Vol. 324 No. 6 ADVERSE EVENTS IN HOSPITALIZED PATIENTS - LEAPE ET AL. 377
THE NATURE OF ADVERSE EVENTS IN HOSPITALIZED PATIENTS
Results of the Harvard Medical Practice Study II
LUCIAN L. LEAPE, M.D., TROYEN A. BRENNAN, M.D., J.D., M.P.H., NAN LAIRD, PH.D.,ANN G. LAWTHERS, Sc.D., A. RUSSELL LOCALIO, J.D., M.P.H., BENIAMIN A. BARNES, M.D.,
LIESI HEBERT, Sc.D., JOSEPH P. NEWHOUSE, PH.D., PAUL C. WEILER, LL.M., AND HOWARD HIATT, M.D.
Abstract Background. In a sample of 30,195 randomlyselected hospital records, we identified 1 133 patients (3.7percent) with disabling injuries caused by medical treat-ment. We report here an analysis of these adverse eventsand their relation to error, negligence, and disability.Methods. Two physician-reviewers independently
identified the adverse events and evaluated them with re-spect to negligence, errors in management, and extent ofdisability. One of the authors classified each event accord-ing to type of injury. We tested the significance of differ-ences in rates of negligence and disability among catego-ries with at least 30 adverse events.
Results. Drug complications were the most commontype of adverse event (19 percent), followed by woundinfections (14 percent) and technical complications (13percent). Nearly half the adverse events (48 percent) wereassociated with an operation. Adverse events during sur-
IN recent years, concern about the increasing cost ofmalpractice-insurance premiums has led to nu-
merous tort reforms. At the same time, and largelyindependently of tort reform, interest in initiatives af-fecting the quality of care has grown. Curiously, how-ever, the problem of medical injury has received com-paratively little attention from either perspective. Butan important objective for those concerned with bothmedical malpractice and quality of care is the preven-tion of iatrogenic injury. A first step in prevention is todevelop a better understanding of the types of suchinjuries and their causes.
In our investigation of accidental injury in patientshospitalized in 1984 in the state of New York, wefound that 3.7 percent of patients had injuries andthat negligent care was responsible for 28 percent ofthem.' In this report we analyze these injuries, includ-ing the types of adverse events, the types most likely toresult in serious disability, the types most likely tobe caused by negligence, the effects of various riskfactors, and the management errors that were respon-sible. Finally, we develop a conceptual framework en-compassing notions of negligence, error, and prevent-ability in an effort to understand iatrogenic injurybetter.
METHODSThe study design, sampling plan, and record-review process have
been described elsewhere.2 In brief, we evaluated 30,195 randomlyselected records in 51 hospitals in the state of New York, using a
From the Departments of Health Policy and Management (L.L.L., A.G.L.,A.R.L., B.A.B., L.H., J.P.N., H.H.) and Biostatistics (N.L.), Harvard Schoolof Public Health; the Department of Medicine, Brigham and Women's Hospital(T.A.B., H.H.); and Harvard Medical School (T.A.B., J.P.N.), all in Boston;and Harvard Law School, Cambridge, Mass. (P.C.W.). Address reprint requeststo Dr. Leape at the Harvard School of Public Health, 677 Huntington Ave.,Boston, MA 02115.
Supported by grants from the New York Department of Health and the RobertWood Johnson Foundation.
gery were less likely to be caused by negligence (17 per-cent) than nonsurgical ones (37 percent). The proportionof adverse events due to negligence was highest fordiagnostic mishaps (75 percent), noninvasive therapeuticmishaps ("errors of omission") (77 percent), and eventsoccurring in the emergency room (70 percent). Errors inmanagement were identified for 58 percent of the adverseevents, among which nearly half were attributed to negli-gence.
Conclusions. Although the prevention of many ad-verse events must await improvements in medical knowl-edge, the high proportion that are due to managementerrors suggests that many others are potentially prevent-able now. Reducing the incidence of these events will re-quire identifying their causes and developing methods toprevent error or reduce its effects. (N EngI J Med 1991;324:377-84.)
two-stage process. All records were screened by trained nurses ormedical-records administrators using 18 screening criteria. Recordsthat met any of our criteria were then reviewed independently bytwo physicians who identified adverse events and instances of negli-gence. We defined an adverse event as an unintended injury thatwas caused by medical management and that resulted in measur-able disability. Negligence was defined as failure to meet the stand-ard of care reasonably expected of an average physician qualified totake care of the patient in question.We asked the reviewers to describe each adverse event and its
relation to medical care and to estimate the degree of disability thatresulted. Disability was rated on a six-point scale' on which "seri-ous" disability was defined as that persisting for more than sixmonths (a score above 2 on the 6-point scale). When the two physi-cians disagreed, we randomly selected one of their two reviews inorder to assign a single disability score to each patient. (The review-ers disagreed in 4 percent of the cases about whether the disabilityscore was greater than 2.) The reviewers also identified the siteinside or outside the hospital where the treatment that had causedthe adverse event had taken place. In addition, the reviewers wereasked to indicate whether each adverse event could have beencaused by a reasonably avoidable error, defined as a mistake inperformance or thought. If so, they classified the error, and if morethan one class of error was found, they ranked the errors in order ofseriousness. They then indicated the specific type of error within theclass. Finally, the reviewers determined whether there had beennegligence after they considered and recorded whether there hadbeen deviation from accepted norms of treatment, the potential (notactual) consequences of the negligence, the frequency of risk, thedegree of emergency, the complexity of the case, the presence ofany coexisting conditions, and the extent to which there was a con-sensus about the correct therapy or diagnosis for a given situation.If they found negligence, they rated its severity on a three-pointscale on which 1 indicated a slight degree of negligence, 2 a moder-ate degree, and 3 a grave degree.Each adverse event was subsequently classified with regard to
type of injury by one of the authors after reading the descriptions ofeach case prepared by both physician-reviewers. An adverse eventwas considered an operative complication if it occurred withinthe first two weeks after surgery or if it was thought to havebeen caused by the operation, regardless of when it occurred. Oper-ative complications were subclassified as technical (e.g., injury oc-curring during an operation, bleeding, or difficulty with woundhealing), nontechnical (e.g., pulmonary embolism, myocardial in-farction, and pneumonia), related to wound infections, caused
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.
by surgical failure (to cure, relieve, or prevent symptoms, such aspregnancy after tubal ligation), or late (bad results and delayedcomplications).
Nonoperative categories of injuries included those that were re-lated to a procedure (which were further classified in the samemanner as the operative complications), diagnostic mishaps (in-juries that resulted from an improper or delayed diagnosis), thera-peutic mishaps (injuries resulting from complications of noninva-sive therapy), and those related to drugs. The last were treatedseparately because of the number and importance of drug reac-tions. We also established separate categories for fractures, injuriesrelated to anesthesia, postpartum injuries, and neonatal injuries,because of the unique nature of the adverse events in these groups.Because we were concerned about all types of adverse events inhospitalized patients, not only those caused by physicians, we alsoestablished separate categories to include falls and system errors,two categories of adverse events that may be more likely to becaused by nursing or support personnel.We oversampled patients in several high-risk, low-volume spe-
cialties, such as neurosurgery and vascular surgery, to ensure thatthere were adequate numbers in each category of injury. To projectthe numbers in the sample to those of the entire population, we usedweights for all our analyses. Thus, the percentages given do notcorrespond directly to the numbers in the sample. The final deter-mination of the occurrence of an adverse event or case of negligencewas based on a calculation of the average of the two reviewers'scores.The significance of the differences in the rates of negligence and
disability between categories of adverse events and locations wastested for the categories in which there were at least 30 adverseevents. Standard errors were computed for the difference betweenthe rate of negligence or disability in the category studied and thatin all other categories combined, with use of the SESUDAAN pack-age of the Research Triangle Institute3 to adjust for the complexsample design and the Bonferroni procedure for simultaneous infer-ences.4
RESULTS
Adverse Events
As reported elsewhere, we identified 1133 adverseevents in our sample of records for 30,195 patientshospitalized in New York in 1984.1 Table 1 lists thedistribution of the kinds of adverse events and negli-gence-related adverse events we discovered. Nearlyhalf the adverse events (48 percent) resulted from op-erations. Wound infections were the most commonsurgical adverse event, accounting for 29 percent ofsurgical complications and nearly one seventh of alladverse events identified in the study.Drug complications were the most common single
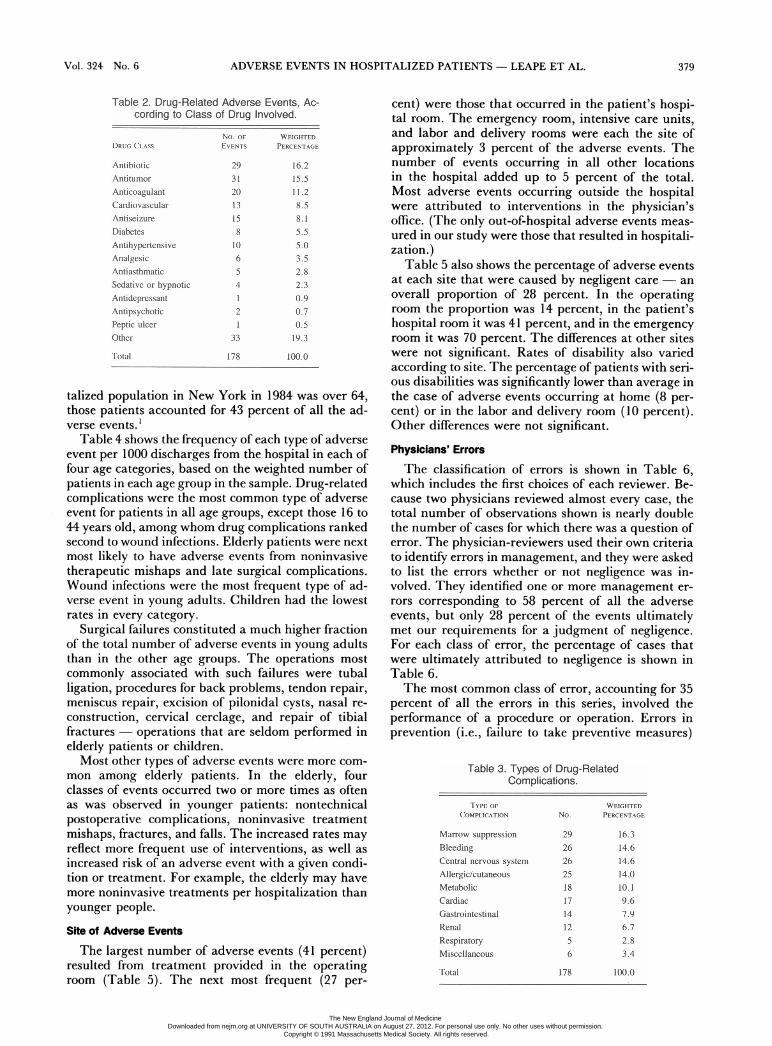
type of adverse event (19 percent). Table 2 lists theclasses of drugs responsible for adverse events in theorder of their frequency, and Table 3 shows the var-ious types of adverse events caused by drugs. Theseevents covered a broad spectrum, from those that wereunpredictable and unpreventable, such as allergic re-actions to drugs to which the patient had had noknown previous exposure, to those that might havebeen unavoidable, such as marrow depression fromantitumor drugs, to those that resulted from errors inadministration or monitoring, such as bleeding associ-ated with the use of anticoagulant agents.
Negligence
Overall, 28 percent of the adverse events werejudged to have resulted from negligent care, but therewas wide variation among categories (Table 1). Sev-
Table 1. Types of Adverse Events and Proportion of EventsInvolving Negligence.
*Dashes denote categones for which dtere were too few observations to deternine apercentage.
tP<0.001 for the difference between this rate and all others in the same column.tP<O.Ol for the difference between this rate and all odters in the same column.Includes nonoperative fractures only.11ncludes nonresarean deliveries only.
enteen percent of the adverse events related to oper-ations were due to negligence, ranging from 13 percentof the wound infections to 36 percent of the surgicalfailures (e.g., persistent back pain that responded to asecond operation to remove a disk that had been treat-ed inadequately in a previous laminectomy). Of theadverse events due to drug treatment, 18 percent re-sulted from negligence. By contrast, negligent carewas identified as causing 75 percent of the adverseevents due to problems in diagnosis (such as failure todiagnose an ectopic pregnancy) and 77 percent ofthose due to a therapeutic mishap (resulting fromnon-drug-related, noninvasive treatment).
Disability
The large majority of the adverse events did notresult in serious disability. More than half the patientshad minimal impairment, recovering completely in amonth or less. Seventy percent recovered completelyin less than six months.' Rates of serious disabilitywere significantly lower than average for technicalcomplications of surgery (12 percent) and drug-relat-ed adverse events (14 percent), and significantly high-er than average for diagnostic mishaps (47 percent)(Table 1).
Effects of AgeWe noted previously that patients over the age of 64
had adverse events and negligence-related adverseevents at rates more than double the rate of patientsunder 45, and although only 27 percent of the hospi-
378 Feb. 7, 1991
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.
ADVERSE EVENTS IN HOSPITALIZED PATIENTS - LEAPE ET AL.
No. oF WEGHTEDEVENTS PERCENTAGE
29
31
2013
158
1065
4
12
133
16.2
15.511.2
8.58.1
5.5
5.03.5
2.8
2.3
0.90.70.519.3
178 100.0
talized population in New York in 1984 was over 64,those patients accounted for 43 percent of all the ad-verse events.'
Table 4 shows the frequency of each type of adverseevent per 1000 discharges from the hospital in each offour age categories, based on the weighted number ofpatients in each age group in the sample. Drug-relatedcomplications were the most common type of adverseevent for patients in all age groups, except those 16 to44 years old, among whom drug complications rankedsecond to wound infections. Elderly patients were nextmost likely to have adverse events from noninvasivetherapeutic mishaps and late surgical complications.Wound infections were the most frequent type of ad-verse event in young adults. Children had the lowestrates in every category.
Surgical failures constituted a much higher fractionof the total number of adverse events in young adultsthan in the other age groups. The operations mostcommonly associated with such failures were tuballigation, procedures for back problems, tendon repair,meniscus repair, excision of pilonidal cysts, nasal re-
construction, cervical cerclage, and repair of tibialfractures operations that are seldom performed inelderly patients or children.Most other types of adverse events were more com-
mon among elderly patients. In the elderly, fourclasses of events occurred two or more times as oftenas was observed in younger patients: nontechnicalpostoperative complications, noninvasive treatmentmishaps, fractures, and falls. The increased rates mayreflect more frequent use of interventions, as well as
increased risk of an adverse event with a given condi-tion or treatment. For example, the elderly may havemore noninvasive treatments per hospitalization thanyounger people.
Site of Adverse Events
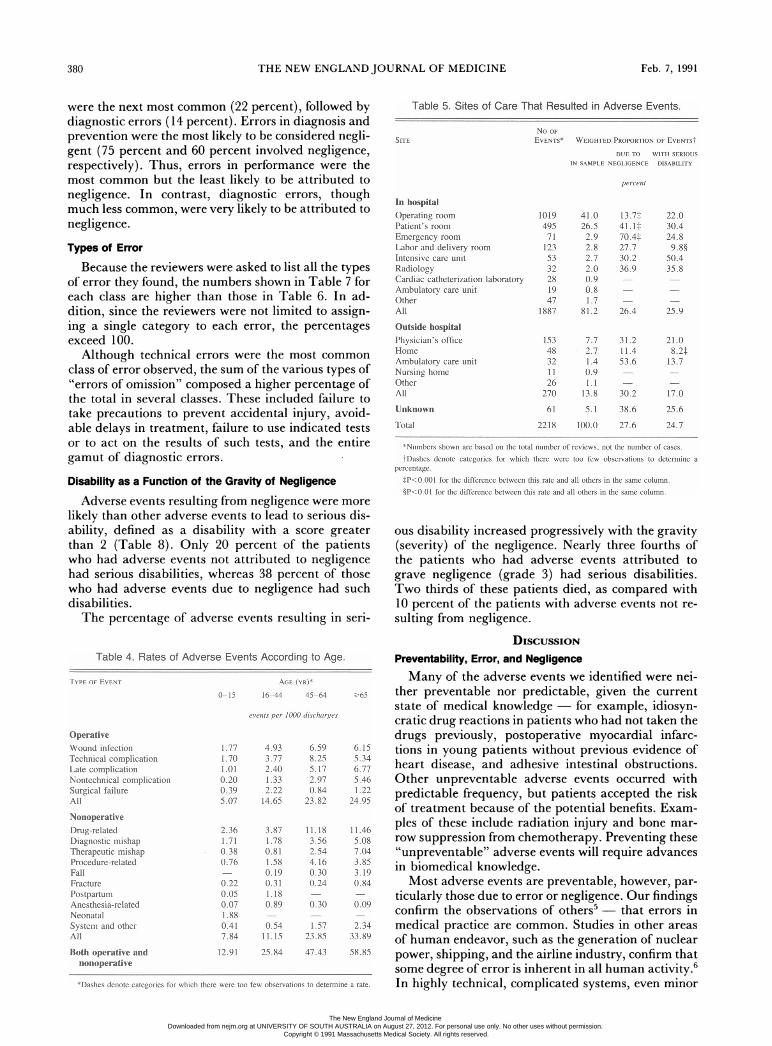
The largest number of adverse events (41 percent)resulted from treatment provided in the operatingroom (Table 5). The next most frequent (27 per-
cent) were those that occurred in the patient's hospi-tal room. The emergency room, intensive care units,and labor and delivery rooms were each the site ofapproximately 3 percent of the adverse events. Thenumber of events occurring in all other locationsin the hospital added up to 5 percent of the total.Most adverse events occurring outside the hospitalwere attributed to interventions in the physician'soffice. (The only out-of-hospital adverse events meas-ured in our study were those that resulted in hospitali-zation.)
Table 5 also shows the percentage of adverse eventsat each site that were caused by negligent care - anoverall proportion of 28 percent. In the operatingroom the proportion was 14 percent, in the patient'shospital room it was 41 percent, and in the emergencyroom it was 70 percent. The differences at other siteswere not significant. Rates of disability also variedaccording to site. The percentage of patients with seri-ous disabilities was significantly lower than average inthe case of adverse events occurring at home (8 per-cent) or in the labor and delivery room (10 percent).Other differences were not significant.
Physicians' Errors
The classification of errors is shown in Table 6,which includes the first choices of each reviewer. Be-cause two physicians reviewed almost every case, thetotal number of observations shown is nearly doublethe number of cases for which there was a question oferror. The physician-reviewers used their own criteriato identify errors in management, and they were askedto list the errors whether or not negligence was in-volved. They identified one or more management er-rors corresponding to 58 percent of all the adverseevents, but only 28 percent of the events ultimatelymet our requirements for a judgment of negligence.For each class of error, the percentage of cases thatwere ultimately attributed to negligence is shown inTable 6.The most common class of error, accounting for 35
percent of all the errors in this series, involved theperformance of a procedure or operation. Errors inprevention (i.e., failure to take preventive measures)
Table 2. Drug-Related Adverse Events, Ac-cording to Class of Drug Involved.
DRUG CLASS
AntibioticAntitumorAnticoagulantCardiovascularAntiseizureDiabetesAntihypertensiveAnalgesicAntiasthnaticSedative or hypnoticAntidepressantAntipsychoticPeptic ulcerOther
Total
Vol. 324 No. 6 379
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.
were the next most common (22 percent), followed bydiagnostic errors (14 percent). Errors in diagnosis andprevention were the most likely to be considered negli-gent (75 percent and 60 percent involved negligence,respectively). Thus, errors in performance were themost common but the least likely to be attributed tonegligence. In contrast, diagnostic errors, thoughmuch less common, were very likely to be attributed tonegligence.
Types of Error
Because the reviewers were asked to list all the typesof error they found, the numbers shown in Table 7 foreach class are higher than those in Table 6. In ad-dition, since the reviewers were not limited to assign-ing a single category to each error, the percentagesexceed 100.
Although technical errors were the most common
class of error observed, the sum of the various types of"errors of omission" composed a higher percentage ofthe total in several classes. These included failure totake precautions to prevent accidental injury, avoid-able delays in treatment, failure to use indicated testsor to act on the results of such tests, and the entiregamut of diagnostic errors.
Disability as a Function of the Gravity of Negligence
Adverse events resulting from negligence were more
likely than other adverse events to lead to serious dis-ability, defined as a disability with a score greaterthan 2 (Table 8). Only 20 percent of the patientswho had adverse events not attributed to negligencehad serious disabilities, whereas 38 percent of thosewho had adverse events due to negligence had suchdisabilities.The percentage of adverse events resulting in seri-
Table 4. Rates of Adverse Events According to Age.
NonoperativeDrug-relatedDiagnostic mishapTherapeutic mishapProcedure-relatedFallFracturePostpartumAnesthesia-relatedNeonatalSystem and otherAll
Both operative andnonoperative
1.771.701.010.200.395.07
2.361.710.380.76
0.220.050.071.880.417.84
12.91
4.933.772.401.332.2214.65
3.871.780.811.580.190.311.180.89
0.5411.15
25.84
6.598.255.172.970.84
23.82
11.183.562.544.160.300.24
0.30
1.5723.85
47.43
*Dashes denote categories for which there wer too few observations to detennine a rate.
Table 5. Sites of Care That Resulted in Adverse Events.
No OFEVENTS*SITE WEIGHTED PRoPORTIoN OF EvENTSt
DUE TO WITH SERIOUSIN SAMPLE NEGLIGENCE DISABILITY
percent
In hospital
Operating roomPatient's roomEmergency roomLabor and delivery room
Intensive care unitRadiologyCardiac catheterization laboratoryAmbulatory care unitOtherAll
Outside hospitalPhysician's officeHomeAmbulatory care unitNursing homeOtherAll
Unknown
Total
10194957112353322819
471887
15348321126
270
61
2218
41.026.52.92.82.72.00.90.81.7
81.2
7.72.71.40.91.1
13.8
5.1
100.0
13.7*41.1*70.4*27.730.236.9
26.4
31.211.453.6
30.2
38.6
27.6
22.030.424.89.8§
50.435.8
25.9
21.08.2*
13.7
17.0
25.6
24.7
*Numbers shown are based on the total number of reviews, not the number of cases.tDashes denote categores for which there were too few observations to detenmine a
percentage.P<0.OOl for te difference between this rate and all others in the same column.§P<0.01 for the difference between tis rate and all others in the same column.
ous disability increased progressively with the gravity(severity) of the negligence. Nearly three fourths ofthe patients who had adverse events attributed tograve negligence (grade 3) had serious disabilities.Two thirds of these patients died, as compared with10 percent of the patients with adverse events not re-sulting from negligence.
DISCUSSIONPreventability, Error, and Negligence
Many of the adverse events we identified were nei-ther preventable nor predictable, given the currentstate of medical knowledge - for example, idiosyn-cratic drug reactions in patients who had not taken thedrugs previously, postoperative myocardial infarc-tions in young patients without previous evidence ofheart disease, and adhesive intestinal obstructions.Other unpreventable adverse events occurred withpredictable frequency, but patients accepted the riskof treatment because of the potential benefits. Exam-ples of these include radiation injury and bone mar-row suppression from chemotherapy. Preventing these"unpreventable" adverse events will require advancesin biomedical knowledge.Most adverse events are preventable, however, par-
ticularly those due to error or negligence. Our findingsconfirm the observations of others5 - that errors inmedical practice are common. Studies in other areasof human endeavor, such as the generation of nuclearpower, shipping, and the airline industry, confirm thatsome degree of error is inherent in all human activity.6In highly technical, complicated systems, even minor
380 Feb. 7, 1991
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.
ed standard of practice. With the present state ofmedical knowledge, such errors are unavoidable andtherefore not negligent.
Furthermore, the standards of practice that formthe basis for suchjudgments are often not well defined,and thus they may be susceptible to considerable vari-ation in interpretation. Perfection can never be thestandard of practice, since the vagaries of biology andhuman behavior make perfection unattainable, in ei-ther execution or outcome, for any form of treatment.Accordingly, standards of practice must always in-clude an acceptance of some degree of error.
Programs of quality assurance should strive to re-
Table 7. Incidence of Specific Types of Errors in a WeightedSample.*
errors may have disastrous consequences. Medicine isno exception; errors in the performance of highly tech-nical procedures, such as brain or open-heart surgery,can also have catastrophic results.Our physician-reviewers identified management er-
rors in more than half the adverse events we studied.Technical errors were by far the most common class oferror, but relatively few of these were judged to resultfrom negligence. In contrast, errors of omission -failure or delay in making a diagnosis or institutingtreatment, and failure to use indicated tests or takeprecautions to prevent injury - were often classed asnegligent. When the errors of omission were com-bined, they were more common than the errors ofcommission.
Error is not the same as negligence.7 In tort law,medical negligence is defined as failure to meet thestandard of practice of an average qualified physicianpracticing in the specialty in question.8 Negligence oc-curs not merely when there is error, but when thedegree of error exceeds an accepted norm. The pres-ence of error is a necessary but not sufficient conditionfor the determination of negligence.Sometimes the evidence of negligence appears
clear-cut, as when a physician fails to evaluate a pa-tient with rectal bleeding. Other cases are less obvi-ous. For example, depending on the circumstances,each of the following could be considered either negli-gent or not: a mistaken diagnosis of acute appendici-tis, misinterpretation of a chest film of pneumonia asinstead showing congestive heart failure, puncture ofthe pleura during the insertion of a central venouscatheter, and perforation of the bowel during an oper-ation to remove adhesive intestinal obstruction.
In the case of the mistaken diagnosis of acute ap-pendicitis, the patient may have had a classic history,typical findings on physical examination, and labora-tory-test results supportive of the diagnosis. If thephysician then failed to make the diagnosis, it wouldbe both an error in diagnosis and a case of negligence.If, however, the diagnosis was made but no appendici-tis was found, there would also have been an error indiagnosis, but not one involving negligence, becausethe surgeon would have followed the generally accept-
TYPE OF EaOR
Performancoe (697)Inadequate preparation of patient before procedureTechnical errorInadequate monitoring of patient after procedureUse of inappropriate or outnoded form of dherapyAvoidable delay in treatmentPhysician or other professional practicing outside
area of expertiseOtherPrevention (397)Faile to take precautions to prevent
accidental injuryFailure to use indicated testsFailure to act on results of tests or findingsUse of inappropriate or outmoded diagnostic testsAvoidable delay in treatmentPhysician or other professional practicing outside
area of expertiseOtherDiagnostcS(265)Failure to use indicated testsFailure to act on results of tests or findingsUse of inappropriate or outmoded diagnostic testsAvoidable delay in diagnosisPhysician or other professional practicing outside
area of expertieOtherReason not apparentDrug eatment (153)Error in dose or method of useFailure to recognize possible antagonistic or
complementary drug-drug interactionsnadequate follow-up of herapyUse of ina i drugAvoidable delay in treatmentPhysician or other professional practicing outside
area of expertiseOtherSystem (68)Defective equipment or suppliesEquipment or supplies not availableInadequte monitoring systemInadequate reporting or communicationsInadequate training or supervision of physician
or other personnlDelay in provision or scheduling of serviceInadequate staffingInadequate functioning of hospital serviceOther
No. PERCENTt
5955961244113
75
178
79806
12016
77
134833
14917
2416
6710
6538218
18
97610372
14
45
2321
1314
19
5032
I556
105
428
4522145
9
8 88 58 10
11 2615 31.
10 145 67 812 20
*Numbers in parentheses afltr each category of error are the number of erors found by thereviewers for that category. Because the reviewers wer asked to list as many emrrrs as fteyfound, the numbers in each class are larger than those in. Table 6. In addition, since thereviewers were not imitedto identifying a singlenason foreach error, the perentagesexceedtoo.
tPercentages are of dte total number of eors in each category.
Vol. 324 No. 6 381
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.
Negligenewaugradedbycase, aslbeavcrage oftbe scoresfrmdietworeviewsorthe scorefomdte singlereview whenthe was only one. Pet1 age do not a po d direcdy to numbers of eventsbe of weighting.
duce rates of error to an optimal level. Because the have more c
cost of preventing adverse events entirely would be underlying d(prohibitive, defining an optimal level requires a realis- risk of such n
tic assessment of the effectiveness of efforts to reduce as myocardiatheir occurrence. In industry, an error rate that ex- pneumonia. I
ceeds defined norms is deemed unacceptable. We be- by children o
lieve that similar considerations should apply in medi- patients whocine. For example, in the absence of evidence of impaired vitanegligence, a rate of wound infection of 1 percent in are at increathe primary repair of hernias may be acceptable, since fractures.'0it is well recognized that infections occasionally devel- Another faop even with carefully executed operations, and trying rate of adversto reduce their occurrence further would not be cost coexisting coreffective. However, even without evidence of negli- conditions ari
gence, if the infection rate for such operations exceeds complications5 or 10 percent, it is reasonable to conclude that the mia, or strokeaseptic precautions followed during the operation coexisting cor
need review and improvement. Norms for acceptable en times as liklevels of various adverse events need to be established. out such condHospitals can then target their quality-assurance ac- BJ, Cleary P]tivities to the areas most likely to respond to such Yet anotheefforts. provided. TI
events resultiRisk Factors
room could b
An important step in reducing the incidence of ad- operations an
verse events is to identify the patients at highest risk. the emergencThe number and variety of adverse events described that occurredin this study testify clearly to the diversity of hazards nostic errors
in modern medical care. In a typical hospitalization, a which the rei
patient may have hundreds of encounters with doc- Emergency r
tors, nurses, hospital staff, and equipment. Unexpect- time physiciaied results or errors can occur with each encounter, care. Becausiperhaps causing an adverse event. physicians haMany factors increase the risk that a patient will Finally, some
have an adverse event during hospitalization. Our through the e
findings suggest that one major determinant is the Our expericomplexity of the disease or treatment. If, as seems ford found thlikely, every intervention carries some level of risk, trauma treatepatients with complicated disease are more likely to serious errors
have adverse events, if only because their care re- errors involvequires more interventions. Thus, it is not surprising were errors ithat nearly half the adverse events we identified re- creased withsulted from operations. In even a simple operation such as alcohthere are dozens, even hundreds, of maneuvers, from ries, but the iskin preparation to wound closure, as well as many physician's irinterventions in the postoperative care. Each presents high rate of c
an opportunity for an adverse event. Our findings are Finally, we
very similar to those of a Californiastudy in which half the potential-ly compensable events (comparableto what we have called adverseevents) were found to result fromtreatment in the operating room.9The high number of drug-related
adverse events in our study mayalso be related in part to the quanti-ty and variety of medications ad-ministered to hospitalized patients.
Characteristics of patients alsoincrease the risk of an adverseevent. Elderly patients, for exam-ple, are far more likely not only to
omplicated disease, but also to haveegenerative conditions that increase theontechnical postoperative complications1l infarction, pulmonary embolism, andInsults or errors that are tolerated wellr young healthy adults can be lethal inare weakened by disease or who have
al organs. In addition, elderly patientssed risk of falling and therefore of hip
.ctor that may account for the increasedse events in the elderly is the presence ofnditions. Greenfield has shown that suche a strong predictor of serious hospitals (such as pulmonary embolism, septice-e after hip surgery). Patients with severenditions on admission are more than sev-kely to have a complication as those with-litions (Greenfield S, Apolone G, McNeilD: personal communication).r risk factor is the location where care ishe high rate of negligence in adverse:ing from treatment in the emergencye caused by several factors. Because noId only a few procedures are performed iny room, the adverse events we identifiedI there were more likely to involve diag-or mishaps of noninvasive treatment,viewers frequently judged as negligent.ooms are sometimes staffed with part-ns who are not well trained in emergencye they are frequently very busy, theseve less time to spend with each patient.of the sickest patients enter the hospitalemergency room.ience is not unique. Dearden and Ruther-iat for 58 percent of patients with severeed in the emergency room there had beenin treatment." Although many of these
ed mistakes or delays in diagnosis, mostin treatment. The risk of error was in-L certain characteristics of the patient,olism and the presence of multiple inju-investigators concluded that the treatingnexperience was the chief cause of theerror.e believe that the risk of injury, particu-
382 Feb. 7, 1991
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.
Vol. 324 No. 6 ADVERSE EVENTS IN HOSPITALIZED PATIENTS - LEAPE ET AL. 383
larly serious injury, is closely related to the medicalnature of the intervention. A momentary lapse thatdelays the diagnosis of a skin rash is usually of littleconsequence, for example, whereas a similar lapseduring a brain operation can have disastrous effects. Itis unlikely that neurosurgeons are more prone to errorthan dermatologists, but the conditions under whichthey work are far less forgiving. As we have seen, cer-tain specialties, such as thoracic surgery, obstetrics,and neurosurgery, had more adverse events than otherspecialties, but the events were not more likely to havebeen caused by negligence.'
Limitations of the Study
Our observations and conclusions must be inter-preted within the limitations of a retrospective reviewof records. Several features of the study could havebiased the results. First, we relied exclusively on datafrom hospital records. Although we have shown thatadverse events can be identified accurately from infor-mation in hospital records,'2 such records may notprovide evidence or insight into the specific causes ofan adverse event. For example, in some of our studypatients, the adverse event was caused by failure todiagnose an ectopic pregnancy. From the informationin most hospital records, it would not be possible totell whether such failures occurred because the physi-cian (1) did not think of the diagnosis, (2) consideredthe diagnosis unlikely and therefore did no furtherfollow-up examinations or testing, or (3) consideredthe diagnosis possible and recommended further test-ing, but the patient did not come for the test (in whichcase the outcome would not have been considered anadverse event). Nor can we tell whether (4) both thephysician and the patient sought the test, but theequipment was broken (or overbooked, unavailable onweekends, or the like), (5) the examination was per-formed but the results were not reported, or (6) anyone of many other possible problems arose that can beimagined.
Second, we relied on implicit, not explicit, review.Because we studied the entire range of medical serv-ices, it was not possible to set up explicit criteria forevery conceivable type of adverse event. Accordingly,we relied on thejudgments of physicians. To minimizevariability therein, we structured the record-reviewprocess by means of an Adverse Event Analysis Form,which required the reviewers to conduct their analysisin a standardized way and to address specific ques-tions about causation.
Third, we used general internists and surgeons asphysician-reviewers, not specialists. For a study ofthis scope and magnitude, it would have been bothdifficult and expensive to do otherwise, since the re-viewers were required to identify adverse events of alltypes. In our pilot study, we found that internists andsurgeons could identify adverse events with a highdegree of accuracy.'3 As they had been instructed todo, the reviewers consulted with a panel of specialistswhen they needed to determine whether the care thathad resulted in a possible adverse event met acceptedstandards.
Finally, our information on the follow-up of the pa-tients was limited to data about care in the hospital(including the outpatient department). Although thereviewers had available the record of care provided atthe same hospital after the index hospitalization, theyhad no access to the information in physicians' privateoffices. However, except for those that are rapidly fa-tal, adverse events not requiring hospital care are un-likely to result in serious disability.
Prevention of Adverse Events
As knowledge increases, in theory more adverseevents will become preventable. Indeed, the safetyand effectiveness of many current medical treatmentsresult from the earlier reduction or elimination ofcomplications similar or identical to those we haveidentified as adverse events here: high rates of heartblock, bleeding, and mortality in the early years ofheart surgery, problems associated with the initial at-tempts at organ transplantation, side effects of manydrugs, and so forth. These were the adverse events ofan earlier day, and they were greatly reduced in fre-quency after research led to an understanding of theircauses.
Future reductions in the occurrence of adverseevents also depend in part on research into causes.In the case of adverse events that are currently un-preventable, progress will come from scientific ad-vances, such as the development of less hazardouschemotherapeutic agents. In the case of events dueto error, control will require scientific advances insome instances, but we believe that progress will alsodepend heavily on systems analysis, education, andthe development and dissemination of guidelinesand standards for practice. Automatic "fail-safe" sys-tems - such as a computerized system that makes itimpossible to order or dispense a drug to a patientwith a known sensitivity - are likely to have an in-creasing role.The reduction of adverse events involving negli-
gence will also require an increased emphasis on edu-cation. To the extent that failure to meet the standardof practice is due to ignorance, improved dissemina-tion and enforcement of practice guidelines might beeffective. The development of better mechanisms ofidentifying negligent behavior and instituting appro-priate corrective or disciplinary action is equally' im-portant.
Preventing medical injury will require attention tothe systemic causes and consequences of errors, aneffort that goes well beyond identifying culpable per-sons.7 Such approaches have paid off handsomely inother highly technical and complicated enterprises,such as aviation.6',4 A similar strategy may work inmedicine as well.
In this context, our description of adverse eventsrepresents an agenda for research on quality of care.Adverse events result from the interaction of the pa-tient, the patient's disease, and a complicated, highlytechnical system of medical care provided not only bya diverse group of doctors, other care givers, and sup-port personnel, but also by a medical-industrial sys-
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.
384 THE NEW ENGLAND JOURNAL OF MEDICINE Feb. 7, 1991
tem that supplies drugs and equipment. Reducing therisk of adverse events requires an examination of allthese factors as well as of their relation with eachother.
REFERENCES
1. Brennan TA, Leape LL, Laird NM, et al. Incidence of adverse events andnegligence in hospitalized patients - results of the Harvard Medical Prac-tice Study I. N Engl J Med 1991; 324:370-6.
2. Hiatt HH, Barnes BA, Brennan TA, et al. A study of medical injury andmedical malpractice: an overview. N Engl J Med 1989; 321:480-4.
3. Shah BV. SESUDAAN: Standard errors program for computing of stand-ardized rates from sample survey data. Research Triangle Park, N.C.: Re-search Triangle Institute, 1981.
4. Miller RG. Simultaneous statistical inference. 2nd ed. New York: Springer-Verlag, 1981.
5. McDonald CJ. Protocol-based computer reminders, the quality of care andthe non-perfectability of man. N Engl J Med 1976; 295:1351-5.
6. Perrow C. Normal accidents: living with high-risk technologies. New York:Basic Books, 1984.
7. Vincent CA. Research into medical accidents: a case of negligence? BMJ1989; 299:1150-3.
8. Brune v. Belinkoff, 354 Mass 102 (1968).9. California Medical Association. Report of the Medical Insurance Feasibility
Study. San Francisco: California Medical Association, 1977.10. Tinetti ME, Speechley M. Prevention of falls among the elderly. N Engl J
Med 1989; 320:1055-9.11. Dearden CH, Rutherford WH. The resuscitation of the severely injured in
the accident and emergency department - a medical audit. Injury 1985;16:249-52.
12. Brennan TA, Localio AR, Leape LL, et al. Identification of adverse eventsoccurring during hospitalization: a cross-sectional study of litigation, qualityassurance, and medical records at two teaching hospitals. Ann Intern Med1990; 112:221-6.
13. Brennan TA, Localio AR, Laird NL. Reliability and validity of judgmentsconcerning adverse events suffered by hospitalized patients. Med Care1989; 27:1148-58.
14. Ricketson DS, Brown WR, Graham KN. 3W approach to the investigation,analysis, and prevention of human-error aircraft accidents. Aviat SpaceEnviron Med 1980; 51:1036-42.
15. Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equip-ment failures in anesthesia management: considerations for prevention anddetection. Anesthesiology 1984; 60:34-42.
16. Berwick DM. Continuous improvement as an ideal in health care. N Engl JMed 1989; 320:53-6.
17. Laffel G, Blumenthal D. The case for using industrial quality managementscience in health care organizations. JAMA 1989; 262:2869-73.
REVIEW ARTICLE
JOHN A. OATES, M.D., EditorALASTAIR J.J. WOOD, M.D., Associate Editor
FLUOROQUINOLONE ANTIMICROBIALAGENTS
DAVID C. HOOPER, M.D.,AND JOHN S. WOLFSON, M.D., PH.D.
TH E introduction of fluoroquinolone antimicrobialagents (Fig. 1) into clinical use is an important
recent advance.`3 These drugs, also called quinolones,include norfloxacin, ciprofloxacin, ofloxacin, enoxa-cin, and pefloxacin. Of these, norfloxacin, ciprofloxa-cin, and ofloxacin have been approved for use in theUnited States. Quinolones are orally absorbed, arepotent in vitro against a broad spectrum of bacterialspecies, and have favorable pharmacokinetic proper-ties. We shall evaluate here the current status of thequinolones, considering mechanisms of action and re-sistance, activity in vitro, pharmacokinetics, clinicalefficacy, adverse effects, and clinical uses. A discussionof the structure-activity relations of the quinolones isbeyond the scope of this article, and this topic hasrecently been reviewed elsewhere.4'5
MECHANISMS OF ACTION AND RESISTANCE
Uniquely among antimicrobial agents in clinicaluse, the primary bacterial target of quinolones is DNA
From the Infectious Disease Unit, Medical Services, Massachusetts GeneralHospital and Harvard Medical School, Boston. Address reprint requests to Dr.Hooper at the Infectious Disease Unit, Massachusetts General Hospital, 32 FruitSt., Boston, MA 02114-2696.
gyrase (bacterial topoisomerase II),6-9 an enzyme thatintroduces negative supertwists into DNA and sepa-rates interlocked DNA molecules. Quinolones antago-nize these enzymatic activities, interfering with DNAreplication, segregation of bacterial chromosomes,transcription, and other cellular processes and damag-ing DNA. Recently, binding to gyrase-DNA complex-es has been reported.'"
Spontaneous single-step mutation to quinolone re-sistance tends to be infrequent (1:< 109), and when itoccurs the resistance is of a low level for many bacteri-al species. High-level resistance can be selected byserial exposure of bacteria to increasing drug concen-trations. Mechanisms of bacterial resistance to quino-lones include chromosomal mutations that either alterDNA gyrase (resistance to quinolones alone) or re-duce drug accumulation in association with changesin bacterial outer-membrane proteins (pleiotropic re-sistance). Destruction or modification of the drug bybacteria has not yet been described, and plasmid-me-diated resistance to fluoroquinolones has not yet beenfound in clinical isolates.
ACTIVITY IN VITROIn general, quinolones have excellent potency in
vitro3" against most Enterobacteriaceae, fastidiousgram-negative bacilli including species of haemophi-lus, and gram-negative cocci, such as Neisseria gonor-rhoeae, N. meningitidis, and Moraxella (Branhamella)catarrhalis (Table 1). Among the drugs listed in Table1, ciprofloxacin is the most potent. Quinolones areactive against Pseudomonas aeruginosa but are less activeagainst other species of pseudomonas. They also havegood activity against Staphylococcus aureus and otherstaphylococci but are less active against species ofstreptococcus and enterococcus. They have minimalactivity against anaerobes and none against Candidaalbicans. Quinolones are active against gram-negative
The New England Journal of Medicine Downloaded from nejm.org at UNIVERSITY OF SOUTH AUSTRALIA on August 27, 2012. For personal use only. No other uses without permission.