155
The Incidental Adrenal Mass Jay T Bishoff, MD, FACS Director, Intermountain Urological Institute Clinical Professor Surgery University of Utah School of Medicine Salt Lake City, Utah
| Date post: | 13-Jan-2017 |
| Category: |
Health & Medicine |
| Upload: | priyatham-kasaraneni |
| View: | 8 times |
| Download: | 0 times |
The Incidental Adrenal Mass
Jay T Bishoff, MD, FACS Director, Intermountain Urological Institute
Clinical Professor Surgery University of Utah School of Medicine
Salt Lake City, Utah

Adrenal Gland
Focus --Test Questions • Anatomy
• Physiology
• Disease Processes
For each disease: Pathophysiology
Diagnosis
Management
• Surgical Treatment

Adrenal Gland
Focus --Test Questions • Anatomy
• Physiology
• Disease Processes
For each disease: Pathophysiology
Diagnosis
Management
• Surgical Treatment
Adrenal Gland
Outline Continued Diseases
• Incidental Adrenal Mass
• Pheochromocytoma
• Primary Hyperaldosteronism
• Cushing’s Syndrome
• Adrenal Insufficiency
• Carcinoma
Adrenal cortical carcinoma
Metastatic cancer
Adrenal Anatomy
Size Length 3 - 5 cm
Width 2.5 - 3 cm
Depth 0.4 - 0.6 cm
Weight 3 - 5 gm
Fetal Adrenal Cortex Involutes after birth,
Ratio of Adrenal to Kidney Weight is:
• Neonate 1:3
• Adult 1:30
Adrenal Anatomy
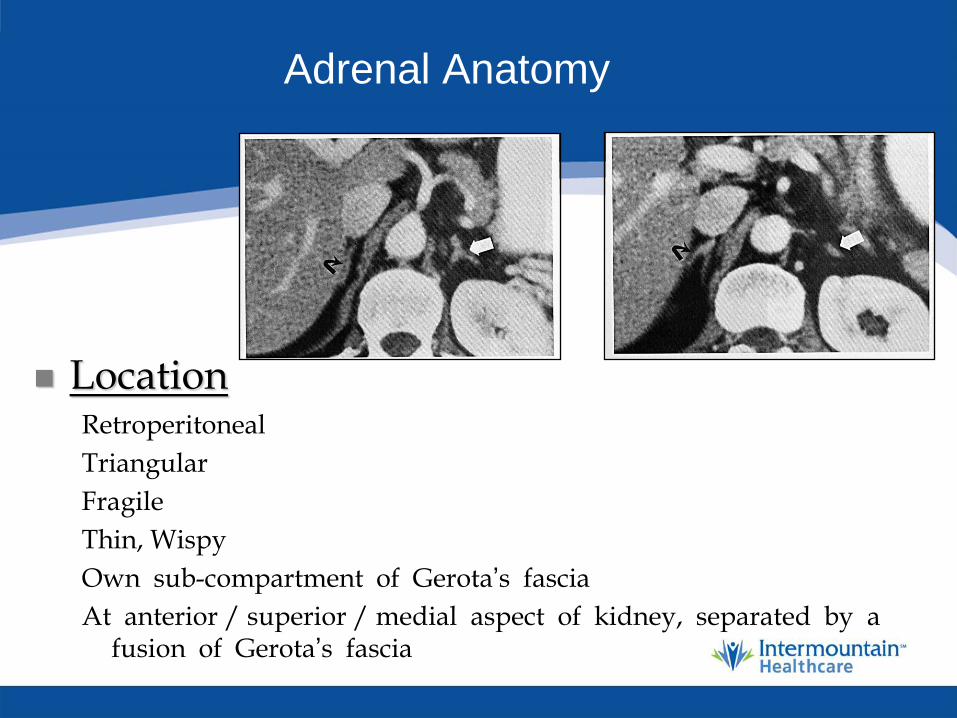
Location Retroperitoneal
Triangular
Fragile
Thin, Wispy
Own sub-compartment of Gerota’s fascia
At anterior / superior / medial aspect of kidney, separated by a fusion of Gerota’s fascia
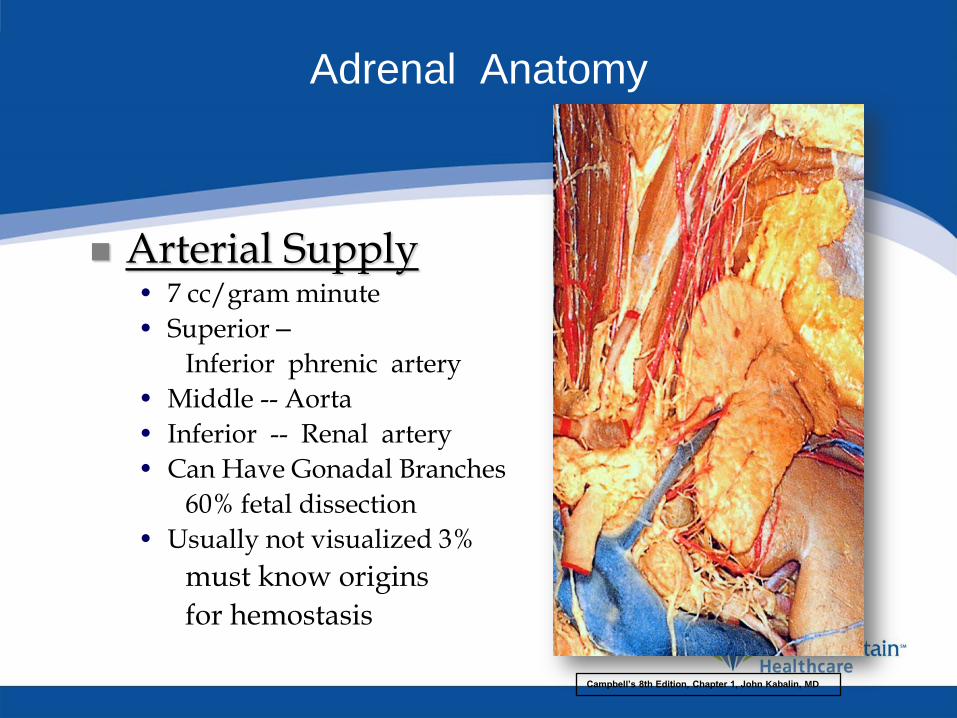
Adrenal Anatomy
Arterial Supply • 7 cc/gram minute
• Superior –
Inferior phrenic artery
• Middle -- Aorta
• Inferior -- Renal artery
• Can Have Gonadal Branches
60% fetal dissection
• Usually not visualized 3%
must know origins
for hemostasis
Campbell’s 8th Edition, Chapter 1, John Kabalin, MD
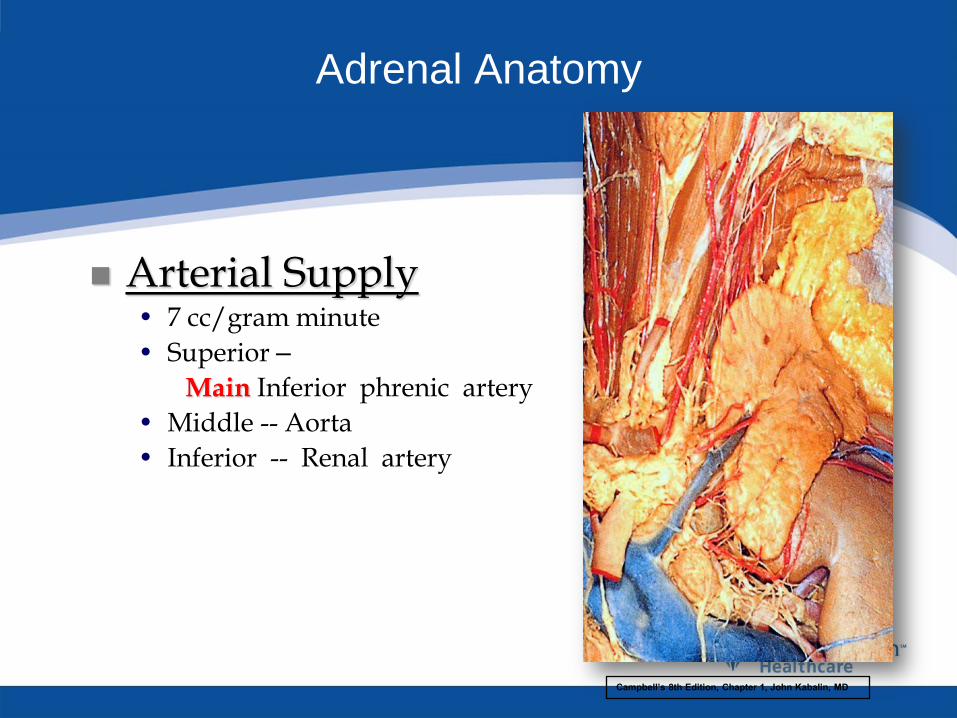
Adrenal Anatomy
Arterial Supply • 7 cc/gram minute
• Superior –
Main Inferior phrenic artery
• Middle -- Aorta
• Inferior -- Renal artery
Campbell’s 8th Edition, Chapter 1, John Kabalin, MD

Campbell’s 8th Edition, Chapter 1, John Kabalin, MD
Adrenal Anatomy
Venous Drainage • Single Main Adrenal Vein
Most important surgical structure
• Right from IVC Gland is often under IVC
Always short
• Left from Renal Vein Variable length
• Left Significant Phrenic Branch
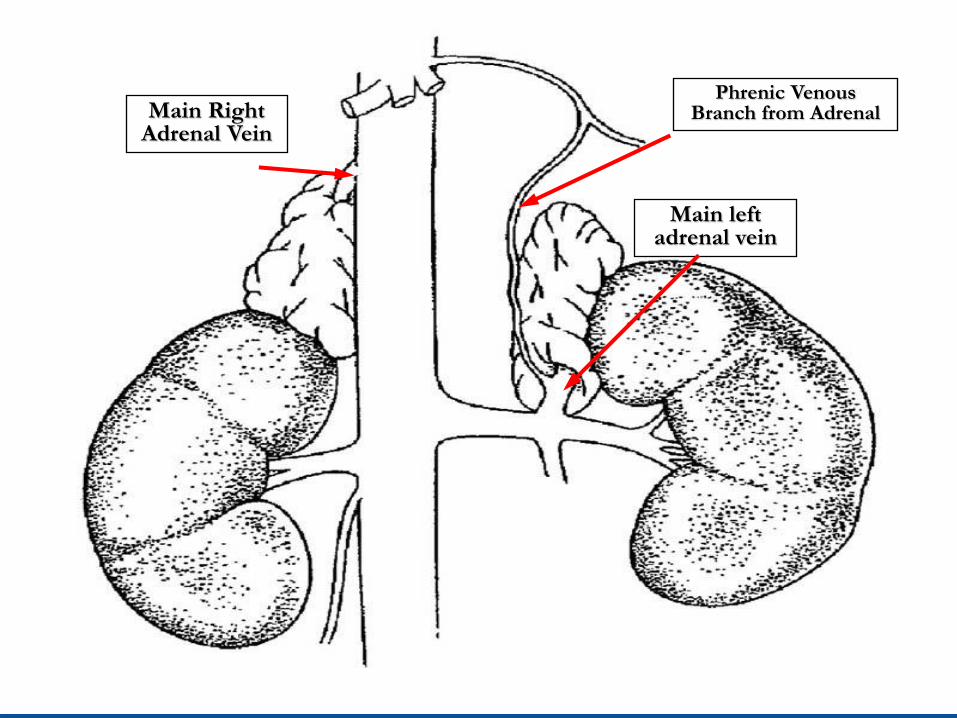
Main Right Adrenal Vein
Main left adrenal vein
Phrenic Venous Branch from Adrenal
Adrenal Anatomy
Nerve Supply • Medulla - Sympathetic Branches
T/10 – L/1
Release of Medullary Hormones:
Epinephrine
Norepinephrine
• Cortex - No Known innervation
Adrenal Anatomy
Lymphatic Drainage • Lateral Aortic Nodes
Renal artery to diaphragm
• Adrenal Carcinoma
Extensive Dissection required for lymphadenectomy
Adrenal Physiology
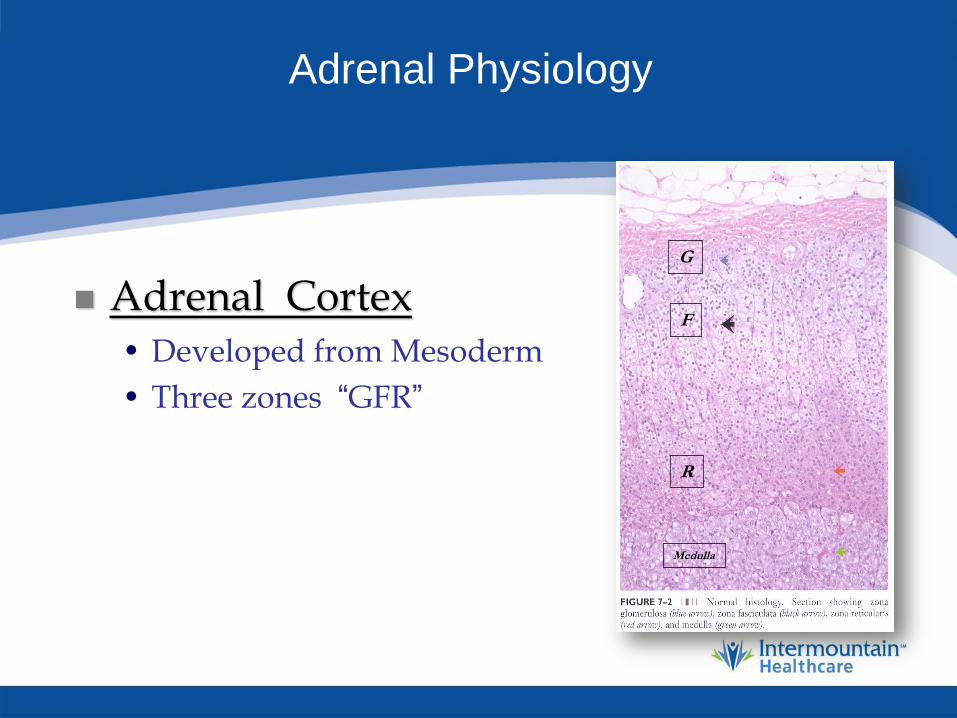
Adrenal Cortex • Developed from Mesoderm
• Three zones “GFR”
G
F
R
Medulla
Adrenal Physiology
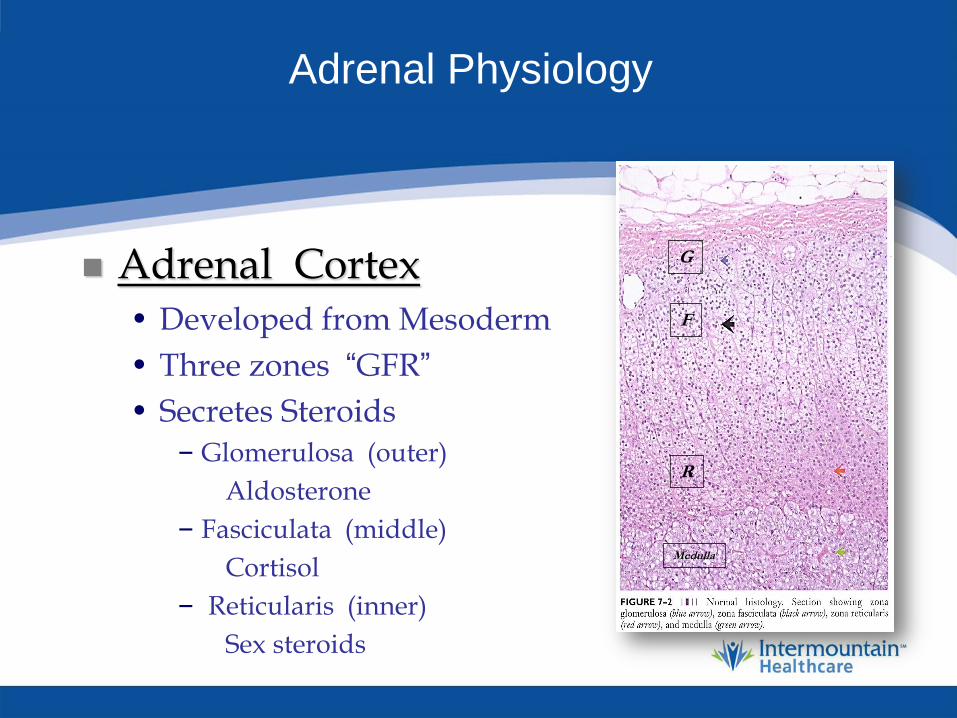
Adrenal Cortex • Developed from Mesoderm
• Three zones “GFR”
• Secretes Steroids – Glomerulosa (outer)
Aldosterone
– Fasciculata (middle)
Cortisol
– Reticularis (inner)
Sex steroids
G
F
R
Medulla

Adrenal Cortex
Hormone Production
Adrenal Physiology
Adrenal Cortex - Aldosterone • Activates Na-K Pump in Nephron:
Retention of Na (water follows Na)
Kidney – Intestine – Salivary gland
Depletion of potassium
• Stimulants of Aldosterone Secretion: Primary Angiotensin II
Secondary – ACTH
Decreased Serum Na
Elevated Serum K
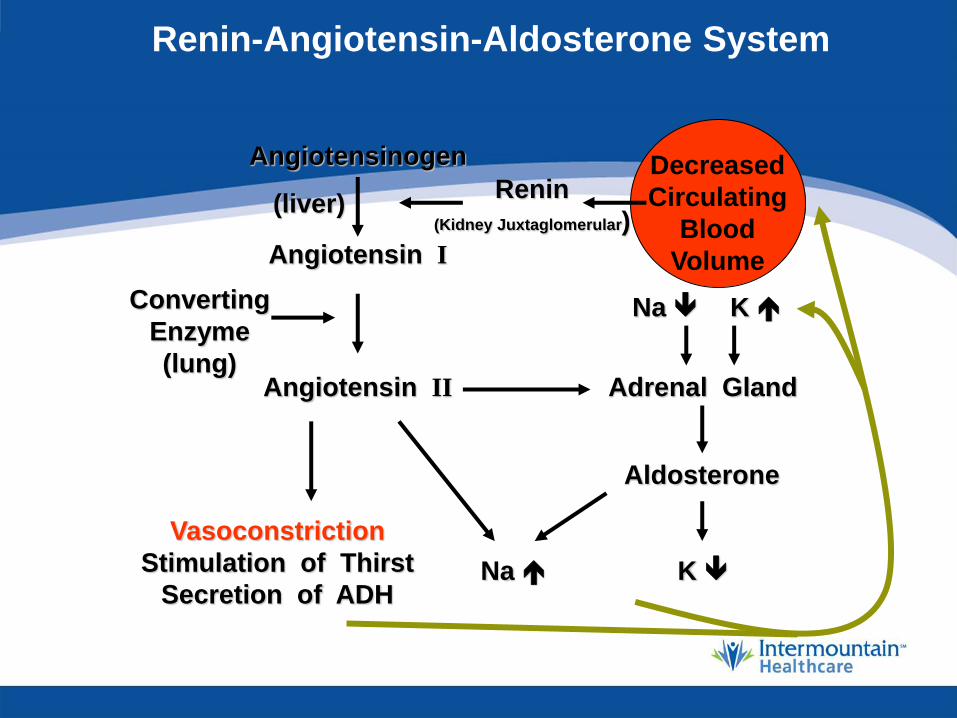
Renin-Angiotensin-Aldosterone System
Angiotensinogen
Angiotensin I
Angiotensin II
Renin
(Kidney Juxtaglomerular)
Converting
Enzyme
(lung)
Vasoconstriction
Stimulation of Thirst
Secretion of ADH
Adrenal Gland
Aldosterone
Na K
Na K
Decreased
Circulating
Blood
Volume
(liver)
Adrenal Physiology
Adrenal Cortex - Glucocorticoids • Multitude of Metabolic Functions:
Salt retention
Skeletal and cardiac contractions
Protein catabolism
Inhibit bone formation
Inhibits collagen synthesis
Increases vascular contractility
Anti-inflammation
Anti-immune activity
Maintains normal GFR
Adrenal Physiology
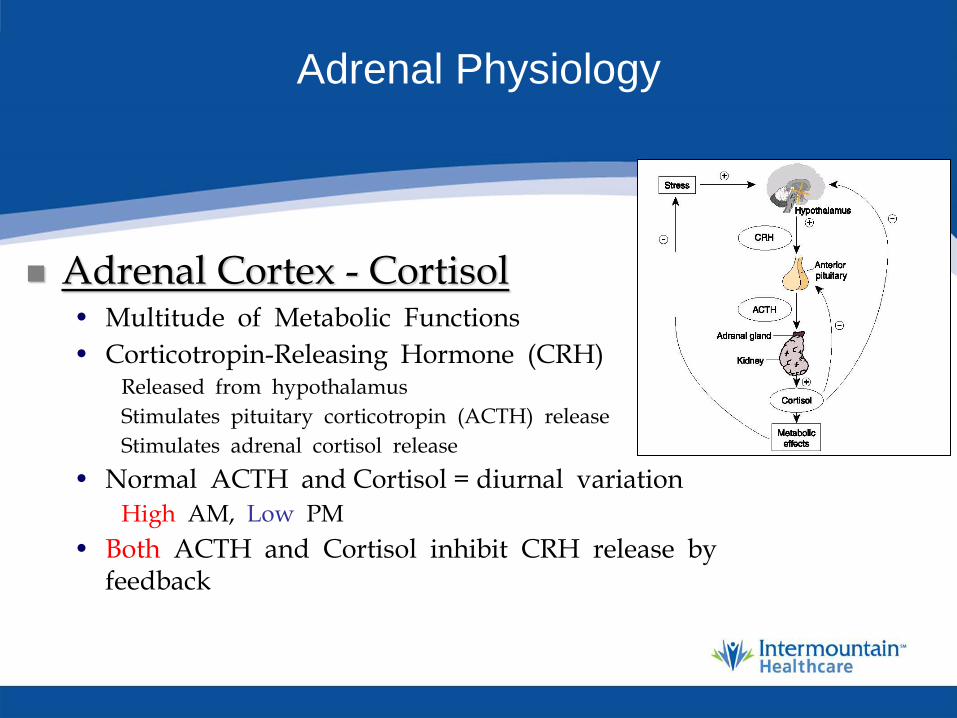
Adrenal Cortex - Cortisol • Multitude of Metabolic Functions
• Corticotropin-Releasing Hormone (CRH) Released from hypothalamus
Stimulates pituitary corticotropin (ACTH) release
Stimulates adrenal cortisol release
• Normal ACTH and Cortisol = diurnal variation
High AM, Low PM
• Both ACTH and Cortisol inhibit CRH release by feedback

Adrenal Physiology
Testosterone and Estrogen • Regulatory Functions
• Sex Steroid Secretion by Adrenal Gland Stimulated by ACTH
Not gonadotropins
• Sex Steroid Secretion by Adrenal Gland
Minor physiologic importance,
Significant only in disease states

Adrenal Physiology
Adrenal Medulla • Distinct from Cortex Embryologically
Derived from neuroectoderm
• Stored in Secretory Cells • Secretes Cathecolamines Sympathetic
Stimulation • Preganglionic Neurons Trigger Release • Can be released with out sympathetic
stimulation Pheochormocytoma
Adrenal Physiology
Adrenal Medulla - Catecholamines
• Large Chromaffin Cells Precursors: Dietary Tyrosine and Phenylalanine
Site of Production: Adrenal, CNS, Adrenergic Nerve Terminals
Adrenal Physiology
Adrenal Medulla - Catecholamines
• Healthy Humans Circulating Catecholamines Norepinehprine 73%
Epinephrine 14%
Dopamine 13%
Adrenal Physiology
Adrenal Medulla - Catecholamines
• Healthy Humans Circulating Catecholamines Norepinehprine 73%
Epinephrine 14%
Dopamine 13%
• Phenylethanolamine-N-methyltransferase (PNMT)
From the Medulla
Methylation of Norepinephrine = Epinephrine

Adrenal Physiology
Adrenal Medulla - Catecholamines
• Healthy Humans Circulating Catecholamines Norepinehprine 73%
Epinephrine 14%
Dopamine 13%
• Phenylethanolamine-N-methyltransferase (PNMT)
From the Medulla
Methylation of Norepinephrine = Epinephrine
Excess Norepi and Epi source is -- Adrenal Pathology
Adrenal Physiology
Adrenal Medulla –
Epinephrine / Norepinephrine • Catecholamine Secretion Neural Meditated
• Half Life 20 seconds Metabolism: Catechol-O-methyltransferase
Monoamine oxidase
Products: Primary Urine vanillylmandelic acid (VMA)
Metanephrine
Normetanephrine
Incidentaloma
Definition • Mass > 1cm
• Discovered on examination for non-adrenal purpose
• Absence of signs or symptoms of adrenal disorder
Incidentaloma
Incidence • Autopsy Studies 87,065 patients 1,2
Overall frequency of adenomas 6% (Range 1-32%)
1 Endocr Met Cl North Am 2000:29:159-185
2 Endocr Rev 1995:16:460-484
3 J Endocrin Invest 2006:29:298-302

Incidentaloma
Incidence • New Physical Examination: Vitals, CT, Physical Exam
• Abdominal CT Incidence 4% 3
• Probability Increases with age
Age 20-29 = 0.2%
Age >70 = 7%
1 Endocr Met Cl North Am 2000:29:159-185
2 Endocr Rev 1995:16:460-484
3 J Endocrin Invest 2006:29:298-302
Incidentaloma
Incidence • New Physical Examination: Vitals, CT, Physical Exam
• Abdominal CT Incidence 4% 3
• Probability Increases with age
Age 20-29 = 0.2%
Age >70 = 7%
• 85% of these are non-functional and benign
• Huge cost of evaluation unless streamlined
• Balance of costs and benefits 1 Endocr Met Cl North Am 2000:29:159-185
2 Endocr Rev 1995:16:460-484
3 J Endocrin Invest 2006:29:298-302

Incidentaloma
Questions to be Asked • Is the Mass Functional?
Physical Signs or Symptoms
Biochemical Evidence
Pheo screen
Potassium Glucocorticoid Screen
• Is the Mass Malignant? History of another malignancy? Imaging suggestive of malignancy?

Incidentaloma
Nature of Mass N=2005
• Non-functioning Adenoma 82%
• Functioning Adenoma Cushing’s Syndrome 5%
Pheochromocytoma 5%
Aldosteronoma 1%
• Malignancy Adrenal Metastasis 3%
Adrenal Cortical Ca. 4%
Young WF, Endocrinol Clin N America 2000

Incidentaloma
Nature of Mass • Medical History and Size
Key Characteristics
• Adrenal Metastasis 6% - No history of cancer
50% - Positive history of cancer
• Adrenal Cortical Carcinoma 2% For all masses
65% For masses > 6 cm
Incidentaloma
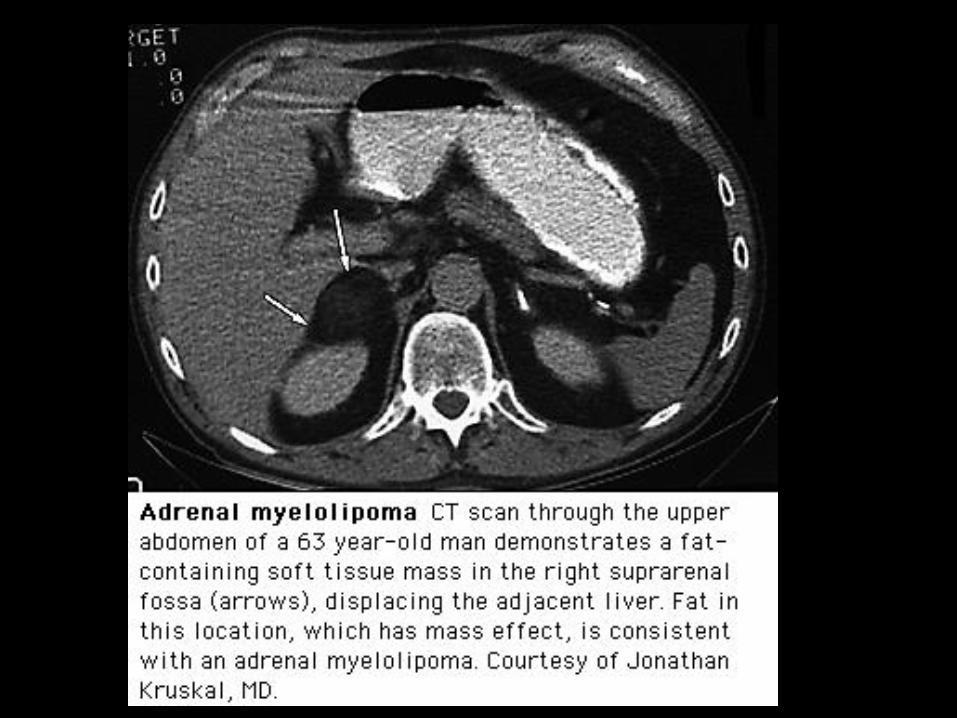
• Other (Rarer) Possibilities • Myelolipoma / Lipoma
CT similar to that of renal angiomyelolipoma (fat)
• Adrenal Cyst / Hematoma Benign cysts can be followed
True cyst or pseudo-cyst
• Ganglioneuroma
• Neuroblastoma

Incidentaloma
Findings • No Overt Symptoms
• Endocrine Activity Cushing’s 5 %
Pheochromocytoma 2 %
Aldosteronoma < 1 %
• Presence of Known Primary Cancer, Adrenal mass is metastasis in 50% - 70 %
Incidentaloma
Sub-Clinical Cushing’s Syndrome • Total 24° Cortisol Production
Often normal
Subtle changes occur - loss of diurnal variation
• Prognosis Variable Normalization
Persistence
Progression to clinical Cushing’s
• Indication for adrenalectomy
May be subtle physical effects
NEJM, 356:6 2007
Incidentaloma
Sub-Clinical Cushing’s Syndrome • Autonomous cortisol secretion
• With out typical signs symptoms of hypercortisolism
• 5% - 20 % of Incidentalomas have SCCS
• Spectrum: Slight attenuation of diurnal cortisol rhythm
Complete atrophy of contralateral gland
Young, EF, Clin North Am, 2000;29:159-185
Ohashi A et al Jendocr J, 2001: 677-683
Young WF et al, J of Medicine, 2007:601-610
MitchellI et al, Surgery, 2007: 900-905
Reincke M, Endocrin Metab Clin North AM, 200, Mar:43-56
Incidentaloma
Sub-Clinical Cushing’s Syndrome
Clinical Manifestations recent or rapid onset:
HTN 80%
Obesity 50%
Diabetes mellitus 40%
Osteoporosis/Osteopenia 25%
Irregular Menses 20%
Young, EF, Clin North Am, 2000;29:159-185
Ohashi A et al Jendocr J, 2001: 677-683
Young WF et al, J of Medicine, 2007:601-610
MitchellI et al, Surgery, 2007: 900-905
NEJM, 356:6 2007
Incidentaloma
Sub-Clinical Cushing’s Syndrome • Best Test
1) 3 mg dexamethasone suppression
serum cortisol suppressed to less 3 mg/dl (80 nmol/L) excludes significant cortisol secretion
2) 8 mg dexamethasone suppression 68% not suppressed
2) Cortisol >5ug/dl
• Glucocorticoid autonomy 91% specific
Young, EF, Clin North Am, 2000;29:159-185
Ohashi A et al Jendocr J, 2001: 677-683
Young WF et al, J of Medicine, 2007:601-610
MitchellI et al, Surgery, 2007: 900-905
NEJM, 356:6 2007
Incidentaloma
Sub-Clinical Cushing’s Syndrome • Surgical Candidates:
• Symptoms: Obesity, HTN, DM, ostopenia
• < 50 yo
• Suppressed plasma ACTH
• Most will progress to overt Cushing's 1-5 years
Young, EF, Clin North Am, 2000;29:159-185
Ohashi A et al Jendocr J, 2001: 677-683
Young WF et al, J of Medicine, 2007:601-610
MitchellI et al, Surgery, 2007: 900-905
NEJM, 356:6 2007

Incidentaloma
Diagnosis • History and Physical Exam
Signs of Hormonal Syndromes
Search for Occult Malignancy
- CXR
- Stool for occult blood
- Mammogram (in women)
Limited Endocrine Evaluation
Pheo -- Potassium -- Cortisol
Incidentaloma
Diagnosis: Limited Endocrine Evaluation • Extent Remains Controversial
• Most Limited Evaluation
- Serum K if hypertensive
R/O Aldosteronoma
Unlikely if not hypertensive
- Plasma Free Metanephrines (normetanephrine and metanephrine)
Most sensitive test (99% sensitive/ 89% specific)
Most important “sub-clinical” entity Pheochromocytoma
- 24 hour Urine Cortisol
Annals of Internal Med,138:5, 2003
Incidentaloma
Diagnosis: Limited Endocrine Evaluation • Extent Remains Controversial
• Consider also obtaining …
- Serum K in all (Aldosteronoma)
- Plasma DHEA (ACC)
- 24° urine cortisol
- low dose dexamethasone suppression test
(Cushing’s Syndrome; last is more sensitive for “subclinical”)
Incidentaloma
Diagnosis: Endocrine Evaluation
• Indications - Complete Endocrine Evaluation - Findings on Examination and H & P
Suggestive of an excess of specific hormone
- Positive Findings on limited evaluation
- Then do workup for that hormone

Incidentaloma
Hypertension -- Adrenal Gland • 15% of Adult Population is Hypertensive
• 1% is Adrenal in Origin 0.5% primary hyperaldosteronism
0.2% pheochromocytoma
0.2% Cushing's Syndrome
• Evaluation is the Same
Incidentaloma
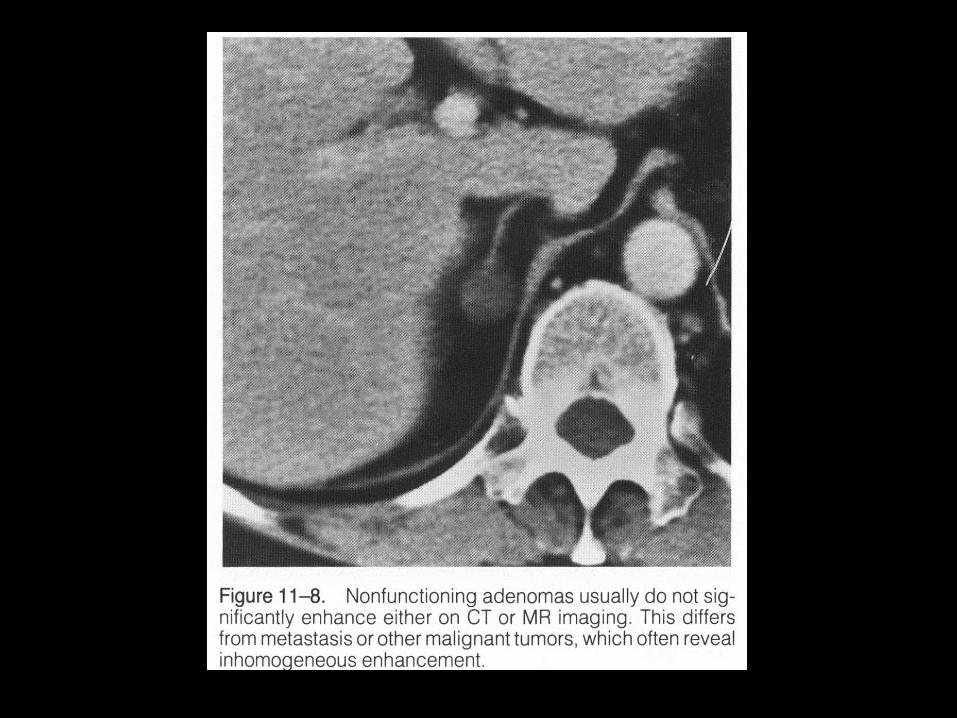
Diagnosis: Imaging • Most Incidentalomas Non-functional
If not a metastasis
non-functioning adenoma
adrenal cortical carcinoma
• Uncertain Progression of Non-functional Adenoma Complicates Issue
• Several reports of conversion to autonomous production
• Follow annually x 4 years
Euro J Endocrin 2002:146:61-66
Euro J Endocrin 2002:147:489-494
Incidentaloma
Diagnosis: Imaging • Uncertain Progression of Non-functional Adenoma
Complicates Issue
o 5-25% increase in size
o 20% develop hormonal overproduction
• Follow annually x 4 years
Euro J Endocrin 2002:146:61-66
Euro J Endocrin 2002:147:489-494
Annals of Internal Med,138:5, 2003

Incidentaloma
Diagnosis: Imaging • Most Series Report No Progression of Small
Adenomas to Cancer Kloos 1997: 3 cancers in patients initial 3 - 5 cm masses that
did not follow-up
Linos 1997: 3 cancers measuring 2.6 - 2.9 cm
Zaluaka, 1998: 311 Incidental Masses 22 Carcinoma (7%)
Tumor Size 3.2 cm – 20 cm
Incidentaloma
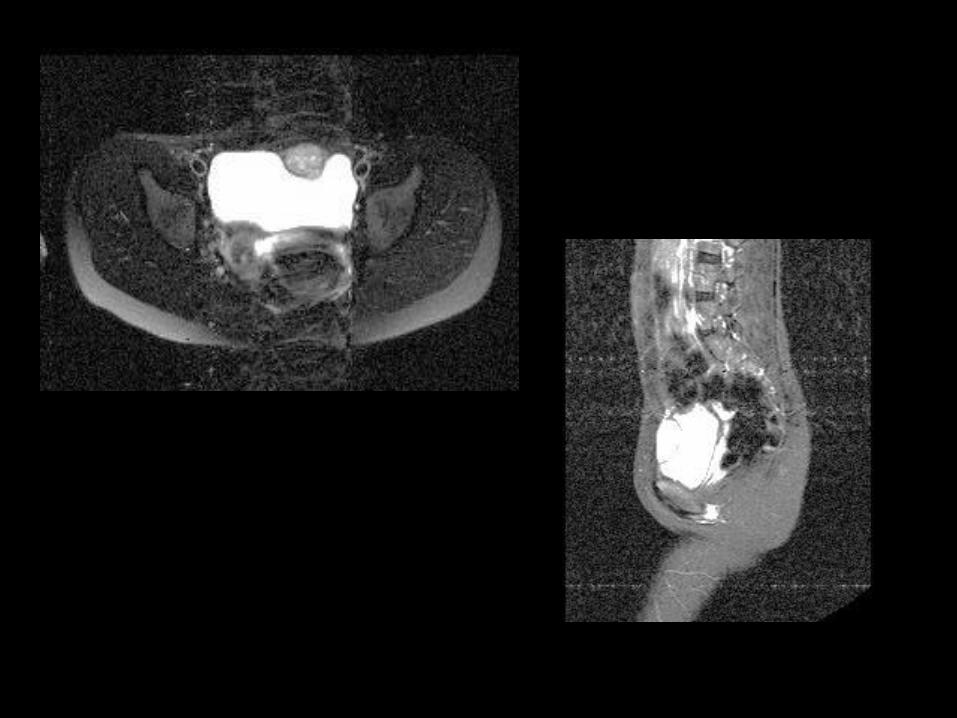
Diagnosis: MRI Carcinoma and Pheochromocytomas
– Hyperintense on T2 images
– (i.e., they “light up” as go from T1 to T2) – Intensity adrenal gland on T2 relative to liver
< 0.8 suggests cortical adenoma
Chemical-shift MRI – Signal from cortical adenomas drops out in
opposed phase
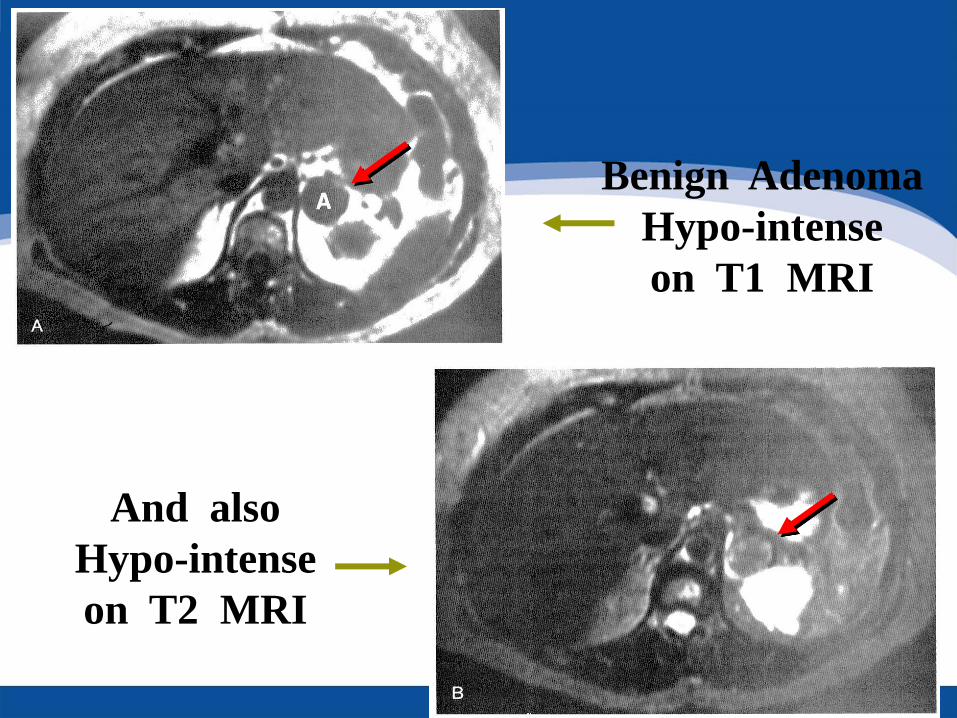
Benign Adenoma
Hypo-intense
on T1 MRI
And also
Hypo-intense
on T2 MRI
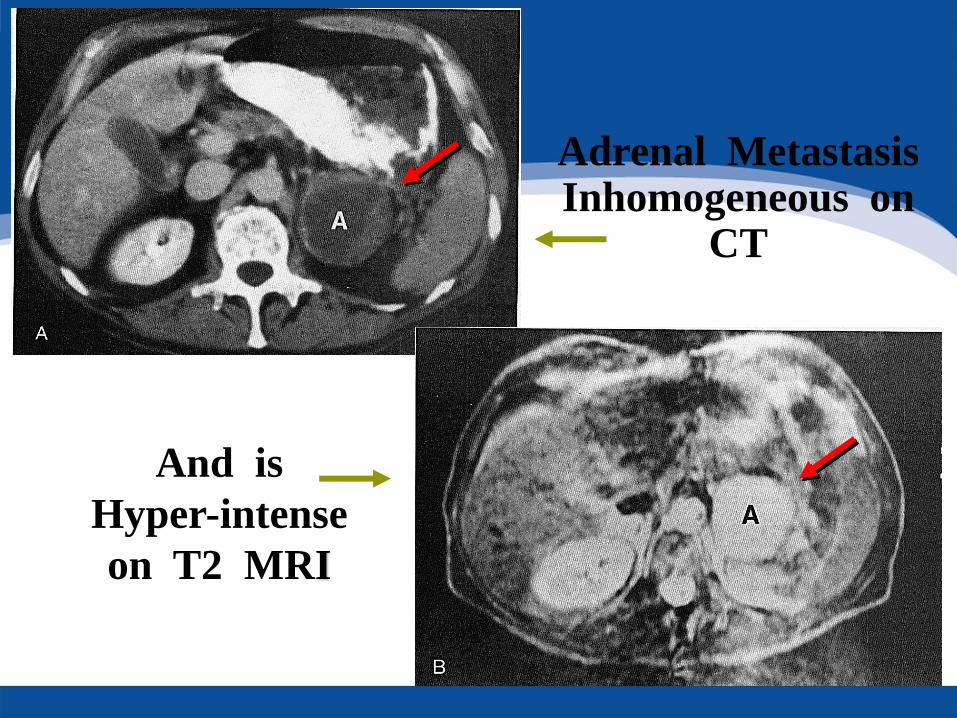
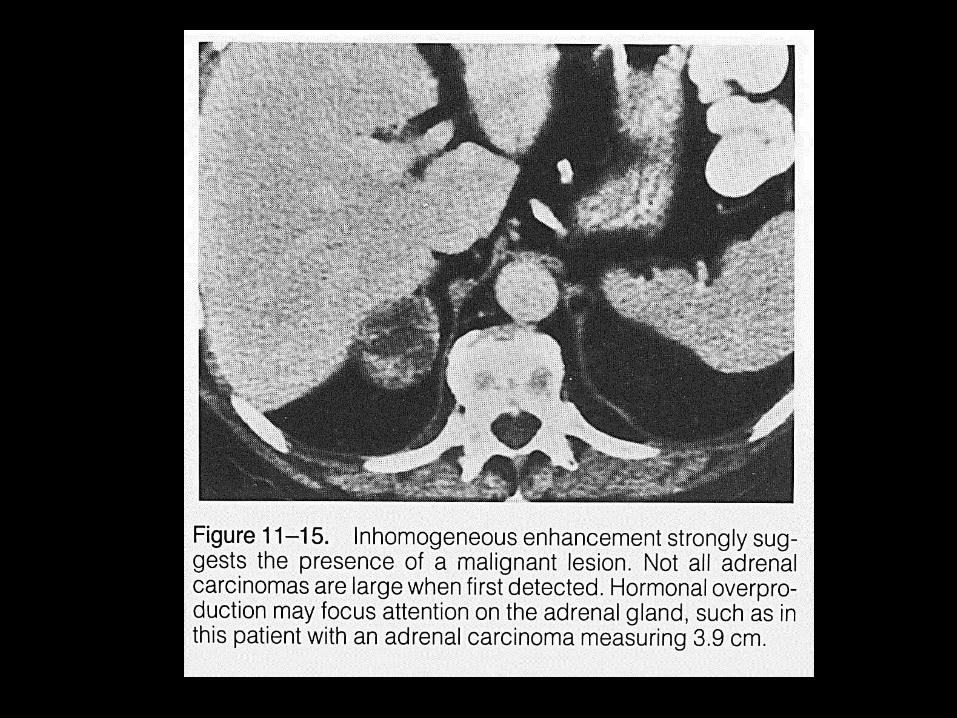
Adrenal Metastasis Inhomogeneous on
CT
And is
Hyper-intense
on T2 MRI
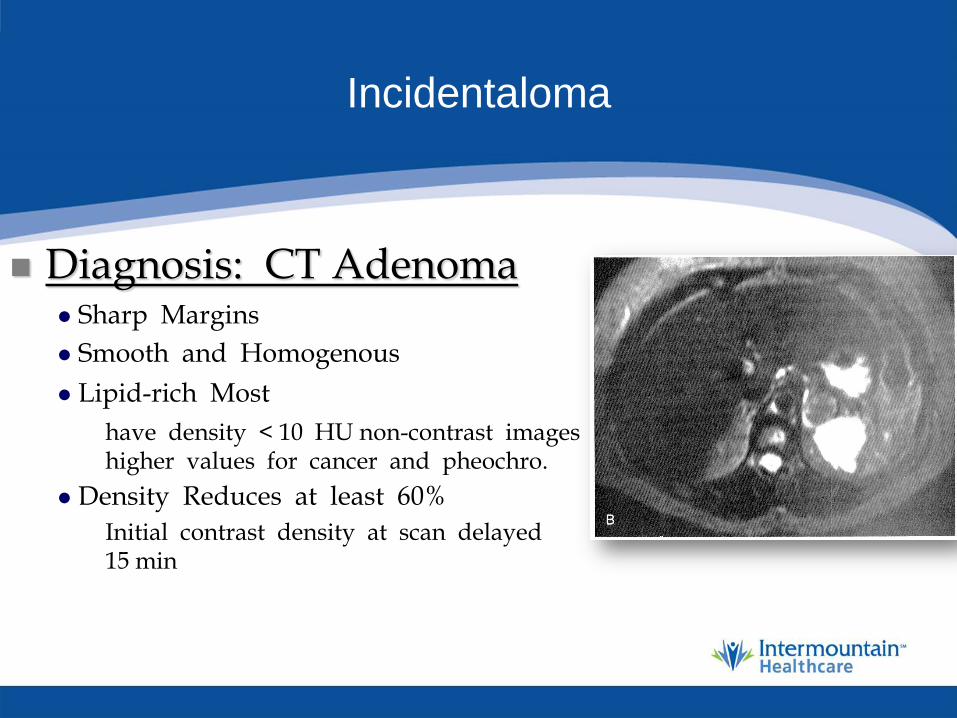
Incidentaloma
Diagnosis: CT Adenoma Sharp Margins
Smooth and Homogenous
Lipid-rich Most
have density < 10 HU non-contrast images higher values for cancer and pheochro.
Density Reduces at least 60%
Initial contrast density at scan delayed 15 min
Incidentaloma
Diagnosis: Nuclear Scintigraphy NP-59 (131I-6b-iodomethyl-norcholesterol)
Taken up by adrenal cortex (inc. adenoma)
Not space occupying lesion (cancer, pheochromocytoma)
Contralateral gland may suppress in Cushing’s
MIBG
Taken up preferentially by pheochromocytoma
Incidentaloma
Diagnosis: Imaging Criteria
Size Criteria 90% adrenal cortical carcinomas > 6 cm
Few Adenomas this large
CT underestimates actual size by 20%
Some recommend Exploration >5 cm
There is no cut-off with perfect accuracy
Incidentaloma
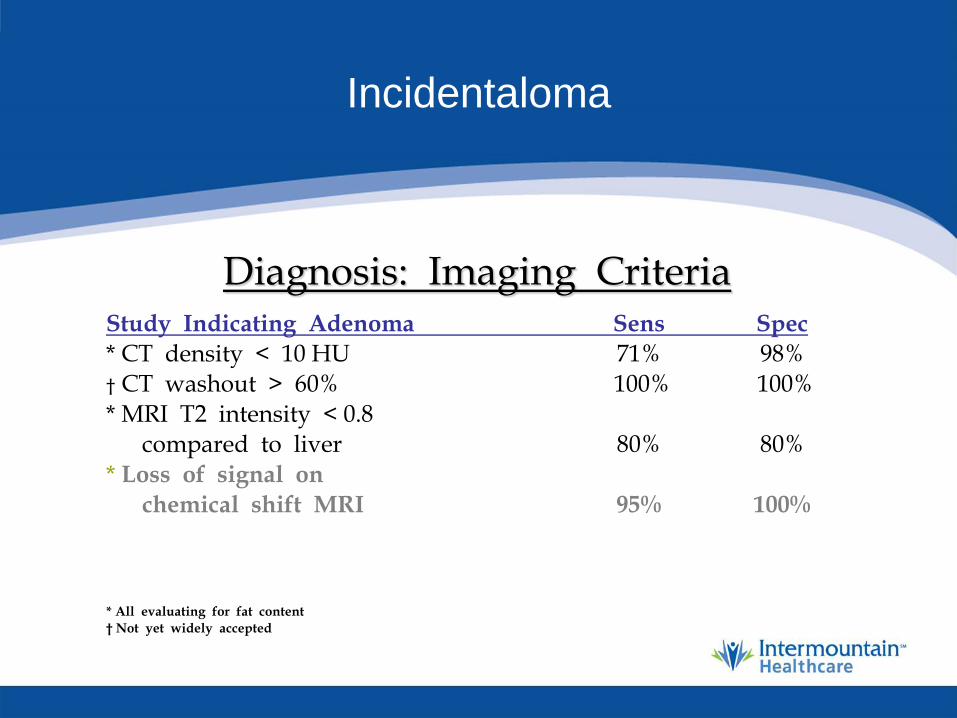
Diagnosis: Imaging Criteria
Study Indicating Adenoma Sens Spec
* CT density < 10 HU 71% 98% † CT washout > 60% 100% 100% * MRI T2 intensity < 0.8 compared to liver 80% 80% * Loss of signal on
chemical shift MRI 95% 100%
* All evaluating for fat content
† Not yet widely accepted

Incidentaloma
Management Recommendations • Hormonally Active Mass
Should be removed
• Hormonally Inactive Mass
If imaging suggests cancer, remove If > 5 cm at any age = remove
If < 3 cm, observe
Incidentaloma
Management Recommendations Observation • Consensus Recommendation
CT at 6 months,
Annual endocrine evaluation for 4 years
Growth/ development of endocrine function, remove
• Emerging Recommendation
If mass stable on scans at 3 and 12 months
No function
Routine follow-up not required

Pheochromocytoma
Incidence and Presentation • Hypertension in 90% of cases
Paroxysmal, Sustained, or both
May have Orthostatic Hypotension
plasma volume
• 30% at Autopsy (death often due to cardiovascular disease)
• Can Arise anywhere in Paraganglion System
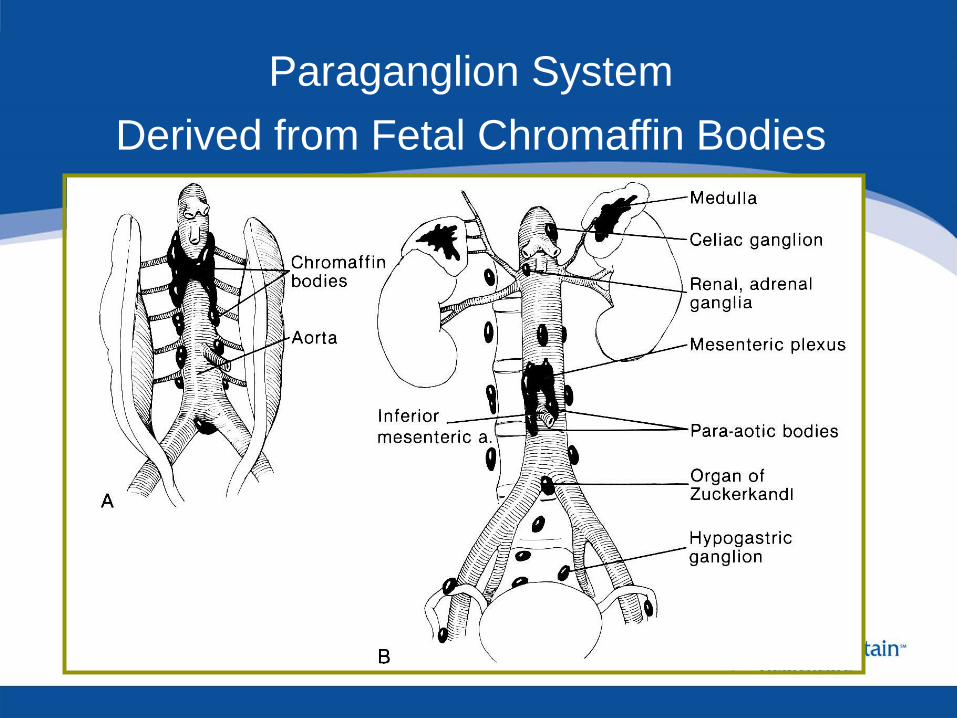
Paraganglion System
Derived from Fetal Chromaffin Bodies

Pheochromocytoma
Pathophysiology • Excessive Secretion of Catecholamines
Norepinephrine
Epinephrine
To lesser extent, Dopamine
• Levels that May be Measured Diagnostically 21 Different tests
Breakdown products of the primary catecholamines
VMA
Metanephrines

Pheochromocytoma
Clinical Findings • Classic Triad:
Episodic Headache
Tachycardia
Diaphoresis

Pheochromocytoma
Clinical Findings • Classic Triad:
Episodic headache
Tachycardia
Diaphoresis
• Most Commonly Young to middle-age adults
Sustained HTN with superimposed paroxysms

Pheochromocytoma
Clinical Findings • Classic Triad:
Episodic headache 49% Tachycardia 46% Diaphoresis 49% Palpitations 46% Hypertension 60%
• Most Commonly Young to middle-age adults Sustained HTN with superimposed paroxysms
• Pheochromocytoma Etiology of Hypertension in Only 0.2% 10% with Pheo are normotensive Presentation during pregnancy
Pheochromocytoma
Clinical Findings Unexpected Cardiovascular Response Anesthesia
Catecholamine-induced Cardiomyopathy
Necrosis Inflammation Fibrosis
~80% mortality for surgery if untreated

Pheochromocytoma
Clinical Findings Unexpected Cardiovascular Response Anesthesia
Catecholamine-induced cardiomyopathy
Necrosis Inflammation Fibrosis
~80% mortality for surgery if untreated
Other Findings: Flushing Tremor
Pallor Anxiety
Pain Nausea / vomiting
Psychosis Sweating
Small Tumors Less Binding of Catehcholamines
Large Tumors More Binding
Pheochromocytoma
Rule of 10s Bilateral in 10%
Familial (non-sporadic) in 10%
Pediatric in 10%
Malignant in 10%
Normotensive in 10%
Extra-adrenal in 10%
Multiple in 10%
* Childhood Presentation Breaks Rules
25% are bilateral, multiple, or extra-adrenal
Pheochromocytoma
Associated Syndromes • von Hippel-Lindau Disease
• Von Recklinghausen’s Neurofibromatosis
• Multiple Endocrine Neoplasia
Suspect Syndrome
Evaluate for other components
Evaluate family members
Pheochromocytoma
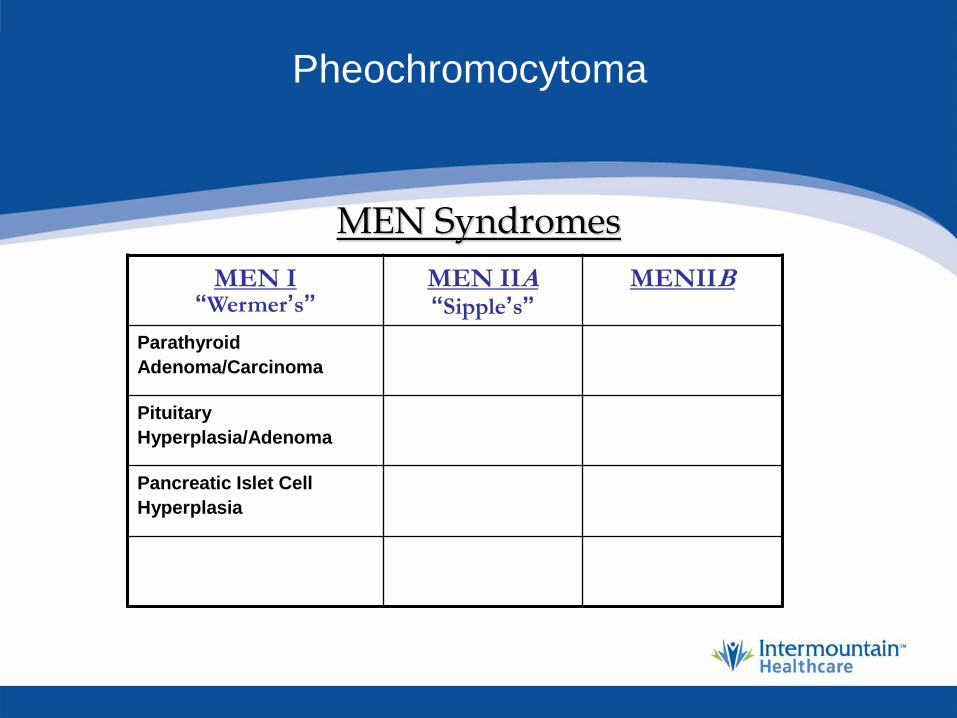
MEN Syndromes
MEN I “Wermer’s”
MEN IIA “Sipple’s”
MENIIB
Parathyroid
Adenoma/Carcinoma
Pituitary
Hyperplasia/Adenoma
Pancreatic Islet Cell
Hyperplasia
Pheochromocytoma
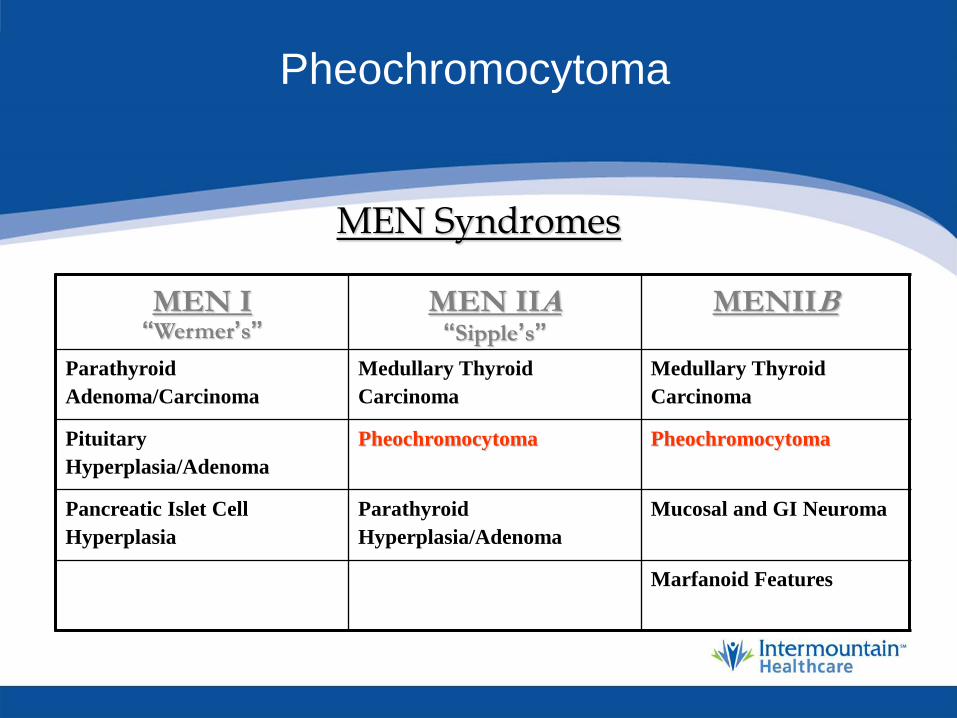
MEN Syndromes
MEN I “Wermer’s”
MEN IIA “Sipple’s”
MENIIB
Parathyroid
Adenoma/Carcinoma
Medullary Thyroid
Carcinoma
Medullary Thyroid
Carcinoma
Pituitary
Hyperplasia/Adenoma
Pheochromocytoma Pheochromocytoma
Pancreatic Islet Cell
Hyperplasia
Parathyroid
Hyperplasia/Adenoma
Mucosal and GI Neuroma
Marfanoid Features

Pheochromocytoma
Diagnosis: First Level • Plasma Free Metanephrines
Most Sensitive Test
• 90% of Patients Have Elevated: - 24° Urinary Catacholamies 2 x normal
Next most sensitive test
- 24° Urinary Metanephrines Total metanephrines and vanillyl mandellic acid (VMA) Most specific tests
• 7% Have normal metanephrines
European J Endocrinology, 2004;150:681-686
Pheochromocytoma
Management • Surgical excision is mainstay
• Evaluate for extra-adrenal, multiple, and bilateral sites
• Primarily radiographic
• Extent of disease staged pre-operatively
• Unless metastatic disease apparent, cannot tell if will be malignant

Pheochromocytoma
Radiographic Localization Imaging Sensitivity Specificity
CT 98% 70%
MRI * 100% 67%
MIBG † 86 - 100% 85 - 99%
* Hyperintense on T2
† Scintigraphy with 123 or 131I-Meta-iodobenzylguanidine
lights up even if not apparent on MRI
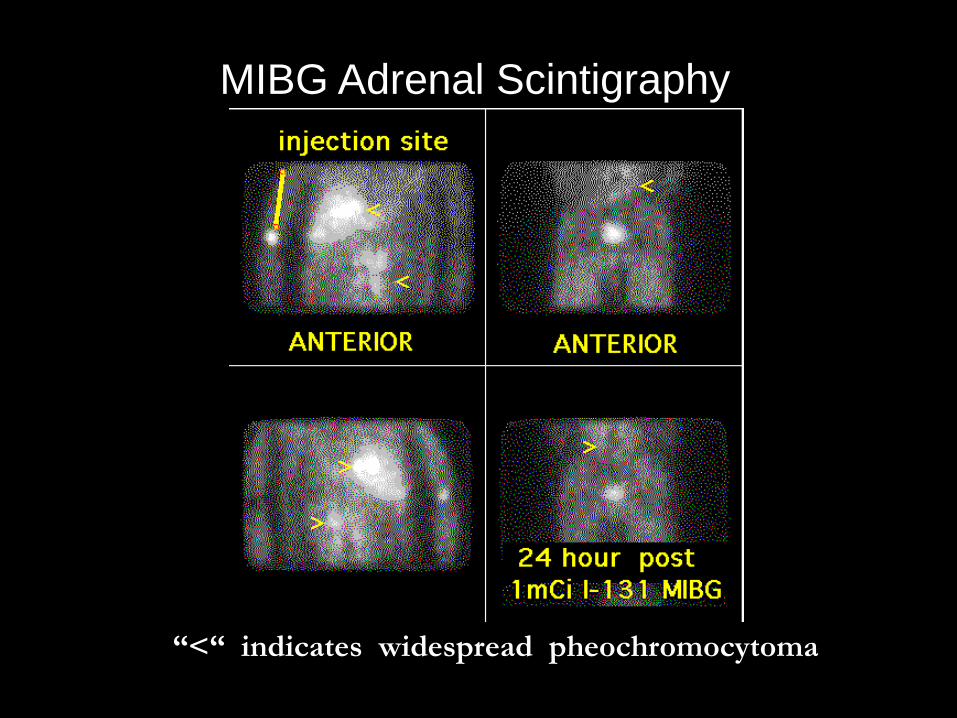
MIBG Adrenal Scintigraphy
“<“ indicates widespread pheochromocytoma
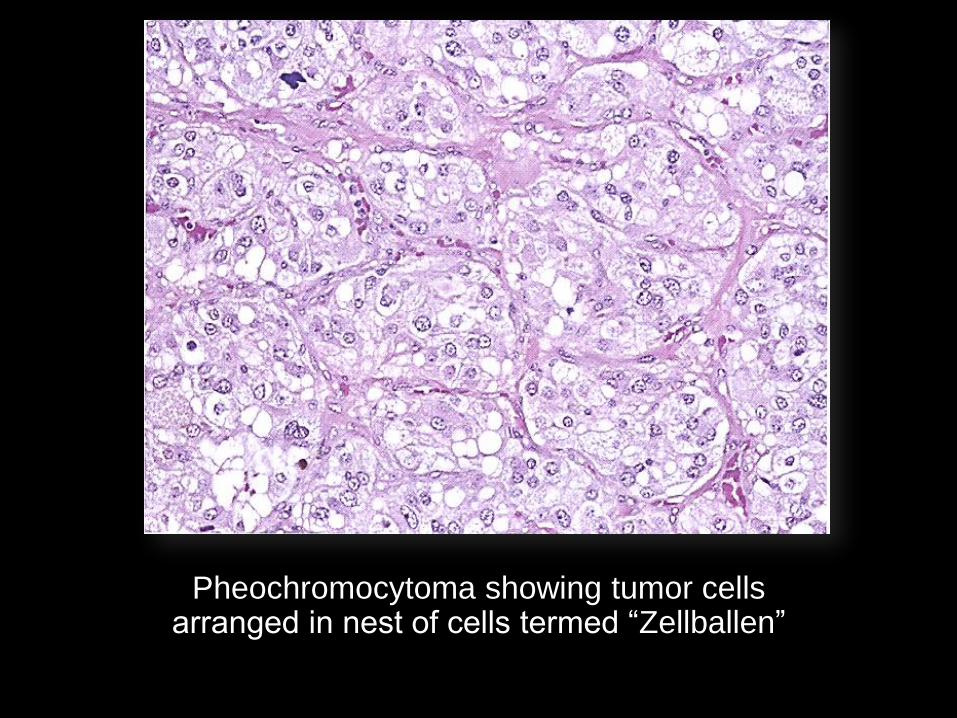
Pheochromocytoma showing tumor cells arranged in nest of cells termed “Zellballen”
Pheochromocytoma
Peri-Operative Management
Is it Necessary?
Pheochromocytoma
Peri-Operative Management • Pharmaceuticals
+ Calcium-channel blocker
with alpha- followed by beta- blocker as needed
Orthostatic hypotension
• Liberalize Water and Salt Intake
• IV Hydration Pre-operative
• Invasive Monitoring Intra-operative
• Careful Post-operative Observation

Pheochromocytoma
Peri-Operative Management • Pharmaceuticals
- Phenoxbenzamine
- Selective Alpha blockers: Doxazosin, terazosin, prazosin
+ Calcium-channel blocker
- beta- blocker as needed for arythmia
- Goal orthostatic hypotension
• Liberalize Water and Salt Intake
• IV Hydration Pre-operative
• Invasive Monitoring Intra-operative

Pheochromocytoma
Pre-Operative Medical Management Mayo 98% phenoxybenzamine N=50
Cleveland 65% alpha blocker N=37
Max Systolic
BP
IV Fluid
Crystalloid
IV colloid Patient needing
Phenylephrine
Mayo 187mmHg 2977 cc
Cleveland 209 mmHg 5000 cc
P value P<0.11 P<0.10
Weingarten TN et al. Urology 2010, Aug 76:508

Pheochromocytoma
Pre-Operative Medical Management Mayo 98% phenoxybenzamine N=50
Cleveland 65% alpha blocker N=37
Max Systolic
BP
IV Fluid
Crystalloid
IV colloid Patient needing
Phenylephrine
Mayo 187mmHg 2977 cc 0 cc 56%
Cleveland 209 mmHg 5000 cc 1000 cc 27%
P value P<0.11 P<0.10 P<0.001 P=0.009
Weingarten TN et al. Urology 2010, Aug 76:508
Pheochromocytoma
Pre-Operative Preparation Required •Mortality up to 80% on untreated patients
•Consultation:
Endocrinologist
Cardiologist
Anesthesiologist
•Goals
Normalize blood pressure
Expand plasma volume
Prevent cardiac arrhythmias
Prevent intra-op hypertension
Minimize post-op hypotension
Pheochromocytoma
Pre-operative Preparation
• Stepwise Plan: Pharmaceuticals
• Consider starting with long acting calcium-channel blocker
Verapamil SR (120 - 240 mg/d)
Nifedipine XL (30 - 90 mg/d)
Addresses both hypertension and arrhythmias
Few adverse effects
MAY be adequate monotherapy
Pheochromocytoma
Pre-operative Preparation • Stepwise Plan: Pharmaceuticals
• Alpha blocker Alpha-1 blocker prazosin (4 - 10 mg/d) good for HTN
refractory to Ca-blocker, but not for monotherapy
Classic initial therapy is non-selective, long acting phenoxybenzamine
start 5 mg bid, 10 mg qod prn to 100 mg bid
beware post-operative hypotension
Pheochromocytoma
Pre-operative Preparation • If refractory arrhythmias (inc. sinus tachycardia), add
beta blocker
Use only after alpha-blockade (exacerbate HTN if unopposed)
Propranolol (20 - 40 mg tid)
Usually not necessary
• Rarely alpha-methyl para tyrosine -- severe cases
Significant adverse effects

Pheochromocytoma
Intra-operative Management • Pre Op Anesthesia Consultation • Low Threshold to Cancel Case If Not Prepared • Certain popular agents avoided
Halothane, propofol, MSO4, pancuronium • To control intra-operative hypertension
Phentolamine, nitroprusside, esmolol • To control post-excision hypotension
Norepinephrine • ~ 5% of have negative studies, so warn anesthesiologist
Pheochromocytoma
Post-Operative Management • Hypotension
Most commonly hypovolemia
• Hypertension Catecholamine levels elevated for several days Essential HTN
Residual unresected tissue
• Hypoglycemia Insulin , use 5% dextrose in IVF

Pheochromocytoma
Surgical Principles
• Ligate Adrenal Vein First Prevent intra-operative catecholamine surge
Some reports suggest fewer catecholamine surges and less cardiovascular instability with laparoscopy
• “Dissect the patient away from the tumor”
Pheochromocytoma
Surgical Outcome • Excision not always lead long term cure
even in patients with a benign tumor
• Benign recurrence 5%
• Malignant recurrence 10%
• Hypertension may persist
related to age / family history
• 80% 20-year cause-specific survival
• Long-term follow-up required
Primary Hyperaldosteronism
Primary Hyperaldosteronism (Conn’s Syndrome)
• 1955 Clinical Syndrome: Hypertension
Hypokalemia
Hy[ernatremia
Alkalosis
Periodic Paralysis
• Primary Hyperaldosteronism (Conn’s Syndrome) • 1955 Clinical Syndrome:
Hypertension
Hypokalemia
Hypernatremia
Alkalosis
Periodic Paralysis
• Today Hypokalemia
Hypertnesion
Depressed Renin
High urine and plasma aldosterone
Primary Hyperaldosteronism

Clinical Features • Refractory Hypertension
• Hypokalemia
• Profound Hypokalemic Response to Diuretics
• Often Asymptomatic
• May Manifest:
muscle weakness, tetany, headache, polydipsia
• Low-Salt Diet Limits Potassium Wasting
less Na available for K exchange
which improves symptoms
Primary Hyperaldosteronism
Primary Hyperaldosteronism (Conn’s Syndrome)
• Cause of Hypertension in ~ 0.5%
• Most Commonly
Caucasian, 30 - 60 years of age
• Pathology
70% aldosteronoma
30% bilateral adrenal hyperplasia
Bilateral adrenal hyperplasia mostly in men
Primary Hyperaldosteronism

Pathophysiology • Primary Hyperaldosteronism
Autonomous (without stimulation) secretion of aldosterone from adrenal gland
Results in salt retention, hypertension, and potassium wasting
May have autonomous overproduction of cortisol
• Secondary Hyperaldosteronism Renovascular HTN -
Aldosterone is 2° to Renin
Primary Hyperaldosteronism

Diagnosis: First Level • Serum K < 3.0 mEq / dl
• Plasma Renin Activity Suppressed (PRA) < 2 ng / ml
25% of essential hypertensives have depressed PRA
But normokalemic
• Plasma Aldosterone > 15 ng / dl
• Aldosterone:PRA > 20:1
• Confirmation High Sodium Diet 3 Days (>200 mEq/Day)
24 hr Urine Aldosterone
Urine aldosterone > 14 mcg / 24°
Urine K > 30 mEq / 24°
Primary Hyperaldosteronism
Diagnosis: Adrenal Vein Sampling • Recommended:
Aldo/Renin Ratio > 20
Serum aldo > 15
• If age > 40 or bilateral imagining findings needs sampling
• If age < 40 years old • Localize with CT or MRI
• If 1 cm or greater
• No sampling needed remove
American Association of Clinical Endocribnilogists
Endocrine Practice Vol 15: Supp 1 July August 2009
Primary Hyperaldosteronism

Diagnosis: Adrenal Vein Sampling • 12 patients
Positive CT findings
Positive Screening tests
• 11 patients Vein sampling 73% positive from CT defined side
18% positive from opposite side
9% positive from both sides!
Schwab et al, J Endourology, 2008
Espiner et al, J Clin Endocri Metab 2003
Magill et al, J Clin Endocri Metab 2001
McAlister et al, Can J Surg, 1998
Primary Hyperaldosteronism



Management •Bilateral Adrenal Hyperplasia
Medical therapy
Spironolactone (aldosterone antagonist)
Normalizes serum K
Painful gynecomastia
HCTZ normalizes blood pressure
•Unilateral Adrenal Adenoma Adrenalectomy following control of HTN and
hypokalemia (amiloride, triamterene, spironolactone) Partial Adrenalectomy
Primary Hyperaldosteronism

Result of Adrenalectomy
• 35% Cured of hypertension
• 56% Improved hypertension
fewer or milder medications
• All but 9% have:
cure or improvement
Primary Hyperaldosteronism


Classic Clinical Findings • Obesity in 90%
80% with Buffalo hump or truncal obesity
Cushing’s Syndrome
Cushing’s Syndrome
Cushing’s Syndrome - Glucocorticoid Excess • Clinical Picture of Hypercorticolism • 1 per 100,000 - 500,000 • ACTH-Dependent Causes (82%)
Cushing’s Disease = Pituitary hypersecretion of ACTH - 70% Ectopic ACTH - 12%
• ACTH-Independent Causes (18%) Adrenal adenoma - 8% Adrenal carcinoma - 6% Bilateral adrenal hyperplasia - 4%
Pathophysiology
• ACTH-Dependent = Primary Excessive ACTH secretion
From pituitary (Cushing’s disease)
Ectopic ACTH secretion ACTH causes increased cortisol
• ACTH-Independent = Primary excessive cortisol secretion
Adrenal adenoma
Carcinoma, or bilateral hyperplasia
Excess cortisol causes Inhibition of ACTH secretion
Cushing’s Syndrome

Clinical Findings • Obesity in 90%
Muscle Weakness 80% Hirsutism 70%
Hypertension 80% Amenorrhea 70%
Diabetes Mellitus 80% Moon Facies 60%
Striae, thin skin 70% Easy Bruising 50%
• Cushing’s rare cause of HTN in ~ 0.2%
Cushing’s Syndrome

Diagnosis: Is this Pseudo-Cushing’s?
• Rule out Exogenous Sources Glucocorticoids
Topical creams, lotions
Review of oral medications
• Non-Endocrine Causes of Hypercorticolism
Major depression
Alcoholism
Cushing’s Syndrome
Diagnosis: A 3 Step Process # 1 - Establish Hypercorticolism
# 2 - Distinguish Between
ACTH-independent vs ACTH-dependent
# 3 - Determine Specific Etiology
ACTH-Dependent
Cushing’s disease pituitary ACTH
Ectopic ACTH secretion
ACTH-Independent Adrenal adenoma
Carcinoma
Bilateral hyperplasia
Cushing’s Syndrome
Diagnosis # 1: Hypercorticolism?
• 24° Urine Free Cortisol > 100 mg / 24 is diagnostic
• If Equivocal: low-dose dexamethasone test – 1 mg at 11 PM, obtain plasma cortisol at 8 AM
– Normal suppresses plasma cortisol to < 5 ng / ml
– No suppression = Cushing’s Syndrome
• Newest Test: Late night salivary cortisol
– Measure at 2300 h
– Cushings cortisol (24.0 +/- 4.5 nmol/L)
– Normal subjects cortisol (1.2 +/- 0.1 nmol/L)
Cushing’s Syndrome
Diagnosis # 2: Relation to ACTH?
• Measure late afternoon ACTH
> 50 pg/ml =ACTH-dependent Cushing’s
(Cushing’s Disease or Ectopic ACTH)
< 5 pg/ml =ACTH-independent Cushing’s
(Primary Adrenal Cushing’s Syndrome)
Cushing’s Syndrome

Diagnosis # 3: Specific Entity? • ACTH-Dependent Cushing’s
High-dose Dexamethasone Test - 8 mg orally at 11 PM
- Plasma Cortisol at 8 AM < 50% reduction = Ectopic ACTH
> 50% reduction = Pituitary tumor
Adenomas and carcinomas fail to suppress cortisol secretion
Pituitary (Cushings Disease) has relative resistance to feedback
Cushing’s Syndrome

Diagnosis # 3: Specific Entity? • Measure Plasma ACTH and Cortisol
• Later afternoon Blood Draw
Cushing’s Syndrome
SUMMARY
Etiology Plasma Cortisol Plasma ACTH
ACTH Independent Adrenal Cushings fails to suppress
> 50 ug/dl < 5 pg/ml
ACTH Dependent Pituitary
Cushings Disease, Ectopic ACTH or
CRH syndrome f
> 50 ug/dl > 5 pg/ml

Diagnosis # 3: Specific Entity?
• ACTH-independent Cushing’s
Imaging (CT) distinguishes:
Adenoma
Cancer
Bilateral hyperplasia
Cushing’s Syndrome
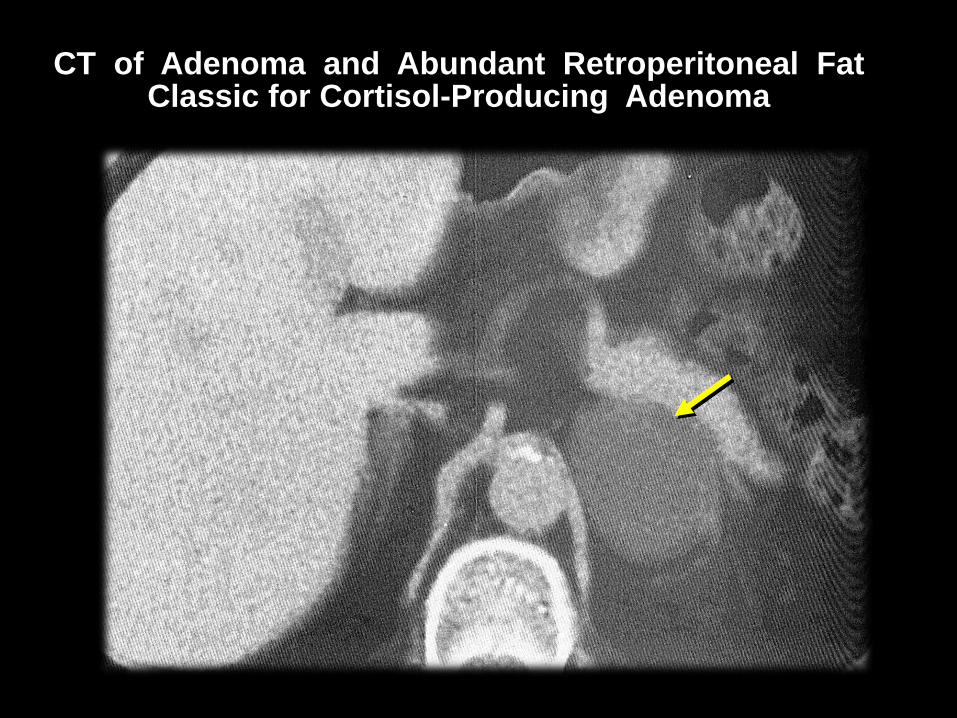
CT of Adenoma and Abundant Retroperitoneal Fat Classic for Cortisol-Producing Adenoma


Management: Adenoma/Cancer • Unilateral Adrenalectomy
• May require pre-operative reduction of cortisol secretion, if markedly elevated (see Ectopic ACTH secretion)
• Excessive Cortisol: Suppresses the other
- intra-operative steroid support
- post-operative steroid taper may be needed
- while the contralateral gland recovers function
Cushing’s Syndrome
Management: Bilateral Adrenal Hyperplasia • Bilateral Adrenalectomy
• 10 - 20% get Nelson’s syndrome
ACTH hyper-secretion by chromophobe adenoma Headache
Deep pigmentation
Visual disturbances
• Lifelong follow-up Sella tursica radiographically
ACTH level
Cushing’s Syndrome
Management • Ectopic ACTH Secretion Resection of tumor if possible
Medical therapy with metyrapone, ketoconozole,
or aminoglutethimide
• Pituitary Tumor Trans-sphenoidal hypophysectomy
For failure
Bilateral adrenalectomy or XRT
Cushing’s Syndrome

Adrenal Insufficiency
Adrenal Insufficiency • 1 per 4,500 - 6,250 hospitalized pts • Third - fifth decade of life • Primary
Autoimmune adrenalitis Infection (TB, HIV most common) Adrenal hemorrhage
• Secondary Metastatic disease Surgical removal, Pituitary disease, Exogenous steroid use

Pathophysiology and Clinical • Deficiency of both glucocorticoid and
mineralocorticoid
• Acute Fever Severe Hypotension Nausea / vomiting Lethargy
Post-operative “crash” without apparent surgical complication
Adrenal Insufficiency
Pathophysiology and Clinical • Deficiency of both glucocorticoid and
mineralocorticoid
• Chronic More Subtle:
Fatigue
Weight loss Anorexia Nausea and Vomiting Abdominal pain
Adrenal Insufficiency

Diagnosis
• Clinical scenario, especially post-operative
• Labs: Hyponatremia, hyperkalemia, azotemia, hypoglycemia
Eosinophilia in 15 - 20%
Rapid IV access
ACTH stimulation -
measure plasma cortisol at 0, 30, 60 minutes
ACTH / CRH levels for 1° vs 2°
Adrenal Insufficiency
Management • Adrenal Crisis
IV access, blood for Chem, ACTH, cortisol
(but don’t wait for result)
2 - 3 liters D5 NS quickly
4 mg dexamethasone IV
(IV cortisol will interfere with dx later)
• Subsequent
Confirm diagnosis
Determine and treat cause
Begin flurocortisone therapy
Adrenal Insufficiency
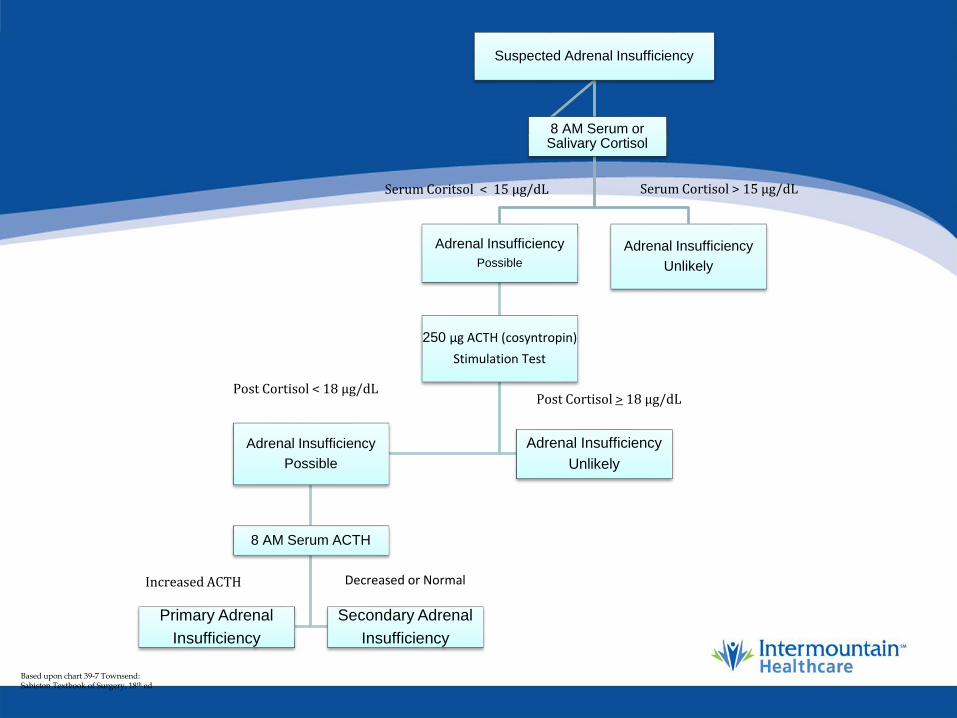
Suspected Adrenal Insufficiency
Adrenal Insufficiency
Possible
250 µg ACTH (cosyntropin)
Stimulation Test
Adrenal Insufficiency
Possible
8 AM Serum ACTH
Primary Adrenal
Insufficiency
Secondary Adrenal
Insufficiency
Adrenal Insufficiency
Unlikely
Adrenal Insufficiency
Unlikely
8 AM Serum or Salivary Cortisol
Serum Coritsol < 15 µg/dL Serum Cortisol > 15 µg/dL
Post Cortisol < 18 µg/dL Post Cortisol > 18 µg/dL
Increased ACTH Decreased or Normal
Based upon chart 39-7 Townsend: Sabiston Textbook of Surgery, 18th ed

Adrenal Cortical Carcinoma
Adrenal Cortical Carcinoma • Rare: 1 per 1.7 million people
• Accounts for 0.02% of cancers, and 0.2% of cancer deaths
• Weiss Criteria for diagnosis High mitotic rate and nuclear grade Atypical mitosis Eosinophilic cytoplasm Diffuse architecture Necrosis Microscopic invasion
Clinical Findings • Constitutional
Weight loss, malaise, fever, etc
• Endocrine (80% functional) Clinical findings of Cushing’s
Sex steroid excess
Oligomenorrhea
Virilization / Feminization
• Can Present as Incidentaloma
Adrenal Cortical Carcinoma
Diagnosis: Endocrine Evaluation • 80% are Functional
• Often Secrete Multiple Hormones
Glucocorticoids 72%
Androgens 43%
Precursors 22%
Estradiol 8%
Aldosterone 4%
• Cushing’s Accompanied by Virilization / feminization is most common
Adrenal Cortical Carcinoma
Diagnosis: Endocrine Evaluation
• Endocrine Fxn Useful in Diagnosis
Finding of multiple hormones suggestive of carcinoma
Carcinoma more often secretes sex steroids (Plasma DHEA, 24° urine 17-ketosteroids) than does adenoma
• Endocrine fxn useful as marker
• Endocrine fxn is not prognostic except for isolated testosterone secretion
Adrenal Cortical Carcinoma
Diagnosis: Radiography • Cross-sectional imaging localization and staging
CT or MRI
Over 90% are > 6 cm
but in one study 16% < 5 cm
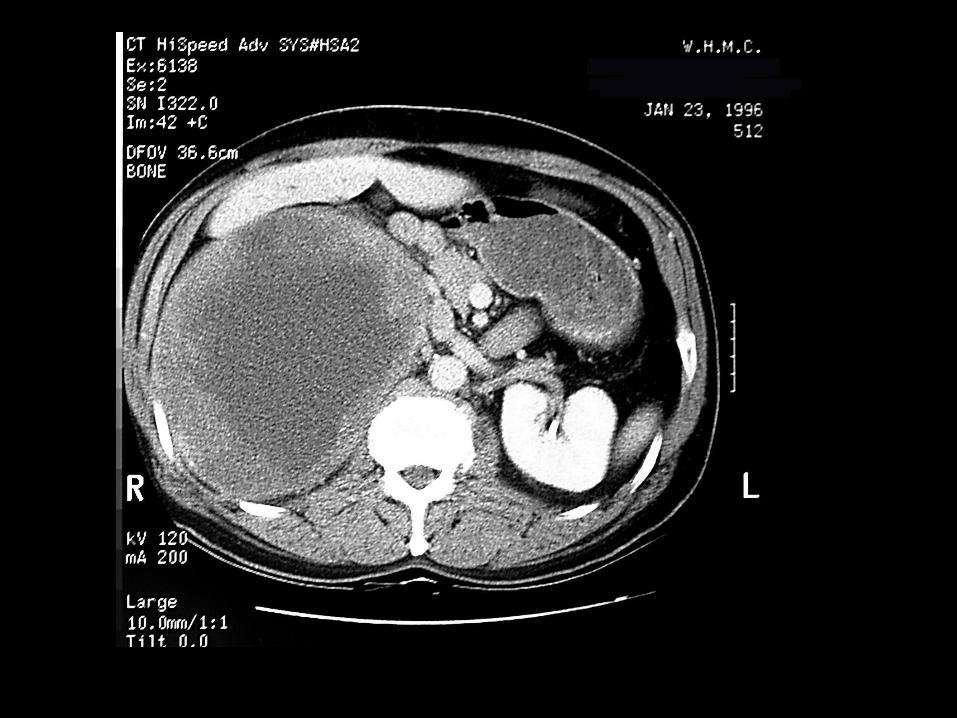
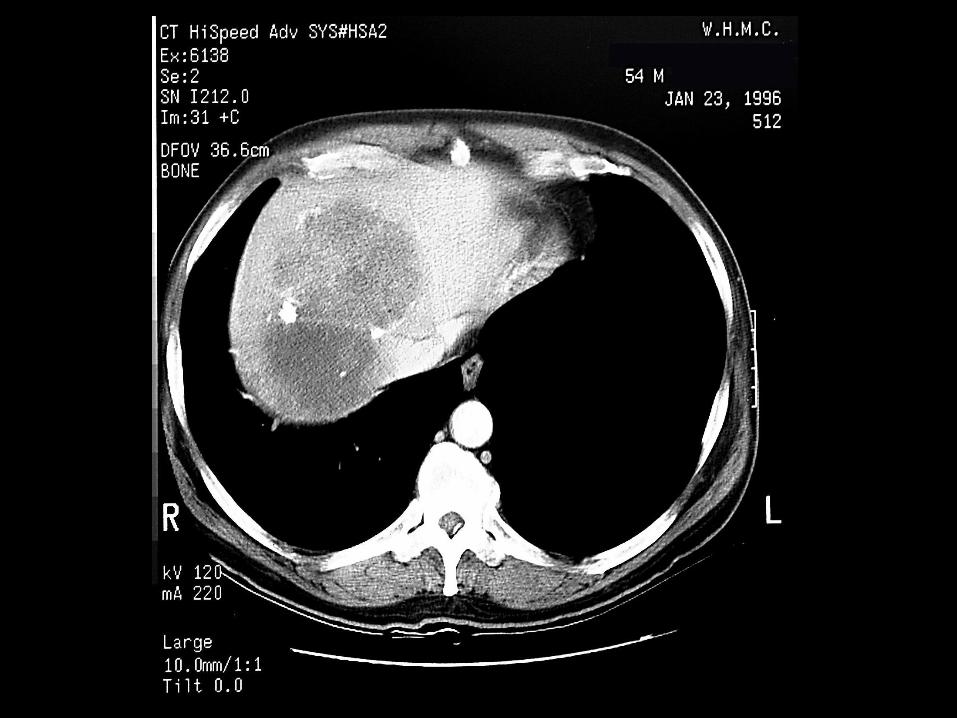
Irregular, inhomogeneous
• Distinction from Adenoma CT ± washout curve
MRI
Adrenal Cortical Carcinoma

Typical ACC “Brightly Lights up”
on T2-weighted MRI
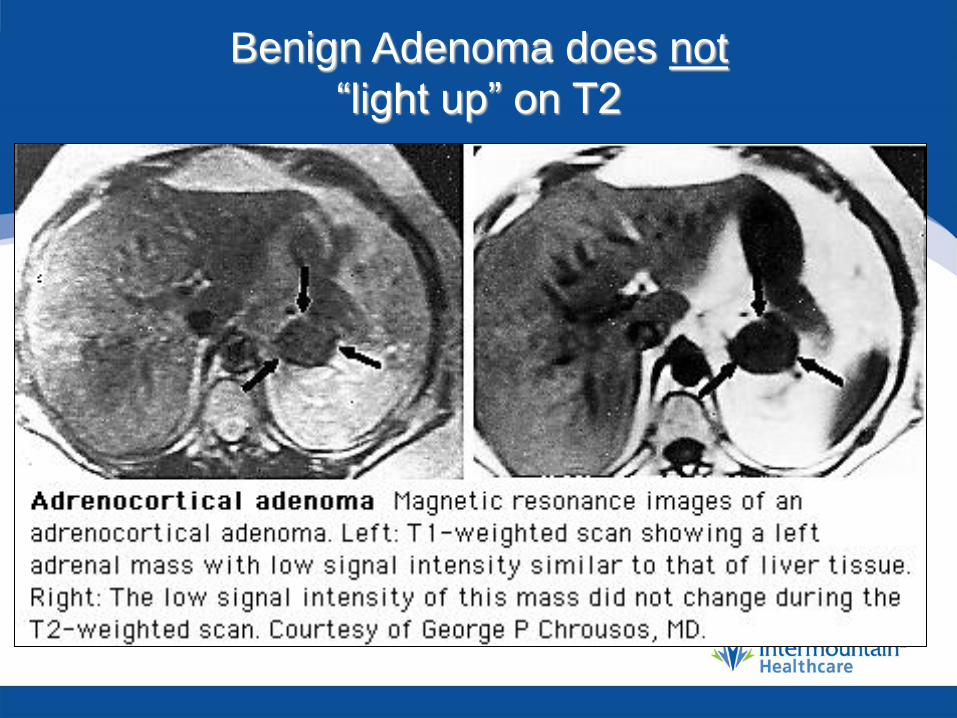
Benign Adenoma does not
“light up” on T2
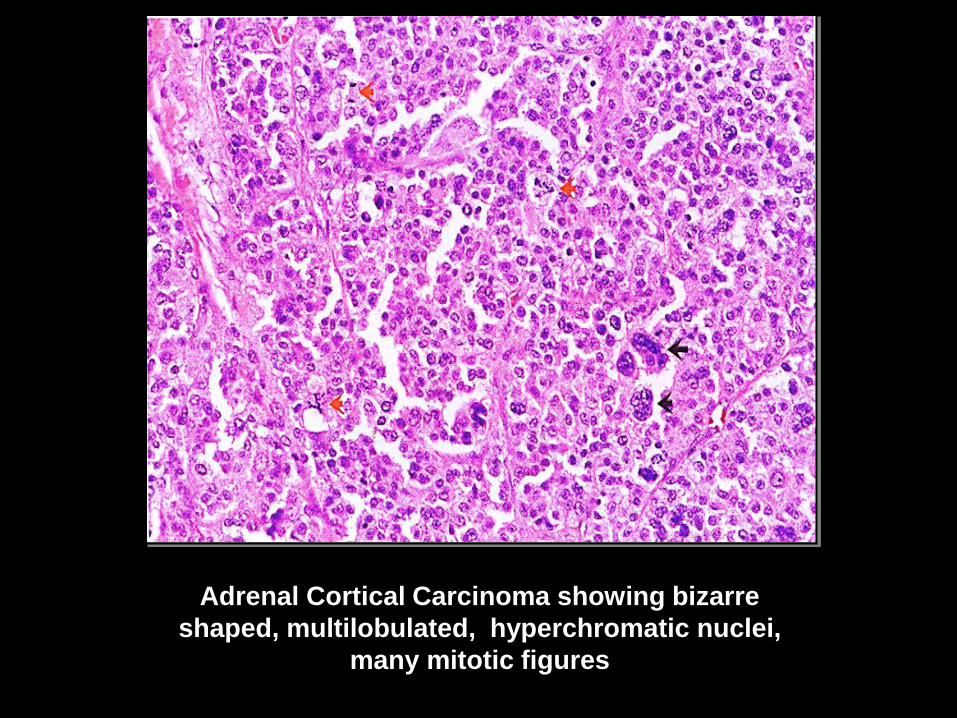
Adrenal Cortical Carcinoma showing bizarre
shaped, multilobulated, hyperchromatic nuclei,
many mitotic figures

Staging • Common Sites of Metastases
Lung
Liver
Lymph nodes
• Staging Studies
CXR
CBC, complete serum chemistry
CT and venogram versus MRI
Adrenal Cortical Carcinoma

Management • Surgery is mainstay
• 5-year survival clinically localized disease 35% • 5-year survival for pathologically confined disease 50%
• Frequently Invading Into Adjacent Structures • Radical en-bloc adrenalectomy with regional
lymphadenectomy and total or subtotal excision of adjacent organs (kidney, spleen, liver, colon, pancreas)
• May require cavotomy, bypass, etc
Adrenal Cortical Carcinoma

Management • Metastatic or Recurrent Disease
Mitotane (o,p’-DDD, a cogener of DDT)
Hormonal response in 75%
Response of tumor mass in 35%
No improvement in survival
(6.5 months median survival)
Severe toxicity
Trials of adjunctive use of mitotane
Adrenal Cortical Carcinoma
Adrenal Metastasis
Adrenal Metastasis • More common than adrenal cortical carcinoma
• 40 - 50% of metastases from:
Melanoma Breast
Lung Kidney
• 8 - 38% of patients with extra-adrenal malignancy will have adrenal metastases at autopsy
• With Known Primary Cancer
adrenal mass is metastasis in 32 – 73 (~50) %
Adrenal Metastasis
Diagnosis • In setting of widespread metastases (most common),
diagnosis obvious
• If no other metastases, do work-up as for adrenal incidentaloma (see below), even with known primary cancer
• Findings suggestive of metastases
No endocrine abnormalities
Irregular / inhomogeneous on CT, bright on T2 images of MRI, cold spot on NP-59 scintigraphy
Diagnosis
• Adrenal metastasis is the best indication for FNA of adrenal gland
• FNA cannot reliably distinguish
adrenal adenoma vs
adrenal cortical carcinoma
• Must rule out pheochromocytoma biochemically before attempting FNA
Adrenal Metastasis

CT-guided FNA of Adrenal Gland
Management • Solitary Metastasis : May be benefit to
adrenalectomy
• Decision in concert with oncologist
• Avoid direct gland manipulation Hemorrhage Tumor Spillage
• Take generous peri-adrenal tissue, but resection into other organs should not be necessary
Adrenal Metastasis
Adrenalectomy
Principles of Adrenalectomy
• Division Adrenal Vein
Most important step = pheochromocytoma
• “Dissect Patient Away From Gland”
• Traction on Adjacent Tissues
• For Open Surgery:
Divide superior and lateral attachments
Allow gland to retracted into operative field
Adrenalectomy
Cortical Carcinoma • Still a Laparoscopic Case • Consider open surgery
• large tumors • High suspicion for invasion • Be prepared for adjacent organ removal
Spleen Kidney Vena Cava Portion of Liver
• This is the model for invasive cancers!
Adrenalectomy
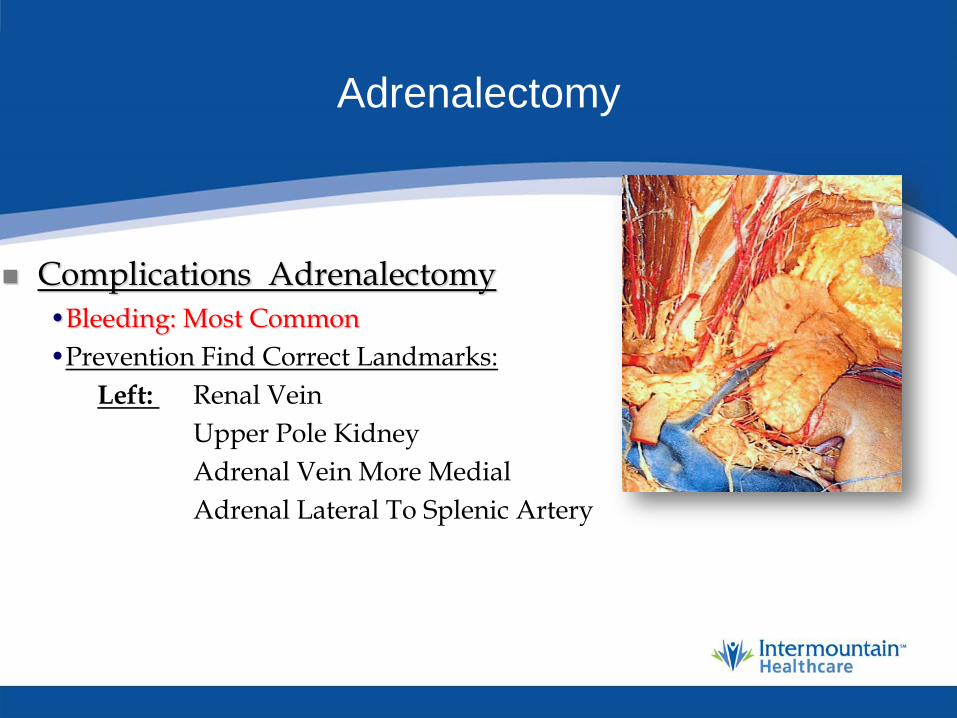
Complications Adrenalectomy
•Bleeding: Most Common
•Prevention Find Correct Landmarks:
Left: Renal Vein
Upper Pole Kidney
Adrenal Vein More Medial
Adrenal Lateral To Splenic Artery

Adrenalectomy
Complications Adrenalectomy
•Bleeding: Most Common
•Prevention Find Correct Landmarks:
Right: Vena Cava
Renal Vein
Adrenal Vein More Superior
•Avoid Hunting Through Fat!!
•Use LigaSure and or Harmonic Scalpel
Adrenalectomy
Complications Adrenalectomy
•Bleeding: Most Common
•Endocrine Imbalance
•Liver or Spleen Laceration
•Pneumothoax Trocar Placement
Diaphram Injury
Adrenal Gland
Take Home Messages Do the limited work up
Follow the patient
Treat surgical lesions laparoscopically
When you go Be Prepared !
Treat with Respect
Pheochromocytoma
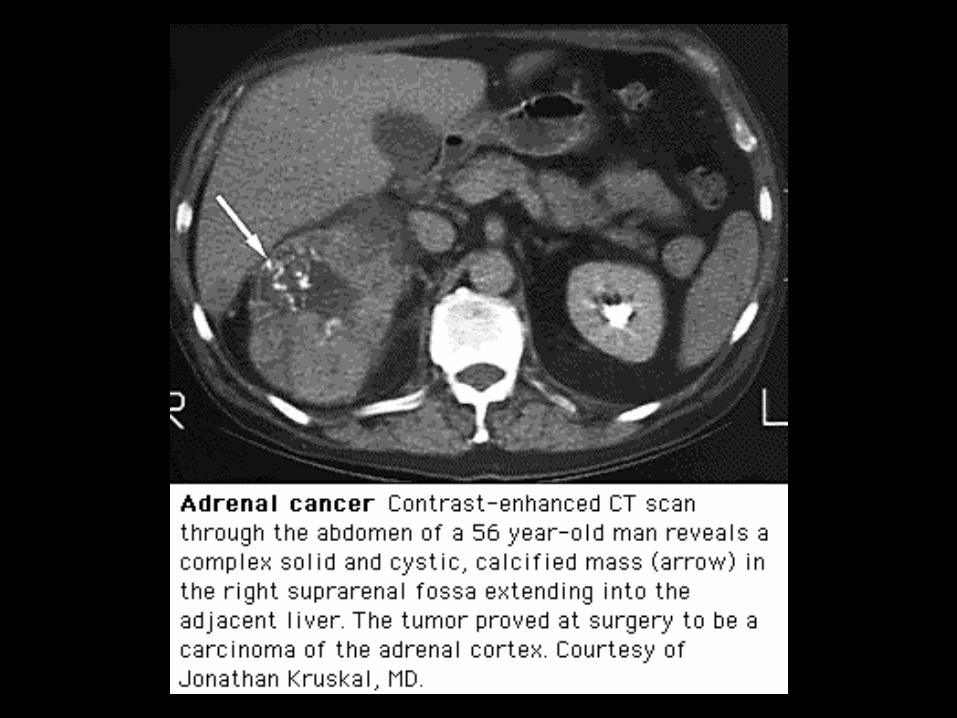
Adrenal Carcinoma
![Adrenal Imaging - University of Floridaxray.ufl.edu/files/2010/02/Adrenal-Imaging.pdfadrenal glands [3], and a metastasis might ... CT, adrenal imaging, adrenal lymphoma imaging, adrenal](https://static.documents.pub/doc/80x56/5b26814c7f8b9a8c0f8b4820/adrenal-imaging-university-of-glands-3-and-a-metastasis-might-ct-adrenal.jpg)




![Review Article Adrenal Tumors with Unexpected Outcome: A ...adrenal mass, even in absence of clinical signs of Cush-ing s syndrome or pheochromocytoma [ , , , ]. Also, clinicians should](https://static.documents.pub/doc/80x56/60f8675ba943c364ae34ff3c/review-article-adrenal-tumors-with-unexpected-outcome-a-adrenal-mass-even.jpg)











