In the meniscus there is a reduction in both water content and non-collagenous matrix leading to
degeneration of the central core. This increases susceptibility to horizontal tears with the potentialfor the development of osteoarthritis.2
The water content and proteoglycan subunits decrease in the intervertebral disc with aging. After
40 the nucleus pulposis becomes increasingly fibrillar, losing its gel form and capacity for shock
absorption. However, disc degeneration though common in old age, is not invariable.3
Aging tendons and ligaments lose elasticity - a combination of reduced water content and altered
collagen and elastin fibre cross linkage. The elderly athlete is more susceptible to sprains and
strains which can be avoided by regular stretching to maintain joint range of motion.
1. Lane, N. E., Block, D. A., Hubert, H. B. et al. (1990) Running osteoarthritis and bone
density : initial 2 year longitudinal study. American Journal of Medicine, 88 : 452-459.
2. Ghosh, P. et al. (1987) : The knee joint meniscus : a fibro-cartilage of some distinction.
Clinics in Orthopaedics, 224, 52 -
3. Twomey, L. T., Taylor, J. R. (1987): Age changes in lumbar vertebra and intervertebral
discs. Clinics in Orthopaedics, 224 : 97
Bone
Maximal bone mass is reached at about the age of 30 and is stable for around ten years.
Thereafter cortical bone mass declines at 0.6% per year and trabecular at 0.7% per year (probably
from an earlier age). The smaller the bone mass accumulated during skeletal growth the greater
the risk of fracture in later life.
There are two distinct phases of bone loss - a protracted slow phase in men and women resulting
in similar losses of cortical and trabecular bone, and a transient accelerated phase after the
menopause in women that results in a disproportionately greater loss in trabecular bone 1. By age
70 in men 20% cortical and 35% trabecular bone mass and in women 35% cortical and 50%
trabecular bone mass has been lost. Determinants of bone loss are genetic and hormonal but also
include modifiable life style factors such as diet (especially calcium) and exercise. Skeletal stressfrom weight bearing exercise stimulates osteoblast function thereby increasing bone mass. Bone
density has been shown in cross-sectional studies to be greater in athletes compared to sedentary
controls. Prospective studies demonstrate that postmenopausal women enrolled in a regular
exercise program gain bone, whereas controls lose it.
2. Rowe, J. W., Reubin, A., Jordan, D. (1976) Effect of age on creatinise clearance in men: a cross-sectional
and longitudinal study. Journal of Gerontology, 31 (2), 155-163.
3. Balcomb, A.C., Sutton, J.R. (1986), Advanced age and altitude illness. In: Sutton, J.R., Brock, R.M., eds.
Sports medicine for the mature athlete. Benchmark Press, 213-24.
Altitude
Research suggests that older climbers may have a reduced incidence and severity of acute
mountain sickness. This condition is commonly experienced by individuals who ascend above
3000 metres. Symptoms include anorexia, nausea, vomiting, weakness, headache and insomnia
within several hours of arriving at altitude. A potentially life-threatening complication is pulmonary
oedema, but in general the symptoms are self-limiting.
Aging is associated with a reduced Pao2 (arterial oxygen partial pressure) and the aging athlete isunable to deliver the same volume of O2 to working muscles compared to the young. At high
altitude the partial pressure of O2 in the atmosphere is less so that less O2 is available to capture
and be carried to the tissues. This compounds older athlete's physiological disadvantage creating a
greater challenge. However, fitness rather than age correlates with the older athlete's ability to
tolerate exercise at altitude.3
Skin
The skin provides a barrier against trauma, infection, U.V. irradiation, heat and cold and is an
energy storage site.1 Changes seen in the aging skin which compromise these functions are due
as much to sun damage as to physiological factors.
Overall the skin is thinner and more fragile. Blisters are more common. Renewal of the epidermis is
slower, leading to delayed healing. The dermis is less cellular and less vascular and there is less
subcutaneous tissue, thus less insulation especially in elderly women. Sweat gland numbers and
function are reduced. Meissner's and Pacinian corpuscles - the cutaneous end-organs responsible
for pressure, vibration and light touch sensation - decrease to approximately one third of their initial
density between the second and ninth decades. The resulting increase in pain threshold may
contribute to skin injury. There is diminished T cell function, Langerhans cell die off and after 50
years melanocytes decline at 2% per year making the aged more susceptible to infection neoplasm
and U.V. damage. Aging athletes can minimise risks by wearing hats, protective clothing, sun
screen, sun avoidance (exercise before 10 a.m. and after 4 p.m.) and good footwear. Sores that
are slow to heal or moles that change must be seen by the doctor.
1 Balin, A. K., Kligman (eds) (1989), Aging and the Skin. Raven Press.
Older athletes are less tense, depressed, angry and confused, have greater vigour, a more positiveattitude and higher self-esteem. Reasons given by older athletes for competing are
• to belong to a group exercise such as walking and swimming, maintains muscle mass
enabling older people to retain their independence thereby postponing frailty. This has
economic advantages and also contributes to self-esteem.1
• to enhance mood
• fitness (in that order). Regular aerobic exercise, even low intensity
Psychological stresses
Aging competitors almost always have more financial, professional, social and family obligations
than the young. This may mean suboptimal training, hurried warm ups and increased risk of injury.
As an aging athlete begins to lose his competitive edge there may be denial, anger then
acceptance (typical grieving process). These mature athletes need to be reassured that they can
still bring skill and wisdom to the game and be an inspiration to the young. Many do this by
remining involved in their sport as trainers and officials. Although some world class athletes
become world class masters, many do not - perhaps because of earlier exhausting training
schedules causing ‘burn-out’ or previous injuries. A positive attitude towards aging is an important
determinant of success for aging both in general and in competition.
1. Shepard, R.J., (1993) Exercise and aging: extending independence in older adults. Geriatrics 48. 61.
2. Ungerleider, S., Golding, J. M., Porter, K. (1989), Mood profiles of masters track and field athletes. Percep. Motor
Skills, 68 : 607-617.
Exercise programs
Assessment
(a) History:
should include
• past/present medical problems: especially recent myocardial infarction, bypass surgery,
pacemaker.
• medications: especially chronotropic and ionotropic drugs
• risk factors for cardiovascular disease: obesity, hypertension, high cholesterol, smoking,
• injury-free (treat prior conditions, contain inflammation quickly, more time to recover
• cross training to maintain fitness after exercise injury
• realistic goals (start slow)
• feedback (diaries, charts, document progress)
• proper equipment/clothing/footwear
• more time to loosen up and recover
• adequate hydration
• exercise with friend/partner
1. Ghosh, P. et al. (1987) : The knee joint meniscus : a fibro-cartilage of some distinction. Clinics in Orthopaedics, 224,
52 -
2. Grimby, G., Physical activity and muscle training in the elderly (1986), Acta Medica Scandinavica 711 (Suppl.) : 233-
37.
3. Gorman, K. M., Posner, J. D. (1988), Benefits of exercise in old age, Clinics in Geriatric Medicine, 4 : 181-92.
Injuries
Aetiology
Exercise related injury in the aged can result from current training, earlier injuries causing trouble in
later life. Of major influence are underlying aging changes, especially reduced compliance, and thenature of the exercise, elderly people engage in less high impact and contact sport. common
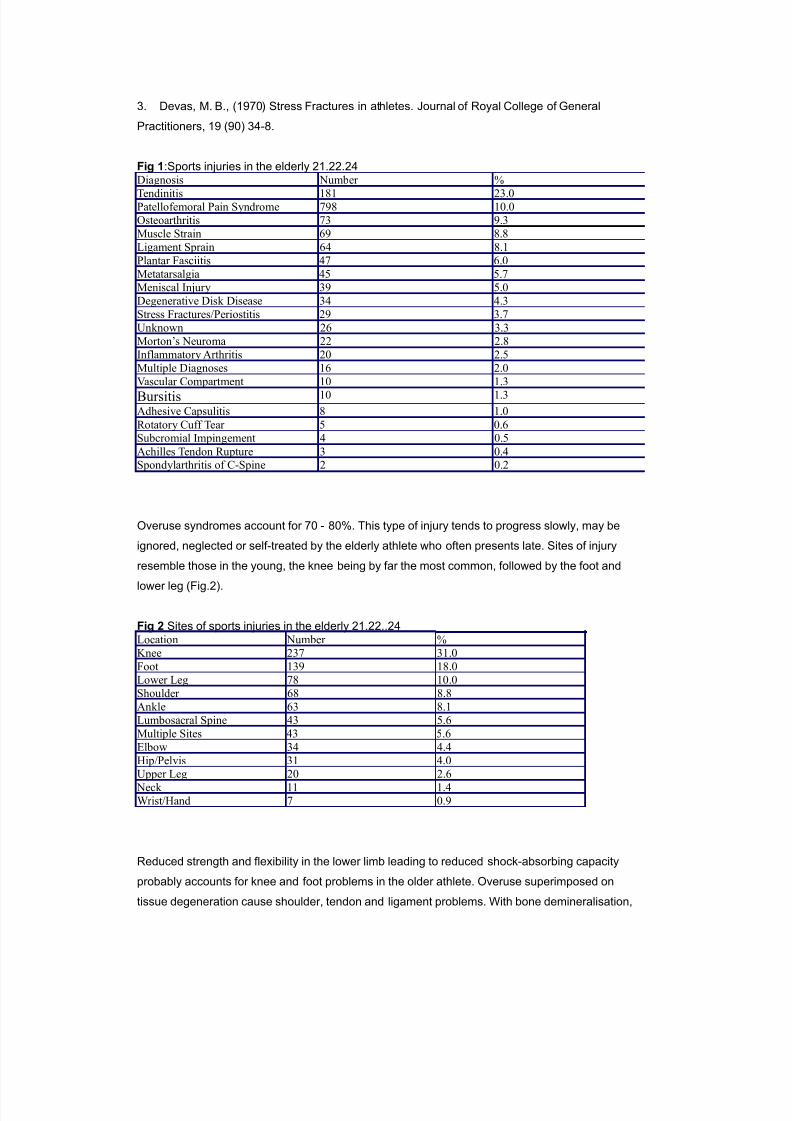
causes of exercise-related injury in the aged are listed in Fig.1.1-2
1. Matheson, G. O., MacIntyre, J. G., Taunton, J. E. (1989), Musculoskeletal injuries associated
with physical activity in older adults. Science Sports and Exercise. 21 (4), 379-385.
2. DeHaven, K.E., Littner, D. M., Cape, R. D. (1986) Athletic injuries : comparison by age, sport
and gender. American Journal of Sports Medicine. 14(3), 218-224.
drugs (diazepam) have a reduced concentration after a given dose, are widely distributed in fat and
thus take longer to excrete when stopped.
c) Pharmacodynamics
i. receptor sensitivity is reduced for some drugs (beta blockers) and increased for others
(benzodiazepines, morphine).
d) Particular drugs
i. NSAIDs cause gastrointestinal bleeding.
ii. Codeine can cause nausea, constipation and confusion.
iii. Paracetamol given regularly (1 gm 4 - 6 hourly) for pain may be more suitable.
iv. Morphine can cause nausea, constipation and confusion and much smaller doses (2.5 - 5.0 mg 4 -
6 hourly) required.
v. Benzodiazepines should be avoided as they cause drowsiness, confusion, ataxia, falling and
postural hypotension.
e) Principles for drug prescribing in the aged:
i. Start low, go slow.
ii. Be aware other medications (stop, if possible).
iii. New symptoms may be an ADR.
iv. Regular review.
3. Therapy for injuries in the old takes longer.2 Start rehabilitation early and plan to treat for twice
as long in those > 60 and for three times as long for those > 75. Decrease activity by 15 - 25% untilsymptoms disappear. Similarly return to activity should be in increments of 15 - 25% over 3 - 6
weeks. Physiotherapy is useful including ultrasound, stretching and gentle manipulation such as
Maitland's mobilisation.3 Exercises ideally to be performed at home but with support to aid
motivation and compliance can be prescribed. Muscle strengthening (agonist-antagonist) exercises
such as quadriceps and hamstring exercises in knee injury can be taught to and performed by the
elderly.
4. Bracing/orthotics may play a role for such problems as Achilles tendinitis, posterior tibial
tendinitis, plantar fasciitis and ankle instability.
5. Local corticosteroid injection should be considered (10%).
6. Surgery may be required rarely (2 - 4%).
1. Atkin, P. A., Ogle, S. J., 1996. Issues in medication compliance and the elderly. Adverse Drug Reactions and
Toxicological Reviews, 15 (2) 109-118.
2 Brown, M. B. (1989), Special considerations during rehabilitation of the aged athlete. Clinics in Sports Medicine, 8(4),
1. Rock, C. L. (1991), Nutrition in the older athlete. Clinics in Sports Medicine, 10(2), 445-457.
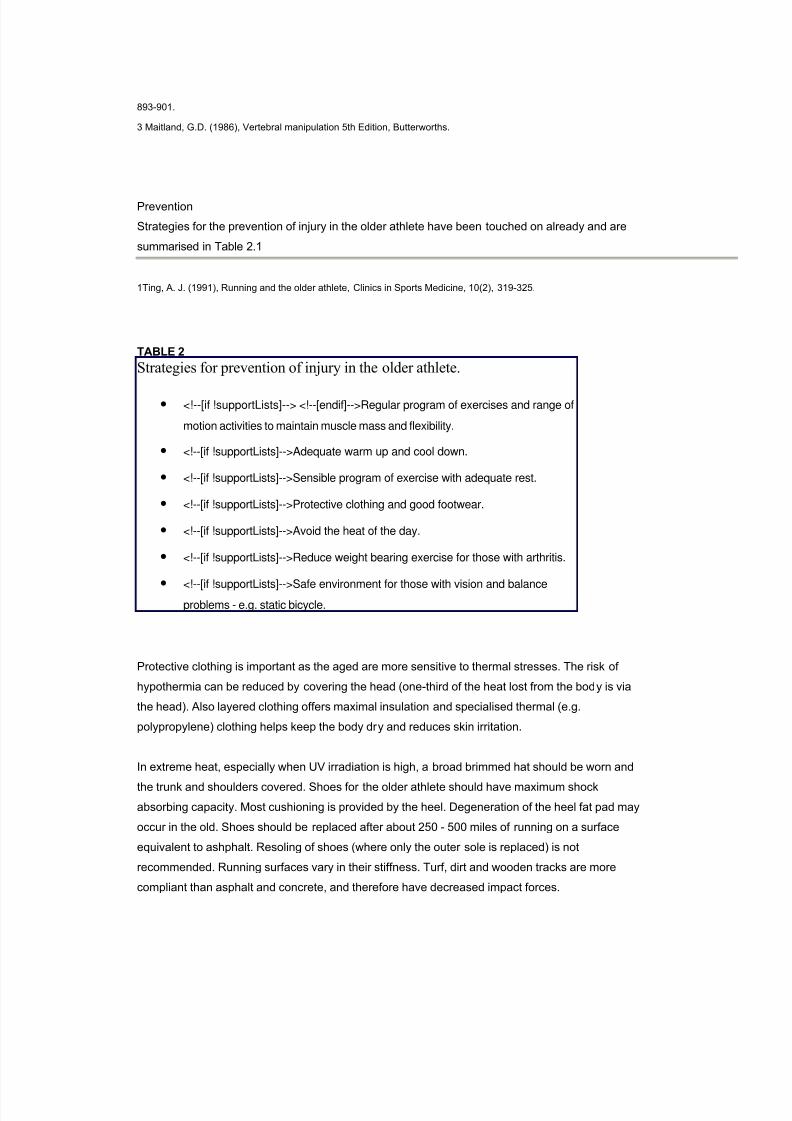
Conclusion
More people are reaching old age and many older people are exercising. The observed physical
changes with aging are compounded by disuse as inactivity is still common amongst the aged. The
benefits of regular aerobic exercise are now well documented and include:- physical (reduced
mortality), psychological (elevated mood) and social (less isolation). Injury, especially overuse
injuries occur but can be treated and prevented.
The doctor's responsibility is to encourage exercise/activity for older people to increase their overallhealth and sense of wellbeing. Provision of pre-exercise evaluation, prescription of an exercise
program, diagnosis and management of injuries plus counselling about prevention and nutrition is
essential for all older athletes.
Addendum. Muscle weakness and high-resistance training in older people.
Greg Bennett,
Tom Gwinn
Introduction
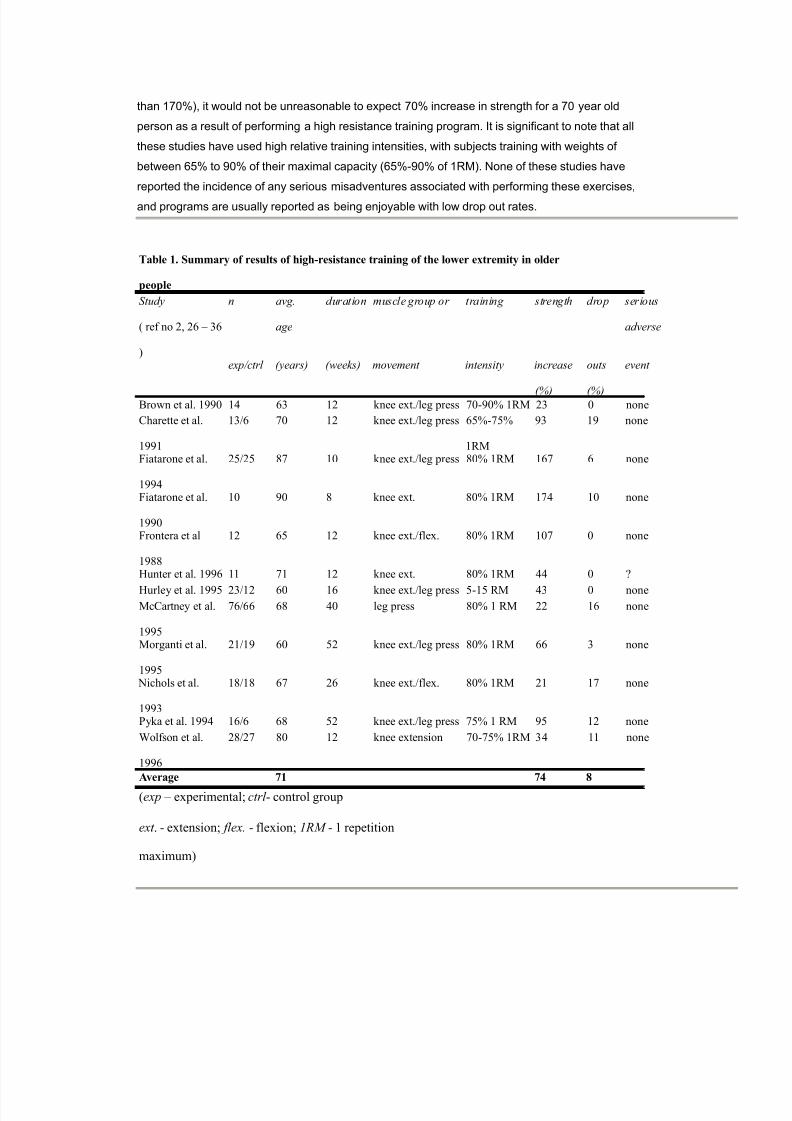
Lean body mass in aged master athletes is maintained into the seventh decade after which it
declines (1). Most of these athletes are participating in endurance training and not resistance
training. Individual examples of very active aged athletes participating in resistance training in
whom little loss of muscle mass is observed over an extended period. On the other hand the typical
80 year old will demonstrate a 30% to 40% decline in the voluntary strength of the muscles of the
leg, arm and back compared to subjects aged 30 years. A significant portion of older people will
experience much larger declines than this average and can be said to define the 'frail elderly'. The
marked loss of muscle strength in the frail elderly not only results in a barrier to participation in
recreational pursuits, but also presents a major hindrance to their ability to perform basic activities
of daily living (ADL).
Several common interrelated factors which often coexist to produce reduced physical activity
include; undernutrition (2), depression, social isolation and muscle weakness (3). Reduced
physical activity exacerbates these factors thereby creating a vicious cycle of progressive inactivity
and accelerated muscle weakness (3). Muscle weakness is well correlated with impaired mobility
and ability to perform ADLs and predicts poor health outcomes, institutionalisation and impaired
incidence of nursing home admission among residents in hostel care (22) and increased risk of
osteoporotic fracture - for example, older Australian males who have a strength deficit of the knee
extensors of one standard deviation or more below the mean have more than double the risk of hip
fracture (23).
Causes of muscle weakness (24,25)
Biological changes of aging and disuse.
Many changes in muscle function and composition which have been described in various otherwise
healthy populations of older people have been attributed to aging per se. It is important however to
note that these changes have been documented in populations of relatively sedentary older
people. On the basis of these studies, it is not possible to separate the effects of long standing
underuse of muscle from the changes associated with healthy optimal aging. A decline in muscle
mass and strength occurs in both sedentary and endurance athletes with age. On the basis of a
small number of individuals studied who have maintained resistance training well into old age, itmay be that muscle mass may decline to a relatively minor degree on the basis of aging alone. The
muscle architectural and microscopic changes of disuse and average aging are very similar.
Undernutrition
Undernutrition has been documented to occur in 20 - 65 % of older people. Based on animal and
human studies protein calorie malnutrition is associated with altered morphology (reduced fiber
One important question is- whether lower limb strength training increases indexes of mobility in
older subjects? Several studies have demonstrated very significant gains in strength in very frail
institutionalised residents. Fisher et al noted improvements in subjects whose initial muscle force
averaged only 50% aged matched controls (37). One of the best studies was by Fiatarone and co-workers demonstrated in a randomised study of 100 frail elderly subjects of average age 87-90
years within a residential setting, that high-resistance strength training three days per week is
effective in increasing functional capacity (2). Of the subjects in this study, 83% required a walking
aid, 66% had fallen during the previous year. Many subjects suffered multiple chronic diseases;
most commonly a history of osteoporotic fracture (44%),arthritis (50%), pulmonary disease (44%),
and hypertension (35%) Cognitive impairment was found in over 50% and 35% met criteria for
depression. After 8-10 weeks of high-intensity strengthening exercise the knee and leg extensor
strength increased in these subjects approximately 170% and 30% respectively. These changes
were associated with significant increases in habitual walking velocity (8-15%), stair climbing
capacity (23-34%), balance ability (48%) and overall level of physical activity (17-51%). Some of
these large responses probably reflect altered patterns of motor unit recruitment, but increases of
muscle mass from 12% to 17% have also been demonstrated by objective radiological techniques
(2,25,32,33) .
In contrast, mixed training programs which include only low resistance high repetition and aerobic
training, produce modest or no improvement (38). For example Mulrow et al describes a 4 month
mixed program combining range-of-motion, strength, balance, transfer and mobility exercises for
frail nursing home residents. The intervention resulted in no significant changes in strength or in
any of the other primary outcome measures (39).
In Fiatarone's study, nutritional intervention with exercise vs exercise alone showed a trend toimproved muscle strength which did not reach significance. Total protein intake was not reported.
Meridith et al found benefit from the daily ingestion of a supplement that added 0.33 g/kg of protein
and 33kJ/kg og food energy to the usual diet (40).
Adverse effects
As demonstrated in the table, high resistance training is associated with little in the way of adverse
effects. Some authors have noted reductions in bodily pain and no adverse effects exercising
arthritic knees. Other authors report reduced arthritic symptoms. Patients require a period of
supervised acclimatisation and build up before high resistance commences. This period should be
approximately one to two weeks.
It is important to note that low adverse effects relate to the relatively low maximal strength of
weaker elderly subjects. Hunter et al found that younger subjects suffered more adverse symptoms
than older subjects (30).
Safety in chronic active medical conditions
Generally speaking, frailty and arthritis present no barriers to resistance training. Significant