Sot. Sri. Med. Vol. 27,No. 7,pp.723-731, 1988 Printed tn Great Britain, All rights reserved 0277-9536/88 $3.00 + 0.00 Copyright 62 1988Pergamon Press plc THE ECONOMY, THE HEALTH SECTOR AND CHILD HEALTH IN ZIMBABWE SINCE INDEPENDENCE DAVID SANDERS’ and ROB DAVIB$ ‘Department of Community Medicine and 2Department of Economics, University of Zimbabwe, Harare, Zimbabwe Abstract-This paper examines the changes in the economic environment which have taken place in Zimbabwe since independence in April 1980, concentrating on those which are relevant to health. It also describes the post-independence restructuring of the health sector itself. Finally, it considers some changes which have taken place in the health status of children. Despite a prolonged drought, economic recession and the imposition of economic stabilisation measures, there is evidence of a sharp improvement in infant and young child mortality. This has resulted almost certainly from an energetic expansion and reorientation of health care provision, and particularly from greatly improved access to immunisation and oral rehydration therapy. The adverse effects of drought and stabilisation measures have been partially offset by aid-supported relief feeding and particular health programmes. However, the economic crisis has resulted in a decline in real incomes for a large number of households since the immediate post- independence boom. This is reflected in high levels of childhood undernutrition which seem to have remained static despite the health care drive. This emerging divergence between death rates and quality of life as reflected by nutrition levels is reflective on the one hand of rapid expansion in effective health care provision, and on the other of little change in socioeconomic conditions for the majority of the population. Key rvords-child health. socio-economic status, Zimbabwe, economic policy INTRODUCTION This paper examines the changes in the economic environment which have taken place in Zimbabwe since independence in April 1980, concentrating es- pecially on those which are relevant to health. It also describes the post-independence restructuring of the health sector itself. Finally, it considers some changes which have taken place in the health status of chil- dren. The lack of data, particularly relating to changes in health and nutritional status, does not allow any firm conclusions about causality to be drawn. Nevertheless. it is possible to speculate on how these factors have influenced health and nutri- tion. The health of children is determined by many factors. These include factors inside the health sector such as provision of hospitals, immunisation pro- grammes and medical personnel. and those outside the health sector. such as levels of real income, educational standards and food subsidy programmes, In colonial Zimbabwe. as in other underdeveloped countries. the greatest burden of death and disease fell on infants (under 1 yr), young children, and women in the child-bearing period. Furthermore, mortality varied substantially by geographical area, race, and class. In 1980 there was a 1:3.5: 10 ratio between whites, urban blacks and rural blacks, corre- sponding to a 39: 5: 1 ratio in incomes [I]. While the better off showed the disease pattern seen in the industrialised countries. the majority of the population suffered nutritional deficiencies, commu- nicable diseases and problems associated with preg- nancy. Low birth weight in IO-20% of all births due to maternal undernutrition, and protein-energy mal- nutrition, were the commonest forms of childhood malnutrition, predisposing the victims to more severe and often fatal infections. The most important of these were measles, pneumonia and tuberculosis-all airborne infections transmitted by respiratory secretions-and diarrhoeal diseases. The latter and also parasitic diseases, such as schistosomiasis, intes- tinal worms and certain skin and eye infections, were widespread water-related diseases. This disease pattern was rooted in the system of production which prevailed in Rhodesia, its distribu- tion being reinforced by the structures of racial domination. Undernutrition, which from historical accounts appears to have increased after co- lonisation, was particularly prevalent in the Tribal Trust Lands (TTLs) and amongst children of workers on commercial farms. Although the TTLs were termed the ‘subsistence sector’, these peasants in- creasingly lost land and received little or no financial assistance and thus were unable to subsist from agriculture alone. By 1977 only 60% of the needed amount of the staple maize was produced in the TTLs, reflecting the overcrowding, overstocking and progressive degradation of these ecologically un- favourable areas. Endemic malaria further under- mined the health of the population in these areas. Increasingly, families were forced to supplement the unreliable agricultural production with cash remitted from the urban industrial or plantation sectors, while the TTLs provided a growing supply of landless wage labour and a dumping ground for aged, diseased and debilitated workers. Airborne infections spread easily in the cramped, housing conditions existing in both urban and rural areas. Poor sanitation and inade- quate water supplies predisposed people to common 123
Transcript
Sot. Sri. Med. Vol. 27, No. 7, pp. 723-731, 1988 Printed tn Great Britain, All rights reserved
THE ECONOMY, THE HEALTH SECTOR AND CHILD HEALTH IN ZIMBABWE SINCE INDEPENDENCE
DAVID SANDERS’ and ROB DAVIB$ ‘Department of Community Medicine and 2Department of Economics, University of Zimbabwe, Harare,
Zimbabwe
Abstract-This paper examines the changes in the economic environment which have taken place in Zimbabwe since independence in April 1980, concentrating on those which are relevant to health. It also describes the post-independence restructuring of the health sector itself. Finally, it considers some changes which have taken place in the health status of children. Despite a prolonged drought, economic recession and the imposition of economic stabilisation measures, there is evidence of a sharp improvement in infant and young child mortality. This has resulted almost certainly from an energetic expansion and reorientation of health care provision, and particularly from greatly improved access to immunisation and oral rehydration therapy. The adverse effects of drought and stabilisation measures have been partially offset by aid-supported relief feeding and particular health programmes. However, the economic crisis has resulted in a decline in real incomes for a large number of households since the immediate post- independence boom. This is reflected in high levels of childhood undernutrition which seem to have remained static despite the health care drive. This emerging divergence between death rates and quality of life as reflected by nutrition levels is reflective on the one hand of rapid expansion in effective health care provision, and on the other of little change in socioeconomic conditions for the majority of the population.
This paper examines the changes in the economic environment which have taken place in Zimbabwe since independence in April 1980, concentrating es- pecially on those which are relevant to health. It also describes the post-independence restructuring of the health sector itself. Finally, it considers some changes which have taken place in the health status of chil- dren. The lack of data, particularly relating to changes in health and nutritional status, does not allow any firm conclusions about causality to be drawn. Nevertheless. it is possible to speculate on how these factors have influenced health and nutri- tion.
The health of children is determined by many factors. These include factors inside the health sector such as provision of hospitals, immunisation pro- grammes and medical personnel. and those outside the health sector. such as levels of real income, educational standards and food subsidy programmes,
In colonial Zimbabwe. as in other underdeveloped countries. the greatest burden of death and disease fell on infants (under 1 yr), young children, and women in the child-bearing period. Furthermore, mortality varied substantially by geographical area, race, and class. In 1980 there was a 1:3.5: 10 ratio between whites, urban blacks and rural blacks, corre- sponding to a 39: 5: 1 ratio in incomes [I].
While the better off showed the disease pattern seen in the industrialised countries. the majority of the population suffered nutritional deficiencies, commu- nicable diseases and problems associated with preg- nancy. Low birth weight in IO-20% of all births due to maternal undernutrition, and protein-energy mal-
nutrition, were the commonest forms of childhood malnutrition, predisposing the victims to more severe and often fatal infections. The most important of these were measles, pneumonia and tuberculosis-all airborne infections transmitted by respiratory secretions-and diarrhoeal diseases. The latter and also parasitic diseases, such as schistosomiasis, intes- tinal worms and certain skin and eye infections, were widespread water-related diseases.
This disease pattern was rooted in the system of production which prevailed in Rhodesia, its distribu- tion being reinforced by the structures of racial domination. Undernutrition, which from historical accounts appears to have increased after co- lonisation, was particularly prevalent in the Tribal Trust Lands (TTLs) and amongst children of workers on commercial farms. Although the TTLs were termed the ‘subsistence sector’, these peasants in- creasingly lost land and received little or no financial assistance and thus were unable to subsist from agriculture alone. By 1977 only 60% of the needed amount of the staple maize was produced in the TTLs, reflecting the overcrowding, overstocking and progressive degradation of these ecologically un- favourable areas. Endemic malaria further under- mined the health of the population in these areas. Increasingly, families were forced to supplement the unreliable agricultural production with cash remitted from the urban industrial or plantation sectors, while the TTLs provided a growing supply of landless wage labour and a dumping ground for aged, diseased and debilitated workers. Airborne infections spread easily in the cramped, housing conditions existing in both urban and rural areas. Poor sanitation and inade- quate water supplies predisposed people to common
123
124 DAVID SANDERS and ROB DAVIES
and debilitating intestinal, skin and eye infections. In the white farming areas, where nearly 20% of the black population lived, conditions were often worse
PI. These negative environmental factors completely
dominated any positive impact the health care system might have had. The health system itself had all the features typical of an inappropriate, inequitably dis- tributed developing country service, compounded by inequalities based on racial discrimination. For ex- ample, in 1980/8 1 the average annual expenditure per head for private sector medical aid society members was $144 compared with $31 for the urban popu- lation using public services and $4 for the rural population [1, p. 301. The latter concealed further disparities, for only districts surrounding urban areas were relatively well served. There were also disparities in the distribution of health care personnel and in access to facilities. In 1980/81, 44% of publicly funded services went to the urban-based sophisticated central hospitals serving about 15% of the population, while only 24% went to primary and secondary level rural health services for the majority of the population [l, p. 331.
Independence saw the ushering in of a new and vigorous thrust in health care based on the primary health care approach. Simultaneously, however, after a brief post-independence economic boom, there has been a decline in the economic well-being of much of the population caused by the combined effects of international recession, prolonged drought, South African destabilisation and domestic macroeconomic policies. The relatively short period in which these processes have been operating provides an illu- minating case study of both the potential of effective health sector interventions and their limitations in the context of a deteriorating economic environment.
MACROECONOMIC BACKGROUND
Zimbabwe’s real national income declined throughout the late 1970s [3]. However, the economy grew rapidly after independence, stimulated by the removal of sanctions, increased consumer demand due to wage increases and an extremely good agricul- tural season in 1980/81. Subsequently the drought, which started in the 1981/82 season and lasted until the end of 1984, coupled with the impact of inter- national recession on export demand and South African destabilisation. led to a domestic recession, Zimbabwe’s post-independence macroeconomic ex- perience can thus be divided into two major phases: the post independence boom of 1980181 and the recession which began in 1982 and which has con- tinued, despite some signs of recovery, since.
Although this general periodisation is correct, some other indicators give a slightly different picture. Inflation rates moved into double figures from 1981 onwards, with no noticeable periodisation in the post-independence period. Although wage employ- ment picked up marginally at independence, there appears to be a long-term structural problem of new job creation. Similarly, although the balance of trade and the current account moved into deficit in 1981 and 1982, slightly preceding the recession we have
identified above, their deterioration had in fact started from 1978.
The government’s economic policies paralleled these changes in the economy. In the boom, government spending on social services rose, minimum wages were increased and the government had a generally optimistic view of how fast it could go in redressing the inequalities inherited from the past. By late 1982 this mood had changed and the government, under the stimulus of an IMF stand-by credit, tried to follow a standard stabilisation package to manage the balance of payments deficit, the budget deficit and inflation. The main components of the package in- cluded devaluation of the Zimbabwe dollar. re- strictions on government credit expansion and a wage freeze.
These changes in government policy are reflected in trends in the central government budget. Expenditure in nominal terms between 1980 and 1984 grew at an average rate of 24% per year, but it had grown at an average annual rate of 17% in the 5 years prior to independence. There was thus an acceleration of an already existing trend, rather than the establishment of an entirely new trend. However, the reasons for the expansion were different; prior to independence it was the increasing cost of defending the Smith re- gime; after independence it was largely the expansion of social expenditures. There was a rapid expansion in real expenditures in 1981 and 1982. Initially reve- nues were also increased rapidly, as the government tried to finance its expanded social expenditure pro- gramme through taxation, so that the deficit was reduced, both in constant price terms and relative to GDP. However, the increase in tax revenues could not be sustained (in the main because of the re- cession) and the deficit grew in 1982. The government then attempted to curtail its expenditures, so that they actually fell in real terms in 1983. There was also a slight reduction in the deficit relative to GDP in 1983. Although the government continued to restrict the expenditure side of the budget in 1984. the continued impact of the domestic recession on tax revenues meant that the deficit increased, both abso- lutely and relatively, in 1984.
From the point of view of this study, the most significant components of the government’s sta- bilisation efforts were the removal of subsidies, the wage freeze and attempts to restrict the growth of government expenditure. The removal of food sub- sidies and the freeze on wage increases combined to affect real earnings seriously, and we believe, had serious direct consequences for nutrition.
Zimbabwe inherited from Rhodesia an extensive system of price controls and subsidies which it con- tinued to operate after independence. Because of the growing burden they placed on the budget, the government wanted to reduce them even before the IMF agreement. However, it was only under the agreement that this happened. Subsidies rose to $112m, or 7.7% of the government’s current ex- penditure, in 1981/82. They continued to rise in nominal terms until 1983/84 when they peaked at $lSOm; in real terms this represented a fall of 5.7%. Subsequently there were more determined efforts to cut them, so that by 1985/86 they had fallen in real terms by 24.6% or 5.3% of current expenditure.
The economic changes in Zimbabwe since independence 725
The government attempted to minimise the impact subsidy removal had on prices by delaying permission to increase retail prices. Nonetheless, substantial price increases were unavoidable. Since the subsidies had applied mainly to basic food items, it was here that the price increases were greatest. In 1982 and 1983, prices rose by some 100% for maize meal, 69-95% for beef, 50% for milk, 25-30% for bread and 25% for edible oils. Apart from these direct effects of the removal of food subsidies, the raising of controlled prices of electricity, railway tariffs and fertihsers also influenced the general price level, albeit not immediately.
The combined effect of these price increases can be gauged from the movement of the consumer price index during the period. Between August and Sep- tember 1983, which was when the most significant removal of subsidies took place, the CPI for low income urban families rose by 15.6% (equivalent to an annual inflation rate of 18.7%) while the index of food prices for this group rose by 27.0% in that month. Clearly, the attempts to reduce and remove subsidies contributed significantly to the rise in the cost of living.
This inflationary impact was reinforced by the 1982 devaluation and subsequent depreciation of the Zimbabwean dollar. Although it is difficult to quantify, the fact that Zimbabwean production is highly import-dependent means that a fall in the value of the dollar is fairly rapidly translated into higher domestic prices.
IMPACT ON REAL EARNINGS AND INCOMES
In the 1982 Census Zimbabwe’s total population was estimated to be 7.55 million. Of these there were 1.7 m (22.5%) in urban areas and 5.85 m in rural areas -1.57 m (20.8%) on commercial farms and 4.28 m (56.7%) on communal lands. We would not expect stabilisation policies to affect each of these groups equally, nor would the impact be uniform within groups. In our discussion, therefore, we look initially at the urban sector, concentrating on wage earners and the urban informal sector. We then look at the rural population which we separate into those living on communal lands and those on commercial farms.
Urban wage earners
Since independence, the government had adopted a policy of controlling wages, particularly for the low paid. There were minimum wages for particular sectors before independence. but the government introduced national minimum wages in July 1980. Because of skewed income distribution the minima are significant for most workers.
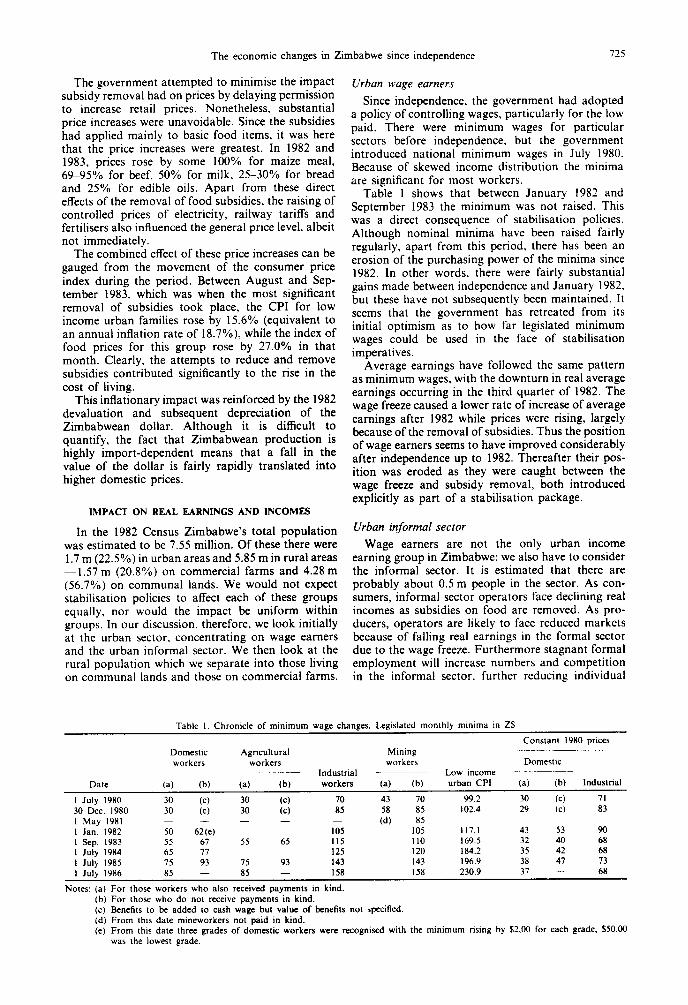
Table 1 shows that between January 1982 and September 1983 the minimum was not raised. This was a direct consequence of stabilisation policies. Although nominal minima have been raised fairly regularly, apart from this period. there has been an erosion of the purchasing power of the minima since 1982. In other words, there were fairly substantial gains made between independence and January 1982, but these have not subsequently been maintained. It seems that the government has retreated from its initial optimism as to how far legislated minimum wages could be used in the face of stabilisation imperatives.
Average earnings have followed the same pattern as minimum wages, with the downturn in real average earnings occurring in the third quarter of 1982. The wage freeze caused a lower rate of increase of average earnings after 1982 while prices were rising, largely because of the removal of subsidies. Thus the position of wage earners seems to have improved considerably after independence up to 1982. Thereafter their pos- ition was eroded as they were caught between the wage freeze and subsidy removal, both introduced explicitly as part of a stabilisation package.
Urban informal sector
Wage earners are not the only urban income earning group in Zimbabwe; we also have to consider the informal sector. It is estimated that there are probably about 0.5 m people in the sector. As con- sumers, informal sector operators face declining real incomes as subsidies on food are removed. As pro- ducers, operators are likely to face reduced markets because of falling real earnings in the formal sector due to the wage freeze. Furthermore stagnant formal employment will increase numbers and competition in the informal sector, further reducing individual
Table I. Chronicle of minimum wage changes. Legislated monthly mmlma m Z$
I July 1980 30 (c) 30 @) 70 43 70 99.2 30 (c) 71 30 Dec. 1980 30 (c) 30 (cl 85 :d”, 85 102.4 29 (C) 83 I May 1981 - 85 I Jan. 1982 50 62 (e) 105 I05 117.1 43 53 90 I Sep. 1983 55 67 55 65 II5 II0 169.5 32 40 68 I July 1984 65 77 I25 120 184.2 35 42 68 I July 1985 75 93 75 93 143 143 196.9 38 47 73 I July 1986 85 - 85 - I58 I58 230.9 37 - 68
Notes: (a) For those workers who also received payments in kind.
(b) For those who do not receive payments in kind.
(c) Benefits to be added to cash wage but value of benefits not specified.
(d) From this date mineworkers not paid in kind.
(e) From this date three grades of domestic workers were recognised with the minimum rising by $2.00 for each grade. $50.00
was the lowest grade.
726 DAVID SANDERS and ROB DAVIES
incomes. Thus, while conditions for those in the informal sector may have improved during the post- independence boom, it is likely that they deteriorated after 1982 in the face of recession and stabilisation policies.
Communal area households
Whether or not the removal of subsidies benefits a communal area household depends on whether it is a net producer or a net consumer of food. For net producers, rising food prices lead to a rise in real income; for net consumers they lead to a fall. Assess- ing the overall impact therefore requires some idea of the degree of stratification in the communal lands.
Settler colonial policies, especially with regard to land, laid the basis for a continuing process of stratification in the rural areas. Most obvious is the stratification between the commercial farming and the peasant or communal areas. Less obvious, but nevertheless of great significance with regard to health and nutrition patterns, is the stratification within the latter. Some indication of the extent of this is given by the results of the National Household Capability Survey 1983/84, which showed, inter alia, that about 6% of households have no access to land; that 50% of the land is controlled by about 20% of households; that approx. 50% of households have no cattle; and that about 10% of households own half the cattle. Similarly figures concerning communal area sales of all agricultural products to marketing boards show great differences between the various provinces. Thus in 1985/86 earnings per head from such sales ranged from $7.30 for Matabeleland North to $104.05 in Mashonaland West [4]. Such large differences between provinces will almost certainly also be reflected amongst households within prov- inces. The process of rural differentiation is likely also to have been accelerated by the drought.
There has been a remarkable rise since indepen- dence in the contribution of communal producers to marketed output, particularly of maize and cotton. By 1985 sales of crops by communal farmers ac- counted for 20% of all sales: prior to independence they had never reached a level of 10%. This rise can partly be attributed to the large expansion in. and thus greater accessibility of, marketing depots as well as to improved access to credit primarily through the Agricultural Finance Corporation’s (AFC) intro- duction of a Small Farm Credit Scheme after Inde- pendence. This resulted in the number of communal farmers receiving short term loans expanding from 24,957 in May 1982 to 95,176 by December 1985 (although the average-loan declined from $308 to $212). These 95,176 farmers receiving loans tend to be among the better off farmers and constitute only about 15% of all communal households. Thus these credit policies are themselves contributing to the process of rural differentiation. The AFC’s recent decision to refuse further loans to anyone in arrears from the previous year will tend to reinforce the above process. The expansion of marketed output from communal areas is consistent with increasing stratification, since progressive concentration of the means of production (mainly land and cattle) in the hands of fewer households will lead to a rise in the marketable surplus.
Therefore there appears to be a significant and growing number of households in rural areas who are net consumers of food and whose real incomes are likely to have been reduced bv the removal of sub- sidies. Moreover, the differential impact of the re- moval of subsidies will further contribute to the stratification process, widening the gap in the real incomes between net producing and net consuming households.
The stagnant economy after 1982 meant that the opportunities for households to compensate for this fall in real incomes by seeking off-farm income have been limited. A large and growing stratum of people thus depends increasingly on remittances from family members in formal wage employment. With no in- crease in the number of people in wage employment and with falling real earnings of those in jobs, there is a growing layer of increasingly impoverished households.
Commercial farmworker households
The removal of food subsidies affects families of commercial farmworkers primarily as consumers. Food prices for farmworkers are considerably higher than for urban consumers [5]. The effect of the removal of food subsidies has therefore affected this group at least as seriously as it has affected urban workers. This negative effect might theoretically have been offset by rising producer prices. However, evi- dence suggests that farm wages are determined by legislation and that, in the short run at least. rising farm profitability will not lead to rising wages. Thus (unlike communal farmers) commercial farmworkers were not directly affected by whether or not the removal of subsidies was accompanied by an increase in agricultural producer prices.
The wage freeze between January 1982 and Sep- tember 1983 also applied to agricultural workers. This restriction of nominal wages, coupled with the price increases, undoubtedly led to a fall in the real earnings of this group.
IMPACT ON THE SOCIAL WAGE
We have concentrated discussion on wages and prices as the most important direct components of household real incomes. However, there have been other changes in the economy and in social and welfare programmes which have also had an influence on standards of living and which thus may have affected health. These include the land resettlement programme, education, water development, devel- opment of co-operatives and the creation of rural growth points. The last two are still at an early stage of development, and will not be discussed here.
Resettlement
The issue of land distribution was central to the liberation struggle. Government introduced a re- settlement programme after independence to try to deal with some of the starker aspects of rural under- development and inequality. This required govern- ment funding both to buy land and to provide infrastructure and support for resettled households. Problems in securing funds meant that actual re-
The economic changes in Zimbabwe since independence 127
settlement took place more slowly than the govem- ment’s stated intentions. The original goal was to resettle 162,000 families by 1985, but the actual number resettled totalled only 31,386 by November 1984 [6]. Funding problems were compounded during the IMF stand-by agreement when the government was attempting to curtail overall expenditure; the severest cuts fell on resettlement programmes. Ex- penditure on land acquisition was cut from $28 million in 1982/83 to $6 million in 1983/84. This expenditure has not been restored in subsequent budgets.
These difficulties have meant not only that fewer families than intended have been resettled but also that resettlement has had mixed effects. On the one hand a number of effectively landless people have been resettled, albeit mostly onto marginal land. On the other hand, because of poor technical support and preparation compounded by the drought and the lack of adequate infrastructure (e.g. stores, transport and health care facilities), settlers are in some areas acknowledged to be the worst off in terms of health and nutrition status.
Education
Apart from its intrinsic contribution to welfare, education affects the health of children in at least two ways: expenditure on education (and accessories) reduces expenditure on nutrition and health, and education probably contributes in the longer term to better health behaviour.
From the point of view of the first of these, the government’s removal of fees for primary education accounted for a substantial rise in the real incomes of households with school-age children, even though parents still had to pay for uniforms, transport to school and, in effect, the lost input of their children. Subsequently, however, economic pressures forced the government to raise the cost to parents of school- ing. In some cases (mainly in the rural areas) parents have been required to provide labour, for example, in helping to build new classrooms, and this has de- tracted from time spent in household food pro- duction. In other cases, schools have been allowed to charge levies. This has put pressure on parents to reduce family expenditure on other items, including food. There is no systematic evidence of the extent to which this has occurred. It has been suggested that supplementary feeding programmes, which provide meals at some schools, have substituted for rather than complemented home meals. This is an indication of the fine balance which poor households have to make between alternative calls on their resources.
Insofar as general education makes a contribution to better health behaviour, Zimbabwe’s phenomenal post-independence expansion in school enrolments must be highly significant. Total numbers at school grew from 892,668 in 1979 to 2,727,162 in 1985, an average annual increase of over 20% [7]. The bulk of this expansion has been at the primary school level. There has also been some progress made in adult education. The impact that this will have on health is likely to show up only in the long run.
Water development and drought relief
Since independence there has been a programme
initiated by the government-under the impetus of the UN International Drinking Water Supply and Sanitation Decade-to improve water supplies and sanitation in the communal lands. Improved water supply and sanitation by themselves probably have little direct impact on health in the short-term, but they contribute indirectly by, for example, reducing time spent in collecting water, allowing more time to be devoted to productive activities which may con- tribute to improved health and nutrition. In 1984 about one-third of the communal area population had access to improved water sources; this propor- tion appears to have risen slowly in recent years and continues to do so.
The government introduced a drought relief pro- gramme in 1982 after the start of the drought. This programme peaked in 1983/84 when it consumed slightly over 2.3% of the government budget. In drought stricken areas it provided a basic food ration to many people and was crucial in mitigating wide- spread nutritional deterioration.
HEALTH SECI-OR IMPAm
There has been a major government thrust in the health sector since independence, with both a qual- itatively new approach and a number of specific programmes being introduced. The objective of these programmes has been stated in documents such as Planning for Equity in Health which advocates the adoption of the primary health care (PHC) approach. Curative and preventive components have been inte- grated in provincial and district health team struc- tures, accountable not only to higher levels of the health sector but also to local government structures at the level of service. The doctor in the district hospital is no longer only a curative professional, but is responsible together with the health team for the range of promotive, preventive, curative and rehabili- tative services as well as the training of new cadres and the coordination with other sectors.
In line with this new approach inter alia the following changes and programmes have been intro- duced since independence:
Free health care. Health care has been provided free of charge to those earning less than $150 per month-the majority of the population.
Hospital and rural health centre building pro- gramme. A vigorous programme of constructing and upgrading health care facilities has been undertaken. By January 1987, 274 rural health centres had been completed and a further 49 were under construction [8]. In addition a number of provincial and district hospitals as well as many rural clinics have been upgraded.
Expanded programme on immunisation (ZEPI). An expanded programme on immunisation against the six major childhood infectious diseases and tetanus im- munisation of pregnant women was initiated in 198 I. Studies on coverage show that the percentage of children between 12 and 23 months who are fully immunised has risen since 1982 in rural Zimbabwe from 25% to 42% in 1984 and in Harare City from 48% to 56% in 1983 [9] and to approx. 80% in 1986 [lo]. Recent data for Manicaland and Mashonaland
728 DAVID SANDERS and ROB DAVIES
Table 2. Central government budget allocation to the Ministry of Health. 1978179 to 1985/86
Vote allocation Actual expenditure Actual growth rates
Sources: 1978;79-83184. Annual Report o/ rhe Comp~oller and Audiror General. Harare. Zimbabwe. 1984/85-86187. Esrimares of Expendirure. Harare. Zimbabwe. 1980 pnce figures are calculated using an index of health sector wages.
East provinces, where coverage is probably better than the country average, show that 63% and 69% respectively of this age group are fully immunised
[111. Diarrhoeal disease control programme (DDCP). In
February 1982 the control of diarrhoeal disease was declared a priority by the government. The major com- ponents of this programme have included improved case management [mainly by oral rehydration therapy (ORT)], epidemic control, improved nutrition with emphasis on prolonged breast feeding, and improved environmental hygiene through water supply and sanitation (see above). Information gathered in October/November 1984 suggests that the number of attendances for diarrhoea at health care facilities has decreased [12]. There also appears to have been a significant increase in the percentage of rural mothers who can prepare a correct solution for ORT [9, 131.
National nutrition programme. A Department of National Nutrition was established, whose activities include nutrition and health education with particu- lar regard to breast feeding and weaning practices, growth monitoring and nutrition surveillance using child health cards, and supervision of the Children’s Supplementary Feeding Programme (CSFP) and food production plots. By June 1984 80% of children aged I possessed a growth card (as against 71% in 1982) and 83% had been weighed at least twice in the first year of life (58% in 1982) [9, p. 141, although only 35% of Harare mothers could consistently and correctly interpret the growth curves [14]. The CSFP was initiated in November 1980 by a number of NGOs and taken over by the MOH a year later. A daily energy-rich supplementary meal was supplied to predominantly undernourished young children in communal areas. The programme operated between 1981 and 1985, covering the height of the drought. At its peak, over a quarter of a million children in over 8000 communal area feeding points received food
1151. National village health worker programme. The
National Village Health Worker Programme (VHW) was launched in November 1981 to train workers selected by, and based in, their own villages. Of a projected eventual 15,000 VHWs about 7000 had been trained by April 1987 [ 161. Related to this programme was the Traditional Midwives Pro- gramme (TMP), designed to upgrade the skills of household-level women operatives in identifying at
Child spacing. The Zimbabwe National Family Planning Council, a parastatal organisation estab- lished in 1981, superseded the voluntary. government-assisted Family Planning Association. Partly as a result of its activities, Zimbabwe has the highest rate of contraceptive usage in Sub-Saharan Africa.
All these and other programmes required the ex- pansion of government expenditure. Table 2 shows how the vote allocations and the actual expenditure of the Ministry of Health (MOH) changed over the period. In current price terms there was an immediate expansion of 44.7%; in real terms 27.5%. The Minis- try’s share of the budget rose to 5.1%, showing that there was a relative shift in emphasis. This growth continued into the next budget year so that by fiscal year 1981/82, the MOH’s actual expenditure had almost doubled in real terms. However, following the downturn in the economy in 1982 and the intro- duction of stabilisation measures in 1983. the real growth of 47% in the 198 l/82 budget was turned into a real decrease in expenditure of 9.1% in the 1982/83 fiscal year.
The share of preventive services in the MOH budget has risen from 7.9% in 1979/80 to 14.0% in 1985/86, while that of medical care has fallen from 87.1% to 77.9% [17]. These figures actually under- state the shift towards preventive care since some of the costs of such care, especially with respect to immunisation, have effectively been reduced by the integration of curative and preventive services. This change reflects the impact of the changed philosophy of the MOH after independence.
There has also been a steady rise in the share of the Ministry’s budget allocated to salaries and allow- ances, from 26.8% in l980/81 to 44.7% in 1985/86 [17]. This reflects increasing personnel, rising wages, and the unwillingness of governments to dismiss salaried employees during a period of budget re- straint.
The MOH makes major grants to the central hospitals in Harare, to local authorities, missions and voluntary organisations. The central hospitals’ share of the MOH budget has been reduced since indepen- dence. The local authorities, missions and voluntary organisations provide health care services at the local
The economic changes in Zimbabwe since independence 729
level particularly in outreach programmes such as immunisation. diarrhoeal disease control and supple- mentary feeding. In real terms their grant increased from S22.2m in 1980/81 to $35.9m in 1981/82 and back to $24.4m in 1984/85. This recent fall in real resources has constrained their work, especially their ability to perform outreach work during 1984 and 1985 [18].
One of the more obvious effects of the Ministry’s attempts to restrict its expenditure was the under- mining of the free health care system. When this was introduced in September 1980 the maximum income for users was set at $150 per month. This ceiling has not subsequently been raised and is more rigorously enforced, presumably because of the cost impli- cations. At the same time, however, nominal wages have risen, so that people have been excluded from the service, et’en though their real incomes have not risen. Thus, in September 1982 when the minimum wage for industrial workers was $105 per month, about 42% of industrial workers earned less than the $150 ceiling. For July 1986 the minimum for indus- trial workers has been raised to $158, so that none qualify for free health care. Furthermore, those who do not qualify for the free service have been affected by rising charges for some services.
We thus see that government funding of health sector services grew substantially after independence but has remained static since 1981/82. Within this trend in overall levels, there has been a shift towards preventive services, reflecting the changing philos- ophy of the government.
The government is the most important but not the only provider of health services in Zimbabwe. There is a substantial private sector, generally funded through medical aid societies. Membership of these societies has grown since independence; however, members are almost wholly drawn from higher income groups and are thus not the focus of interest in this paper. It should be noted, however, that the government subsidises the private sector substantially both directly and indirectly [l. p. 681. Furthermore its continued operation and growth distorts the allocation of resources and functioning of personnel within the health sector to the detriment of poorer groups.
Resources are also provided to the health sector by foreign aid donors. who play an important part in easing some of the constraints faced by the govern- ment. Although the total amount of aid going to the sector has not been large in comparison with the overall MOH budget, it has been significant in re- lation to the funding allocated to specific projects. In the expanded programme on immunisation in 1983 18% of the budget came from bilateral and multi- lateral aid donors, Similarly, the funding for the CSFP has come primarily from aid agencies [9, p. 801.
CHANGES IN THE HEALTH AND NUTRITION STATUS OF CHILDREN
In reviewing the status of children’s health we emphasise that there is very little consistent and comprehensive data, particularly for mortality and morbidity. Further. time series data on these is virtually non-existent.
Pre-independence estimates of infant mortality rates vary, but it is agreed that for the African population as a whole the IMR was of the order of 120, with wide disparities between urban and remote rural areas and between whites and blacks [19]. Since independence the only IMR derived from a nation- wide survey is 83, a figure calculated from the 1982 Population Census [20]. There are no other data, but it is agreed by most workers in the field, on the basis of small studies and casual observation, that the IMR has declined significantly since 1980. Data on child (14 yr) mortality are even more scanty. The Census calculations, however, suggest that here too there has been a fall since before independence.
The Childhood Morbidity and Mortality Survey conducted in August 1983 shows that for children under the age of 5, diarrhoea and respiratory tract infections each cause 27% of deaths; combined they cause 48%. Measles and prematurity/neonatal tetanus/other neonatal causes each result in 15% of deaths [21]. Malnutrition is hardly ever cited as a cause of death but is acknowledged to be an im- portant associated cause especially in the cases of diarrhoea and measles.
Other data on child morbidity are either hospital based or very fragmentary. However, the morbidity pattern closely parallels the above pattern of mor- tality with the addition of certain communicable diseases such as whooping cough, tuberculosis, men- ingitis and poliomyelitis, malaria, schistosomiasis, various intestinal parasitoses. and skin and eye dis- eases.
It is difficult to do other than speculate about the precise impact of the health sector interventions described earlier on child mortality and morbidity, given the paucity of data. However, the aggregate de- clines in mortality noted above can be attributed with some certainty to these interventions. Even if disease specific data were available it would be impossible to disaggregate the summative impacts so as to appor- tion impact to individual programmes. In addition there will be time lags between intervention and impact, more so for some interventions than for others. For example, in the case of diarrhoeal disease mortality and morbidity, nutrition interventions will have a longer lag than ORT case management. Finally, even the actual or expected benefits of these interventions-individual and summative-might have been offset by the drought which lasted from 1982 to 1984.
Nevertheless, it is likely that certain programmes (particularly ZEPI and DDCP) have had and con- tinue to have a rapid positive impact on child survival and morbidity. Some reduction in deaths from diar- rhoea is likely to have resulted from increased usage of oral rehydration therapy, as well as a smaller proportion from protection against measles by immu- nisation. Similarly measles deaths have probably been reduced by improvement in immunisation cov- erage and neonatal tetanus deaths may have been reduced slightly by immunisation of pregnant women and more hygienic child birth practices resulting from the TMP. Some reduction in deaths from pneumonia and other respiratory infections as well as meningitis has probably resulted from greater accessibility to health care. Also some positive impact on perinatal
730 DAVID SANRERS and Roe DAVIES
and neonatal deaths may have accrued from the TMP. Malaria deaths may have experienced some reduction as a result of better access to health care especially through VHW-administered treatment.
However, any significant impact on deaths re- sulting from respiratory infections, prematurity and other neonatal causes, meningitis and deaths re- sulting directly or indirectly from malnutrition (not cited as a cause of death) would require im- provements in nutritional status of both children and mothers. Also reductions in levels of crowding and further improvement in access to health care would be needed. Indeed even a sustained reduction in deaths from diarrhoea and measles would also re- quire the above more general improvements, as well as improved environmental and personal hygiene in the case of diarrhoea.
It is impossible at this stage to predict the likely longer term impact of the above health sector pro- grammes on child health. Those programmes which incorporate preventive or promotive components (e.g. ZEPI, Child Spacing, VHW and TMP) will, if they continue to expand, have a summative and cumulative positive long term effect. The VHW pro- gramme, and even such programmes as the rural health centre building programme, will also lay the infrastructural basis for sustained health sector inter- ventions in the future.
The main effect of the recessionary period has been to restrict the MOH’s ability to finance services, although in the case of the free health service there has actually been a reduction. Insofar as the health sector interventions introduced have had a positive impact on child health, it might be expected that because of these restrictions the rate of improvement will not have been sustained during the recession period. However, any negative impact will have been somewhat offset by the relative shift towards pre- ventive care, the integration of preventive and cura- tive services and by aid inflows.
The restrictions on funding may also have long term effects. Reduced provision (e.g. slowing down the rural health centre building programme) or util- isation (e.g. by disqualifying people from free health care) of such facilities will, because of the integration of curative and preventive services, adversely affect the spread of ORT knowledge and immunisation. Finally, the slowing down of infrastructural devel- opment will have longer term effects on all aspects of health care programmes.
Thus, despite the paucity of data, particularly of a serial nature, it is arguable that the recession has slowed the rate of reduction of child mortality (and some areas of morbidity) because of constraints on health sector interventions. However, it is likely that its impact on health through the general economic environment and, in particular, real incomes, has been more significant. This impact will in part be mediated through the effect reduced incomes have had on health facility utilisation. However, the main impact will be through their effect on the nutritional status of children.
In 1982 the Ministry of Health carried out a survey of 1776 children. This showed the proportion of underweight children aged 0 to 3 to be 18-22% in
non-urban areas and 10-l 1% in urban. Wasting was found in 9% of non-urban and 13.5% of urban children. 36% of children below 4yr in non-urban areas were stunted and 16% in urban [21, p. 351. A MOH survey conducted in July 1984 showed 48% of rural children between 12 and 59 months of age to be under the Harvard tenth centile and 16.4% below 80% of the fiftieth centile of the NCHS standard [21]. These two MOH surveys provide the only nationwide time series data on children’s nutrition. The 1982 survey distinguished between urban and rural chil- dren, while the 1984 study surveyed clusters drawn from rural and urban areas, excluding Harare, Bul- awayo and Chitungwiza. Because of this lack of comparability the only conclusion that can be drawn from the above figures is that there has probably been no significant change in the prevalence of under- nutrition amongst rural children. This conclusion is not contradicted by available data from smaller surveys.
Loewenson has shown that there appears to have been a reduction in measured levels of both chronic and acute forms of undernutrition between 1981/2 and 1983 [5] in commercial farming areas, communal areas and mining areas. Since equivalent reductions in undernutrition were observed on commercial farms which had initiated health projects and those which had not, it seems likely that they were due to a general improvement in living conditions rather than to health sector interventions. Loewenson’s surveys covered the period of economic boom and thus coincided with rising real earnings. Unfortunately there are no equivalent data for the later period when real earnings fell for both wage workers and many communal house- holds.
Thus there is little evidence that changes in the nutritional status of young children in Zimbabwe have followed any discernible pattern since indepen- dence. This is somewhat surprising given the fall in real incomes resulting from the recession. In our opinion, the most plausible explanation of this incon- sistency is the impact of the Drought Relief Pro- gramme and the CSFP. Both of these programmes were externally assisted and resulted in wide distribu- tion of food supplements.
Some authors have commented on the paradox that while Zimbabwe has relatively low mortality rates as compared with other underdeveloped coun- tries, its levels of undernutrition are high+specially in view of its overall food surplus. This is explained in a World Bank Report by a combination of factors: Zimbabwe has a relatively safer infection/disease environment; water supply and sanitation are better than in many countries; and rural Zimbabwean culture places a high premium on cleanliness and tidiness [22]. Given our earlier observations about rural stratification, we would add that it is probable that undernourished children come predominantly from the lower strata and that disparities in mortality rates are likely to be quite wide, but that these rates. even in this group, have been reduced by relatively good and rapidly improving immunisation coverage, spread of knowledge about ORT and better access than in many African countries to curative health care.
The economic changes in Zimbabwe since independence 731
CONCLUSION REFERENCES
This paper has reviewed child health and the economy in Zimbabwe from the immediate pre- independence period through the periods of post- independence economic growth and recession. It has attempted to show in particular how the recession affected the general economic environment and how this in turn may have influenced childhood mortality, morbidity and nutrition. It has also examined the effect of recession and the stabilisation policies adop- ted on a reoriented and rapidly expanding health sector, and has assessed the likely impact on child health. Although data are inadequate and patchy, some general conclusions may be drawn.
I
2
3.
4.
Ministry of Health. Planning for Equity in Health. p. 6. Government of Zimbabwe. Harare. 1984.
The pre-independence health situation is reviewed in Gilmurray J., Riddell R. and Sanders D. The Struggle for Health. Catholic Institute for lnternational Re- lations. London. 1979. This section has been drawn from Davies R. and Sanders D. Adjustment policies and the welfare of children in Zimbabwe, 198&1985. In Adjustment wifh a Human Face (Edited by Comia A.. Jolly R. and Stewart F.). Vol. II. UNICEF, New York. 1988. Zimbabwe: Local Processing, Storage and Input Supply Project Preparation Reporr. World Bank. Washington. no date.
There is evidence that infant and young child mortality in Zimbabwe have shown a sharp im- provement despite drought, recession and sta- bilisation policies. Our impression is that these im- provements have resulted mainly from an energetic expansion and reorientation of health care provision. The adverse effects of drought, recession and sta- bihsation policies have been offset respectively by aid-supported relief feeding programmes and particu- lar health care programmes. On the other hand, economic recession and stabilisation attempts have reduced real incomes for large numbers of rural and urban households since the immediate post- independence boom. This reflects itself in discrep- antly high levels of childhood undernutrition which seem to have remained static or improved only very slightly despite the health care drive. This apparent inconsistency expresses a fundamental shortcoming in what is becoming known as the “selective health care approach”. where targetted technical inter- ventions can rapidly reduce mortality but more basic causes of undernutrition and ill-health are not ad- dressed. These basic causes are rooted in the economy and society and are unlikely to be amenable to short-term technical solutions. Indeed these selective health care interventions, often aid-supported, partic- ularly when delivered through ‘vertical’ programmes, may have the effect of delaying the development of the material and human infrastructure necessary to begin to address the fundamental causes of childhood ill-health. This is not to eschew the need for such important and effective components of primary health care such as immunisation and ORT: rather it is to insist that the PHC approach should also incorporate a longer term strategic goal of equipping communities to improve not only their survival chances but also their health, nutrition and quality of life through social and economic development.
10
I1
12
Loewenson R. Farm labour in Zimbabwe: a compara- tive study in health status. Hlth Policy Planng l(l), 48-57. 1986. Ministry of Finance. Socio-Economic Report. p. 127. Government of Zimbabwe, Harare, 1986. Central Statistical Office. Quarterly Digest of SIarisrics. Government of Zimbabwe. Harare, September 1986. Ministry of Health, personal communication. Ministry of Health. Reporr on a Joint Mission 10 EraI- uate Primary Health Care in Zimbabwe. Government of Zimbabwe. Harare. 1984. City Medical Officer of Health, personal commu- nication. Ramji S. Provincial Epidemiologist, personal commu- nication.
13
14
Cutts F. The use of oral rehydration therapy in health facilities in Zimbabwe. Save the Children Fund. London School of Hygiene and Tropical Medicine, 1984. De Zoysa I. er al. Home-based oral rehydration therapy in rural Zimbabwe. Trans. R. Sot. trap. Med. Hyg. 78, 102-105, 1984; Mtero S. er al. Assessment of knowl- edge, attitudes and practices in the management and prevention of diarrhoea in Zimbabwe. Ministry of Health, Harare, 1985: Ramji S. personal commu- nication; Sanders D. personal observation. Ministry of Health. A study to determine the knowledge of the child health card and maternal and childhood immunisation of mothers attending children’s clinics. Mimeo, Harare. 1985.
15
16 17
18.
19
Arkno,~,led~enlenrs-This paper is adapted from a paper written for UNICEF and appearing in Cornia A., Jolly R. and Stewart F. (Eds). Adjusrmenl ulirh CI Human Face Vol. II. UNICEF. New York, 1988. We would like to thank K. Boratav. A. Corn& R. Decoster, L. Loxton and C. Todd for comments and assistance. We remain responsible for the views expressed.
20
21.
22.
Working Group. The Children’s Supplemenrary Feeding Programme in Zimbabwe. Harare, 1982; Ministry of Health. The Evaluation of the Child Supplemenrary Feeding Programme. Harare 1984. Ministry of Health, personal communication. Government of Zimbabwe. Annual Reports of the Comprroller and Audiror General. Harare, various dates; Government of Zimbabwe. Estimares of Expendirure. Harare, various dates Zimbabwe Association of Church Related Hospitals, personal communication. Sanders D. Maior MCH nroblems in Zimbabwe. In Maternal and Child Healih Workshop. Ministry of Health, Juhasdale, 1983. Central Statistical Office. Starisrical Yearbook 1985. Government of Zimbabwe, Harare, 1986. Women and Children in Zimbabwe: a Siruarion Analysis. UNICEF, Harare, July 1985. Zimbabwe: Population, Health and Nutrition Sector Re- view. Vol. II, p. 10. World Bank, Washington, 1983.