6 tion of staff at the beginning of training may provide the best means of protection against transmission of hepa- titis B infection between patients and staff in either direction. Vaccines have been developed and are being assessed for safety and efficacy.19 Meanwhile, anti-HBs immunoglobulin is available for prophylaxis after acci- dental inoculation or contamination of abrasions and mucous membranes with HBsAg positive material. We are greatly indebted to the family doctors for their generous re- sponse to the request for assistance; by completing and returning the study records they ensured an almost complete follow-up of the pa- tients who remained in their care. We thank the staff of the records department and the theatre and obstetric staff at hospitals A and B, clerical and secretarial staff of the area health authority, and the Epi- demiological Research Laboratory for the large contributions they made to the study. All the collaborators have chosen to remain anonymous to facilitate the reorganisation of their colleague’s professional life. The epidemiological studies were made by the following: the hospi- tal control of infection officer and nursing officer; the district medical officer for environmental health and a senior registrar in community medicine, area health authority; a statistician, PHLS Communicable Disease Surveillance Centre; a senior registrar, Virus Reference Laboratory and a consultant epidemiologist, Epidemiological Research Laboratory, Central Public Health Laboratory. The virological studies were done at the Department of Virology, Middlesex Hospital. Some specimens were also examined at the Virus Reference Laboratory, Central Public Health Laboratory. Requests for reprints should be addressed to the Epidemiological Research Laboratory (Hepatitis), Central Public Health Laboratory, Colindale Avenue, London NW9 5HT. REFERENCES 1. Public Health Laboratory Service. Communicable disease weekly reports, 1973-79. Unpublished. 2. World Health Organisation. Viral hepatitis. World Health Org Tech Rep Ser no. 570, 1975. 3. World Health Organisation. Advances in viral hepatitis. World Health Org Tech Rep Ser no. 602, 1977. 4. Rimland D, Parkin WE, Miller GB, Schrack WD. Hepatitis B outbreak traced to an oral surgeon. N Engl J Med 1977; 296: 953-58. 5. Heathcote J, Cameron CH, Dane DS. Hepatitis B antigen in saliva and semen. Lancet 1974; i: 71-73. 6. Barbara JAJ, Mijovic V, Cleghorn TE, Tedder RS, Briggs M. Liver enzyme concentrations as measure of possible infectivity in chronic asymptomatic carriers of hepatitis B. Br Med J 1978; ii: 1600-02. 7. Tedder RS. Testing for e antigen and e antibody by immunodiffusion. J Med Virol 1978; 3: 51-57. 8. Department of Health and Social Security. Annual Report of the Chief Med- ical Officer. London: H.M. Stationery Office, 1974. 9. Stewart JS, Farrow LJ, Clifford RE, et al. A three-year survey of viral hepa- titis in West London. Quart J Med 1978; 47: 365-84. 10. Garibaldi RA, Rasmussen CM, Holmes AW, Gregg MB. Hospital-acquired serum hepatitis. JAMA 1972; 219: 1577-80. 11. Levin ML, Maddrey WC, Wands JR, Mendeloff AI. Hepatitis B transmission by dentists. JAMA 1974; 228: 1139-40. 12. Snydman Dr, Hindman SH, Wineland MD, Bryan JA, Maynard JE. Nosoco- mial viral hepatitis B: a cluster among staff with subsequent transmission to patients. Ann Intern Med 1976; 85: 573-77. 13. Grob PJ, Moeschlin P. Risk to contacts of a medical practitioner carrying HBsAg. N Engl J Med 1975; 293: 197. 14. Sampliner RE. The duration of hepatitis B surface antigenemia. Arch Intern Med 1978; 138: 145-46. 15. Alter HJ, Chalmers TC, Freeman BM, et al. Health-care workers positive for hepatitis B surface antigen. N Engl J Med 1975; 292: 454-57. 16. Glenwright HD, Edmondson HD, Whitehead FIH, Flewett TH. Serum hepatitis in dental surgeons. Br Dent J 1974; 136: 409-13. 17. Medical Manpower Division, Department of Health and Social Security. Medical staffing and prospects in the NHS in England and Wales 1977. Health Trends 1978; 10: 61-64. 18. Health and Personal Social Services Statistics for England 1977. H.M. Sta- tionery Office, 1977. 19. Gunby P. Clinical trial of vaccine for type B hepatitis to begin next month. JAMA 1979; 241: 979-80. THE INCIDENCE OF HEPATITIS B INFECTION AFTER ACCIDENTAL EXPOSURE AND ANTI-HBs IMMUNOGLOBULIN PROPHYLAXIS A COMBINED MEDICAL RESEARCH COUNCIL* AND PUBLIC HEALTH LABORATORY SERVICE† REPORT Summary In a two-year period 322 persons who reported accidental exposure to material containing hepatitis B surface antigen (HBsAg) and who were HBsAg negative, were given 500 mg anti-hepati- tis-B immunoglobulin (anti-HB Ig) within 14 days of the accident. Afterwards serum samples were taken each month for six months, with others after nine months and a year. Of the 240 who completed the follow-up 21 (9%) had pre-existing anti-HBs detectable by radioimmunoas- say. Acute hepatitis B developed in 7 individuals (3%) and 4 (2%) acquired anti-HBs without symptoms. Introduction IMMUNOGLOBULIN (anti-HB Ig) with high titres of anti- body (anti-HB,) to hepatitis B surface antigen (HBsAg) became available in England and Wales in 1973. Its use among a small number (unpublished observations, Y. E. Cossart) and experience with a similar preparation in France’ suggested that it was protective. A follow-up study was made from September, 1973, to September, 1976, of persons given anti-HB Ig within two weeks of accidental exposure to HBsAg positive material. It was not considered justifiable to include a control group. Materials Plasma was separated from blood donations collected by the National Blood Transfusion Service. Donations found HBsAg negative by counterimmunoelectrophoresis (CIE) and having an anti-HBs titre of at least 2 were used by the Blood Products Laboratory to prepare anti-HB Ig. The preparation has been described.2 The solution was issued in vials of 5 ml containing 10 g percent total protein. The anti-HB titres of the five batches were similar (table I). Methods The following accidents were included: inoculation, con- tamination of the conjunctiva or of skin cuts or abrasions, in- gestion of (or massive contamination of apparently unbroken skin with) HBAg-positive blood, laboratory reagents, or body fluids from HBsAg positive patients. 5 patients given HBsAg positive transfusions or renal transplants were included. After an accident was reported the inoculum was tested for HBsAg, and serum from the inoculated or contaminated per- * MRC Hepatitis Working Party: Dr C. J. BURRELL, Dr Y. E. COS- SART, Mr I. D. HILL (secretary), Prof. D. N. S. KERR (chairman), Sir WILLIAM MAYCOCK, Dr C. S. OGG, Dr S. POLAKOFF, Dr M. SMITH, Dr R. S. WILLIAMS. t PHLS Hepatitis Committee: Dr C. M. P. BRADSTREET, Dr S. K. R. CLARKE, Dr Y. E. COSSART (chairman), Dr J. CpASKE, Dr A. D. EVANS, Dr T. H. FLEWETT, Dr J. V. T. GOSTLING, Dr J. H. HALE, Dr M. H. HAMBLING, Dr R. J. C. HART, Dr D. M. JoNES, Dr J. B. KURTZ Dr F. 0. MACCALLUM, Dr J. NAGINGTON, Dr S. POLAKOFF (secretary), Dr G. C. TURNER, Dr M. A. WILSON. The study was co-ordinated and the report was prepared by Dr Sheila Polakoff, Epidemiological Research Laboratory, Central Public Health Laboratory, London NW9 5HT.
Transcript
6
tion of staff at the beginning of training may provide thebest means of protection against transmission of hepa-titis B infection between patients and staff in eitherdirection. Vaccines have been developed and are beingassessed for safety and efficacy.19 Meanwhile, anti-HBsimmunoglobulin is available for prophylaxis after acci-dental inoculation or contamination of abrasions andmucous membranes with HBsAg positive material.
We are greatly indebted to the family doctors for their generous re-sponse to the request for assistance; by completing and returning thestudy records they ensured an almost complete follow-up of the pa-tients who remained in their care. We thank the staff of the recordsdepartment and the theatre and obstetric staff at hospitals A and B,clerical and secretarial staff of the area health authority, and the Epi-demiological Research Laboratory for the large contributions theymade to the study.
All the collaborators have chosen to remain anonymous to facilitatethe reorganisation of their colleague’s professional life.
The epidemiological studies were made by the following: the hospi-tal control of infection officer and nursing officer; the district medicalofficer for environmental health and a senior registrar in communitymedicine, area health authority; a statistician, PHLS CommunicableDisease Surveillance Centre; a senior registrar, Virus ReferenceLaboratory and a consultant epidemiologist, Epidemiological ResearchLaboratory, Central Public Health Laboratory. The virological studieswere done at the Department of Virology, Middlesex Hospital. Somespecimens were also examined at the Virus Reference Laboratory,Central Public Health Laboratory.
Requests for reprints should be addressed to the EpidemiologicalResearch Laboratory (Hepatitis), Central Public Health Laboratory,Colindale Avenue, London NW9 5HT.
REFERENCES
1. Public Health Laboratory Service. Communicable disease weekly reports,1973-79. Unpublished.
2. World Health Organisation. Viral hepatitis. World Health Org Tech Rep Serno. 570, 1975.
3. World Health Organisation. Advances in viral hepatitis. World Health OrgTech Rep Ser no. 602, 1977.
4. Rimland D, Parkin WE, Miller GB, Schrack WD. Hepatitis B outbreaktraced to an oral surgeon. N Engl J Med 1977; 296: 953-58.
5. Heathcote J, Cameron CH, Dane DS. Hepatitis B antigen in saliva andsemen. Lancet 1974; i: 71-73.
6. Barbara JAJ, Mijovic V, Cleghorn TE, Tedder RS, Briggs M. Liver enzymeconcentrations as measure of possible infectivity in chronic asymptomaticcarriers of hepatitis B. Br Med J 1978; ii: 1600-02.
7. Tedder RS. Testing for e antigen and e antibody by immunodiffusion. J MedVirol 1978; 3: 51-57.
8. Department of Health and Social Security. Annual Report of the Chief Med-ical Officer. London: H.M. Stationery Office, 1974.
9. Stewart JS, Farrow LJ, Clifford RE, et al. A three-year survey of viral hepa-titis in West London. Quart J Med 1978; 47: 365-84.
17. Medical Manpower Division, Department of Health and Social Security.Medical staffing and prospects in the NHS in England and Wales 1977.Health Trends 1978; 10: 61-64.
18. Health and Personal Social Services Statistics for England 1977. H.M. Sta-tionery Office, 1977.
19. Gunby P. Clinical trial of vaccine for type B hepatitis to begin next month.JAMA 1979; 241: 979-80.
THE INCIDENCE OF HEPATITIS B INFECTIONAFTER ACCIDENTAL EXPOSURE AND
ANTI-HBs IMMUNOGLOBULIN PROPHYLAXIS
A COMBINED MEDICAL RESEARCH COUNCIL* AND PUBLICHEALTH LABORATORY SERVICE† REPORT
Summary In a two-year period 322 persons whoreported accidental exposure to material
containing hepatitis B surface antigen (HBsAg) and whowere HBsAg negative, were given 500 mg anti-hepati-tis-B immunoglobulin (anti-HB Ig) within 14 days of theaccident. Afterwards serum samples were taken eachmonth for six months, with others after nine months anda year. Of the 240 who completed the follow-up 21 (9%)had pre-existing anti-HBs detectable by radioimmunoas-say. Acute hepatitis B developed in 7 individuals (3%)and 4 (2%) acquired anti-HBs without symptoms.
Introduction
IMMUNOGLOBULIN (anti-HB Ig) with high titres of anti-body (anti-HB,) to hepatitis B surface antigen (HBsAg)became available in England and Wales in 1973. Its useamong a small number (unpublished observations, Y. E.Cossart) and experience with a similar preparation inFrance’ suggested that it was protective.A follow-up study was made from September, 1973,
to September, 1976, of persons given anti-HB Ig withintwo weeks of accidental exposure to HBsAg positivematerial. It was not considered justifiable to include acontrol group.
Materials
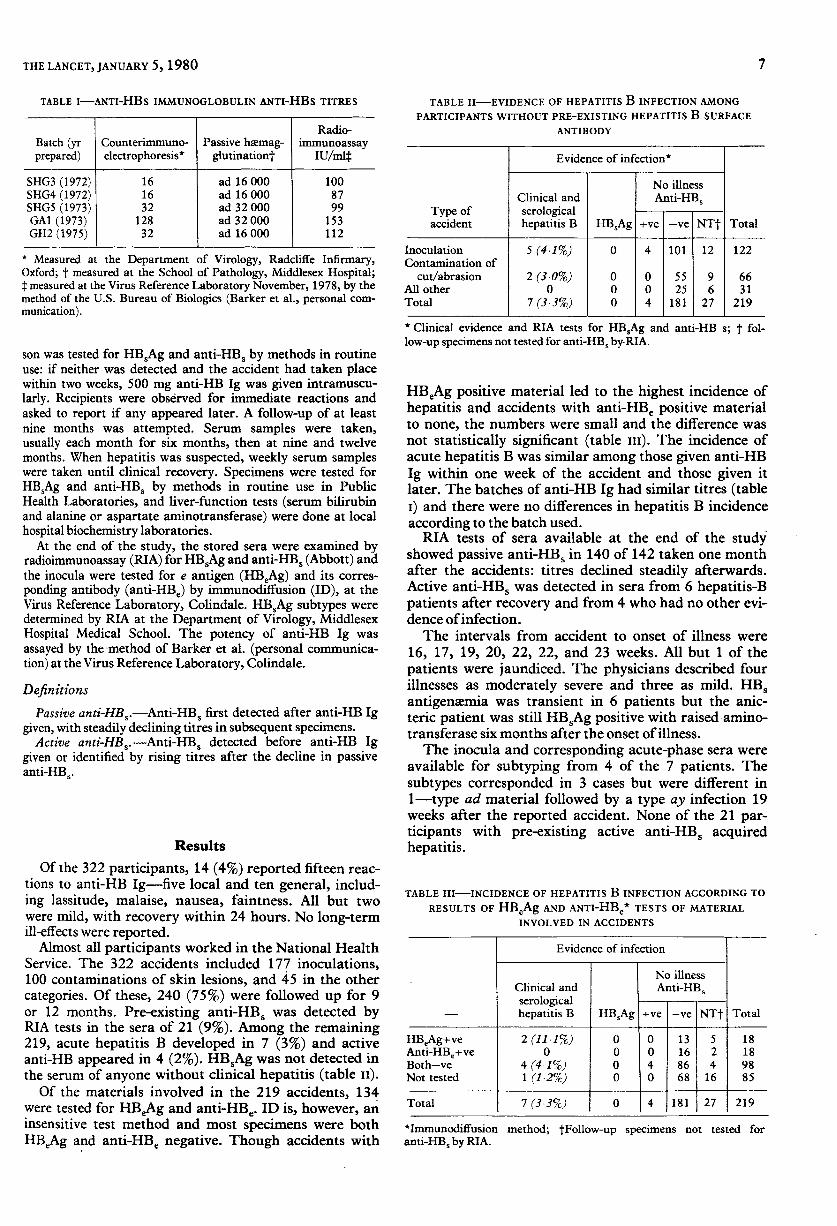
Plasma was separated from blood donations collected by theNational Blood Transfusion Service. Donations found HBsAgnegative by counterimmunoelectrophoresis (CIE) and havingan anti-HBs titre of at least 2 were used by the Blood ProductsLaboratory to prepare anti-HB Ig. The preparation has beendescribed.2 The solution was issued in vials of 5 ml containing10 g percent total protein.The anti-HB titres of the five batches were similar (table I).
Methods
The following accidents were included: inoculation, con-tamination of the conjunctiva or of skin cuts or abrasions, in-gestion of (or massive contamination of apparently unbrokenskin with) HBAg-positive blood, laboratory reagents, or bodyfluids from HBsAg positive patients. 5 patients given HBsAgpositive transfusions or renal transplants were included.
After an accident was reported the inoculum was tested forHBsAg, and serum from the inoculated or contaminated per-
* MRC Hepatitis Working Party: Dr C. J. BURRELL, Dr Y. E. COS-SART, Mr I. D. HILL (secretary), Prof. D. N. S. KERR (chairman), SirWILLIAM MAYCOCK, Dr C. S. OGG, Dr S. POLAKOFF, Dr M. SMITH, DrR. S. WILLIAMS.
t PHLS Hepatitis Committee: Dr C. M. P. BRADSTREET, Dr S. K. R.CLARKE, Dr Y. E. COSSART (chairman), Dr J. CpASKE, Dr A. D.EVANS, Dr T. H. FLEWETT, Dr J. V. T. GOSTLING, Dr J. H. HALE, DrM. H. HAMBLING, Dr R. J. C. HART, Dr D. M. JoNES, Dr J. B. KURTZDr F. 0. MACCALLUM, Dr J. NAGINGTON, Dr S. POLAKOFF (secretary),Dr G. C. TURNER, Dr M. A. WILSON.
The study was co-ordinated and the report was prepared by DrSheila Polakoff, Epidemiological Research Laboratory, Central PublicHealth Laboratory, London NW9 5HT.
* Measured at the Department of Virology, Radcliffe Infirmary,Oxford; t measured at the School of Pathology, Middlesex Hospital;t measured at the Virus Reference Laboratory November, 1978, by themethod of the U.S. Bureau of Biologics (Barker et al., personal com-munication).
son was tested for HBsAg and anti-HBs by methods in routineuse: if neither was detected and the accident had taken placewithin two weeks, 500 mg anti-HB Ig was given intramuscu-larly. Recipients were observed for immediate reactions andasked to report if any appeared later. A follow-up of at leastnine months was attempted. Serum samples were taken,usually each month for six months, then at nine and twelvemonths. When hepatitis was suspected, weekly serum sampleswere taken until clinical recovery. Specimens were tested forHBsAg and anti-HBs by methods in routine use in PublicHealth Laboratories, and liver-function tests (serum bilirubinand alanine or aspartate aminotransferase) were done at localhospital biochemistry laboratories.
At the end of the study, the stored sera were examined byradioimmunoassay (RIA) for HBsAg and anti-HBs (Abbott) andthe inocula were tested for e antigen (HBeAg) and its corres-ponding antibody (anti-HBe) by immunodiffusion (ID), at theVirus Reference Laboratory, Colindale. HBsAg subtypes weredetermined by RIA at the Department of Virology, MiddlesexHospital Medical School. The potency of anti-HB Ig wasassayed by the method of Barker et al. (personal communica-tion) at the Virus Reference Laboratory, Colindale.
DefinitionsPassive anti-HBs.—Anti-HBs first detected after anti-HB Ig
given, with steadily declining titres in subsequent specimens.Active anti-HBs.—Anti-HBs detected before anti-HB Ig
given or identified by rising titres after the decline in passiveanti-HBs’
Results
Of the 322 participants, 14 (4%) reported fifteen reac-tions to anti-HB Ig-five local and ten general, includ-ing lassitude, malaise, nausea, faintness. All but twowere mild, with recovery within 24 hours. No long-termill-effects were reported.
Almost all participants worked in the National HealthService. The 322 accidents included 177 inoculations,100 contaminations of skin lesions, and 45 in the othercategories. Of these, 240 (75%) were followed up for 9or 12 months. Pre-existing anti-HBS was detected byRIA tests in the sera of 21 (9%). Among the remaining219, acute hepatitis B developed in 7 (3%) and activeanti-HB appeared in 4 (2%). HBsAg was not detected inthe serum of anyone without clinical hepatitis (table n).Of the materials involved in the 219 accidents, 134
were tested for HBeAg and anti-HBe. ID is, however, aninsensitive test method and most specimens were bothHBeAg and anti-HBe negative. Though accidents with
TABLE II-EVIDENCE OF HEPATITIS B INFECTION AMONGPARTICIPANTS WITHOUT PRE-EXISTING HEPATITIS B SURFACE
ANTIBODY
* Clinical evidence and RIA tests for HB.Ag and anti-HB s; t fol-low-up specimens not tested for anti-HB. by-RIA.
HBeAg positive material led to the highest incidence ofhepatitis and accidents with anti-HBe positive materialto none, the numbers were small and the difference wasnot statistically significant (table in). The incidence ofacute hepatitis B was similar among those given anti-HBIg within one week of the accident and those given itlater. The batches of anti-HB Ig had similar titres (tablei) and there were no differences in hepatitis B incidenceaccording to the batch used.RIA tests of sera available at the end of the study
showed passive anti-HBs in 140 of 142 taken one monthafter the accidents: titres declined steadily afterwards.Active anti-HBs was detected in sera from 6 hepatitis-Bpatients after recovery and from 4 who had no other evi-dence of infection.The intervals from accident to onset of illness were
16, 17, 19, 20, 22, 22, and 23 weeks. All but 1 of thepatients were jaundiced. The physicians described fourillnesses as moderately severe and three as mild. HBsantigenæmia was transient in 6 patients but the anic-teric patient was still HBsAg positive with raised amino-transferase six months after the onset of illness.The inocula and corresponding acute-phase sera were
available for subtyping from 4 of the 7 patients. Thesubtypes corresponded in 3 cases but were different in1-type ad material followed by a type ay infection 19weeks after the reported accident. None of the 21 par-ticipants with pre-existing active anti-HBs acquiredhepatitis.
TABLE III—INCIDENCE OF HEPATITIS B INFECTION ACCORDING TO
RESULTS OF HBeAg AND ANTI-HBe* TESTS OF MATERIALINVOLVED IN ACCIDENTS
*Immunodiffusion method; tFollow-up specimens not tested for
anti-HB, by RIA.
8
Non-accidental cases
3 patients who had received HBsAg positive trans-fusions were given 500 mg anti-HB Ig and were followedup. The transfused HBsAg was detected by RIA insera taken between 3 and 11 days after transfusion.Active anti-HBs was detected in the sera of 2 of the 3within five months. 2 patients who had received renaltransplants from the same donor were given 1 g anti-HBIg within 3 days. HBSAg from the transplant wasdetected by RIA in 1 patient’s serum shortly after theoperation. Later this disappeared and anti-HBs wasdetected; a further 1 g anti-HB Ig was given after amonth and the level of anti-HBs increased, then declinedagain until raised levels at six and nine months indicatedactive anti-HB, production. The other patient did notreceive a second dose of anti-HB Ig because of a criticaltransplant rejection episode. Levels of passive anti-HBsdeclined swiftly in her serum and HBsAg appeared at sixmonths and persisted. Neither patient had clinical hepa-titis.
Discussion
The protective efficacy of anti-HB Ig cannot beassessed without an untreated or placebo control group.Nevertheless, the results of this study are of interest,particularly to health-service staff who are exposed to in-fection in the course of their work. It is reassuring thatmost of the 240 participants had no ill-effects from theiraccidents and that, of the 7 who had acute hepatitis B,6 recovered completely and only 1 still had HBsAg withhepatic dysfunction six months after the onset of illness.Moreover, the use of anti-HB Ig did not lead to persist-ent HBS antigenaemia without symptoms. The hepatitiscaused by a virus of a different subtype from that of theinoculum in the reported accident can be explained onlyin terms of another unrecognised exposure.The incidence of clinical hepatitis was probably less
than the estimated 3% among those with a complete fol-low-up. Almost certainly the others, who had either goneabroad or were reluctant to provide serial blood samples,would have reported an attack of clinical hepatitis.Two variables, other than prophylaxis with anti-HB
Ig, which would affect the hepatitis B attack-rate afteraccidental exposure are the nature of the accident andthe infectivity of the inoculum. All the accidents werereal in the sense that they happened, that the inoculawere HBsAg positive, and that the subjects believed thatthey had been exposed; but some subjects may in facthave escaped the contact. Tests for HBeAg and anti-HBeare good, though not absolute, markers of infectivity,3and though the method used in the study was not sensi-tive enough to categorise most of the inocula, the inclu-sion of accidents with minute inocula of low infectivityprobably lowered the incidence of hepatitis irrespectiveof the effect of anti-HB Ig.An early experimental study made in the U.S.A. with
a control group suggested that anti-HB Ig protectedwhen given on the same day as inoculation of infectivematerial.4 Studies of anti-HB Ig prophylaxis after acci-dental inoculation have not included randomly selecteduntreated control groups. In two randomised trials inthe U.S.A., however, subjects were given either normalIg or extremely high titre anti-HB Ig: in one, anti-HBIg seemed to protect;5 in the other, the incubation period
was prolonged but the infection was neither preventednor modified. 6, The following explanations of the lackof protection were suggested: infection was due to re-exposure when serum levels of anti-HB Ig had waned;the potency ofthe anti-HB Ig had been reduced by frag-mentation of molecules in preparation; delay in adminis-tration of prophylaxis had reduced the protective effect.
In the present study the anti-HB titre, measured bypassive haemagglutination, of the immunoglobulin waslower than those of the U.S.A. trial preparations. Asthere was no International Standard when the Americanwork was done the actual difference is not known. Apartfrom the anti-HB Ig titres, differences in the amount andtime of dosage and in the possibility of re-exposure dur-ing the follow-up period make direct comparisonsbetween this and the U.S.A. studies impossible. Never-theless, these results, in which no incubation period waslonger than 23 weeks and only 4 participants acquiredactive anti-HBs without symptoms, resemble more close-ly the findings of the study in which anti-HB Ig pro-tected5 than that in which it failed. 6, 7
Chance provided a comparison of the effects of dif-ferent doses given to 2 susceptible recipients of infectedkidney transplants from the same donor. Individual dif-ferences may have affected the outcome; nevertheless,development of active anti-HBs by the recipient of thelarger divided dose and the persistent HBs antigensemiain the recipient of the smaller single dose suggest thatthe larger dose protected. We do not know what the inci-dence of hepatitis B would have been if anti-HB Ig hadnot been given after the accidents, or whether largerdoses of anti-HB Ig would have prevented any of the 7cases, but the results suggest that the material is protec-tive.
We are indebted to the physicians who reported the accidents andsupplied virological specimens, results of biochemical tests, and clinicalinformation. We thank the directors of regional transfusion centres ofthe National Blood Transfusion Service for providing plasma, DrD. S. Dane and Dr A. Lawn for examining the immunoglobulin solu-tions used, and Dr T. E. Cleghorn and Dr Dane who collected andselected the plasma used to prepare the immunoglobulin. We are par-ticularly indebted to Dr Dane for determining subtypes by RIA tests.We thank Mrs C Rawlinson and other members of the staff of the Epi-demiological Research Laboratory and Mrs P. R. Schweitzer of theVirus Reference Laboratory for their assistance.
Requests for reprints should be addressed to Dr Sheila Polakoff,Epidemiological Research Laboratory, Central Public Health Labora-tory, London NW9 SHT.
REFERENCES
1. Soulier JP, Blatix C, Courouce MA, et al. Prevention of virus B hepatitis(SH hepatitis). Am J Dis Child 1972; 123: 429-34.
2. Polakoff S, Maycock W d’A. Anti-HBAg immunoglobulin after inoculationinjuries International Symposium on Viral Hepatitis, Milan, December,1974. (Develop Biol Standard 1975; vol 30.) Basel: S. Karger, 1975:329-34.
3. Grady GF, Gitnick GI, Prince AM, et al. Relation of e antigen to infectivityof HBsAg-positive inoculations among medical personnel. Lancet 1976; ii.492-94.
4. Krugman S, Giles JP, Hammond J. Viral hepatitis, type B (MS-2 strain).Prevention with specific hepatitis B immune globulin. JAMA 1971; 218:1665-70.
5. Seeff LB, Wright EC, Zimmerman HJ, et al. Type B hepatitis after needle-stick exposure: prevention with hepatitis B immune globulin. Ann InternMed 1978; 88: 285-93.
6. Grady GF, Lee VA. Hepatitis B immune globulin-prevention of hepatitisfrom accidental exposure among medical personnel. A preliminary reportN Engl J Med 1975; 293: 1067-70.
7. Grady GF, Lee VA, Prince AM, et al. Hepatitis B immune globulin for acci-dental exposures among medical personnel: final report of a multicentercontrolled trial. J Infect Dis 1978; 138: 625-37.