The Epidemiology of The Epidemiology of Alcohol Use, Abuse and Alcohol Use, Abuse and Dependence Dependence Deborah Hasin, Ph.D. Deborah Hasin, Ph.D. Columbia University Columbia University New York State Psychiatric Institute New York State Psychiatric Institute
Transcript
The Epidemiology of Alcohol Use, The Epidemiology of Alcohol Use, Abuse and DependenceAbuse and Dependence
Deborah Hasin, Ph.D.Deborah Hasin, Ph.D.Columbia UniversityColumbia University
New York State Psychiatric InstituteNew York State Psychiatric Institute
What is Epidemiology?What is Epidemiology?
Descriptive epidemiologyDescriptive epidemiology: The distribution of health : The distribution of health conditions and diseases in populationsconditions and diseases in populations– Purposes: to identify time trends, groups at special risk, need for Purposes: to identify time trends, groups at special risk, need for
policies and servicespolicies and services
PrevalencePrevalence: : Proportion of cases in a total populationProportion of cases in a total population
IncidenceIncidence: : Proportion of new cases developing in a specific time Proportion of new cases developing in a specific time among those without the disease at the outsetamong those without the disease at the outset
Analytic epidemiologyAnalytic epidemiology: Investigation of potential causes/risk : Investigation of potential causes/risk factors (genetic variants, contextual circumstances) of illness, factors (genetic variants, contextual circumstances) of illness, often done through:often done through:– Retrospective comparison of cases to non-casesRetrospective comparison of cases to non-cases
– Prospective study of disease developmentProspective study of disease development
First things first: not all drinking is badFirst things first: not all drinking is bad
Reasons for drinking include Reasons for drinking include enhanced sociability, enhanced sociability, enjoyment, festivitiesenjoyment, festivities
In many countries, drinking In many countries, drinking alcohol is normative alcohol is normative
Light to moderate drinking is Light to moderate drinking is protective against protective against cardiovascular disease and cardiovascular disease and mortalitymortality
Alcohol in excess – Alcohol in excess – a major public health problema major public health problem
Excess alcohol consumption Excess alcohol consumption 33rdrd largest largest cause of U.S. cause of U.S. preventable mortalitypreventable mortality (Mokdad et al., 2000)(Mokdad et al., 2000)
Excess alcohol consumption Excess alcohol consumption 55thth largest largest cause of cause of preventable disability worldwidepreventable disability worldwide ((EzzatiEzzati et al., 2002) et al., 2002)
Excess alcohol consumption and alcohol use disorders Excess alcohol consumption and alcohol use disorders aassociated with:ssociated with:
Accidents, traffic fatalities, domestic violenceAccidents, traffic fatalities, domestic violenceFetal Alcohol SyndromeFetal Alcohol SyndromeNeuropsychological impairment Neuropsychological impairment Poor medication adherence, e.g., HIVPoor medication adherence, e.g., HIVEconomic costs and lost productivityEconomic costs and lost productivityPsychiatric comorbidity, functional disabilityPsychiatric comorbidity, functional disability
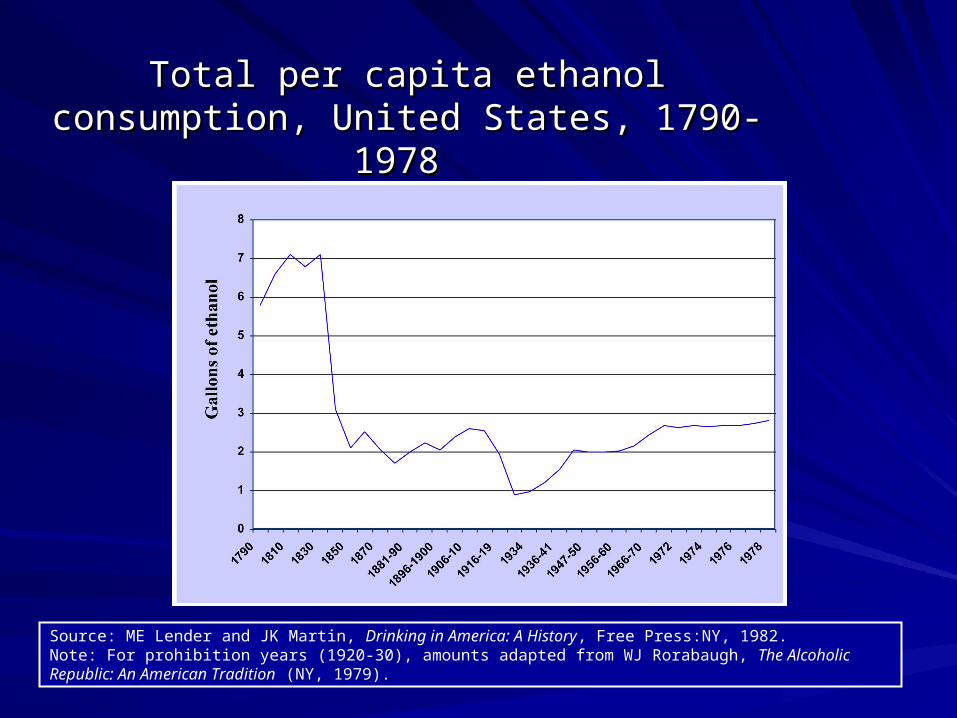
Total per capita ethanol consumption, United Total per capita ethanol consumption, United States, 1790-1978 States, 1790-1978
Source: ME Lender and JK Martin, Drinking in America: A History, Free Press:NY, 1982.Note: For prohibition years (1920-30), amounts adapted from WJ Rorabaugh, The Alcoholic Republic: An American Tradition (NY, 1979).
Total per capita ethanol consumption, United Total per capita ethanol consumption, United
States, 1935–2005States, 1935–2005
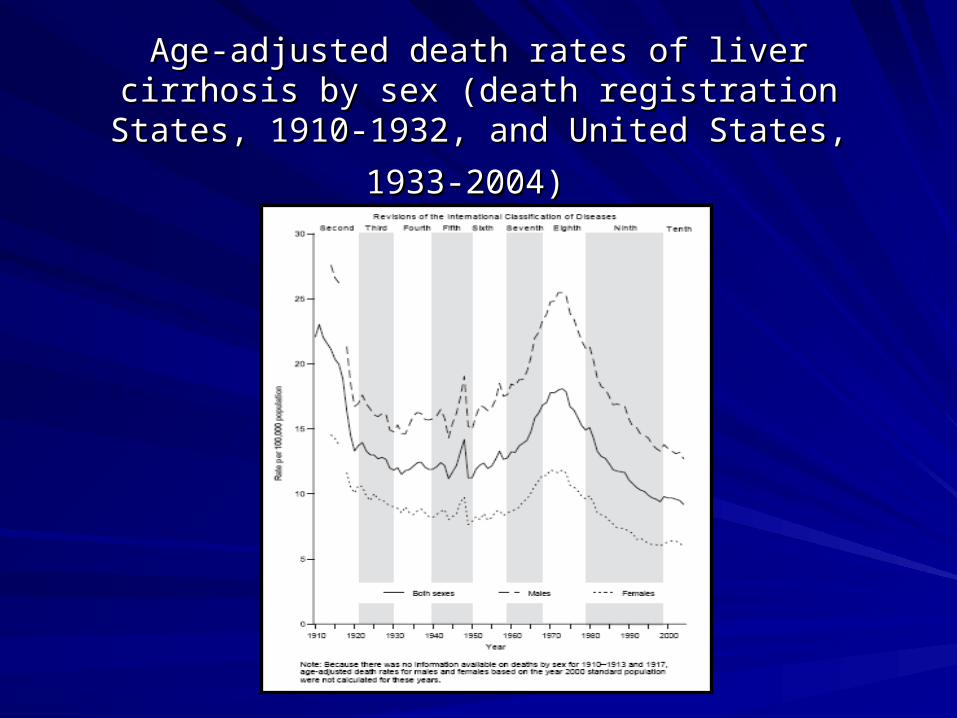
Age-adjusted death rates of liver cirrhosis by sex Age-adjusted death rates of liver cirrhosis by sex (death registration States, 1910-1932, and United (death registration States, 1910-1932, and United
States, 1933-2004)States, 1933-2004)
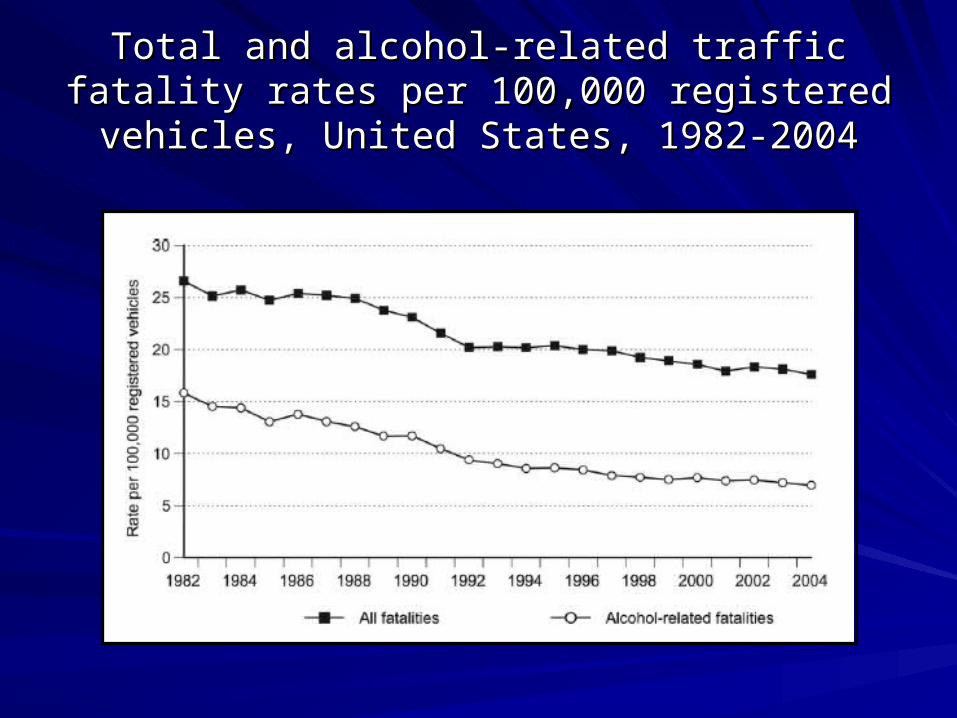
Total and alcohol-related traffic fatality rates per Total and alcohol-related traffic fatality rates per 100,000 registered vehicles, United States, 1982-100,000 registered vehicles, United States, 1982-
20042004
Monitoring the Future (MTF) study Monitoring the Future (MTF) study Drunk (past 30 days) Drunk (past 30 days)
and disapprove of heavy drinkingand disapprove of heavy drinking
Image Removed – Awaiting Copyright Permissions
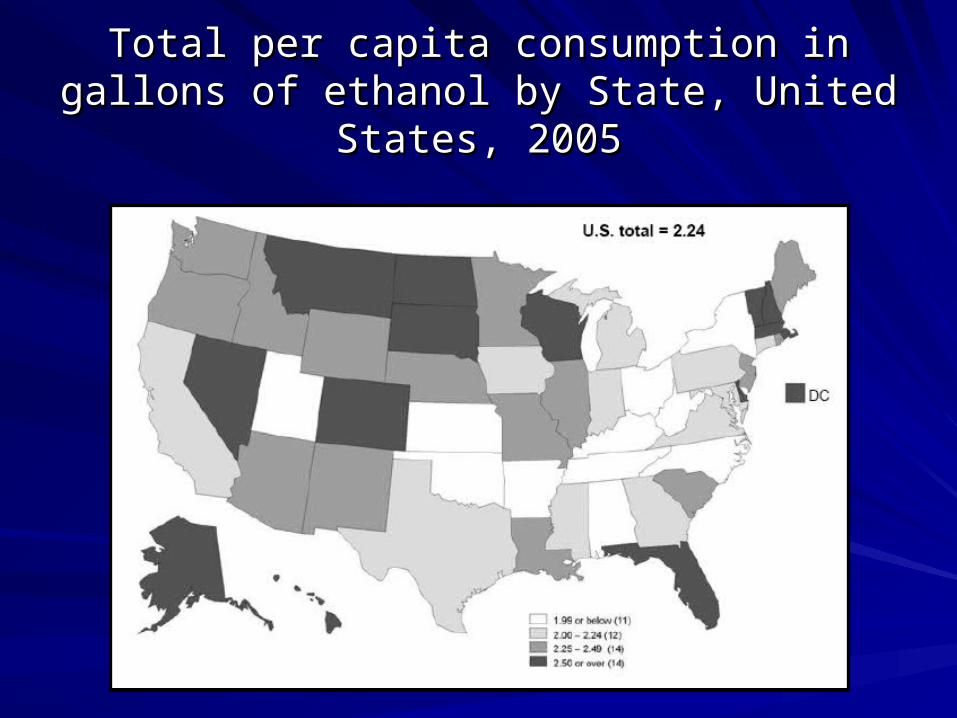
Total per capita consumption in gallons of Total per capita consumption in gallons of ethanol by State, United States, 2005ethanol by State, United States, 2005
Total Alcohol Consumption by Country, 2002Total Alcohol Consumption by Country, 2002High-consumption countries (WHO)High-consumption countries (WHO)
RankRank CountryCountry Litres pure alcoholLitres pure alcohol22 UgandaUganda 18.5718.57
Total Alcohol Consumption by Country, 2002Total Alcohol Consumption by Country, 2002Intermediate-consumption countries (WHO)Intermediate-consumption countries (WHO)
RankRank CountryCountry Litres pure alcoholLitres pure alcohol4848 JapanJapan 9.69.6
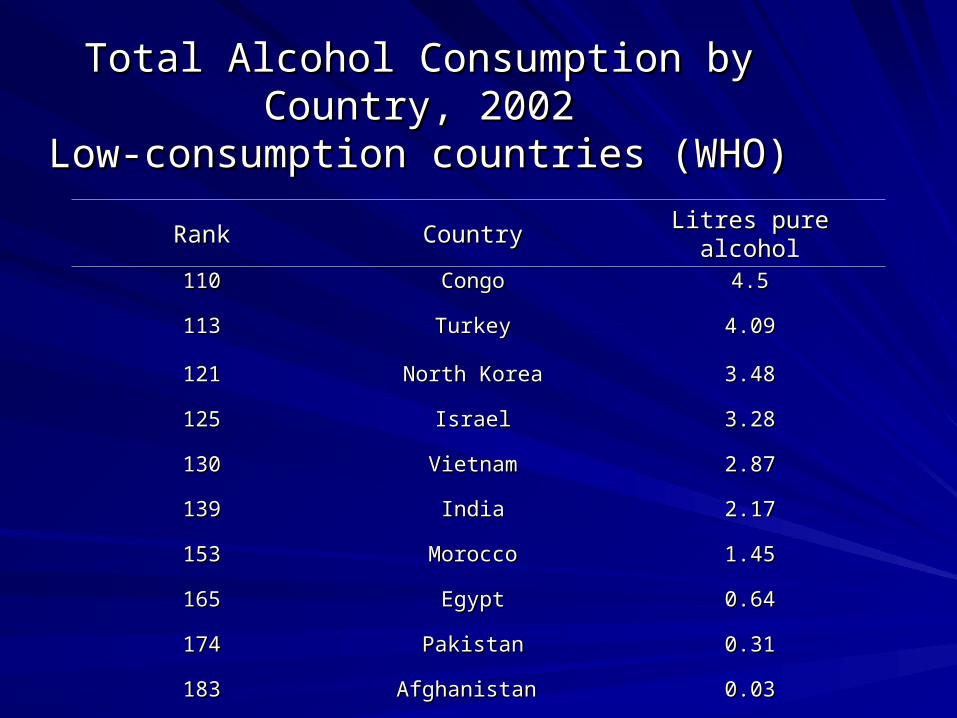
Total Alcohol Consumption by Country, 2002Total Alcohol Consumption by Country, 2002Low-consumption countries (WHO)Low-consumption countries (WHO)
RankRank CountryCountry Litres pure alcoholLitres pure alcohol110110 CongoCongo 4.54.5
113113 TurkeyTurkey 4.094.09
121121 North KoreaNorth Korea 3.483.48
125125 IsraelIsrael 3.283.28
130130 VietnamVietnam 2.872.87
139139 IndiaIndia 2.172.17
153153 MoroccoMorocco 1.451.45
165165 EgyptEgypt 0.640.64
174174 PakistanPakistan 0.310.31
183183 Afghanistan Afghanistan 0.030.03
Wave of attacks on Iraqi alcohol sellers
Shops selling alcohol have become targets in a wave of attacks. BBC World News, July 22, 2004
Substance Availability Can Change
Substance availability throughout the world can change rapidly, as a result of changes in government regulation, taxation, confiscation, wars, religious conflicts, marketing efforts, etc.
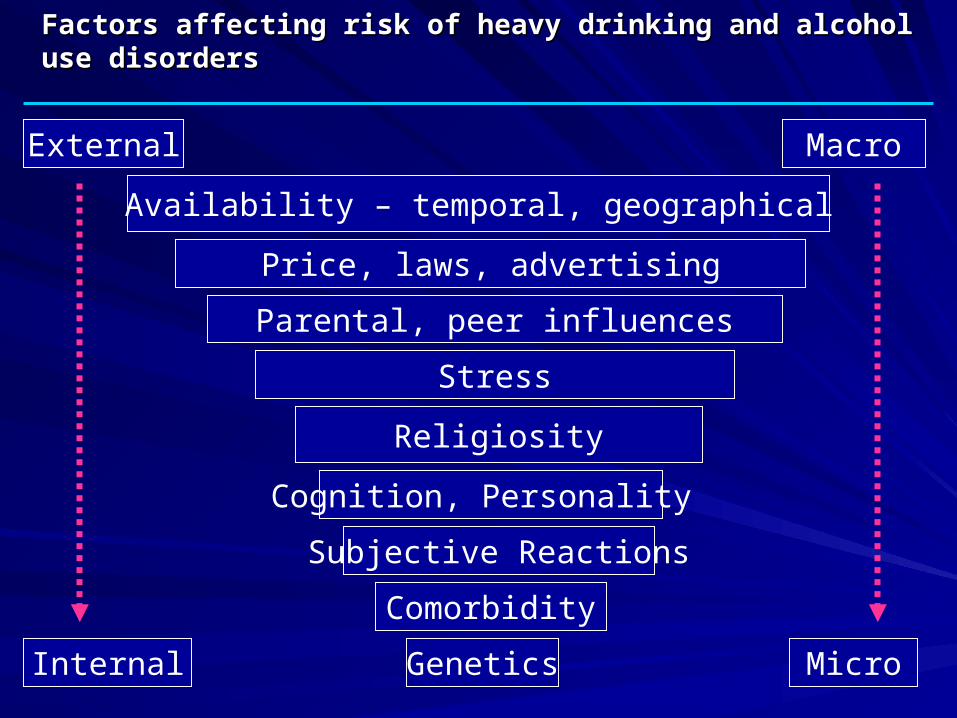
Factors affecting risk of heavy drinking and alcohol use disordersFactors affecting risk of heavy drinking and alcohol use disorders
Availability – temporal, geographical
Price, laws, advertising
Parental, peer influences
Stress
Religiosity
Cognition, Personality
Comorbidity
Genetics
External Macro
Internal Micro
Subjective Reactions
Measurement issues in alcohol consumptionMeasurement issues in alcohol consumption
Per capita consumption usually shows higher consumption Per capita consumption usually shows higher consumption than surveysthan surveysMany factors affect survey reports of alcohol, including Many factors affect survey reports of alcohol, including – ethanol content of different drinks ethanol content of different drinks
– amounts poured in different circumstances amounts poured in different circumstances
– time frame coveredtime frame covered
– Context of questions in the survey Context of questions in the survey
Survey methods do adequate job, but new methods under Survey methods do adequate job, but new methods under investigation to improve survey reports of alcohol consumption investigation to improve survey reports of alcohol consumption (Greenfield & Kerr,2008)(Greenfield & Kerr,2008)
MMaladaptive drinking leading to clinically significant aladaptive drinking leading to clinically significant impairment or distress, shown by 3+ of the following in impairment or distress, shown by 3+ of the following in the same 12-month periodthe same 12-month period::
1.1. Drinking more or longer than intendedDrinking more or longer than intended2.2. Persistent desire or unsuccessful efforts to cut down or Persistent desire or unsuccessful efforts to cut down or
stopstop3.3. A great deal of time spent on drinking or getting over its A great deal of time spent on drinking or getting over its
effectseffects4.4. Important activities given up or reduced because of Important activities given up or reduced because of
drinkingdrinking5.5. Continued drinking despite knowledge of a serious Continued drinking despite knowledge of a serious
physical or psychological problemphysical or psychological problem6.6. ToleranceTolerance7.7. Withdrawal, or drinking to avoid or relieve drinkingWithdrawal, or drinking to avoid or relieve drinking
Alcohol Dependence SyndromeAlcohol Dependence Syndrome(Edwards and Gross, 1976)(Edwards and Gross, 1976)
Dependence concept based on close Dependence concept based on close observation of patientsobservation of patients
The concept: a combination of physiological and The concept: a combination of physiological and psychological processespsychological processes
Dimensional rather than yes or noDimensional rather than yes or no
Bi-axial distinction of core alcohol dependence Bi-axial distinction of core alcohol dependence syndrome from its consequences the basis for syndrome from its consequences the basis for dependence/abuse dependence/abuse
DSM-IV Alcohol AbuseDSM-IV Alcohol Abuse
NNot dependent, ot dependent, and and maladaptive drinking leading to maladaptive drinking leading to clinically significant impairment or distress, shown by 1 clinically significant impairment or distress, shown by 1 + of the following+ of the following::
1.1. Continued use despite social/interpersonal problemsContinued use despite social/interpersonal problems
2.2. Hazardous use (e.g., driving when impaired by alcohol)Hazardous use (e.g., driving when impaired by alcohol)
3.3. Frequent drinking leading to failure to function in major Frequent drinking leading to failure to function in major rolesroles
4.4. Legal problemsLegal problems
National Epidemiologic Survey on Alcohol and National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) Wave 1: 2001-2002Related Conditions (NESARC) Wave 1: 2001-2002
National sampleNational sampleN= 43,093N= 43,093Response rate 81%Response rate 81%NIAAA & NIDA NIAAA & NIDA sponsoredsponsoredHousehold, group Household, group residentsresidentsOversamples Blacks, Oversamples Blacks, Hispanics, young Hispanics, young adults (18-24 yrs)adults (18-24 yrs)DSM-IV diagnosesDSM-IV diagnosesIn-person interviewsIn-person interviews
Alcohol Use Disorders and Associated Alcohol Use Disorders and Associated Disabilities Interview ScheduleDisabilities Interview Schedule (AUDADIS)(AUDADIS)
Grant et al., Ruan et al., Grant et al., Ruan et al., Drg Alch DepDrg Alch Dep 1995; 2003 2008 1995; 2003 2008
Fully structured, designed for lay interviewersFully structured, designed for lay interviewers
Coverage: Major Axis I disorders and all Axis II disordersCoverage: Major Axis I disorders and all Axis II disorders
Family history of alcohol, drug, antisocial and depressive disordersFamily history of alcohol, drug, antisocial and depressive disorders
Treatment utilizationTreatment utilization
Medical problemsMedical problems
Overall functioningOverall functioning
Early and adult stressful eventsEarly and adult stressful events
DiscriminationDiscrimination
Current and Lifetime Prevalence DSM-IV Alcohol Abuse and Dependence
Current Lifetime
Alcohol abuse 4.7 17.8
Alcohol dependence 3.8 12.5
Any alcohol disorder 8.5 30.3
Hazard Rates for Age at Onset of DSM-IV Alcohol Abuse and
Dependence
Image Removed – Awaiting Copyright Permissions
Average age at onset and durationAverage age at onset and duration
Alcohol AbuseAlcohol Abuse Onset: Onset: 22.5 years22.5 years
Duration: Duration: 32.9 months32.9 months
Alcohol DependenceAlcohol Dependence Onset: Onset: 21.9 years21.9 years
Duration: Duration: 44.1 months44.1 months
Number of lifetime episodesNumber of lifetime episodes
Most (72.0%) had Most (72.0%) had only oneonly one episode episode
Of those with >1 episode of Alcohol AbuseOf those with >1 episode of Alcohol Abuse
Mean number episodes 5.2Mean number episodes 5.2
Of those with >1 episode of Alcohol DependenceOf those with >1 episode of Alcohol Dependence
Mean number episodes 5.1Mean number episodes 5.1
Current DSM-IV Alcohol Use Disorders Current DSM-IV Alcohol Use Disorders by Genderby Gender
12.4
6.9
5.44.9
2.6 2.3
0
2
4
6
8
10
12
14
Any alcohol usedisorder
Alcohol abuse Alcohol dependence
Male
Female
Pre
vale
nce
(%
)
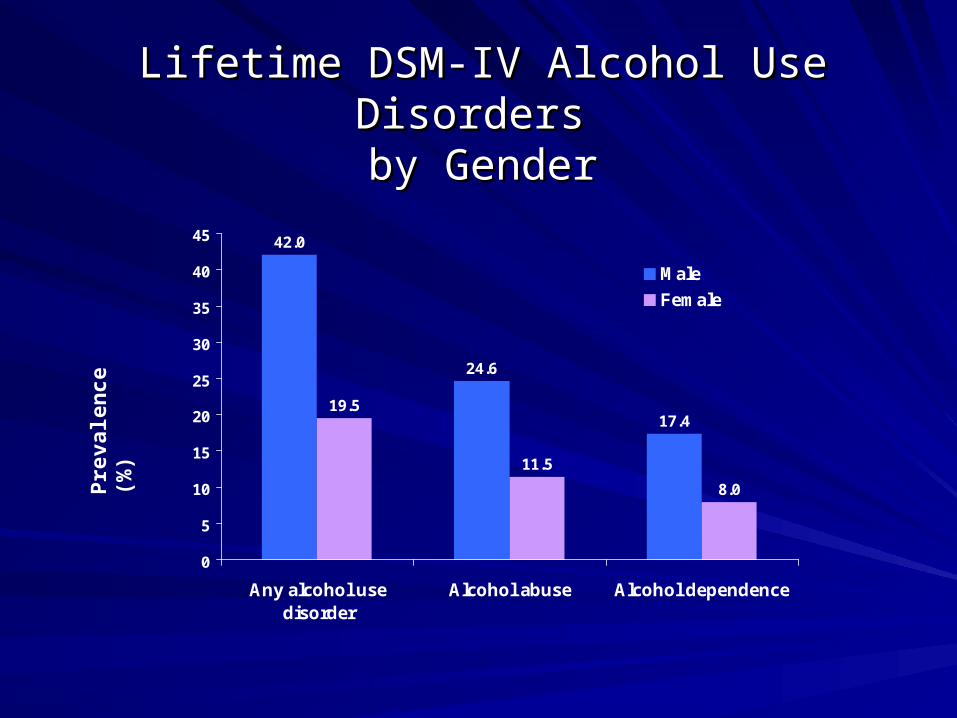
Lifetime DSM-IV Alcohol Use Disorders Lifetime DSM-IV Alcohol Use Disorders by Genderby Gender
42.0
24.6
17.419.5
11.5
8.0
0
5
10
15
20
25
30
35
40
45
Any alcohol usedisorder
Alcohol abuse Alcohol dependence
Male
Female
Pre
vale
nce
(%
)
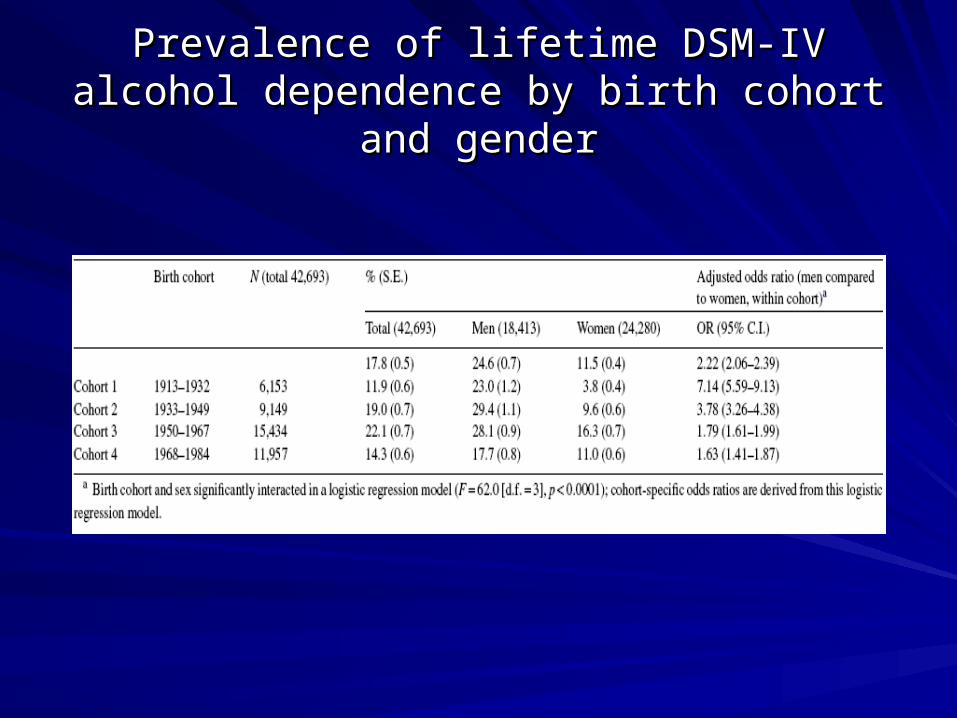
Prevalence of lifetime DSM-IV alcohol Prevalence of lifetime DSM-IV alcohol dependence by birth cohort and genderdependence by birth cohort and gender
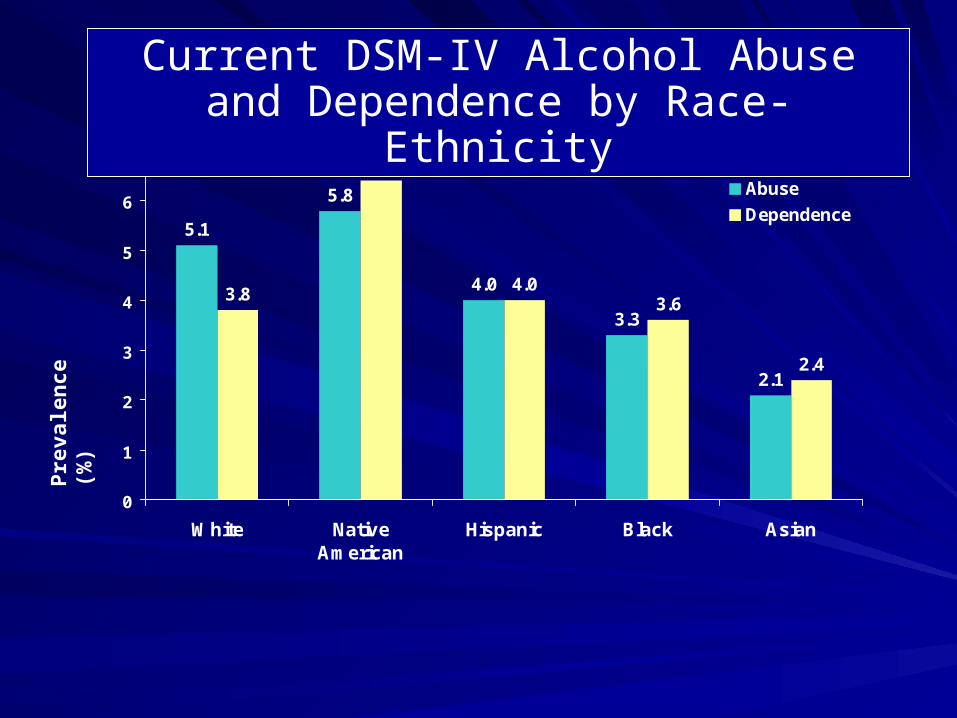
5.1
5.8
4.0
3.3
2.1
3.8
6.4
3.6
2.4
4.0
0
1
2
3
4
5
6
7
White NativeAmerican
Hispanic Black Asian
Abuse
Dependence
Current DSM-IV Alcohol Abuse and Dependence by Race-Ethnicity
Pre
vale
nce
(%
)
20.3
22.9
11.5 12.2
5.6
13.8
20.1
8.4
6.0
4.0
0
5
10
15
20
25
White NativeAmerican
Hispanic Black Asian
Abuse
Dependence
Lifetime DSM-IV Alcohol Abuse and Dependence by Race-Ethnicity
Pre
vale
nce
(%
)
4.54.0
2.9
2.2
3.2
5.5
6.26.6
0
1
2
3
4
5
6
7
8
$0-19,999 $20,000-34,999 $35,000-$69,999 $70,000+
Dependence
Abuse
Current DSM-IV Alcohol Dependence and Abuse by Income
Pre
vale
nce
(%
)
Disability by diagnosis, and by number of Disability by diagnosis, and by number of dependence criteriadependence criteria
Image Removed – Awaiting Copyright Permissions
Treatment RatesTreatment Rates Current DSM-IV Abuse and Dependence Current DSM-IV Abuse and Dependence
1991-1992 and 2001-20021991-1992 and 2001-2002
13.8
12.1
4.4
3.1
0
2
4
6
8
10
12
14
16
NLAES 1991-1992 NESARC 2001-2002
Alcohol Dependence
Alcohol Abuse
Tre
atm
ent R
ates
(%
)
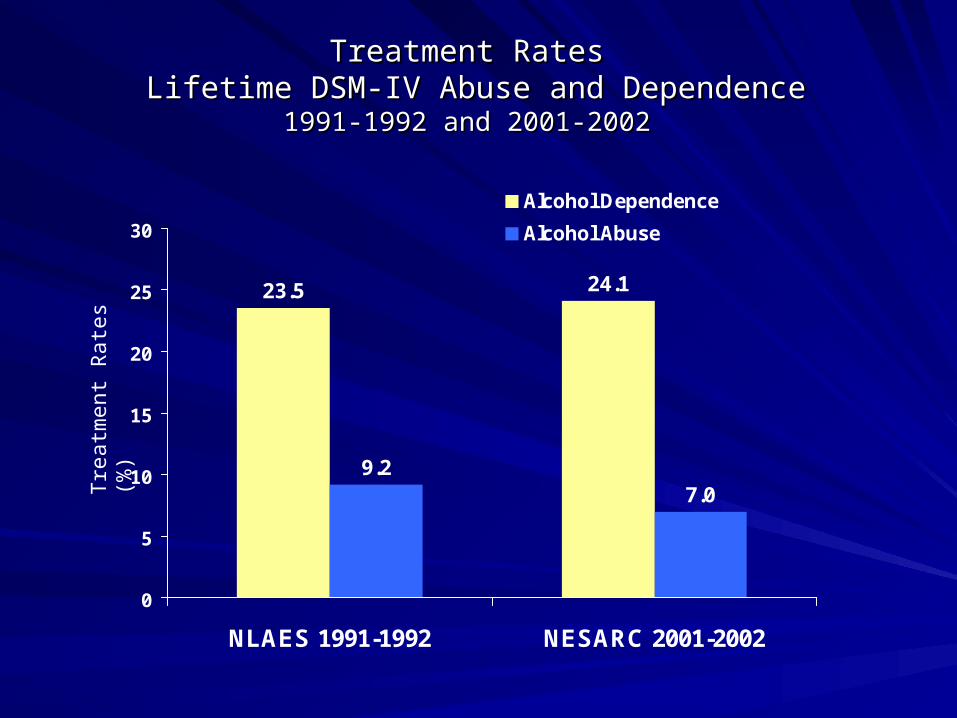
Treatment RatesTreatment Rates Lifetime DSM-IV Abuse and Dependence Lifetime DSM-IV Abuse and Dependence
1991-1992 and 2001-20021991-1992 and 2001-2002
23.5 24.1
9.27.0
0
5
10
15
20
25
30
NLAES 1991-1992 NESARC 2001-2002
Alcohol Dependence
Alcohol Abuse
Tre
atm
ent R
ates
(%
)
Most Common Alcohol Treatment/Help Seeking Settings Among Individuals with Current Alcohol Abuse or
Dependence
Treatment/Help Seeking Setting
Alcohol Abuse
Alcohol Dependenc
e
Physician or other health care professional 0.6% 6.7%
Alcohol dependence is a highly reliable, valid alcohol Alcohol dependence is a highly reliable, valid alcohol diagnosis, however:diagnosis, however:
– Should a Should a severityseverity indicator of dependence be added, as indicator of dependence be added, as has been used in small-sample/low-frequency genetics has been used in small-sample/low-frequency genetics studies (studies (Hasin et al., 2002; Heath et al., 2001Hasin et al., 2002; Heath et al., 2001)?)?
– Should Should drinking leveldrinking level be added as a criterion or as an extra be added as a criterion or as an extra requirement (Li et al., 2007), e.g., Project COMBINE? requirement (Li et al., 2007), e.g., Project COMBINE? (Anton (Anton et al., 2006)et al., 2006)
– Can biological Can biological endophenotypesendophenotypes be identified that would aid be identified that would aid in the diagnosis, e.g., the COGA study? in the diagnosis, e.g., the COGA study? (Hesselbrock et al., (Hesselbrock et al., 2001; Edenberg et al., 2004)2001; Edenberg et al., 2004)
Alcohol abuse is less clear Alcohol abuse is less clear
– Keep abuse as it is now? Keep abuse as it is now?
– Diagnose it independently from dependence?Diagnose it independently from dependence?
– Combine abuse and dependence criteria (Saha et Combine abuse and dependence criteria (Saha et al., 2006)?al., 2006)?
– Drop abuse entirely on the assumption that it is Drop abuse entirely on the assumption that it is just a prodromal phase of dependence?just a prodromal phase of dependence?
Evidence for dependence as continuous Evidence for dependence as continuous condition with graded severity: NESARCcondition with graded severity: NESARC
National Epidemiologic Survey on Alcohol and National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) Wave 2: 2004-2005Related Conditions (NESARC) Wave 2: 2004-2005
National sampleNational sampleN= 34,653N= 34,653Cumulative response rate Cumulative response rate 70.2%70.2%Covered period since Wave Covered period since Wave 1 interview, incorporting 1 interview, incorporting information from Wave 1 information from Wave 1 through computerized through computerized interviewinterviewAdded additional diagnoses, Added additional diagnoses, risk factors and risk factors and consequences of alcohol consequences of alcohol and other disordersand other disordersDSM-IV diagnosesDSM-IV diagnosesIn-person interviewsIn-person interviews
Incidence of alcohol use disordersIncidence of alcohol use disorders (Grant et al., Molecular Psychiatry 2008)(Grant et al., Molecular Psychiatry 2008)
First time studied in the U.S. general populationFirst time studied in the U.S. general population
– One-year incidence rates (cases per 100 person-years at One-year incidence rates (cases per 100 person-years at risk) of alcohol dependence and abuse were among the risk) of alcohol dependence and abuse were among the highest of all disorders: 1.70 for dependence, 1.02 for abusehighest of all disorders: 1.70 for dependence, 1.02 for abuse
– Demographic predictors similar to those previously shown Demographic predictors similar to those previously shown for prevalence (male, unmarried, younger) for prevalence (male, unmarried, younger)
Relapse of alcohol dependence Relapse of alcohol dependence (Dawson et al., Alch Clin Exp Rsch 2007)(Dawson et al., Alch Clin Exp Rsch 2007)
First time studied in the U.S. general populationFirst time studied in the U.S. general population
– 1,772 had current alcohol dependence at Wave 1 and were re-1,772 had current alcohol dependence at Wave 1 and were re-interviewed at Wave 2interviewed at Wave 2
– Type of remission predicted likelihood of relapseType of remission predicted likelihood of relapse
– Three types: high-risk drinker (according to Clinician’s Guide), low Three types: high-risk drinker (according to Clinician’s Guide), low risk drinker, abstainerrisk drinker, abstainer
– In respondents aged 35+, symptom recurrence differed significantly In respondents aged 35+, symptom recurrence differed significantly by remission status at Wave 1: 51.0% in high-risk drinkers, 27.2% by remission status at Wave 1: 51.0% in high-risk drinkers, 27.2% in low-risk drinkers, and 7.3% in abstainers. in low-risk drinkers, and 7.3% in abstainers.
– Risk of relapse did not differ significantly by Wave 1 remission Risk of relapse did not differ significantly by Wave 1 remission status in respondents aged 34 or lessstatus in respondents aged 34 or less
SummarySummary
Alcohol consumption, abuse and dependence show Alcohol consumption, abuse and dependence show much variability by time, geographic location and much variability by time, geographic location and individual characteristicsindividual characteristics
Risk is affected by many factors, from availability and Risk is affected by many factors, from availability and laws to personal experiences to geneslaws to personal experiences to genes
All of this variability potentially points out directions for All of this variability potentially points out directions for policy and the investigation of etiologypolicy and the investigation of etiology
Much more needs to be done to understand these Much more needs to be done to understand these factors fully, and NESARC data are available to factors fully, and NESARC data are available to stimulate further studiesstimulate further studies
AcknowledgementsAcknowledgements
Bridget Grant, Ph.D., Ph.D.Bridget Grant, Ph.D., Ph.D.Katherine Keyes, M.P.H. Katherine Keyes, M.P.H. Fred Stinson, Ph.D. Fred Stinson, Ph.D.
NIAAA and NIDA for the NESARC dataNIAAA and NIDA for the NESARC data
Current support: R01 AA013654, Current support: R01 AA013654, K05 AA014223K05 AA014223, , R01 DA018652, R01 DA018652, New York State Psychiatric New York State Psychiatric InstituteInstitute
Contact information for Dr. Hasin: Contact information for Dr. Hasin: [email protected]@columbia.edu