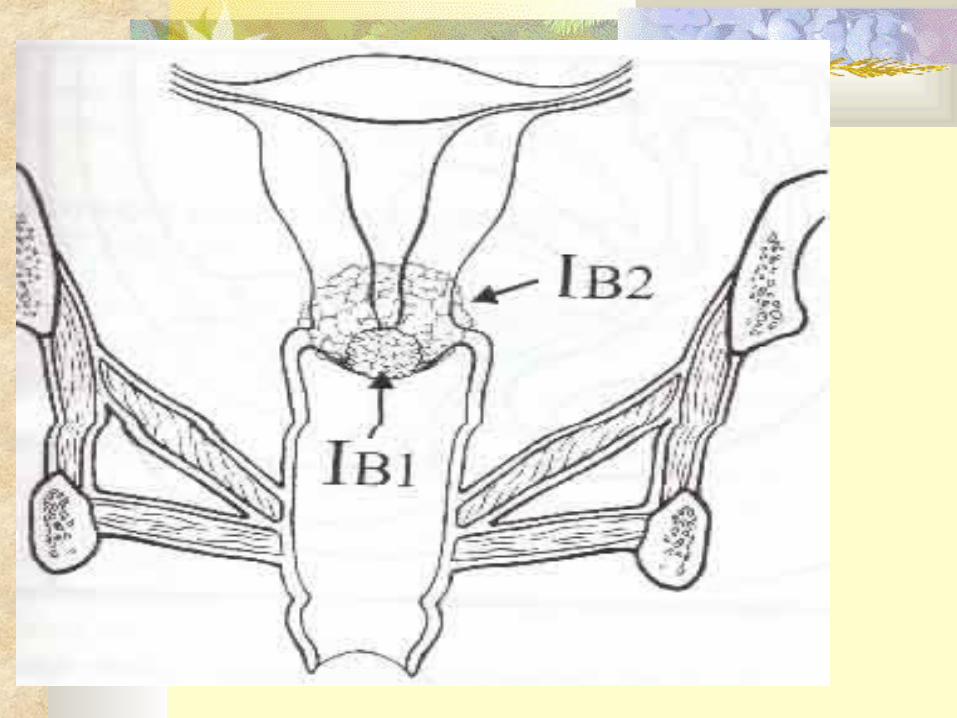
IB Clinical lesions confined to cervix or preclinical lesions greater than stage IA.
IB1 Clinical lesion no longer than 4.0 cm in size
IB2 Clinical lesion greater than 4.0 cm in size
Stage II
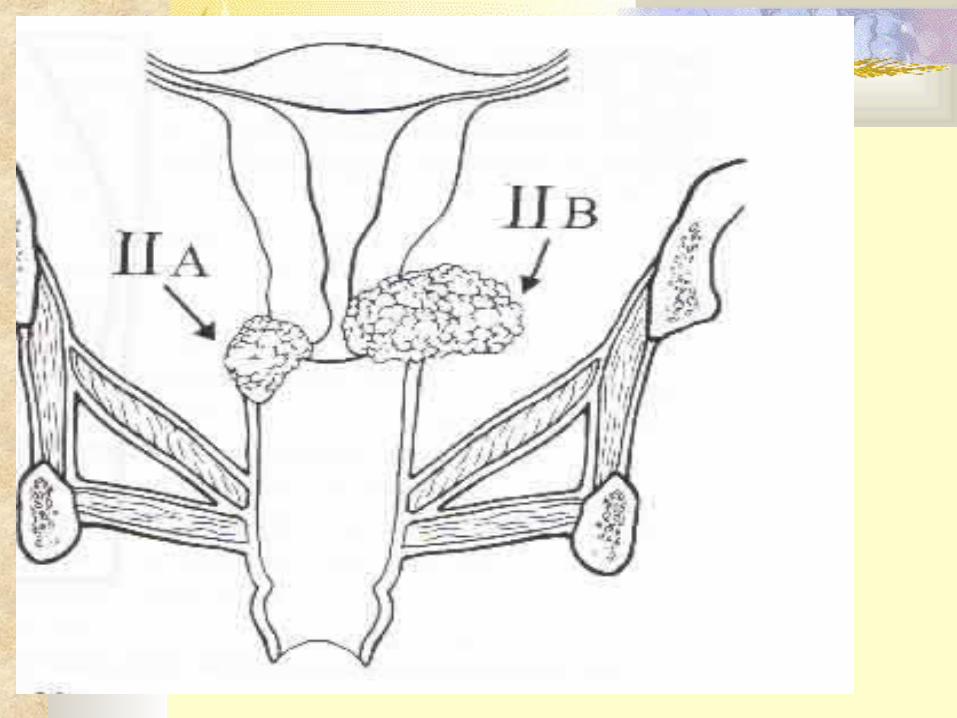
II Extension beyond cervix but not to pelvic wall. Involves vagina, but not the lower third.
IIA Involves vagina, but not lower third. No obvious extension to parametrium.
IIB Involves vagina, but not lower third. Obvious parametrial involvement.
Stage III
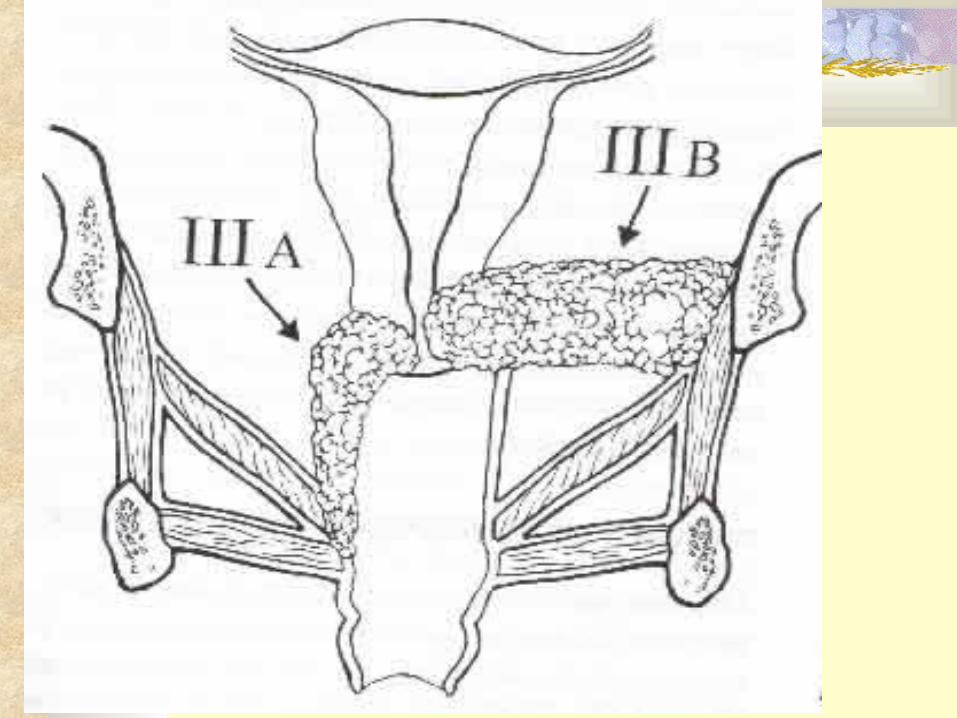
III Extension to pelvic wall. On rectal exam, no cancer-free space between tumor and pelvic wall. Involves lower third of vagina.
IIIA No extension to pelvic side wall.
IIIB Extension to pelvic side wall.
Stage IV IV Extension beyond true pelvis, involvement of bladder or rectal mucosa.


Clin
ical find
ings
Clinical Finding:
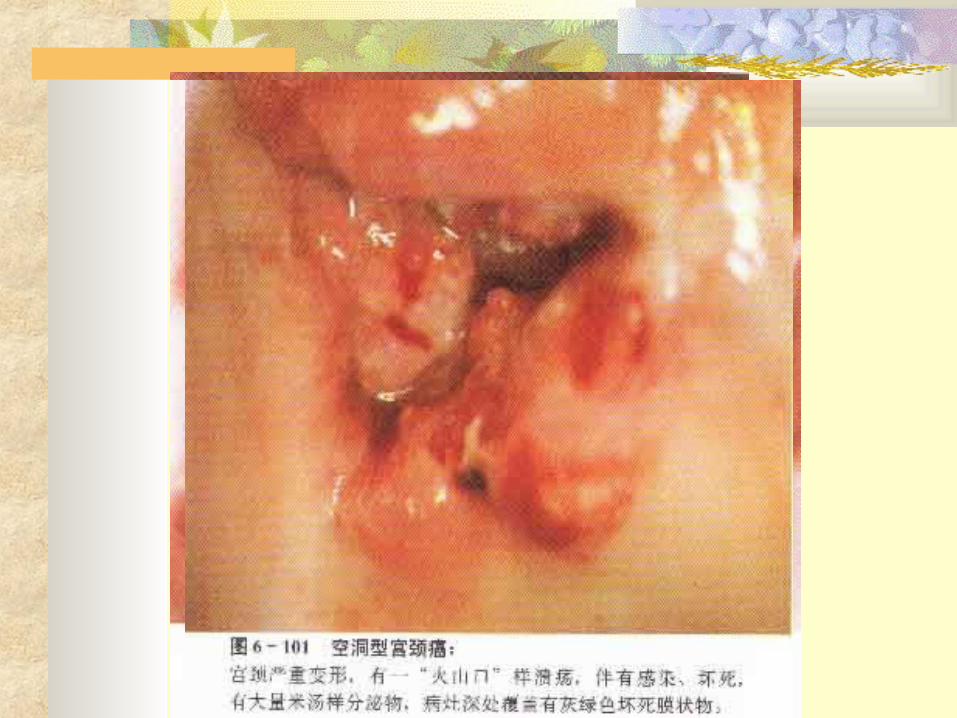
⒉Signs Gross inspection
⒈Symptoms :①Vaginal bleeding②Vaginal discharge③Pain④Involvement of adjacent organs⑤Cachexia
Early stage: postcoital bleedingMid and end stage : blood stained leukorrhea, spotting, frank bleeding
White or sanguineous PurulentOdorousCopious
Unilateral, radiatingHip or thignAdvanced stage ,
Bladder involvementFrequency and difficulty in urination, bloody urinePainful bowel movementDiarrheaRectal symptoms ectophytic
endophytic ulcerating endocervical
Signs of metastasis
Frozen pelvis : last stageThickened Parametrial tissueNo tumor-free space between cervix and pelvisIncarcerated uterus
① Pap smear
② Schiller test
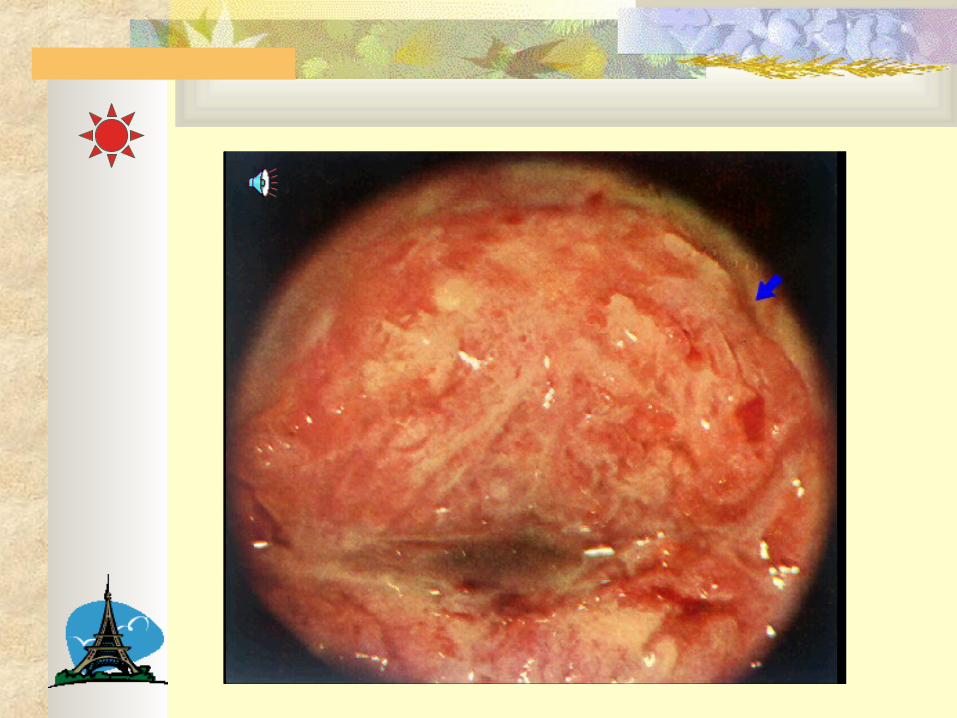
③ Colposcopy and biopsy
④ Punch biopsy and ECC
Laboratory examinationDiagn
ostic p
rocedu
res
⑤ Conization
⑥ Chest X-ray, IVP, lymphoangiography, cystoscopy, CBC, barium enema, chemistry

Differential diagnosis Chronic cervicitis Cervical TB Cervical papilloma Cervical metastasis of endometrial
carcinoma
Treatment: operation, radiation therapy, chemotherapy
Operation: IA-IIb Ia1: total hysterectomy or conization
Ia2- IIb: radical hystrectomy+ pelvic lymphadenectomy
Ovarian preservation for young women

Treatment: operation, radiation therapy, chemotherapy
Radiation therapy Ib- IIb: poor surgical candidates
Patients with more advanced diseases More extensive LN involvement High-dose external beam + intracavitary irradiation Ovarian function destroyed Complications: radiation cystitis and proctitis Preoperative or postoperative

1. Cisplatin based regimen.
2. Adjuvant treating modality to operation and radiation.
3. Systematic administration or radiographic interventional therapy
Treatment: operation, radiation therapy, chemotherapy

regimens (squamous carcinoma)
DDP 50mg/m2 1d }3WBIP BLM 15mg 1d IFO 1mg/m2 1-5d
DDP 50mg/m2 1dPVB BLM 20mg 1-3d }3W VCR 1mg/m2 1d
DDP 60mg/m2 1dPAM MTX 30mg/m2 1d }3W ADM 50mg 1d
Prognosis
Stage, LN invasion, tumor volumn, depth of cervical stromal invasion, pathologicla type
5-year survival for stage I >91%, stage IIA, stage IIIA, IV are 83%, 45%, 14%
Uremia Hemorrhage Infection Cachexia
Follow-up study



复习题
单
选
题
Cervical carcinoma is most likely to arise from A . Squamous epithelium B . Columnar epithelium C . SCJ D . Endocervical epithelium E . Squamous epithelium undergoing hyperp
lasia

Colposcopy is best used for the diag
nosis of :
A Submucous myoma
B Endometriosis
C Endometrial carcinoma
D Cervical carcinoma
E Endometrial polyp

she , 35y , increased amount of vaginal discharge for 1 y , occasional postcoital bleeding ,yellow vaginal discharge without odor, chronic pain in the lower back. Signs: cervical erosion II, granule, normal pelvis. Cervical cytology: ± she should receive which following procedure:
A . Repeat pap smear and cytological evaluation B . Ioding test C . Colposcopy + biopsy D . Diagnostic curretage E . Hysteroscopy

谢 谢 !
Thanks!

















