47
THE FODMAP DIET Christina Berberich, PharmD, MPH, RD September 17 & 18, 2015

THE FODMAP DIET Christina Berberich, PharmD, MPH, RD
September 17 & 18, 2015
Disclosure
• The content of this program has met the continuing
education criteria of being evidence-based, fair and
balanced, and non-promotional.
• This educational event is supported by Abbott Nutrition
Health Institute, Abbott Nutrition.
• I am currently an employee of Abbott Nutrition
2

Learning Objectives
• List the 6 FODMAP groups and name one food source for
each
• Name the condition that the low FODMAP diet is used for
and describe how it is purported to reduce symptoms
• Describe how to initiate and manage a patient on a low
FODMAP diet and list 2 potential concerns
3

Overview
• Provide the definition of FODMAPs and examples of each
• Define functional bowel disorders, specifically irritable
bowel syndrome (IBS)
• Discuss the relationship between IBS and FODMAPs
• Review the current research on low FODMAP diets for
IBS
• How to start and manage a patient on a low FODMAPs
diet
• Describe the potential concerns with a low FODMAPs diet
4
Definition
• FODMAPs:
• Fermentable Oligo-, Di-, Monosaccharide and Polyols
• Short-chain carbohydrates and sugar alcohols
• Fructose, lactose, fructans, mannitol, sorbitol, galactans
• Used to ease symptoms of functional bowel disorders
5
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8.

Functional Bowel Disorders
• Bowel looks normal but has disordered actions
• Irritable bowel syndrome (IBS), chronic diarrhea or
constipation or bloating
• Cause(s) unknown
6
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8

Irritable Bowel Syndrome (IBS)
• Condition of hypersensitivity leading to an abnormal
reaction in the gut
• Characterized by abdominal pain, gas, bloating, diarrhea,
constipation
• Different subtypes
• Diarrhea-predominate
• Constipation-predominate
• Mixed
7
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

Rome III Criteria
8
ROME III
Symptoms for at least 6 months
Positive diagnosis must include the following:
1. Abdominal pain/discomfort at least 3 days/mo for last 3
months, and 2 of the following true >25% of the time:
-Improvement with defecation
-Onset associated with change in
stool frequency
-Onset associated with change in
stool appearance
2. Symptoms not caused by an inflammatory, metabolic,
anatomical, or neoplastic condition
Drossman, DA. The functional gastrointestinal disorders and the Rome III process. Gastroenterology. 2006;130:1377-1390.
Drossman, DA. Rome III: The Functional Gastrointestinal Disorders. McLean, VA: Degnon Associates; 2006:896.

IBS
• Food can trigger symptoms
• No effect on underlying condition
• FODMAPs are potential triggers due to their effects within
the gut
• Potential to mitigate symptoms though avoiding offending
foods
9
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

FODMAPs and IBS
• FODMAP carbohydrates are minimally absorbed in the
small intestine
• High osmolality
• Fermentable
• Normal process that is generally not problematic in
healthy individuals
• In an abnormally hypersensitive gut, can lead to
symptoms
10
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

Osmotic effect of FODMAPs
11
GUT PERITONEAL SPACE PERITONEAL SPACE

Osmotic effect of FODMAPs
12
GUT PERITONEAL SPACE PERITONEAL SPACE

Osmotic effect of FODMAPs
13
GUT PERITONEAL SPACE PERITONEAL SPACE

Bacterial effect of FODMAPs
14
GUT PERITONEAL SPACE PERITONEAL SPACE

Osmotic effect of FODMAPs
15
GUT PERITONEAL SPACE PERITONEAL SPACE

Other potential effects on the gut
• ↑ Gut motility
• Possible activation of hormonal/neural feedback pathways
during osmotic pressure changes and short chain fatty
acid production
• Abnormal GI endocrine cells in IBS
• Release hormones having endocrine effects leading to
increased GI motility and sensation
16
El-Salhy M, Gilja OH, Gundersen D, Hatlebakk JG, Hausken T. Interaction between ingested nutrients and gut endocrine cells in patients with irritable bowel syndrome. Int J Mol Med.
2014;34:363-371.
Piche T, Zerbib F, Varannes SB, et al. Modulation by colonic fermentation of LES function in humans. Am J Physiol Gastrointest Liver Physiol. 2000;278:G578-G584.
Piche T, des Varannes SB, Sacher-Huvelin S, Holst JJ, Cuber JC, Galmiche JP. Colonic fermentation influences lower esophageal sphincter function in gastroesophageal reflux disease.
Gastroenterology. 2003;124:894-902.

FODMAPs and Gut Bacteria
• Gut bacteria generally fall into 3 categories:
• Both absolute number and species type affect health
• Many FODMAPs are prebiotics
• Encourage the growth of helpful bacteria
17
Helpful Harmful Neither
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

FODMAPs and Gut Bacteria
• Condition of small intestinal bacterial overgrowth (SIBO)
• Occurs in some with IBS
• May lead to:
• ↑ Gut permeability
• Fermentation and gas production within the small intestine
• May delay transit time leading to constipation
18
Pimentel M, Lin HC, Enayati P, et al. Methane, a gas produced by enteric bacteria, slows intestinal transit and augments small intestinal contractile activity. Am J Physiol Gastrointest
Liver Physiol. 2006;290:G1089-G1095.

FODMAPs and Gut Bacteria
• In the large intestine multitude of FODMAP-digesting
bacteria species
• Gas production may be hydrogen or methane
• Not all fermentation is gas producing
19
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

Where’s the FOOD?
20

Foods - Examples
21
Excess Fructose
• Apple, watermelon, pear, asparagus, sugar snap peas, high fructose corn syrup, honey, agave
Lactose
• Milk (cow, sheep, goat), evaporated, sweetened condensed, dry powder, custards, dairy desserts
Fructans
• Wheat, onion, leeks, FOS
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

Foods - Examples
22
Mannitol
• Watermelon, cauliflower, mushrooms, snow peas, sweetener
Sorbitol
• Apples, apricots, nectarines, peaches, pears, plums, sweetener
Galactans
• Chickpeas, legumes, lentils
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

Why Excess Fructose is a problem
23
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8.
Gibson PR, Newnham E, Barrett JS, Shepard SJ, Muir JC. Review article: fructose malabsorption and the bigger picture. Aliment. Pharmacol. Ther. 2007;25:349-63.
Small intestine
lumen Capillary
Enterocyte
GLUT2
GLUT5 Fructose
Glucose Fructose
SGLT1
Galactose
Apical membrane Basolateral membrane
GLUT2
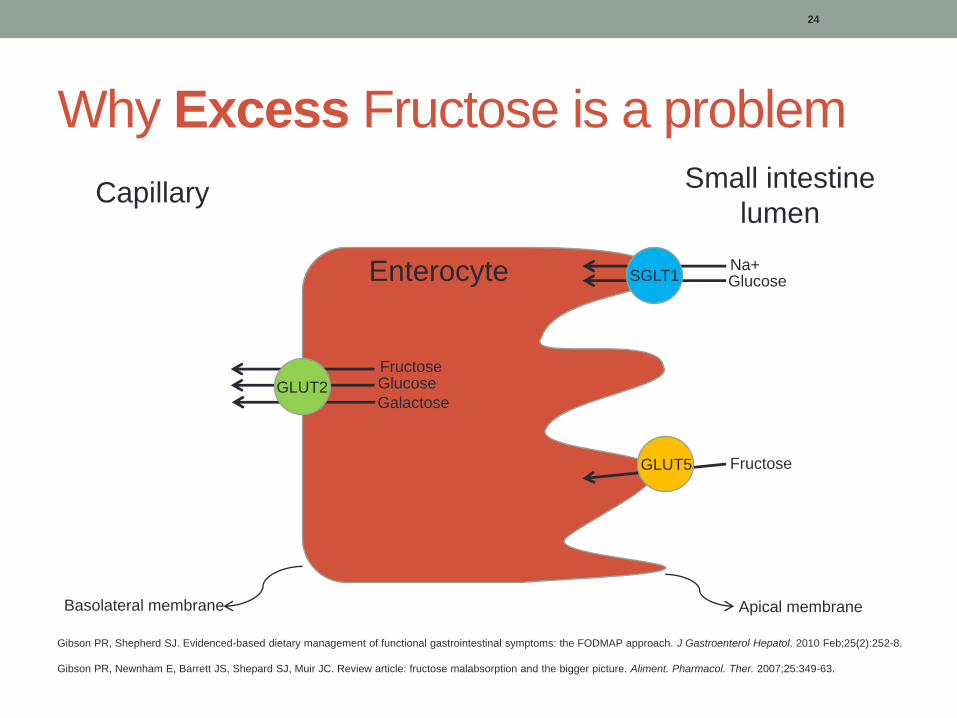
Why Excess Fructose is a problem
24
Small intestine
lumen Capillary
Enterocyte
GLUT2
GLUT5
Glucose
Fructose
Na+
Glucose Fructose
SGLT1
Galactose
Apical membrane Basolateral membrane
GLUT2
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8.
Gibson PR, Newnham E, Barrett JS, Shepard SJ, Muir JC. Review article: fructose malabsorption and the bigger picture. Aliment. Pharmacol. Ther. 2007;25:349-63.

Why Excess Fructose is a problem
25
Small intestine
lumen Capillary
Enterocyte
Glucose
GLUT5
Glucose
Fructose
Na+
Fructose
SGLT1
Galactose
Apical membrane Basolateral membrane
GLUT2
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8.
Gibson PR, Newnham E, Barrett JS, Shepard SJ, Muir JC. Review article: fructose malabsorption and the bigger picture. Aliment. Pharmacol. Ther. 2007;25:349-63.
FODMAP Research
• Objective: to investigate the effects of a low FODMAP diet
vs typical Australian diet in IBS and healthy individuals
• Study Design:
• Randomized, controlled, single-blind, crossover
• n=38, 30 ROME III IBS, 8 healthy
• 21 d of study/control diet → 21 d washout → 21 d control/study diet
• Subjective/objective assessments
• Total FODMAP content in the study diet = <0.5 g per sitting
(meal/snack)
26
Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014 Jan;146(1):67-75.e5

Results
• IBS subjects (~70%)
• ↓GI symptom scores
• ↓Bloating, pain, gas
• ↑Satisfaction with stool consistency
• Only diarrhea predominate IBS subjects had significant changes to
stool
• Healthy subjects
• No significant changes between diets
27
Halmos EP, Power VA, Shepherd SJ, Gibson PR, Muir JG. A diet low in FODMAPs reduces symptoms of irritable bowel syndrome. Gastroenterology. 2014 Jan;146(1):67-75.e5

FODMAP Research
• Objective: evaluate the effects on colonic health after a
low FODMAP diet vs typical Australian diet
• Study Design:
• RCT
• n=33, 27 ROME III IBS, 6 healthy
• 21 d of study/control diet → 21 d washout → 21 d control/study diet
• Total FODMAP content in the study diet = average 3 g/day
• Measured stool pH, SCFA concentration, bacterial number and
species diversity
28
Halmos EP, Christophersen CT, Bird AR, Shepherd SJ, Gibson PR, Muir JG. Diets that differ in their FODMAP content alter the colonic luminal microenvironment. Gut. 2015
Jan;64(1):93-100.

Results
• Low FODMAP diet
• ↑pH (7.37 vs 7.16)
• ↓Bacterial number
• No difference in SCFA concentrations
• Typical Australian and habitual diets (washout)
• ↑ numbers of several species of health promoting bacteria
29
Halmos EP, Christophersen CT, Bird AR, Shepherd SJ, Gibson PR, Muir JG. Diets that differ in their FODMAP content alter the colonic luminal microenvironment. Gut. 2015
Jan;64(1):93-100.

FODMAP Review
• Objective: summarize evidence of a low FODMAP diet to
manage food intolerance in IBS
• Study design:
• 40 articles, 31 studies, 9 reviews
• Evaluated evidence on FODMAP possible mechanisms, benefits,
limitations, concerns, and dietary management
30
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub
ahead of print]

Results
• Evidence points to the role of food triggering IBS
symptoms
• Dietary changes potentially can decrease symptoms and
increase QOL
• Further study needed on:
• Nutrition concerns related to restrictive nature
• Specific populations where effect is greatest
• Identifying non-IgE-mediated food allergy biomarkers
• Evaluation of other foods that effect visceral hypersensitivity,
immunity
31
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of
print]

FODMAP Research
• Objective: to study the efficacy of a low FODMAP diet in
children and determine if microbial composition are
associated with diet efficacy
• Study Design:
• Randomized, double blind, crossover
• 33 children ROME III IBS
• 7 day habitual diet → 48 h FODMAP/typical American childhood
diet (TACD) → 5 day habitual diet → 48 h TACD/FODMAP diet
• Intervention diet food was provided (9 g/d vs. 50 g/d FODMAP
content)
• Stool were collected and analyzed for microbial composition prior
to interventional diets
32
Chumpitazi BP, Cope JL, Hollister EB, Tsai CM, McMeans AR, Luna RA, Versalovic J, Shulman RJ. Randomised clinical trial: gut microbiome biomarkers are associated with clinical response
to a low FODMAP diet in children with the irritable bowel syndrome. Aliment Pharmacol Ther. 2015 Aug;42(4):418-27. doi: 10.1111/apt.13286. Epub 2015 Jun 24

Results
• Pain
• Less abdominal pain during low FODMAPs vs habitual
• More pain episodes during TACD vs. habitual
• Stool microbial composition
• Responders had significantly different microbial biomes compared
to Nonresponders
• Taxa found in Responders known for high saccharolytic metabolic
capacity
• Potential for use as a biomarker to predict diet efficacy
33
Chumpitazi BP, Cope JL, Hollister EB, Tsai CM, McMeans AR, Luna RA, Versalovic J, Shulman RJ. Randomised clinical trial: gut microbiome biomarkers are associated with clinical response
to a low FODMAP diet in children with the irritable bowel syndrome. Aliment Pharmacol Ther. 2015 Aug;42(4):418-27. doi: 10.1111/apt.13286. Epub 2015 Jun 24

Implementation of low FODMAPs Diet
34
Comprehensive diet assessment
Explain scientific basis
Give low FODMAPs diet
specifics
Teach ways to maintain
compliance away from home
Start Diet!

Low FODMAPs Diet
• 1. Diet Assessment:
• To get an accurate view of what patient is eating/patterns of
consumption
• Goal is find out which FODMAPs the patient consumes on a daily
basis
• Use to better direct the patients dietary choices to make the most
effective use of the restrictions
35
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8

Low FODMAPs Diet
• Limitations to Diet Assessment
• Limited availability of published data on FODMAP content of
various foods
• No strong consensus on FODMAP content threshold
• What level is low?
• Low FODMAP content in excess
• How many low FODMAP foods does it take to make a high FODMAP
diet?
36
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8

Low FODMAPs Diet
• 2. Explain scientific basics to patients:
• Better understanding can lead to better diet compliance
• Aim for providing an understanding of:
• The malabsorption that occurs
• How subsequent fermentation leads to symptoms
37
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8
Low FODMAPs Diet
• 3. Give patients the specifics on the diet • High and low FODMAP content foods
• How long they should be on the diet
• Recording foods and symptoms
• Awareness that some chewing gums and beverages contain FODMAPs
too
• The good news – global restriction shouldn’t be long term
38
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8

Low FODMAPs Diet
• 4. Teach patients strategies to deal when patient is not in
control of their food prep • Carry low FODMAP snacks
• Pack lunch
• Find an option or two on restaurant menu before going in
• Planning is the key
39
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8

Low FODMAP Food Examples
40
Grains:
• quinoa, rice, corn, oats
Fruits:
• banana, grapes, pineapple, strawberry, prickly pear
Vegetables:
• broccoli, potato, lettuce, tomato, zucchini
Dairy:
• ripened cheeses, butter, cream, lactose free dairy
Sweeteners:
• table sugar (sucrose), stevia, aspartame, glucose
Other:
• tofu, seeds, flax, herbs, nonstarch polysaccharides
Mullen GE, et al. Irritable Bowel Syndrome: Contemporary Nutrition Management Strategies. J Par Ent Nut. 2014;38(7):781-799.

Low FODMAPs Diet Example
41
• Oatmeal, banana Breakfast:
• Lettuce salad with tomato, grilled chicken, quinoa, and a herbed vinegar/oil dressing Lunch:
• Baked fish (or beef, pork, or tofu) with rice, mashed potatoes, steamed broccoli Dinner:
• grapes, strawberries, sunflower seeds, rice cakes Snacks:

Low FODMAPs Diet
• Continue until achieve symptom relief (no more than 6-8
weeks)
• Begin reintroduction to avoid unnecessary restriction
• If inadequate response:
• Determine compliance
• If compliance established:
• Reduce resistant starch, soluble/insoluble fiber
• Consider gluten, food chemicals, caffeine, fat, meal size and regularly
42
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]
Gibson PR, Shepherd SJ. Evidenced-based dietary management of functional gastrointestinal symptoms: the FODMAP approach. J Gastroenterol Hepatol. 2010 Feb;25(2):252-8

Rechallenge Foods
43
• 2 tsp honey
Fructose
• 240 mL milk
Lactose
• 2 slices wheat bread
Fructans
• ½ cup lentils/legumes
Galactans
• 4 dried apricots
Sorbitol
• ½ cup mushrooms
Mannitol
Mansueto P, Seidita A, D’Alcamo A, Carroccio A. Role of FODMAPs in patients with irritable bowel syndrome: a review. Nutr Clin Pract. 2015. pii: 0884533615569886. [Epub ahead of print]

Enteral Feeding-Associated Diarrhea
• Could it be related to FODMAP content?
• Review: majority of cases not related to the formula
• C. diff and other intestinal infections
• Antibiotics
• Hyperosmolar medications
• Inulin in large doses can cause excess gas
• FOS can enhance resistance to C. diff, large doses can
cause bloating
• Prebiotic fiber dose and mixture can improve tolerance
44
Barrett JS, Shepherd SJ, Gibson PR. Strategies to manage gastrointestinal symptoms complicating enteral feeding. JPEN J Parenter Enteral Nutr. 2009;133:21-26.
Heimburger DC, Sockwell DG, Geels WJ. Diarrhea with enteral feeding: prospective reappraisal of putative causes. Nutrition. 1994;10:392-396.
Sobotka L, Brátova M, Slemrová M, Manák J, Vizd’a J, Zadák Z. Inulin as the soluble fiber in liquid enteral nutrition. Nutrition. 1997;13:21-25.
Lewis S, Burmeister S, Brazier J. Effect of the prebiotic oligofructose on relapse of Clostridium difficile-associated diarrhea: a randomized, controlled study. Clin Gastroenterol Hepatol.
2005;3:442-448.
Elia M, Engfer MB, Green CJ, Silk DB. Systematic review and metaanalysis: the clinical and physiological effects of fibre-containing enteral formulae. Aliment Pharmacol Ther.
2008;15(27):120-145.

Potential Issues
• Quite restrictive, especially carbs and fiber
• Can be expensive
• No long term safety data
• Long term use not recommended
• Not recommended in healthy people or those without
bowel problems
45

FODMAPs Summary
• Seem to show a modest decrease in IBS symptoms in
about 70% of patients
• Decreases in healthful gut bacteria are seen when
FODMAPs are restricted
• Some FODMAPs are prebiotics and have a beneficial
effects on gut health
• Long term use of a low FODMAPs diet has not been
studied at this time and is not recommended
46

Thank you!
• Questions?
47

















