The Five Main Rubrics of Epidemiology, As Applied to Drug Dependence Syndromes James C. (Jim) Anthony, Ph.D. Professor and Chairman Department of Epidemiology College of Human Medicine Michigan State University [email protected]www.epi.msu.edu Copyright, J. Anthony, 2007
Transcript
The Five Main Rubrics of Epidemiology, As Applied to
Drug Dependence Syndromes James C. (Jim) Anthony, Ph.D.Professor and Chairman
Department of EpidemiologyCollege of Human MedicineMichigan State University
1. By the end of the session, the learner will be able to sort the main evidence from epidemiological studies into relation to the five main rubrics of (1) Quantity, (2) Location, (3) Causes, (4) Mechanisms, and (5) Prevention and Control.
2. The learner also will be able to describe the main clinical features associated with syndromes of drug dependence, and to discuss separable relationships between drug dependence and drug-related socially maladaptive behavior that sometimes appears in different phases of the drug dependence process.
3. The learner will be able to discuss the 'no causation without manipulation' theme of contemporary epidemiology, in relation to the example of early social maladaptation and later risk of drug use and dependence.
Is Epidemiology Just A Matte r of Counting Up Cases and Sorting Them Into Bins With
Labels for Static “Risk Factors”?
No!Epidemiology is a branch of the biomedical sciences that uses population-oriented research approaches to answer specific
questions.
Does it make sense to define epidemiology in terms of
jargon words such as ‘distribution and dynamics of
disease’?No!
What’s the use of a definition that is understood only by individuals who
have studied epidemiology?
What of Jeremy Morris’ Seven Uses of Epidemiology?
Are They Useless?No!
For anyone who can remember the seven uses, they serve as equally useful orienting concepts to the ‘content’ of epidemiology
(as opposed to the ‘methods’ of epidemiology).But I rarely encounter anyone who can recite all 7 uses.
Teaching epidemiology from 1978 through 1999, I learned that almost everyone can remember and retain 5 rubrics of
epidemiology, which subsume Morris’ 7 uses.
As shown on the next page, a helpful mnemonic starts with the first question, “How many?” and then proceeds to these
questions: “Where?” “Why?” “How” and “What Can We Do?”
Five Main Rubrics of Epidemiological Research
and The Associated Research Questions
1. Quantity: How many?2. Location: Where?3. Causes: Why?4. Mechanisms: How?5. Prevention & Control: What Can We Do?
These rubrics make it possible to specify an alternative definition for epidemiologists to use when describing their research to the public. Namely, in epidemiology, we seek increasingly definitive answers to scientific and public health questions under five main
rubrics.1. Quantity: Within the population, how many are affected? How many are becoming affected?
2. Location: Where, in the population experience, are cases more or less likely to occur, and where are they more or less likely to be found?
3. Causes: What accounts for some becoming affected while others are spared?
4. Mechanisms: What are the linkages of states and processes that account for people becoming cases and remaining cases? What accounts for the observed natural history and clinical course, comorbidities, secondary impairments, residual disabilities?
5. Prevention & Control: How can we prevent, delay, or ameliorate the condition?
Epidemiology is not the only branch of biomedical sciences
that seeks to answer these questions; it is distinguished by its population orientation, consistent with an exchangeable term
to define the field of inquiry: ‘medical ecology.’
What Is One of the Unique Skill Sets Practiced By
Epidemiologists Under the First Rubric (Quantity)?
MEASURING DISEASE OCCURRENCE AND FREQUENCY IN
POPULATIONS
Tobacco, 1 in 3
Heroin, 1 in 4-5
Cocaine HCl, 1 in 6
Stimulants otherthan cocaine, 1 in 9Cannabis,
1 in 9-11
Anxiolytic,sedative, &hypnoticdrugs, 1 in 11
AnalgesicDrugs, 1 in 11
Psychedelicdrugs, 1 in 20
Inhalantdrugs, 1 in 20
Estimatedfractionof drug userswho havedeveloped asyndrome ofdependence
Epidemiological Population Estimates
for theUnited States,
1992-1998
Crack + HCl, 1 in 5
Alcohol, 1 in 7-8
(Adapted from Anthony et al., 1994; Chen & Anthony, 2002)
General Concept of Drug Dependence(generally adapted to each drug)
We can define and measure a drug dependence syndrome in relation to:
(i) disturbances of the mental life (e.g.,obsession-like ruminations and recurrent thoughts or cravings);
(ii) disturbances of behavior (e.g., sometimes expressed in the form of compulsion-like repetitions of drug-involved behavior);
(ii) manifestations of neuroadaptation secondary to drug exposures (e.g., experienced as a subjective feeling that the same dose of drug is less efficacious, or observable in the form of clinical features of a withdrawal syndrome after long-sustained daily or near-daily consumption).
For a Scientific Reason, This General Concept of Drug Dependence Does Not Include a Criterion for Legal or
Social Maladaptation, Which Needs to Be Defined, Conceptualized, and Measured Quite Separately.
• Drug-induced social maladaptation (e.g., getting into trouble with the law) is not necessary under this concept of drug dependence. We think of the social maladaptation as a distinguishable phenomenon that has as much to do with the legal and social responses to a person’s drug use.• Many examples of drug dependence without social maladaptation exist. These cases are not differentiable from other cases unless we allow drug dependence to be defined, conceptualized, and measured without reference to drug-induced or drug-related socially maladaptive behavior.• Moreover, due to time and place variation in drug laws, and to variations in enforcement, prosecution, and judicial response to drug law violations, a case definition that appeals to concepts of legal and social maladaptation will induce epidemiological variations from place to place and time to time.
(Anthony et al.., Clinical Neuroscience Research, 2005).
The Concepts of Drug Dependence Were Derived By Studying Cases In Contact With Specialty Treatment Services.
But What Do We Know About The Fraction of Community Cases Who Seek or Enter Treatment?
Another Epidemiological Parameter Estimated Under the Rubric of 'Quantity':
What Proportion Make First Treatment Contact Within 5-10 Years After Onset of
Dependence?Within 5 Years:
AlcoholControlled Substances 12-18%
40-45%
25-30%55-60%
Within 10 Years:AlcoholControlled Substances
Estimates from National Comorbidity Survey Replication, USA (Wang et al., 2005)
What Is One of the Unique Skill Sets Practiced By
Epidemiologists Under the Second Rubric (Location)?
Identifying when, where, and within which population
subgroups the cases are more or less likely to arise.
Data from NHSDA, Late 1990s, reported by Gfroerer et al., 2002
TIME TREND IN THE ESTIMATED ANNUAL INCIDENCE RATEFOR NEW CANNABIS USE IN THE U.S., BY AGE
Adapted by Anthony, 2006
Locational parameters of interest:When: The Time Dimension, 1965-1999Who: Facets of Person, Ages 12-17, 18-25Where: Facets of Place, USA
UPPER BOUND
LOWERBOUND
From: Anthony, 2006
Based upon these estimates, during the late 1990s, the US was accruing as many new cases of cannabis use as were being accrued during the last interval of peak incidence during the Vietnam and immediate post-Vietnam era.
Under the Location Rubric: Are Crack-Cocaine Smokers More Likely To Experience Rapid-Onset of Cocaine
Dependence?Locational Parameter of Interest:
Facets of Person, What Form of Cocaine Use?Cocaine Hydrochloride Powder only, typically intranasally, versus Recent Cocaine HCl powder
use plus crack-smoking, versus Past Cocaine HCl powder use plus crack smoking.
HealthProblems
ReducedActivities
Tolerance
EmotionalProblems
UsedMoreThan
Intended
Salience InabilityTo CutDown
Cocaine HCl(n=572)
Crack-smoking (Recent HCL)
(n=190)
Crack-smoking (Past HCL)
(n=93)
35
0
5
10
20
Estimated risk of
experiencing each clinical features
associated with rapid-
onset of cocaine
dependenceShould we
think of thisas a 'causal association'? Here, we shift to the third rubric “Of Causes”
Chen & Anthony, Psychopharmacology, 2004
What Are Unique Skill Sets Practiced By
Epidemiologists Under the Third Rubric (Causes)?
Population-Level Research on the
Suspected Causes of Health Conditions
Question Under the Rubric of Causes: Is there increased risk of rapid-onset cocaine dependence in response to crack-cocaine smoking?
We do not yet have definitive evidence to answer this question. The government has dug in its heels and will not release the data required to push forward on this research front.
Why don’t we have the definitive evidence?
Crack-cocaine smoking is not distributed at random in the population; some subgroups are more likely than others to smoke crack-cocaine – e.g., Males age 20-29, of African-American heritage.
This subgroup also is more likely to progress rapidly to cocaine dependence, once cocaine use starts – even when crack-smoking is not in the picture (O’Brien & Anthony, Neuropsychopharmacology, 2005).
Is this an example of underlying gene-based or cultural vulnerability inherent to African-American males?
Probably not. When we hold constant neighborhood conditions, White non-Hispanic males and African-American males are equally likely to have started smoking crack-cocaine? (Lillie-Blanton, Anthony, Schuster, JAMA, 1993)
So we are left with an unanswered epidemiological research question.NSDUH data have been gathered so that we might to press forward toward increasingly definitive evidence, but these data are not being released for analyses, due to concerns about potential violation of federal law that protects privacy of research participants.
What Are Unique Skill Sets Practiced By
Epidemiologists Under the Fourth Rubric
(Mechanisms)? Population-Level
Research on Suspected Mechanisms, Natural History, and Clinical
Course
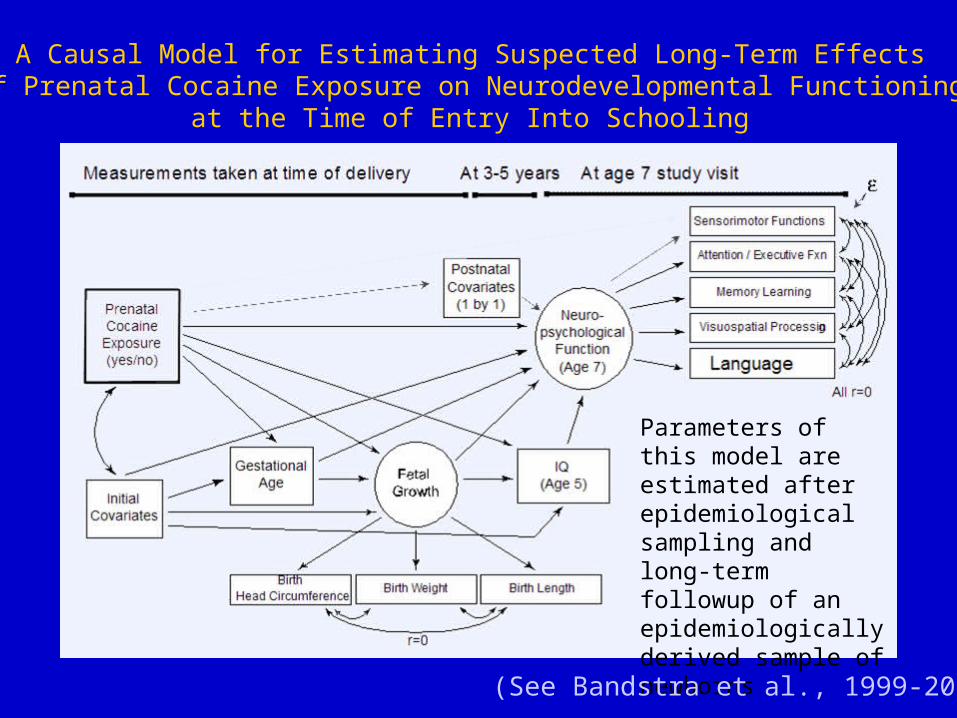
A Causal Model for Estimating Suspected Long-Term Effectsof Prenatal Cocaine Exposure on Neurodevelopmental Functioning
at the Time of Entry Into Schooling
Parameters of this model are estimated after epidemiological sampling and long-term followup of an epidemiologically derived sample of newborns
(See Bandstra et al., 1999-2006)
An Elaboration of the Causal Model to Pose a Specific Question:Does the evidence tend to support a specific causal effect of prenatal cocaine exposure upon sensorimotor functioning, over and above more general impact upon levels of neurodevelopmental functioning?
To date, our evidence tends to support this specific causal path, but the jury still is out.
(See Bandstra et al., 1999-2006)
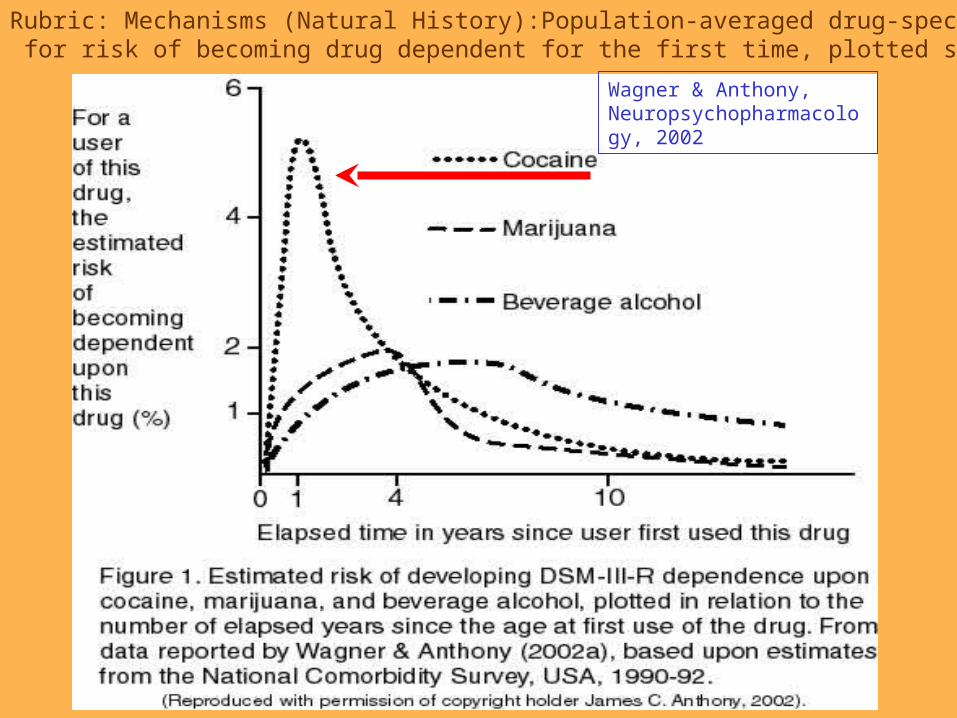
Rubric: Mechanisms (Natural History):Population-averaged drug-specific estimates for risk of becoming drug dependent for the first time, plotted since first use.
Wagner & Anthony, Neuropsychopharmacology, 2002
What Are Unique Skill Sets Practiced By
Epidemiologists Under the Fifth Rubric (Prevention &
Control)? Population-Level
Prevention and Public Health Experiments
Current Theme We Are Debating in Epidemiology
No causation without manipulation?
The debate is pushing epidemiology in the direction of intersections with experimental sciences and toward greater mastery of randomized controlled trial designs and randomized instrumental variable designs.
Exemplar Problem 1As already discussed, Crack Smokers seem to be more likely to develop a rapid-onset syndrome of cocaine dependence.
Is this because crack 'causes' increased risk of the syndrome?
Is it because crack-smokers were different to begin with, before crack-smoking (e.g., increased levels of a susceptibility trait)?
Is it because crack 'recruits' highly susceptible individuals?
We can’t experiment by assigning crack at random, but we CAN randomly assign crack-prevention programs!
To the extent that these programs actually reduce crack cocaine smoking, there ought to be concomitantly reduced risk of rapid-onset cocaine dependence in that experimental subgroup – if crack smoking is causing rapid-onset cocaine dependence.
Exemplar Problem 2We have seen evidence that prenatal cocaine exposure might be causing long-term impairments in neurodevelopmental functioning, and perhaps a specific impairment in sensorimotor functioning.
But were all potentially confounding variables brought under control?
Isn't it possible that some background characteristic, condition, or process is accounting for what now is observed as a spurious relationship between prenatal cocaine exposure and later sensorimotor deficits?
Here again, we cannot experimentally induce prenatal cocaine exposure at random, but we can randomly assign programs that seek to reduce prenatal cocaine exposure, with followup to check sensorimotor functioning deficits in the newborns whose mothers did not have the benefit of that program.
Exemplar Problem 3Youths, especially boys, with a history of conduct problems and other socially maladaptive behavior, are more likely to (a) engage in early-onset drug use, and (b) experience drug dependence syndromes, once
drug use starts.Years of observational studies confirmed the robustness of this aspect of 'location of cases' but never could resolve the causal question:
Was the early social maladapation a 'cause' of the later drug involvement?
Adopting the 'no causation without manipulation' perspective, we undertook a population-level randomized controlled trial to probe this causal question.
Perc
en
t S
tart
ing
Tobac c
o U
s e Usual & Customary Control
Good Behavior Game
MasteryLearning
22%
49%
6 8 AGE
12 14 0
10
20
30
40
50
60
RCT: Good Behavior Game universal intervention in Grades 1-2:Estimated ~50% reduction in risk of starting to smoke tobacco
by age 14 among males.
Kellam & Anthony, Am J Public Health, 1998
REPLICATIONS & EXTENSION OF THIS WORK
Storr and colleagues (Drug & Alcohol Dependence, 2002) have reported results from an independent replication, also consistent with an enhanced Good Behavior Game impact on risk of early onset tobacco smoking.
Via follow-up of these young people to the early years of young adulthood, Storr and colleagues (under review) now are reporting that the long-term impact of the Good Behavior Game appears to include reduced risk of tobacco dependence syndromes. That is, delay of onset of tobacco smoking was followed by reduced risk of becoming tobacco dependent.
NEXT STEPS
Working with collaborators in the Colleges of Education and with community, school, and parent leaders, members of our research group hope to learn whether this type of primary school intervention might yield beneficial impact in other local communities.
Via secondary effects on others, these preventive interventions directed toward youthful tobacco smoking should have lasting public health benefits in addition to benefit in relation to the health of individual participants.
Recap: Learning Objectives
1. By the end of the session, the learner will be able to sort the main evidence from epidemiological studies into relation to the five main rubrics of (1) Quantity, (2) Location, (3) Causes, (4) Mechanisms, and (5) Prevention and Control.
2. The learner also will be able to describe the main clinical features associated with syndromes of drug dependence, and to discuss separable relationships between drug dependence and drug-related socially maladaptive behavior that sometimes appears in different phases of the drug dependence process.
3. The learner will be able to discuss the 'no causation without manipulation' theme of contemporary epidemiology, in relation to the example of early social maladaptation and later risk of drug use and dependence.
The End!
Thank you for your kind attention.Photo credit: Pan American Health Organizationhttp://www.paho.org/English/DPI/categ02.htm