Eastern Illinois University e Keep Masters eses Student eses & Publications 2003 e Effect of Choice Order on Off Task Behavior in a Child with Autism Lisa R. Cole Eastern Illinois University is research is a product of the graduate program in School Psychology at Eastern Illinois University. Find out more about the program. is is brought to you for free and open access by the Student eses & Publications at e Keep. It has been accepted for inclusion in Masters eses by an authorized administrator of e Keep. For more information, please contact [email protected]. Recommended Citation Cole, Lisa R., "e Effect of Choice Order on Off Task Behavior in a Child with Autism" (2003). Masters eses. 1375. hps://thekeep.eiu.edu/theses/1375
Transcript
Eastern Illinois UniversityThe Keep
Masters Theses Student Theses & Publications
2003
The Effect of Choice Order on Off Task Behaviorin a Child with AutismLisa R. ColeEastern Illinois UniversityThis research is a product of the graduate program in School Psychology at Eastern Illinois University. Findout more about the program.
This is brought to you for free and open access by the Student Theses & Publications at The Keep. It has been accepted for inclusion in Masters Thesesby an authorized administrator of The Keep. For more information, please contact [email protected].
Recommended CitationCole, Lisa R., "The Effect of Choice Order on Off Task Behavior in a Child with Autism" (2003). Masters Theses. 1375.https://thekeep.eiu.edu/theses/1375
THESIS/FIELD EXPERIENCE PAPER REPRODUCTION CERTIFICATE
TO: Graduate Degree Candidates (who have written formal theses)
SUBJECT: Permission to Reproduce Theses
The University Library is receiving a number of request from other institutions asking permission to reproduce dissertations for inclusion in their library holdings. Although no copyright laws are involved, we feel that professional courtesy demands that permission be obtained from the author before we allow these to be copied . . ~LEASE SIGN ONE OF THE FOLLOWING STATEMENTS:
Booth Library of Eastern Illinois University has my pennission to lend my thesis to a reputable college or university for the purpose of copying it for inclusion in that institution's library or research holdings.
Date
I respectfully request Booth Library of Eastern Illinois University NOT allow my thesis to be reproduced because:
Author's Signature Date
The Effect of Choice Order on Off Task Behavior in a Child with Autism
BY
Lisa R. Cole
THESIS
SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF
Master of Arts in Clinical Psychology
IN THE GRADUATE SCHOOL, EASTERN ILLINOIS UNIVERSITY CHARLESTON, ILLINOIS
2003 YEAR
I HEREBY RECOMMEND THIS THESIS BE ACCEPTED AS FULFILLING THIS PART OF THE GRADUATE DEGREE CITED ABOVE
August 4, 2003 Date
August 4, 2003 Date
Running head: CHOICE ORDER ON OFF TASK BEHAVIOR
The Effect of Choice Order on Off Task
Behavior in a Child with Autism
LisaR. Cole
Eastern Illinois University
Abstract
This research project was designed to examine the effects of child-choice versus
clinician-choice over the ordering of activities during speech-language therapy sessions.
The dependent variables included disruptive/inappropriate behavior, non-task related
verbal behavior, and redirection to the task. The independent variable was the
presentation of choice over the ordering of activities within a therapy session.
The subject in this case study was a nine-year-old boy diagnosed with autism. At the
beginning of each therapy session either the child or the clinician decided on the ordering
of activities. A picture board and picture cards showed the activities that would be
completed in each therapy session. Behaviors were then recorded to determine if the
amount of off-task behavior varied significantly across the two conditions.
Results of the study revealed a significant difference in the amount of
disruptive/inappropriate behavior across the two conditions when the child selected the
order of activities. No significant differences were found in the number of times the
clinician redirected the child or the number of non-task related verbal behaviors. A
significant relationship was found between redirecting the child and disruptive behavior
and non-task related verbal behavior when the clinician had control over the ordering of
therapy activities. There were no similar correlations when the child selected the order of
activities.
The study provides a foundation to further examine the effect of choice on the
ordering of activities on off-task behavior in children. The implications of this study
could be extended to various settings.
11
Acknowledgments
I would like to thank everyone whose thoughts and ideas contributed to my interest
in the field of psychology and autism. A special thanks to Dr. William Kirk and my
classmates for their support and guidance. I would have never made it without you.
I am very grateful to Ms. Marjorie Hanft-Martone and Dr. Joseph Williams, thesis
committee members, and Ms. Chris Chambers, Ms. Kristy Baker, and Ms. Dorothy
Taylor for their assistance. The insight, ideas, and support for my thesis from this group
of individuals was invaluable. ·Thank you is not strong enough to express my gratitude to
Dr. Linda Leal, thesis chair, for her never-ending support, guidance, and faith during this
project.
To Gabe, Casey, and Jodi; I would have never gotten through this year without your
support, encouragement, and understanding. Thanks for sticking by me through all the
good and bad times. Finally, to my parents, your love, patience, and encouragement
during the good and bad times this year have kept me going in the pursuit of my dream.
Your unfailing support has shown me that I can overcome multiple obstacles to strive to
be the best person possible. This thesis could not have been completed without the
encouragement and support of each and every one of you who have touched my life.
Dependent variable and definitions ......................................... 25
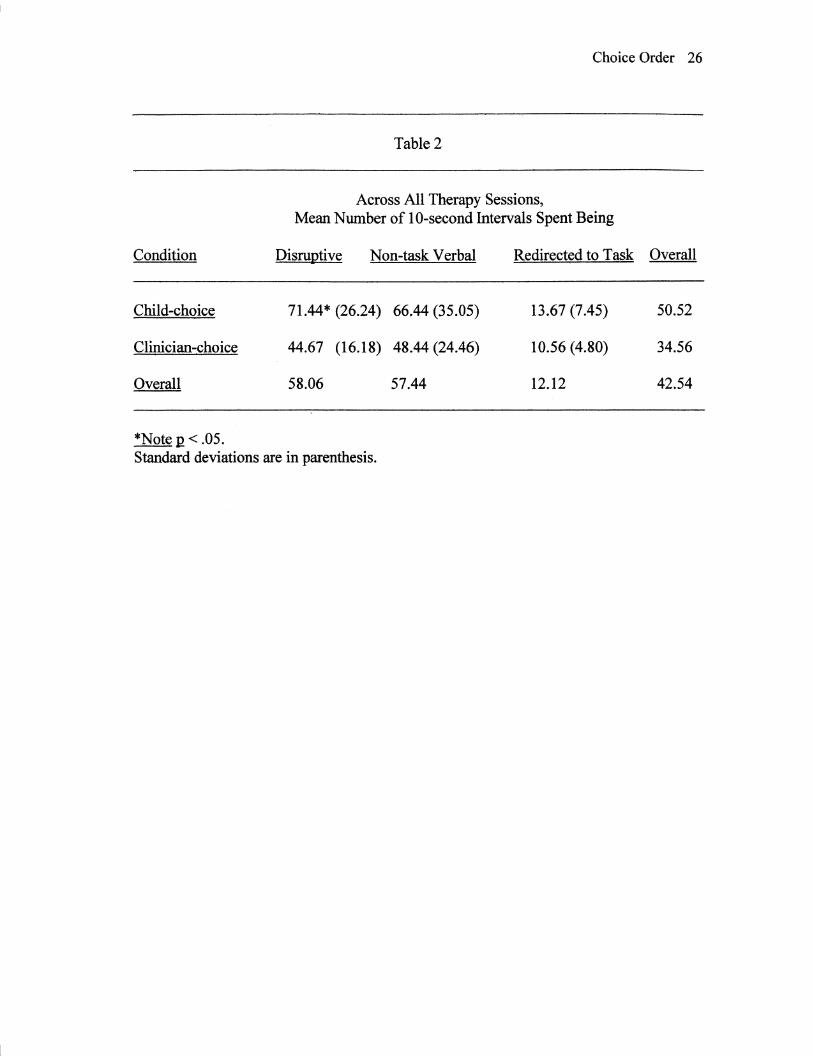
Mean number of 10-second intervals for each dependent variable .... .26
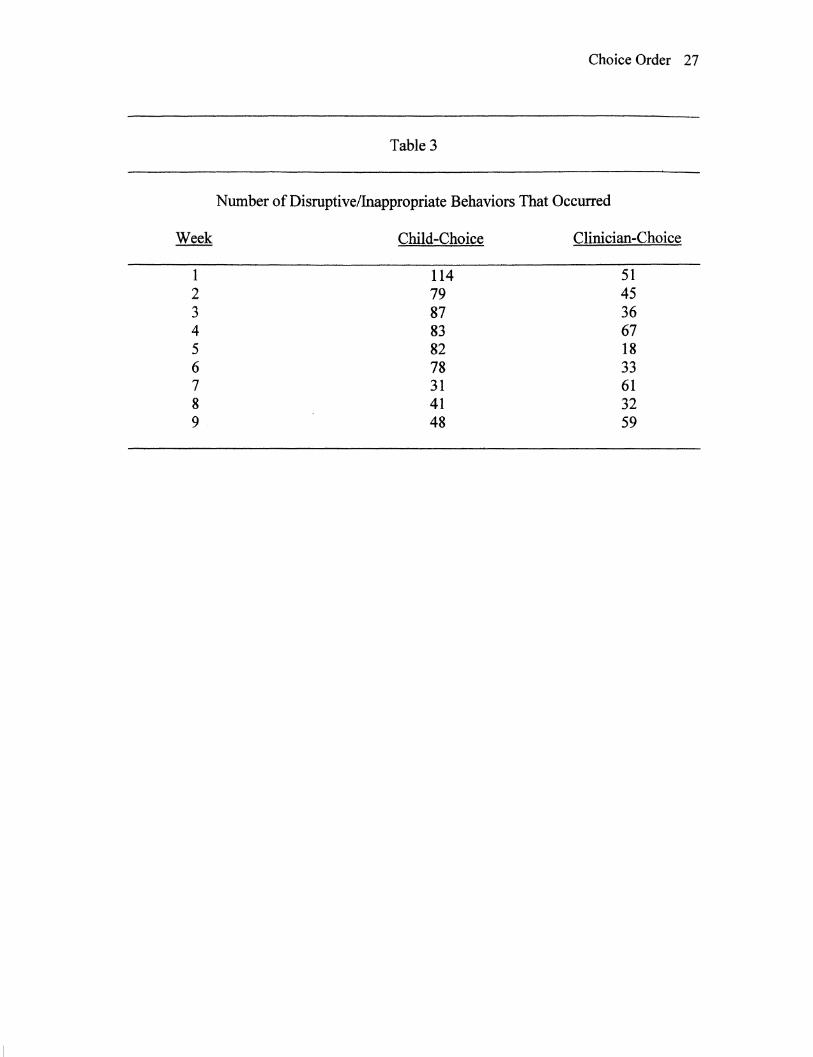
Number of disruptive/inappropriate behaviors ........................... .27
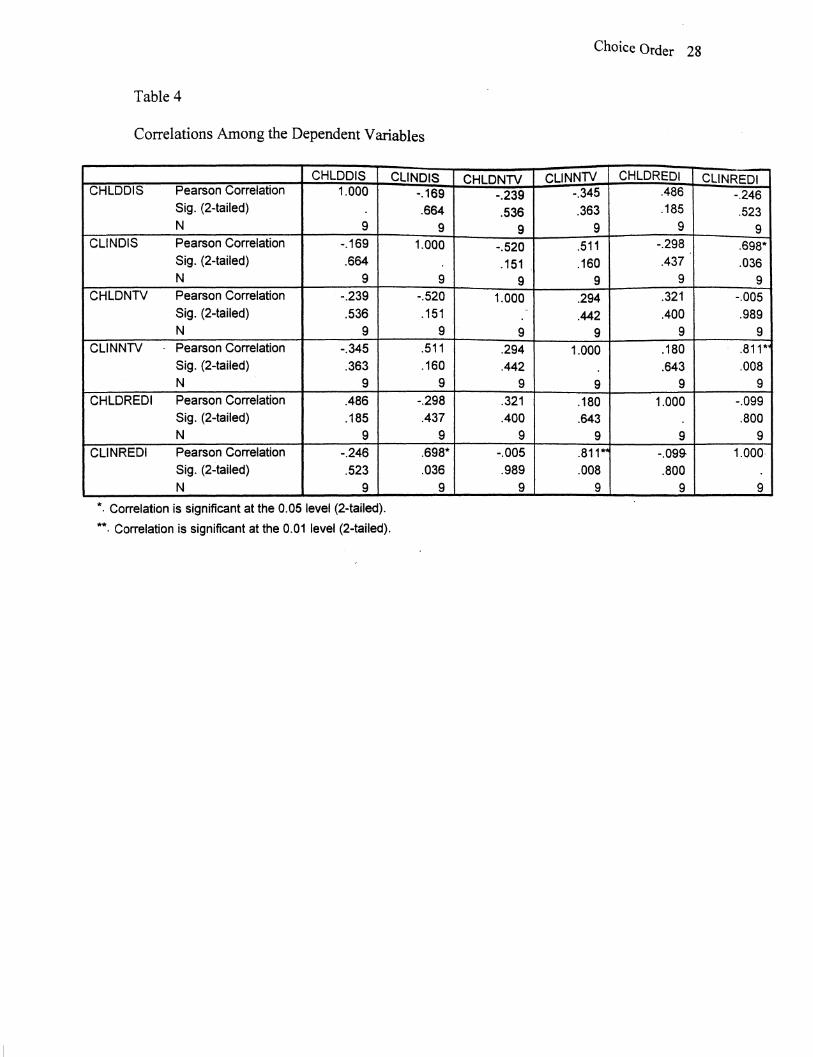
Correlations among the dependent variables .............................. 28
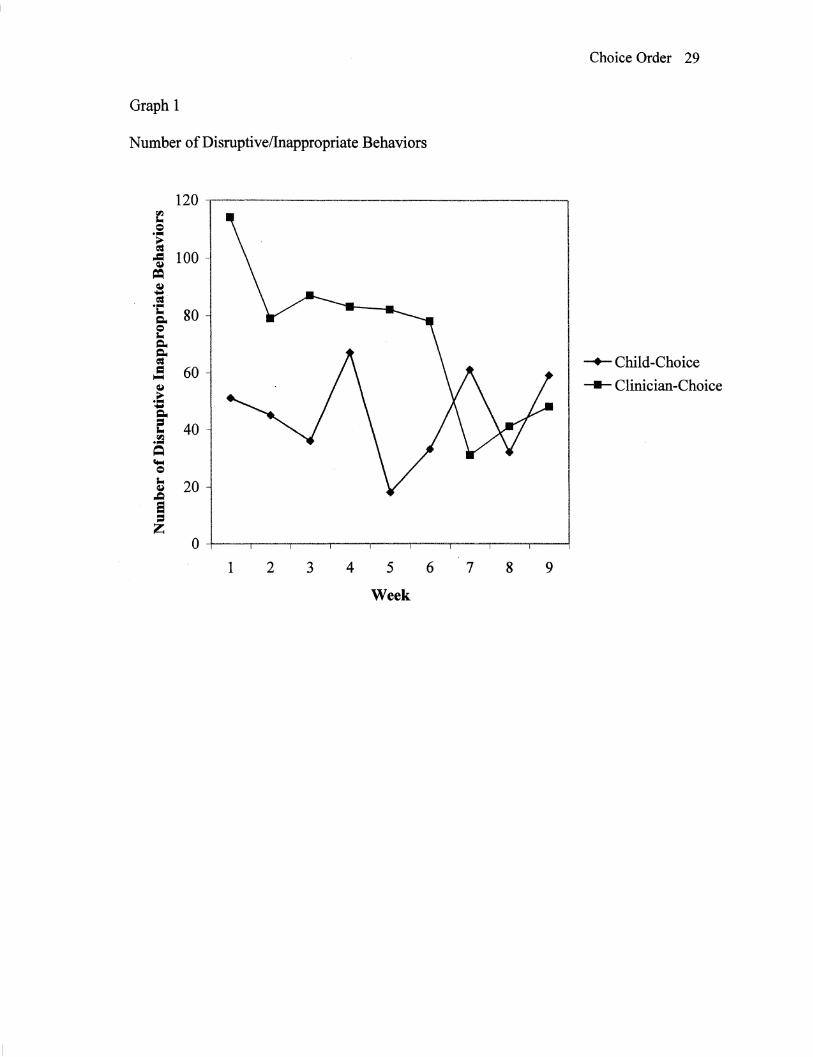
Number of disruptive/inappropriate behaviors ........................... 29
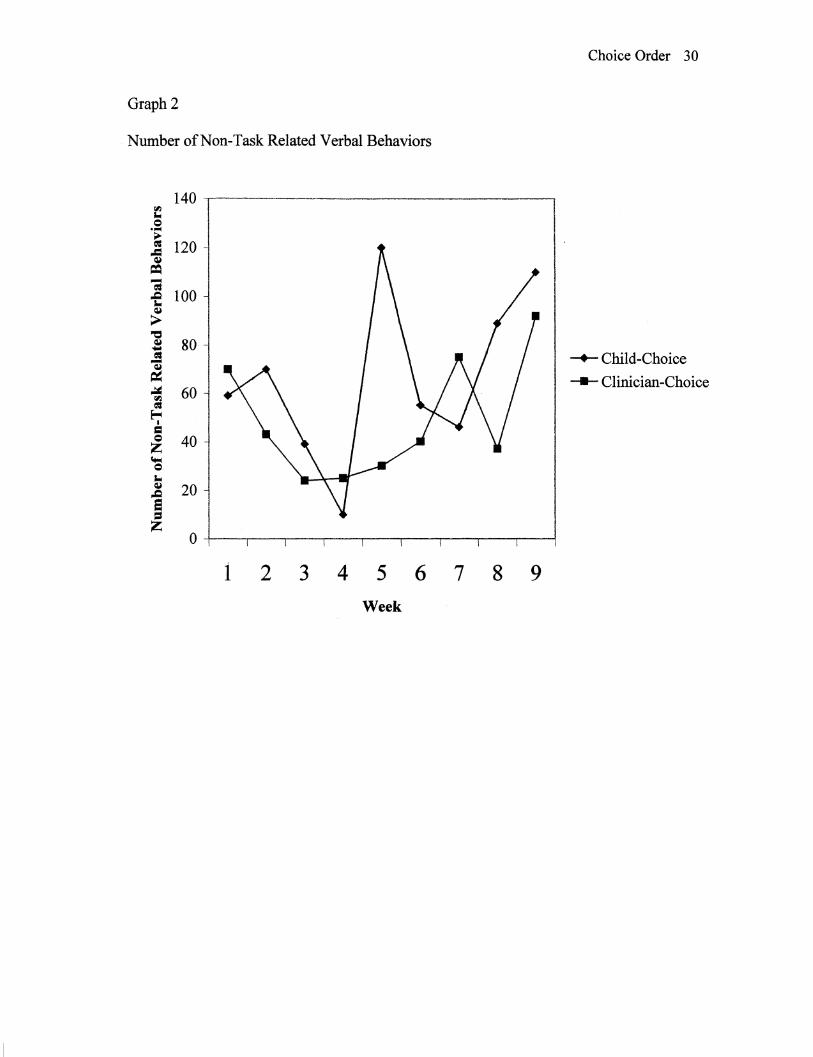
Number of non-task related verbal behaviors ............................. 30
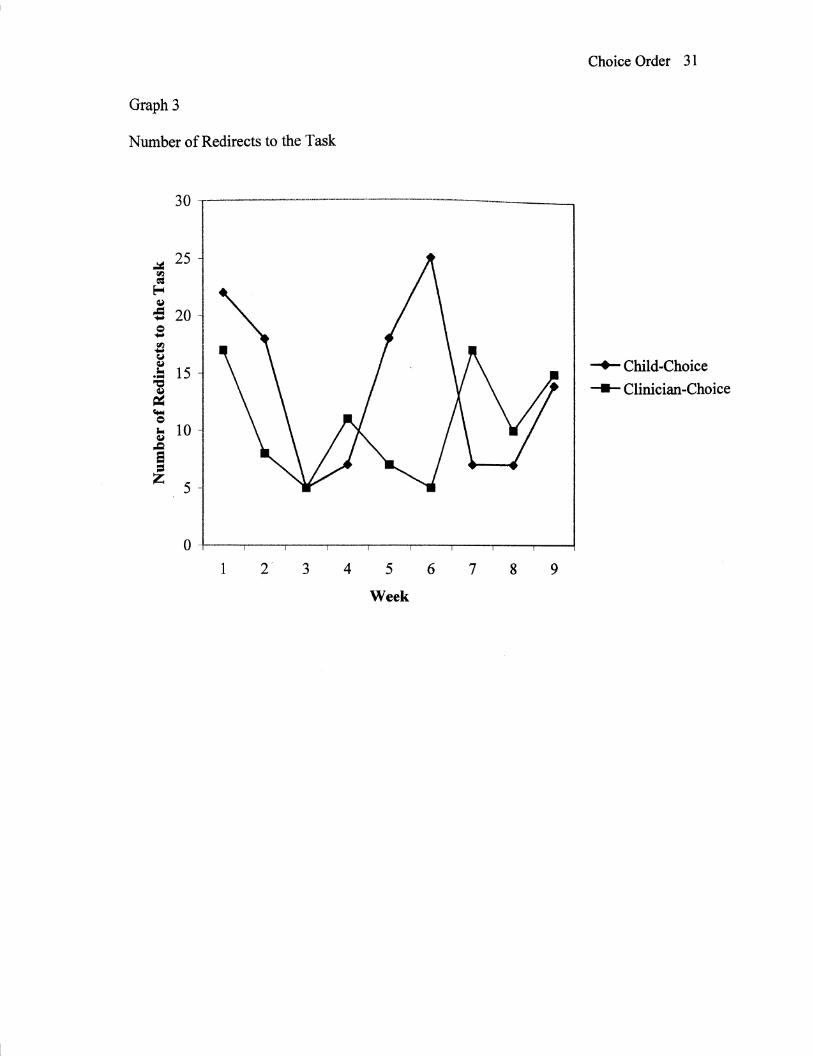
Number of times redirected to the task ..................................... 31
v
Appendix A.
Appendix B.
List of Appendices
Parental Permission Form ................... .32
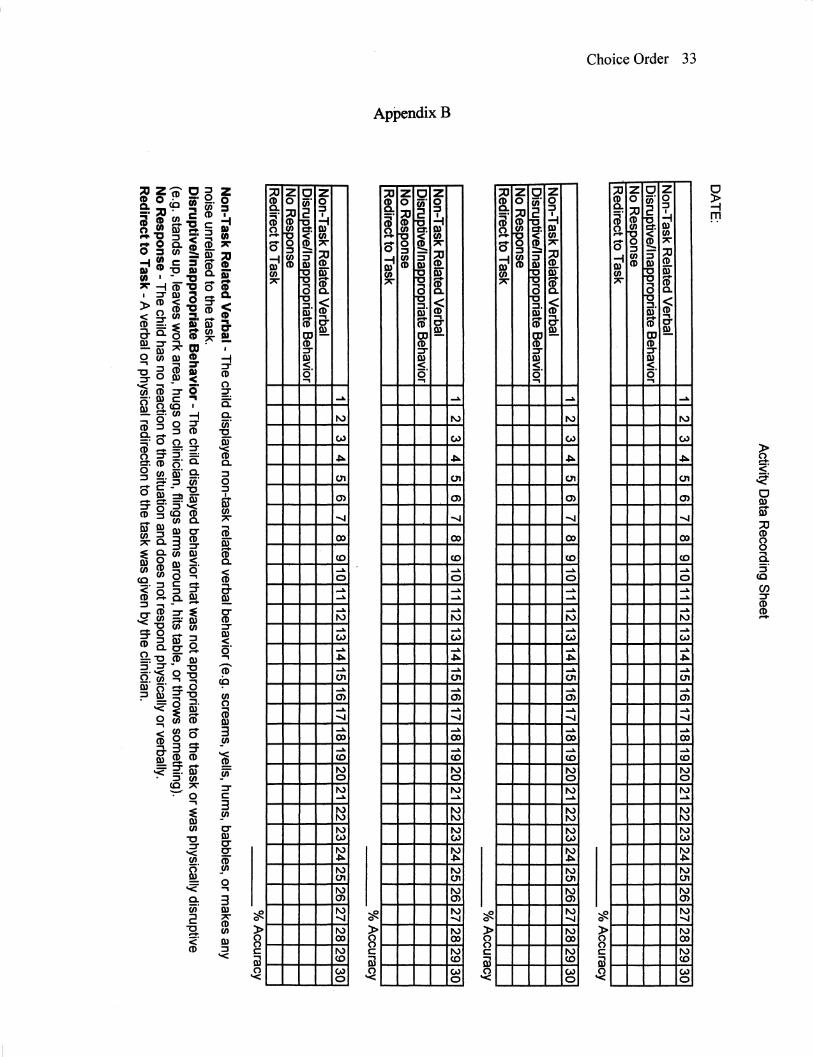
Activity Data Recording Sheet .............. 33
vi
The Effect of Choice Order on Off Task
Behavior in a Child with Autism
Choice Order 1
Dr. Leo Kanner first described the term autism in 1943 when he did a systematic
observation on eleven children with a previously unrecognized syndrome. He noted a
variety of behavioral features that were characteristic of all eleven children. These
characteristics differentiated the eleven children from children with other psychiatric
disorders. These features included an inability to develop relationships with other people,
a delay in speech acquisition, the noncommunicative use of speech after it developed,
delayed echolalia, pronominal reversal, repetitive and stereotyped play activities, an
obsessive insistence on the maintenance of sameness, a lack of imagination, a good rote
memory, a normal physical appearance, and an onset during infancy. The most
discriminating characteristic of these children was social isolation (Rutter, 1978). The
term Kanner coined, autism, means "self' because the children seemed to be intrinsically
focused on their own personal world. Since Kanner first identified the syndrome, various
definitions have been proposed to identify and designate the characteristic of autism, but
Kanner's identification of features has retained its saliency (Richard, 1997).
Autism is a disorder that is included in the category of pervasive developmental
disorders. A pervasive developmental disorder, as defined by the Diagnostic and
Statistical Manual of Mental Disorders, Fourth Edition Text Revision (DSM-IV-TR)
(American Psychological Association, 2000), is a disorder characterized by severe
impairment in several separate areas of development. These include social interaction
skills, communication skills, stereotyped behavior, interests and activities. Onset is
considered to occur by age three years. Included as pervasive developmental disorders
Choice Order 2
are Rett's Disorder, Childhood Disintegrative Disorder, Asperger's Disorder, Pervasive
Developmental Disorder-Not Otherwise Specified, and Autistic Disorder. The DMS-IV-
TR (pg. 7 5) outlines the following as the criteria for the diagnosis of Autistic Disorder:
A. A total of six (or more) items from ( 1 ), (2), and (3 ), with at least two from
(1), and one each from (2) and (3):
(1) qualitative impairment in social interaction, as manifested by at least two of the following:
(a) marked impairment in the use of multiple nonverbal behaviors such as eye-to eye-gaze, facial expression, body posture, and gestures to regulate social interaction
(b) failure to develop peer relationships appropriate to developmental level ( c) a lack of spontaneous seeking to share enjoyment, interests, or
achievement with other people (e.g., by a lack of showing, bringing, or pointing out objects of interest)
( d) lack of social or emotional reciprocity
(2) qualitative impairment in communication as manifested by at least one of the following:
(a) delay in, or total lack of, the development of spoken language (not accompanied by an attempt to compensate through alternative modes of communication such as gestures or mime)
(b) in individuals with adequate speech, marked impairment in the ability to initiate or sustain a conversation with others
(c) stereotyped and repetitive use of language or idiosyncratic language (d) lack of varied, spontaneous make-believe play or social imitative play
appropriate to developmental level
(3) restricted repetitive and stereotyped patterns of behavior, interest, and activities, as manifested by at least one of the following:
(a) encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus
(b) apparently inflexible adherence to specific, nonfunctional routines or rituals
( c) stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements)
( d) persistent preoccupation with parts of objects
B. Delays or abnormal functioning in at least one of the following areas, with onset
Choice Order 3
prior to age 3 years: (1) social interaction, (2) language as used in social communication, or (3) symbolic or imaginative play.
C. The disturbance is not better accounted for by Rett' s Disorder or Childhood Disintegrative Disorder.
As can be inferred from the diagnostic criteria, the most current descriptive literature
considers autism as a spectrum disorder which affects all aspects of a child's
development, including communication, social interaction, and behavioral patterns.
Autism is the third most common developmental disability, affecting approximately
15 children in every 10,000 births however; current epidemiological studies suggest a
significantly higher incidence (Richard, 1997). There is a higher incidence of autism in
the male population, ranging from 2.6 males to every female, to 4.1 males to every
female (Richard, 1997). Gillingham (1995) reported that 60% of people with autism
have IQ scores below 50, 20% between 50 and 70, and 20% have scores greater than 70.
Other statistics have reported that 2/3 to 3/4 of all children with autism have an IQ below
70 (Richard, 1997). These statistics show that autism is a prevalent disorder that can
include a component of cognitive impairment.
As described by Kanner and the DSM-IV-TR criteria, autism has many behavioral
characteristics associated with it. These characteristics can directly influence the
effectiveness of therapy with an individual with autism (Lovaas, Litrownik, & Mann,
1971). For instance, one of the characteristic features is self-stimulation. Self-
stimulatory behaviors, or stereotypies, are repetitive behaviors that the individual with
autism engages in, sometimes for prolonged periods of time. These can include hand
flapping, twirling objects, body rocking, and other behaviors that provide sensory or
Gillingham, G. (1995). Autism: Handle with care. Arlington, TX: Future Education
Choice Order 23
Incorporated.
Kem, L., Koegel, R.L., & Dunlap, G. (1984). The influence of vigorous verses mild
exercise on autistic stereotyped behaviors. Journal of Autism and Developmental
Disorders, 14, 57-67.
Koegel, R. L., Dyer, K., & Bell, L. K. (1987). The influence of child-preferred activities
on autistic children's social behavior. Journal of Applied Behavior Analysis, 20, 243-
252.
Koegel, R.L. & Koegel, L.K. (1995). Teaching Children with Autism. Paul H. Brooks:
Baltimore, MD.
Koegel, R. L., Koegel, L .K., & Surrant, A. (1992). Language intervention and
disruptive behavior in preschool children with autism. Journal of Autism and
Developmental Disorders, 22, (2), 141-153.
Lovass, 0. I., Litrownik, A., & Mann, R. (1971). Response latencies to auditory stimuli
in autistic children engaged in self-stimulatory behavior. Behavior Research and
Therapy, 9, 39-49.
Lovass, 0.1. (1977). The autistic child: Language development through behavior
modification. New York: Irvington Publishers.
Moes, D.R. (1998). Integrating choice-making opportunities within teacher-assigned
academic tasks to facilitate the performance of children with autism. The Journal of
the Associationfor Persons with Severe Handicaps, 23, 319-328.
Prizant, B.M. (1983). Language acquisition and communicative behavior in autism:
Toward an understanding of the "whole" or it Journal of Speech and Hearing
Disorders, 48, 296-307.
Choice Order 24
Richard, G. (1997). Source for Autism. East Moline: Lingui Systems.
Rutter, M. (1978). Diagnosis and definition of childhood autism. Journal of Autism and
Childhood Schizophrenia, 8, 139-161.
Singh, N. N. (Ed.). (1997). Prevention and treatment of severe behavior problems:
Models and methods in developmental disabilities. Pacific Grove, CA: Brooks and
Cole.
Tager-Flusberg, H. (1996). Pervasive developmental disorder, commonly abbreviated as
PDD (editorial). Journal of Autism and Developmental Disorders, 27, 364·377.
Choice Order 25
Table 1
Dependent Variables and Definitions
Non-Task Related Verbal The child displayed non-task related verbal behavior (e.g. screams, yells, hums, babbles, or makes any noise unrelated to the task).
Disruptive/Inappropriate Behavior The child displayed behavior that was not appropriate to the task or was physically disruptive (e.g. stands up, leaves work area, hugs on clinician, flings arms around, hits table, hits self or clinician, or throws something).
Redirection to the task A verbal or physical redirection to the task was given by the clinician.
(adopted from Gibson, 1999)
Choice Order 26
Table 2
Across All Therapy Sessions, Mean Number of 10-second Intervals Spent Being
Condition Disruntive Non-task Verbal Redirected to Task Overall