REVIEW ARTICLE The effect of exercise-based management for multidirectional instability of the glenohumeral joint: a systematic review Sarah A. Warby, BPhysio(Hons) a, *, Tania Pizzari, PhD, BPhysio(Hons) a , Jon J. Ford, PhD, MPhysio, BAppSci(Physio), CredMDT b , Andrew J. Hahne, PhD, BPhysio(Hons) b , Lyn Watson, BAppSci(Physio), GradDip b,c a Department of Physiotherapy, Faculty of Health Sciences, La Trobe University, Bundoora, VIC, Australia b Musculoskeletal Research Centre, Department of Physiotherapy, Faculty of Health Sciences, La Trobe University, Bundoora, VIC, Australia c LifeCare Prahran Sports Medicine Centre, Prahran, VIC, Australia Background: The most commonly recommended treatment for multidirectional instability (MDI) of the glenohumeral joint is exercise-based management. The primary objective of this review was to evaluate the effectiveness of exercise-based management in patients with MDI. The secondary aim was to observe the types of exercise protocols and outcomes used, as well as any adverse results associated with exercise. Methods: The Cochrane Database of Systematic Reviews, Medline, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature), PEDro, Current Contents, Allied and Complementary Medicine (AMED), Australasian Medical Index (AMI), Ausport, and Clinical Trials Registers were searched for published and unpublished studies from the inception date to June 2012 using the keywords multidirectional instability, gle- nohumeral, and exercise. Selection criteria included all study designs (except case reports and case series) and par- ticipants with clinically diagnosed MDI using exercise-based management. Inclusion criteria were not limited by outcomes. The authors’ own risk-of-bias tool was used for quality assessment of studies. The GRADE approach (Grading of Recommendations, Assessment, Development and Evaluation) was used to synthesize the evidence. Results: The risk of bias was high in all 7 included studies. For before-and-after comparisons of exercise-based management, GRADE assessment showed very low–quality evidence for improvements in shoulder kinematics, the Rowe score, overall status rating, and peak muscle strength. Conclusions: The effect of exercise-based management on MDI was variable across the included studies because of study heterogeneity and a high level of bias. There is a need for high-quality intervention studies to be undertaken to validate the effect of exercise for MDI. Level of evidence: Level IV, Systematic Review. Ó 2014 Journal of Shoulder and Elbow Surgery Board of Trustees. Keywords: Multidirectional instability; glenohumeral; shoulder; exercise-based management; impairment; patient focused No ethics committee approval was required to conduct and produce this systematic review. *Reprint requests: Sarah A. Warby, BPhysio(Hons), Department of Physiotherapy, La Trobe University, Level 5, HS3, Corner of Kingsbury Drive and Plenty Road, Bundoora, Victoria 3086, Australia. E-mail address: [email protected](S.A. Warby). J Shoulder Elbow Surg (2014) 23, 128-142 www.elsevier.com/locate/ymse 1058-2746/$ - see front matter Ó 2014 Journal of Shoulder and Elbow Surgery Board of Trustees. http://dx.doi.org/10.1016/j.jse.2013.08.006
Transcript
No ethics comm
systematic revie
J Shoulder Elbow Surg (2014) 23, 128-142
1058-2746/$ - s
http://dx.doi.org
www.elsevier.com/locate/ymse
REVIEW ARTICLE
The effect of exercise-based management formultidirectional instability of the glenohumeral joint:a systematic review
Sarah A. Warby, BPhysio(Hons)a,*, Tania Pizzari, PhD, BPhysio(Hons)a,Jon J. Ford, PhD, MPhysio, BAppSci(Physio), CredMDTb,Andrew J. Hahne, PhD, BPhysio(Hons)b, Lyn Watson, BAppSci(Physio), GradDipb,c
aDepartment of Physiotherapy, Faculty of Health Sciences, La Trobe University, Bundoora, VIC, AustraliabMusculoskeletal Research Centre, Department of Physiotherapy, Faculty of Health Sciences, La Trobe University, Bundoora,VIC, AustraliacLifeCare Prahran Sports Medicine Centre, Prahran, VIC, Australia
Background: The most commonly recommended treatment for multidirectional instability (MDI) of theglenohumeral joint is exercise-based management. The primary objective of this review was to evaluatethe effectiveness of exercise-based management in patients with MDI. The secondary aim was to observethe types of exercise protocols and outcomes used, as well as any adverse results associated with exercise.Methods: The Cochrane Database of Systematic Reviews, Medline, Embase, CINAHL (Cumulative Index toNursing and Allied Health Literature), PEDro, Current Contents, Allied and Complementary Medicine(AMED), Australasian Medical Index (AMI), Ausport, and Clinical Trials Registers were searched for publishedand unpublished studies from the inception date to June 2012 using the keywords multidirectional instability, gle-nohumeral, and exercise. Selection criteria included all study designs (except case reports and case series) and par-ticipants with clinically diagnosed MDI using exercise-based management. Inclusion criteria were not limited byoutcomes. The authors’ own risk-of-bias tool was used for quality assessment of studies. The GRADE approach(Grading of Recommendations, Assessment, Development and Evaluation) was used to synthesize the evidence.Results: The risk of bias was high in all 7 included studies. For before-and-after comparisons of exercise-basedmanagement, GRADE assessment showed very low–quality evidence for improvements in shoulder kinematics,the Rowe score, overall status rating, and peak muscle strength.Conclusions: The effect of exercise-based management on MDI was variable across the included studiesbecause of study heterogeneity and a high level of bias. There is a need for high-quality intervention studiesto be undertaken to validate the effect of exercise for MDI.Level of evidence: Level IV, Systematic Review.� 2014 Journal of Shoulder and Elbow Surgery Board of Trustees.
Multidirectional instability (MDI) is symptomatic gle- Methods
nohumeral joint subluxation or dislocation occurring inmore than 1 direction.1,2,5,15 Discrepancies exist in thecurrent literature concerning the precise definition, classi-fication, and pathogenesis of MDI,2,5,35 making selectionof the most appropriate management regimen chal-lenging.2,5,35 The classification of shoulder instability existsas a continuum of pathologies, with traumatic, structural,unidirectional instability at one extreme and atraumatic,nonstructural, multidirectional instability at the other.29,34
Many patients fall somewhere between these extremes,which contributes to difficulties in definitive diagnoses.29,34
There is general agreement that MDI is due to repetitivemicrotrauma imposed on a congenitally lax and redundantjoint capsule.1,15,26,35,40 Patients with MDI can present witha variety of symptoms ranging from reports of vagueshoulder pain without the perception of instability to dailyoccurrences of symptomatic subluxations or frank dislo-cations with activities of daily living.2 Typically, patientshave reduced scapula upward rotation, an imbalance ofmuscle strength, and suboptimal neuromuscular control ofshoulder function when compared with normal controlsubjects.28,31,35,38 MDI is fundamentally a different pa-thology than unidirectional instability, which is typicallythe result of a traumatic event imposed on a normal gle-nohumeral joint.10,29
The most commonly recommended treatment for MDI isnonoperative with an emphasis on exercise-based man-agement.1,2,5,8,10,15,35,48 This is based on the rationale thatstrengthening the scapula and rotator cuff muscles com-pensates for the lack of passive stability and assists in activecontrol of the shoulder.5,15,35 Surgery to tighten the gle-nohumeral joint capsule, usually an inferior capsular shift,may be indicated in some cases in which conservativemanagement has failed.2,5,15 However, the long-term out-comes of surgery on a capsule that has a high susceptibilityto stretch35 are still unknown.3,5,15 Given the important rolethat muscle plays in the stability of the shoulder35 and giventhat poor muscle patterning is a contributing factor toinstability in this population,29 rehabilitation is consideredthe primary treatment option.5,15
To date, there have been no published systematic reviewsinvestigating the conservativemanagement ofMDI. BecauseMDI is a pathology that is becoming increasingly recognizedin the clinical setting,52 it is appropriate to review the sci-entific literature to evaluate what is currently known aboutthe efficacy of exercise-based management for MDI to allowfor planning of future research in this area.
The primary objective of this systematic review was toevaluate the evidence on exercise-based management inpatients with clinically diagnosed MDI. The secondaryobjective of this review was to identify the exercise pro-tocols and outcomes used, as well as any adverse resultsassociated with exercise-based management, within theincluded studies.
The authors of this article, before conducting a literature search,developed a review protocol that is summarized herein.
Eligibility criteria
Study designThis review included both randomized and nonrandomized studies(NRS). Non-controlled ‘‘before-and-after’’ studies with 10 pa-tients or fewer were classified as case reports or case series andwere excluded42 because of their inherently high level of bias.25
Including NRS enabled the reviewers (S.A.W., T.P., and J.J.F.)to examine the case for undertaking future research by providingan explicit evaluation of the weaknesses, benefits, and harms ofavailable NRS.25
ParticipantsStudies were included if they involved at least 1 group of humanparticipants with clinically diagnosed MDI, with instability in atleast 2 directions. The diagnosis of MDI must have been estab-lished by a physiotherapist, medical doctor, or surgeon and basedon the following:
1. A positive sulcus sign or test for inferior laxity49
2. A positive load-and-shift test or positive sign of pain and/orapprehension in loading of the glenohumeral joint in at least1 of the positions that stress the anterior (arm abduction at90�, external rotation) or posterior (flexion, adduction) jointcomplex13,36,44,49,50
Although there are discrepancies in the diagnostic criteria forMDI,2,5,15 the reviewers made the decision to use the previouslymentioned inclusion criteria to reduce the likelihood that partici-pants with unidirectional instability would be included, whichcould confound the outcomes of the review. Where necessary,authors were emailed to clarify any uncertainties regarding theirparticipant inclusion criteria. If an author did not respond within2 months, the article was excluded.
Types of interventionsStudies were included if at least 1 group with MDI receivedexercise-based management. Studies using only surgical inter-vention or non–exercise-based conservative management (eg,acupuncture) were excluded.
Types of outcome measuresInclusion criteria were not limited by outcome measures becauseit is recommended to search for studies investigating all effects ofan intervention when including NRS.25
Search methods and study selection
Studies published in any language were located by a comprehensivecomputer-aided search of the following databases from the date ofinception to June 30, 2012: Medline, CINAHL (Cumulative Index toNursing and Allied Health Literature), Embase, PEDro, CurrentContents, Allied and Complementary Medicine (AMED),
130 S.A. Warby et al.
Australasian Medical Index (AMI), Ausport, SportDiscus, CochraneCentral Register of Controlled Trials, and Cochrane Database ofSystematic Reviews. To maximize sensitivity, a 3-term search strat-egy was used,51 combining the keywords ‘‘multidirectional insta-bility,’’ ‘‘shoulder,’’ and ‘‘exercise.’’ A list of terms relating to thepathology, the anatomic region, and the intervention is presented inTable I. All terms were applied to every database, and the searchstrategy for Medline is outlined in Appendix A (available on thejournal’s website at www.jshoulderelbow.org). Depending on thedatabase, each term was searched as a MeSH or subject heading, aswell as a keyword. Truncation symbols and explosion of keywordswere applied where appropriate. The Clinical Trials Registers (http://www.clinicaltrials.gov, http://www.anzctr.org.au/default.aspx) weresearched for unpublished studies, citation tracking was performed onall relevant articles through the ISIWeb of Science, and bibliographysearches were conducted on all relevant articles retrieved.
Two reviewers (S.A.W. and T.P.) independently selected thetrials to be included in the review. Initial search results wereelectronically exported to Endnote X547 and duplicate studiesdeleted. If titles or abstracts did not provide sufficient informationto independently evaluate an article for inclusion, the full text wasretrieved. The review’s inclusion and exclusion criteria wereapplied to the full text to obtain the final number of includedstudies. Any disagreement on the inclusion of an article would beresolved through discussion between the 2 reviewers (S.A.W. andT.P.) and, if necessary, a third reviewer (J.J.F.).
Data extraction
Data for each study were extracted using a customized dataextraction form that included features recommended by the NonRandomised Studies Methods Group (NRSMG)25 and the Trans-parent Reporting of Evaluations with Non Randomised Designs(TREND) statement30 for reporting and evaluating NRS. The typeof data extracted included (but was not limited to) study inclusionand exclusion criteria, details of methodology, outcome measures,confounding variables, and any statistical analyses.
Data analysis: quality assessment of studies
Because of the variety of study designs classified as NRS and theirvarying susceptibility to different biases, reviewers often need toformulate their own tool for quality assessment.25 For this systematicreview, the reviewers developed a quality tool based on a tool used bymethodologists in a review of NRS on human immunodeficiencyvirus.46 This tool assesses the recommended domains of bias25 andalso enables the development of customized domains to be assessedbased on a combination of theoretical and empirical considerations.25
Specific criteria were created to evaluate bias in study design, theassessment of MDI participants, the execution and reporting of anexercise intervention, and the specificity of outcomes. Guidelines forthe tool’s application are outlined in Appendix B (available on thejournal’s website at www.jshoulderelbow.org). This tool was thenused to formulate an overall judgment on the level of bias for eachindividual study to be used in evaluation of the evidence based on asystematic review using NRS, the GRADE approach (Grading ofRecommendations, Assessment, Development and Evaluation),11
and guidelines by the Cochrane Collaboration.25
The criteria for the overall risk of bias were as follows: ‘‘Lowrisk overall’’ was defined when all types of biases were considered
low risk. ‘‘Moderate risk overall’’ was defined when at least 1 biaswas considered moderate risk and the others were low. ‘‘High riskoverall’’ was defined when at least 1 bias was considered high riskand the others were low or moderate.
Data synthesis
When 2 or more exercise-based interventions for MDI werecompared, the standardized mean difference with 95% confidenceintervals would be calculated for continuous data23 and relativerisks with 95% confidence intervals would be calculated fordichotomous data.24 When data obtained only before and afterintervention or only after intervention were made available withno exercise-based control or comparison group, additional tablesand text would be used to present results in a systematic format.Data synthesis would not be performed when exercise-based in-terventions were compared with non-exercise-based interventions(eg, surgery) because this was beyond the aims of the review. Ameta-analysis of pooled data was planned if 2 or more trials wereconsidered to be clinically homogeneous, defined as sufficientlysimilar in participant characteristics, interventions, and out-comes.25 There was no planned sensitivity or subgroup analysis.
Quality assessment of evidence
A qualitative analysis using the GRADE approach12,25,41 wasplanned. This method provides a rating of the quality of evidencefor each primary outcome based on 5 domains: limitations of thetrial design, inconsistency, indirectness, imprecision of results,and publication bias.12,41 The assessment of each domain leads toan overall rating of the quality of evidence for each outcome: high,moderate, low, or very low (Appendix C, available on the journal’swebsite at www.jshoulderelbow.org).4,45
Results
Search results
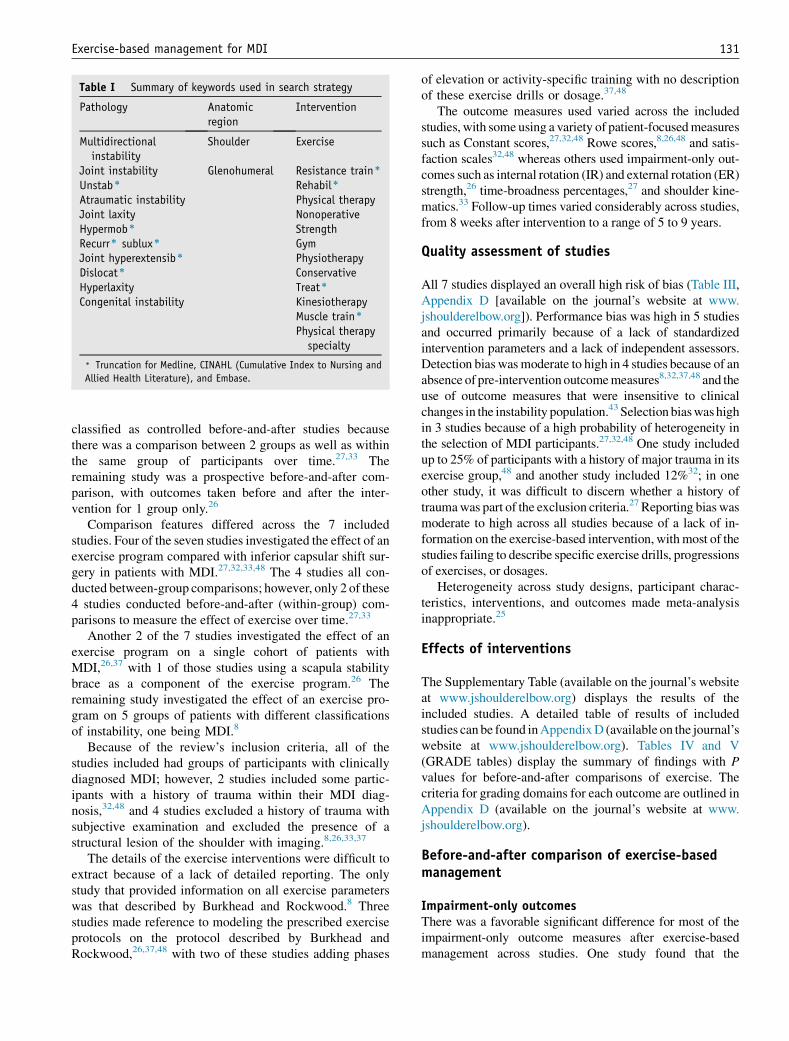
After omission of duplicate citations, the search yield was6,619. After omission of citations that were clearly irrele-vant, 114 full-text articles were identified for full-textretrieval. Of these, a total of 7 articles met the inclusioncriteria for the review. The number of results received ateach stage of the review process, along with the number ofstudies excluded and reasons for exclusion, is outlined inFigure 1.
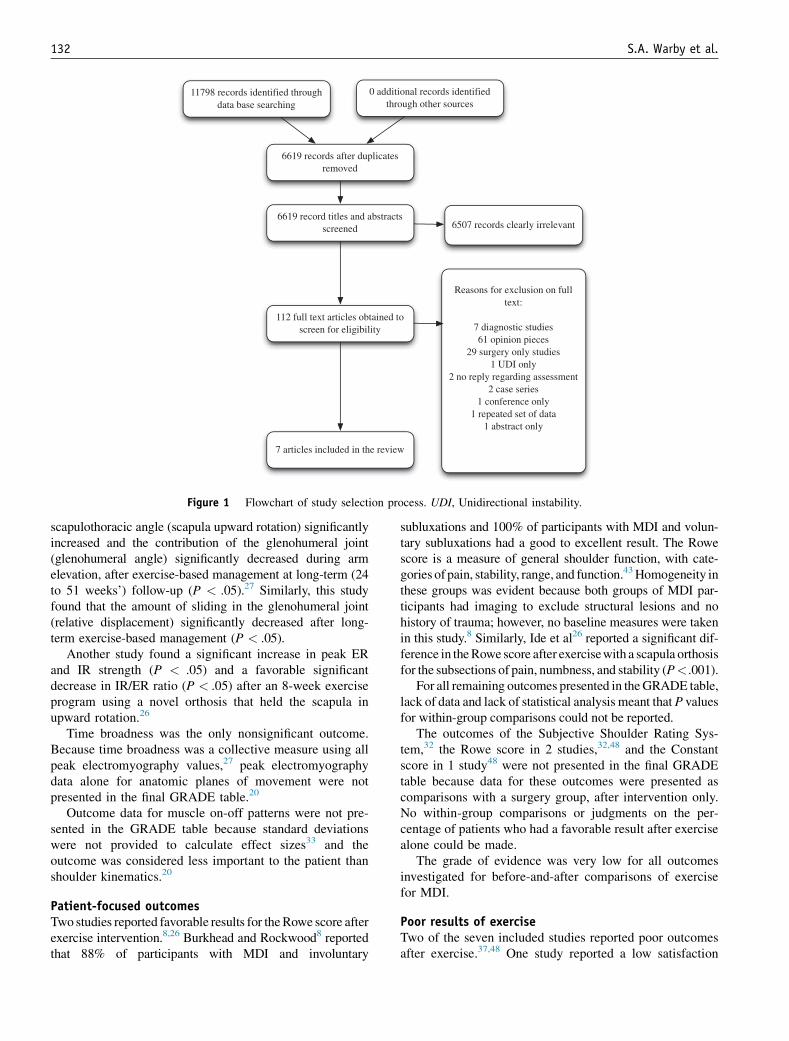
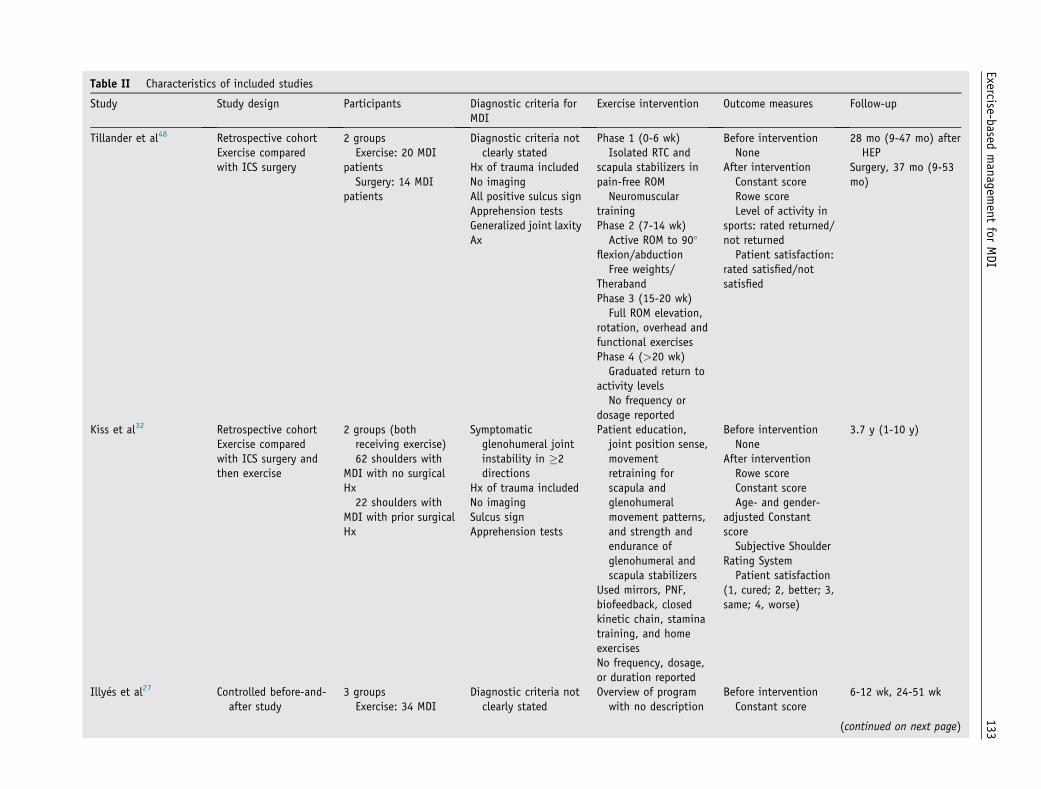
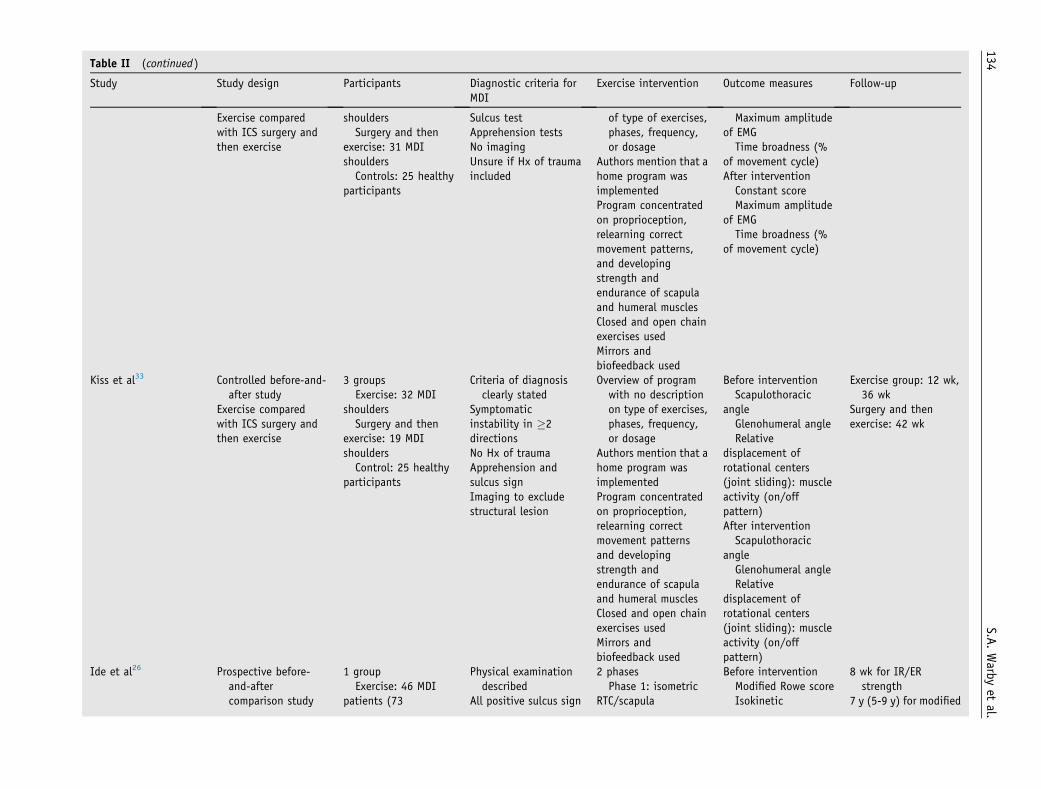
Characteristics of included studies
Table II displays the characteristics of the included studies.Study design was classified according to Cochrane list ofstudy design features25 and varied across the includedliterature. Four of the seven studies were classified asretrospective cohorts because participants were identifiedretrospectively and outcome measures were only obtainedafter intervention.8,32,37,48 Two of the seven studies were
) Truncation for Medline, CINAHL (Cumulative Index to Nursing and
Allied Health Literature), and Embase.
Exercise-based management for MDI 131
classified as controlled before-and-after studies becausethere was a comparison between 2 groups as well as withinthe same group of participants over time.27,33 Theremaining study was a prospective before-and-after com-parison, with outcomes taken before and after the inter-vention for 1 group only.26
Comparison features differed across the 7 includedstudies. Four of the seven studies investigated the effect of anexercise program compared with inferior capsular shift sur-gery in patients with MDI.27,32,33,48 The 4 studies all con-ducted between-group comparisons; however, only 2 of these4 studies conducted before-and-after (within-group) com-parisons to measure the effect of exercise over time.27,33
Another 2 of the 7 studies investigated the effect of anexercise program on a single cohort of patients withMDI,26,37 with 1 of those studies using a scapula stabilitybrace as a component of the exercise program.26 Theremaining study investigated the effect of an exercise pro-gram on 5 groups of patients with different classificationsof instability, one being MDI.8
Because of the review’s inclusion criteria, all of thestudies included had groups of participants with clinicallydiagnosed MDI; however, 2 studies included some partic-ipants with a history of trauma within their MDI diag-nosis,32,48 and 4 studies excluded a history of trauma withsubjective examination and excluded the presence of astructural lesion of the shoulder with imaging.8,26,33,37
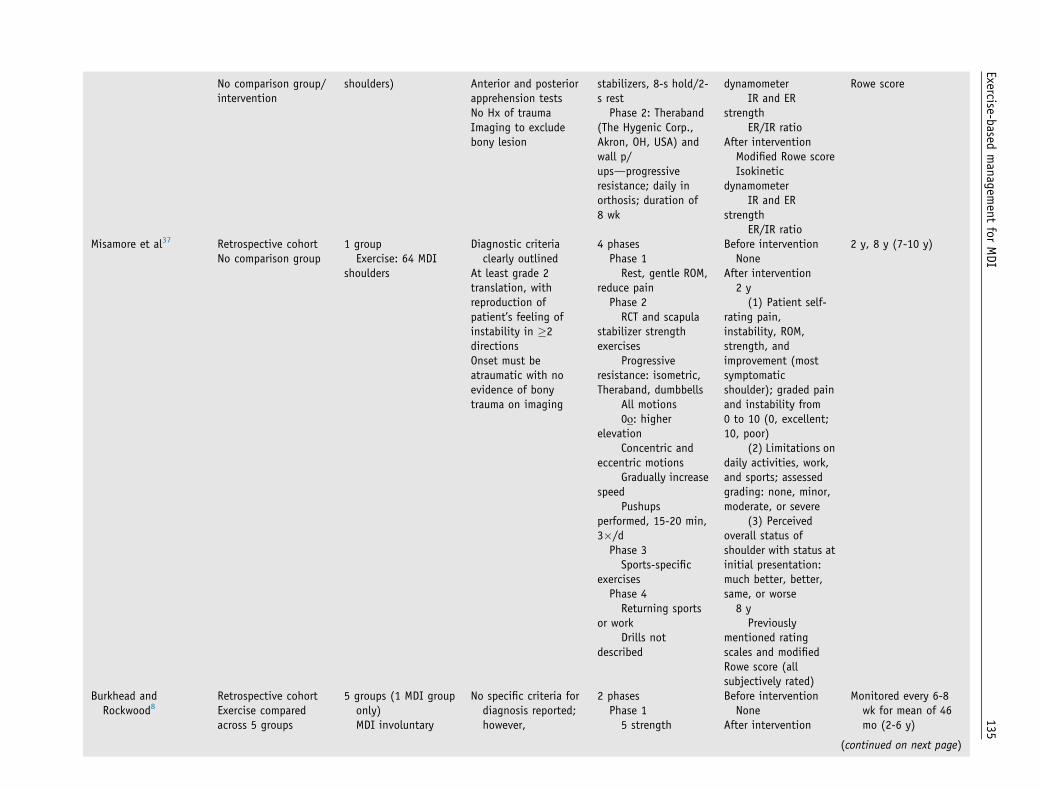
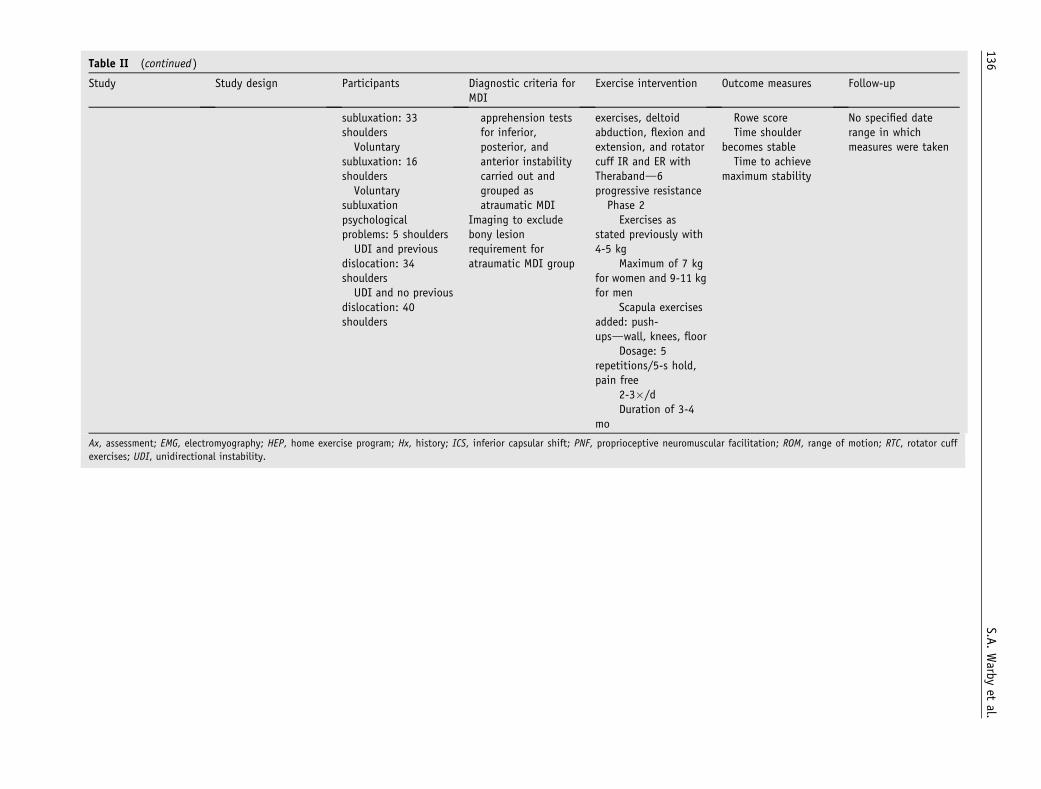
The details of the exercise interventions were difficult toextract because of a lack of detailed reporting. The onlystudy that provided information on all exercise parameterswas that described by Burkhead and Rockwood.8 Threestudies made reference to modeling the prescribed exerciseprotocols on the protocol described by Burkhead andRockwood,26,37,48 with two of these studies adding phases
of elevation or activity-specific training with no descriptionof these exercise drills or dosage.37,48
The outcome measures used varied across the includedstudies, with some using a variety of patient-focusedmeasuressuch as Constant scores,27,32,48 Rowe scores,8,26,48 and satis-faction scales32,48 whereas others used impairment-only out-comes such as internal rotation (IR) and external rotation (ER)strength,26 time-broadness percentages,27 and shoulder kine-matics.33 Follow-up times varied considerably across studies,from 8 weeks after intervention to a range of 5 to 9 years.
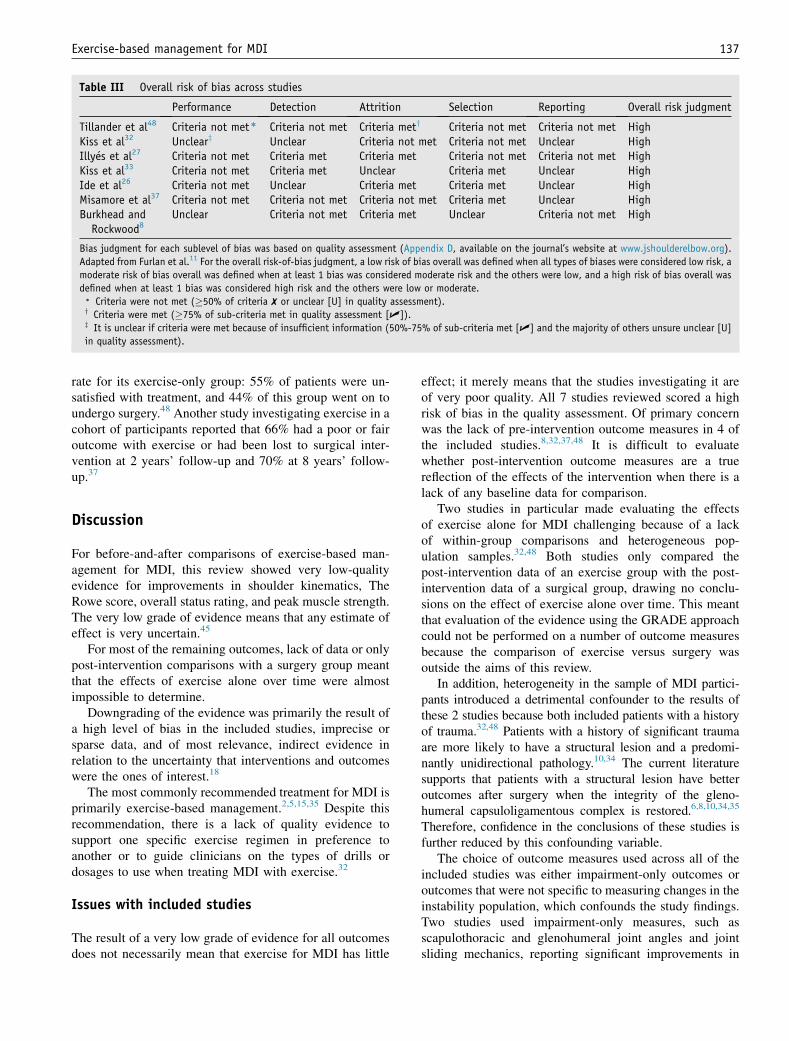
Quality assessment of studies
All 7 studies displayed an overall high risk of bias (Table III,Appendix D [available on the journal’s website at www.jshoulderelbow.org]). Performance bias was high in 5 studiesand occurred primarily because of a lack of standardizedintervention parameters and a lack of independent assessors.Detection bias wasmoderate to high in 4 studies because of anabsence of pre-intervention outcomemeasures8,32,37,48 and theuse of outcome measures that were insensitive to clinicalchanges in the instability population.43Selection biaswashighin 3 studies because of a high probability of heterogeneity inthe selection of MDI participants.27,32,48 One study includedup to 25% of participants with a history of major trauma in itsexercise group,48 and another study included 12%32; in oneother study, it was difficult to discern whether a history oftraumawas part of the exclusion criteria.27 Reporting bias wasmoderate to high across all studies because of a lack of in-formation on the exercise-based intervention, withmost of thestudies failing to describe specific exercise drills, progressionsof exercises, or dosages.
Heterogeneity across study designs, participant charac-teristics, interventions, and outcomes made meta-analysisinappropriate.25
Effects of interventions
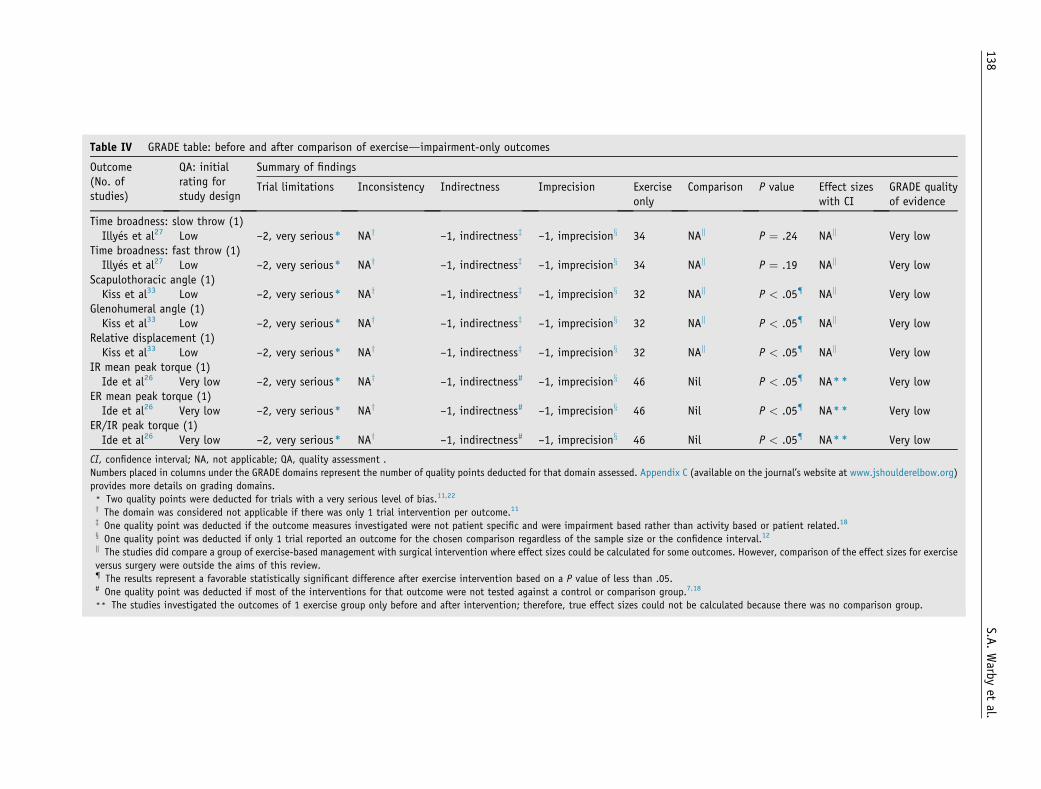
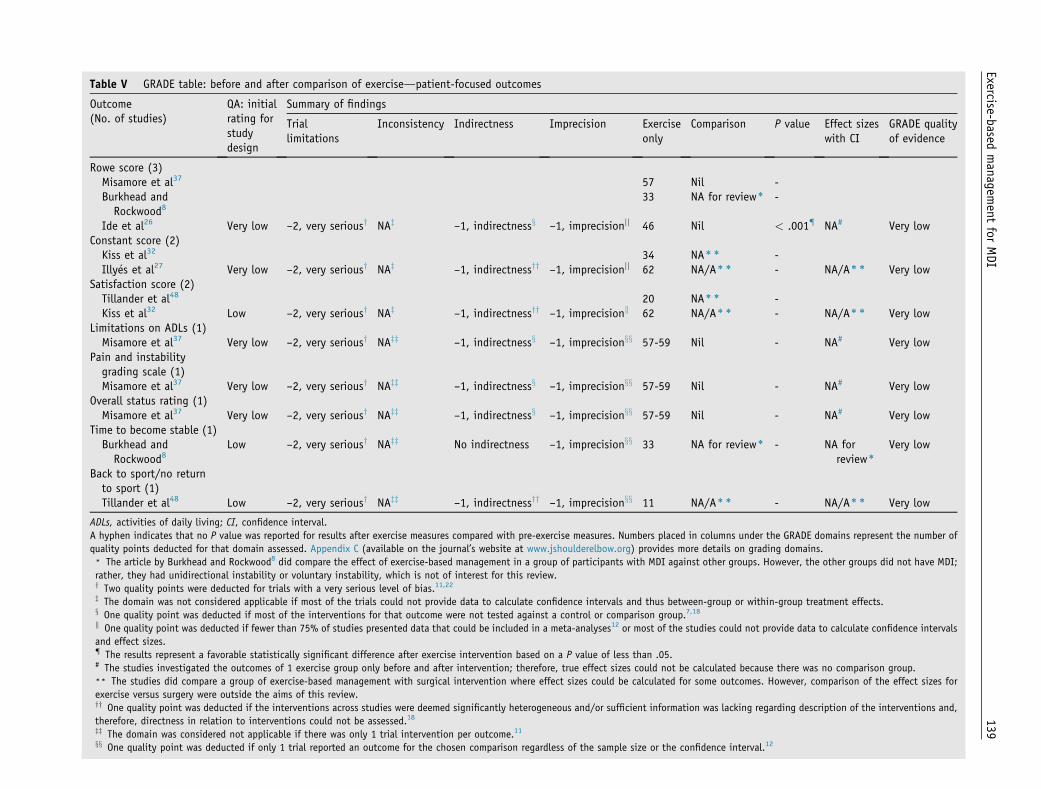
The Supplementary Table (available on the journal’s websiteat www.jshoulderelbow.org) displays the results of theincluded studies. A detailed table of results of includedstudies can be found inAppendixD (available on the journal’swebsite at www.jshoulderelbow.org). Tables IV and V(GRADE tables) display the summary of findings with Pvalues for before-and-after comparisons of exercise. Thecriteria for grading domains for each outcome are outlined inAppendix D (available on the journal’s website at www.jshoulderelbow.org).
Before-and-after comparison of exercise-basedmanagement
Impairment-only outcomesThere was a favorable significant difference for most of theimpairment-only outcome measures after exercise-basedmanagement across studies. One study found that the
11798 records identified through data base searching
6619 records after duplicates removed
0 additional records identified through other sources
Reasons for exclusion on full text:
7 diagnostic studies61 opinion pieces
29 surgery only studies1 UDI only
2 no reply regarding assessment2 case series
1 conference only 1 repeated set of data
1 abstract only
7 articles included in the review
6507 records clearly irrelevant 6619 record titles and abstracts
screened
112 full text articles obtained to screen for eligibility
Figure 1 Flowchart of study selection process. UDI, Unidirectional instability.
132 S.A. Warby et al.
scapulothoracic angle (scapula upward rotation) significantlyincreased and the contribution of the glenohumeral joint(glenohumeral angle) significantly decreased during armelevation, after exercise-based management at long-term (24to 51 weeks’) follow-up (P < .05).27 Similarly, this studyfound that the amount of sliding in the glenohumeral joint(relative displacement) significantly decreased after long-term exercise-based management (P < .05).
Another study found a significant increase in peak ERand IR strength (P < .05) and a favorable significantdecrease in IR/ER ratio (P < .05) after an 8-week exerciseprogram using a novel orthosis that held the scapula inupward rotation.26
Time broadness was the only nonsignificant outcome.Because time broadness was a collective measure using allpeak electromyography values,27 peak electromyographydata alone for anatomic planes of movement were notpresented in the final GRADE table.20
Outcome data for muscle on-off patterns were not pre-sented in the GRADE table because standard deviationswere not provided to calculate effect sizes33 and theoutcome was considered less important to the patient thanshoulder kinematics.20
Patient-focused outcomesTwo studies reported favorable results for theRowe score afterexercise intervention.8,26 Burkhead and Rockwood8 reportedthat 88% of participants with MDI and involuntary
subluxations and 100% of participants with MDI and volun-tary subluxations had a good to excellent result. The Rowescore is a measure of general shoulder function, with cate-gories of pain, stability, range, and function.43Homogeneity inthese groups was evident because both groups of MDI par-ticipants had imaging to exclude structural lesions and nohistory of trauma; however, no baseline measures were takenin this study.8 Similarly, Ide et al26 reported a significant dif-ference in theRowe score after exercisewith a scapula orthosisfor the subsections of pain, numbness, and stability (P< .001).
For all remaining outcomes presented in theGRADE table,lack of data and lack of statistical analysis meant thatP valuesfor within-group comparisons could not be reported.
The outcomes of the Subjective Shoulder Rating Sys-tem,32 the Rowe score in 2 studies,32,48 and the Constantscore in 1 study48 were not presented in the final GRADEtable because data for these outcomes were presented ascomparisons with a surgery group, after intervention only.No within-group comparisons or judgments on the per-centage of patients who had a favorable result after exercisealone could be made.
The grade of evidence was very low for all outcomesinvestigated for before-and-after comparisons of exercisefor MDI.
Poor results of exerciseTwo of the seven included studies reported poor outcomesafter exercise.37,48 One study reported a low satisfaction
Table II Characteristics of included studies
Study Study design Participants Diagnostic criteria forMDI
Exercise intervention Outcome measures Follow-up
Tillander et al48 Retrospective cohortExercise comparedwith ICS surgery
Used mirrors, PNF,biofeedback, closedkinetic chain, staminatraining, and homeexercisesNo frequency, dosage,or duration reported
Before interventionNone
After interventionRowe scoreConstant scoreAge- and gender-
adjusted ConstantscoreSubjective Shoulder
Rating SystemPatient satisfaction
(1, cured; 2, better; 3,same; 4, worse)
3.7 y (1-10 y)
Illy�es et al27 Controlled before-and-after study
3 groupsExercise: 34 MDI
Diagnostic criteria notclearly stated
Overview of programwith no description
Before interventionConstant score
6-12 wk, 24-51 wk
(continued on next page)
Exercise-based
managem
entforMDI
133
Table II (continued )
Study Study design Participants Diagnostic criteria forMDI
Exercise intervention Outcome measures Follow-up
Exercise comparedwith ICS surgery andthen exercise
shouldersSurgery and then
exercise: 31 MDIshouldersControls: 25 healthy
participants
Sulcus testApprehension testsNo imagingUnsure if Hx of traumaincluded
of type of exercises,phases, frequency,or dosage
Authors mention that ahome program wasimplementedProgram concentratedon proprioception,relearning correctmovement patterns,and developingstrength andendurance of scapulaand humeral musclesClosed and open chainexercises usedMirrors andbiofeedback used
Maximum amplitudeof EMG
Time broadness (%of movement cycle)After intervention
Constant scoreMaximum amplitude
of EMGTime broadness (%
of movement cycle)
Kiss et al33 Controlled before-and-after study
Exercise comparedwith ICS surgery andthen exercise
3 groupsExercise: 32 MDI
shouldersSurgery and then
exercise: 19 MDIshouldersControl: 25 healthy
participants
Criteria of diagnosisclearly stated
Symptomaticinstability in �2directionsNo Hx of traumaApprehension andsulcus signImaging to excludestructural lesion
Overview of programwith no descriptionon type of exercises,phases, frequency,or dosage
Authors mention that ahome program wasimplementedProgram concentratedon proprioception,relearning correctmovement patternsand developingstrength andendurance of scapulaand humeral musclesClosed and open chainexercises usedMirrors andbiofeedback used
Ide et al26 Prospective before-and-aftercomparison study
1 groupExercise: 46 MDI
patients (73
Physical examinationdescribed
All positive sulcus sign
2 phasesPhase 1: isometric
RTC/scapula
Before interventionModified Rowe scoreIsokinetic
8 wk for IR/ERstrength
7 y (5-9 y) for modified
134
S.A.Warb
yet
al.
No comparison group/intervention
shoulders) Anterior and posteriorapprehension testsNo Hx of traumaImaging to excludebony lesion
stabilizers, 8-s hold/2-s restPhase 2: Theraband
(The Hygenic Corp.,Akron, OH, USA) andwall p/upsdprogressiveresistance; daily inorthosis; duration of8 wk
dynamometerIR and ER
strengthER/IR ratio
After interventionModified Rowe scoreIsokinetic
dynamometerIR and ER
strengthER/IR ratio
Rowe score
Misamore et al37 Retrospective cohortNo comparison group
1 groupExercise: 64 MDI
shoulders
Diagnostic criteriaclearly outlined
At least grade 2translation, withreproduction ofpatient’s feeling ofinstability in �2directionsOnset must beatraumatic with noevidence of bonytrauma on imaging
Tillander et al48 Criteria not met) Criteria not met Criteria mety Criteria not met Criteria not met HighKiss et al32 Unclearz Unclear Criteria not met Criteria not met Unclear HighIlly�es et al27 Criteria not met Criteria met Criteria met Criteria not met Criteria not met HighKiss et al33 Criteria not met Criteria met Unclear Criteria met Unclear HighIde et al26 Criteria not met Unclear Criteria met Criteria met Unclear HighMisamore et al37 Criteria not met Criteria not met Criteria not met Criteria met Unclear HighBurkhead and
Rockwood8Unclear Criteria not met Criteria met Unclear Criteria not met High
Bias judgment for each sublevel of bias was based on quality assessment (Appendix D, available on the journal’s website at www.jshoulderelbow.org).
Adapted from Furlan et al.11 For the overall risk-of-bias judgment, a low risk of bias overall was defined when all types of biases were considered low risk, a
moderate risk of bias overall was defined when at least 1 bias was considered moderate risk and the others were low, and a high risk of bias overall was
defined when at least 1 bias was considered high risk and the others were low or moderate.) Criteria were not met (�50% of criteria ✗ or unclear [U] in quality assessment).y Criteria were met (�75% of sub-criteria met in quality assessment [U]).z It is unclear if criteria were met because of insufficient information (50%-75% of sub-criteria met [U] and the majority of others unsure unclear [U]
in quality assessment).
Exercise-based management for MDI 137
rate for its exercise-only group: 55% of patients were un-satisfied with treatment, and 44% of this group went on toundergo surgery.48 Another study investigating exercise in acohort of participants reported that 66% had a poor or fairoutcome with exercise or had been lost to surgical inter-vention at 2 years’ follow-up and 70% at 8 years’ follow-up.37
Discussion
For before-and-after comparisons of exercise-based man-agement for MDI, this review showed very low-qualityevidence for improvements in shoulder kinematics, TheRowe score, overall status rating, and peak muscle strength.The very low grade of evidence means that any estimate ofeffect is very uncertain.45
For most of the remaining outcomes, lack of data or onlypost-intervention comparisons with a surgery group meantthat the effects of exercise alone over time were almostimpossible to determine.
Downgrading of the evidence was primarily the result ofa high level of bias in the included studies, imprecise orsparse data, and of most relevance, indirect evidence inrelation to the uncertainty that interventions and outcomeswere the ones of interest.18
The most commonly recommended treatment for MDI isprimarily exercise-based management.2,5,15,35 Despite thisrecommendation, there is a lack of quality evidence tosupport one specific exercise regimen in preference toanother or to guide clinicians on the types of drills ordosages to use when treating MDI with exercise.32
Issues with included studies
The result of a very low grade of evidence for all outcomesdoes not necessarily mean that exercise for MDI has little
effect; it merely means that the studies investigating it areof very poor quality. All 7 studies reviewed scored a highrisk of bias in the quality assessment. Of primary concernwas the lack of pre-intervention outcome measures in 4 ofthe included studies.8,32,37,48 It is difficult to evaluatewhether post-intervention outcome measures are a truereflection of the effects of the intervention when there is alack of any baseline data for comparison.
Two studies in particular made evaluating the effectsof exercise alone for MDI challenging because of a lackof within-group comparisons and heterogeneous pop-ulation samples.32,48 Both studies only compared thepost-intervention data of an exercise group with the post-intervention data of a surgical group, drawing no conclu-sions on the effect of exercise alone over time. This meantthat evaluation of the evidence using the GRADE approachcould not be performed on a number of outcome measuresbecause the comparison of exercise versus surgery wasoutside the aims of this review.
In addition, heterogeneity in the sample of MDI partici-pants introduced a detrimental confounder to the results ofthese 2 studies because both included patients with a historyof trauma.32,48 Patients with a history of significant traumaare more likely to have a structural lesion and a predomi-nantly unidirectional pathology.10,34 The current literaturesupports that patients with a structural lesion have betteroutcomes after surgery when the integrity of the gleno-humeral capsuloligamentous complex is restored.6,8,10,34,35
Therefore, confidence in the conclusions of these studies isfurther reduced by this confounding variable.
The choice of outcome measures used across all of theincluded studies was either impairment-only outcomes oroutcomes that were not specific to measuring changes in theinstability population, which confounds the study findings.Two studies used impairment-only measures, such asscapulothoracic and glenohumeral joint angles and jointsliding mechanics, reporting significant improvements in
Time broadness: slow throw (1)Illy�es et al27 Low –2, very serious) NAy –1, indirectnessz –1, imprecisionx 34 NAk P ¼ .24 NAk Very low
Time broadness: fast throw (1)Illy�es et al27 Low –2, very serious) NAy –1, indirectnessz –1, imprecisionx 34 NAk P ¼ .19 NAk Very low
Scapulothoracic angle (1)Kiss et al33 Low –2, very serious) NAy –1, indirectnessz –1, imprecisionx 32 NAk P < .05{ NAk Very low
Glenohumeral angle (1)Kiss et al33 Low –2, very serious) NAy –1, indirectnessz –1, imprecisionx 32 NAk P < .05{ NAk Very low
Relative displacement (1)Kiss et al33 Low –2, very serious) NAy –1, indirectnessz –1, imprecisionx 32 NAk P < .05{ NAk Very low
IR mean peak torque (1)Ide et al26 Very low –2, very serious) NAy –1, indirectness# –1, imprecisionx 46 Nil P < .05{ NA)) Very low
ER mean peak torque (1)Ide et al26 Very low –2, very serious) NAy –1, indirectness# –1, imprecisionx 46 Nil P < .05{ NA)) Very low
ER/IR peak torque (1)Ide et al26 Very low –2, very serious) NAy –1, indirectness# –1, imprecisionx 46 Nil P < .05{ NA)) Very low
CI, confidence interval; NA, not applicable; QA, quality assessment .
Numbers placed in columns under the GRADE domains represent the number of quality points deducted for that domain assessed. Appendix C (available on the journal’s website at www.jshoulderelbow.org)
provides more details on grading domains.) Two quality points were deducted for trials with a very serious level of bias.11,22
y The domain was considered not applicable if there was only 1 trial intervention per outcome.11
z One quality point was deducted if the outcome measures investigated were not patient specific and were impairment based rather than activity based or patient related.18
x One quality point was deducted if only 1 trial reported an outcome for the chosen comparison regardless of the sample size or the confidence interval.12
k The studies did compare a group of exercise-based management with surgical intervention where effect sizes could be calculated for some outcomes. However, comparison of the effect sizes for exercise
versus surgery were outside the aims of this review.{ The results represent a favorable statistically significant difference after exercise intervention based on a P value of less than .05.# One quality point was deducted if most of the interventions for that outcome were not tested against a control or comparison group.7,18
)) The studies investigated the outcomes of 1 exercise group only before and after intervention; therefore, true effect sizes could not be calculated because there was no comparison group.
Rowe score (3)Misamore et al37 57 Nil -Burkhead andRockwood8
33 NA for review) -
Ide et al26 Very low –2, very seriousy NAz –1, indirectnessx –1, imprecisionjj 46 Nil < .001{ NA# Very lowConstant score (2)Kiss et al32 34 NA)) -Illy�es et al27 Very low –2, very seriousy NAz –1, indirectnessyy –1, imprecisionjj 62 NA/A)) - NA/A)) Very low
Satisfaction score (2)Tillander et al48 20 NA)) -Kiss et al32 Low –2, very seriousy NAz –1, indirectnessyy –1, imprecisionk 62 NA/A)) - NA/A)) Very low
Limitations on ADLs (1)Misamore et al37 Very low –2, very seriousy NAzz –1, indirectnessx –1, imprecisionxx 57-59 Nil - NA# Very low
Pain and instabilitygrading scale (1)Misamore et al37 Very low –2, very seriousy NAzz –1, indirectnessx –1, imprecisionxx 57-59 Nil - NA# Very low
Overall status rating (1)Misamore et al37 Very low –2, very seriousy NAzz –1, indirectnessx –1, imprecisionxx 57-59 Nil - NA# Very low
Time to become stable (1)Burkhead andRockwood8
Low –2, very seriousy NAzz No indirectness –1, imprecisionxx 33 NA for review) - NA forreview)
Very low
Back to sport/no returnto sport (1)Tillander et al48 Low –2, very seriousy NAzz –1, indirectnessyy –1, imprecisionxx 11 NA/A)) - NA/A)) Very low
ADLs, activities of daily living; CI, confidence interval.
A hyphen indicates that no P value was reported for results after exercise measures compared with pre-exercise measures. Numbers placed in columns under the GRADE domains represent the number of
quality points deducted for that domain assessed. Appendix C (available on the journal’s website at www.jshoulderelbow.org) provides more details on grading domains.) The article by Burkhead and Rockwood8 did compare the effect of exercise-based management in a group of participants with MDI against other groups. However, the other groups did not have MDI;
rather, they had unidirectional instability or voluntary instability, which is not of interest for this review.y Two quality points were deducted for trials with a very serious level of bias.11,22
z The domain was not considered applicable if most of the trials could not provide data to calculate confidence intervals and thus between-group or within-group treatment effects.x One quality point was deducted if most of the interventions for that outcome were not tested against a control or comparison group.7,18
k One quality point was deducted if fewer than 75% of studies presented data that could be included in a meta-analyses12 or most of the studies could not provide data to calculate confidence intervals
and effect sizes.{ The results represent a favorable statistically significant difference after exercise intervention based on a P value of less than .05.# The studies investigated the outcomes of 1 exercise group only before and after intervention; therefore, true effect sizes could not be calculated because there was no comparison group.)) The studies did compare a group of exercise-based management with surgical intervention where effect sizes could be calculated for some outcomes. However, comparison of the effect sizes for
exercise versus surgery were outside the aims of this review.yy One quality point was deducted if the interventions across studies were deemed significantly heterogeneous and/or sufficient information was lacking regarding description of the interventions and,
therefore, directness in relation to interventions could not be assessed.18
zz The domain was considered not applicable if there was only 1 trial intervention per outcome.11
xx One quality point was deducted if only 1 trial reported an outcome for the chosen comparison regardless of the sample size or the confidence interval.12
these outcomes after long-term exercise.27,33 Yet, it is un-known if the significant findings correlate with meaningfuldifferences for the participants because no functional,instability-specific outcome measures were used. Incontrast, in the studies that did use patient-focused outcomemeasures, the Constant score and/or the Rowe score wasused, and these scores are not specific or sensitive tomeasuring change in the instability population.43
The large variation in follow-up times makes comparisonsof studies difficult. Outcome measures across studies weretaken from 8 weeks after intervention to a range of 5 to9 years. Only 1 study mentioned measuring the compliancelevel of participants during the program,37 and it was unclearin all of the studies whether participants were instructed tocontinue following a maintenance program or in fact wereadhering to such a program. This is a large potentialconfounder of the results of exercise therapy, wherecompliance is a key component of favorable outcomes.9
Poor reporting of the interventions across most of thestudies is also a major confounding factor that reducesconfidence in the results of the included studies. All studiesexcept one failed to report all exercise parameters for theirinterventions.8 Most of the studies vaguely described sub-categories of their interventions, such as ‘‘rotator cuff ex-ercises, scapula stabilizing exercises and proprioceptionexercises,’’ but did not describe the type of drills the pa-tients performed, the amount of resistance used, and thefrequency of the program. This is an issue for a number ofreasons. First, exercise prescription is very specific,39 andwithout information on the parameters of the intervention,we cannot be certain if they were appropriate for optimumstrength gains and functional outcomes for these patients.Second, it would be almost impossible to replicate theprogram for most of these studies; thus, their externalvalidity is essentially redundant. Third, and of primaryimportance to this review’s main objective, is that becauseof the lack of intervention reporting, homogeneity of theexercise programs must be assumed. Evaluation of the trueeffect of standardized exercises programs for MDI is thusextremely difficult because of the likely variety in the de-livery, structure, execution, and therefore outcomes for thispopulation.
Determining the true benefits of exercise for MDI isdifficult because of the poor quality of included studies andthe very low-quality evidence for outcomes. Exercise doesappear to have some benefit for participants with MDIbecause most of the studies reported improvements in out-comes after exercise. However, an estimation of the trueeffect of exercise for MDI would be more conclusivelydetermined through a randomized controlled trial comparingone exercise-based management program with another.
Of the two studies that reported poor outcomes with exer-cise, one included some participants with a history of trauma48
and the other performed no baseline assessments or statisticaltests for patients’ exercise outcomes and had a high level ofdropout to surgery for reasons that were unclear.37
Limitations of review
Aside from not being able to conduct a meta-analysis, alimitation of this review was that the reviewers had toexpand the standard GRADE criteria with their own addi-tional criteria for evaluating the quality of evidence, whichhas the potential to introduce author bias. However, thiswas deemed necessary because the poor quality of theincluded NRS could not be evaluated alone using thestandard GRADE criteria. Expansion of the criteria wasperformed in consultation with all reviewers, with advicefrom a GRADE working group methodologist,14 and withclose reference to current GRADE guidelines.16-22
Conclusion
This review showed that there is large heterogeneityamong studies of very poor quality for the effects ofexercise for MDI. Exercise appears beneficial for pa-tients with nontraumatic MDI; however, its true effectsare difficult to evaluate because of literature fraught withhigh levels of bias. Exercise protocols are poorly definedin the literature, making evaluation of their true effectschallenging. There is a fundamental need for high-quality intervention studies to be undertaken to in-vestigate the effect of exercise-based management onfunctional and specific outcomes of patients with clini-cally diagnosed, nontraumatic MDI.
Disclaimer
The authors, their immediate families, and any researchfoundations with which they are affiliated have notreceived any financial payments or other benefits fromany commercial entity related to the subject of this article.
Supplementary data
Supplementary data related to this article can be foundonline at http://dx.doi.org/10.1016/j.jse.2013.08.006.
References
1. An YH, Friedman RJ. Multidirectional instability of the glenohumeral
joint. Orthop Clin North Am 2000;31:275-83.
2. Bahu MJ, Trentacosta N, Vorys GC, Covey AS, Ahmad CS. Multi-
directional instability: evaluation and treatment options. Clin Sports
Med 2008;27:671-89. http://dx.doi.org/10.1016/j.csm.2008.07.002
3. Baker CL III, Mascarenhas R, Kline AJ, Chhabra A, Pombo MW,
Bradley JP. Arthroscopic treatment of multidirectional shoulder
instability in athletes: a retrospective analysis of 2- to 5-year clinical