The Effect of Pregnancy on the Murmurs of Mitral and Aortic Regurgitation By FRANK I. MARCUS, M.D., GORDON A. Ewy, M.D., ROBERT A. O'RouRKE, M.D., BERNARD WALSH, M.D., AND ALLAN C. BLEICH, M.D. SUMMARY The effect of pregnancy on the intensity of murmurs of aortic and mitral re- gurgitation has not been reported previously. Twenty-five women with these mur- murs, singly or in combination, were examined when pregnant as well as when not pregnant. During pregnancy the murmur of aortic regurgitation decreased in intensity or became inaudible in 10 patients, remained unchanged in four, and increased in one. The murmur of mitral regurgitation decreased in intensity or became inaudible in eight patients, became shorter in duration in two, was un- changed in three, and became louder in one. Three of the patients who did not show a decrease in intensity of the mitral or aortic regurgitation murmur and the patient whose murmurs increased during pregnancy had the appearance or persistence of systemic hypertension during pregnancy. Phenylephrine consistently increased the loudness of the murmurs, usually to the level present in the nonpregnant state. The diminished intensity of these murmurs may be related to the decrease in peripheral resistance known to occur during pregnancy. It is apparent that (1) aortic regurgitation or mitral regurgitation may be missed during pregnancy, since these murmurs may become inaudible, and (2) the severity of these cardiac lesions may be underestimated clinically because of a decrease in intensity of these murmurs during pregnancy. It is important to determine the existence of valvular heart disease, since endocarditis is a hazard during parturition, and prophylactic antibiotic therapy should be given to these patients. Additional Indexing Words: Hypertension Rheumatic heart disease Phenylephrine Tricuspid insufficiency Rheumatic fever T HE EFFECT of pregnancy on the intensity of the murmurs of mitral and aortic regurgitation has not been reported. It would be anticipated that these murmurs From the University of Arizona College of Medicine, Tucson, Arizona, Georgetown University Medical Division, District of Columbia General Hospital, and the Obstetrical Cardiac Clinic, Wash- ington, D. C., and Grady Memorial Hospital, Emory University, Atlanta, Georgia. Address for reprints: Dr. Frank I. Marcus, Cardiology Division, Department of Intemal Medi- cine, University of Arizona College of Medicine, Tucson, Arizona 85721. Received December 1, 1969; revision accepted for publication January 12, 1970. Circulation, Volume XLI, May 1970 would become less intense during pregnancy, since the degree of mitral and aortic regurgita- tion is directly dependent upon systemic blood pressure and peripheral resistance,'l and these parameters decrease during pregnan- cy.4-8 Methods Over a 5-year period, 25 women with either mitral or aortic regurgitation, or both, were examined during pregnancy and either before pregnancy or after delivery. Nine patients had aortic regurgitation alone, three had aortic regurgitation and mitral regurgitation, and nine had mitral regurgitation alone. During pregnancy, three of the 25 patients (J. B., S. H., and W. S.) had the murmur of mitral stenosis in addition to aortic regurgitation or mitral regurgitation, and 795 by guest on May 19, 2018 http://circ.ahajournals.org/ Downloaded from
Transcript
The Effect of Pregnancy on the Murmurs of
Mitral and Aortic RegurgitationBy FRANK I. MARCUS, M.D., GORDON A. Ewy, M.D.,ROBERT A. O'RouRKE, M.D., BERNARD WALSH, M.D.,
AND ALLAN C. BLEICH, M.D.
SUMMARYThe effect of pregnancy on the intensity of murmurs of aortic and mitral re-
gurgitation has not been reported previously. Twenty-five women with these mur-
murs, singly or in combination, were examined when pregnant as well as whennot pregnant. During pregnancy the murmur of aortic regurgitation decreased inintensity or became inaudible in 10 patients, remained unchanged in four, andincreased in one. The murmur of mitral regurgitation decreased in intensity or
became inaudible in eight patients, became shorter in duration in two, was un-
changed in three, and became louder in one. Three of the patients who did not showa decrease in intensity of the mitral or aortic regurgitation murmur and the patientwhose murmurs increased during pregnancy had the appearance or persistence ofsystemic hypertension during pregnancy. Phenylephrine consistently increased theloudness of the murmurs, usually to the level present in the nonpregnant state.The diminished intensity of these murmurs may be related to the decrease inperipheral resistance known to occur during pregnancy. It is apparent that (1)aortic regurgitation or mitral regurgitation may be missed during pregnancy, sincethese murmurs may become inaudible, and (2) the severity of these cardiaclesions may be underestimated clinically because of a decrease in intensity of thesemurmurs during pregnancy. It is important to determine the existence of valvularheart disease, since endocarditis is a hazard during parturition, and prophylacticantibiotic therapy should be given to these patients.
T HE EFFECT of pregnancy on theintensity of the murmurs of mitral and
aortic regurgitation has not been reported. Itwould be anticipated that these murmurs
From the University of Arizona College ofMedicine, Tucson, Arizona, Georgetown UniversityMedical Division, District of Columbia GeneralHospital, and the Obstetrical Cardiac Clinic, Wash-ington, D. C., and Grady Memorial Hospital, EmoryUniversity, Atlanta, Georgia.
Address for reprints: Dr. Frank I. Marcus,Cardiology Division, Department of Intemal Medi-cine, University of Arizona College of Medicine,Tucson, Arizona 85721.
Received December 1, 1969; revision accepted forpublication January 12, 1970.
Circulation, Volume XLI, May 1970
would become less intense during pregnancy,since the degree of mitral and aortic regurgita-tion is directly dependent upon systemic bloodpressure and peripheral resistance,'l andthese parameters decrease during pregnan-cy.4-8
MethodsOver a 5-year period, 25 women with either
mitral or aortic regurgitation, or both, wereexamined during pregnancy and either beforepregnancy or after delivery. Nine patients hadaortic regurgitation alone, three had aorticregurgitation and mitral regurgitation, and ninehad mitral regurgitation alone. During pregnancy,three of the 25 patients (J. B., S. H., and W. S.)had the murmur of mitral stenosis in addition toaortic regurgitation or mitral regurgitation, and
The Effect of Pregnancy on the Murmur of Aortic Regurgitation
Pregestation exam Exam during gestationAge Blood Pulse Blood Pulse
during pressure (beats/ Murmur pressure (beats/ MurmurPatient pregnancy Mo (mm Hg) min) (grade) Mo (mm Hg) min) (grade)
Patients in whom the murmer decreased during pregnancy32 - - - - 8th 110/6018 1 120/82 80 I/VI 7th 116/8032 12 130/80 80 II/VI 3rd
5th7th
7th9th
18 12 - - II-III/VI 7th
26 6 200/120 - I/VI 2nd
23 - - - - 9th
24 - - - - 7th
19 - - - - 5th
21 12 130/70 84 I-II/VI Monthly2nd thru9th
36 6 140/84 90 II/VI 6th
115
88
130/60-40 120
0
0
0
I/VI100/55-50 100
110/60 -
140/70 -
120/70 -
120/80 -
100/60 -
100-110/50
I/VI00
0
0
- I/VI (3-6 mo)- 0 (7-9 mo)
100/60 0
Patients in whom the murmur did not decrease during pregnancy- - - - 7th 85/65
- 9th38 - - - - 9th
115/75
140/90
It/VII/VI
II/VI
26 24 120/95 78 I-II /VI 8th
17 2 120/80 - II/VI 3rd9th
*Patients who had additional murmurs but not mitral insufficiency.tPatients who also had mitral insufficiency. See table 2.tThis patient had murmurs of aortic, mitral, and tricuspid insufficiency, as well as mitral stenosis.
one patient (M. L.) had murmurs consistent withaortic and mitral regurgitation, mitral stenosis,and tricuspid regurgitation.
The majority of patients were referred forcardiac evaluation during pregnancy because of
the presence of rheumatic heart disease or a pasthistory of rheumatic fever. They were all seen inoutpatient clinics. The selection of patients wasbased on the presence of the murmur of mitral oraortic regurgitation during pregnancy or when
Patients in whom the murmur decreased during pregnancy- - - - 1 140/80 - III/VI No
- - -- 2 120/80 80 I-II/VI Yes
- - - - (1 day) 130/60-40+ 1 mo
- - - - (1 day) 110/60+ 1 mo 100/60-50
- - - - 4 110/60
90
6480
II/VI No Ejection click persisted eventhouigh the murmur disap-peared.
II/VIII/VI
Murmur could not be heard dur-ing pregnancy when patientwas in supine position, but itwas easily heard in this positionafter delivery.
- II/VI ?
9th 150/1007th 145/1007th 130/80
- II/VI 1 130/100
- I/VI
- I/VI
1 130/90
1 120/80
- - - - (1 wk) 130/80
- _ _ - 2i2 130/84
- I/VI Yes
- I/VI Yes
- II/VI Yes
- II/VI Yes Murmur started to decrease inintensity by 5th month. Ejec-tion click persisted during preg-nancy.
- II/VI Yes
Patients in whom the murmur did not decrease during pregnancy- _ - - 1 110/70 - II/VI No
- - - - 1 120/80- - - - 1 135/90
- - - - (2 wk) 110/60
- I/VI ?- II/VI ? Blood pressure higher during
pregnancy.
- I-II/VI Yes Right heart catheterization andangiogram 2 years before preg-nancy because configuration ofmurmur suggested pulmonaryinsufficiency. Unable to def-initely confirm pulmonary in-sufficiency by catheterization.
- - 2 144/92 - II/VI Yes Murmur increased from II/VIto III/VI with onset of hyper-tension during pregnancy.
not pregnant. In addition, patients were includedonly if they were examined by the same physicianduring pregnancy and when not pregnant.Otherwise, all patients with these murmurs wereincluded. The high incidence of patients withaortic regurgitation, unusual in women withrheumatic valvular disease, may be explained bythe possibility that these patients were referredCirculation, Volume XLI, May 1970
once our interest in the behavior of thesemurmurs during pregnancy become known tophysicians.
These patients did not have hemodynamicallysevere regurgitation. This evaluation was basedon the observations that none of the patients hada history of heart failure prior to or duringpregnancy, that only one patient had a murmur
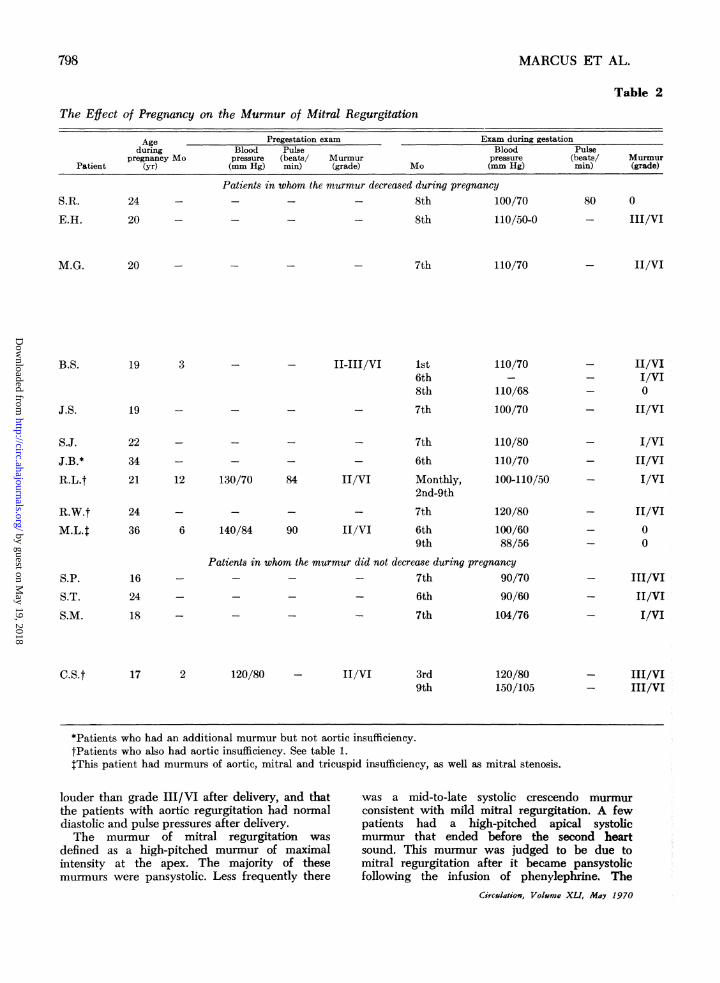
The Efect of Pregnancy on the Murmur of Mitral Regurgitation
Age Pregestation exam Exam during gestationduring Blood Pulse Blood Pulse
pregnancy Mo pressure (beats/ Murmur pressure (beats/ MurmurPatient (yr) (mm Hg) min) (grade) Mo (mm Hg) min) (grade)
S.R. 24
E.H. 20 -
Patients in whom the murmur decreased during pregnancy- - - 8th 1C
- - - 8th ll
00/70
10/50-0
80 0
- III/VI
20 - - - 7th 110/70 - II/VI
B.S. 19 3
J.S.
- - II-III/VI 1st6th8th
19 - _ - 7th
110/70
110/68
100/70
- II/VI- I/VI- 0
- II/VI
S.J. 22 - - -
J.B.* 34 - - _
- 7th- 6th
21 12 130/70 84 II/VI
24
Monthly,2nd-9th
- 7th
36 6 140/84 90 II/VI
16
24
6th9th
110/80110/70
100-110/50
120/80100/6088/56
Patients in whom the murmur did not decrease during pregnancy- - - - 7th 90/70
18 - - -
- 6th- 7th
90/60104/76
- I/VI- II/VI- I/VI
- II/VI_ 0
_ 0
- III/VI- II/VI- I/VI
17 2 120/80 - II/VI 3rd9th
120/80150/105
- III/VI- III/VI
*Patients who had an additional murmur but not aortic insufficiency.tPatients who also had aortic insufficiency. See table 1.tThis patient had murmurs of aortic, mitral and tricuspid insufficiency, as well as mitral stenosis.
louder than grade III/VI after delivery, and thatthe patients with aortic regurgitation had normaldiastolic and pulse pressures after delivery.The murmur of mitral regurgitation was
defined as a high-pitched murmur of maximalintensity at the apex. The majority of thesemurmurs were pansystolic. Less frequently there
was a mid-to-late systolic crescendo murmurconsistent with mild mitral regurgitation. A fewpatients had a high-pitched apical systolicmurmur that ended before the second heartsound. This murmur was judged to be due tomitral regurgitation after it became pansystolicfollowing the infusion of phenylephrine. The
Patients in whom the murmur decreased during pregnancy- - - - 4 110/60 70 II/VI Yes
1 120/60
- 130/80 - II/VI 1 125/80
- IV/VI Yes A thrill was felt post partum butwas not palpable during preg-
nancy.
- II/VI Yes During pregnancy the apicalmurmur was not holosystolicand was not diagnostic ofmitral regurgitation. Afterphenylephrine and postpar-tum, the murmur becameholosystolic.
- - - No Murmur was II/VI at lst mo;I/VI at 6 mo, and not heardat all in 8th mo.
7th 130/85 - II/VI 1 110/70
- - - - 1 120/80- 130/80
7th 145/100
- III/VI 1 125/80
- - (1 week) 130/80
- III/VI 1 130/90- - 212 130/84
- II/VI No (Same comment as for M.G.above)
- II-III/VI No
- III/VI No
- II/VI Yes Murmur decreased in intensityby the 5th mo.
- III/VI Yes
- II/VI Yes
Patients in whom the murmur did not decrease during pregnancy
- - - - 1 130/80 -
- - - - 1 110/70 -
- - - - 1 120/80 80
- - - - 2 144/92 -
III/VI Yes
II/VI ?
I/VI Yes The murmur was late systolicand was introduced by a
mid-systolic click during andafter pregnancy.
II/VI Yes Murmur increased from II/VIto III/VI with the onset ofhypertension during preg-
nancy.
murmur of aortic regurgitation was defined as ahigh-pitched murmur occurring early in diastole.The murmur was heard best at the left sternalborder. The intensity of the murmurs was gradedon the basis of I to VI.9 Patients were examinedwhile both in the supine and the sitting positionsfor the murmur of aortic regurgitation, and in theleft lateral position for the murmur of mitralregurgitation. At each examination, auscultationwas performed before the physician looked at thepatient's record where his previous findings hadCsrculation, Volume XLI, May 1970
been recorded.Phenylephrine, 0.25 mg, was injected intra-
venously in seven women during pregnancy.* If
*Phenylephrine was given to other pregnant womensuspected of having aortic or mitral regurgitation, butmurmurs indicative of these lesions were not elicitedduring the test. Post partum, these murmurs were notheard; therefore, these patients were not included inthis report.
this dose did not raise the systolic pressure by 15to 20 mm Hg in 2 to 3 min, 0.5 mg was thengiven. The induced hypertension usually caused adecrease in heart rate of 10 to 20 beats/min.
ResultsThe effect of pregnancy on the murmur of
aortic regurgitation is presented in table 1.The murmur was not heard during pregnancyin eight of 15 patients with aortic regurgita-tion. When these same patients were notpregnant, a grade I to III/VI high-pitcheddiastolic murmur was heard. The murmur ofaortic regurgitation decreased in intensity inone patient and became audible late inpregnancy in another. The murmur wasunchanged in four patients, one of whom washypertensive during pregnancy. The murmurincreased in intensity in one patient (C.S.),who had an increase in blood pressurebetween the third and the ninth month ofpregnancy corresponding with the increase inloudness of the murmur. Patient M.T. mayhave had pulmonic regurgitation. In thispatient there was a clearly discernible intervalbetween the second sound and the onset ofthe murmur. This uncertainty existed evenafter right heart catheterization, pulmonaryangiography, and intracardiac phonocardiog-raphy.
Phenylephrine was given to three patientssuspected or known to have aortic regurgita-tion, but in whom the murmur of aorticregurgitation was not heard at the time of thetest. An audible murmur consistent with aorticregurgitation was elicited in all three patientsafter the phenylephrine was given (table1).The effect of pregnancy on the murmur of
mitral regurgitation is presented in table 2.Fourteen patients had this murmur beforepregnancy or after delivery. During pregnan-cy this murmur was inaudible or becamesofter in eight patients, became shorter induration in two (M.G. and J.S.), wasunchanged in three, and increased in onepatient. The diagnosis of mitral regurgitationwas aided by the injection of phenylephrine inpatients M.G. and J.S., since its administra-tion resulted in a lengthening of the murmur
to that of a typical pansystolic murmur. Afterdelivery, these two patients had pansystolicmurmurs.
Miscellaneous ObservationsTwo patients, L.L. and R.L., with aortic
regurgitation had a prominent ejection click.In both patients the murmur could not beheard during some part of pregnancy. How-ever, the ejection click persisted and wasunchanged in intensity during pregnancy.Three patients, J.B., W.S., and M.L., hadapical diastolic rumbling murmur heard onlyduring pregnancy. This finding was inter-preted as indicating the presence of mitralstenosis. None of these subjects was thoughtto have sufficient mitral regurgitation toaccount for the presence of a diastolic "flow"murmur or sufficient aortic regurgitation tohave an associated Austin Flint murmur.
M.L. had tricuspid regurgitation. This diag-nosis was based on the finding of a systolicmurmur heard best at the lower left sternalborder. Before pregnancy this murmur wasgrade I/VI and increased to grade II/VI withinspiration and also with amyl nitrite inhala-tion. During pregnancy it was grade II/VIduring expiration, and increased to gradeIV/VI during inspiration. In pregnancy themurmur had a "whooping" sound duringinspiration.
Time Course of the Change in Intensity ofAortic and Mitral RegurgitationMurmurs with PregnancyThree patients were examined on several
occasions during pregnancy. L.L. had a gradeII/VI murmur of aortic insufficiency beforepregnancy. She was examined when 3 monthspregnant. The murmur of aortic regurgitationcould not be heard, nor could an aorticinsufficiency murmur be detected in the fifthand seventh months. A grade II/VI diastolicblowing murmur was heard on the firstpostpartum day. In R.L. the murmur of aorticregurgitation started to decrease in intensityby the fifth month and was inaudible duringthe sixth and ninth months. A similar timecourse was present in this patient with regardto the decrease in the murmur of mitral
regurgitation. In patient B.S., the murmur ofmitral regurgitation was unchanged duringthe first month of pregnancy, was decreased atthe sixth month, and could not be heard at allduring the eighth month.
DiscussionIt is clear from these observations, extend-
ing over 5 years, that the murmurs of mildaortic and mitral regurgitation will generallybecome softer or even inaudible duringpregnancy (tables 1 and 2). Attempts weremade to document these findings by phono-cardiography; however, the majority of thesemurmurs were not only of high frequency, butwere soft. The combination of low amplitudeand high frequency required amplificationsufficient to produce a wavering base line.Therefore, the records were usually unsatisfac-tory. Nonetheless, these observations arethought to be valid for the following reasons:The study was prospective, and each patientwas examined during pregnancy and eitherbefore or after pregnancy by the samephysician. The element of bias cannot beexcluded from these observations since grad-ing of murmurs is subjective. Certain nota-tions made during this study were helpful inverifying the validity of the change in themurmur during pregnancy. For example, itwas noted during the second pregnancy ofpatient L.L. that the murmur of aorticregurgitation was not heard when the patientwas supine but was heard only when thepatient was in the upright position. Postpartum, it was readily heard when the patientwas supine. In patient E.H. an apical systolicthrill was present post partum but was not feltduring pregnancy. In 11 patients the murmurof aortic or mitral regurgitation could not beheard at all during pregnancy but was heardbefore or after pregnancy. In six of thesepatients the murmur was of grade II/VI orIII/VI when the patient was not pregnant. Itis unlikely that these murmurs would havebeen missed. During the course of the study itwas considered possible that the murmurs ofaortic and mitral regurgitation did not changein intensity but rather were altered in locationCirculation, Volume XLI, May 1970
of maximum intensity because of a morehorizontal position of the heart. This hypothe-sis could not be verified by auscultation of theentire precordium in many patients. Also,phenylephrine infusion during pregnancy in-creased the intensity of the murmurs, at whichtime they were heard best at the anticipatedlocation. Finally, spontaneous variations in theintensity of the murmur, unassociated withpregnancy, could not be excluded as anexplanation for the change in murmurs duringpregnancy. The consistency of change inintensity correlated with pregnancy is againstthis possibility. Serial examinations on thesame patients such as L.L., who was examinedbefore and after two pregnancies, also servedto exclude spontaneous variations in themurmurs.The reasons for the decrease in the intensity
of the murmurs of aortic and mitral regurgita-tion during pregnancy may be related to thediminution in systemic vascular resistanceaccompanying pregnancy. The hemodynamicalterations occurring during pregnancy thatappear to be pertinent to this study may besummarized as follows.4-8 An increase incardiac output can be demonstrated by theeighth to the twelfth week of pregnancy.Cardiac output continues to rise until the 24thto 28th week. Thereafter, traditionally, it hasbeen taught that the cardiac output declinesin the third trimester. However, this is basedupon data gathered during measurements inthe supine position. Recently, Lees andassociates6 and Kerr'0 documented that theincrease in cardiac output is maintainedduring the latter part of the second andthroughout the third trimester. They measuredcardiac output with the subjects in the lateral,as well as in the supine positions, anddetermined that the decrease in cardiacoutput observed in the supine position in thelatter part of pregnancy is due to decreasedvenous return caused by partial vena cavalcompression by the fetus. There is generalagreement that systemic vascular resistancedecreases during the first and second trimes-ters, since the mean blood pressure is un-changed or decreased despite the increase in
cardiac output. Sites of low vascular resistanceinclude the placenta, the kidney, skin, andprobably the breasts.5 If we accept theobservation that cardiac output is maintainedat or near peak level until delivery, thesystemic vascular resistance must also contin-ue low, since the mean arterial blood pressure
does not rise during the latter part ofpregnancy.
It has long been appreciated that themurmurs of aortic and mitral regurgitationcan be altered by change in systemic arterialresistance. These murmurs will become louderfollowing injection of vasopressor agents such
as phenylephrine or methoxamine"l-13 and willdiminish in intensity after inhalation of a
vasodilating drug such as amyl nitrite'3-18 or
the administration of a ganglionic blockingagent. 9 The change in intensity of thesemurmurs directly reflects changes in thevolume of mitral or aortic regurgitation.Wiggers and Maltby' found that an increasein peripheral resistance caused an increase inthe volume of aortic regurgitation in experi-mental animals. Rodbard and Williams,20using an artificial model, and Braunwald andco-workers,2 using dogs, confirmed the obser-vations of Wiggers and Feil2' that an increasein systemic vascular resistance increased theamount of mitral regurgitation. Increase in thedegree of mitral regurgitation due to an
augmentation of systemic vascular resistanceinduced by methoxamine has been docu-mented in patients.3 Therefore, the decreasein intensity of the murmurs of aortic andmitral regurgitation may be explained on thebasis of the decreased systemic vascularresistance during pregnancy.
Some patients whose murmurs of aortic or
mitral regurgitation did not decrease duringpregnancy had the onset or exacerbation ofhypertension to account for the lack of changein these murmurs. In others, the reason for thelack of alteration of murmur with pregnancy
is not clear. Jose and associates3 noted thatmethoxamine did not cause an increase inmitral regurgitation in patients thought tohave fixed or rigid valves. Whether thisobservation is pertinent to the lack of change
of the mitral regurgitation murmur in thisseries is not known. The few observationsregarding the effect of pregnancy on murmursother than those of aortic and mitral regurgi-tation serve only to suggest that the murmursof mitral stenosis and tricuspid regurgitationmay increase during pregnancy as they dowith inhalation of amyl nitrite. The persis-tence of the ejection click in two patients whohad murmurs of aortic regurgitation onlywhen not pregnant suggests that this sign maybe the only clue to the presence of aorticregurgitation in some pregnant patients withthis lesion.These observations have both diagnostic
and therapeutic significance. It is taught that"organic heart disease may usually be ex-cluded in the absence of a diastolic murmur,unequivocal cardiomegaly, a systolic murmurmore than grade II in intensity, and severearrhythmia."22 The present study indicatesthat organic heart disease must be suspectedduring pregnancy when there is a history ofrheumatic fever or rheumatic heart disease,even in the absence of the murmur of aortic ormitral regurgitation. Under these circum-stances, particular attention must be given toprevious examinations before pregnancy. Thisstudy also suggests the importance of examin-ing a patient post partum before stating thatthe patient has no auscultatory evidence ofheart disease. If the physician wishes todetermine the presence of aortic or mitralregurgitation during pregnancy, he may injectphenylephrine intravenously and listen im-mediately following infusion for these mur-murs. Phenylephrine seems to be innocuous tothe fetus. Vasoactive drugs, including phenyl-ephrine, do not appear to cross the placenta indogs or in sheep.23 24 Systemic hypertension isa relative contraindication to the use of thisdrug.The murmurs of aortic and mitral regurgita-
tion may be accentuated during squatting.25The effect of this maneuver is to increase thesystemic blood pressure.26
It is important to diagnose valvular diseaseduring pregnancy, because of the hazard ofsubacute bacterial endocarditis occurring at
the time of delivery.27-0 If valvular heartdisease is present or if there is a history of anorganic murmur prior to pregnancy, thephysician should prescribe antibiotic prophy-laxis at the time of delivery and for severaldays thereafter.31 The diagnosis of subacutebacterial endocarditis or rheumatic fever maybe suspected in women found to have the"appearance" of the murmur of mitral oraortic regurgitation after pregnancy (see caseW.P.). Under these circumstances, the possi-bility should be considered and that the mur-mur disappeared or was missed during preg-nancy.The physician may underestimate the sever-
ity of the cardiac lesion if the patient is firstexamined during pregnancy, since one of theparameters for assessing the degree of mitraland aortic regurgitation is the intensity of themurmur.32 In surveys regarding the effect ofpregnancy on the course of rheumatic heartdisease, these observations must also be takeninto account. It is interesting to speculate thatone factor contributing to the favorable courseof pregnancy in patients with aortic or mitralregurgitation may be the actual decrease inthe degree of aortic or mitral regurgitationduring pregnancy. This decrease in valvularregurgitation may in part compensate for theincrease in the work of the left ventricle dueto the hemodynamic demands of pregnancy.The following two case reports are illustra-
tive of the problems encountered before it wasappreciated that the murmurs of aortic andmitral regurgitation may diminish duringpregnancy.
Report of Cases
Patient W.P.A 32-year-old female, gravida 7, para 6, was
seen during her eighth month of pregnancy. Atthat time she complained of vague discomfort ofher chest and cardiac consultation was requested.There was no history of rheumatic fever. Vitalsigns were as follows: The blood pressure was110/60 mm Hg, and the pulse rate was 115/minand regular. The left ventricular impulse wasdisplaced laterally and was more forceful thananticipated, even in pregnancy. The patient wasexamined by two cardiologists, neither of whomcould hear a murmur suggestive of valvular heartCirculation, Volume XLI, May 1970
disease. There was voltage criteria for leftventricular hypertrophy by electrocardiogram. A6-foot PA roentgenogram of the chest showedmild cardiomegaly. In the absence of heartmurmurs and the presence of cardiac enlarge-ment, primary myocardial disease was thought tobe present. The patient was seen 9 days prior todelivery, and again, no murmurs were heard. Onthis occasion blood pressure was 110/70 andpulse rate was 120/min. Delivery was uneventfuland without complications.
Because of the findings of cardiomegaly andtachycardia, the patient was seen 3 weeks afterdelivery. At that time, her blood pressure was140/80. A grade III/VI diastolic blowing murmurwas heard. Because this murmur had not beenheard previously, there was concern that she mayhave had a recent episode of acute rheumaticfever. Other possibilities included dissection ofthe aorta or endocarditis. She was hospitalized forfurther investigation. On admission, a bloodpressure of 130/80 was recorded. Her pulse ratewas 80/min and regular. She was afebrile. Thejugular venous pulse and carotid pulse were ofnormal contour. The left ventricular apicalimpulse was in the fifth intercostal space at themidclavicular line. The first heart sound was notaccentuated. A grade III/VI systolic ejectionmurmur was present along the left sternal border,and a high-frequency diastolic blowing murmurof grade III/VI was heard along the left sternalborder. Six blood cultures were negative. Sheremained afebrile. Her antistreptolysin (ASO)titer, C-reactive protein, CBC, sedimentation rate,LE cell preparation, and serum electrophoresiswere all within normal limits. There was noevidence of enlargement of the ascending aortaby chest roentgenogram. Since there was noevidence to substantiate a diagnosis of acuterheumatic fever, aortic dissection, or endocarditis,the possibility was considered that the murmur ofaortic regurgitation was not present duringpregnancy because of the hypotension andtachycardia then present. To simulate thesedynamic changes, auscultation was performedbefore and during the inhalation of amyl nitrite.The reflex tachycardia increased the pulse ratefrom 96 to 120. Amyl nitrate inhalation decreasedthe intensity of the diastolic murmur. Rheumaticfever prophylaxis was instituted. Although therewas no history of rheumatic fever, this was themost likely etiology of the murmurs.
Patient S.R.This 24-year-old woman was referred to the
Cardiac Clinic of Georgetown University MedicalDivision for evaluation of possible heart disease.She had a history of dyspnea on exertion of 2months' duration. She had had rheumatic fever at
the ages of 12 and 19 years, although she was nottold of the presence of any heart disease at thetime of rheumatic fever.On examination she had a blood pressure of
110/70 mm Hg; her pulse was 80 and regular.There was no evidence of cardiomegaly byexamination. The first heart sound was split, thesecond heart sound was single, and a grade IIejection murmur was heard at the second leftinterspace. Neither an apical systolic nor an aorticdiastolic murmur was heard. She was thought notto have valvular heart disease. Antibiotic prophy-laxis during delivery was not prescribed. Deliverywas uneventful. She was seen 4 months afterpregnancy. In the interim, she felt well and didnot have symptoms of rheumatic fever. The onlydifference in cardiac examination, performed bythe same physician, was the presence of a gradeII/VI pansystolic murmur at the apex whichradiated to the axilla. No diastolic blowingmurmur was heard.
AcknowledgmentThe authors wish to thank Mr. Clyde A. Baker,
Chief, Medical Illustration Service, Veterans Admin-istration Hospital, Tucson, Arizona, for his assistancein preparing the tables, and Mrs. Elizabeth Baconand Mrs. Judy Huber for secretarial assistance.
References1. WIGGERS CJ, MALTBY AB: Further observations
on experimental aortic insufficiency: IV.Hemodynamic factors determining the charac-teristic changes in aortic and ventricularpressure pulses. Amer J Physiol 97: 689,1931
2. BRAUNWALD E, WELCH GH JR, SARNOFF SJ:Hemodynamic effects of quantitatively variedexperimental mitral regurgitation. CirculationResearch 5: 539, 1957
3. JOSE AD, TAYLOR RR, BERNSTEIN L: Theinfluence of arterial pressure on mitral incom-petence in man. J Clin Invest 43: 2094,1964
4. BADER ME, BADER RA: Cardiovascular hemody-namics in pregnancy and labor. Clin ObstetGynec 11: 924, 1968
18. BECK W, SCHIIRE V, VOGELPOEL L, ET AL:Hemodynamic effects of amyl nitrite andphenylephrine on the normal human circula-tion and their relation to changes in cardiacmurmurs. Amer J Cardiol 8: 341, 1961
19. PARTNOPE E, HARVEY WP, Quoted by LEONARIJJ, ALLENSWORTH E: Differential diagnosis ofthe early diastolic murmur. In Theory andPractice of Auscultation, edited by Segal BL.Philadelphia, F. A. Davis Co., 1964, p 487
20. RODBARD S, WILLIAMS F: The dynamics ofmitral insufficiency. Amer Heart J 48: 521,1954
22. BURWELL CS, METCALFE J: Heart Disease andPregnancy: Physiology and Management. Bos-ton, Little, Brown & Co., 1958, p 55
23. LINKIE DM, BOBA A, PLOTZ EJ: Fetal effects ofphenylephrine injection. Amer J Med Sci 252:277, 1966
24. ADAMS FH, ASSALI N, CUSHMAN M, ET AL:Interrelationships of maternal and fetal circula-tions: I. Flow-pressure responses to vaso-activedrugs in sheep. Pediatrics 27: 627, 1961
25. VOGELPOEL L, NELLEN M, BECK W, ET AL: Thevalue of squatting in the diagnosis of mild
26. NELLEN M, GOTSMAN MS, VOGELPOEL L, ET AL:Effects of prompt squatting on the systolicmurmur in idiopathic hypertrophic obstructivecardiomyopathy. Brit Med J 3: 140, 1967
27. LEIN JN, STANDER RW: Subacute bacterialendocarditis following obstetric and gynecolog-ical procedures. Obstet Gynec 13: 568, 1959
32. SCHRIRE V: The relation of the apical systolicmurmur to mitral valve disease. Amer Heart J68: 305, 1964
Bedside Medicine
Need for a Wider Horizon
.... The call for teaching at the bedside is old and there again is a demand toreplace most lectures by bedside instruction. As I told you, I was not addicted to formallectures myself but I have to point out that many aspects of clinical knowledge cannotbe taught at the bedside. Prevention of diseases, in my opinion the highest form ofmedicine, cannot be taught at the bedside because the protected persons are welland walking around. Prenatal diseases which can be so devastating to the unborn child,are another example. They cannot be taught at the bedside since neither the mothernor the embryo or fetus is in bed during the fateful days. At the bedside you can seea tiny sector of the area that must be known. But you have to learn to supplementthese quick glimpses by intensive studies of books or with other devices.-From WAR-KANY, JOSEF: Convocation Address at the opening of the 150th year of medical classesat the University of Cincinnati, September 29, 1969. Medical Alumnal Bulletin of theUniversity of Cincinnati 22: 1, Winter, 1969.
WALSH and ALLAN C. BLEICHFRANK I. MARCUS, GORDON A. EWY, ROBERT A. O'ROURKE, BERNARDThe Effect of Pregnancy on the Murmurs of Mitral and Aortic Regurgitation
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.41.5.795
1970;41:795-805Circulation.
http://circ.ahajournals.org/content/41/5/795located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions: