Page 1
The Emerging Role of
Mechanical Devices in Heart
Failure
Paul Mather, MD Advanced Heart Failure and Cardiac Transplant Center
Jefferson Medical College of Thomas Jefferson University
Philadelphia, PA | USA
Page 3
Learning Objectives:
Indications for implantable LVADs and exclusion
criteria
History of LVAD use
Management guidelines for LVADs
Complications of LVADs
Page 4
ADHF Treatment Dilemma
Most patients hospitalized for acutely
decompensated heart failure improve.
For those who DO NOT IMPROVE or
take a LONG TIME TO IMPROVE, does
one stay the course or is it time to
add-on to medical management?
Page 5
Questions to Consider
Have we reached a neurohormonal plateau in
the management of the end-stage heart failure
patient?
Are we looking for a replacement device?(a surrogate
for a failing pump) or…
Are we looking for a device to negate the underlying
pathophysiologic processes, potentially interrupting
the neurohormonal cascade thereby reversing
ventricular remodeling and/or improving renal and
vascular function.
Page 6
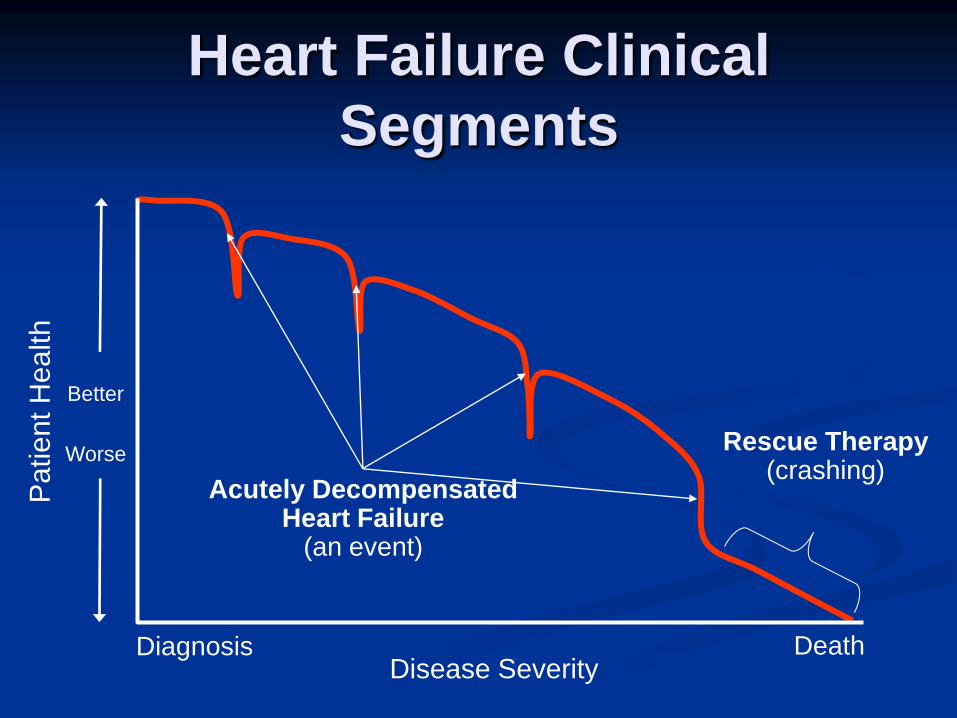
Heart Failure Clinical
Segments
Diagnosis Death
Rescue Therapy (crashing)
Patient H
ealth
Acutely Decompensated Heart Failure
(an event)
Disease Severity
Better
Worse
Page 7
Today’s Treatment Options C
ard
iac In
dex
Good
Poor
Mild Hypo-tension Severe Hypo-tension
ADVANCED
PHARMACOLOGIC
THERAPY
IV Diuretics
IV Inotropes
IV Vasodilators
Unmet need with current medical
and device therapies
Transplant & VAD
CARDIOGENIC SHOCK
Pumps & Assist Devices
THE GOAL: Turn-Around Disease
Progression
Page 8
NYHA Heart Failure Class
Mo
re
Invasiv
en
ess
L
ess
Cardiac Resynchronization Therapy (CRT)
VADs
Transplants
Another Way of Looking at It
Beta Blockers / ACE
Diuretics
Inotropes
Aldosterone blockade
Page 9
VADs:
Indications for Use
Salvage
Cardiogenic shock
Recurrent sustained Vtach or Vfib despite adequate pharmacologic treatment
Likely a scenario for ECMO
Bridge to Transplant
Patients with functional class III or IV CHF
Irreversible left heart failure with EF <25% with need for continuous inotropic support
Imminent risk of death
Page 10
VADs:
Indications for Use
Bridge to Transplant
Patients must prove to be candidate for cardiac transplantation
No significant end organ damage
Age appropriate
Socially acceptable
Family support
Refrains from drugs, tobacco and alcohol
Page 11
VADs
Indications for Use: Bridge to Recovery
Acute Myocarditis
Acute MI
Post cardiac surgery
Destination Therapy
— NYHA Class IIIB or IV heart failure
— Optimal medical therapy 45 of last 60 days
— Not candidate for cardiac transplantation due to age or co-morbidities
Page 12
Heart Transplant
The Dilemma:
Donor organ shortage: currently 3,100 people
in the US waiting for a heart transplant
2010: 1,934 heart transplants done in US
Wait can be long….
Page 13
ECMO for Cardiac Support Class: external,
continuous flow
Common use: short-term (adults); long-term (ped.)
Indications:
post-cardiotomy (adult&ped.)
rapidly deployed ACLS
Supported angioplasty
bridge to pulm. recovery
Limitations:
no LV decompression
heparin required
circuit changes
Page 14
Evolution of Continuous Flow
VADs Centrifugal pump
Debakey VAD
Heartmate II
Page 15
15
Benefits of a Rotary Device
Smaller size
60% Smaller than HeartMate I (XVE)
Smaller driveline
Ease of surgical implantation
― Standard sternotomy vs. extended midline excision
― Smaller preperitoneal pocket
Enhanced patient comfort
Silent, vibration-free operation
Designed for extended durability
Reduced infection risk
Page 16
Jarvik 2000 Heartmate II
Current Long term
Non-pulsatile Devices
-
Page 17
17
HeartMate II LVAD A surgically implanted, rotary
continuous-flow device in parallel with the native left ventricle Left ventricle to ascending aorta
Percutaneous driveline
Electrically powered Batteries & line power
Fixed speed operating mode 6,000-15,00 RPM
Flow range: 3 – 10 L/min
Home discharge
Page 21
(from: Texas Heart Inst. 2000)
Page 22
VAD Complications:
Peri-operative Infection
Ischemic Stroke
Pulmonary issues:
Prolonged ventilation
Pneumonia
Death
Hemolysis
Cannula malpositioning
Pump failure
Intracranial bleed
Page 23
Modification of Pre-operative
Risk Factors:
Malnutrition
Supplement oral intake with tube feeds if
necessary
RV dysfunction
Unload RV by ultrafiltration, pulmonary
vasculature vasodilation or inotropic support
Reverse coagulopathy
Vit K
FFP
Page 24
24
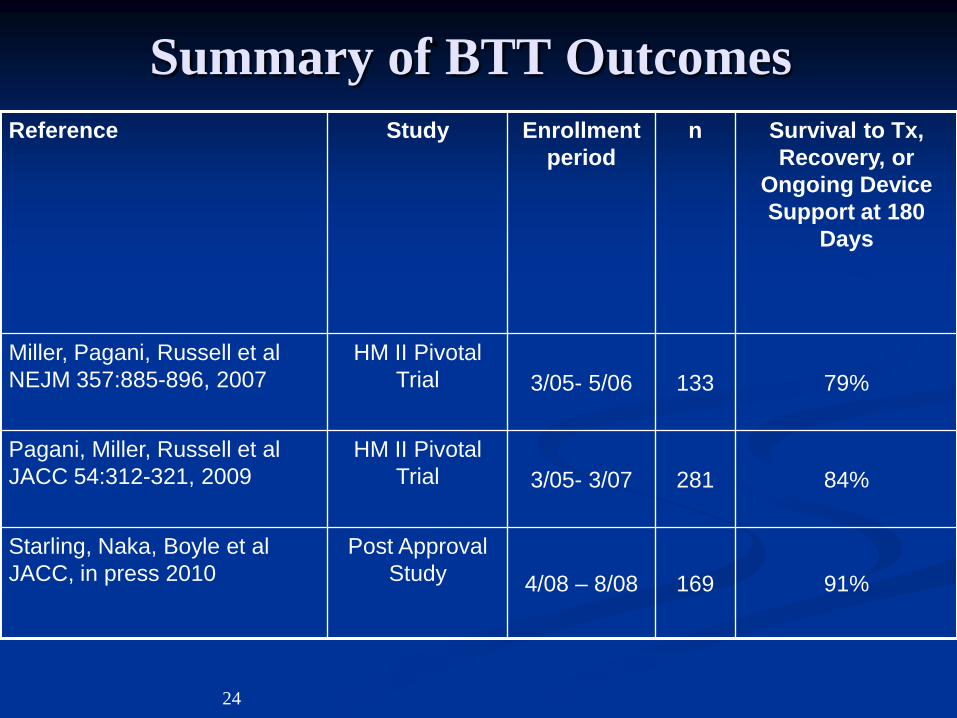
Summary of BTT Outcomes
Reference Study Enrollment
period
n Survival to Tx,
Recovery, or
Ongoing Device
Support at 180
Days
Miller, Pagani, Russell et al
NEJM 357:885-896, 2007
HM II Pivotal
Trial 3/05- 5/06 133 79%
Pagani, Miller, Russell et al
JACC 54:312-321, 2009
HM II Pivotal
Trial 3/05- 3/07 281 84%
Starling, Naka, Boyle et al
JACC, in press 2010
Post Approval
Study 4/08 – 8/08 169 91%
Page 25
25
BTT Actuarial Survival
Starling, Naka, Boyle JACC, in press 2010
Post Approval Study
90% 6-Month
Survival
85% 1-Year
Survival
Page 26
26
Study Outcomes
90% of patients were transplanted, recovered or had ongoing support at 6 months
Operative 30-day survival was 96%
Survival was superior to that which has been previously reported with LVAD usage
Page 27
27
Time (Months)
0 6 12 18 24
Pe
rce
nt
Su
rviv
al
0
10
20
30
40
50
60
70
80
90
100
Mid trial (N=281)
Early trial (N=133)
74 ± 3%
68 ± 4%
64 ± 3%
58 ± 4%
At Risk:
281133
21595
18882
16769
9462
P(log-rank) = 0.134P(adjusted for BSA) = 0.162
Average Support Duration
Early trial = 2.0 ± 1.6 years (longest: 5.5 years)
Mid trial = 1.5 ± 1.0 years (longest: 3.4 years)
Improvements in DT Survival
Park, S. presented at AHA 2010, Chicago
Early Trial vs Mid Trial
* P value adjusted for body surface
area
Page 28
28
Summary of DT Outcomes
Reference Study Enrollment
period
n One-Year
Survival
Two-Year
Survival
Slaughter, Rogers, Milano
et al N NEJM
2009;361:2241-51
HM II Pivotal Trial 3/05- 5/07 134 68% 58%
Park, S, presented at AHA
2010
HM II Pivotal Trial 5/07- 3/09 311 74% 64%
Page 29
29
Worldwide Clinical Experience*
Patients supported ≥ 1 year: 1810
Patients supported ≥ 2 years: 622
Patients supported ≥ 3 years: 209
Patients supported ≥ 4 years: 47
Patients supported ≥ 5 years: 11
Patients supported ≥ 6 years: 1
More than 5,000 patients worldwide have now
been implanted with the HeartMate II LVAS.
As of October 2010 *Based on clinical trial and device tracking data
Page 30
Conclusions:
VADs are currently used as bridges to recovery and
transplant, and as destination devices.
Preoperative optimization and early referral are the
keys to decreasing postoperative complications
Implantable VADs should not be placed in
emergent/salvage situations
Page 31
Conclusions:
Outpatient follow up of mechanical assist
patients requires a solid institutional
infrastructure.
Future assist devices will aim to decrease
complications and increase durability
There is no PERFECT device YET