The Devil is in the Details The Devil is in the Details R. J. Frascone, MD, R. J. Frascone, MD, FACEP FACEP Medical Director EMS Medical Director EMS Regions Hospital Regions Hospital EMS, St. Paul, MN EMS, St. Paul, MN Professor of Professor of Emergency Med Emergency Med University of University of Minnesota Minnesota 1
Transcript
The Devil is in the DetailsThe Devil is in the Details R. J. Frascone, MD, FACEPR. J. Frascone, MD, FACEP
Medical Director EMSMedical Director EMS Regions Hospital EMS, St. Paul, Regions Hospital EMS, St. Paul, MNMN Professor of Emergency MedProfessor of Emergency Med University of MinnesotaUniversity of Minnesota
1
These trials were studying two These trials were studying two different things, in two very different things, in two very
different waysdifferent ways
The RESQ Trial studied the The RESQ Trial studied the combination of ACD/ITD CPR vs S-combination of ACD/ITD CPR vs S-CPRCPR
ROC PRIMED studied ITD CPR vs S-ROC PRIMED studied ITD CPR vs S-CPRCPR
But,But, The RESQ Trial looked at only The RESQ Trial looked at only
ACD/ITD vs S-CPRACD/ITD vs S-CPR ROC PRIMED looked at two different ROC PRIMED looked at two different
things: Early vs late defibrillation and things: Early vs late defibrillation and ITD CPR vs S-CPR and they did it with ITD CPR vs S-CPR and they did it with a multifactoral approacha multifactoral approach
Both trials were complex, but Both trials were complex, but PRIMED was extraordinarily complexPRIMED was extraordinarily complex
First A ReviewFirst A Review(sorry)(sorry)
Standard CPRStandard CPR
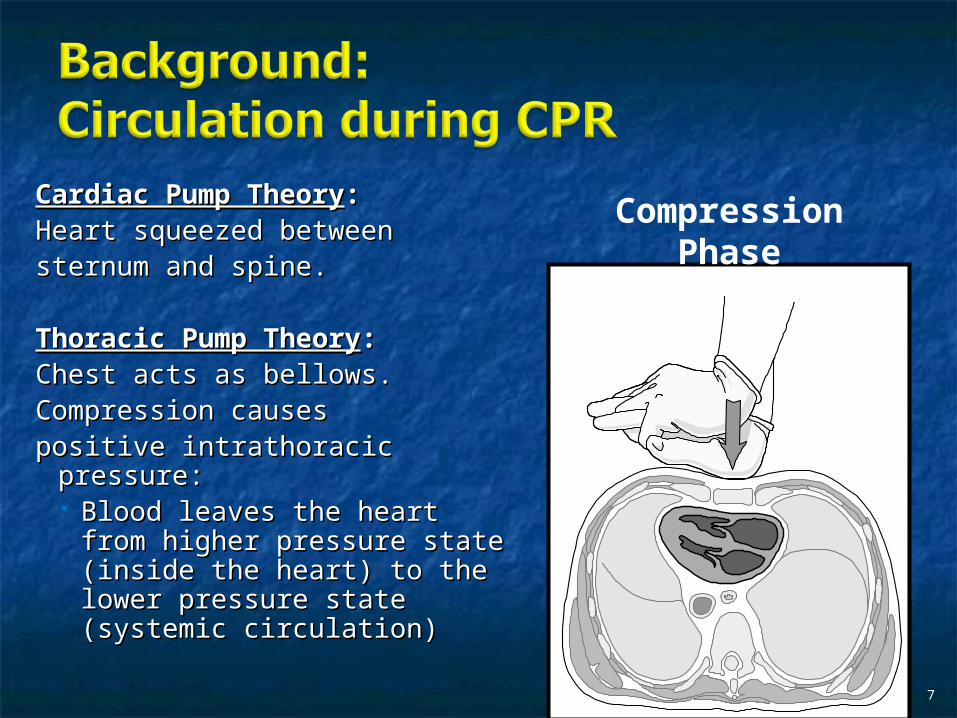
Cardiac Pump TheoryCardiac Pump Theory::Heart squeezed betweenHeart squeezed betweensternum and spine.sternum and spine.
Thoracic Pump TheoryThoracic Pump Theory::Chest acts as bellows.Chest acts as bellows.Compression causesCompression causespositive intrathoracic pressure:positive intrathoracic pressure:
Blood leaves the heart from Blood leaves the heart from higher pressure state higher pressure state (inside the heart) to the (inside the heart) to the lower pressure state lower pressure state (systemic circulation)(systemic circulation)
7
Compression Phase
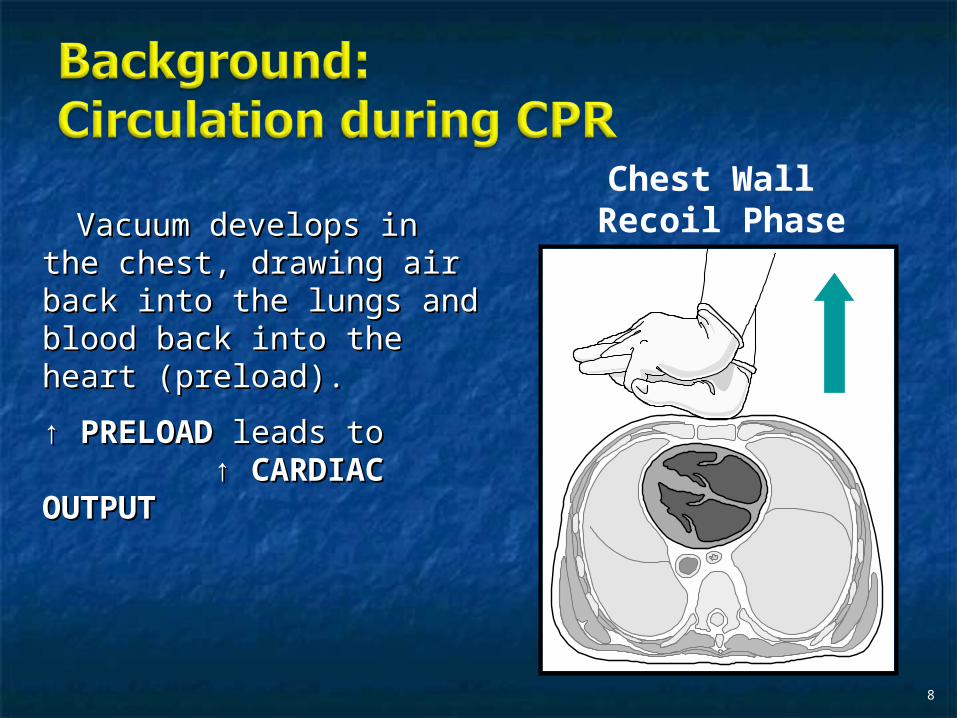
Vacuum develops in the Vacuum develops in the chest, drawing air back chest, drawing air back into the lungs and blood into the lungs and blood back into the heart back into the heart (preload).(preload).
↑ ↑ PRELOADPRELOAD leads to leads to ↑ ↑ CARDIAC OUTPUTCARDIAC OUTPUT
8
Chest Wall Recoil Phase
10
Inefficiency #1Inefficiency #1 Filling of the heart (preload) is Filling of the heart (preload) is
dependent upon the chest walldependent upon the chest wall’’s ability s ability to recoil during decompression phase.to recoil during decompression phase.
Chest wall recoil may be compromised Chest wall recoil may be compromised by:by: A stiff chestA stiff chest Broken ribsBroken ribs Just doing it wrongJust doing it wrong
11
Inefficiency #2Inefficiency #2 Air rushes in through an open airway Air rushes in through an open airway
and wipes out the vacuum weand wipes out the vacuum we’’re re relying on to fill the heart.relying on to fill the heart.
Heart stops filling as soon as vacuum Heart stops filling as soon as vacuum is equalized.is equalized.
13
ACD CPRACD CPR
15
Metronome Force Gauge
Handle
Suction Cup
16
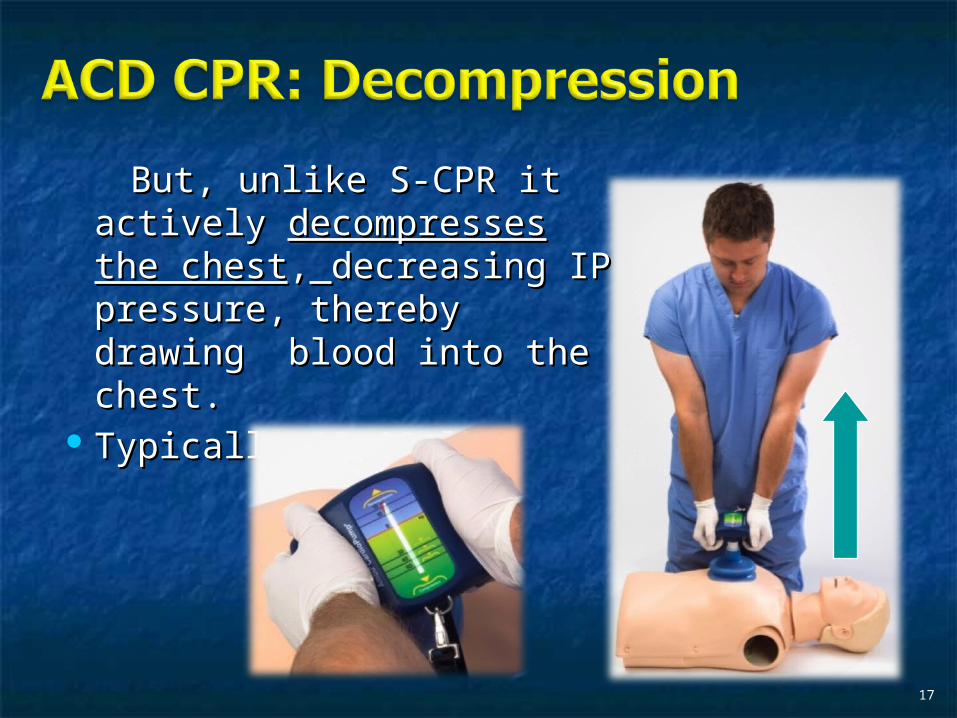
Actively Actively compressingcompressing the the chest, increasing IP pressure chest, increasing IP pressure and thereby forcing blood out and thereby forcing blood out of chestof chest, j, just like s-CPR.ust like s-CPR.
Same position as standard CPRSame position as standard CPR 40 – 50 cm (1 ½ - 240 – 50 cm (1 ½ - 2””))
But, unlike S-CPR it actively But, unlike S-CPR it actively decompresses the chestdecompresses the chest,, decreasing IP pressure, decreasing IP pressure, thereby drawing blood into thereby drawing blood into the chest.the chest.
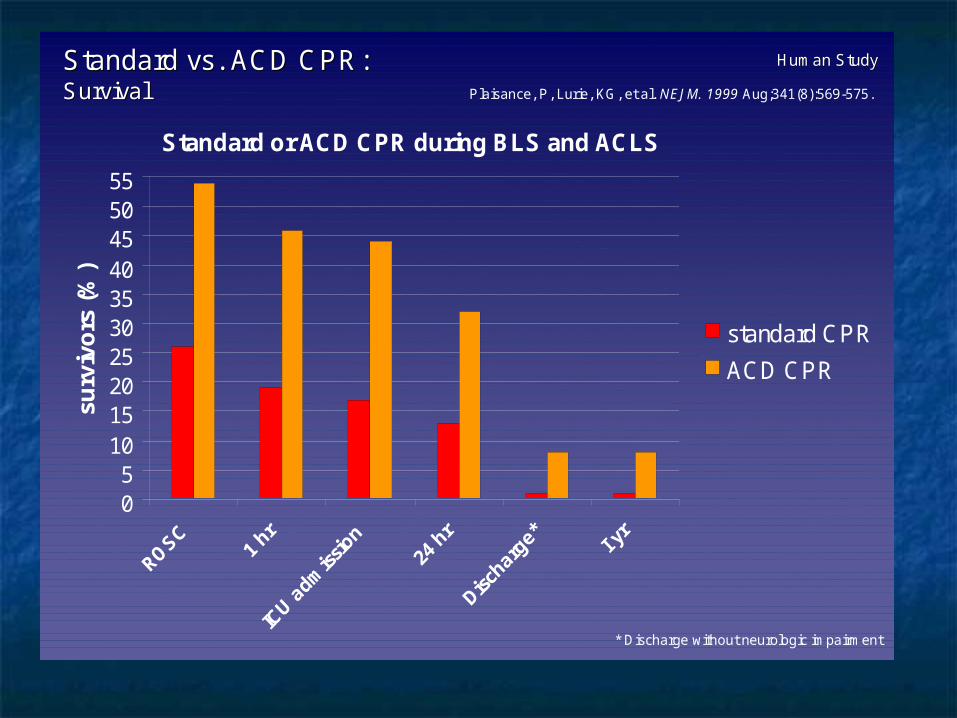
Standard vs. ACD CPR: Standard vs. ACD CPR: SurvivalSurvival Plaisance, P, Lurie, KG, et al. NEJM. 1999 Aug;341(8):569-575.
Human StudyHuman Study
Standard or ACD CPR during BLS and ACLS
05
10152025303540455055
surv
ivo
rs (%
)
standard CPR
ACD CPR
ACD CPRACD CPRThe Problem is:The Problem is:
Air rushes in through an open airway Air rushes in through an open airway and wipes out the vacuum weand wipes out the vacuum we’’re re relying on to fill the heart.relying on to fill the heart.
Heart stops filling as soon as vacuum Heart stops filling as soon as vacuum is equalized.is equalized.
The SolutionThe Solution
Enter the Impedence Threshold Enter the Impedence Threshold Device Device
(ITD)(ITD)
25
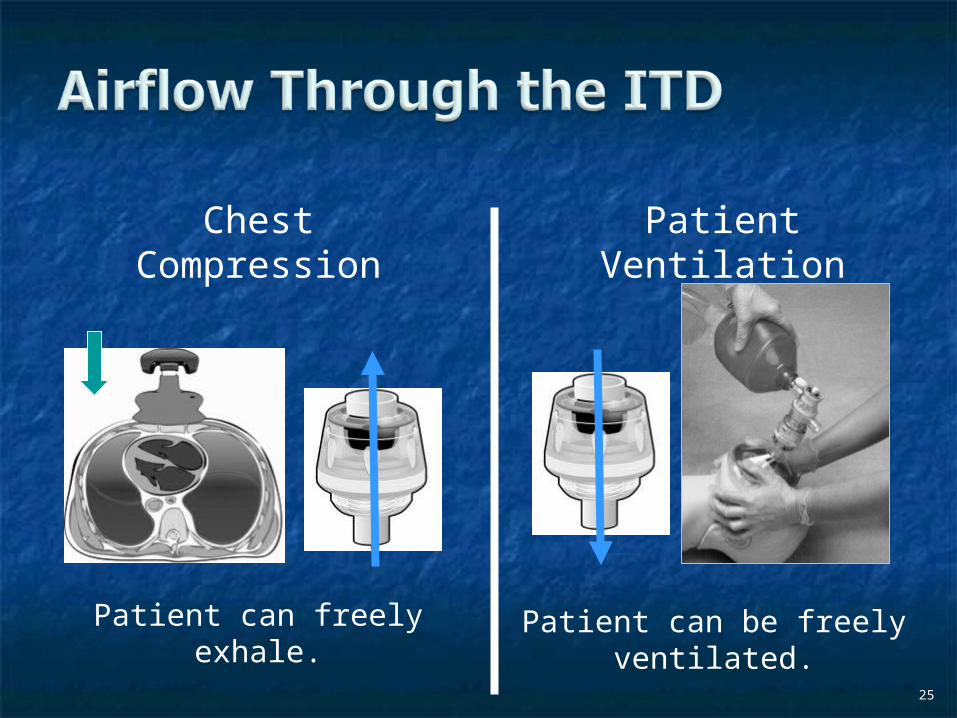
Patient can be freely ventilated.
Patient Ventilation
Patient can freely exhale.
Chest Compression
26
Air will enter if patient creates at least -10 cmH2O pressure with respiratory
effort.
Spontaneous Breathing
Influx of air is prevented, enhancing the vacuum in the
chest.
Chest Decompression
Greater vacuum (negative pressure) in Greater vacuum (negative pressure) in the chest during chest wall recoil phasethe chest during chest wall recoil phase
27
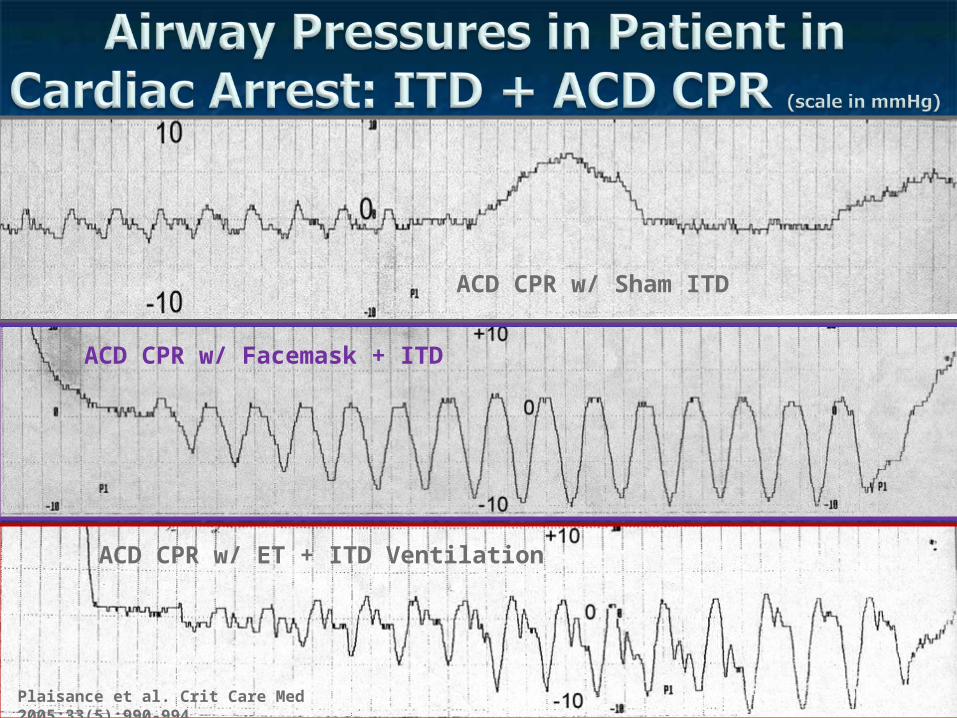
ACD CPR w/ Sham ITD
ACD CPR w/ Facemask + ITD
28Plaisance et al. Crit Care Med 2005;33(5):990-994
ACD CPR w/ ET + ITD Ventilation
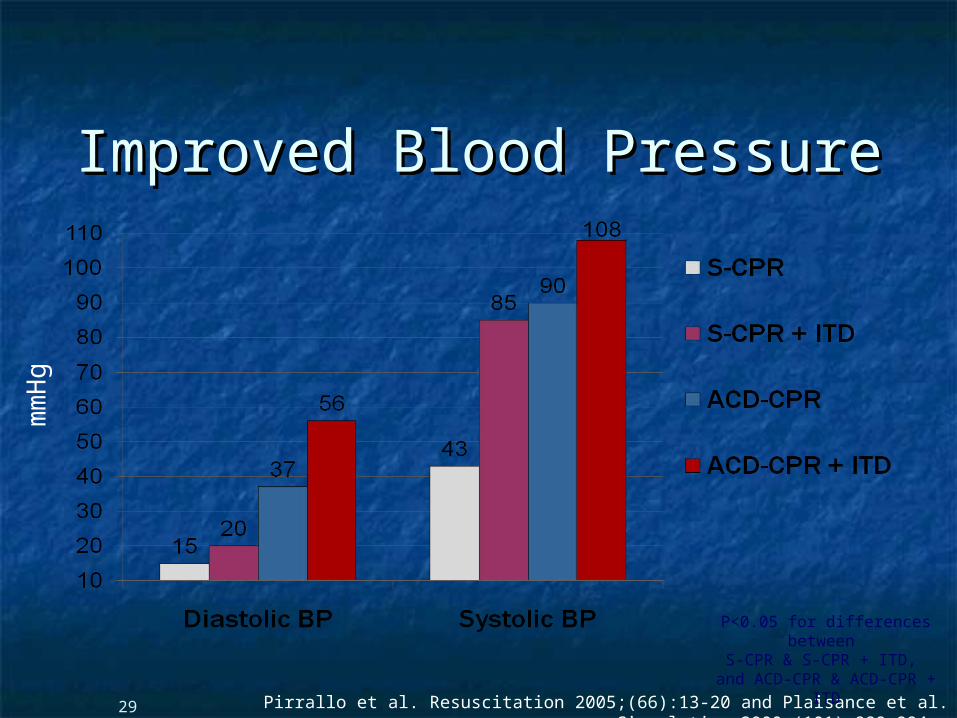
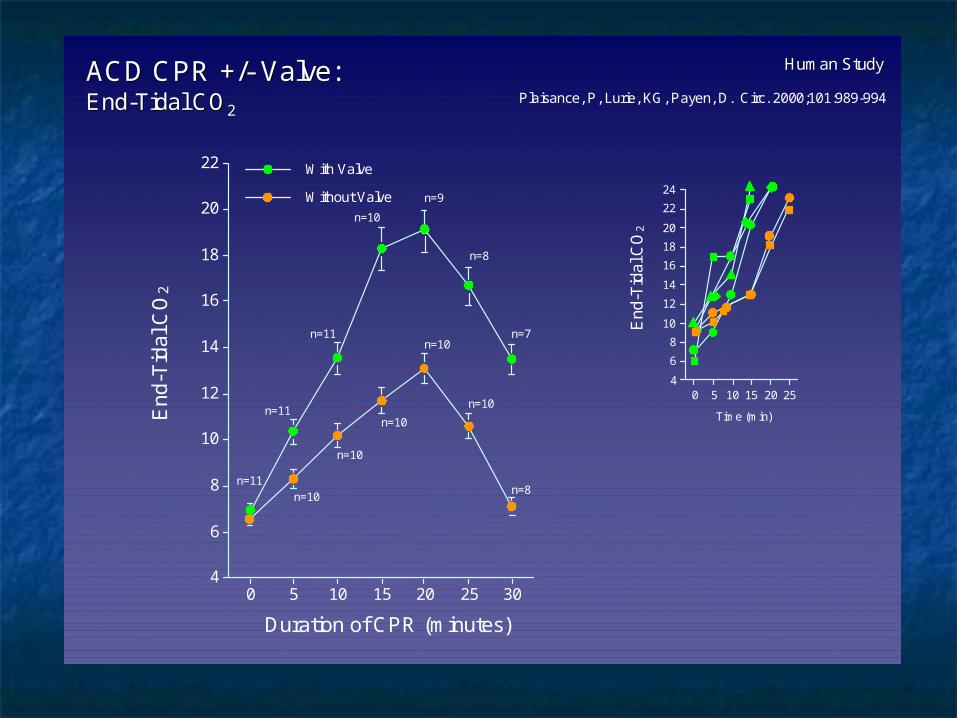
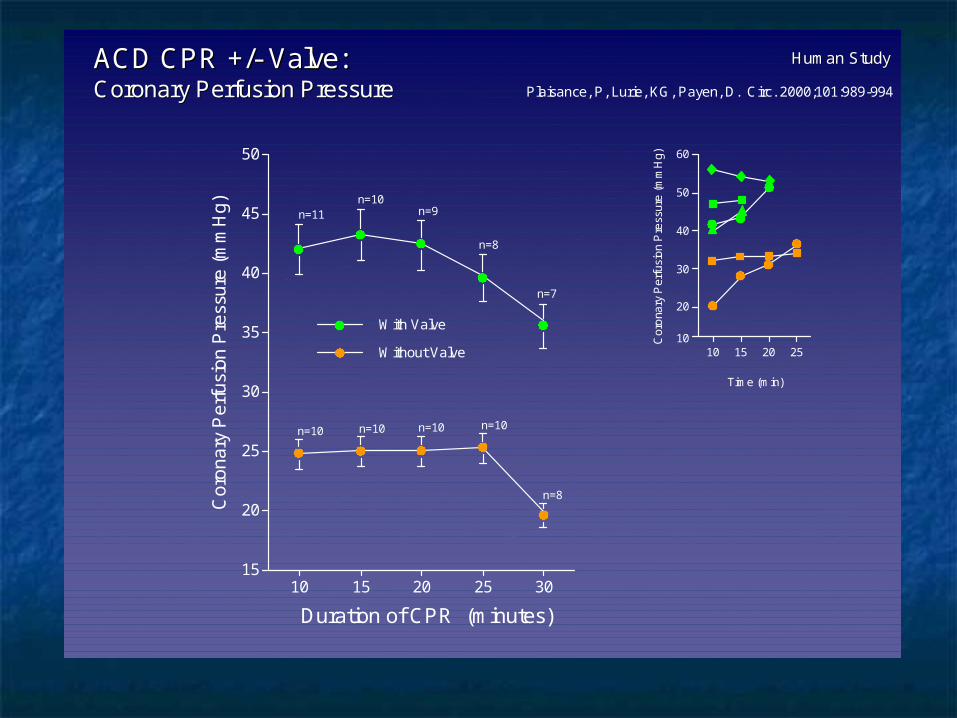
Improved Blood PressureImproved Blood Pressure
29
mm
Hg
Pirrallo et al. Resuscitation 2005;(66):13-20 and Plaisance et al. Circulation 2000;(101):989-994.
P<0.05 for differences between
S-CPR & S-CPR + ITD, and ACD-CPR & ACD-CPR +
ITD
Many other trials both in animals and human that prove
the effectiveness of the ITD alone or in combination with
Tom P. Aufderheide, MD; Ralph J. Frascone, MD; Marvin A. Wayne, MD; Brian D. Mahoney, MD; Robert A. Swor, DO; Robert M. Domeier, MD; Michael L. Olinger, MD; Richard G. Holcomb,
PhD; David E. Tupper, PhD; Demetris Yannopoulos, MD; Keith G. Lurie, MD
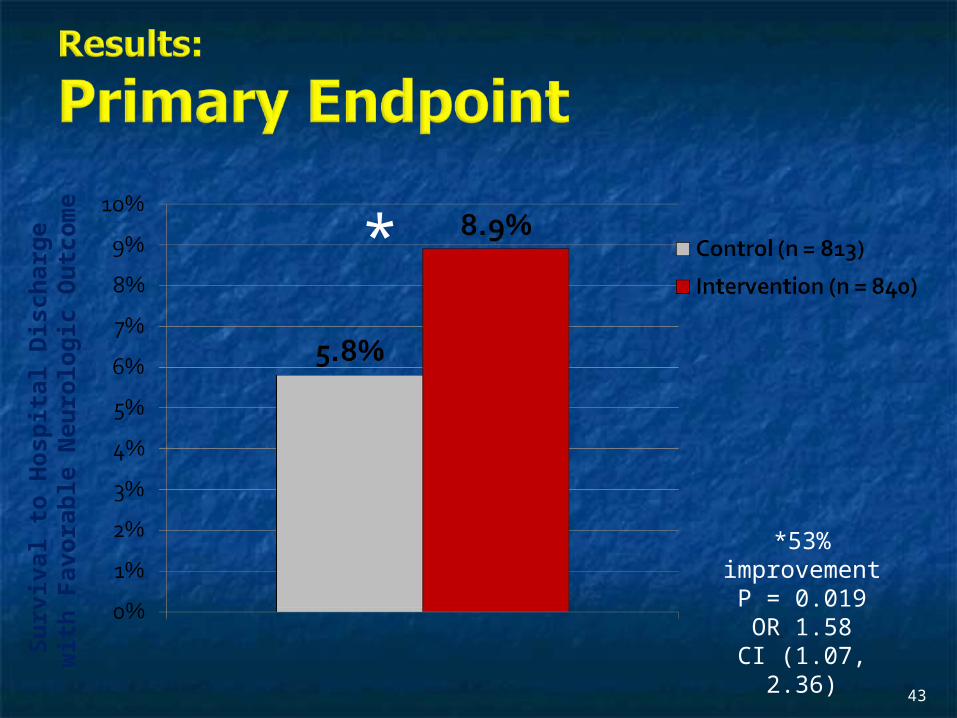
Compared to standard CPR, ITD + ACD-CPR Compared to standard CPR, ITD + ACD-CPR resulted in significantly increased survival to resulted in significantly increased survival to hospital discharge with favorable neurological hospital discharge with favorable neurological function (53%). function (53%).
One year after OOHCA, survival rates with similar One year after OOHCA, survival rates with similar neurologic function were also significantly higher neurologic function were also significantly higher in the intervention group (49%). in the intervention group (49%).
48
Aufderheide et al. A trial of an impedance threshold device Aufderheide et al. A trial of an impedance threshold device in out-of-hospital cardiac arrest. NEJM 2011365;798-806.in out-of-hospital cardiac arrest. NEJM 2011365;798-806.
49
PurposePurpose
To determine if use of an active To determine if use of an active (versus sham) ITD during standard (versus sham) ITD during standard CPR (no ACD used) would improve CPR (no ACD used) would improve rates of hospital discharge with rates of hospital discharge with functional neurological survival in functional neurological survival in adult (modified Rankin Scaleadult (modified Rankin Scale [mRS] [mRS] score ≤3score ≤3)), non-traumatic, out of , non-traumatic, out of hospital cardiac arrestshospital cardiac arrests
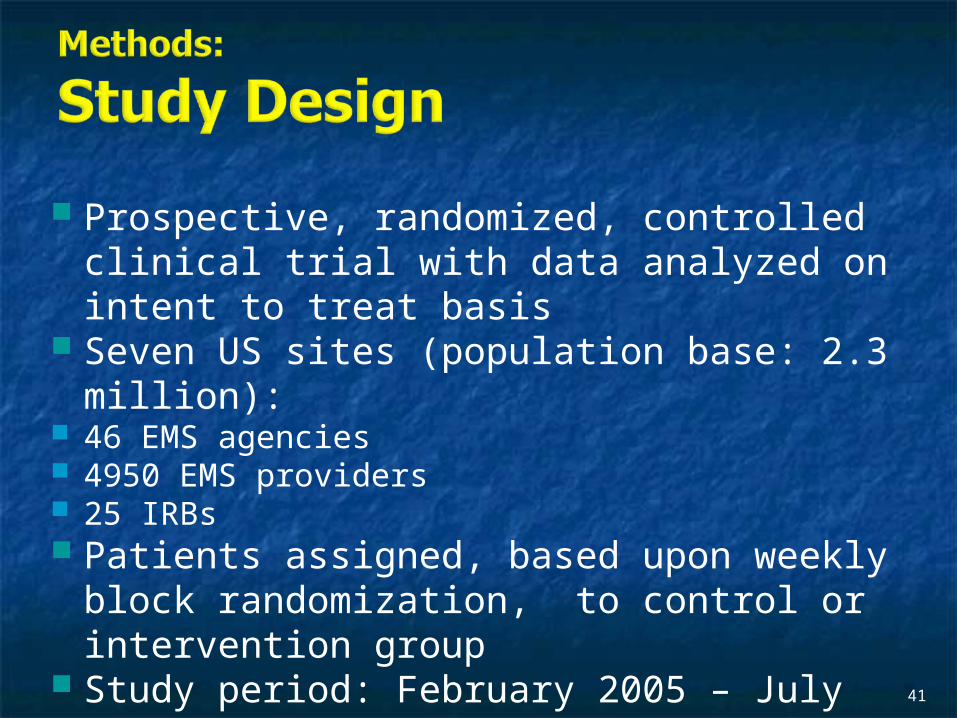
Description/Methods 10 sites in US and Canada Prospective, randomized, blinded Subjects: adults with arrest from presumed cardiac etiology 2 x 2 multivariate study design
Analyze Early (30 secs CPR) vs Analyze Later (3 min CPR) Stiell et al. NEJM 2011
Sham vs Active ITD Aufderheide et al. NEJM 2011
Impact of immediate CPR feedback utilizing QCPR device @ three sites
Hostler et al. BJM 2011
Results
ResultsResults Overall results in sham vs active ITD were similar Overall results in sham vs active ITD were similar
(≈6%)(≈6%) November 2, 2009, NIH announced study November 2, 2009, NIH announced study
terminated early (at the 2/3 enrollment point) as it terminated early (at the 2/3 enrollment point) as it was not going to be possible to detect any overall was not going to be possible to detect any overall significant difference between either of the study significant difference between either of the study groups (AnE vs AnL, or sham vs active ITD) even if groups (AnE vs AnL, or sham vs active ITD) even if study continued to 14,000 patients (stopped study continued to 14,000 patients (stopped because of futility)because of futility)
No safety concerns with ITDNo safety concerns with ITD
ConclusionConclusion Compared with standard CPR, Compared with standard CPR,
use of the ITD did not use of the ITD did not significantly improve functional significantly improve functional survival from out-of-hospital survival from out-of-hospital cardiac arrest. cardiac arrest.
When implemented under similar When implemented under similar conditions, routine use of the ITD conditions, routine use of the ITD is not supported. is not supported.
What are the Problems with ROC?
The Devil is in the Details
ProtocolsProtocols Three different BLS protocols Three different BLS protocols ALS protocols per site medical ALS protocols per site medical
directordirector
Various ROC Study ProtocolsVarious ROC Study Protocols
BLS CPR BLS CPR MethodMethod
ITD ITD StudyStudy11
AE vs AL AE vs AL StudyStudy22
QCPRQCPRStudyStudy33
Sites Sites ParticipatinParticipatin
gg
30:2 compression 30:2 compression to ventilation ratioto ventilation ratio
Continuous chest Continuous chest compressions with compressions with asynchronous asynchronous ventilations @ ventilations @ 10/min10/min
Did not Did not participateparticipate
Vancouver, Vancouver, CACA
Did not Did not participateparticipate
Feedback Feedback ON ON
vs Feedback vs Feedback OFFOFF
Seattle (King Seattle (King County), WACounty), WA57
1Aufderheide et al. NEJM 2011 2Stiell et al. NEJM 2011 3Hostler et al. BMJ 2011
Study ProtocolRespond to scene and determine pulselessness.Perform 1 – 4 simultaneously:1.Review enrollment criteria for AE vs AL study
a) If eligible and in V-Fib, perform either 30 secs or 3 min of CPR prior to analyzing and shocking if indicated.
b) If eligible and in asystole or PEA, or not eligible, perform conventional resuscitation
2.Review enrollment criteria for QCPR studya) If eligible, place QCPR device; then, based upon cluster
randomization, audible and visual feedback either will or will not be given to rescuers.
b) If not eligible, do not place QCPR device and perform conventional resuscitation.
3.Review enrollment criteria for ITD studya) If eligible, select ITD in serialized order and place on patient.b) If not eligible, perform conventional resuscitation.
4.Perform other conventional activities of resuscitation (e.g. airway management, IV/IO, administer medications, defibrillate)
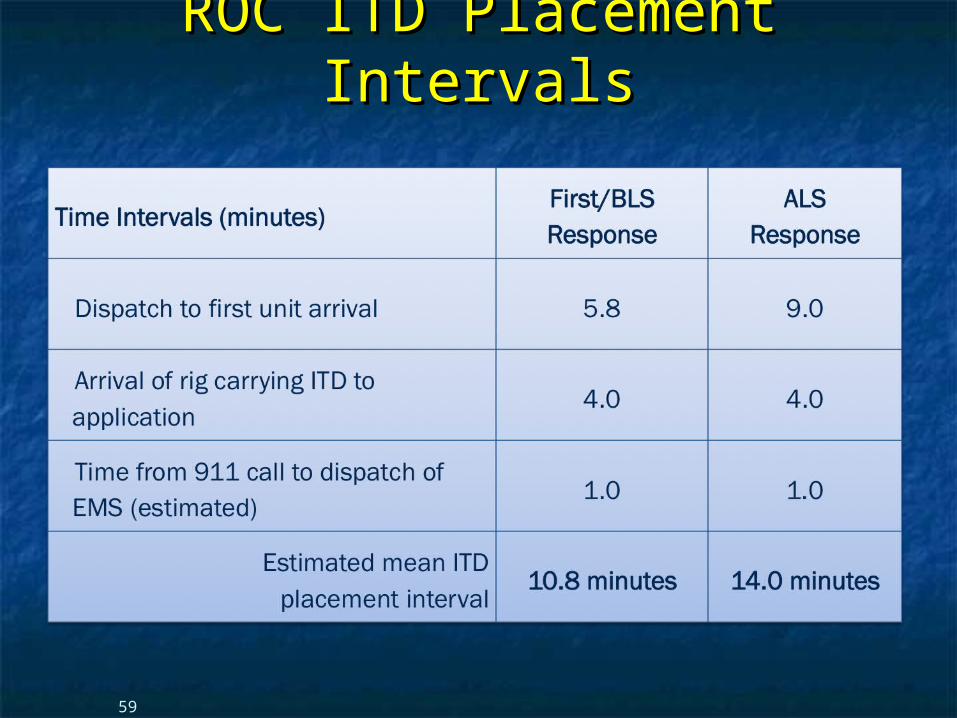
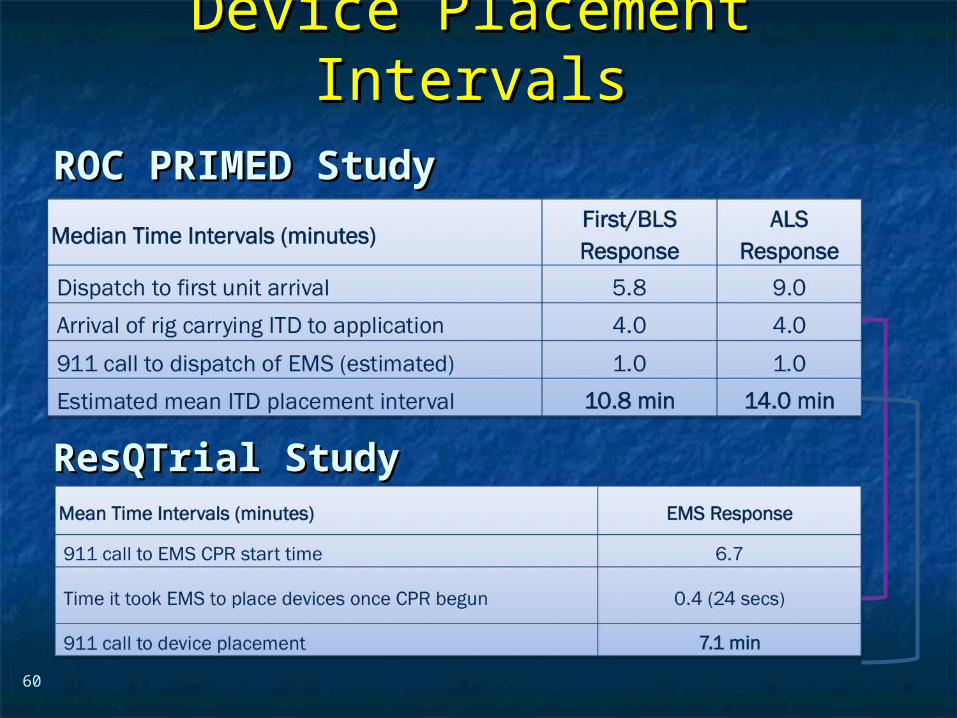
Device Placement IntervalsDevice Placement IntervalsROC PRIMED StudyROC PRIMED Study
ResQTrial StudyResQTrial Study
60
ProblemsProblems Complicated Analyze Early vs Analyze Later & QCPR Complicated Analyze Early vs Analyze Later & QCPR
protocols, multivariate design caused multiple protocols, multivariate design caused multiple problems:problems: ITD placement was very delayed (up to 14 minutes)ITD placement was very delayed (up to 14 minutes) Almost 40% of cases did not have ITD placed within Almost 40% of cases did not have ITD placed within
the planned time interval (under 5 minutes)the planned time interval (under 5 minutes) All the patients who survived in under approximately All the patients who survived in under approximately
4 minutes were not eligible for the ITD4 minutes were not eligible for the ITD Essentially all cases of early use were on asystolic Essentially all cases of early use were on asystolic
patientspatients Treatment protocols were inconsistentTreatment protocols were inconsistent
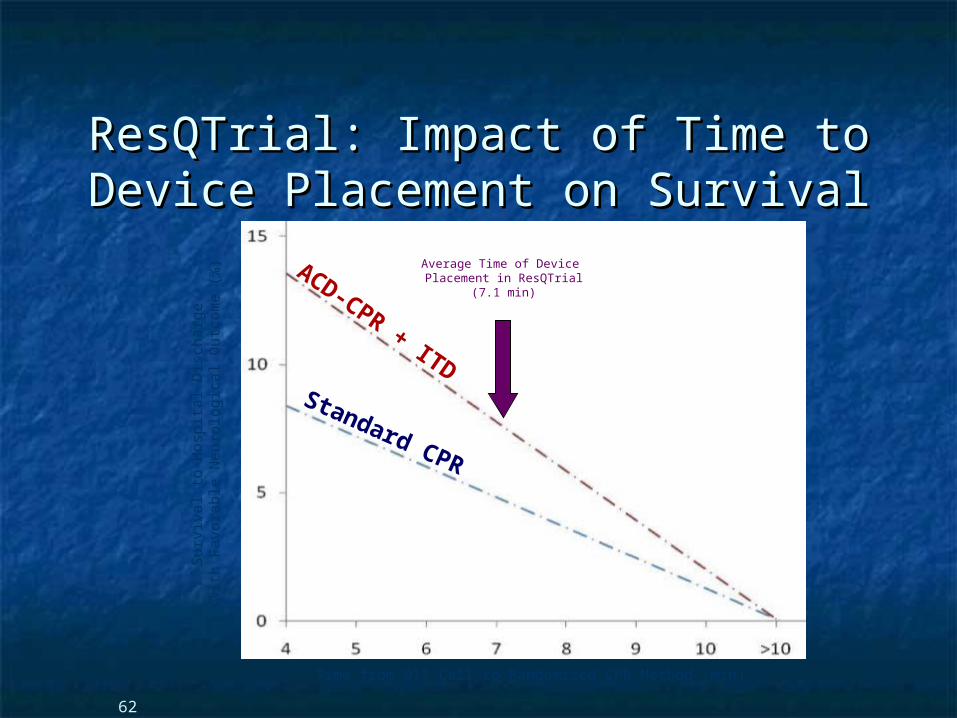
ResQTrial: Impact of Time to Device ResQTrial: Impact of Time to Device Placement on SurvivalPlacement on Survival
62
Surv
ival to
Hosp
ital D
isch
arg
e
wit
h F
avora
ble
Neu
rolo
gic
al O
utc
om
e (
%)
Time from 911 Call to Randomized CPR Method (min)
Average Time of Device Placement in ResQTrial
(7.1 min)
ACD-CPR + ITDStandard CPR
ROC PRIMEDROC PRIMED
All the patients who survived All the patients who survived in under approximately 4 in under approximately 4
minutes were not eligible for minutes were not eligible for the ITD.the ITD.
The Bottom LineThe Bottom LineTwo Very Different StudiesTwo Very Different Studies