47
Dr Alison Wint Macmillan GP and Clinical Lead for Cancer S. Glos CCG The New NICE Suspected Cancer Guidelines May 2016
Dr Alison Wint Macmillan GP and Clinical Lead for Cancer S. Glos CCG
The New NICE Suspected Cancer Guidelines
May 2016

Aims?
What are your aims & objectives for this session?
Dr A Wint: May 2016

Aims
• Background to the guidance • The new TWW Guidelines –
principles & overview. • What aids are available? • The Primary care role in
cancer diagnosis. • Case studies • Consider follow-up actions
Dr A Wint: May 2016

Cancer – always in the news
Dr A Wint: May 2016

National Policy Documents
Dr A Wint: May 2016
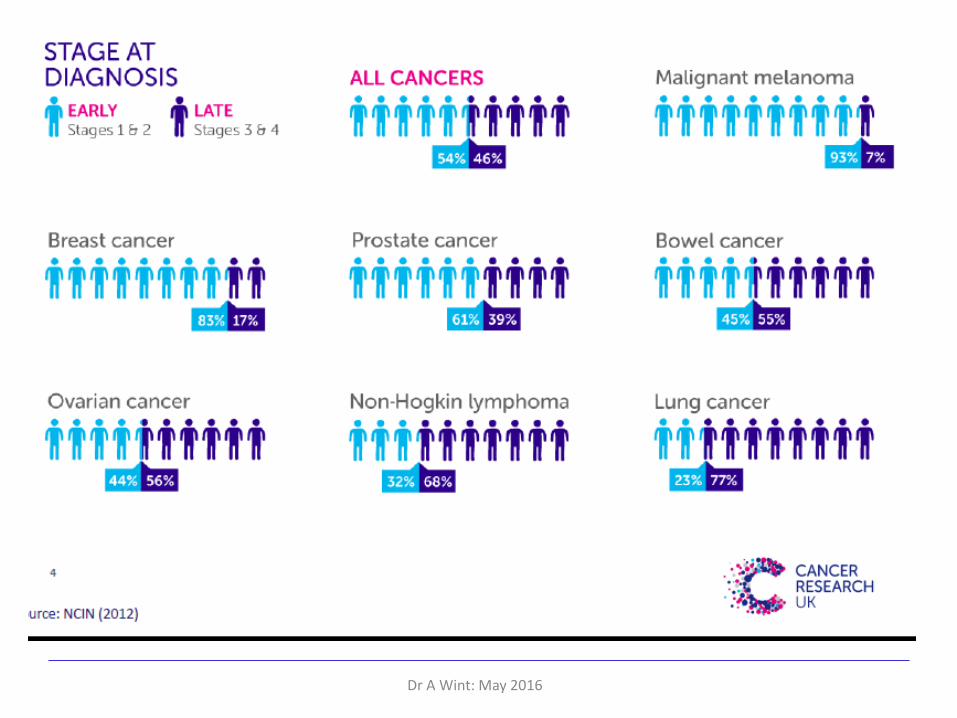
The Cancer Story is changing
• Public awareness of symptoms & risk factors rising
• More cancers are being diagnosed, 300,000/yr
• 50% of those born after 1960 will get cancer
• 200 different types of cancer
• New screening tests are being introduced
Dr A Wint: May 2016
There is a New cancer Story
Dr A Wint: May 2016
• Treatments are more effective
• More people are surviving.
• Cancer a new long term condition
• End of Life Care in UK exemplary.
Cancer is no longer a death sentence

The primary care Challenge
Patients present with vague symptoms.
Dealing with an ageing population
Frailty can mimic cancer
More likely to have co-morbidities.
The average GP diagnoses 8 pts/year.
But a GP considers a cancer diagnosis several times/day.
Dr A Wint: May 2016

Dr A Wint: May 2016
Dr A Wint: May 2016
Dr A Wint: May 2016
Benefits of Earlier Diagnosis
For Clinicians: • Higher standards & job satisfaction.
• Fewer complaints and risks of litigation.
For patients: • Less intrusive treatment & better quality of
life. • Avoidance of emergency admissions
For Commissioners: • Costs less and saves more lives
Dr A Wint: May 2016
Why New Guidelines
• 10yrs since the initial TWW guidance was published.
• Then it was a cultural change in how GPs referred patients with suspected cancer.
• It was resisted at the time by GPs who were used to referring to a named clinician.
• It was a challenge for Secondary Care Consultants who thought GPs were referring inappropriate patients as only 10% had cancer
• It was an administrative challenge as the PCTs & Trusts were being rated nationally on their achievement of the 14day target.
Since then there has been a growing body of research evidence on the benefits of earlier diagnosis of cancer.
Dr A Wint: May 2016
The New NICE suspected Cancer Guidance
Overarching Principles
• The 2005 TWW guidance was based on Secondary care data
• 2015 Guidance based on evidence from symptoms presenting to Primary Care.
• Positive Predictive Value of 3% for presenting symptoms is used to inform recommendations. 5% used in 2005
Dr A Wint: May 2016

The Role of Primary care
• 90% of cancers are diagnosed based on presenting symptoms
• 85% are seen in Primary care
• Patients diagnosed via TWW pathway have better clinical outcomes.
Dr A Wint: May 2016
Risk Factors
Dr A Wint: May 2016
Lifestyle, genetic and industrial exposure risk factors are important, and must be addressed, but do not affect how cancers present clinically.
Screening Outside the scope of this talk
Primary Care responsibility to keep abreast of changes & encourage pts to take part.
Screening now available
• Breast
• Cervical
• Colorectal – FIT Test and Bowel scope of all 55yr olds.
Note also: HPV vaccination and PSA testing for men who request it.
Dr A Wint: May 2016

The new guidance provides
• Advice on when to refer urgently.
• When to use TWW referral process.
• The referral criteria for most clinical sites remains the same.
• Suggestions for investigations within Primary Care
• Emphasises that these are recommendations and not requirements and are not intended to override clinical judgement
Dr A Wint: May 2016
Layout of Guidance
Cancer Site
Patient support
Symptoms
Dr A Wint: May 2016
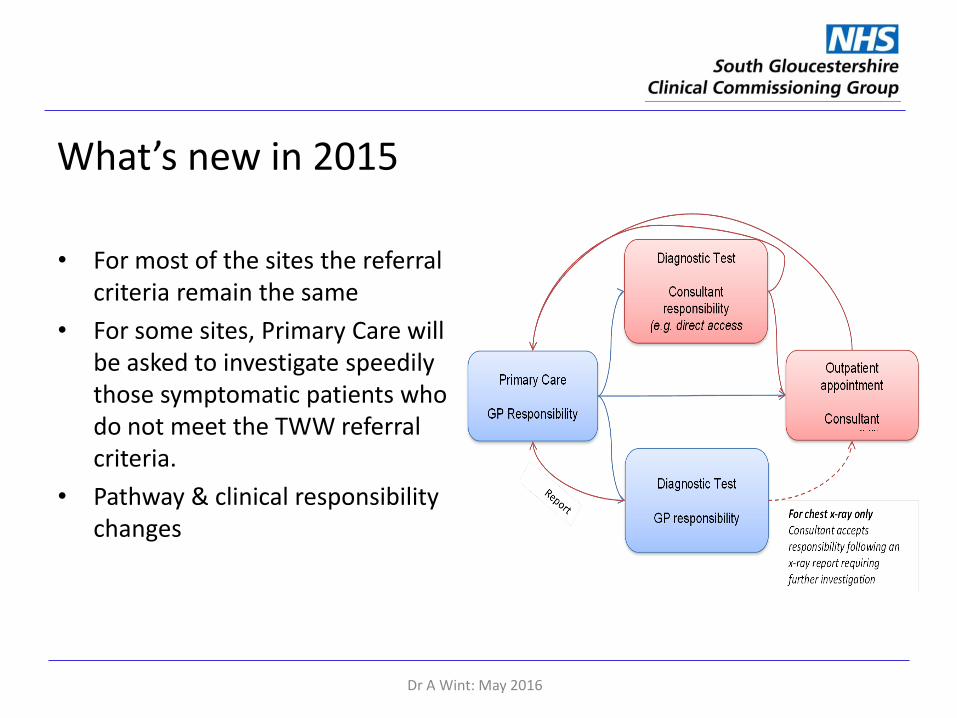
What’s new in 2015
• For most of the sites the referral criteria remain the same
• For some sites, Primary Care will be asked to investigate speedily those symptomatic patients who do not meet the TWW referral criteria.
• Pathway & clinical responsibility changes
Dr A Wint: May 2016
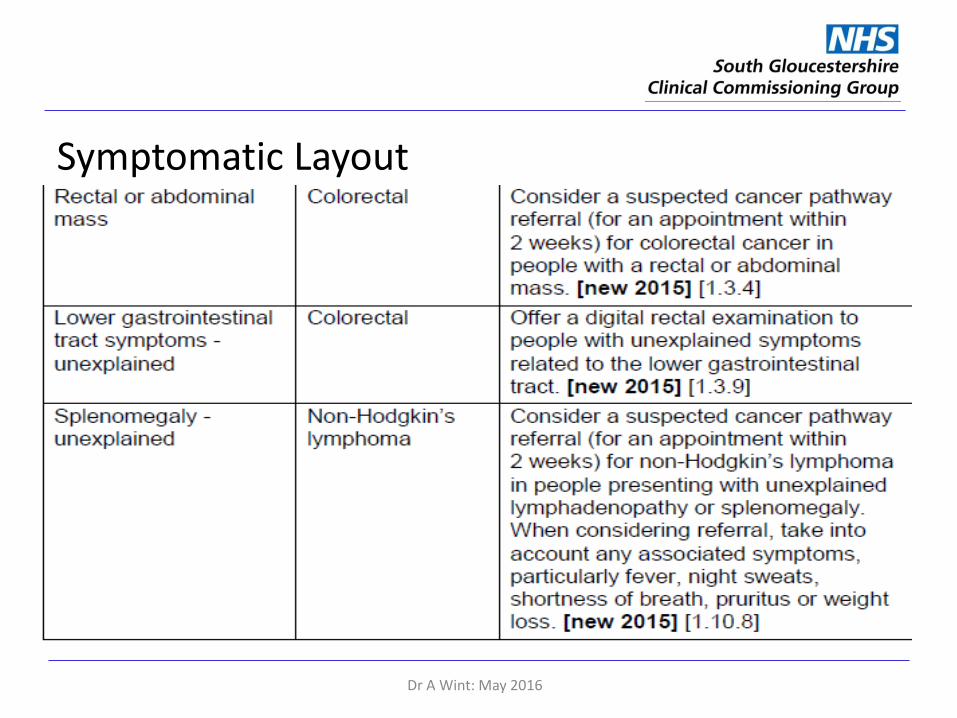
Symptomatic Layout
Dr A Wint: May 2016
The New Cancer Story
• How has the GPs role changed with the new guideline?
• What’s new for investigations?
• Patient Support & Safety netting.
• What aids are available to help?
• What action can we each take?
Dr A Wint: May 2016
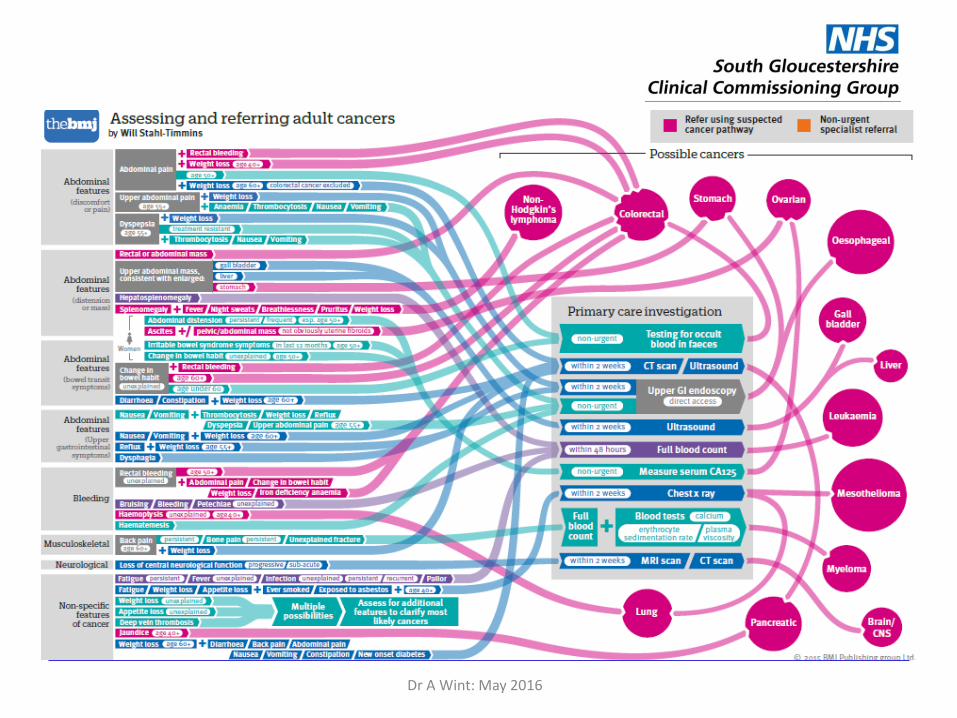
Primary Care Investigation
• What investigations should be carried out from Primary Care?
• To identify the groups of symptomatic people with greatest risk of cancer.
• To minimise the number of referrals for patients who do not
have cancer.
Dr A Wint: May 2016
Primary Care Investigations
• PSA
• Ca125
• Ca+
• Leucopenia
• Anaemia
• Iron deficiency
• Non-visible haematuria
Dr A Wint: May 2016
Thrombocytosis
• 40% risk of cancer
• Lung – CXR
• Endometrial – USS
• Oesophagus/stomach – endoscopy
• CT chest or Abdo
Dr A Wint: May 2016
Investigation Cont’d
• FOB/FiT – GI symptoms without rectal bleeding
• New diagnosis diabetes with weight loss >60yrs – consider pancreatic cancer
• Leucocytosis with non-visible haematuria >60yrs consider bladder Cancer
Dr A Wint: May 2016
Direct Access Investigation
Urgent direct access from Primary Care for investigation within 2 weeks is recommended in several cancer sites.
• CXR
• Endoscopy
• Non-obstetric USS
• MRI of brain
Dr A Wint: May 2016
Safety Netting • Actively monitor symptomatic patients
who are do not meet the referral criteria. “Low risk, but not no risk”
• Specific advice to patient.
• When to return if symptoms continue.
• What symptoms to aware of.
• How to and when to get results
• Clear practice protocol for management of results
• Beware of false negative results
Dr A Wint: May 2016
Patient Support
• Shared decision making & informed patients a key principle
• Information at the time of referral: on process, investigations, risks & likelihood of cancer.
• Reassurance and information for
patients with low risk symptoms.
Dr A Wint: May 2016

GPs Gatekeeper Role?
• GPs should no longer have a gate-keeper role.
• The presence of symptoms should trigger investigation rather than be a filter.
• Lower the threshold for investigation.
Diagnosing cancer earlier will lead to less invasive treatment and result in improved survival
Dr A Wint: May 2016
Aids
Dr A Wint: May 2016
Macmillan, CRUK & BMJ and Red Whale GP Up-date have all published aids for GPs to use the guidelines
Macmillan
Dr A Wint: May 2016

Dr A Wint: May 2016
Dr A Wint: May 2016
Dr A Wint: May 2016

Dr A Wint: May 2016
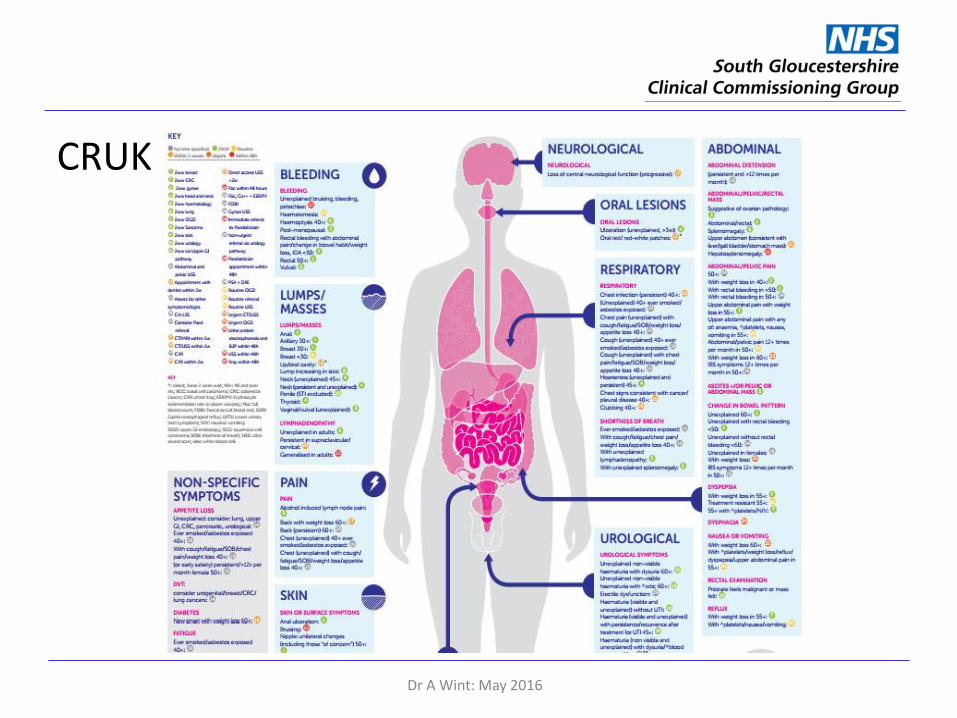
CRUK
Dr A Wint: May 2016

CRUK
Dr A Wint: May 2016

What can You do?
• Find a decision support tool you can work with.
• Familiarise Yourself with the layout of the new guidance.
• There is a lot that will stay the same.
• Be aware of the referral routes in your area.
• Availability of investigations may change.
Dr A Wint: May 2016

Action Plan Suggestions.
• Carry out a Significant Event Analysis of a cancer diagnosis.
• Take part in continuing education and Peer review.
• Do an audit of the outcomes of your TWW referrals.
Dr A Wint: May 2016
Case Discussions Using Aids
• Mrs T
• Mrs W
• Weight Loss
• Abdominal pain
Dr A Wint: May 2016

Practice Profiles The practice profiles are produced annually
Compare a variety of parameters at Trust, CCG and Practice level
• Age
• Deprivation
• Screening Up-take
• TWW referrals, conversion & detection rate
• Specific data: Dermatology, Lung, Lower & Upper GI
• Emergency presentation of cancer
www.fingertips.phe.org.uk/profile/cancerservices
Dr A Wint: May 2016

Dr A Wint: May 2016

Dr A Wint: May 2016
Remember: Medicine can be messy!
Cancer diagnosis is important, but -
• Things are never black or white.
• Every patient is unique
• Raise our index of suspicion
• Lower our threshold for investigation.
Dr A Wint: May 2016
The New cancer Story
Dr A Wint: May 2016
Our challenge is to each be part of creating the new cancer story.
Think Cancer!

Dr A Wint: May 2016

















