Trauma Services FISCAL YEAR STATISTICS 2005 ANNUAL REPORT. The Medical Center of Louisiana is a member of the LSU Health Sciences Center – Health Care Services Division, and is affiliated with LSU and Tulane Schools of Medicine. Table of Contents. 2. - PowerPoint PPT Presentation
The Medical Center of Louisiana is a member of the LSU Health Sciences Center – Health Care Services Division, and is affiliated with LSU and Tulane Schools of Medicine. Trauma Services FISCAL YEAR STATISTICS 2005 ANNUAL REPORT
Transcript
The Medical Center of Louisiana is a member of the LSU Health Sciences Center – Health Care
Services Division, and is affiliated with LSU and Tulane Schools of Medicine.
Trauma ServicesFISCAL YEAR STATISTICS
2005ANNUAL REPORT
Table of Contents
2
I. Introduction Trauma Program Representatives ..........................................3 Trauma Program Overview....................................................4
II. 2005 Fiscal Year Report – Patient Statistics Patient Demographics ............................................................9 Fatal Trauma ..........................................................................10 Parish of Injury Vs. Residence...............................................11 Patient Triage Summary ........................................................12 Mechanism of Injury..............................................................13 Severity of Injury ...................................................................14 Patient Transportation ............................................................15 Injury Severity Score (ISS) by Mechanism of Injury ...........16 Etiology By Intent..................................................................17 Intentional Injuries .................................................................18 Trauma Activation Levels by Injury Severity Score .............19 Vehicular Trauma ..................................................................20 Emergency Center Trauma Admissions by Day Of Week ....21 Emergency Center Trauma Admissions by Shift...................22 Emergency Center Major Trauma Patient Turnaround Time.23
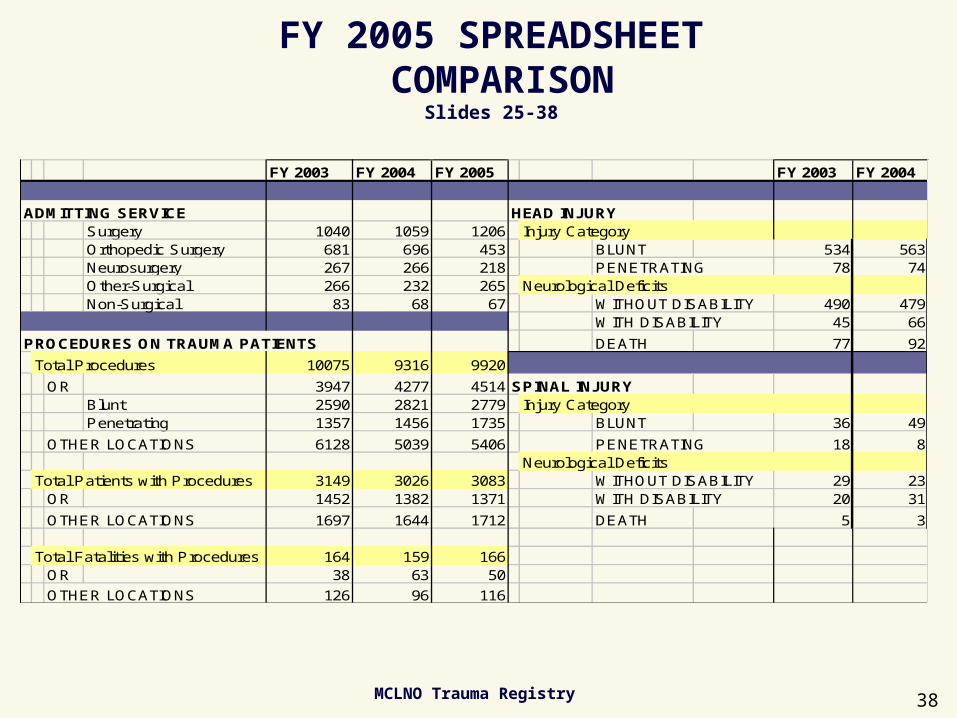
Emergency Department Disposition ......................................24 Admitting Service ..................................................................25 Procedures on Trauma Patients..............................................26 Head Injury ............................................................................27 Spinal Injury...........................................................................28 Hospital Discharge Disposition .............................................29 Eye & Organ Procurement.....................................................30 Drug & Alcohol Results for Trauma Activations ..................31 Reimbursement Summary......................................................32 FY 2003 Spreadsheet Comparison
Trauma is endemic in young Afro-American males in Orleans Parish. These data mirror national data which demonstrate that trauma is a disease of young people
and the #1 cause of death in people less than age 44.
(Pediatrics: 0-12; Adults: 13-64; Elderly 65+)
FY 2005
MCLNO Trauma Registry 9
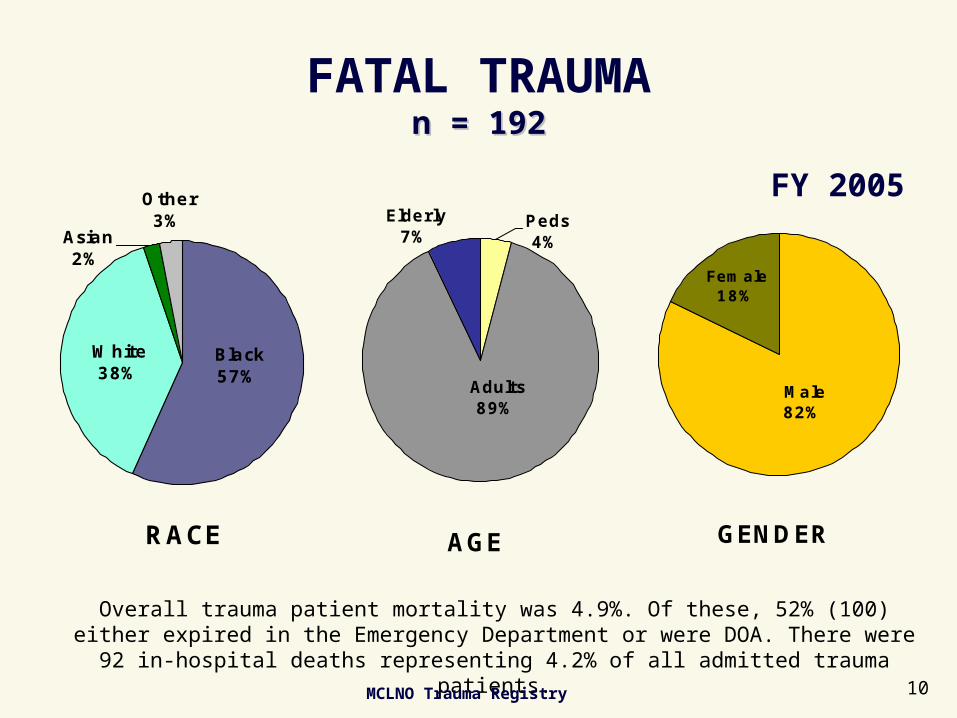
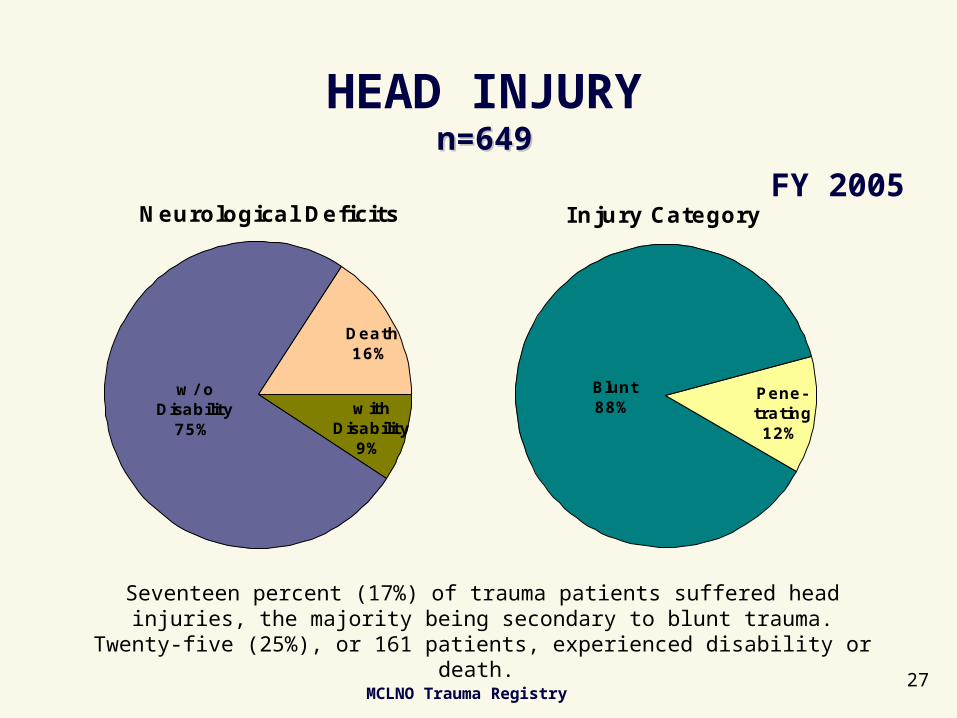
FATAL TRAUMAn = 192n = 192
RACE
White38%
Black57%
Asian2%
Other3%
AGE
Elderly7%
Peds4%
Adults89%
GENDER
Female18%
Male82%
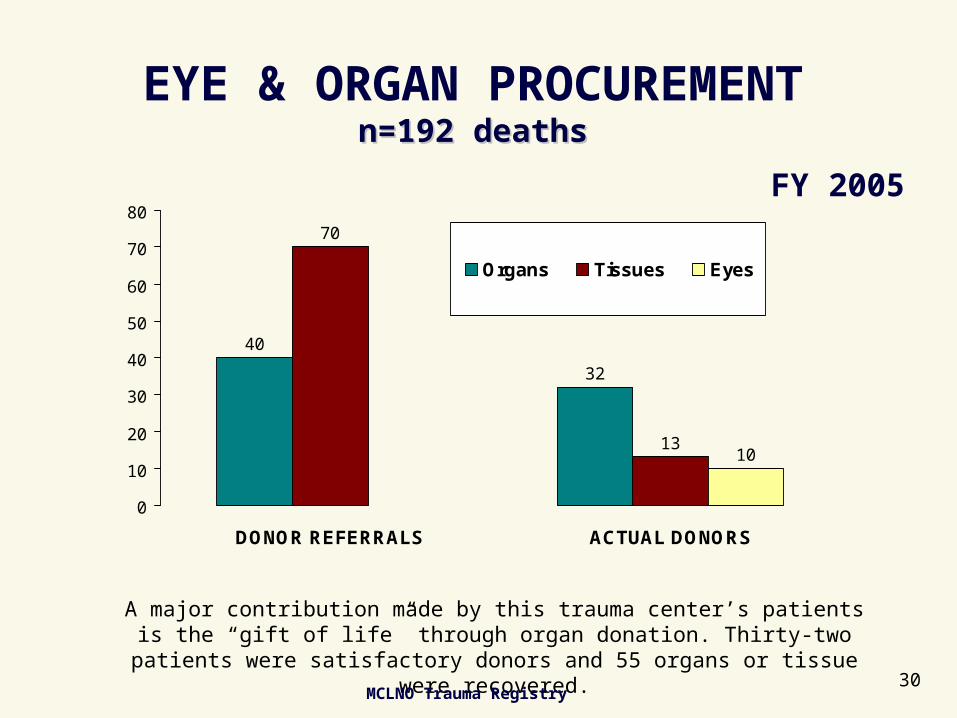
Overall trauma patient mortality was 4.9%. Of these, 52% (100) either expired in the Emergency Department or were DOA. There were 92 in-hospital deaths
representing 4.2% of all admitted trauma patients.
FY 2005
MCLNO Trauma Registry 10
PARISH OF INJURY vs. RESIDENCEn=3907n=3907
46% of patients treated were residents of parishes other than Orleans. Patients who were known to be injured in outside parishes accounted for 10% of all evaluations
and/or admissions. The actual number increased from 417 last year to 585 this year. This increase is the result of recent contractual agreements with outside parishes.
Parish of I njury
Plaque-mines1%
Unknown32%
Other3%Wash./ St.
Tamm2%
Saint Bernard
1%
J efferson8%
Orleans53%
Parish of Residence
Plaque-mines1%
Unknown1%
Out of State3%
Wash./ St. Tamm
5%
Other14%
St. Bernard4%J efferson
16%
Orleans56%
FY 2005
MCLNO Trauma Registry 11
PATIENT TRIAGE SUMMARYn=2092n=2092
True +43%
False +39%
False -13%
True -5%
True + {Predicted Major Trauma/Actual Major Trauma
OVERTRIAGE=False + {Predicted Major Trauma/Actual Non-Major Trauma
UNDERTRIAGE=False – {Predicted Non-Major Trauma/Actual Major Trauma
FY 2005
MCLNO Trauma Registry12
MECHANISM OF INJURYn=3907n=3907
Blunt71%
Burn1%
Penetrating28%
Blunt trauma accounts for 71% of all trauma cases seen by this facility, which is designated as the official Orleans Parish Trauma Center. Penetrating trauma
accounts for 28% which has increased by 5% since FY 2004.
FY 2005
MCLNO Trauma Registry13
SEVERITY OF INJURYn=3907n=3907
Major & Non-Fatal
50%
Major & Fatal5%
Minor45%
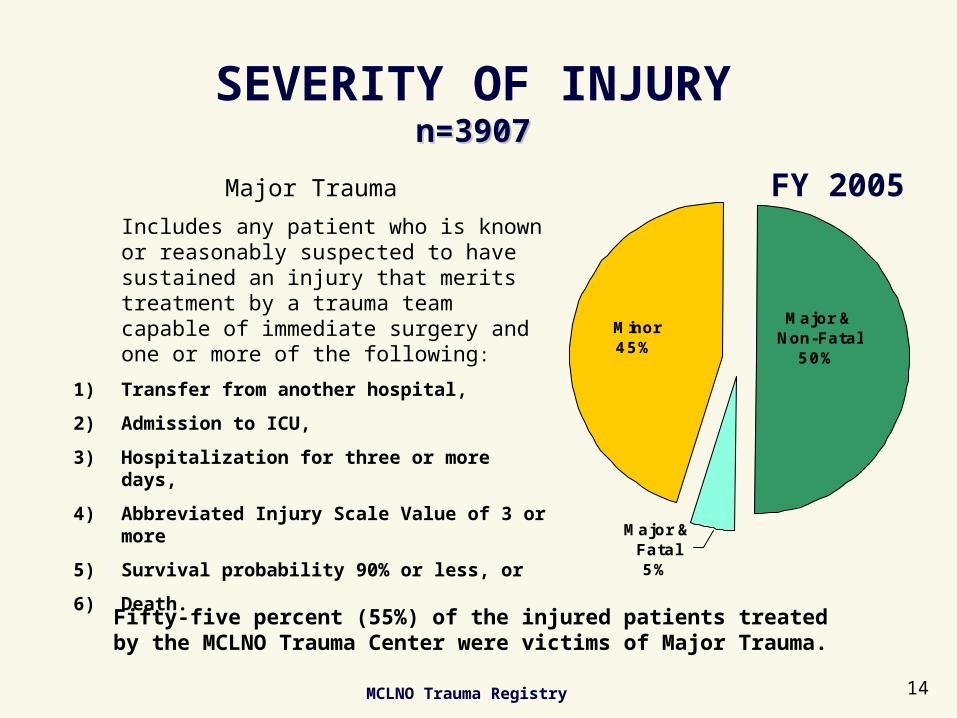
Fifty-five percent (55%) of the injured patients treated by the MCLNO Trauma Center were victims of Major Trauma.
Major Trauma
Includes any patient who is known or reasonably suspected to have sustained an injury that merits treatment by a trauma team capable of immediate surgery and one or more of the following:
1) Transfer from another hospital,
2) Admission to ICU,
3) Hospitalization for three or more days,
4) Abbreviated Injury Scale Value of 3 or more
5) Survival probability 90% or less, or
6) Death.
FY 2005
MCLNO Trauma Registry 14
PATIENT TRANSPORTATIONn=3907n=3907
OverallTransports
Inter-hospitaln=57615%
Pre-hospitaln=2623
67%
Self13%
Police3%
Other2%
PrehospitalTransport
West Jeff6%
Guardian1%
Other EMS 6%
East J eff5%
Acadian5%
NOHD72%
Lifeguard2%
Air3%
I nterhospitalTransport
NOHD9%
Other EMS21%
AMR1%
EmergyStat4%
Air EMS11%
AMED2%Acadian
EMS52%
Seventy-nine percent (79%) of patients transported were brought to MCLNO via an ambulance. The New Orleans Health Department ambulance service, was
responsible for 72% of the pre-hospital care.
FY 2005
MCLNO Trauma Registry15
INJURY SEVERITY SCORE (ISS)BY MECHANISM OF INJURY
n=1500n=1500**
167
86
118
149
278
167
665454
48
159154
0
50
100
150
200
250
300
ISS 1-5 ISS 6-10 ISS 11-15 ISS 16-20 ISS 21-25 ISS >25
# o
f P
ati
en
ts in
Th
ou
sa
nd
s
BLUNT
PEN
The injury severity score (ISS) is a way of assigning severity of injury numerically for standardization and outcome prediction. ISS is related linearly with mortality, and an ISS >= 15 is considered major trauma.
*Activated Patients who were either
admitted or died in the ED.
FY 2005
MCLNO Trauma Registry 16
ETIOLOGY BY INTENTn=3907n=3907
Accidental66%Assault
31%
Undetermined2%
Self-Inflicted1%
Thirty-one percent (31%) of all patients seen and treated were victims of intentional assault. Violence prevention remains a top priority of the Trauma
Center’s Outreach and Community Activity Program.
FY 2005
MCLNO Trauma Registry17
INTENTIONAL INJURIESn=1296n=1296
Stab24%
Other25%
Firearm48%
Self-inflicted3%
vs. Another97%
Where the data are known, 97% of intentional injuries were the result of an assault and 3% were self inflicted. Gunshot and stabbings continue to be the
major cause of intentional injuries.
FY 2005
MCLNO Trauma Registry 18
TRAUMA ACTIVATION LEVELSBY INJURY SEVERITY SCORE
n=1502n=1502**
Injury Severity Score
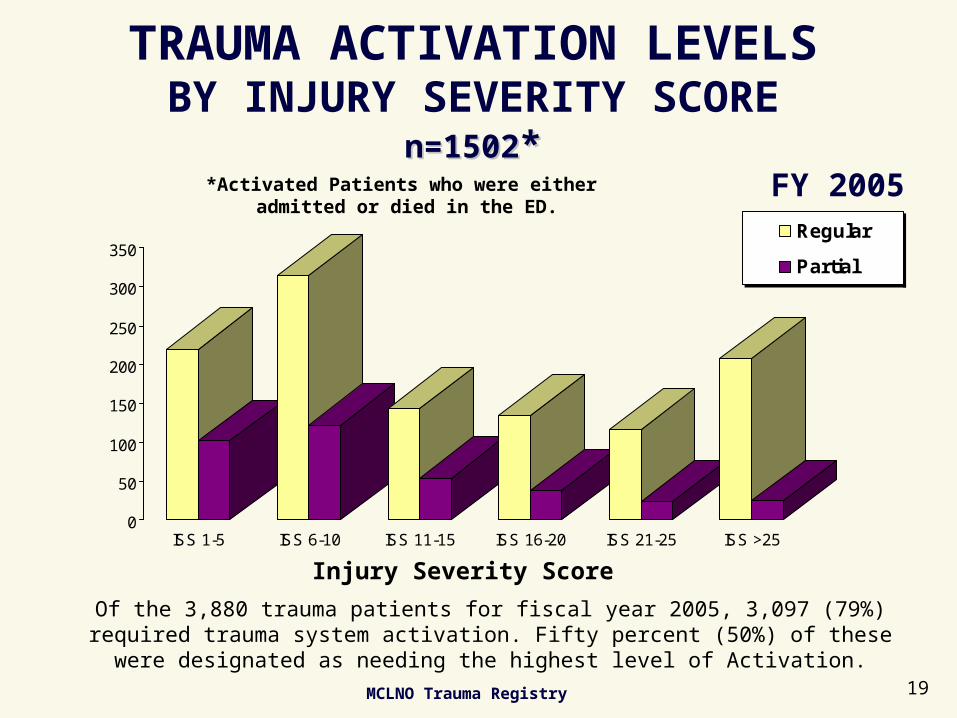
Of the 3,880 trauma patients for fiscal year 2005, 3,097 (79%) required trauma system activation. Fifty percent (50%) of these were designated as needing the
highest level of Activation.
0
50
100
150
200
250
300
350
ISS 1-5 ISS 6-10 ISS 11-15 ISS 16-20 ISS 21-25 ISS >25
Regular
Partial
*Activated Patients who were either admitted or died in the ED.
FY 2005
MCLNO Trauma Registry 19
VEHICULAR TRAUMA
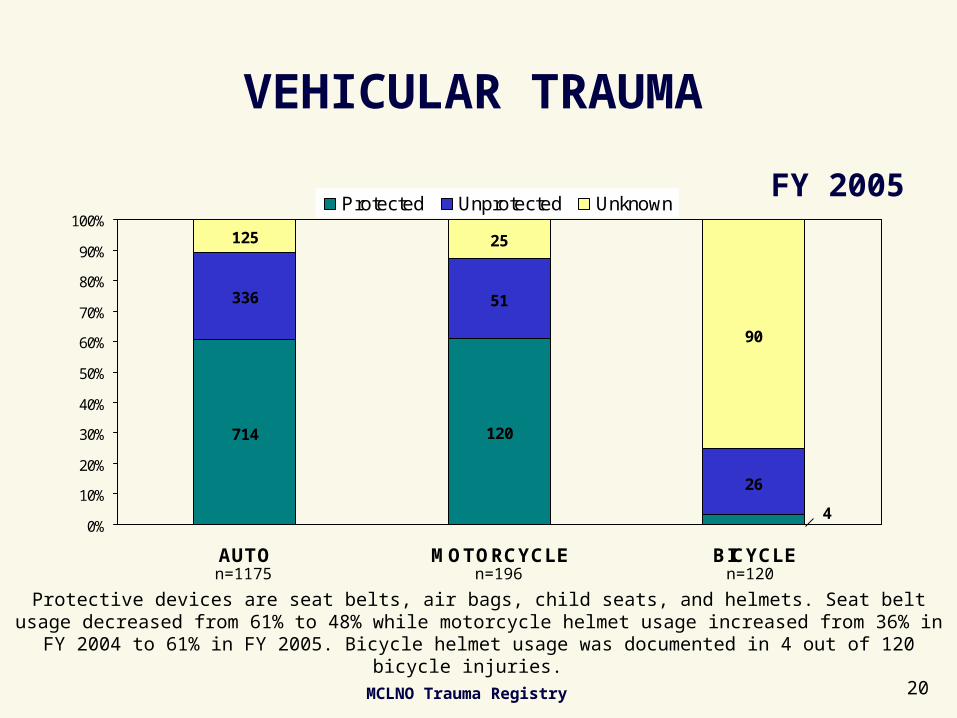
Protective devices are seat belts, air bags, child seats, and helmets. Seat belt usage decreased from 61% to 48% while motorcycle helmet usage increased from 36% in FY 2004 to 61% in FY
2005. Bicycle helmet usage was documented in 4 out of 120 bicycle injuries.
714 120
336 51
26
125 25
90
40%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
AUTO MOTORCYCLE BICYCLE
Protected Unprotected Unknown
n=1175 n=196 n=120
FY 2005
MCLNO Trauma Registry 20
EMERGENCY CENTER TRAUMA ADMISSIONSby Day of Week
n=3907n=3907
692
548490
528484
539
626
0
100
200
300
400
500
600
700
SUN MON TUE WED THU FRI SAT
DAY
Weekends remain the most active period, with Saturday, Sunday, and Monday accounting for 48% of the total weekly admissions. (Day
is 0800 to 0759.)
FY 2005
MCLNO Trauma Registry 21
EMERGENCY CENTER TRAUMA ADMISSIONSby Shiftn=3512n=3512
982
1603
1140
0
200
400
600
800
1000
1200
1400
1600
1800
0801 - 1600 1601 - 2400 0001 - 0800
SHIFT
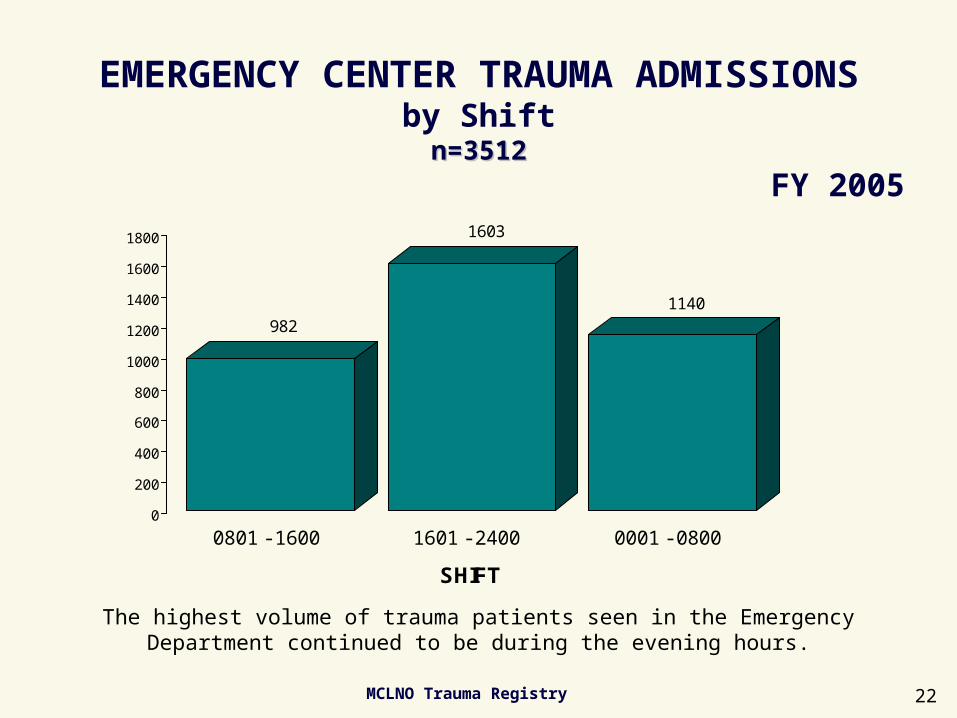
The highest volume of trauma patients seen in the Emergency Department continued to be during the evening hours.
FY 2005
MCLNO Trauma Registry 22
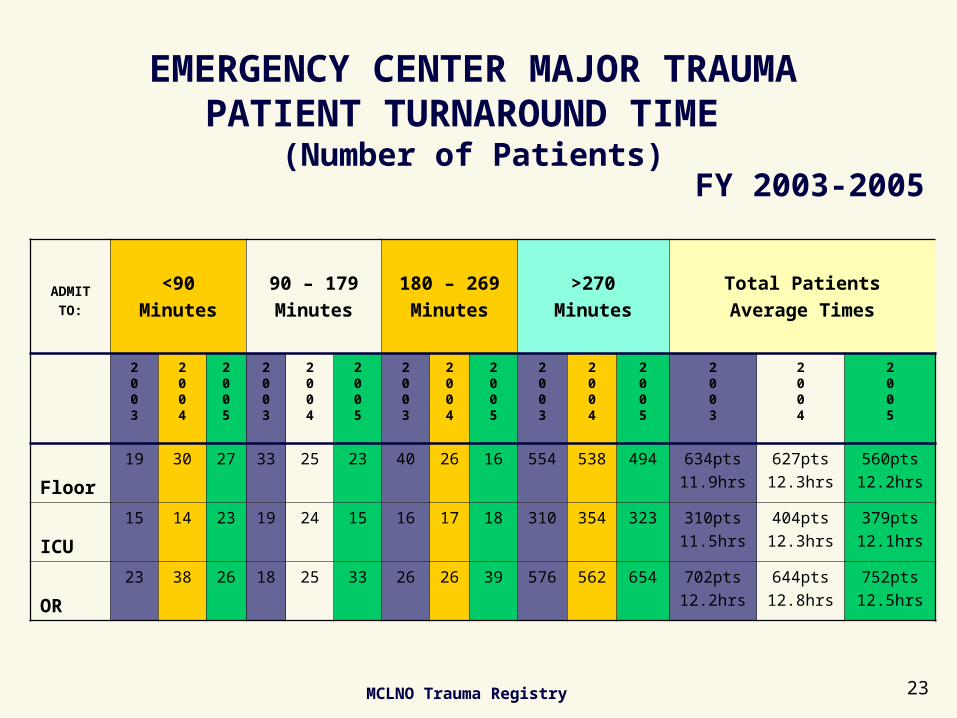
EMERGENCY CENTER MAJOR TRAUMAPATIENT TURNAROUND TIME
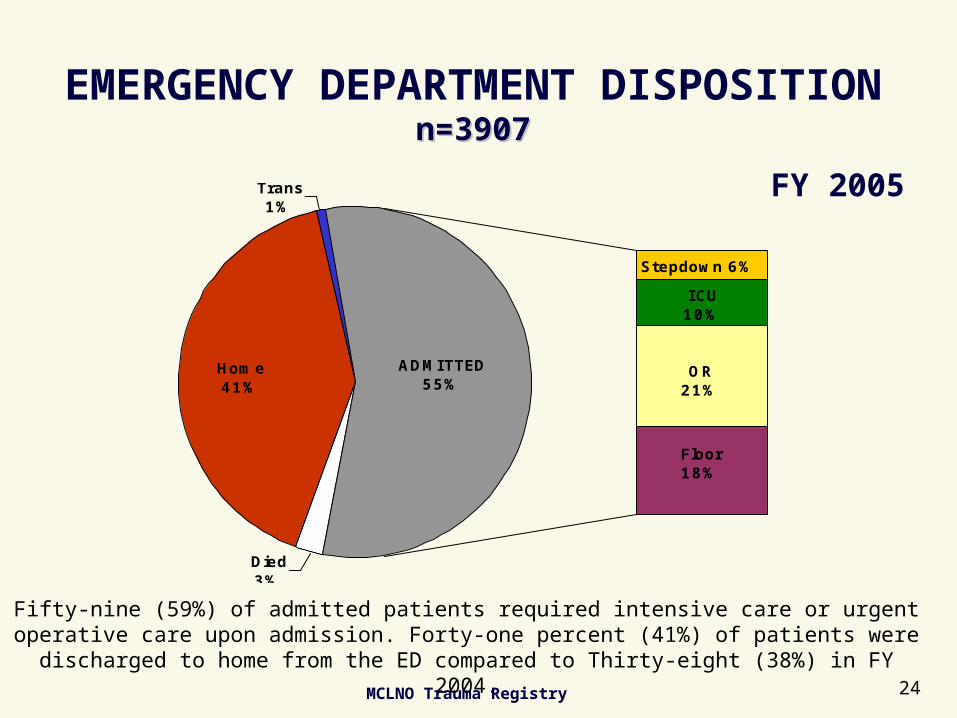
Fifty-nine (59%) of admitted patients required intensive care or urgent operative care upon admission. Forty-one percent (41%) of patients were discharged to home from
the ED compared to Thirty-eight (38%) in FY 2004.
FY 2005
MCLNO Trauma Registry 24
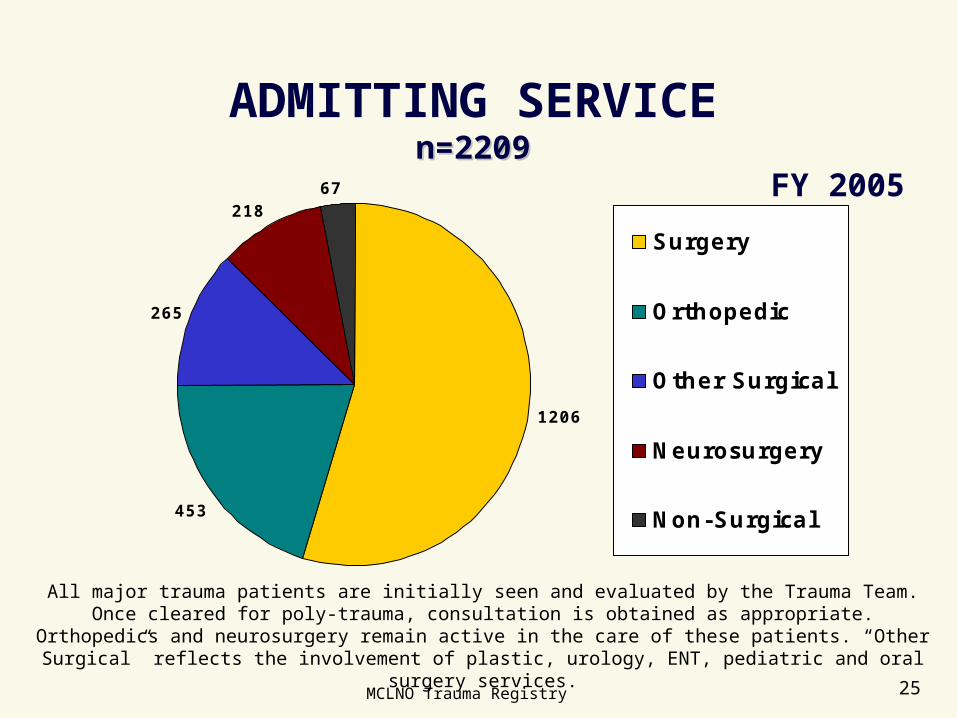
ADMITTING SERVICEn=2209n=2209
1206
453
265
21867
Surgery
Orthopedic
Other Surgical
Neurosurgery
Non-Surgical
All major trauma patients are initially seen and evaluated by the Trauma Team. Once cleared for poly-trauma, consultation is obtained as appropriate. Orthopedics and neurosurgery remain
active in the care of these patients. “Other Surgical” reflects the involvement of plastic, urology, ENT, pediatric and oral surgery services.
FY 2005
MCLNO Trauma Registry 25
PROCEDURES ON TRAUMA PATIENTS
Number of ProceduresN=932
Number of ProceduresN=9,920
Total Patients(with Procedures)
n=3,083
O.R.44%
Other Loca-tions56%
Total Fatalities(with Procedures)
n=166
O.R.43%Other
Loca-tions57% Total Procedures
n=9,920
OR-Blunt28%
Other Locations
54%OR-
Penetrating18%
OR46%
There were 9,920 total procedures performed on 3,083 patients (79% of all trauma patients).