89
The Health Status of Gypsies and Travellers in England Report of Qualitative findings 2004 Patrice Van Cleemput Kate Thomas Glenys Parry Jean Peters Julia Moore, Cindy Cooper
| Date post: | 16-Aug-2018 |
| Category: |
Documents |
| Upload: | nguyenkhuong |
| View: | 218 times |
| Download: | 0 times |

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
2004
Patrice Van Cleemput
Kate Thomas Glenys Parry Jean Peters
Julia Moore, Cindy Cooper

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 2
CONTENTS
Introduction and Methods Page 4 Background Page 5-7 Sampling Page 7-8 Access Page 8-10 Data collection Page 10-11 Data Analysis Cultural Beliefs and Attitudes Page 12-13 Introduction Page 13-14 Identity Page 14-15 Racism and Discrimination Page 15-16 Nomadism Page 16-18 Kinship- Family Ties Page 18-19 Privacy Page 19-20 Religion Page 21-22 Education Page 22 Cleanliness and Pollution concerns Page 23-24 Pride in home and personal appearance Page 24 Food and appetite Page 24-25 Self-reliance Page 25-26 Motivation and Accomplishment Page 26-27 Control and self determination Page 27-28 Conclusion

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 3
Health -related beliefs and attitudes
Page 29-32 Attitudes to health services Page 32-34 Lay referral
Page 34-35 Family Care Page 36-38 Attitudes to illness and health
Page 38-41 Attitudes to death and dying
Page 41-43 Attitudes to screening and diagnosis
Page 43-45 Conclusion Health experience
Page 46 Introduction
Page 46-49 Maternal Health Page 49-55 Chronic Ill health Page 55-60 Depression and psychological ill health Page 60-63 Substance and Alcohol Misuse
Page 63-64 Other Health issues and Conclusion Barriers to accessing health care Page 65 Introduction Page 65-67 Communication Page 67-68 Staff awareness of cultural factors affecting use of health care Page 69 Continuity and knowledge of family Page 69-70 Experience of and reactions to discrimination and racism Page 71-72 Effects of lack of knowledge and understanding on use of health care Page 72-73 GP registration Page 73-75 Appointment systems

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 4
Page 76 Health Records Page 76 Conclusion
Environmental factors Page 77 Introduction Page 77-78 Living Arrangements Page 78-79 Living in a trailer and unauthorised camping Page 80-81 Living in a trailer on a rented site Page 81-83 Housing Page 83 Privately owned family site Page 83-84 Process of securing appropriate accommodation Page 84 Hostility and fear of violence Page 85-86 Work Page 86 Conclusion Page 87 References

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 5
Introduction and Methods
This is a comprehensive account of the qualitative element of the fuller research study commissioned by Department of Health, Inequalities in Health programme. The full research study of the health of Gypsies and Travellers in England was designed to address health policy objectives by identifying the inequalities in health status between Gypsy Traveller and non-Gypsy Traveller populations and to explore culturally specific health beliefs, and attitudinal and practical barriers to accessing health services. There were three separate strands to this study and this full account of the qualitative study is a supplement to the highly condensed summary of findings that are contained in the full report of The Health Status of Gypsy Travellers in England (Report of Department of Health Inequalities in Health Research Initiative Project 121/7500). Background to the full research study Prior to the full study a pilot study had been carried out in 1999.1 On the basis of the successful pilot study, a bid was submitted to the Department of Health, Inequalities in Health programme in May 2000 to conduct multi-centre research in Sheffield, Leicester, Norfolk, London and Bristol. The study commenced in January 2002. Current health policy places particular emphasis on reducing inequalities in health and targeting socially excluded groups 2 and this research was undertaken to redress the omission within health policy. Qualitative study Research Questions The factors affecting equity of access to health services are complex and interacting. Good methodological quantitative research is required to demonstrate health status of Gypsy Travellers and the relative impact of associated variables such as ethnic minority group membership, educational attainment, lifestyle factors etc. Results from our pilot study, reading of the wider literature, and subsequent consultation with Gypsy Travellers and other members of the Gypsy Council helped us to identify the wider questions that needed to be explored. For example, in the pilot study, frequency of travel was the independent variable that had a significant influence on both the EQ5D index score and the visual analogue score. The Gypsy Travellers who travelled more frequently had better EQ5D and Visual analogue scores. Ginnetty, in her qualitative study of Travellers’ perspectives on health, observed “the meaning of living in a house is linked to a range of emotions from isolation, loneliness, loss of identity to feeling ‘closed in’.” On the other hand, one might expect a negative impact on health of the lack of basic amenities on Travellers stopping on unauthorised sites and the lack of a permanent address further reducing access to health and related services. Qualitative investigation is required to fully explore the influence and meaning of associated variables, in the context specific circumstances relating to their social situation, in order that culturally competent services can be developed and implemented.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 6
We identified these questions to explore the relationship of cultural beliefs, attitudes and perceptions of Gypsy Travellers health and their access to health care using a qualitative approach:
• How are the self perceived health needs of Gypsy Travellers met by their use and
experiences of health and related services • What are the health beliefs and attitudes of Gypsy Travellers in relation to health
service usage and access? • What are the perceived barriers to accessing health and related services • What are Gypsy Travellers’ experiences in accessing health care and the cultural
appropriateness of services provided? Bryman defines qualitative research as: “ the way in which people being studied understand and interpret their social reality”3
A qualitative approach to these questions is essential in order to discover and understand the beliefs, values, decisions, and actions of Gypsy Travellers in relation to health and access to health care and the meaning that they attach to them. When quantitative methods are used alone, in favour of combined qualitative studies that seek explanation, there is a possible danger in how the results may be interpreted. For example, studies that demonstrate the negative association of cultural lifestyle on health outcomes can be interpreted in the light of a need to change the lifestyle rather than for health services to adapt or respond in a culturally appropriate manner. Sampling A form of purposive sampling, known as maximum variation was used.4 This form of sampling deliberately includes widely varying phenomena that are based on prior knowledge of important characteristics of the group. The aim is to be able to include participants from across a wide and heterogeneous group.
Sampling was undertaken in the four localities to include Gypsy Travellers of both genders, across four age categories (16-25, 26-45, 46-65, over 65), four different types of accommodation (roadside/council site/private site/housed), and two geographical origins, English/Welsh and Irish Travellers. The settings were the same as for the main study with the interviews either conducted in the participants’ homes or a local neutral venue of their choice. The sample comprised of Gypsy Travellers who had been identified from the main study as having significant health problems. A sampling grid was used to ensure that a spread of interviewees was achieved across each category. Interviews were also conducted across the spread of seasons in order to reduce the likelihood of seasonal variations on mood and on health states having undue influence on the perceptions of the participants. Achieved sample The protocol allowed for purposive sampling of between 24 and 48 interviews
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 7
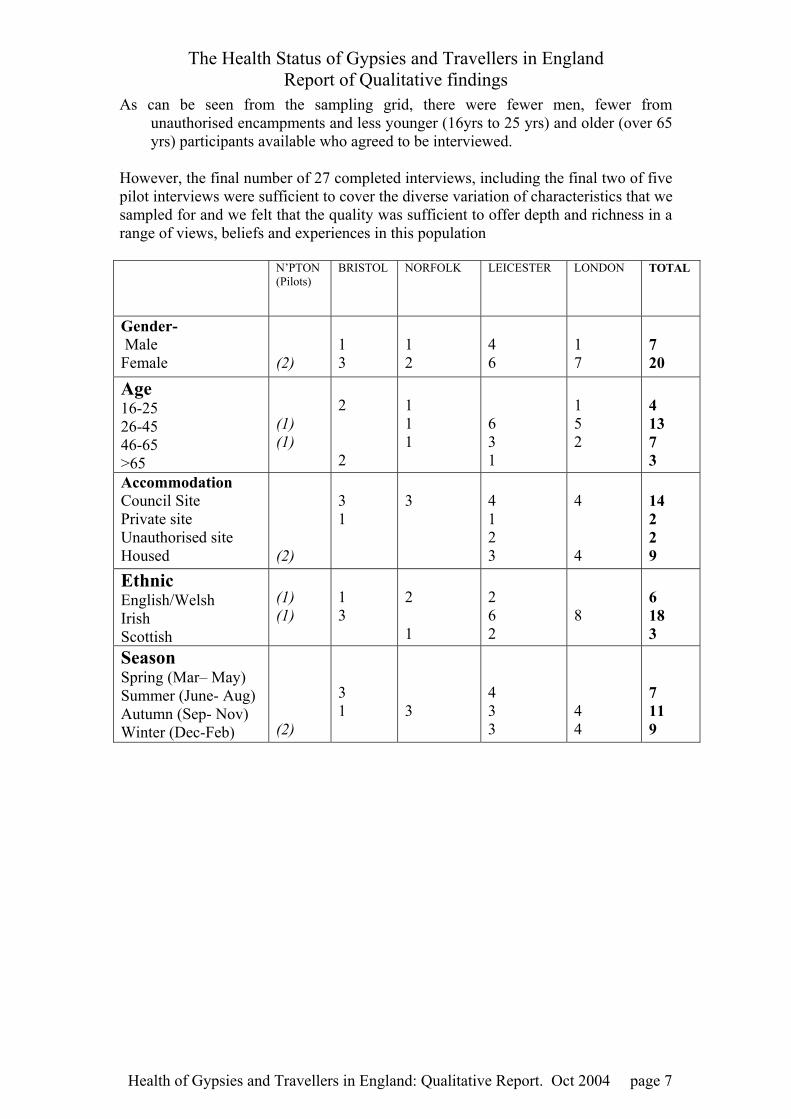
As can be seen from the sampling grid, there were fewer men, fewer from unauthorised encampments and less younger (16yrs to 25 yrs) and older (over 65 yrs) participants available who agreed to be interviewed.
However, the final number of 27 completed interviews, including the final two of five pilot interviews were sufficient to cover the diverse variation of characteristics that we sampled for and we felt that the quality was sufficient to offer depth and richness in a range of views, beliefs and experiences in this population
N’PTON (Pilots)
BRISTOL
NORFOLK LEICESTER LONDON TOTAL
Gender- Male Female
(2)
1 3
1 2
4 6
1 7
7 20
Age 16-25 26-45 46-65 >65
(1) (1)
2 2
1 1 1
6 3 1
1 5 2
4 13 7 3
Accommodation Council Site Private site Unauthorised site Housed
(2)
3 1
3
4 1 2 3
4 4
14 2 2 9
Ethnic English/Welsh Irish Scottish
(1) (1)
1 3
2 1
2 6 2
8
6 18 3
Season Spring (Mar– May) Summer (June- Aug) Autumn (Sep- Nov) Winter (Dec-Feb)
(2)
3 1
3
4 3 3
4 4
7 11 9

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 8
Table 1 Final sampling grid
Interviewed Whole Sample % Sample % Characteristics n=24 n=293 Gender: Male Female
29 71
35 65
Age group: 16-25 26-45 46-65 Over 65
17 42 29 12
24 51 21 4
Attended school ‘regularly’ as child (yes/no)
77 67
Age left school (mean years) 12.4yrs 12.6yrs Accommodation: Site Empty land Housed In temporary (homeless)
67 4 25 4
44 29 27
Has children under 16yrs 88 85 Travelling patterns: All of the time Part of the time Rarely
0 21 79
24 26 49
Anxious or depressed today (EQ-5D response = ‘a lot’ or some of the time”)
50 28
Registered with any GP 92 84 Seen a GP in past year 96 79 Smoker (current) 75 57 Long-term illness, health problem or disability that limits daily activities or work
67 39
Table 2 Characteristics of interviewed sample Access Given the mobile lifestyle of Gypsy Travellers and the various priorities arising from the demands of daily living which we knew they faced, we anticipated some difficulty in being able to carry out the required range of interviews, even if there was agreement for us to do so in principle. The researcher (pvc) was given contact details of those who agreed to be interviewed when approached by the interviewers with whom they completed the questionnaires. The researcher was familiar with Gypsy Traveller society, having previously spent several years as a health visitor with Gypsy Travellers in Sheffield. The prior knowledge gained from this experience was a useful insight into the questions that needed to be asked and her understanding and appreciation of their culture helped in engaging with participants. There was an awareness that, based on this experience, false assumptions could be made with consequent lack of exploration for deeper understanding and this was borne in mind as she recorded her a priori knowledge for

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 9
later comparison with findings. Although she did not hide her familiarity with Gypsy Traveller culture, the researcher avoided reference to her previous experience as a health care worker in order to minimise the likely probable influence on the
direction of the interviews. There was an attempt, whenever possible, to make advance arrangements to interview willing participants, often through the help of the local health visitors, but often arrangements had to be finalised on arrival in the location. This was partly due to mobile lifestyle of the participants and lack of certainty about when they would be free. Most preferred to be contacted by mobile phone, with little advance notice, on a basis of “ if I’m free you can come” or alternatively via their local health visitor, who had originally been the intermediary for the questionnaire phase of the study. However, out of the 26 days spent in fieldwork locations in order to conduct the interviews there were 38 specific failed contacts compared to 25 successful interviews conducted. The process of making suitable arrangements to conduct the interviews was often protracted and involving several repeat attempts. The most common reasons for postponement or for failed contacts were family illness or crisis, funeral attendance or the family having moved on. With the exception of 2 opportunistic interviews when it was necessary to also complete the questionnaire, the participants were readily willing to give up their time to be interviewed and appeared to appreciate the experience. The men were generally more reticent about being interviewed. An attempt to carry out opportunistic interviews with men, who had not previously completed a questionnaire proved to be problematic. One of these men did agree to be interviewed but there was an impression that he agreed in order to please his health visitor and in the event, by the time he had completed the questionnaire he had only a short time available for the interview. The limited time that families were able to stay at unauthorised encampment sites meant that it was much more difficult to follow up those who had agreed to participate in the qualitative study. The younger age groups were also more difficult to recruit for the questionnaires, in both the Gypsy Traveller group and also the comparison groups. In the case of older Gypsy Travellers there were less numbers available to recruit. The final numbers of completed interviews, including the final two of five pilot interviews, were sufficient to obtain the range of views, experiences and beliefs relating to the research questions in this population. Method and process of data collection Individual depth interviews with Travellers in their own homes or trailers, or other venue of their choice, were the chosen method of data collection. This method of data collection was chosen to ensure that privacy and confidentiality are enhanced. The potential sensitive and private nature of the subject matter did not lend itself to focus group methods as an option. However, following the initial analysis, the broad key

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 10
findings were delivered and discussed with groups of Gypsy Travellers in each of the study areas. This allowed for early interpretation of results to be tested or challenged by a wider group of Gypsy Travellers and for additional comments to
be made. When an agreed venue and time had been arranged for interview the researcher checked with each participant that the purpose of the whole study had been understood (from their initial contact for the main study) and gave further information, paraphrased from the information sheet, about the specific purpose of the qualitative study. Most participants had made an informed decision to be interviewed and had no further concerns or questions. Several made direct comments or intimated that if their health visitor trusted the research study that they could. Signed consent was obtained and a copy of the information sheet left with the participants. All but one interview was audiotaped with the participants’ permission in order for analysis of the transcripts to be carried out after each interview. The one participant who refused permission was willing for contemporaneous notes to be taken during and after the interview. A post interview record of extra information about feelings, rapport, insights and other non-verbal features of the interview was also completed to illuminate the analysis Topic Guide A topic guide (see below) was developed from existing knowledge and from initial pilot interviews. This was refined during subsequent pilot interviews, and used to ensure that relevant areas were covered to inform the research questions. Non−directive interview questions, allowed exploration of health behaviours, beliefs and barriers to access and use of Health Services. Additional issues that arose spontaneously, such as pertinent information about Gypsy Traveller identity and culture, suggestions for improved service provision, were explored and incorporated in subsequent interviews. The participant guided the order of topics covered and the guide was only used as a prompt All but the one short interview mentioned, lasted between one to two hours.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 11
Interview topic guide Icebreakers
How long have you lived here? (Leicester, Bristol etc). How long on site/road etc). How many of family around /with /near you?
Health experience How is your health at the moment/ how are you feeling? Do you consider yourself to be healthy? Could you tell me about the last time you had any health problems? (Best experience, worst experience, management of chronic illness, management of minor illness, cover attitudes; understanding; first line of action; differences in action when interviewee is unwell or their child)
Access & Use Of Health Services GP registration, Use of GP service, Use of A&E, Hospital attendance-
Outpatient; referrals- appointments. Prevention
Ways that you try to keep self and family healthy? What do you think is bad for your health? Attendance for health screening for self ( smears; flu vacs, dental etc) attendance for children ( immunisations; hearing tests , dental etc) Ante-natal care
Knowledge How knowledge is acquired. Extent of knowledge in relation to issues spoken of .
Impact Of Lifestyle on Health Impact of travelling/ living in house/ on sites, Any other factors affecting health or access to care Beliefs
Main reasons for illness and ill health? (same for Gypsy Travellers as gorgios?). Main health worries (i.e. illnesses / conditions most afraid of) What would most improve health of Gypsy Travellers? What advice you would give to friend/family member who had trouble with nerves, depression, mental problems and what would most help them?
If not raised and appropriate to ask Sexual health (STDs; contraception). Substance misuse, alcohol, smoking, drugs
Thematic analysis of qualitative data The framework approach was be the chosen method of data analysis5 . This method was chosen as it was specifically designed to answer policy related questions that allows for rigorous and transparent data management. It is a structured process of inductive thematic analysis with distinct but interconnected stages. It enables the identification of relationships and patterns in the data so that explanations and theories can be developed. It is grounded in the data, in that it is driven by the original accounts of the participants and the observations made by the researcher. A software package, Atlas TiTM, was used to enable more complex organisation and retrieval of data. After familiarisation with the transcripts, recurring themes were noted from the early transcripts. Following coding of the first eight interviews 5 broad themes were identified. The coding framework developed from the identified grouped themes was then applied to each transcript. Refinements were made during indexing of successive transcripts. On completion of indexing of all the transcripts, all the coded data for each theme was charted and sub themes were identified. When all the data had been charted, patterns, exceptions and associations were systematically examined as part of the final analytic process.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 12
Validation
The analysis was subjected to peer review at all stages of the process. Each transcript was read by an experienced member of the research team (KT). The coding, the framework, descriptive accounts and interpretative analysis were all developed using continuous peer review. The final themes were validated by study participants and their peers in a series of road shows held in each of the original study locations. At each event presentation of the qualitative study findings the following questions were asked of each group: • How credible the findings seemed to them • How transferable the findings would be to other groups of Gypsy Travellers • Were there any concerns re confidentiality from the quoted speech used There was a general consensus that findings rang true “yes that’s us”. Everyone agreed that the findings would be transferable and nobody raised any concerns about confidentiality. In addition they were asked to comment on each of a range of suggested options for improvement in health service provision for Gypsy Travellers that had come either from some of the people interviewed or from initiatives already in place in other areas. There was useful discussion concerning issues raised by these various options for improvement in service provision. The following chapters include verbatim quotes. These have been anonymised but given a unique identifier (see table). It will be noted that there are 28 people identified. This is because individual interview (F6) became a joint interview when she allowed her husband to contribute. As data from his contributions have been included he is identified also . (M3)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 13
Cultural Beliefs and Attitudes
Introduction Keesing has defined culture as “systems of shared ideas, systems of concepts and rules and meanings that underlie and are expressed in the ways that human beings live”. Each person within a group learns the shared perceptions of the world and how to live in that world through these cultural guidelines, although these guidelines will differ for different members of the group according to their various social categories within the group e.g. men or women, young or old, wealthy or poor, Irish Traveller or English Gypsy etc. Many members of a group will also absorb some of the cultural attributes of the wider society. Gypsy Travellers are not a homogenous group, and there is no suggestion that their culture is the sole explanation for the way in which they experience health and use health care services. There are many other factors beside individual experience, such as educational attainment, socio economic status and environmental factors that will influence health and attitudes to health services. However, cultural background is one of these important factors and there was a strong overriding theme from the interviews that highlighted the cultural identity of Gypsy Travellers. This chapter is an analysis of the features that emerged during interviews that are central to the culture and their underlying beliefs.
“Accounts of health and illness are more than a description of one’s physical condition and more than views about what people in society should do to avoid disease. They also articulate a person’s situation in the world and indeed articulate that world in which the individual will be held accountable to others” ” 6
Cultural beliefs and attitudes Stoicism, self-reliance, and family involvement in health are particular specific beliefs that appear to be products of the shared culture of Gypsy Travellers. Other beliefs were also offered spontaneously in the context of accounts concerning health and health care that will be covered in the next chapter. It is necessary to comprehend the strong sense of cultural identity and the wider context of their lives in order to put their health experience, use of, and access to health services into context. Some of the respondents themselves spoke of the desire for health workers to have a greater cultural understanding of themselves as Gypsy Travellers and this chapter addresses that need. The importance of this topic was evident from the frequent and spontaneous talk abut what it meant to be a Gypsy Traveller and the strength of feeling evident in many of the comments made. It is not possible to do justice to the full range and richness of beliefs within the confines of this study, nor is it possible in this report to attempt to explore these beliefs in depth or attempt to build theory. Instead important underlying factors are described that need to be understood and considered by health care providers when

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 14
deciding on appropriate responses to the health and health concerns of Gypsy Travellers.
The following aspects of Gypsy Traveller culture are part of the discreet culture that is known and implicit to those within the culture but not necessarily shared with or evident to outsiders. This chapter is the ‘cultural lens’ through which the other chapters can be viewed and understood in their wider context.
Identity “it’s who we are” Travellers interviewed in this study perceive themselves as a distinct ethnic group with a strong sense of identity and of belonging to a Gypsy Traveller culture Although Irish and Scottish Travellers and English Gypsies were interviewed, their self-identity was as a Gypsy Traveller first and foremost “ we didn’t ask to be borned into Travellers. We didn’t ask to be brought up this way. It’s like my kids, they didn’t ask for it, but it’s who we are” (F14) The respondents who spoke of trying to maintain their identity emphasised the importance of ‘cultural codes of conduct’. The most frequently mentioned ‘rules’ concerning gender roles and sexual behaviour have particular relevance to health and use of health services. Although several respondents spoke of more freedom for the younger generation of Travellers there were certain absolute ‘rules’ that were still spoken of, such as the importance of remaining a virgin until married. One young Traveller explained “ but if she was an English girl she is going to have more than one man, that’s her way and up to her… but like a Traveller girl.. gets married to the boy” (F5) Men also hold this view, “not all Travellers, but most Travellers believe when you marry your wife, your wife should be pure, you know, she should be a virgin as such” (M4 ) Identifying features that defined a ‘Traveller way of life’ were seen as important for keeping the culture and passing it on to the children. Some respondents expressed concern that their culture is dying out and this was most commonly attributed to moving into houses and giving up the Traveller lifestyle. “…it’s obvious Travellers is changing because they’re moving into houses and this and that. Their lifestyle’s changing...they’re not sticking together like what they used to years ago. They’re just all like housed people.” (M7) Some Travellers who feel that the pressures are too great and change their lifestyle as a result, face the added threat of loss of identity and a feeling of ‘being outcast’ from their own community. There was an acknowledgment that any culture is dynamic, rather than static, and this appeared to some respondents to be a threat in itself. “ young girls are not allowed to go and mix…that’s not a mistake, you’re not allowed to make a mistake like that, … they’re sort of outcasted …They know the rules and regulations. But girls are changing; they’re not like they used to be when I first got married. They just won’t take it now…when I got married; I always say I left a boss to get a boss. I never had them in between years where you was your own

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 15
boss…We never had any in between years to be carefree. So they tell their children to do it.” (F9)
There was an expressed fear of a loss of their culture arising from a change of lifestyle “I started to mix more with Gorgers as we call them, and I seemed to be getting more and more in their way of life than a Traveller’s life.” (M1) The threat of this loss is seen as being partly imposed by a society that strongly rejects them. “It is frightening being a Traveller love, because no-one wants you…if they could, they’d build a hole and they’d shove all the Travellers into it and they’d just bury them all there. If there was no law they would do that” (F14) One result of this threat is for Gypsy Travellers to make efforts to maintain their separateness and to attempt to continue their traditional lifestyle despite the threats. This appears to reinforce their cohesion as an ethnic group “ at the end of the day Travellers are an ethnic minority and we do live in our own way, we do speak our own language, yeah, we do all that. So we should be treated like that… we want equal rights the same as anybody else” (M4) However, the extent of the racism that they experience and anticipate in all areas of life results in wide mistrust, and there is often a felt need to hide their identity in order to avoid discrimination. “they try and avoid [giving] the address, they try to pretend they’re not a Traveller in other words… but it don’t make no difference, I think they just look at you and they know who you are” (F9) The dilemma posed by whether to deny or reveal identity was illustrated by one respondent who had been trying to get her child into a Catholic school- “I said [to her husband] ‘you go in’ because they know I’m a Traveller. So I said, smarten yourself up and go in…The head teacher copped he was a Traveller and he said ‘yeah I am, I don’t deny who I am’. You won’t say it, but if someone asks you you’ll say it” (F14) Several Travellers interviewed were of mixed parentage or had some relatives from the settled community who had ‘married in’. The sense of a separate Traveller identity was as strong for Travellers of dual heritage “I’ve had my feet in 2 camps all my life” and “she’s sort of pulled 2 ways”, but clearly caused some conflict for individuals as to which culture they belonged to or were seen as belonging to. Racism and discrimination “in people’s eyes you’re a nobody and that’s it , honestly it does hurt” The experience of racism and negative stereotyping was pervasive, with many examples given from all areas of life, and was automatically anticipated as result. “ you expect through some course of the day to face that racial thing , every day of your life” (F9) Reactions to the experience of discrimination varied between:

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 16
defensive hostile reactions, often in expectation of discriminatory treatment “ oh that’s alright then, ‘I’m only a Gypsy, I’ll come to you when I’m dead’ and I put the phone down on ’em”,
(F2) resourcefulness in overcoming discrimination “ that was all lies, I only said that cos they didn’t… to make them do something”, (F14) avoidance of encounters with unknown ‘Gorgers [non Gypsy Travellers]’ “ you know the ones you can go to”, (F13) to obvious despair and impotence at the inability to overcome racism
“ it makes you feel that no matter what happens, there’s nothing you can do about it”. (F13) The overall widespread outcome was a mistrust of others and this mistrust was demonstrated even when unexpected positive treatment was experienced “ and then I thought perhaps they’re only putting that as a show on” (F12) One respondent expressed an attitude in response to the alienation he experiences that illustrates a defiant stoicism and resistance to submission. “ you are what you are and that’s it ….you’ve just to accept who you are”
(M3) Generally, the widespread experience of racism and mistrust was translated into an expectation of discrimination in encounters outside the community and was an added reason for keeping amongst their own community, and avoiding isolation in houses. “ we had one neighbour complaining because my dog was barking and the dog was only 6 weeks old, and it wasn’t nothing to do with the dog, it was the sheer fact that we were Travellers…..so I’d rather be with your own kind of people, you know, people that moves with your life” (M4) Nomadism “ it’s in the blood” Most of the respondents were living either on sites or in houses at the time of interview, but many of them expressed a belief that travelling was an essential part of their lifestyle. One Traveller pointed out that the reason Travellers have to travel is for work purposes “ to earn the money” but he also expressed the feeling that travelling was a way of life “…they can’t stay in the same place , do you know what I mean? It’s a way of life. It’ll never be changed: (M4) Others expressed acute loss at no longer being able to travel “ you miss it for the children …. They’ll kind of losing our culture the children over it… because it was our proper culture” (F13) The suggestion that travelling was inherent was illustrated by stories of Traveller children who had been reared in houses but later in life took readily to living in a trailer. However, Travellers did not define their identity by whether they physically
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 17
travelled. One respondent digressed in the interview to emphasise that her children were Travellers regardless of whether they travelled. “ these 2 Gypsy boys [her sons] , because they’d never travelled, but they’re still
Gypsies, they’re still travelling boys, you can see that…” (F11) Freedom, choice and socialising were seen as the most important benefits of travelling, as well as being a necessity for men to obtain employment. “ sometimes you see people you haven’t seen for years and then they welcome you with open arms” (M1) Negative aspects of travelling such as being continually moved on, lack of access to basic facilities and difficulties in accessing services were also mentioned and were often reasons given for abandoning the travelling lifestyle for all or much of the time, but the strong sense of loss for many was evident. “You’re just as well stay in the one place and just learn to live every day because there literally is nowhere out there that you can stay and have a week or fortnight and move on again…” (F9) In the past when most Gypsy Travellers still travelled there was regular connection with extended family, but also the choice of when to move away. “ used to be lovely.. it used to be different because you’d get two or three weeks in one place and you’d be with all different families and just nice..” (F5) Since nomadism is associated with freedom, the sense of loss of freedom was described as having a profound effect on the psyche of Gypsy Travellers “because they’re used to sort of getting up in the mornings, seeing people all the time. You get up in the morning and you don’t do it, they call that lonely. And when you get lonely so you’re getting depressed aren’t you” (F18) Some respondents expressed a strong aversion to house dwelling as an alternative lifestyle because it seemed so unnatural ‘ it was like the place was haunted… all the creaks , noises and the stairs, couldn’t stand it, could never live in a house (F16) For others, living on a site felt equally inappropriate and they still felt the need to move on because they became “ fed up being in the one place all the time” (M1) Kinship – family ties “ kids are everything to Travellers, that’s why they get married for it’s to have kids and rear children up” The importance of close extended family is paramount in an otherwise hostile ‘world’ and is a major feature of Gypsy Traveller culture “ we come from a very big family community love, very big family,… And we’re all very close” (F13) Respondents spoke in terms of their goal and purpose being to raise their family and in being there for them “ kids are everything to Travellers, that’s why they get married, for it’s to have kids and rear children up”. (F19)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 18
Although positive views were expressed about availability of contraception by some Travellers there was still frequent mention of a desire to have several
children and of children being a major cherished feature of their lives. “ when I was growing up I was looking after kids anyway, always looking after kids, if it wasn’t my brothers and sisters it was my cousin’s kids and friends kids…I don’t know what I’d do without them to be honest (F19) The focus on the children’s emotional and physical needs, and the warmth and respect shown towards children were observed in women and men during the interviews. Utmost patience and calm was observed with crying babies or toddlers. It was particularly striking that not a single respondent ever suggested any feelings of exasperation or talked about any need for a break from the children, even among those who were depressed or anxious. One respondent explained that having children around her helps her to stay healthy “ being around the children. I think you feel more alert when the children are around you and you’ve got the courage to go on every day with them…I don’t think I’d want to live without them” (F12) There is a cultural expectation and desire for the family to give support and care to each other, “we look after our own ourself”, although there is also a desire to avoid burdening each other “ my family is there like, but you’ve got to help yourself” Roles within the family were clearly understood. The women saw their roles as being good mothers and it was important to be seen be fulfilling this role. An older respondent describes the division of roles between her and her husband “ Your work’s important… and keeps you going… [bringing up family] that was my work…I used to work, look after them and keep them clean and feed them. He was the reins, to put them in their place and what they had to do and what they did and they listened” (F17) The respect and deference to older relatives did not appear to diminish as they aged “they’ll come to me and they say ‘what do you think of this Mum, and what do you think of that’, and I tells them” (F17) The size of families led to there being close ties to other Traveller families by marriage, especially as there was an expressed preference by many for keeping relationships within the Traveller community “ everybody, somewhere along the line has got someone who’s married into one family or another. You’re tied somewhere along the line” (F9) For some this was a positive feature that meant a strong family support network. One respondent spoke of having over one hundred cousins and over two hundred second cousins “ and we’re all very close” (F13) However for others it was more difficult to maintain contact with kin family

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 19
“ I like to be with my side as well as his side but sometimes my husband don’t do it that way, he wants to be all his side and not my side” (F10)
There was some evidence of awareness of the possibility of genetically inherited conditions arising from cousin marriages .One respondent expressed her opinion that certain families were known for this and spoke of families where several family members had the same genetic condition “ the X’s now, they love marrying into their own” but that “not every Traveller does it” (F5)
There was an apparent ambivalence about living among a close-knit family, in respect of the need for privacy. This was illustrated by several examples of ‘conspiracy of silence ‘ in order to ‘protect’ family members from distressing news or else not to present as a burden. One great grandfather suspected that his family was keeping the suspected knowledge of their child’s drug abuse from him “ I think the family’s keeping it quiet, they won’t tell me… I’m sure now that there’s something wrong” (M2) Such examples demonstrate a tension inherent in the lifestyle of many Gypsy Travellers: as a community of Travellers versus ‘outsiders’ there is mutual support but within the community there is sometimes less support due to the desire for privacy and the perceived risks of sharing personal problems. Privacy “it’s just the way that we were brought up, very very private, Privacy was a feature that Travellers identified as pertaining to ‘how they were brought up’. For one young Traveller mother, understanding of the need for privacy was the second thing that came to mind (after religion) when asked what would really make a difference in terms of cultural understanding “ and about contraception, and about being pregnant, that’s really embarrassing for us, that’s like we keep that private for ourselves and find it embarrassing going to the doctors about things like that” (F19) Emphasis was given to the fact that this was perceived as a cultural feature and not an individual trait, and neither was it age or generation related, “ maybe it’s just through the way we were brought up, it’s our kind of shyness and embarrassment whatever” (F18) References to ‘upbringing’ relate to the ‘cultural codes of conduct’ regarding gender roles and expectations. The secrecy and restrictions on relations with the opposite sex appear to increase the embarrassment. One mother described how her daughter had reacted to a male teacher giving sex education lesson to her class “she just got up and left”. The rules appear to be more relaxed for boys. One young father, who stayed on at school later than most boys, said he attended sex education lessons “because I was a boy, if I was a girl I wouldn’t have done… just that boys will be boys” (M4)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 20
However, there were different aspects to the perceived importance of privacy. Embarrassment at receiving physical personal care or needing intimate examinations was cited as something to be avoided as far as possible. One female
Traveller highlighted the significance of this attitude by dropping her voice to a whisper when describing her need for such care “ and personal things, like, I need washing and stuff.” (F1) No men mentioned privacy in relation to embarrassment, and gave different reasons for avoiding access to health care. A young Traveller father refuted the idea of embarrassment preventing access to care in the context of a hypothetical sexual problem “I’d go straight to the Doctor and I’d tell him, because in my status I’m married you know, so the fact that I had some problem I’d go because of sex with my wife” (M4) However, one Traveller woman spoke for her husband and described his embarrassment at the thought of having nurses wash him etcetera as “It’s pride”. (F9) Privacy in the context of avoiding gossip is also important and connected to concern about impressions formed by others in the community. “ you don’t want people knowing your business; your own business is your own business” (F19) This fear of gossip is also closely linked to lack of trust particularly regarding confidentiality in accessing services “ privacy’s the main thing- no one else would know about it” (F19) However, shame was another reason that emerged for keeping things to oneself. One mother, describing the prevalence of drug use, explained “ well the ones I know, it’s never talked about. Bury it under the carpet. It’s a shaming thing ‘oh my boy musn’t do that’” (F9) The concept of privacy is also closely linked to independence and self-reliance. When discussing the merits of living on someone’s land as opposed to having his own ‘plot’ on a communal council owned site, one male Traveller explained “you still haven’t got really your own independence…..what I mean, we liked our own privacy, which we can get here now” (M1) Religion “ Religion is a big part of our lives” The comfort and strength derived from religious belief and practice is seen as fundamentally important. “ everybody prays to the Lord if they need him, don’t they” (F12)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 21
Religion is an integral part of the experience of the lives of many Travellers, particularly Irish Traveller Catholics and evangelical Christians across all groups. Apart from family, religion is the other ‘comfort and support’ in the lives of
many Travellers “ all they have to turn to is God and religion, and hope that it will get better” (F18) Most Irish Travellers spoke of their strong Catholic upbringing and faith. Some placed great belief and hope in the ‘curing people’ and of going to great lengths or of great desire to travel to see specially ‘holy’ people for their intercession. “ You know, my father in law, he was very ill and he found the curing people helped a lot…he found it helpful, really helpful and his wife found it helpful…that’s like that’s a part of our religion. That’s what we believe in” (F14) The importance of going for healing to pilgrimage shrines such as at Lourdes, Knock or Medjugorje was also emphasised “ I just want to go for like a holy weekend, just pray…” (F1) One respondent, speaking of her belief in faith healers and going to ‘Lourdes, Knock and places like that, explained “ if you pray hard enough and like Padre Pio and all the other angels and saints and all the rest and they sometimes things do come true” acknowledged that “sometimes it’s just going to be in the mind.” However, she added “ it helps anyway, It doesn’t hurt you to believe anyway, so yeah , we do have strong belief in that kind of thing” (F18) Increasingly other Gypsy Travellers are turning to Evangelism (‘Light and Life’) or ‘born again Christian church’ and find this a support “ I became a Christian and Jesus put that peace in me. You know, when I’m content I could live on top a mountain. As long as I can get to a meeting, you know what I mean, and fellowship- then I’m content” (M1) Many Travellers of any religious persuasion feel that their destiny is determined according to ‘God’s will. “ if God borned you to have a short life , you had a short life; if He borned you to have along life you’d have a long life- nothing you could do to alter it’ (F17) Views though, are often polarised and for other Travellers, ‘born again Christians’ in particular, may be viewed with suspicion. “I know there’s hundreds and hundreds of Travellers turning into these Christians and personally myself, I think they’re hypocrites ….I think they’re clutching at something to try and change their life” (F9) This can create a divisive and anxious situation for families with mixed beliefs, particularly those where there is a belief that other family members need to be converted to be ‘saved’ “ My mum and dad are Christian… they’ve opened up their hearts and let the Lord come in… the Lord will help them more than he would me … now they’ve let the Lord go in their heart … I would be wanting to do it, but me husband won’t come… he won’t be one, he don’t believe in it.” (F10)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 22
Education “…bottom of the food chain and stuff because they don’t know nothing, don’t know how to read , don’t know how to write, don’t know how to use computers ,
don’t know anything” (F19) Respondents clearly express their sense of disadvantage that results from non- literacy ‘Form aversion’ was frequently mentioned in association with lack of formal education and poor literacy. There was evidence that although an inability to read and write was often regretted it was accepted that it had been an inevitable result of being a Traveller. Older respondents explained the lack of opportunity for education for most as school children. Those who were travelling found it difficult to access schools and there were also family priorities “ I did go to school but I didn’t go much no, because I was the oldest of the family like” (F17) Some older respondents who had received some formal education explained how the family had needed to given up travelling in order to achieve this opportunity “ we came to Manchester and then my mother and father got a house . Before that I was travelling and that, and none of us that time knew how to read or write or anything. So I went to school for about 2 or 3 years. I learnt to read in Manchester so” (F18) One older Traveller woman expressed the suggestion that an older Traveller’s identity might be questioned if she had been educated “ I mean, Mum was educated, though she was real Gypsy she was educated” (F2) However younger parents explained some of the current external barriers that still exist. One barrier described was the frequency of moves, which for many respondents was forced rather than chosen “so like my kids, they lost a good bit of education…but like when you’re doing that all the time and moving, your kids cannot learn to read and write” (M7) The difficulty for some of getting their child into a chosen faith school was another barrier that was sometimes seen by respondents as resulting from racial discrimination. Equally the risk of Traveller children being discriminated against or bullied in school was another barrier “ I wouldn’t like him to go to school by himself. They’d call him Gypsy this and Gypsy that. If it was a case of him going to school by himself or having a group of Travelling children being taught on the ground, I’d rather have that” (M4) Although more of the younger Travellers had gone to school there was still the traditional expectation that you left school at a younger age to take up expected roles in the family Exceptions were considered noteworthy “I went to school till I was 12, so I know about these things…I suppose I’ve got the upper hand a little bit because I went to school a bit longer than most of them” (M4)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 23
However, observations were made about the changing world and need for education “ I mean if you’ve got to have degrees now and O’levels to be a road sweeper. Anybody can use a brush on the road, but you have actually got to have O’levels
to get that type of job. So I can’t, I just don’t see much future for Travellers to be quite honest” (M3) Embarrassment of explaining an inability to read or write was also accompanied by a fear of being identified as a Traveller and was an explanation for avoidance of such situations. This also has implications for reluctance to attend new health care settings until absolutely necessary. “ you’ve got to do all this on forms and or whatever, and say you can’t do that, straight away you’ve got to tell them who you are” (F18) Cleanliness and pollution concerns “ you always keep the place always clean” The importance of cleanliness and hygiene was evident among the women interviewed in this study. Interviews were often timed to make sure they did not interfere with this daily task. The importance of cleaning was not seen solely as a precaution against pollution or infection, but was also a matter of image and pride, and was central to the importance of social relations. It was seen as an aspect of how you are judged by others and an important feature of identity “ you always keep the place always clean, because somebody might come and visit you and it’ll all be dirty” (F5) The centrality of cleaning is emphasised by respondents who mention it as an aspect of keeping healthy. One respondent who is suffering the loss of mobility due to a chronic disabling illness bemoans the consequences, as she says, “ Good health is everything you know … I was so unlucky, I loved life, I loved life, I love the cleaning, I love the cleaning” (F1) The link between cleaning and health was emphasised in answer to a question posed about actions to ensure that they or their families stayed healthy, the first thing that came to mind in response for this respondent was “ normal things is it? Clean up. Make sure things is clean and place is clean” (F15) The importance of having a clean and hygienic environment was a factor for a respondent who once needed to go into a refuge but because it was “scruffy” said, “ I couldn’t cope with it”. Another explained the importance for her well-being by saying “ like if this place wasn’t clean, I’d be depressed” (F4) Hygiene also featured in relation to food and one older Traveller explained her caution about the food she bought and about ‘eating out’ She explained her concerns by commenting on a TV cookery programme where meat was being cooked “took it straight from the cellophane and dropped it in the pan. And you think to yourself they that does the packing, how many hands do go through them ? Eh and they put it straight in the pan!” (F17)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 24
Pride in home and personal appearance
“You always keep the place always clean because somebody might come and visit you…” (F5) Although links are made between hygiene and cleanliness, the link between cleanliness and appearance remains strong. In the case of this older respondent, when the ability to carry out all cleaning tasks are lost, (‘I’m still able to dust and do, but can’t do anything like the windows’), she ensures that her home is still presentable “ but I’ve got good daughters see, she comes down every so often and does a good clean up for me” (F17) In fact the smart décor and cleanliness of all the homes visited for these interviews are notable features that indicated great pride in presentation. The intimation that presentation is important because of people who may visit, and may therefore judge by appearances, extends to physical appearance in the eyes of some respondents. One respondent who has a daughter with a facial deformity emphasises how well she is accepted outside of the home and includes in her list of attributes that make her acceptable to others “…she takes a lot of care about her appearance , doesn’t want to get fat , dresses nice , likes make-up…” (F16) Although her child has other disabling symptoms such as severe hearing impairment, this mother exhibited most distress about the implications of choosing to allow her daughter to undergo corrective surgery. Among the factors that most distress her is “ the mind part of it”, her fear that in choosing for her to have the operation, her daughter would think she was ‘not accepted’ the way she looks now. “ I just don’t want her to think I don’t like her the way she is” (F16) There is a general emphasis on the importance of appearance and presentation that appear to be linked to psychological well-being and to feeling being acceptable to others. This young Traveller illustrates this link “ you’ll always make sure to have make-up on and fix yourself because you don’t know who you’re going to see (F5) Another mother expresses her pride in her daughter but also illustrates the importance of appearance, when explaining that her daughter has a particular health problem (not obvious visibly) “ ah she’s very pretty though, eh? [then to the child] ‘Are you a pretty girl? Show the woman your nice eyes’” (F13) The significance of dignity and pride is another link with the importance of appearance and presentation in relation to health. This daughter who feels that her mother should not have undergone amputation particularly illustrates this “ I mean she was dying anyway, they could have let her the dignity and have a little bit, but to have no feet and no legs …” (F2)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 25
The pride in having a presentable home and appearance are consistent with the dignity and resilience that Gypsy Travellers value in them. To fail to maintain these standards would be consistent with ‘giving in’ or losing control.
Food and appetite “ Travellers love fat children, they love fat children” Hygiene was not the only important consideration concerning food. Making sure that you were a ‘good parent’ was closely associated with the nurturing aspect of food provision “ …‘I’m not a good mother, she’s hungry and all this” (F4) “even now with Travellers, when there’s a miniature child walking around ‘that child’s neglected’, ‘that child never got food’, ‘that mother doesn’t know how to rear her own child’” (F5) The importance of tonics was often mentioned in the context of giving a child a good appetite so that they would eat more. Although for many, a big child was viewed as a healthy child, one respondent mentioned limits to this concept when describing a particular extended family who she felt went too far by giving their children ‘Complan to make them big’ “ and they’d be in the pram and be as big as me!” She went on to express concern about the health problems that such children would have in later life. The same view of big being healthy did not extend to adults. Most Traveller women spoke of being very concerned about being overweight. “We’re obsessed with being overweight” However, the desire to be thinner was attributed to body image and not health reasons “ like if I was really overweight I know it would really bother me…I’d feel like fat and I wouldn’t feel nice… it’s how I’d look” (F19) The type of food provided was often of secondary importance to making sure the children were not hungry. This may be partially explained by the recent history of some Traveller families’. One older father of 12 children explained “ my wife now , God Bless her[ deceased] , just like my mum before me , they were used to big cauldrons of food you know. Anything you could get- loads of meat, loads of potatoes, throw it all in the pot like,…. A hungry child‘ll eat anything” (M2) Self- reliance “ you’ve got to be tough and get on with it” Self-reliance, closely associated with resilience, were cultural characteristics in which Gypsy Travellers took great pride. These traits were seen as arising from adversity and exclusion. There are a number of recollections of past adversity, when fighting for survival (literally and metaphorically) was a necessity. One woman who was
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 26
widowed as a younger woman and left with eight children under the age of seven explains
“… I always had a hard life … when you have to cope, you have to cope” (F8) General mistrust in wider society reinforces the cultural belief that one should be ‘tough’ and not ‘give in’ to difficulties and worries There was evidence of this trait being fostered at an early age. One young Traveller father, who displayed real affection for his toddler child, simultaneously said to him, almost with pride, when he had fallen and banged his head “you’re a tough man aren’t you” (M4) This attitude towards stoicism and self reliance causes some ambivalence for this respondent however in whether to allow her children to experience hardship in order to make them strong or to make things easier for them and give them opportunities that she had been denied. She explains “ when I was like my daughter , now I fetched her up to be a bit softer. But I think sometimes at the end of the day you’re not doing them any favours. Because it’s still hard but you’re trying to cushion it, soft for them and make life easier for them” (F9) However another father, who had earlier spoken of how he had been reared to be self -reliant explains why he was rearing his children in the same way “Me and their mam we can help them, but at the end of the day, me and her aren’t going to be here all the time for them, one day we’re going to go too… They’ll have more hardship because it’s getting harder now….” (M3) A belief in working for oneself rather than paid employment is another aspect of self-reliance. Families spoke with pride about their men’s work ethic and saw it as an absolute priority for boys to learn how to earn their living “ when young Traveller boys15,16 years, they’re more interested in learning how to go out and earn a living, whereas at 15, 16 most kids up and down estates are bunking off school …………a 15,16 year old in a house ‘ll get a factory job,…. whereas when you’re a Traveller you’ve got to learn” (M4) Motivation and accomplishment “ I don’t care about myself, it’s my kids” There is an expressed urgent need to be there for the children. This reflects the strong role expectation and sense of duty in being a good parent by rearing and protecting the children from the many hardships that they expect them to encounter. This respondent, while describing how her children recognise when she is upset, stresses the indications that she has succeeded to date in being a good mother “ they [her children] do little things to make me feel ok and that makes me feel good , like I must have been doing a good job” (F16) The value placed on the children’s well being is also of fundamental importance, and fear of any harm coming to them underlies such remarks as this mother made.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 27
“ I don’t care about myself, it’s my kids” (F14)
Men are strongly motivated to provide for their family and take pride in their independent work ethic. They also try to make sure that their son’s follow their example. They compare themselves favourably to settled families in this respect and see it as protection from falling into bad habits. A female Traveller of dual identity, discussing differences between Travellers and settled people, admired this trait “ Travellers are good workers” (F5) There was a favourable attitude to work, whatever the conditions. It was also seen as a beneficial character building opportunity for young men, particularly in encouraging resourcefulness. There was a perceived threat of cultural erosion in this regard from moving apart from other Travellers by moving into a house. The threat was seen as the lost opportunity to develop initiative, resourcefulness and motivation as modelled by older Travellers and taken on board by the younger ones “ the boys more or less learned how to earn a living of all the other Travellers because if they was doing a day’s work, and the boys with them , they’d say ‘come on’ and it just , they’d teach each other what to do and how to do it , so they can always turn their hand to something . And then when they were old enough and got married, thank goodness, they were capable of thinking for themselves” (F9) Attitude to time and an apparent sense of urgency is a significant aspect of motivation Time appeared to be a paradoxical concept that featured regularly in regard to cultural factors. Time spent with people and the importance of listening was frequently emphasised, particularly in regard of desirable characteristics of health workers. However, conversely the sense of urgency and lack of time was emphasised in the context of the lives of Travellers. One male Traveller tried to explain this in the context of life on the road compared to life in a house “like, say, in the house , if you’ve got something wrong with the motor or whatever, you’ll just leave it , ‘I’ll do it tomorrow’, but when you’re in the caravan it’s ‘oh I better do that’ and you’ll go out and do it, you know? What I mean like, you’ve more go in you, I don’t know, you’ve got to do things more when you’re in a caravan than you have when you’re in a house” (M3) His wife agreed “ you can’t put it off for a day and say ‘Ill do that tomorrow, it’s got to be done when you’re in a caravan” (F6) Keeping busy and therefore not having time was also used as a coping mechanism by not thinking too much about adversity or giving in to it “ I ain’t got time to complain” [about troubles]. Control and self-determination “Somebody can be stressed out over something that can’t be changed you know” (F11)
A need to exercise control is closely linked to the described belief in self-reliance and resourcefulness as necessary traits for survival and well-being. Lack of autonomy underlies the need to exercise some degree of control in any given situation where one

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 28
has few choices in life. One of the hardships frequently described by the respondents in this study is the lack of control that Gypsy Travellers have over their destiny, in light of policies that restrict their self-determination and authorities that
exclude them in various ways. The sense of being powerless is a frequent theme that arises in the context of being unable to freely choose a preferred lifestyle. One way in which this is manifested is in the belief that succumbing to an imposed or alien way of life and giving up the will to fight as a result, will lead to dire consequences for Travellers well- being. The impotence felt by such unequal power relations result in despair for some respondents, while others resist domination and fight hard to achieve as much control as possible. One respondent, who talks specifically about “ having some control over your life”, explains how her father exercised some control when the police failed to compromise and used their power to force him to move on “if they insisted that we had to move ,he’d say ‘well I don’t mind what you do about it old son, but we’re staying here, we’re resting tonight, we’ll be here tomorrow’ because he used to take the cartwheel of….and chuck it in the pond. And so we didn’t feel victimised or picked on because, like I say, we used to speak up for ourselves” (F11) Another aspect of autonomy is the need to be able to demonstrate outward signs of success. Demonstration of success and accomplishment is the reverse to displaying weakness or revealing hardship and in a sense appears to be a means of fighting against adversity and retaining a sense of self worth. One respondent, after describing how her father became a “different man” [depressed] after he had moved into a house, explains how the need to “keep up with the Jones” with outward signs of success in the form of “tackle and cars and diamonds” could be a motivating and positive aspect of Traveller life “ you’ve got to keep up with the Jones’s and I think when you move in a house it takes some of the pressure off. If you don’t mix with the Travellers so much because of, you know we call them Gorgers, they’ve still got ambition and right nice things but they chill out …they haven’t got anything to prove after a while and I think they just enjoy a laid back lifestyle, cos they’re not getting up every day of their life and going out there … haven’t got to fight so hard and I think eventually they were just content to get up, earn a wage, pay the rent, go on holiday once every so often and whatever and that done them. The ambition was gone and they didn’t want to try to keep up with the Jones’s or get this and get that. And they just give in” (F9) Conclusion Travellers interviewed in this study perceive themselves as a distinct ethnic group with a strong cultural identity. Fear of the loss of this cultural identity contributed to their cohesion as an ethnic group. The threat to identity is seen as being partly imposed by a society that strongly rejects them. One result of this threat is for Gypsy Travellers to make efforts to maintain their separateness and to attempt to continue

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 29
their traditional lifestyle. However, the extent of the racism that they experience and anticipate in all areas of life results in wide mistrust, and there is often a felt need to hide their identity.
Some Travellers, who feel that the pressures are too great and change their lifestyle as a result, face the added threat of a feeling of ‘being outcast’ to an extent from their own community. When encounters with wider society are necessary, there is a pattern of anticipatory defensive and hostile communication on the part of Travellers in expectation of the racist behaviour that they have become accustomed to. Poor access to education and resulting low literacy levels further compromise formal communication. These factors, alongside poor cultural awareness on the part of settled people, lead to difficulties when Travellers need to engage with services. Avoidance is another strategy for dealing with these difficulties. The importance of the close extended family is paramount in an otherwise hostile ‘world’. In the past when most Gypsy Travellers still travelled there was regular connection with extended family, but also the choice of when to move away. Privacy and freedom were both possible. There is a paradox today for many Travellers who now live most of the year together on a site. There is rarely much choice regarding who they can live amongst. They are living so that privacy is not possible, and feel restricted in that they cannot easily connect with wider extended family members. Such close living compromises the privacy and also the freedom for which many Travellers express a need. Families in houses are more likely to achieve privacy, but the cost may be isolation. These factors all have implications for how Travellers seek support when they experience personal difficulties, including ill health. Whereas there is a cultural expectation and desire for the family to give support and care to each other, there is also a desire to avoid burdening each other and to be self-reliant. There is also an expectation that one should be ‘tough ‘and resilient and therefore not ‘give in ‘ to difficulties and worries. Self-reliance and resilience require behaviours that may prevent Travellers from seeking the help and support that they need. Apart from family, religion is the other ‘comfort and support’ in the lives of many Travellers. For Irish Travellers, in particular, religion often plays an important role in their lives. Religious belief can provide explanations that can be ‘accepted’, and may account to some extent for the fatalistic attitude to adversity seen on the part of some Travellers. For most Travellers however, religious belief is a source of hope and of comfort. Some Gypsy Travellers are turning to Pentecostalism and find this a support. Views though, are often polarised and for other Travellers, ‘born again Christians’ may be viewed with suspicion. This can create a divisive situation for families. Amongst Travellers, there are various cultural beliefs that have implications for health, such as hygiene and pollution beliefs, views concerning the nurturing aspect of food provision, and attitudes about privacy. Without this background knowledge and an understanding of these beliefs, there is scope for great misunderstanding. These themes will be explored further in connection with health in subsequent sections.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 30
Health -related beliefs and attitudes This chapter picks up on specific beliefs have been touched on where they specifically relate to the health issues discussed. Other beliefs were also offered spontaneously in the context of accounts concerning health and health care. These struck powerfully as having a specific role in improving the understanding of health-related behaviour. The purpose of this section is to give space to those beliefs, in order to describe their impact. Attitudes to health services
“ to be honest we didn’t believe the doctor so we’ll just do our own thing”
A society that demonstrates widespread hostility towards them, and has done for many generations, strengthens the belief among Gypsy Travellers that they should be wary, and slow to invest their trust in outsiders. The reality, according to the accounts of most respondents, is that the frequency of racist encounters in different areas of their lives do have a significant adverse affect on the psyche and fuel a general mistrust of settled people, particularly those in authority. This is particularly well illustrated by this women’s description of her experiences. She describes sample conversational exchanges with non-Travellers “ lady, please may we please use your toilet?”- “ No, it’s out of order, you can’t use it” “ I’m pregnant” - “No you still can’t use it” “Even when you’re pregnant you know? that’s when people put away half the trust that you’d have in people, you know. It’s awful…they make up a hundred excuses, they won’t actually say because you’re a Gypsy…” (F1) The general mistrust of non-Travellers in wider society includes health staff. Many comments about mistrust of health workers are concerned with perceived negative and discriminatory attitudes. One respondent illustrates this as she first starts by describing a doctor’s misdiagnosis of a Traveller child who had meningitis, but goes on to explain why no Travellers will now see that doctor. “ they will not go near him. They don’t like him whatsoever. My husband won’t even go to him and he’ll go and see any doctor, but he will not see him. He said it’s like he’s scared he gets a case of leprosy if he touches yer. He looks at you like that and does not come near you, but he’s about the worst I’ve ever seen” (F9) This has important implications for use of health services. Although several respondents in this study described positive experiences of health services, they were often depicted as exceptions to the norm. Overall expectations of health services were low and often manifested as fears of illness, either of investigations, procedures or treatments.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 31
Alternatives to use of primary care services were often mentioned in respect of actual or perceived failings of the services. In the absence of a trusted doctor, in addition to ignoring a need to access services at all, some Travellers preferred to
confide in a religious healing person. Several Travellers spoke of their strong religious faith helping them to overcome or to cope with ill health. Some Irish Travellers also spoke of their preference for and experience of consulting specific religious healers or curing people. One explained how her son was cured by a ‘healing woman’ from a ‘scar on the brain’ and was then taken off all medication “because we believe that Travelling people is cured by healers … [ mentions one healer] anyone seeking help used to ring her… don’t get me wrong , it’s not everybody who can cure you ….you could go to one hundred but still make no difference , but you will get the one who can cure you” (F8) Others such as the following respondent dismissed this belief “ some Travelling peoples believes in healing men and I don’t believe in any of that … like some go all the way round the country, say if they’ve got something like arthritis or something like that --- I think if you’re sick you should go to the doctors” (F4) Some women dealt with their reluctance to attend a doctor for their own health care by using their child’s’ health as a pretext. One mother who needed regular and unpleasant treatment in the form of injections for anaemia admitted her reluctance to attend and explained how she used her child’s health in this way “ when I make an appointment for the baby , well I tell the doctor about myself “ (F13) There was no avoidance when it came to fears about a child’s health. In such situations, there is desperation to make sure the child is seen promptly. Stories of other’s experiences of misdiagnosis fuel this urgency. One relative relates an experience of her child being taken to the doctors and diagnosed with a head cold before the parents, who weren’t convinced, took the child to hospital where the child was diagnosed with meningitis. Another account came from a mother whose doctor told her that her child had a viral infection and to take him home, and she was equally unconvinced due to her prior fears of meningitis. She explained “ and my little boy had meningococcus , the dangerous one in the bloodstream .If I had listened to him and taken the boy home and lying him down, I wouldn’t have him today that’s for dead cert.” (F20) Such experiences of misdiagnosis were given as examples to explain mistrust of doctors. These two separate accounts of a family member having a child misdiagnosed and then subsequently being found to have meningitis seem disproportionate to the actual prevalence of a relatively rare serious childhood illness. However, when the size of the extended families are taken into account the number of people who would be

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 32
acquainted with or even related to one of the affected children can explain the extent of the fear.
This mother’s account illustrates this “there’s a young girl at the top [of the site], she’s my niece’s daughter in law and the baby wasn’t well…” (F9) There was also a fear of the inevitability of a fatal outcome, following diagnosis with certain conditions such as cancer. This added to a reported fear of hospitals “I think they’ve got this old fashioned stigma that you’re not going to come out once you go in, honestly they do” (F9) Such fears often reflected a deep-rooted lack of trust in the staff concerned. Some respondents had themselves experienced or knew of a ‘close other’ that had experienced an apparent medical mishap and these experiences underlined pre-existing mistrust “ there’s more they could do with this hip, but my aunt, she had one hip done and she was mental after she had the other one done… they gave her too much anaesthetic” (F2) Hence, the mother who was worried about her daughter undergoing an anaesthetic explained, “because so many little kids is dying through anaesthetics” (F14) This mother told me that she had given her daughter breakfast on the morning of the planned extraction under anaesthetic, telling me “ and I shouldn’t have”. The doctor had to postpone the procedure as a result, but he recognised her fear and spent time reassuring her. She explained “ he said ‘ what if I do it in a proper theatre ; I promise you and I give you my word he said , that she will be in and out in 15 minutes ‘….When he was doing it then I knew [ it would be alright] and I said to my husband , and my husband doesn’t trust like I do and I said to him , and he was nearly crying, and I said, she’s fine” (F14) Lack of accurate information available to assist in weighing the risks of such relatively rare mistakes was an important factor in decisions about accessing care. In some circumstances the collective knowledge within the family or community appears to override a need to challenge or seek an independent view or understanding. This was sometimes reinforced by a fear of displaying ignorance to health staff. Reluctance to seek a medical opinion was also evident in fears relating to reported side effects from medication. This woman describes her anecdotal knowledge of side effects of particular medication. “ but I heard that you can get a stroke from that, can’t you , from the tablets, from the side effects, so I wouldn’t go on them” (F8) The reluctance to access services until it is seen as a real necessity and the low expectations held of those who provide the services is strongly associated with this mistrust.
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 33
One of the most frequently cited reasons for satisfaction with a health worker was that they ‘understood Travellers’ or knew their personal or family history. This appeared to be a strong factor in the more obvious trust invested in health visitors
for the respondents in this study. In cases where someone has demonstrated that they are trustworthy and show respect for Gypsy Travellers the trust and respect is reciprocated, along with consequent high expectations of that person “when you find somebody good you appreciate it.” News of a good doctor or health worker spread rapidly. One father, grateful for a locum doctors prompt diagnosis and treatment of his child, recommended everyone to go to him and it was reported that the doctor was driven to phone him up and ask him to stop, because his list was growing so big that he couldn’t take any more. However, even for those who have chosen to stay with a practitioner the doubts are ever present. “it’s just that you check , you check everything. That’s just the ways I am, check everything, all medication, even for myself. (M7) It would seem that as long as society in general is experienced as hostile to Gypsy Travellers and appears to support discriminatory policies towards them, it will be difficult for them to build trusting relationships with any non-Travellers, including health workers. Any apparent trusting relationship will nearly always be tested and cannot be assumed Lay referral The independence, self-reliance and belief in family or community support may be explanatory factors, in addition to mistrust already described, for a reluctance to seek professional medical advice. One woman who was often approached by younger woman for advice on various matters, including health, explained her father’s views on independence and self-reliance “ if any of us pick up assistance[welfare] it will be worse for us, good Gypsies are good foragers” (F11) Although she was keen to impart advice she also had reservations about the possible effects of creating dependency. She explained how the women would say “ ah I’ll take it to ‘Y’, ah yes, don’t understand it, don’t want to, I’ll go to ‘Y’”. However, her concern arose from her being seen as an advisor on all matters “ what about when ‘Y’’s not there? … you can spoon feed the people sometimes, you know” She went on to describe a few situations where she advised both women and men on health matters. Her advice was mainly in favour of natural or ‘mind over matter’ treatment and she actively dissuaded people from using prescribed medicines. She was anxious to point out that she advised them to check with their doctors. She reported how she had advised one woman “ if those pills aren’t absolutely necessary , talk to your doctor first, but get yourself off them if you can, because you’ve got far too many pills up there”

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 34
However, in advising her own son she was unconcerned with seeking a doctor’s approval and was very definite in her advice to dismiss medical advice to use a
prescribed inhaler after he told her he had been diagnosed with asthma. She reported that he accepted her advice “ I said to my son ‘baloney’ you’re full of toxins….cos you’ve laid rough…you’ve got to get to bed , get water down you ,proper food down you , you’re going to be alright son…So I wondered, she’s trying to keep herself in a frigging job. My boy hasn’t got asthma. He never had asthma. How many people in this country have said they’ve got asthma? How many asthma pumps kicking around? There’s no such thing. It’s fear.” Lay referral was the most common alternative to use of health services. Others used such avenues to seek reassurance that they should see a doctor. One elderly male Traveller who had been describing some of the natural remedies that Travellers used to use, spoke of how this was common practice in the past “in Travelling groups, if one woman didn’t know what to do with the child, like the next one would tell her try this, try that” (M2) The same respondent who had described natural cures he used for his dogs and horses pointed out definite gender role differences in caring responsibilities. When asked if he would use similar remedies for his children he replied “ I wouldn’t, the children were entirely up to their Mums, their mothers” One young Traveller spoke of self-diagnosis and of using lay advice in a different way, to obtain the treatment that she thought appropriate, without going to a doctor. She reported that many of her friends did the same “ I thought it were a kidney infection, but I just said to someone, have you got antibiotics?” (F4) The same respondent also used lay advice to confirm her own suspicion that her daughter had chicken pox, but then ignored subsequent advice. She explained why “ it was like all here on her chest, there was a rash, but it had heads on them, so I thought straight away it was chicken pox. I brought her down to some of the women, I said ‘look, I’m going to bring her to the hospital and they said, there’s no need, it’s only chicken pox, there’s nothing they can give you. I said, no, I’ll bring her, for me own peace of mind. I wouldn’t be able to sleep so I brought her up anyway” However, she also spoke of going against her own intuition by accepting her mother’s advice about her daughter’s dental care. “ I’m not giving her them antibiotics any more because of her teeth. Mum said, they’re only her first teeth, she’ll have more, just carry on giving it to her. I said ‘alright’, I’m very easily led” Several Travellers spoke of consulting their mothers about whether to see a doctor. One woman described her action should she discover ‘a lump’ “ we wouldn’t go to the doctor love, … we would like, but we would have to talk about it”

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 35
Interviewer. Who would you talk to? “My mum” Interviewer. So you’d speak to your mum about anything you were worried
about? “I’d show it to her, say ‘what do you think they are? And if she says,’ no harm, but go to the hospital’, we listen to that. But then by the time we’re there the sweats falling of us” (F19) Some Travellers used lay advice for practical reasons, due to illiteracy. One woman explains “ there’s a good friend of mine , comes up here very often… and if I go the doctors , if I get a new tablet that I know I haven’t been on for a while , I have never been on, well I’ll get the leaflet out and I’ll get her to read it to me , and to read the side effects what’s on it. She’ll tell me them” (F8) Support within their network was spoken of as an alternative to going to doctors for reassurance “say someone was out somewhere and met somebody and if they had problem , the women will talk and they will tell you what’s wrong with them and that . It’s been hundreds of times, been said to me.. ‘I don’t know where this is coming from’ or ‘I wouldn’t know what to do about it and I’m ashamed to this’ … and so you would tell them and then probably the other person would say, you should do such a thing, you should go to the doctors” (F18) However some Travellers would not seek lay advice, even from family. One young Traveller mother when asked, replied “not really to be honest. If it’s personal, it’s like that’s personal, you don’t want everybody knowing your business” (F19) There were fewer reports of men seeking health advice at all. One Traveller man who was asked what sort of advice he might give to a mate who was depressed said “ there’s not a lot I could do, I shouldn’t imagine that like one of my mates would come to me about that sort of thing” (M4) In further discussion however, he commented that if they were bad enough to need a doctor he would probably notice without them mentioning it and would proactively say that they needed to go somewhere or would tell their brothers. He conceded that Traveller men were more likely to keep such matters to themselves, or at best go to their family “their mum and dad or their brothers and sisters, or if they’re married like, their wife” Family care General mistrust in the wider society further reinforces their belief in the importance of mutual family support. Gypsy Travellers believe in providing for and caring for their own family members and speak of putting their welfare, particularly the children’s, before all other priorities. This mother in her 30’s expressed her purpose in life in this way

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 36
“ I’ve had my life, I’ve had what I wanted, 5 lovely children…it was the children that mattered” (F16)
Similarly this elderly mother explained her priority “I don’t care if God spares me if I can see my children grow up and that I think to myself as long as I can see the littlest, to see they grow up and they can look after themselves” (F17) The preference for seeking help from within the community extended to a preference for caring for a chronically sick relative at home wherever possible, but gender roles were strictly adhered to when possible by some. One woman described how her father had carried out all the physical care at home for his own terminally ill father, and went on to say “ we don’t believe in women seeing to men, because men sees to men and women sees to women” (F12) However, she explained that these rules would be relaxed in the face of no alternative family member being available “ me brother always says he’s there for me dad and like we’re there for me mum, but if anything happened to me brother and me dad did need to look after , then we would look after him ourselves” She described how her father had carried out all the physical care at home for his own terminally ill father, and went on to say “ my grandfather needed help for a bath and that. They wouldn’t have home help. They looked after him. We don’t believe in home help. We look after our own ourself, and me Dad used to carry him upstairs to the bathroom, bath him, dress him, and bring him back. If he wanted to go to bed, me Dad would lift him into bed. If he wanted to go for a walk, me Dad would take him out in his wheelchair” The cultural expectation that the family should care for sick family as far as possible means that care at home is the preferred alternative to any form of day care or residential social care . The idea of a relative going into a care home was particularly deplored. One respondent fully accepted her husband driving down immediately to bodily remove his mother from a care home on discovering that his sister had placed her there for temporary respite. She explained “she was used to somebody every night sitting chatting to her, but she was in a room and had the door locked (F2) This has very positive benefits for those family members, who can trust that loving and supportive family will care for them in ill health and adversity, as far as is possible. It is however an increased burden on the carers, many of whom do not receive outside support. “… I had never been apart from my mother …my mother got worse when she thought I was going to leave and when she thought I was going to stay she got better and when I was about to leave she got worse again … But I soon joined up with her again when I was married” (F11)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 37
Attitudes to illness and health “I don’t feel top twenty like, but I feel fine” (M2)
The WHO definition “ Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity” appeared a remote ideal that wouldn’t be considered a realistic goal. There generally appeared to be an acceptance by respondents that some degree of ill health could be expected and that one would not be considered to be ‘in poor health’ as a result of one or two complaints. One young Traveller, who described a chronic back problem for which she was regularly seeking treatment, described her health as “ perfect, really lovely” when asked at the beginning of the interview. Another, older male Traveller described a few health problems but described his health in terms of being good for his age “ I have a few complaints- not too bad- I’m seventy one” This stoical attitude was particularly evident among Travellers who spoke of dealing with depression alone in preference to accepting a need for medical help. Mistrust of others reinforced the belief in self-reliance “ when it comes down to the nitty gritty it’s down to yourself, and if you’re not willing to help yourself, then you’re not going to get it, are you? (M3) It is not therefore surprising that one man reported that if a mate was depressed he would expect him to ‘sort himself out’. This aspect of stoicism is closely related to the concept of standing up for oneself and not risk being seen as weak. Although this particular respondent feels that things are easier today, the attitude persists among younger Travellers, as illustrated by this mother “ you can’t just sit and let yourself be depressed. You have to get on and do things. I think ‘oh my children, they’ve lost their father and I have to carry on” (F16) This same respondent speaks of how she earned more respect within her community by demonstrating her independence as she describes how her family were ostracised when they were ‘down’, but when she ‘got on her feet’ they got respect. The fear of being seen as weak or ‘lazy’ by other members of the community appears to be a factor in self- reliance and stoicism. A respondent expresses some guilt at her attitude towards a relative who is suffering from depression and appears to her to be giving in to it. “ to me she’s got a good life. She hasn’t got to get up every morning and go out there to work and worry about her living. (F9) Another reason given for a stoical attitude of keeping hardship and suffering to oneself is to protect family members from their distress. This respondent had kept her suffering to herself for a long time before eventually breaking down and telling her older sister because “ I didn’t want to put the burden on her, and she’s the oldest sister, but we look up to her, she’s like a second mum to us” (F12)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 38
Being strong and stoical for the sake of the family was a motivating factor for another respondent “ I don’t get a chance to get ill, because if I do, I just have to keep going day by
day because of my kids” (F12) There were also examples of a fatalistic attitude to the experience of ill health “ I don’t think you can stop any ailment” and “there’s not a lot I can do just, if it’s going to happen, it just happens” There was an evident cultural pride in being tough and self reliant and not admitting to minor complaints. This older man appeared disapproving that Travellers today seemed to be attending more for health problems and commented “I’ve seen a lot of them at clinics there and all that, like headaches and pains and aches and all that .I often tells them I often got a bit of a tent in the ground, I’d be wet all over …feel nothing about it” (M2) He expressed the belief in an evident pride in being seen as fit as he boasted that his six sons were “super fit” He explained “ they’re athletics [sic], they’re boxers, they’re everything- super fit” The self-reliance reported by respondents when suffering from ill health often results in delayed access to health services “ you’ve got to be tough and get on with it, or ‘you don’t want to go to the doctors.’ This belief, coupled with mistrust and low expectations of services, or poor outcome, can increase the anxiety and sense of urgency that is reported when services need to be accessed. “ …I said you’re a waste of time, I’ve been coming her for months, getting worse and you won’t even examine me, you don’t have the faintest idea what’s the matter with me” (F9) Restricted autonomy for Gypsy Travellers generally and particularly for women, with their strong cultural role expectations, appears associated with a strong need to retain control. The inability to exercise some control over situations adds to the burden of stress that many Gypsy Travellers experience. This need to retain control is an evident underlying attitude in many situations involving access to health care. The fear of being dependent on anti depressants and belief that this will cause loss of ability to control ones’ situation is also a factor in fear of depression itself. This fear appears to be connected to a dread of capitulation and dependency “you can’t fight it yourself you’re dead, you get worser. If you just think you haven’t got it, just let it go, try and control yourself, it’s better” (F20) The strong expectation that the wider family is involved in caring for and supporting a sick member in preference to outside support was readily accepted regardless of the additional stress for the carers. The belief in independence and stoicism however, can contribute to a sense of guilt in the person being cared for. This elderly respondent eventually asked her daughters who had taken turns to stay and care for her at nights, to go back home to their young families, explaining

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 39
“ “I’m selfish, you go on back, and go to see to your children and that … And I said I’m all right, if I ain’t all right , I got the phone near me or I said I can ring
you up or you can ring me up .So from that love I put a stop to it” (F17) A positive aspect of this stoical attitude is that Gypsy Travellers report an ability to recover quickly and ‘get on with their lives’ following an episode of illness or surgery. This is in contrast to an attitude of helplessness and dwelling on misfortune that others could hold in similar situations. One respondent gave an example of how this had been noted by others in hospital following her operation “Because, they come round and said, like do you need any painkillers now. And I said no, I’m fine and then like all the other women was ringing bells and asking for painkillers and they was going to be ill and all that. And I said, I never noticed until one of the women said, well you’re recovering quicker than what the other women are. And you’ve had more surgery…and they seem to think it was because we was Travellers, we had like you say magic power has made you better quicker. You didn’t need all the fuss and all that…The consultant said … you’ve took the attitude there’s something wrong, get it sorted, do what you’ve got to do and I’m going to get better. And that’s what he kept saying”. (F9) Attitudes to Death and Dying “ it’s like a tremble through the heart” Respondents in this study speak powerfully about death and dying in the context of health care. Investment in the family and in rearing the children is often reflected in extreme fears about separation from them through death. One young Traveller father speaks of his fear of ‘something like cancer’ in these terms “like dying young, fear of my kids and my wife being left by themselves” (M9) The fear of separation through one’s own death appears equalled by the fear of death in a close other. This young respondent explained her first reaction to learning that someone is sick “the first thing you do is pray and please don’t let them die” She described her reaction to witnessing a sister’s epileptic fit; “and I was a mile up there , out of the gap away, and I was pulling all me hair out and I was crying and I was scratching myself… I was frightened she’d die” (F4) The running away that was described by this respondent, although more likely to have been an instinctive fear reaction, has parallels with avoidance of any associations with death that are described by other respondents. More often, the desire to avoid associations with death was attributed to stirring of the grief reaction of past bereavements.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 40
As death and bereavement are so strongly feared, and there is a belief in keeping one’s grief and distress hidden in order to ‘protect’ other family members, this can result in a heavy burden of conspiracy of silence.
There is the extreme grief, expressed by this bereaved son “ it was like , what do you want to live for . I just felt like doing away with meself through drink to be truthful” (M1) There is then the added burden from the failure to share it, as expressed by this widower “ I wouldn’t like to worry them. They used to be worried about me” (M2) There was an anticipation that grief will be enduring, and accounts of relatives or respondents ‘never getting over the death’ were common. One respondent described this anticipation “ dead is a bad feeling , because you miss that person terribly for the rest of then until you die yourself” (F14) The grief of bereavement was perceived as a cause of illness and often as an indirect cause of death. Even though ill health commenced a whole year after the death of her husband this respondent attributed the onset of asthma to her bereavement “… a year from when he died… a year after, I was took with asthma, very very bad…I was a strong and healthy person; I think the cause of his death caused my illness” (F17) The following respondent illustrated the circular nature of this belief that actual and anticipated bereavement can cause serious fatal illness “ my aunt died of cancer … and her husband died before that. I mean she had the cancer but of the worry he got, he got the cancer. He got cancer over her having it. He worried so much about her, he got the cancer, and then he died. She got the cancer back. She died” (F20) Bereavement is also described as a precipitating factor in the use of harmful health behaviours such as smoking and excessive alcohol intake. This woman explained her reasons for smoking being due to the pressure of “ my mother being dead and pressure of that boy dead [a cousin’s husband] now as well, murdered and 5 children left” (F13) The prolonged and extreme grief reactions described might appear surprising in light of the close and supportive extended family that rally round when someone has died. However there are several aspects to family involvement that appeared to give conflicting benefits. It was clearly reported that close family members will ensure that the bereaved relative is never left to be on their own following the death. “ and there’s someone with you all the time then, you’d have somebody with you nearly all the time , very good when anybody’s in trouble” (F13) This would seem to be particularly important for Gypsy Traveller families, as it would be so unusual in their experience to have ever been alone. A few bereaved respondents spoke of this and it adds further to the acute sense of loss that is experienced when a death occurs. One widower said

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 41
“ she hasn’t been out of my mind for one minute…. We never had a night away from one another in 47 years” (M2)
The memory of the dead person is kept alive through regular grave visiting .Graves would be visited regularly and well-tended years after the death, as this woman widowed for 20 years describes “ And I was talking to an old gentleman up the cemetery once who was up on a Sunday morning, talking about I went to put these flowers on my husbands grave and we was talking about it [ God] and he said I suppose now you‘ll go to the church. And I said no, I’m not going to church and I said I’m going home and cook a bit of dinner” (F17) The need to be close even after death was reflected in the expressed importance of kin family being buried in the same ‘family graveyard’. This respondent explained “ me dad was took back to Cambridge . That’s where we come from, well where he come from. The same church that had his mum, his dad, his brother in law, all buried there. Brother in laws, sister in laws, they’re all sort of together. They don’t believe in cremation so” (F2) Any failure to be able to have a close relative buried with the family is a cause of extreme added distress to the bereaved. One young respondent spoke of her own and her parent’s tremendous grief because her sister in law had broken this convention by having her husband (the respondent’s brother) buried near to where she (and they) all lived in England instead of allowing the deceased’s parents to have him taken back to the family graveyard in Ireland for burial. Another way in which the memory of the dead person is kept alive is through naming of subsequent children born in to the family after the deceased. The significance of naming subsequent children after a deceased family member was alluded to by this young woman, speaking about a close uncle who had died when she was 12 years, as she describes the deep impact his death still has on her seventeen years later “ my uncle died when I was 12 and I never went to his funeral” Me Do you regret that now? “No because I was very close to him, because my little boy’s called after him, and me uncle was only 19 when he died… Like my mum wanted us to go and I wouldn’t go because I was too close to him. I seen him when he was laid out and I was sorry that I did go to see him when he was laid out. I still get to see him now” (F12) There is some conflict between the need to preserve the memory of the person and the need to avoid the grief reactions that are stirred by association with the place of death. One elderly respondent, who has been widowed for 20 years, still spoke of being unable to face going into churches since her husband died “I can’t face it. I think a young one was buried yesterday … and my daughter in law went there to take a wreath for a friend. I think if I’d have gone into that church I think they would have had to carry me out. Because it was all the same songs and same prayers as to what was at my husband’s funeral. Don’t think me wrong like, thinks that I was evil, but I just can’t cope with it” (F17)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 42
Gypsy Travellers, with such large and close extended families, inevitably have a larger number of funerals to attend than many non-Travellers. Funerals are also culturally important occasions when many extended family members meet up,
but also when they show solidarity in numbers that reflects the dead person’s standing. Respondents spoke in terms of the priority in attending funerals, as this woman described “… the week before that I was in Ireland for my aunt, she died, so I had to go back to Ireland ; back and over straightaway… ” (F14) The respondent who described being unable to cope with funerals described how she deals with the necessity “ I’ve been to funerals but I’ve kept out of the way. I’ve been there with people, show me respects and take a wreath [but] I goes in and keeps in the background” (F17) Respondents speak of moving after someone had died “ we had a house…Then when my son hung himself, we left… we took back to the road again” (F8) Another respondent moved to avoid having to continually pass the scene of death “ I was living in my cousin’s caravan site which she owned, but he went off the road and died at the wheel, so I just didn’t want to stay. We had to go by it every day, so we moved” (F2) The urge to move away is possibly a more common coping method for Gypsy Travellers who speak of moving when they are experiencing other difficulties. For some there is an apparent superstitious fear of staying in a place where someone has died “I had a house in x and I was in there and I could here things in the house, noises and things, so I went and got a priest and he told me an old lady died in the house … he said it’s best you just leave”. (F20) Those who hold religious beliefs, whether Catholic or evangelical Christians, describe great comfort as a result of their belief that helps them to cope with their grief. “ religion is a big part of our lives…. If someone dies, it gets us through, the grief of it” (F19) Attitudes to screening and diagnosis “ I thought I might find out something that I wouldn’t want to know” Fear of a terminal prognosis was the usual reason given for an intense fear of cancer “ I started screaming, I said no ,… for the fright, for the shock of hearing it …“because I knew [if I had it] I was going to die right quick” (F8) There is a generally held assumption that a diagnosis of cancer is an inevitable death sentence, as this seems to be born out of most respondents’ experience. Where there is also a fatalistic belief that ‘nothing can be achieved by attending for screening or potential early diagnosis’ this can result in more serious outcomes that then reinforce the belief that terminal illness is an inevitable outcome.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 43
“I think cancer is one of the biggest fears of Travelling people… I would talk to 5,000 Travelling people and [if] the first word is that, anything at all about that
they just dies, they just falls to pieces” (F8) The belief held by respondents, that death will be inevitable following a diagnosis of cancer, appears to be a partial explanation for avoiding the opportunity for diagnosis. There is also a belief expressed on behalf of others that the diagnosis in itself was implicated in a fatal prognosis “ a lot of Travellers blame [it on] if him or her didn’t find out they had it , they’d live for another 30 years and all that ….a lot of people going for check ups have found out and when they’ve found out they’ve died straight away you know. But if they hadn’t gone that’s what they’d claim like, … He might live for another 10 or 20 years” (M2) Another suggested a similar fear as she cited an aunt, a grandfather, a grandmother and two uncles who all had cancer and said of one uncle “he got diagnosed on the Monday and he had cancer and on the Friday he died. He lived 5 days” (F12) Such fears about cancer appear to result in late rather than early presentation. This respondent had recently attended her doctor and been referred with a possible cancer diagnosis herself, yet when asked at what stage she consulted him she replied “ I’ve had it [lump] about 12 month now so it's only recently that I went to the Doctors about it” (F12) Beliefs about the relevance of screening are a major factor in whether preventative measures are seen as a priority by respondents, “ if God borned you to have a short life , you had a short life if he borned you to have along life, you’d have a long life- nothing you could do to alter it” (F17) Her fatalism reinforced this respondent’s perception that nothing could be done to prevent the likelihood of disease such as heart disease, strokes etc. Even when it was mentioned that some people did exercise or watched what they ate, she felt that such behaviour “doesn’t make any difference” A belief in God’s will produces varying views in how respondents interpret the action of seeking medical intervention to prevent ill health or to prevent worsening health. This respondent who believed that certain conditions such as AIDS and cancer were “God’s will” felt that she didn’t want more information because “ what I don’t know can’t hurt me” (F4) For one respondent, whose religious faith was fundamental, trust in God is an alternative to the need for her to continue with anti depressants “ when I got them depression tablets I took them for a while… and I sat down , I said to Jesus … and I’m not taking no more tablets because I’m going to trust in you” (F14)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 44
However, another respondent who is also a ‘born again Christian’ has a different interpretation on God’s will. In explaining his commitment to taking measures to prevent complications of his diabetes, he says
“ I’ve got to do it health wise, otherwise I’m going to kill myself aren’t I, and I know God wouldn’t want that…God put doctors on this earth didn’t he? (M1) Other respondents who believe in prevention are not motivated by their religious belief, but by recognition or fear of the health consequences. One woman who was anxious to ensure that her blood pressure is monitored regularly and who is also taking steps to follow other health promotion advice in relation to exercise and diet explains “ like cos of me having a stroke, it could happen again….. I don’t want that to happen with five kids” (F10) Among less fatalistic respondents, a range of attitudes to prevention was apparent. Whereas those with a fatalistic attitude had a tendency to ‘live for the day’ and not talk of long term goals, this young Irish Traveller illustrates a different attitude “I think of the future very much. I think, I must smoke about 10 fags a day now and I’m 21, what am I going to be like in 20 years – so that’s why I’m going to give up [smoking]” (F4) Perceptions of the causes of ill health, as well as perceived expected outcomes, play an important role in attitudes towards prevention. In contrast to the avoidance of screening due to fears of prognosis that was reported by many respondents in earlier sections, a fear of cancer does prompt this same respondent to avail of screening as she explains her optimistic belief that early detection is possible and will be beneficial “ I’d like that they check you out from head to bottom and they’d know like everything through your system…for all the bad complaints … cancer and all that” (F5) Some respondents are emphatic in generalising about Gypsy Travellers attitudes towards screening, whichever end of the spectrum they stand upon. In emphasising her view of the importance of attending for smears this respondent states “ I don’t honestly know one woman, say on this ground, that don’t go for them… didn’t maybe 15 or 20 years ago” (F9) Conversely, in emphasising her reasons for not attending for smears, another woman says “ I don’t think any Traveller woman does [go for smears]” (F19) Conclusion The experience of a society that demonstrates widespread hostility towards them, and has done for many generations, strengthens the belief among Gypsy Travellers that they should be wary, and slow to invest their trust in outsiders, until convinced otherwise. This has important implications for use of health services. The reluctance to access services until it is seen as a real necessity and the low expectations held of those who provide the services is strongly associated with this mistrust. In cases where someone has demonstrated that they are trustworthy and show respect for

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 45
Gypsy Travellers the trust and respect is reciprocated, along with consequent high expectations of that person.
However, general mistrust in the wider society further reinforces a belief in the importance of self-reliance and mutual family support. Gypsy Travellers believe in providing for and caring for their own family members and speak of putting their welfare, particularly the children’s, before all other priorities. These twin beliefs in self- reliance and stoicism in the face of ill health seem to be embedded in child-rearing practice and are evident in all age groups among the respondents in this study. A positive aspect of this stoical attitude is that Gypsy Travellers report an ability to recover quickly and ‘get on with their lives’ following an episode of illness or surgery. This is in contrast to an attitude of helplessness and dwelling on misfortune that others could hold in similar situations. The belief in ‘keeping up appearances’ also associated with pride and dignity reinforces this independent and stoical attitude. However, there was a certain degree of lack of sympathy for those expressing difficulties with coping. Self-reliance and stoicism reported by respondents when suffering from ill health often result in delayed access to health services. This, along with the mistrust and expectation of discrimination or poor outcome can increase both the anxiety and a sense of urgency that is often reported when services are accessed. The extreme fear of cancer is another factor that contributes to delayed presentation, and where there is also a fatalistic belief that ‘nothing can be achieved by attending for screening or potential early diagnosis’ this can result in more serious outcomes that then reinforce the belief that terminal illness is an inevitable outcome. As death and bereavement are also strongly feared and there is a belief in keeping one’s grief and distress hidden in order to ‘protect’ other family members, this can result in a heavy burden of conspiracy of silence. The comfort and strength derived from religious belief and practice is also important to the well being of many sick relatives. There is a reported intentional low use of care homes and day centres for their family members. This has very positive benefits for those family members, who can trust that loving and supportive family will care for them in ill health and adversity, as far as is possible. It is however an increased burden on the carers, many of who do not receive outside support. The combination of denial of symptoms, delayed presentation and reluctance to accept outside support has consequences on the lack of early intervention for both physical and psychological ill health. It is important for health workers to ‘see behind the brave face’ in a sensitive and understanding approach to offering advice and support that takes these beliefs and attitudes into account. Many misunderstandings can arise on the part of health staff who lack an awareness and understanding of these beliefs and attitudes. Many of the potential misunderstandings about the health related behaviour of Gypsy Travellers, for example, apparent inappropriate use of emergency services, refusal of investigations, missed appointments, failure to accept referrals etc might be avoided with increased awareness and proactive reassurance and explanations. A proactive response and

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 46
understanding of the cultural need for family involvement in care can also enhance the relationship between health staff and Gypsy Traveller patients and their relatives.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 47
Health experience “ to enquire about the subject’s own health is to invoke biography”7;7
Mildred Blaxter This section deals with the self-reported health and ill health experiences of respondents. For the interviews a pre requisite for selection was to have some experience of ill health, so the extent of their morbidity is unlikely to be representative of the wider community. However, there are certain common themes that have emerged in the ways that health and ill health are experienced. A stoical attitude towards ill health and understating of ill health, as already described in previous chapters, is the norm. Overall there was wide range of morbidity described by respondents, not only concerning their own health, but also that of their families. Within the range of symptoms and specific medical conditions experienced there were some that featured often or were given prominence due to the particular impact on the lives of the respondents and their families. Symptoms of chronic ill health, rather than specific conditions were given most prominence and these were invariably those that limited the ability to carry out day-to-day responsibilities, such as restricted mobility and shortness of breath. For most conditions it was the daily impact of the symptoms that were significant rather than the perceived long-term implications of the diagnosis (if known or acknowledged). Other conditions were given prominence due to fears arising from lack of knowledge or from the reality of their impact on the wider family, notably depression, and bereavement and substance misuse. Cancer was a notable exception; this condition was so strongly feared, that it was mostly avoided in discussions about health experience. Respondents were most likely to have experienced bereavement as a result of cancer and not the experience of anyone being successfully treated. The cultural desire for large families and centrality of children in the lives of Gypsy Traveller women meant that prominence was also given to the maternal health issues. Maternal health “like all Traveller women, they’ve all got lots of kids” Most respondents who were married either had or planned to have children, and this was viewed as an expected and welcomed course of events. Large families were often desired and the children all cherished. One mother of four (so far) said “I’d like 10 …because if you’ve got one, if you’ve got 10 you just feed them and look after them the same…… because I love children, I’ve been reared with children all me life, and I can’t remember life without a child. I was 19 when I was a mother so” (F12) Others welcomed the fact that contraception was available so that they could control the size of their families, which, as recently as the last generation had commonly been

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 48
into double figures. An older woman, who had not had the opportunity of contraception when she was childbearing, commented that it was a good thing “ four children is plenty for anyone now.” A sense of hopelessness for their
future influenced her reasoning, however, “ because there’s nothing for lots of children now isn’t there; there’s so much going around, drugs and everything…” (F8) The following account from a young mother of four (one of whom suffers a disability) describes a general attitude towards children “ If you sit down and you get tired, but if you’ve got kids, like all Traveller women, they’ve all got lots of kids, they just keep going for the day and that, at night they just have an early night and that’s it. I mean, that’s just what keeps us going really is the kids” (F19) The strong desire to have children resulted in great anxiety at the thought of infertility. One young woman, still single, who was experiencing amenorrhoea, said she was thinking “ oh Lord, what if I never get them [periods] again, I’ll never be able to have a baby” (F5) Many respondents had experienced distressing events surrounding pregnancy and childbirth. These included infections during pregnancy, ectopic pregnancies, miscarriages, stillbirths, and premature births and in one case, onset of a serious long term disabling condition precipitated by the birth of her child. The impact of a miscarriage is profound for many women; however, the Traveller women who had experienced such a loss appeared particularly traumatised. One woman who had miscarried at seven weeks gestation in her 6th pregnancy (the others resulting in five healthy children) described, with her husband, their reaction “ I lost one [bairn] last year and I felt horrible” “ Depressed we were, the 2 of us” (F6,M3) The reaction with the subsequent pregnancy was an urgent desire to attend all antenatal appointments to obtain reassurance that all is well. When circumstances forced her to miss one of these appointments she described her extreme distress “that put me in a bad depression, I went mental.. I was bawling, and shouting, I was angry, I didn’t want anybody around me. I just wanted to be on my own… it was the thought of missing the appointment” (F6) Some women experienced practical difficulties in accessing antenatal care, particularly if they were travelling. One brother described his family experience when they were travelling and the police came to move them on “and the one girl was ready to have her baby … before they could even see the health visitors or anything they made them move. So the girl found a health visitor and told her where she was; she was on her way down and they were gone before she got there” (M4) However, it was a common experience for women, if they perceived that the pregnancy was progressing satisfactorily, to avoid antenatal appointments until later in pregnancy in order to avoid having intimate examinations
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 49
“ like me aunt now , when she gets pregnant she doesn’t go till the last few
months ; she finds it embarrassing” (F19) This has been explained earlier with regard to embarrassment and the cultural attitudes towards privacy. One respondent who had attended hospital early in her pregnancy, because of severe pain resulting from an infection, described her reaction to the experience of having a vaginal examination (which she calls an “internal scan”) “I had an internal scan, … they shouldn’t do them things when you’re pregnant. They should when you’re delivering a baby, they should pamper with you to see that you’re ok. …but when you’re pregnant, they can damage the baby” (F20) It is easy to see how fears of an internal examination in such circumstances could have exacerbated the distress of the whole situation. The rest of the consultation was described and appeared to result in a complete breakdown of communication which finally led to this respondent leaving and being taken by her husband to another hospital for treatment instead. Other women who had attended early antenatal appointments had been considerably upset by the lack of cultural sensitivity shown when being offered investigations such as HIV test or amniocentesis. One woman explained her reason for refusal when offered an amniocentesis “She [midwife] said ‘ are you sure?’ I said, well look, if it’s sick or not I’m going to keep it anyway so” (F4) One of the older women put a different perspective on attitudes to antenatal care, which again relates to the valued cultural trait of self-reliance and resilience. She informed me that, years ago, when she was in her childbearing years there was no antenatal care, and they coped, although she felt it was good that it was now available. I enquired about differences for Traveller women today and was told “ there’s no way they’d be able to cope … A weaker strain – must have been different women going at that time, that’s my making of it” (F8) One respondent with very limited knowledge of what to expect and who was terrified of the unknown described the frightening experience of first time labour at the age of 18 or 19 years old “but I wanted to get started off , like I was 2 weeks over and I was very fed up because it , like they wouldn’t , nothing was happening .I didn’t understand, I was too young and all… (F4) When the staff resisted her pleas to be induced she described how she reacted “ I got really, really upset with her. I was shouting at her, screaming at her… it was because I was fed up”1 1 The term ‘fed up’ is often used by Gypsy Travellers in context of depression and has stronger connotations than the majority population use of the term
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 50
Her situation was another occasion when communication breakdown and misunderstanding resulted in her enduring pain unnecessarily when pain relief was on offer.
Although in the past Gypsy Traveller women had often given birth at home (“ used to deliver on the side of the road”), all the respondents now chose to deliver in hospital. Many regretted that it was not possible to have a longer postnatal hospital stay. One older respondent who had been used to a longer period of rest and care following a hospital birth commented “ they come out next morning. It’s a shame, they should rest more” (F8) Within living memory of older Gypsy Travellers, postnatal women were not allowed to do anything for some weeks apart from nursing the child, and indeed, were seen as ‘unclean’, needing to be ‘churched’. One pregnant mother in this study who described a good experience of being kept in for a couple of extra days and a rare experience of having a break from the caring role explained the reason for this desire “ it’s like when you’re in hospital you don’t need to do nothing , all you do you get on your bed and they come hand and feet to you…having things done for you and it’s a good break, believe me it is and then when you come back you’re either cooking or you’re cleaning or you’re changing and washing ..” (F6) Chronic ill health “ I haven’t got the best of health… I think it’s in every bit of my body actually, my neck and feet, legs, arms” Understatement of chronic ill health The experience of chronic ill health was marked but understated. General reporting of overall good health often belies considerable suffering that only emerges after some discussion. One young respondent who had described her health as perfect is a typical example, as she went on to say “ I only have a bad back all the time- that’s since I was 15” (F5) There were few respondents who did not suffer from a long-term chronic condition and most suffered considerable polymorbidity. The extent of understatement could easily distort the overall picture of the state of health, particularly with the associated low use of health care services. All respondents who described chronic ill health were either receiving health care or had sought treatment for their condition, but there were many indications that this was only when strictly necessary and that ‘putting up with it’ was no longer possible. There was particular difficulty if the condition experienced was one that produced intermittent symptoms. The previous young respondent reported her difficulty in getting diagnosed and receiving appropriate treatment.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 51
“ because one day is a good day and tomorrow could be a bad day, and more likely I could be in bed the bad days and then when I feel better I go to the doctors and they say ‘oh you can move this way so you’re not that bad’. So I don’t know”
(F1) Others would minimise their own ill health by reporting the symptoms with qualifying remarks such as “….short of breathing sometimes, not all the time” Men, including young men, in particular appeared to dismiss complaints. One 21 year old described himself as ‘ pretty healthy’ despite coughing frequently during the interview. When asked about his cough he dismissed it as being a consequence of “just like me working in the rain …I don’t think it’s nothing too major ..I haven’t had it forever, I think it’s this last four or five months” (M4) Some respondents recounted a list of complaints suffered, yet did not describe themselves as being particularly unhealthy as a result. One lady, who had described herself as suffering from a heart problem, a bowel problem and arthritis, said that she felt ‘pretty good’. She qualified this by saying that it was her attitude in that she didn’t “sit and worry about it.” However, despite much evident stoicism, most respondents described a multitude of complaints, many of them chronic and serious. The only respondent who described her health as being “ very poorly” explained that she had “ nine complaints altogether”. These complaints included heart disease, arthritis, a painful lump in her arm, a kidney/bladder problem and depression. One younger respondent, aged 50 years, who recounted an even greater list of symptoms and conditions, described her health as “quite poorly” There appeared to be an acceptance of their chronic ill health as long as day-to-day management of symptoms could be readily achieved. This lady who had recently been given a “ spray… for heartgina [angina]” said “ so I still got this stuff… when I starts walking and I finds I’m getting a little pain or a bit breathless, I just takes that. So I’m very happy” (F17) Carers of family members with chronic ill health Two respondents were carers of a young child suffering with a chronic health problem or disability since birth. In both cases, whilst ensuring that their respective children attended their appointments and received the necessary care, they otherwise appeared to treat them no differently to their siblings. Both of these mothers were now single parents with at least three other children, but in neither case was anything made of any possible burden from extra the demands in providing for their needs. Other respondents either were or had been carers for other adult close family members. Although it was accepted that family cared for their chronically ill relatives at home as far as possible, one daughter described the enormous stress she had experienced caring for her mother who had suffered with dementia

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 52
“ her nerves were very bad after my father died. She was, she’d er , she was sort of paranoid, schizophrenic?, kind of extreme really. I didn’t know how to cope with that and I had two small sons and a business and we were very hard up…”
(F11) However, there was also concern expressed by respondents in chronic ill health about the impact on their relatives. This mother who was unable to give a label to her condition (“ something syndrome”), but had obvious disabling symptoms described how she copes at home “ well I have an 18 yr old daughter here , she’s just gone shopping and I have a 14 yr old son and really , anything has to be done, she has to do it- more than the heavy things , the little things… there’s lots of things I can’t do . But she doesn’t work or anything; she doesn’t draw no dole. If she did she’s get a job She said she’s stay at home there, but the young lad he goes to school … if she wanted to go and leave me, he’d stay, things like that. Because I did go up the stairs one day and I fell down you know and ever since that day they wouldn’t let me alone because they’re afraid if I go for a kettle, things like that” (F18) She was now being helped to apply for an attendance allowance but the family had originally been ambivalent about this “ he told me you should be entitled… but we wouldn’t think about it…she [ daughter] would think, nah, why would they be doing this” Even with help however, they experienced a struggle over an eighteen-month period with having to attend appeals processes due to original absence of medical information. Management and treatment of chronic ill health Few respondents describing symptoms such as chronic pain or reduced mobility were able to tell me the cause, although most were receiving prescribed medication for their symptoms. In most cases the medication was described as ‘not helping very much’. One man described the severity of some of his symptoms “I’m crippled, I can hardly walk. My back has gone, me leg is gone, me hands is gone. If I go to walk, try to walk, I know I’m going to fall” (M5) Although he was receiving treatment, when asked about the cause he replied “ he never tell me”. One likely explanation, in view of his polymorbidity is that he failed to consult about all of his various symptoms at once and only focused on a particular area of most immediate concern. He was most concerned about his psychological health and was desperate to move from his present sheltered accommodation. His focus when he attended the doctor was primarily to get a letter in support of a move. Others describe repeated consultations but an eventual resignation that they will not obtain relief or satisfaction. This mother describes her many attempts to get treatment for her musculo-skeletal symptoms and the outcome “ these 2 knees they come and give me a lot, now yesterday that knee was swelled and I could barely walk . I don’t know why…sometimes the power just leaves and I fall because there’s no power there to hold me up…… …so when I went to my GP and

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 53
he give me these tablets, naming out whatever it was , and I took the tablets and I still have the same problem” (F14)
Her resignation was summed up in response to my question about whether she intended to return to her GP [to report that the tablets weren’t effective] “ no , this has gone on for the last two and a half years, three years” Impact on daily life Many respondents described their state of health, irrespective of severity or extent, in terms of ability to perform daily tasks. It was as important for women as for men to be able to continue working, whether it was to earn a living or maintain the home. This lady in her 80’s describes her limitations, resulting from asthma, arthritis, angina and a frozen shoulder, in the context of being unable to carry out the same range of housework that she had previously managed “ I can bounce about the place and just dust and do what I can reach and that, but there’s like, clean windows, can’t do anything like that” (F17) Most did their best to carry on doing the same level of activity without changing their lifestyle in response to ill health. Often it was felt that there was no alternative, as they needed to maintain the home, care for the children, or earn a living. This mother of 5 children under 10 years of age, living in a field, a mile from the nearest school, had continued to suffer ill health since having a mild stroke a year earlier. She experiences unpleasant symptoms on exertion but continues to make three return journeys on foot to the school each day, (because the youngest only does half days), in the absence of help from neighbours. She describes her experience “ I haven’t seen anybody about it, but I do get out of breath quick a lot. I get to the bottom of this hill and I’ve got to sit down for a minute and get me breath. So I get out of breath quick and I get drowned in sweat” (F13) In some circumstances this attitude of carrying on as normal appeared to be beneficial and was perhaps helped by an evident lack of anxiety for some over the possible significance of their symptoms. Living for the day rather than worrying about future progression was made easier with this lack of awareness and the possible predicted course. Equally, there is a risk that life- threatening conditions could go undiagnosed or untreated. One elderly woman whose daughter had eventually witnessed her symptoms was persuaded to see her doctor and she was subsequently diagnosed as having suffered “mini strokes.” Her own response to the symptoms that she had experienced, a series of episodes where “ down below your face freezed right up and I couldn’t open me mouth” had been “ I thought I just had a cold or something or other”. Following her eventual diagnosis she commenced prophylactic medication. There were many respondents whose chronic ill health was so severe that they were unable to carry on their daily activities. Some of these respondents were in receipt of aids to daily living, such as this lady, living on a caravan site but who had a bath in her small amenity block. She was not able to bath herself and had been given “ a thing to leave over the top of the bath like a chair and one of my daughters do wash me” (F3)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 54
Others described difficulties in coping without any aids. One widow, whose difficulties in coping with arthritis had caused her to move from a caravan site
into a house, explained “ the taps I can’t turn properly on and off because I’ve got arthritis” (F2) She described the support she received from family, but unless family are living permanently in the same household or immediate vicinity there are still many difficulties that cannot be easily overcome for someone experiencing chronic ill health. One young mother who has a severe disabling condition described the pain she frequently experienced, particularly during exacerbations. She also lived alone in a house with her young children, all under the age of eleven, although she had family close by. Whilst clearly able to describe her pain to me she pointed out that she couldn’t make her doctor understand. “I couldn’t think of nothing else-I’m in pain you know. And I couldn’t tell anyone because no-one seemed to understand. Even if I went to the doctor, I didn’t think they understood. You just don’t realise” (F1) This is how she described her pain “ you don’t want to move nothing, don’t move your hands , don’t move your feet because they’re painful, you know, just keeping them in the one situation , but then I’ve found out that doesn’t help me because then when I try to get up I’m more stiffed , they’ve locked themselves in places and they doesn’t and sometimes this arm locks and if he locks he won’t bend and this is the way it will be for a long time and it will go on for a week like that . It’s painful, very painful” These symptoms affected her daily living to the extent that she had to have a bed downstairs and needed help with self-care from her sisters “ it’s not very nice . Having to get someone to brush your hair for you, having to bath you, because I couldn’t get in the bath by myself. I have to have help … it’s like a proper invalid you know” One of the worst aspects of ill health for this woman had been her inability to enjoy her new baby. Her condition had been precipitated by this last pregnancy “ Each hand was like two put together you know, me arms, face, head, so I literally couldn’t move ….I felt so depressed just having a baby. I wanted to enjoy it. I couldn’t enjoy the pregnancy and then I couldn’t enjoy the baby when I had it and then I had the worry of her down one part of the hospital [she was premature] and I was in another special unit, apart, you know” The children were of extreme importance in the context of coping with chronic ill health. This same respondent (who had three other children) explained “they keep you going. That’s I mean I think it’s having all the kids you know, they’re all full of life and active. I think, Oh God, I’ve got to do something you know, I’ve got to try anyway. And now with the medication I think they’ve got me to the stage where some days I can wash myself, you know and I can have a bit of interest in myself, but when I get them days, I don’t want to spend it on myself, I want to spend it on the children”

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 55
She also explained how she wanted to be well for the children’s sake “ I don’t want them to have a sick Mammy all my life, because I don’t want to
spoil it for them. So I just tell them ‘Mammy doesn’t feel too well, she has to lie down for a little while. I know it’s lying to them, you know, but I don’t want to ruin their childhood for them, thinking ‘ oh I was brought up and Mammy was sick’ … I want them to remember Mammy a bit when she wasn’t sick” Some respondents, as already described, continue to endure chronic ill health rather than undergo feared investigations or treatments that may provide opportunity for relief or cure. One respondent with an obvious limp had endured persistent chronic back pain since being involved in a car accident eight or nine years previously. This did not prevent her from responding to a general question about her health “ my health has been good really” (F11) Despite efforts to get treatment and relief from different practitioners, staff had failed to find a treatable cause for her severe and disabling back pain and she felt finally that she had been viewed as a malingerer. This feeling prevented her from persisting with efforts to get effective treatment and to persevere without support. “ They said there was nothing wrong with me, I tried desperately to get better” Eventually she did have another X-ray for subsequent hip pain that showed she had also had an earlier fractured vertebra. She explained “ it’s got me one sided and it’s making wear in my hip… and when they found the crack, they said you must have had an iron will to get better from that, and looking back on it , I really did” Impact on psychological health Only one respondent made a link with mental ill health being a natural consequence of much physical suffering. She described a litany of serious conditions that had compounded her chronic ill health: a stomach ulcer, diverticular disease, recent infective arthritis of her knee joint following surgery for a torn cartilage and a post operative chest infection. In addition she had also had abdominal surgery that had resulted in postoperative complications requiring intensive care. She was enduring constant pain that regularly woke her at night despite analgesia. This description of her chronic ill health included the fact that she suffered from depression. She explained “ well you would with one sickness after another , wouldn’t yer” (F8) However, there was a circular view that certain conditions such as cancer, heart disease and strokes were a result of stress. One woman explains this view “ if you’re worried and you bottles up and bottles it , it cause you like high blood pressure or a mild stroke, because it happened to me mam” (F10) Another respondent made a distinct connection between mental and physical ill health. She felt that all illnesses are stress related

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 56
“ that if we were happy we were well, if we weren’t happy we weren’t well, so happy and well went together” (F11)
Although she conceded that she felt that some conditions could not be explained in this way and did not want to appear to be blaming people for their own ill health, she drew on her mother’s experience and of her own experience as her carer to connect feelings of guilt with psychosomatic illness. “ It’s the mind that cripples the body really. I was reminded of the story where Jesus said to the crippled man, ‘take up thy bed and walk’. Well before he could take up his bed and walk, he’d cleared him of all the guilt and remorse that he’d ever felt, so it’s almost like the mind will cripple the body” However, despite many respondents reporting experience of both depression and chronic physical ill health, most did not attribute their psychological ill health to their physical suffering. Depression and psychological health “ I just don’t see much future for Travellers to be honest with you” The psychological health of Gypsy Travellers in this study was a strong recurrent theme that invariably arose in the context of the multiple difficulties and struggles that they faced. Virtually all respondents spoke of personal experience or of a close relative suffering from clinical depression. Several spoke of severe depression that had resulted in suicide attempts or ECT treatment or other long-term psychiatric care. The prevalence may surprise some who come into contact with the community as respondents also spoke of the extent to which they will try to keep their experience hidden, as far as possible, even from close family members. One man explained “I said I felt great and happy and all that, you know, gave them a bluff” (M2) Definitions; terminology and recognition There was some variation in the level of understanding of the term and what it signified. Many respondents did not use the term depression for what were described as evident symptoms of the condition, but spoke of being “bad with me nerves” or “ fed up” or “suffering pressure”. One woman who had been diagnosed by her doctor as suffering with depression and did not accept the diagnosis, explained “ we says like we’re feeling bad now, in a bad mood, we thinks it’s a bad mood we’re in and we try to get out of it ourselves” (F20) Some, conversely, used the term depression to describe feeling low or down in spirits. One respondent who was under the care of psychiatric services described his confusion over the diagnosis “ I was impressed, embarrassed, depressed like. I was never aware of being mentally ill, I was never on no medication for mentally ill or anything like that”. (M5) He understood his ‘depression’ in terms of the perceived cause “ I was bad with me nerves for two years after leaving my wife and kids”

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 57
He also made the point that interventions from health professionals required discussion and explanation “I don’t know what they’re giving me, but I’m on medication… they should have
explained to me what it was all about you know. I’m not saying I would be any better with my health, but I’d be more happier” Respondents spoke differently about how they would perceive someone who they would term as depressed compared to someone who was “ really, really depressed.” One woman spoke about how she would recognise the latter “Well you’d know when someone was really depressed, they wouldn’t be doing much talking and you know, fed up and crying and everything wouldn’t they? You can know by somebody just by looking at how distressed they are” (F8) There was a sense that respondents felt that there was the sort of depression that ‘everyone gets’ and the more serious depression that ultimately requires medical intervention. The former ‘sort’ was identified as being able to be resolved by self-help and others being around to bring you out of it “you’ve got run down and fed up… I used to give myself a talking to…I’d just get up and get on with it” (F9) Concern was expressed about the extent of ‘real’ depression “ People worry a lot about depression…because a lot of people are getting depression and they’re not being able to come out of it” (F19) Secrecy surrounding depression Part of the reticence in admitting to depression was fear of the consequences of the diagnosis. There were various negative outcomes perceived, which differed slightly for men and for women, although both were concerned about how they would be viewed by other Travellers. Women were particularly concerned that, not only might other Travellers feel that they were incapable of adequate parenting, but that authorities may also take that view and remove their children into care. One young mother, who had made a previous suicide attempt, spoke of weaning herself off her medication because “ I thought my children’s more important than me and I really thought my children would have been took off me over being on ‘nerves’ tablets.” (F12) Others suffered in secret and wouldn’t talk to others for similar reasons “You wouldn’t talk to someone like you now, it’s private … you’d feel like that people’s thinking that they wasn’t looking after their kid’s properly” (F19) Denial was made easier by use of less emotive terminology than ‘depression’, and this woman explained how she played it down, while suggesting that she was not alone in doing this

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 58
“I just shrug it off and just get on with it…. I think the most Traveller women ever say to each other is ‘I’m fed up, miserable. I could do with a week away’. That’s
about as far as it goes …” (F9) Men spoke also of keeping their depression secret but implied that it was something that men should not admit to or give in to. One young respondent said that in the unlikely event that one of his mates would come to him over ‘that sort of thing’ he would “probably tell him to sort himself out and pull himself together… probably go for a few pints and that would be the end of it” (M4) An added fear that deterred respondents from seeking medical help was the fear of being prescribed medication. One woman explained “ because I was hearing so much people that you won’t go on depression tablets … they get addicted to them” (F18) There was also an evident sense of shame attached to the diagnosis, by men and women, as illustrated by the same respondent “ you’d be sort of seen ‘how would you get yourself to that stage… what have you around that would push you to that stage” There was the added fear of the stigma of being labelled as ‘mentally ill ’ “ you wouldn’t want to say that you’d been at a psychiatrist because people’d think that you’re round the bend” (F18) These examples help to explain the denial and real extent of suffering experienced by those with depression. This respondent (who later mentioned that she sometimes feels ‘like throwing herself at the wall’ or ‘downstairs to break her neck’) expresses the stoical attitude that she adopts as part of her denial strategy “ if you just think you haven’t got it , just let go , try and control yourself, it’s better…. try and clean and leave it out of your head, because if you try and think , turn my depression off, you don’t think I’ve got depression. I don’t need to see the doctors, I don’t have depression love, I say, I’m fine” (F20) Such denial and fear of seeking help can result in unrelieved suffering. One woman who resisted medication revealed the extent of her suffering “I’m having no anti depression tablets, because I reckoned if I had getten on them, I felt that bad I reckon I wouldn’t be off them” (F1) However, despite all the attempts at secrecy and denial many respondents spoke of being aware of depressed relatives or acquaintances and of ‘seeing through their denial attempts.’ This respondent explains “ they tend to make out , well I’m fed up , but everything in the garden’s lovely…… they don’t confide, but people know anyway…. Everybody knows everybody’s business in some way or another” (F9) She went on to say that even if women did open up to an extent about their experience

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 59
“ they always hold something back,.. or the next day if you see them ‘oh I was just panicking yesterday”
Depression was not the only aspect of psychological ill health described. There were also clear examples of chronic anxiety that were being experienced without recourse to medical help. One young mother described the symptoms of a panic attack that she suffered in a car whilst stuck in traffic “I’d be sitting there and I’d be pinching me skin till it bleeds, I’m pulling me hair out till it’s in me hands …..well it’s just being stuck, being no way out, …… oh I couldn’t cope with it, it was the worst thing I ever had in me life…. ” (F4) She described other similar examples of extreme panic but when asked about seeking help replied “ no , because I think I’ll snap out of it, won’t I , just be calm and smoking” Many who did seek medical help only did so ‘as a last resort’. One relative explains “ he had no choice about going to the doctor because he was really bad” (F19) Some who kept their distress hidden and refused to seek medical help paid the ultimate price. One woman said he ‘never let on that he was depressed’ as she described her grief over her son’s suicide. Another respondent, unrelated, spoke of “ an awful lot after [having] committing suicide” (M2) Impact on daily life The ability to perform daily activities was as significant when mental ill health was the presenting complaint, as it is when physical ill health is the limiting factor. This lady who described her ill health in terms of feeling increasingly “tired, moody and restless” did not describe herself as suffering from depression but recounted these symptoms “ I used to have stacks of energy; I’d clean and do, clean and do, but I can’t be bothered now” (F9) Her lack of ability to summon up energy to do the housework was a seriously worrying effect. For many others the necessary, intense day-to-day activity was a means of escape or a coping strategy to ‘keep busy’ and an attempt to ‘blot out the depression.’ If the lifestyle changed and made this option less relevant, problems were accentuated. More than one respondent made the comment that for those who lived in houses the reduced need to work so hard was a detriment to mental health. The overall misery and impact of depression was most clearly articulated by this lady who, when asked what helps her when she is feeling fed up or depressed, replied “ nothing really…. For four or five mornings I woke up and I couldn’t just stop the tears just coming, they were floating out of my eyes. Crying. And like this heavy load over the top of me mind…” (F8) In addition to the suffering experienced by individuals affected by depression or other psychological distress, there was an additional burden of fear and distress for the family.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 60
“ I knew I had to do something about it because I didn’t want me children seeing
me that way like” (M7) Many family members attributed their own depression or distress to suffering the effects of their depressed partner’s behaviour. This was particularly acute in the case of a sole daughter in a family who had been trying to cope with her mother’s dementia while rearing a young family. She struggled with the dilemma of being advised to place her mother in a home but resisted this advice despite the acute psychological distress that she experienced. She spoke of having no choice, because of her family role and duty, but also because of the interdependence with her mother that she described. She became emotional as she described how her mother reacted to the specialist who was trying to persuade her to go into a home because of the strain on her daughter “ you’re better to leave me with my girl because she understands me , she knows” (F17) Other female relatives were quoted as taking on a caring role, such as the older sister who prevented her sister being ‘sectioned’ [detained under the mental health act] by taking her home to care for her when she was suicidal. More common examples given were from women who were struggling to cope with the results of their partners drinking, which they attributed to the men’s depression. One young mother who had explained that her husband was on medication for depression gave an example of the stresses she endured “ with my husband now , he has a drink, but he’s sober now , he’s very nice , but when he drinks he tries to look for trouble in the house , tries to smash things, …. Sometimes I can’t face it the mood…but he don’t know what he’s doing, because he’s not well and he’ll drink” (F20) One man who described his own longstanding depression described the impact through generations. He described how his mother only started drinking when his father died and the effects that this had on his life. “ when I was eleven I had to be an adult immediately after my father dying like, she [ his mother] went into a place called St Teresa’s because she was suffering with her nerves” (M7) The enduring nature of grief following bereavement was a common precipitating factor in depression. One widow, whose husband had died 20 years previously, illustrated this “ I’ve never been a happy woman since I lost my husband; I’ve never been right” (F17) One woman described how both her own parents had been affected respectively by the deaths of her grandparents “My mum’s been on nerve tablets since she’s been 18; since she lost her mum and she’s still on them today” and, in explaining her father’s heart disease she said “he lost his father 2 years ago and he couldn’t accept that my grandfather died. So me Dad thinks that could have caused it” (F12)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 61
Other family members experienced added grief from witnessing the grief of their close relatives. The widow mentioned earlier explained how her son’s grief, when his wife had died, was too painful for her to bear. The awareness of the
impact on family members seemed to be a factor in the ‘conspiracy of silence’ by which efforts were made to try to conceal suffering in order to protect each other. It appears doubtful whether this was often effective and more likely added to the burden of those ‘suffering in silence’. One woman described how her grandmother wouldn’t see her small grandchildren when she was dying because “she wouldn’t like to see the pain she brought to them while she is suffering” (F12) The strategies employed to deal with grief and depression were themselves often an added cause of ill health, most notably, substance and alcohol misuse. Substance and Alcohol Misuse “I just felt like doing away with myself through drink to be truthful” Alcohol misuse Alcohol has already been mentioned as a response to depression, grief or bereavement, but the number of times it was mentioned by different respondents in these contexts suggests not only that it is a common response to try to ‘drown sorrows’ but that it is seen by some as predictable. One woman whose husband was depressed and a heavy drinker, explains “they suffer with depression , that’s why the men turns to drink…that’s why a lot of the women turns to drink because they’ve nothing else to turn to , or no-one else to turn to” (F14) Alcoholism and depression were so inextricably linked for some that one man actually described the condition for which he was attending his doctor as his “alcohol depression” However, in common with many in the wider society, there was a lack of alcohol awareness. Some affected by alcohol dependency felt that weren’t at risk because they did not fit the supposed typical picture of an alcoholic One man who had also started drinking after the deaths of his parents and had successfully given up alcohol since becoming a “Christian” explained “ I wasn’t what you’d call a real consistent drinker, one time it was just weekends… then after a while it started getting to me and I used to see people drinking on the streets, on old benches and things and I used to think ‘poor people, how can anybody get into that state’, but I ended up going to these people for a drink and then I was a regular with them, I was getting that low” (M1) More than one respondent reported deaths in their immediate family that were a result of drinking. The previous respondent recognised that he could have become a similar victim of alcohol if he hadn’t stopped when he ‘became a Christian’ “I’d have been heavy on the drink and I’d have probably killed myself”

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 62
Not all mention of alcohol was in the context of a coping response. One mother gave a picture of drinking being one goal for boys as a normal stage in ‘passing into manhood’
“the big thing with Travelling boys is passing their[driving] test, smoking and drinking” (F9) However, not all mothers accepted this behaviour and another said of her sons “ I never let them drink or smoke before they got married – after they got married I can’t do nothing about it” (F18) The picture was very different for girls and it was implied that their male peers as well as parents helped to ‘protect’ girls. One young woman who had once “tried a drink” on a rare occasion, when she was out with girls only, said “ and I’m not meant to because I’m not married yet.” She went on to explain “ all the other times [that she went out] it’d be girls and boys there, so I couldn’t get up to nothing” (F5) It appeared that on the whole families were less frightened about effects of drinking in young people, but the reported drug use in the community that was a more recent issue had a major devastating impact on users and families and was a big source of fear and anxiety. Substance misuse Two male respondents reported previous personal drug use but more spoke of known drug use among younger family members, and many more spoke of knowledge of use within the wider community. One young woman said “that’s the most biggest problem is drugs at the moment because an awful lot of Traveller men are taking them” (F19) A grandfather who had more than one young relative affected by drugs and had a nephew who died as a result, reported “the grave yard up there is full of young Travellers…all Travellers, all drugs, dead” (M1) Most were terrified of their own children taking drugs, not least because of knowledge of the dreadful effects that they had heard about. Most did not distinguish between different types of drugs when discussing their fears. The fear among families was fuelled however by lack of knowledge. One young Traveller man explained “it frightens them because they don’t understand… whereas drink, they obviously know about drink” (M4) A young mother who had a brother addicted to drugs spoke of the impact on her wider family “it really breaks the family and devastates them, they don’t know what to do , they don’t know how to help” (F19) As with alcohol, there was less reported use among women

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 63
“don’t get many girls [on drugs] – it’s a sin and disgrace if they get drunk” (F9)
The ‘disgrace’ factor increased the burden and isolation for those affected. One woman explained how she would keep her family away from any family of a known drug user “I wouldn’t let mine mix because I’d be afraid …so they get left out” (F18) The need to hide drug use because of the shame and anticipated rejection meant that it was far less likely for outside support to be sought, or even support from the wider community” “it’s never talked about, bury it under the carpet” (F9) As with other mentioned ‘conspiracies of silence’ hidden issues were rarely as secret as was hoped. The grandfather who had already lost one nephew was aware of another grandchild who he thought was affected, but said his family were trying to keep it from him “because they don’t know I know, but I do”. He added that older men wouldn’t tell me about drug use This level of secrecy also suggests that service providers would be unlikely to be aware of the level of need for specific support on this issue. One woman explained that even for alcohol addiction, despite knowledge of the existence of ‘drying out clinics, “ no-one will go into them …because I think they’re frightened they’ll find out they’re attending the clinics….because of course that brings embarrassment on mothers and fathers” (F18) In addition, many felt that there was no possibility of help anyway. One young woman who had a relative addicted to heroin said “There’s no help for them ….if you take drugs you die, that’s it” (F4) She perceived a difference between alcohol misuse with the adverse effects being gradual and drug abuse where they were perceived as immediate “ drink is if you drink it a long time your kidneys and liver fail…. There's a lot of problems, but drugs if you take it once you abuse your body already” Although many respondents experienced despair and impotence at the threat of drug addiction within their family there were reports that some families would try desperately to do something without outside help. One woman reported the reaction of a father “ and he said ‘I’m taking him either up to Scotland or down to Wales , where it’s quiet and there’s nobody there and he said I’m getting him off it and he did .He said he’s not going down that road he said I’ll lose him through drugs” (F9) She went on to explain how he achieved this “ he literally never left him on his own, and when he was what you call ‘cold turkey’ he used to tie him to the bed and wash his hands and face … and stayed with him like that for about 5 months and he said ‘you’re not going to go that way’”

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 64
The stress experienced by families was clearly described and some said that if there were a private (in the sense of hidden away) clinic they could put their affected children into they would do
“… if you could go in there and get a child better, away from drugs without any Travellers knowing” (F18) Others felt that the only recourse was to their religious faith. One woman talked about doing ‘9 day Novena’s’ (series of prayers) for her husband to ‘get him off drugs’. One of the ‘knock on effects’ of both alcohol and drug use was the use of violence,. but it was notable that one respondent felt that cannabis use was a benefit in preventing violence. One respondent admitted to having previously used ‘hard drugs’ and he blamed them for his present ‘nervous disability’ that caused him to become violent when stressed “I got that through drugs to be quite honest” He compared cannabis use favourably to alcohol and discussed the different effects noted in an acquaintance. “you could not sit and drink in that man’s company because the minute the drink was finished he’d get up and break the bottle across your head… but give that man a couple of joints and he’s the nicest man in the world… If you take drink, you’re cheeky, you upset your family… but if you smoke a bit of hash you’re not going to get into any trouble with that, you’re mellow…. I’ve smoked cannabis since I was about 15 years old and I’m 33 now” (M3) Tobacco smoking was another strategy mentioned, mostly by women, for dealing with stress. Many acknowledged that smoking was not good for their health. One woman who suffered from severe asthma, as had her deceased mother, said she would like to give up, but “ I smoke all the time, 20, 30 a day …sometimes a cigarette calms you down. If something’s wrong or anything’s going on, a cigarette calms you down” (F15) Another, who recognised the dangers of smoking and said she ‘didn’t smoke around the kids’, explained that she’d tried numerous times to give up “ but I can’t . It’s something I can’t give up. It’s just like a nerve. For your nerves, Calms you down. I think for me anyway it does. It really calms me down the cigs” (F19) Smoking as part of male Traveller youth culture has been mentioned, but there is another cultural dimension to the issue of smoking that concerns ‘respect’ for parents. This Traveller man explains how he would not smoke in front of his parents even though they knew he smoked and that they knew that he was aware of their knowledge. “I’d never do anything in front of my parents- like I wouldn’t ever smoke in front of them, you know, even when I became of an age…I had respect” (M1) OTHER HEALTH ISSUES Experience of trauma, accidents and infectious disease were all mentioned but not given prominence. Certain conditions such as cancer were reported as prevalent

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 65
among families and extremely feared, but none of the respondents had personal experience of suffering with cancer.
Conclusion The extent to which Gypsies and Travellers understate their experiences of ill health and express a stoical attitude that one should ‘put up with it’ can easily distort outsiders’ perceptions of the actual level of health need. In addition, the cultural importance of family care in preference to outside support further conceals the additional health impact of being a carer that is being carried by many respondents and their families. The experience of ill health is exacerbated for many respondents by communication failures that result in sub-optimal management and unnecessary endurance of symptoms. Lack of knowledge and resulting fears about certain conditions often result in delayed presentation, which in turn may result in deteriorating health. The high level of physical ill health described by some families is endured and managed with minimal fuss and complaint. Psychological ill health, seen as a result of the many hardships faced in their daily lives, is also endured and often results in harmful coping strategies that further intensify the overall burden of ill health for the individuals concerned and for their families.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 66
Barriers to accessing health care
Introduction This chapter is concerned with the reported accounts of experiences with the health service. Many Travellers reported the experiences of close others and described how these had had a profound effect on their own expectations and also on where they chose to attend for health care. However, much of the data presented here relates to accounts of first-hand experiences. Reputations of different doctors and their practices and also of different hospitals were well circulated within Traveller communities, and these services either frequented or avoided accordingly wherever possible. In this study most Travellers were interviewed in locations where there was specialist health visitor provision and in this respect their experience is not universal. However, many of the Travellers had also lived in areas where this service was not available. Desirable characteristics of health staff were frequently mentioned, and in this context the demonstration of cultural sensitivity, and granting the same respect to Travellers as to other patients, featured most emphatically. Many Travellers supported the idea of a separate dedicated service in order to achieve this desired outcome. Staff behaviour and, most importantly, communication difficulties were the overriding concerns and the factors that most influenced Traveller’s impressions of their health care experience. The various elements that contributed to poor communication were key to health and health care outcomes. Communication Communication difficulties with health professionals resulted in many respondents being unclear about their actual diagnoses and in some cases unclear about the potential significance of their conditions. Attempts to inform me of their diagnosis included I’ve got “ something syndrome” and “ I have a brain that’s not wired in”. One male respondent described having been in hospital for “ a big needle through my back into my kidneys and liver. I still don’t know what’s wrong……everything’s working out right now so far” (M2) This limited information and understanding may help to explain some of the variance attached to significance of a diagnosed condition and the greater weight attached to day-to-day symptoms experienced. Typically any misunderstandings arising from communication difficulties were rarely discussed. Many health workers may believe that their explanations are understood, but as one Traveller explained “they told me , but I wouldn’t know; they did [explain] but I didn’t understand” (M2) Many Gypsy Travellers, particularly older people, described the effects of a lack of formal education for many Gypsy Travellers in relation to access to health care.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 67
Lack of familiarity with the standard use of vocabulary “ all the big words” and fears about inability to communicate were major concerns
“ I don’t open up to a lot of people…I’m not a very good communicator” (F4) This was associated with a lack of confidence in the ability to communicate their needs for fear of being thought of as stupid for ignorance of health matters or for expressing particular health concerns. “ I wouldn’t go to the doctor now about anything like that [sexual or maternal health matters]…Because they think I’m a fool [that] I don’t know about them things” (F4) Some unspoken fears can give rise to conflicting views between the patient and doctor about the perceived relevance or urgency for a consultation. One respondent who was concerned about her amenorrhoea explained her anxiety to me “ cos I was a bit worried about not seeing them [periods] because I thought it go up to your head and that was probably causing the headaches, …. I was getting worried about it when I didn’t see them, but I’ve seen them now “ (F10) Poor communications in consultations can give rise to misunderstanding about prescribed treatment and the purpose and appropriate use of medication. In some cases, extreme anxiety can lead to angry and hostile styles of communication. This in turn can lead to staff feeling that Travellers abuse the system and are behaving unreasonably and a cycle of communication breakdown can ensue. The following example is an illustration “ my husband he went completely mad, that was his baby and he was going to kill the doctor . Honestly he lost his temper. This other doctor came in and calmed him down and that and she was in there 14 days. But this specialist came and said why don’t you just go home. ‘If we go home, we take the baby home’. He said ‘why don’t you Gypsies get your own doctor’ ” (F2) However, in encounters with any groups or individuals, these defensive reactions are common where other communication strategies are unavailable. There is evident need for health professionals to be aware of the importance of eliciting the accuracy of the Traveller’s understanding about their diagnosis, the implications and imparted advice. Gypsy Travellers often reported taking a family member to an appointment in order to assist communication. However, this could also hinder effective communication. One Traveller spoke of withholding information from her doctor because of the family being around. “ when I got to the hospitals and all that with my family around me I would never say I’m a [diagnosis] or anything like that” (F13) For many Travellers, therefore, their dedicated health visitor was the preferred advocate to accompany them when possible.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 68
Large numbers of relatives trying to seek information compound communication difficulties, as one Traveller, who had tried to get an explanation for her mother’s ill health, explained
“There’s eleven of us … , they told one one story and then tell a different one a different story and there were three or four different surgeons there”. (F13) Further problems can arise from the cultural practice of large numbers of extended family visiting a hospitalised relative. One woman explained that her relatives would be thrown out if they came in a large crowd and inability to be able to communicate the cultural need for this practice further disempowered her. “ It doesn’t cause any problem for them, but it would cause it for me because they said you can’t have this much visitors visiting you” (F8) Interviewer: What do you say? “You couldn’t say anything could you?” Staff awareness of cultural factors affecting use of health care Non-attendance for cervical screening appointments and also for early antenatal appointments were often attributed to embarrassment by those interviewed. “ I’ve only ever had 2 smears and I would never get another….it’s very personal … you see Traveller women don’t like strange people looking at their private parts whatever” (F19) Indirect communication was the preferred way that many Gypsy Travellers deal with private matters within their own families “ I tell them in different ways, I don’t come right out with it…well you’re hinting and that sort of thing.” (F18) Direct questioning about embarrassing or sensitive issues from health staff can inhibit further communication. It was remarked that, rather than admit their embarrassment in a consultation, some respondents would stoically sit through it but would simply make a decision not to return “ if it’s a male doctor I wouldn’t say nothing, put up with it and just fly out of the door…make sure I didn’t go back again” (F18) The felt need to keep private matters to oneself can prove detrimental. One respondent spoke of an occasion when she had attempted suicide and had been referred to a psychiatric nurse. She made the comment about the nurse, saying, “ she couldn’t understand why I was suffering with it” [depression], yet on exploring this in the interview it transpired that she had not felt able to explain to the nurse that she had been experiencing domestic violence.
Desirable characteristics of health staff were frequently mentioned, and the demonstration of cultural sensitivity, whilst granting the same respect to Travellers as to other patients, featured most emphatically. Many supported the idea of a separate dedicated service in order to achieve this desired outcome. One respondent emphasised the difference it made in having a worker who really understood the culture when she described her health visitor (specialist for Travellers)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 69
“ it’s so easy to talk to her because she understands how Travellers go . She understands everything about them”…you can talk to; you can sit down and you
can have a conversation with her and really confide in her, which you can’t with most people” (F19) The trusted dedicated health visitor is often viewed as a back up to the doctor “ if I go to the doctor and he tells me there is anything wrong and I’ll ring [Health Visitor] and I’ll ask her” (F8) Others expanded on a need for a dedicated service for ‘private things’ by recounting previous experience “because they do that in Ireland and that like in the sites, a mobile comes round for the Travellers…. and they’ve been coming round for years and they really understand the Travelling culture and everything and their religion, so they know what its’ like for Travellers” (F19) There were numerous examples given of health staff, and doctors in particular who failed to ‘listen’ or to take them or a family member seriously. “ they don’t listen to you, they tell you what they feel….it’s like you are there, but in their eyes you’re not there” (F14) Doctors who did listen were much appreciated for seeming to value them. The same respondent also spoke of a positive experience and emphasised not only that this doctor listened but also that he examined her. “ He said talk to him, but he was very good like that he listened … he just wanted to listen. I explained all that to him and he examined me…” (F14) Many Travellers spoke of lack of confidence in the doctors for their failure to examine them (or their child) as they attached great importance to ‘being checked over.’ It was also important for doctors to be convincing in their diagnosis. One Traveller was particularly unimpressed with her doctor who said she thought her child’s rash was due to chicken pox “She didn’t tell me, she said I think it is, which is different… she was a divvy I think” (F4) It appears to be the cultural understanding in particular that helps to engender trust and reliance on specialist health visitors. The varied nature of the support expected and provided by a dedicated health visitor for Travellers included, making appointments, reminding about appointments, accompanying to appointments and acting as an interpreter between the client and other health professionals during and after an appointment. They were also reported to carry out an outreach role in work more usually associated with a practice nurse, such as regular monitoring a respondent’s blood pressure and ensuring that she was taking the correct medication. It was apparent that there was a dearth of available support outside of the community, with dedicated health visitors being seen as willing advocates in situations affecting their lives and well being in the wider sense “without having [Health Visitor] there we wouldn’t have got a house … she’s helped me out a lot here to try and get re-housed” (F6)
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 70
Continuity and knowledge of family One cited reason for satisfaction with a health worker was that they knew their
personal or family history. This knowledge and understanding from the health worker instilled confidence that they would not need to explain their background or their situation. One respondent gave a typical example of a neighbour who went to great lengths to ensure continuity for the care of her chronically disabled child “ Her mum has been all over the country and no matter where she’s been, if she had an appointment with that hospital she’d drive all the way back, even if she had to live with relatives or book in bed and breakfast, she’d drive all the way back and get her seen by that same doctor. She won’t take them to any doctor, they stick with the one that they know” (F9) Having to reveal details of their life and risk misunderstanding or discrimination from an unknown health professional was an obvious deterrent to seeing a new doctor “ well like I’ve just told you and you understood, but they [ others who don’t understand Travellers] would think ‘oh isn’t she thick’ So I’d not be bothered with them . Let them think that and I’ll not bother.” (F16) This desire for returning to a trusted doctor was also connected with a fear that a new doctor would not have the information to hand to treat them appropriately. “If I kept swapping over, like if I said I was going to this one and left that doctors and the files would be gone by the time I go there. So I just stick to the one doctor” (F5) Experience of and reactions to discrimination and racism Cultural insensitivity, either unintentional through ignorance or resulting from racist attitudes, was a strong feature of compromised communication. “you can tell in a second , you can tell by their attitude, they don’t look you in the eye, it’s just sort of ‘what’s the problem’…… they do palm you off the minute they find out you’re Travellers” (F9) Racism was also blamed for failure to obtain services, with several experiences reported of inability to get registered with GP’s. Certain hospitals were named as being discriminatory towards Travellers as illustrated by this respondent “ the x hospital, they’re not interested in Travellers” (F6) Discrimination was not always overt, but excuses were readily recognised. One Traveller described a typical scenario where she would be asked for her address and be told ‘oh well the doctor’s busy he can’t see you ’. She went on to explain “You know we’ve got it so many times through the years …it’s got to be [an excuse] (F20) Receptionists acting as gatekeepers were often described as showing particularly hostile or unsympathetic attitudes “ the receptionists are harder to get past. They’re not nice I think they’re doing the doctor a favour …keeping you away from him- ‘ I did something good today, I kept the Gypsies away’ ” (F9)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 71
The overriding need was to be treated equally. It was deemed sufficiently uncommon to be worth mentioning when respondents felt that they had not been subject to discrimination. Positive comments about treatment were sometimes qualified by
the explanation that they were treated the same as other people. “ they were very good, they never treated you no different from nobody else” (F9) The pervasive experience of racist and hostile attitudes reported by Gypsy Travellers, with resulting anticipation of such treatment, can lead to suspicion and general mistrust. One Traveller who had been told her expected baby was going to be born with spina bifida (which was later born in a healthy state without the condition) and was offered a termination of pregnancy reacted “ but I think myself it was they wanted to take my life in their hands and get rid of the baby…. My husband was with me and he really did lose it…. But the way I looked at it, it was because I was Traveller, just less Travellers born to, just abort it and sterilise her and that’s it” (F14) Defensive and hostile behaviour from respondents was one of several reactions to the experience of actual or suspected discrimination. One woman, who suspected that her doctor was being dismissive and patronising towards when giving her tablets that he said ‘would make her feel better’, said “so I picked them up and throwed them back at him and I said , I don’t want your tablets ….I said you’re a waste of time, I’ve been coming her for months , getting worse and you won’t even examine me, you don’t have the faintest idea what’s the matter with me” (F9) Protective hostile behaviour from relatives on behalf of the patient is also mentioned “ I was afraid, and I was terrified and I was that bad that the dentist was being that rough that my husband was going to hit him” (F4) There was an acknowledgment and understanding by several Travellers that their behaviour was often anticipatory and sometimes calculated to ensure that treatment was obtained. One mother said “ they just wouldn’t accept us because we were not registered and we had to kick up a fuss at the desk to try and get her seen” (F6) Many will avoid the perceived risk of delayed or sub optimum care, especially for a sick child, and go straight to Accident and Emergency departments, although here can they can still encounter barriers to accessing care. “ She had a virus through her body and I took her to the hospital and they wouldn’t see her. They told me to fetch her back to her own GP and I told him that our own GP is in Norwich and it was like a 3-hour journey to get back. I mean they still wouldn’t let me see her ……I said straight, because I lost my temper, it’s all because we’re a Gypsy, that’s why you won’t see my child … They didn’t see her so I had to take her to another hospital”. (F12)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 72
Effects of lack of knowledge & understanding on use of health care Lack of prior knowledge about the body in general, medical conditions,
prevention of ill health and related health matters influenced the likelihood for attendance for health care. Illiteracy was frequently mentioned as a handicap in respect of acquisition of knowledge “ if you don’t read and write it’s difficult to get information” (F19) In the absence of education there were two main sources of information. The commonest source was information handed down or deliberately sought from family or peers in the community. One mother, explaining where she acquired her health information from, replied “ just learnt it for myself, picked it up from the old people, from me great grandparents and me own mother and father” (F3) The other main source of information was from the media, mainly television. Stories from the media more often created fear in the absence of counter information. However, in some cases personal experience compensated for lack of formal knowledge. One young mother illustrated this by commenting that “when you rear four kids you know when they’re really really unwell” (F19) Preference was expressed for schools and for health visitors to provide health information. However, in some instances, particularly for young people concerning sexual health or information surrounding childbirth, it was felt by older generations that knowledge was a bad thing. One grandmother bemoaned the current trend to openness about such information “ the teachers told me we have to show them the facts of life .Says I , they know too much…it destroys them, it ruins families” (F3) For others, however, lack of knowledge increased the fear factor and the fear had a considerable negative impact on the perceived significance. One male respondent, aged 55 yrs, described his initial fearful reaction to the diagnosis of diabetes “ I thought it was a very serious illness… [I was afraid] that me leg would fall off, that I’d lose me eyesight, you know you hear all these kinds of things” (M1) This man’s fears and perceptions were influenced, as in many other cases, by stories of other’s health experiences. These influences, in addition to fears about health consultations or the clinical process itself have an impact on the extent to which respondents in some circumstances will continue to suffer symptoms rather than opt for possible investigations or treatments. One Irish Traveller woman, now in her late 30’s, diagnosed in childhood with a chronic condition affecting her digestion, was no longer having the special prescribed diet. She explained that this was because her diagnosis was not recorded. Although it was suspected that her condition was contributing to serious debilitating anaemia, for which she was receiving regular painful injections, she opted to decline the offered investigation to confirm the diagnosis, because of her mother’s account of the procedure.
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 73
“ They take away a piece of your gut. Me mum was often telling me it was a very severe test, so I didn’t really want to have it done again” (F13)
Embarrassment was made worse by lack of knowledge, and when workers displayed unintentional lack of cultural sensitivity over explanations of procedures. One respondent spoke of her distress at an antenatal hospital appointment “ and the woman said to me ‘do you want an AIDS test, HIV whatever. I said ‘no love…I felt like, insulted …So she said are you sure, what do you call it routine, ‘no love I don’t need one, I’ve only ever been with me husband…I got really upset with the woman; I didn’t have one anyway.” (F4) Further distress was experienced at the subsequent offer of an amniocentesis. Lack of knowledge and reluctance to seek explanations resulted in some respondents enduring ill health or, in the case of one woman who feared blood transfusions, receiving unpleasant alternative treatments “ he[doctor] wants me go up and get a blood transfusion …I wouldn’t go for one…I’m frightened of the AIDS and all that …….I have the iron injections every second day , 11 of them” (F13) Others, in using denial as a coping strategy, prefer not to have knowledge of certain conditions that were taboo. A respondent who was upset when offered a routine antenatal HIV test and confessed she knew little about AIDS said, when offered more information “No I don’t want to know, what I don’t know can’t hurt me” (F4) However this was the same respondent who had earlier avidly sought information due to her lack of knowledge about drugs. This would suggest that the strong cultural taboos concerning sexual knowledge are particularly hard to overcome. These cultural beliefs are prominent among the older generation and their influence may continue to inhibit the acquisition of such knowledge by the younger generation. Lack of knowledge and understanding was a contributory factor to extreme fears about certain conditions. These fears were often compounded by personal family experience. Cancer was the most feared condition, but to an extreme that some Travellers preferred not to even use the word. The belief that a diagnosis of cancer was an automatic death sentence that couldn’t be avoided has been referred to, with associated delayed attendance for diagnosis of symptoms as well as reduced likelihood of attendance for screening. GP registration The issue of trust and expressed need for continuity has already been mentioned, but apart from a conscious desire to travel to a known doctor, there were considerable practical difficulties encountered in trying to re -register in a new area. One respondent when asked what about the greatest obstacle to Travellers being healthy replied “ to get signed on with a doctor” (F16) There was a consensus that it was more difficult to obtain health care when travelling

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 74
“ if you’ve no fixed abode , they’ll no register you” (F6)
However, one respondent commented that this had not always been her experience and that in the past a Traveller could get seen “ just walk into any doctor’s and tell them you’re just moving around… but that was about 20 odd years ago. … See there’s a lot of doctors now won’t see you temporarily” (F6) Some Travellers who were not continually travelling and had a local permanent address used the system quite happily by effectively having a local temporary GP and a permanent GP elsewhere and choosing which to go to according to their needs. There were several accounts of Travellers ‘getting around the system’, knowing that a permanent address is required. One typical example is described “ it took em nearly 12 months to be registered because you used to go in and fill in a form and say temporary or if they filled in temporary they might not be accepted . So what they’d do was, I’d say I’m over with my cousins and I’m having a week here, just so the doctor would see em while they was here” (F9) Several Travellers described being seen as temporary residents, but more often only for specific minor immediate needs. For chronic conditions or anything considered serious enough, there was a general preference to return to a GP with whom they were registered and in whom they had built a trusting rapport. Even the fact that an appointment would be required was no deterrent to travelling long distances to be seen by a trusted GP. One respondent’s account demonstrates how the apparent obstacle of living away was overcome, “One of the children had a boil on the leg, she could have seen the nurse down here, but she wouldn’t. She got in the car and drove the 70 miles back and stayed with her mother till she got an appointment” (F9) One housed respondent who stated that she had no trouble in registering with a doctor mentioned the importance of understanding the system. She explained however that her aunt who had come over from Ireland had experienced difficulty in getting any doctor to take her on until the specialist health visitor finally helped her to get registered Appointment systems The combined factors concerning time, urgency and apprehension help to explain one respondent’s explanation for her local surgery having set up a children’s health clinic on the site. “because Gypsies have had a problem about making appointments , keeping it and waiting in surgery” (F11) By getting to know the doctor and developing confidence in him at the site clinic visits this particular respondent eventually trusted him enough to consult him about herself and then felt able to take up his suggestion of making an appointment to see him at his surgery – something that she had previously avoided.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 75
For many Travellers, the specialist health visitors, consistently valued in this study for their cultural competence, were the preferred advocates to accompany them, when possible, to help them to access health care, both in terms of finding a GP
who would register them, either temporarily or permanently, and in terms of acting as an advocate, by being willing to help them to obtain and keep appointments “I went down to visit her [daughter] and I took real bad …there was this health visitor came out, she was a lovely woman and made this emergency appointment for me at this doctor” (F8) Another way in which one respondent viewed the health visitor as assisting access, was in instilling self-confidence “we always embarrassed to go to the doctor .. you know a conversation with someone , it’s embarrassing . She’s taught us like that to have your say, you know? You’re entitled, you’re entitled to a doctor like everyone else” (F1) Avoidance was a preferred option for many to making an appointment and then failing to keep it. The majority of respondents spoke of making conscientious efforts to keep appointments that they had sought for themselves. One elderly respondent explains her reasons “ I don’t let he down and he wouldn’t let me down I don’t think… I don’t miss cos I think to myself, when he was waiting for me and I’d had an argument with myself saying he’s misglecting somebody else, and I wouldn’t do that” (F17) Unsolicited appointments for smears or other undesirable procedures were less likely to be kept. One respondent avoided having to miss antenatal appointments and then explain her absence by consciously avoiding telling anyone that she was pregnant “I just kept away until I was perhaps six months. They’d say where have you been?” (F11) The major concerns expressed about appointments were the unacceptable delay if there was serious concern about a child and the practical obstacle or lack of confidence for some in feeling able to make an appointment. Some respondents however felt quite able to make appointments themselves with their own doctor. One respondent explained that she accessed a dentist when she was desperate and her health visitor was not available “ but would you believe, I did go myself to the dentist, I knew it was really bad. So I thought, yeah, I have to go to the dentist now; I can’t miss my appointment. I went myself and found the dentist” (F5) The busy hardworking lives of women were often mentioned as an explanation for non-attendance at GP surgery or at hospital appointments. When I asked one mother why she never kept her referral appointment for a scan, she explained “time went so quick, when you have kids you haven’t got enough hours in the day , the time goes so fast. I still do suffer with my side” (F14) The awareness that appointments could be time consuming can reduce the likelihood of attendance in the context of busy lives. This respondent did keep her appointment but explained

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 76
“they keep you, you’re there for hours in’t yer… it’s hours and hours waiting around” (F15)
However some respondents spoke of the importance that they attached to certain appointments. One spoke of her profound distress at her inability to keep an antenatal appointment, which was important to her after a previous miscarriage. She was also very upset at being let down herself as she had prioritised staying at home for an appointment that a housing officer had arranged but then failed to keep. “ I got up at about half past eight and I had an appointment at the hospital for 12 o’clock which I never miss, my antenatal appointments and I sat there a full day waiting and she never came and that put me in a bad depression, I went mental, I went absolutely mental…I was bawling, I was shouting, I was angry, I didn’t want anybody around me I just wanted to be on my own…” (F6) The women portrayed the men as being very reluctant to wait for appointments “they don’t like having to wait in a queue and sit and listen” (F19) Time may be the factor here, but others factors mentioned, such as embarrassment, may be equally valid explanations. One respondent explained the difference it made when his psychiatrist gave him time “ he was all in a rush at you , the doctor GP , but she talks slow and gives you time to think, there’s no rushing you” (M7) Fear is an added explanation for the urgency sometimes exhibited when an appointment is sought. This fear is intensified when it is the respondent’s child that requires medical attention. One respondent explained her reason for going to a hospital emergency department rather than wait in a “walk in and walk out centre” “ you would have had to wait a long time and we would have had to wait about seven to ten hours … it was quite long enough and she was burning up and being sick” (F12) When children’s health was at stake absolute priority was given in respect of time and urgency, in contrast to the lack of priority of time for their own health needs. One mother explained how she was prepared to wait and insist on her child being treated even though the hospital staff felt that his case wasn’t urgent and were going to send him home to return the next day. “ if you have to see to a sicker kid, go ahead I said, I won’t stop you … could have waited if it was matter of life and death , but I’m telling you [he] is not well , it’s just when you’re ready , I said , look at him …. We will sleep on the floor, we don’t mind, … get the business done” (F20) Prior experience of time being crucial to the prompt diagnosis and treatment emphasised this urgency. One mother who had experienced a near fatal delay in diagnosis of meningitis in her sick child stated “I imagine every minute counts when a baby’s not well because you don’t know what it could be” (F1)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 77
Health records Although it was usual for Gypsy Travellers to carry and use their pre-school
children’s health records, only one respondent with chronic ill health mentioned self-held health records for herself in the context of travelling. “ got all me records; I’ve even got the papers where they’ve got me scanned” (F10) However, it was a concern for many Travellers that doctors would not have their records available if they were only temporarily registered. This has already been highlighted as an important reason for wanting continuity of care with a known doctor. This importance attached to records and continuity was given as a reason for it being easier to be healthy if living in a house compared to travelling “ if you were travelling and you were going in all different places … how would a doctor know about you?…whereas at least if you are in house your doctor, like my doctor’s got all my records” (F18) There was also a lack of trust that information would be passed on safely between hospitals. One respondent explained why she continued to return to a London hospital for her child’s appointments rather than accept an offer of transfer to a local hospital “ I’m afraid, because I think, like all these tests that they’ve got all on paper at their hospital, I think they’ll get lost and she won’t get seen properly” (F4) Conclusion For various reasons, some arising from extended mistrust of non-Travellers generally, Travellers in this study demonstrated low expectations and poor experience of standard health service provision. Reputations of different doctors and their practices, and also of different hospitals, were well-circulated within Traveller communities. Wherever possible, these services were either frequented or avoided accordingly. The role of the specialist health visitor featured positively and prominently, particularly her/ his role as an advocate, and was a significant factor in access to and experience of health services. These findings give weight to the reported need for health service staff and service provision to be culturally competent.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 78
Environmental factors
Introduction Despite a tendency towards a fatalistic attitude concerning health, environmental factors were seen as strongly influential. Two major aspects were seen as significant in respect of health: the conditions per se associated with where and how Gypsy Travellers lived, and the degree of control or choice they had to influence these conditions. The cultural meaning, already discussed, that is attached to these lifestyle factors also seemed significant. The most important factors referred to were external ones such as accommodation and work. Other factors concerned with individual behaviour, such as diet, were generally given less prominence. LIVING ARRANGEMENTS “ it would be good for me to get out of that place , because while I’m here I’m getting worse and worse and worse and worse “ Accommodation was the overriding factor, mentioned by every respondent, in the context of health effects. These effects are seen to be far reaching and, although clearly seen as crucial, are not exclusively concerned with actual living conditions. For most respondents the ability to choose their style of accommodation and to decide for themselves whether, or how, they continue to live a traditional travelling lifestyle is of fundamental importance and crucial to their sense of independence and autonomy. Many talk in terms of a ‘Hobson’s choice’. The lack of choice and/or the intolerable conditions, which the majority of respondents speak of, are an indication to them of the negative way in which they are viewed by the non –Traveller society. It is this feeling of injustice and persecution that is often forcibly expressed as much as concern about the adverse effects of the conditions per se. In an earlier chapter it was pointed out that respondents saw their depression in the context of multiple difficulties faced. Accommodation issues were among the most common such difficulties described. Respondents referred to various important considerations in respect of their accommodation preferences. These include access to services and ability to register with a GP, support and security of being close to extended family, a non-hazardous environment, security of tenure and the notion of freedom for the children. All of these impact on health but can be conflicting, thus make their prioritisation of needs and choices more difficult. There are also other factors aside from health considerations that come into play such as availability of work and access to education. The respondents in this study are living in a variety of types of accommodation: council- run permanent Traveller caravan sites; temporary transit site; privately

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 79
owned family sites; caravans (trailers) on unauthorised stopping places; houses and a hostel.
Many respondents gave health reasons for their most recent change of accommodation, particularly for a move into housing, but no single type of accommodation was identified as a satisfactory solution. Living in a trailer and unauthorised camping Whichever type of accommodation they are presently living in, virtually all respondents have experienced the ‘ traditional’ travelling lifestyle in a trailer, either in the distant or more recent past. Almost without exception it is the traditional travelling lifestyle that is still craved, “ the travelling way”, although with qualifications, “ as long as you had water and toilets and showers”. The seemingly inherent yearn to live in a trailer, even by those Gypsy Travellers who were brought up in a house, is expressed by this housed Traveller “ I don’t know what it is, but it never leaves you, never leaves you, no” (F18) On of the most frequently mentioned health benefits of living a travelling lifestyle, and often the first called to mind by respondents, is the freedom associated with being out doors. As mentioned in the section on beliefs in relation to mind and body, this is often described in terms of the importance of “fresh air”. This respondent explains “ I was happy if I was in a caravan… freedom and all that… you know, fresh air. I’m used to plenty of fresh air” (M5) Fresh air and freedom is particularly emphasised in relation to children. One young mother explained her regret at needing to move into a house in terms of the perceived lost health benefits for her children “ in a house they’re always indoors , most of the time indoors , but in a caravan they’re always outside , running around , playing or doing whatever .. that’s better for them. They never really get ill” (F19) Travelling is seen as offering another type of freedom, in giving choice and ability to move away from actual or potential trouble, either to escape hostility or victimisation from housed neighbours or to escape from a particular notorious criminal travelling family. This “obligation to avoid” is a cultural way of dealing with such problems within the community8 The importance of close kinship relations is one of the major considerations that features in relation to travelling. The chance to meet different people and socialise with other Gypsy Travellers is also an important requisite. “you’re going to some place , and you’re pulling in and say it’s a nice green field and there’s like, it could even be 10 other trailers with you. I mean, other different families and people and you pull in, and I mean, its company … I mean it’s good” (F5) Respondents spoke despairingly of the stress arising from a lack of choice in being able to stay anywhere before they are forcibly moved on. This respondent who would prefer to still try to travel but cannot because her husband no longer will, explains

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 80
“ you’re just as well to stay in one place and just learn to live every day because there literally is nowhere out there you can stay ……So that is what a lot of people do now, they just don’t bother going, The only thing you do is go to a Traveller fair,
say have a week on Appleby, a week on Stowe or whatever. That’s about it” (F9) This expresses her feelings as she describes her reasons for moving onto a site “ If I had a choice, I’d sooner hang out and find a piece of ground somewhere, because the only reason we moved on here was because we had the kids all small and we were sick of being moved” (F9) However, as one respondent pointed out there are many Gypsy Travellers who are compelled to continue travelling because they are unable to gain one of the limited available places on a permanent site. She explained “ there’s a lot of sick people out there that can’t get a place to stay” (M2) The hardship entailed in accessing basic facilities was also cited as a motivation for abandoning a travelling lifestyle. This respondent, who described how she suffered a nervous breakdown when she was younger, gave this explanation for her parents moving into permanent accommodation “ where we were in the camp we were stuck in this fool of a place , like in the middle of miles of bus stops but there was no bus …. I used to have to walk from there and do all the cooking and cleaning and get all the clothes and bring them to the laundry on the far side of town and walk and push a big pram with a black bag of clothes… I felt my father wasn’t well enough… and I had to get the water and everything and it all got on top of me… (F7) The travelling lifestyle was also seen as potentially hazardous in view of limited safe stopping places. This father points to the risks from nearby fly tipping “ when they’re dumping from the housing estate, you don’t know if they’re dumping any medical things and you’ve got to be aware of that; your eyes are constantly on your kids in case they pick something up and say that’s sweets … I mean them woods there , there’s’ sets of dirty needles and that lying …” (M3) The hardship from weather conditions was mentioned by parents, and by older respondents who pointed out that the wet and damp endured from years of travelling and living on the road in all weathers has had a detrimental effect on their health. Many blame these conditions for their arthritis and chest complaints. “ I do know people that has been affected with chest problems, over this and plus back problems, you know with all the wetness that we get” (M1) Despite the references to health risks, this older respondent goes on to reminisce about the positive benefits of travelling “I sit with some Travellers who are not as old as me, they say ‘I’d love to have then days back again, you know. We’d love to have them back again’” (M2) Today, the benefits of a travelling lifestyle were, for most, now outweighed by the difficulties

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 81
Living in a trailer on a rented site
Most respondents interviewed on sites were living on rented council sites and for them more disadvantages were reported than benefits. The perceived impact on health varied according to the type of site, conditions and geographical location, but also according to ownership of the site and how it was managed. The main advantage to living on a site was the option to live amongst other Gypsy Travellers and, where possible, amongst other family. One respondent explains how he was able to bring his sister down to live on the site he was on, in order for her to be supported by relatives “ because my sister , she had no-one to turn to … since me brother died , she’s closed herself away and I thought by bringing her on here , there’s people , there’s young girls she gets on with, relations she gets on with …. She’s been coming out a little bit” (M1) Although respondents who lived in houses spoke of going to visit family on sites, this did not suffice, as this young housed mother explained “ it’s not the same is it, do you know what I mean ? You like to be living with them. You like to be together like” (F20) For some respondents the lack of choice of close neighbours on a site was viewed as a drawback “ I would not like too much of a mixture [of families], different Travellers, because that’s where all this trouble comes in” (F18) One of the desired benefits that lead to seeking a place on a site is to access facilities, otherwise unavailable when stopping on unauthorised sites or poorly serviced transit sites. This respondent, in extreme poor health, living on a transit site explained that she would love to be on a council site because “ there’s a bathroom and hot and cold water”, whereas on the transit site there are “ no civilities like that” However the cost implication was seen as a downside. In contrast to renting a council house where structural maintenance is included in the rent, the rent for a council site only includes the pitch and any outbuildings and services. The family is responsible separately for providing and maintaining their trailers (owned or privately rented). This respondent explains “ it costs you a fortune to live on a council site. If you’ve got 2 caravans they charge you rent for them [each of the pitch spaces] and that can be £100 per week just for 2 caravans and then you’ve still got to pay community charge, electric, your own water bills and things like that … it was just too expensive to live on there plus try and earn a living and save money …… so that’s why a lot more Travellers are settling down in houses (F9) The overwhelming disadvantages to living on a site, reported by many, were the site conditions and the surrounding environment where they were located.
The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 82
“ I blame moving there caused my health … I mean it’s a health hazard down there…that’s when my health started to go wrong. See I’m right against the motorway, then the tip and then the sewerage (F2)
The immediate location of a site near to hazards such as railway lines and canals, as well as hazards on site, were a major cause of concern to families with young children. Such concerns resulted in this mother restricting her children’s freedom to play outside, unsupervised on the site. “ when you leave them you’ve got a canal. You need a site maybe in a safe community…. You need your electric done proper … behind there that’s where the electric wires runs for the caravans, well they’re just open to kids … a lot of hazards … That’s why I keep them in all the time” (F14) This respondent speaks of two different sites in a particular geographical area that were seen as a source of ill health for her children “ I was never away from X hospital… diarrhoea, sickness, things like that, the flies come in and they’ve gone on the bairn’s bottles and things like that… any of them 2 sites there, you’re guaranteed if you go on them and you’ve got a bairn under 2 years old that you’re going to the hospital in the first week” (F6) Location in respect of access to amenities, including health services, was also a factor. For many respondents, particularly older ones who had longer prior experience of the ‘freedom’ of travelling, the feeling of being confined was source of real distress “ I see something like those railings [site boundary railings] and it would feel like a prison” (M1) Another erosion of freedom was the general lack of autonomy and control over their lives “they’ve got a thousand rules and regulations” Housing Most respondents spoke of their decision to live in a house as being forced by circumstances rather than a preference. Several respondents spoke of family members and peers who could never settle in a house. One explained her reaction after being given temporary housed accommodation when her caravan had been destroyed by fire ‘couldn’t stick it and begged to leave after one night … could never live in a house’ (F16) Being able to register with a doctor is an often-reported benefit of living in a house “ it would be easier in a house because if you’re ill your doctor’s around and everything” (F18) However, although a move into housing for health reasons may seem to be beneficial in order to acquire necessary services and facilities, the psychological impact of giving up a travelling lifestyle and the potential ‘culture shock’ can counteract this perceived benefit. This mother with a chronic illness explains “ the house is like toilets, baths , warmth, comfort that I didn’t have in the caravan. I could handle the caravan before I was sick but there when I got unwell I couldn’t, it was just getting too much for me … because you’d have to move every day basically.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 83
Police would move you on every…, whenever the council… so that weren’t helping, not at all…… I wish I had my health back because I imagine I wouldn’t be here. I don’t know (sighs) It’s just the way you’re reared up isn’t it” (F1)
The same feeling of confinement that was mentioned by some respondents in relation to living on sites was also mentioned in respect of living in a house. This was particularly highlighted by the behaviour of children who had not previously been used to this style of living. This mother explains “ when they go into her [relative’s ] house they just go wild . It’s like they can’t handle it … It’s like they’re in prison. It’s like they’re locked up, they just can’t help it. And it’s the same for me love, I just can’t handle it either” (F14) Central heating was a source of blame attributed to houses in causing ill health. She explained this specific concern “I went into a house … my two kids were very ill, they weren’t used to the central heating. You see, with Traveller kids, they’re used, this cold doesn’t affect them like it affect a settled kid because they’re brought up to tha.t But when you put them in a house, my kids had chest infections. They were so ill and the doctor, every night, there was an ambulance called … they were so ill for being indoors, they weren’t used to it” (F14) She went on to explain the difference between central heating in a house compared to that in a trailer “ the central heating in houses and the central heating in a caravan is two different , because you’ve got a lot of air, you’re in and out …. In a house the heat comes from each side, it comes from your neighbour… I never had mine on and it come right up through” Other respondents also point to the benefits of fresh air as being in contrast to living in a house “I’d say living in a trailer’s healthy for you because you get a lot more air … In a house you’re always bunged up with all central heating on… we only lived there [in a house] for about 5 months and I found my face was all paler.” (M4) Other respondents though felt that houses were a healthier option in the winter for their children compared to conditions when travelling. A significant disadvantage and cause of distress for many respondents no longer able to travel is the feeling of isolation. It is this aspect of house dwelling that is implied by this respondent “ if you was in a house and you got very badly depressed and everything well they’d blame it on the house …they’d say if you was out travelling , and this that and the other way and out with your childer , you wouldn’t be like this , it’s because you’re stuck in a house” (F18) Another respondent, living in a house but badly wanting to move to a site to be close to her deceased husband’s family, explains how she could deal with “pressure” when she is with them, but said… it’s bad living in a house love, you can’t see nobody” (F20)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 84
The fear that a move into housing will destroy cultural values has been mentioned. This failure, by Gypsy Travellers who move into houses, to continue living the same cultural lifestyle is seen as a severe loss that can precipitate depression.
This has been partly explained by the perceived damaging effects to the motivation, resourcefulness and ambition of Travellers. Although other respondents refute that house dwelling is a threat and are quick to argue that identity is not dependent on where you live “ we’re the one people”, the perceived erosion of the culture and adoption of damaging lifestyle habits from their closer associations with non-Travellers, is seen as the risk to the young. For those who feel housing is their only option there is still an expressed need to limit these effects by ensuring that the house will not be in a ‘bad housing estate’. “there’s young girls up there at 15 who are selling their bodies on the street”, come on.” (M3) Privately owned family sites Some respondents talked of a small privately owned family site as the ideal living situation if they can no longer travel. The importance of having a secure base for family to come to, if in need, was an important feature of this desired option. One respondent, now on her own pitch on someone’s privately owned site explains why this would prevent her from moving, even though she has identified that being rooted in the one spot is a cause of her present distress. “I think I’d rather have somewhere that I knowed if one of my children was desperate to go somewhere or they couldn’t find anywhere, then they’ve got somewhere like this…because they knows at any time now, if they turned up now for some reason there is room for them and they haven’t got to worry about it. It’s security for them” (F9) It was conceded that there is very little opportunity of such an option for most at present. One housed respondent, who would not move into a site from choice, expressed this wish “ if I had my way , if I had a little site where I could have all my children in trailers, [ most of whom are adults and are scattered ] I would prefer it , but you just can’t get them things so we stay put” (F18) Process of securing appropriate accommodation The difficulty in obtaining suitable accommodation is a cause of insecurity for many Gypsy Travellers. Whenever respondents felt compelled to move onto a site or into housing, sometimes for health or related reasons, the process was often lengthy and required intervention and support from advocates in order to succeed. This respondent describes the stress of trying to move from a poorly serviced transit site to a place on a permanent council site

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 85
“this was killing me love, it’s making me brain go violent inside me , it’s really upsetting me…. I must have been after getting 6 letters from me doctors and handing them and still making no progress … I haven’t got enough points”
(F8) For some respondents this lack of choice, with the difficulties and obstacles involved in living their lifestyle, reflect to them their perceived position in society. Hostility and fear of violence Another consideration in respect of living arrangements arises from enduring racist hostility from neighbours in the absence of surrounding supportive family. Some respondents had moved out of housing and back to travelling to escape hostility or victimisation from housed neighbours. “ we had a house in X , but we couldn’t live in it ….the people on the housing estate , they were hurting the kids and one thing and another. They were big women fighting me 11 year old daughter… and when the kids were going to school and getting bullied ‘ you’re only Gypsies’ and all the names under the sun” (F6) One respondent, in similar circumstances to another respondent who was fearful of a notorious Traveller family, saw a benefit to the isolation of living in a house. He explained his choice “ too much trouble , there’s too much trouble with them . A row might happen a hundred years ago now and it’s there for life … They’re a rough gang and they want to keep you afraid of them … so in other words like 5 or 6 of them will beat the likes of me…that’s why I wouldn’t live on a site, I’d sooner be in a house, I feel safer” (M7) Others felt that travelling was a safer way to avoid such potential violence. Freedom in the form of escape from trouble was cited. This respondent explains the need to travel many miles away to escape from a particular notorious criminal travelling family as he points out the reason that he feels Travellers can’t rely on the police to deal with this type of trouble “ you cannot go to the police , fair enough they may no get you , but the family that’s left , like my brothers and her brothers and sisters and mother and all that, it would get took out on them … it always backfires on the rest of the family , that’s the way it is” (M3) However, the level of violent crime from the settled community in certain neighbourhoods was also expressed as a fear about living in housed accommodation. “ because if you go up the high street and you’ve a child it takes 2 minutes – someone went in yesterday and give a woman a box in the mouth, took her money and ran . You can’t walk up the street with a chain round your neck… cos they snap them” (F20)

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 86
WORK
Another cause of stress and anxiety, and for some, a cause of despair, is the implication for future work opportunities The importance of the man’s role of family provider has been described. This father indicated the pride in the work ethic by his inference in comparison to non- Travellers “ they’ll not be getting married to nobody from a housing estate , they’ll get married to a young travelling boy who can go out and work for his living “ (M3) Women also describe pride in working hard, but for many this work is unpaid work in binging up and caring for the family and home. Some women also spoke of having to have gone out to earn money “all me life apart from the past 5 years I’ve had to work, get up in the rain and cold” (F9) Most respondents did not attribute any ill health to such hard work, but spoke favourably of work, despite the conditions. Those who spoke of occupations described physical work “ I go out and I do tree work, I do rubbish jobs, but I never took a course” and “ that feller over there, he scraps lorries and that”. This type of occupation leaves little scope for diversification without further qualifications if serious ill health prevents further physical work. This father, whose young sons presently go out working with him, expressed his concern at the increased need for qualifications, registration (to obtain recognised identification) and computer skills in order for Travellers to succeed in the job market “I think work like that will be virtually impossible to get in the next 5 years” (M3) Several respondents spoke of less work availability for Travellers, particularly in the type of work that whole families could engage in. The implication for this woman is that these changes are also a threat to Traveller identity “ we used to do a lot of field work, all field working all over the country, taters, strawberries…. But we were more Travellerfied then than what we are now” (F9) The need to travel and also to travel further in order to obtain work was an added potential pressure on families if they were not able to travel as a family “ a lot of the time the men leave the women on there and they go away working . They take a little tourer and they go away working and come back weekends or come back every fortnight, but you’ve got no option” (F9) Although work that involved ‘calling’ was seen as getting harder to obtain there was distaste for working in factories and shops “ like gorjers”. Lack of education and resulting poor literacy was also seen as a barrier to running an effective business.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 87
The concern about revealing identity as a Traveller was a major factor with regard to becoming licensed or in applying for an advertised job. This respondent foresaw no chance of being accepted if he had to give an address on a Gypsy site and
added “ so I would imagine people think you’re a thief or you’re going to do something” (M4) Several respondents expressed concern at their perception of a bleak future in regard to work opportunities. There was little evidence of any belief that Traveller youths might diversify and change from previous patterns of self employed occupations in order to adjust to diminishing work opportunities. One explanation for this merged in the context of the experience of racism “even my little boy with the secondary school and if he had the best exams that anyone could ever have , where would it get him? He wouldn’t be took into a job. The minute they know where he came from, they wouldn’t take him in. They wouldn’t trust him. They wouldn’t allow him to work in an office. They wouldn’t allow him to work in a shopping centre with a till” (F14)
This lack of confidence in applying for a job, based on apparently realistic appraisal of the situation, prevents some Travellers from even considering pursuit of their dreams One widowed mother who would ‘love to work with young Traveller girls’, because she can talk to them, believed that this wasn’t remotely possible. The same respondent wants her children to have an education but has no realistic expectations that it will enable them to get jobs and explains “there’s no hope.” She talks of her daughters’ aspirations to be a beautician and teacher respectively, but says “but they’d never be let get those jobs” [as Travellers]
The cultural need to have family members sharing the roles as carers was an added problem when it reduced that carer’s ability to be available for work. One young mother, who needed frequent support for daily living activities as well as help to maintain the home and care for the children explained her situation “she had to get money to pay to look after me, obvious, because she couldn’t actually get out and work. So now she’s out working, she’s doing no for herself because they’ve stopped giving me the money I needed for her to come in and help me” (F1) Conclusion The far-reaching consequences of environmental factors on the health and psychological well being of Gypsies and Travellers are powerfully expressed by respondents in this study. Poor accommodation and living conditions, and diminished work opportunities were frequently were seen to exacerbate ill health, and in particular to increase the stress and depression associated with a lack of choice and control and poor access to services. Crucially, in addition to the health and social effects of poor living conditions, participants described an associated difficulty in maintaining a chosen cultural lifestyle. The perceived consequence of this was an erosion of their culture. Moreover, this was seen as a deliberate strategy and a sign of

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 88
the majority society’s desire for a policy of assimilation. This added factor contributes to the feelings of injustice and persecution and further jeopardises the climate for mutual trust with health staff from the majority society.

The Health Status of Gypsies and Travellers in England Report of Qualitative findings
Health of Gypsies and Travellers in England: Qualitative Report. Oct 2004 page 89
Reference List
1. Van Cleemput P,.Parry G. Health status of Gypsy Travellers. Journal of Public
Health Medicine. 2001;23:129-34.
2. Botes S, Cowley S, and Hudson R. A submission to Sir Donald Acheson's independent enquiry into inequalities in health. 1997. London, CPHVA .
Ref Type: Report
3. Bryman A. Quantity and Quality in Social Research. London: Unwin Hyman, 1998.
4. Crabtree B.F MWLe. Doing Qualitative Research. Thousand Oaks, CA: Sage, 1999.
5. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. In Bryman A, Burgess R.G., eds. Analyzing Qualitative Data , London: Routledge, 1994.
6. Radley A,.Billig M. Accounts of health and Illness:Dilemmas and representations. Sociology of Health and Illness 1996;18:220-40.
7. Blaxter M. Whose Fault is it? People's own conceptions of the reasons for health inequalities. Social Science & Medicine 1997;44:747-56.
8. Spencer S. A Better Road: An information booklet for health care and other professionals. 2003. Derbyshire Gypsy Liason Group.

















