ACTA OPHTHALMOLOGICA 67 (1989) Supplementum 192 The optical quality of the peripheral cornea David Miller, Neal Atebara and Robert Stegmann’ Department of Ophthalmology (Head: C. Dohlman) Harvard Medical School, Boston MA, USA, and Department of Ophthalmology’(Head: R. Stegmann), Medical University of Southern Africa Abstract. The cornea can be considered to be an organ divided into a central and peripheral zone. Although the central cornea is responsible for producing a sharp reti- nal image, our experiments suggest that areas of isolated peripheral cornea can produce retinal images compat- able to 20/30 visual acuity. Key words: cornea - corneal periphery - corneal optics - optical iridectomy - optical bipass - iridodialysis. The concept of the cornea divided into a central zone or cap and a flatter periphery was originated by Aubert in 1885. The concept has the support of topographic studies of the corneal surface (Rzymkowsky 1954; Reynolds 1959; Knoll 1961; Mandell 1965). Al- though there exists a great deal individual varia- tion, in general the studies show the cornea to have a central zone of constant and symmetrical curva- ture, of between 4 to 6 mm in diameter. A central corneal zone of 4 to 6 mm is also in keeping with optical theory which suggests that the central zone should be about the size of the entrance pupil of the eye. In the photopic eye, this should measure about 4.5 mm (Miller & Carter 1988). These fmd- ings are also consistent with studies modeling a clear corneal transplant surrounded by a cloudy host cornea. They show that a minimum central clear area of about 5 mm is needed to maximize contrast in the face of veiling glare (Miller & Wolf 1969). Does the corneal periphery have an optical func- tion? We have some clues from the experimental lit- erature, demonstrating some unique properties of the corneal periphery which help in maintaining good vision. The peripheral flattening diminishes the spheri- cal aberration of the cornea, allowing for sharp im- ages even when the pupil dilates. Fig. 1 shows the widening of a bar of light pro- duced by the peripheral bovine cornea (Le Grand 1967). The wider image connotes a flatter curva- ture in the periphery, which would correct spheri- cal aberration. Can an isolated region of the peripheral cornea, in and of itself, form a clear image on the retina? Reports on visual acuity through an optical iri- dectomy range from ‘disappointing‘ and always less than 6/60 (Philps 1961) to 20/40 (Aijian 1955). This variation may also be related to the fact that an eye requiring optical iridectomies for an opaque central cornea may also have disease of the lens and retina. Thus, in this study, we attempted to determine the optimal image formingpotential of the periph- eral cornea using a) optical bench techniques, b) simulation experiments on normal subjects and c) clinical cases. Methods Fig. 2 describes an optical experiment in which a camera was placed on an optical bench with an il- luminated Snellen chart as the object. An opaque 165
Transcript
A C T A O P H T H A L M O L O G I C A 67 (1989) Supplementum 192
The optical quality of the peripheral cornea
David Miller, Neal Atebara and Robert Stegmann’
Department of Ophthalmology (Head: C. Dohlman) Harvard Medical School, Boston MA, USA, and Department of Ophthalmology’ (Head: R. Stegmann), Medical University of Southern Africa
Abstract. The cornea can be considered to be an organ divided into a central and peripheral zone. Although the central cornea is responsible for producing a sharp reti- nal image, our experiments suggest that areas of isolated peripheral cornea can produce retinal images compat- able to 20/30 visual acuity.
The concept of the cornea divided into a central zone or cap and a flatter periphery was originated by Aubert in 1885. The concept has the support of topographic
studies of the corneal surface (Rzymkowsky 1954; Reynolds 1959; Knoll 1961; Mandell 1965). Al- though there exists a great deal individual varia- tion, in general the studies show the cornea to have a central zone of constant and symmetrical curva- ture, of between 4 to 6 mm in diameter. A central corneal zone of 4 to 6 mm is also in keeping with optical theory which suggests that the central zone should be about the size of the entrance pupil of the eye. In the photopic eye, this should measure about 4.5 mm (Miller & Carter 1988). These fmd- ings are also consistent with studies modeling a clear corneal transplant surrounded by a cloudy host cornea. They show that a minimum central clear area of about 5 mm is needed to maximize contrast in the face of veiling glare (Miller & Wolf 1969).
Does the corneal periphery have an optical func- tion?
We have some clues from the experimental lit- erature, demonstrating some unique properties of the corneal periphery which help in maintaining good vision.
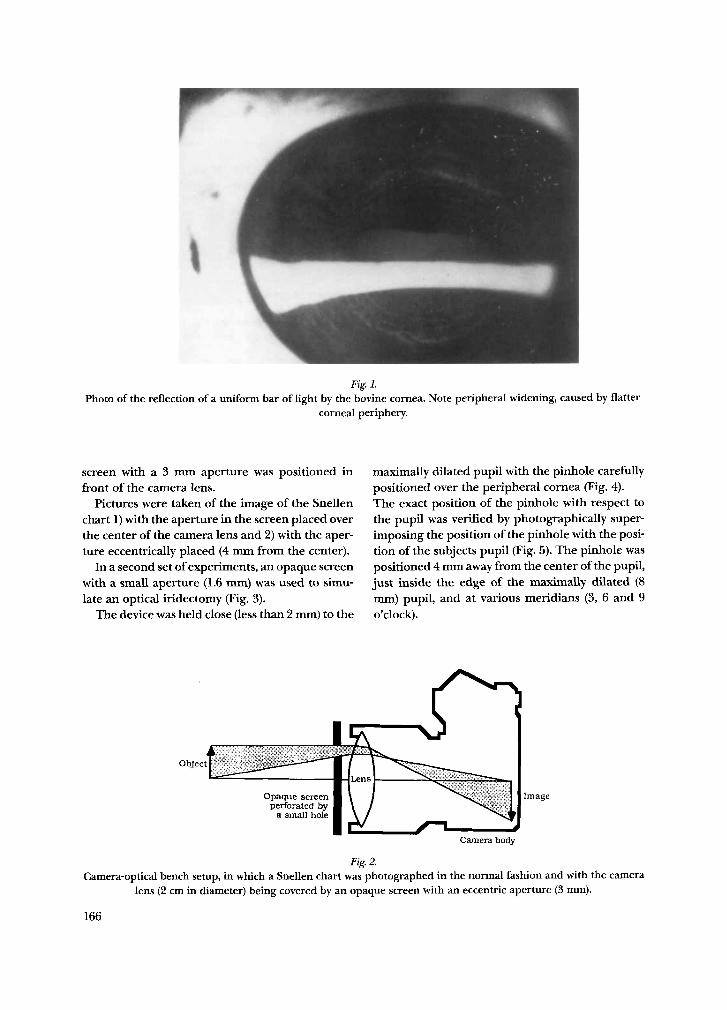
The peripheral flattening diminishes the spheri- cal aberration of the cornea, allowing for sharp im- ages even when the pupil dilates.
Fig. 1 shows the widening of a bar of light pro- duced by the peripheral bovine cornea (Le Grand 1967). The wider image connotes a flatter curva- ture in the periphery, which would correct spheri- cal aberration.
Can an isolated region of the peripheral cornea, in and of itself, form a clear image on the retina?
Reports on visual acuity through an optical iri- dectomy range from ‘disappointing‘ and always less than 6/60 (Philps 1961) to 20/40 (Aijian 1955). This variation may also be related to the fact that an eye requiring optical iridectomies for an opaque central cornea may also have disease of the lens and retina.
Thus, in this study, we attempted to determine the optimal image formingpotential of the periph- eral cornea using a) optical bench techniques, b) simulation experiments on normal subjects and c) clinical cases.
Methods
Fig. 2 describes an optical experiment in which a camera was placed on an optical bench with an il- luminated Snellen chart as the object. An opaque
165
Fig. I. Photo of the reflection of a uniform bar of light by the bovine cornea. Note peripheral widening, caused by flatter
corneal periphery.
screen with a 3 mm aperture was positioned in front of the camera lens.
Pictures were taken of the image of the Snellen chart 1) with the aperture in the screen placed over the center of the camera lens and 2) with the aper- ture eccentrically placed (4 mm from the center).
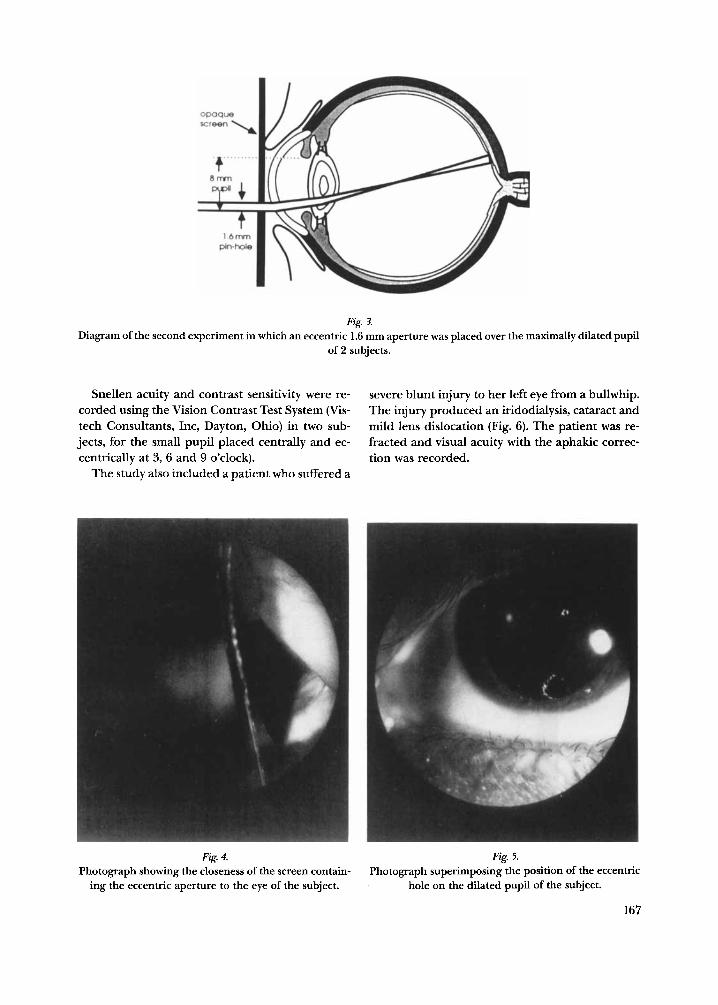
In a second set of experiments, an opaque screen with a small aperture (1.6 mm) was used to simu- late an optical iridectomy (Fig. 3).
The device was held close (less than 2 mm) to the
maximally dilated pupil with the pinhole carefully positioned over the peripheral cornea (Fig. 4). The exact position of the pinhole with respect to the pupil was verified by photographically super- imposing the position of the pinhole with the posi- tion of the subjects pupil (Fig. 5). The pinhole was positioned 4 nun away from the center of the pupil, just inside the edge of the maximally dilated (8 mm) pupil, and at various meridians (3, 6 and 9 o'clock).
Objr 'C
Opaque screen perforated bv
a small hofe I ~ \ lrnage
Camera body
Fig 2. Camera-optical bench setup, in which a Snellen chart was photographed in the normal fashion and with the camera
lens (2 cm in diameter) being covered by an opaque screen with an eccentric aperture (3 mm).
166
Fig. 3. Diagram of the second experiment in which an eccentric 1.6 mm aperture was placed over the maximally dilated pupil
of 2 subjects.
Snellen acuity and contrast sensitivity were re- corded using the Vision Contrast Test System (Vis- tech Consultants, Inc, Dayton, Ohio) in two sub- jects, for the small pupil placed centrally and ec- centrically at 3, 6 and 9 o’clock).
The study also included a patient who suffered a
severe blunt injury to her left eye from a bullwhip. The injury produced an iridodialysis, cataract and mild lens dislocation (Fig. 6). The patient was re- fracted and visual acuity with the aphakic correc- tion was recorded.
Fig. 4. Fig 5. Photograph showing the closeness of the screen contain-
ing the eccentric aperture to the eye of the subject. Photograph superimposing the position of the eccentric
hole on the dilated pupil of the subject.
167
Fig. 6. Photograph of the eye of a patient with a bullwhip induced cataract, and indodialysis
(courtesy Robert Stegmann, MD).
through the same aperature, this time positioned over the periphery of the camera lens.
Note, most lines of the chart can be seen, al- though the contrast using the peripheral aperture is poorer.
Visual acuity for each of the two subjects looking
Results
Fig. 7 left, is the control photo of the Snellen chart, taken with the small aperture of the opaque screen positioned over the center of the camera lens. Fig. 7 right, is the the picture of the chart taken
Fig. 7. The photograph of the Snellen chart on the left was taken in the normal manner. The photograph on the right was
taken with the same camera, but through the eccentric aperture over the camera lens.
168
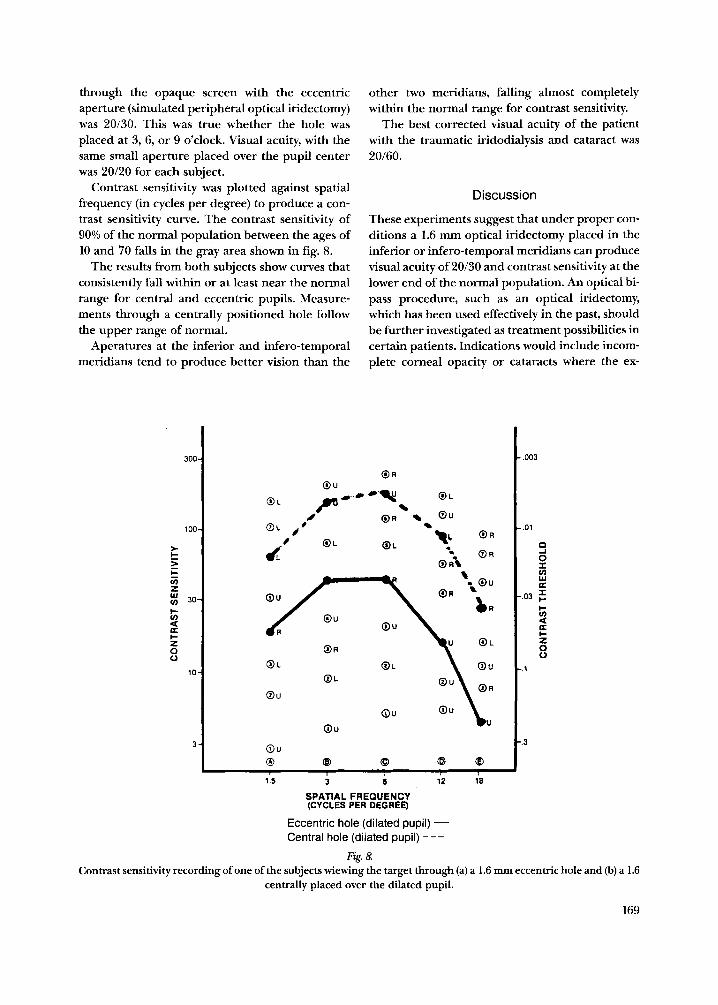
through the opaque screen with the eccentric aperture (simulated peripheral optical iridectomy) was 20/30. This was true whether the hole was placed at 3, 6, or 9 o'clock. Visual acuity, with the same small aperture placed over the pupil center was 20/20 for each subject.
Contrast sensitivity was plotted against spatial frequency (in cycles per degree) to produce a con- trast sensitivity curve. The contrast sensitivity of 90% of the normal population between the ages of 10 and 70 falls in the gray area shown in fig. 8.
The results from both subjects show curves that consistently fall within or at least near the normal range for central and eccentric pupils. Measure- ments through a centrally positioned hole follow the upper range of normal.
Aperatures at the inferior and infero-temporal meridians tend to produce better vision than the
other two meridians, falling almost completely within the normal range for contrast sensitivity.
The best corrected visual acuity of the patient with the traumatic iridodialysis and cataract was 20/60.
Discussion
These experiments suggest that under proper con- ditions a 1.6 mm optical iridectomy placed in the inferior or infero-temporal meridians can produce visual acuity of 20/30 and contrast sensitivity at the lower end of the normal population. An optical bi- pass procedure, such as an optical iridectomy, which has been used effectively in the past, should be hrther investigated as treatment possibilities in certain patients. Indications would include incom- plete corneal opacity or cataracts where the ex-
Contrast sensitivity recording of one of the subjects wiewing the target through (a) a 1.6 ~LII eccentric hole and (b) a 1.6 centrally placed over the dilated pupil.
169
pensive, highly technical, and resource-demand- ing operations are unavailable.
In truth, the majority of the world's surface is se- verely deficient in ophthalmologists, eye banks, technical equipment, and medical resources and is, therefore, deprived of conventional, first world, vision-restoring operations. The majority of the world's 30 million blind people reside in Develo- ping Countries, primarily in the more rural areas. Africa alone has up to 5 million blind (IABP 1984), and the Middle East has approximately 7.5 million blind (IABP p 32). Worldwide, approximately 17 million are blind due to cataract (IABP p 8) and about 6-9 million due to corneal scarring.
Because of the enormity of the number of blind worldwide and the relative scarcity of medical re- sources, the authors propose that optical bipass operations, operations like the optical iridectomy or optical iridodialysis, should be considered as one approach to ameliorationg to the problem of world blindness.
References
Aijian K M (1955): Optical iridectomy: Results in Nine Eyes. Am J Ophthalmol39: 866-867.
Aubert H (1985): Nahert sich die Hornhaut Krummung am meisten der Ellipse. Pfluger's Arch Geo Physiol35: 597-621, 1885.
Duke Elder S (1970): A System of Ophthalmology. Vol V Ophthalmic Optics and Refraction, p 131: H. Kimpton, London.
IAPB (1984): (International Agency for the Prevention of Blindness) World Blindness and Its Prevention. Vol 2, p 8, p 18, p 32. Oxford University Press.
Knoll H (1961): Corneal contours in the general popula- tion as revealed by the photokeratoscope. Am J Optom
LeGrand Y (1967): Form and Space Vision, pp 24-59. Translated by Milladot M & Heath G G. Indiana University Press. Bloomington, IN.
Mandell R B (1965): Contrast Lens Practice: Basic and Advanced C. L. pp 42-44. Thomas, Springfield IL.
Miller D & Carter J (1988): A proposed new division of corneal functions. In: Cavanagh D (ed). Third World Congres on the Cornea. pp 155-159. Raven Pres, New York.
Miller D & Wolf E (1969): A model for comparing optical properties of different sizes corneal grafts. Am J Oph- thalmol67: 724-728.