61
THE PHYSICIAN RECRUITING MAKEOVER: HOW TO MAKE YOUR FACILITY A DOCTOR MAGNET Presented to: The GHA Center for Rural Health Annual Meeting
| Date post: | 16-Dec-2015 |
| Category: |
Documents |
| Upload: | allen-richard |
| View: | 216 times |
| Download: | 0 times |
THE PHYSICIAN RECRUITING MAKEOVER:
HOW TO MAKE YOUR FACILITY A DOCTOR MAGNET
Presented to: The GHA Center for Rural Health Annual Meeting

PHYSICIAN RECRUITING IN 2013
THERE’S GOOD NEWS AND BAD NEWS

FIRST, THE BAD NEWS
THE PHYSICIAN SHORTAGE IS LIKELY TO GET WORSE BEFORE IT GETS BETTER

50 million more people from 2000 to 2020
(we will be adding the
population of England)
RISING DEMAND

RISING DEMAND
150,000,000 Additional Physician Visits Per Year By 2020 Based On Population Growth Alone(3.0 visit per/pop X 50 million population growth)
Does not factor in age
demographic

75 MILLION BABY BOOMERS BEGAN TURNING 65 IN 2011

PATIENT VISITS BY AGE
0-15 yrs.
16-24 yrs.
23-35 yrs.
35-45 yrs.
46-65 yrs.
66+ yrs.
0.0 1.0 2.0 3.0 4.0 5.0 6.0 7.0
2.0
1.5
2.2
3.4
5.4
6.0
Physician Visits By Age
# of Annual Visits
Source: National Ambulatory Medical Care Survey; www.cdc.gov

FLORIDA IS OUR FUTURE
By 2030, the entire country will be as old, on average, as Florida
is now.
Source: U.S. Census Bureau

PHYSICIAN SUPPLY HAS BEEN STATIC FOR ABOUT 20 YEARS
24,000 – 25,000 new doctors per year
SUPPLY STATIC

A Voice for Physicians
10
THE PHYSICIANS FOUNDATION
www.physiciansfoundation.org
New Survey Available in September 2014

SHRINKING FTEs
The Physicians Foundation reports physicians are working 6% fewer hours versus four years ago…
A loss of 44,000 FTEs
Source: The Physicians Foundation/ Merritt Hawkins 2012 Survey of America’s Physicians

CHANGING WORK PATTERNS
• Physicians are seeing 16.5% fewer patients per day than in 2008
• They are working 6% fewer hours• They spend 22% of their time on non-clinical
paperwork
Source: A Survey of America’s Physicians: Practice Patterns and Perspectives, The Physicians Foundation/Merritt Hawkins, 2012
RESULT: A “SILENT EXODUS”
• A 6% reduction in work hours = a loss of 44,250 FTEs
• 16.5% fewer patients seen per = over 100 million fewer patient encounters
• 22% of time spent on paperwork = a loss of over 165,000 FTE’s

HOW MANY MORE PCs?
30 million newly insured patients X
2 additional patients visits per year=
60 million patient visits divided by
4,000=
15,000 additional primary care doctors
Source: The Lewin Group

PROJECTED SHORTAGE OF PHYSICIANS BY SPECIALTY BY 2025
Doctor Deficits
Primary care………46,000 (37% deficit)
Surgery……………….41,000 (33% deficit)
Other patient care…29,000 (23% deficit)
Medical specialties….8,000 (7% deficit)
Source: Association of American Medical Colleges/Modern Healthcare/December 1, 2008

GEORGIAPHYSICIAN WORKFORCE
Georgia State Median Rank
214.7 244.5 39th
Georgia State Median Rank
76.1 90.3 41st
Active Physicians per 100,000
Active Primary Care per 100,000
Source: 2013 State Physician Workforce Data Book

Georgia State Median Rank
31.4% 30.8% 22nd
Georgia State Median Rank
20.6% 18.2% 22nd
Percentage of Active Female Physicians
Percentage of International Medical Graduates
Percentage of Active Physicians Age 60 or Older
Georgia State Median Rank
24.7% 26.5% 43rd
Source: 2013 State Physician Workforce Data Book
GEORGIAPHYSICIAN WORKFORCE

NOW, THE GOOD NEWS
Physicians are seeking alternatives…
Is your grass greener?
Footer Text: Detail/Disclaimer 01/07/10
Recruitment Process
• Opportunity Analysis– Objective review of the opportunity
• What are the strengths? What are the challenges?– Four Quadrants
• Quality of Life • Quality of Practice• Geographic Location• Financial opportunity
– Practice positioning• No opportunity is all things to all people• How do you stand out? How are you different?

Footer Text: Detail/Disclaimer 01/07/10
How do we stand out in a crowded market?
• In rural America, 50-60% of the hospitals are actively recruiting primary care.
• What differentiates our opportunity from all of the hospitals in a 100 mile radius?– Work schedule (5 days, 4 days, extended
hours)– Outpatient vs. Traditional– Daily hours– Be flexible

Footer Text: Detail/Disclaimer 01/07/10
Inpatient care
• Hospitalist program– Neighboring community hospitalist group– Independent service provider– Have local physician provide hospitalist
service• Provide call coverage compensation
– Impacts candidate profile– ED physician assistance– Pediatrics
Footer Text: Detail/Disclaimer 01/07/10
How do we bring the physician into our community?
• Hospital employment model– New recruits looking for employed position– Local physicians looking to leave PP
• Private practice model– Partnering with practice groups
• Local• Neighboring community
– Community health center– Solo private practice

Sharing Common Vision
74% of hospital leaders say they plan to employ a greater percentage of physi-cians in the next 12-
36 months. 74% Yes26% No
Source: HealthLeaders Media | IntelligencePhysician Alignment in an Era of ChangeSeptember, 2010
23
71% of hospital leaders say they have received in-
creases in requests from physician groups for em-
ployment.71% Yes29% No

Footer Text: Detail/Disclaimer 01/07/10
Think outside the box
• Strategic community partners– Community Health Centers
• http://gaphc.org/ Primary Care Association• Duane Kavka, Executive Director• NACHC
– Physician employment organizations

Footer Text: Detail/Disclaimer 01/07/10
Build a firm foundation
• Establish a recruitment process from the start to the arrival of the new physician– Finalized contract and Letter of Agreement
(LOA)!!!– Defined roles on your team– Have a project orientation vs. an ongoing
process• All efforts toward concluding the search effort and
don’t stop until the search is completed.• Have a 120 day time frame for completion

Footer Text: Detail/Disclaimer 01/07/10
Build a firm foundation
• Compensation/Benefits– How is salary determined?– Production bonus?– Benefits
• Vacation• Sign on bonus (forgivable loan)• Retirement• Be aware of the value of your benefit package

Footer Text: Detail/Disclaimer 01/07/10
Who are we looking for?
• Candidate profile• Cast a wide net• % of physicians are 46 and older• International Medical graduates• Candidates on visas (Shusterman.com)
– Understand what is needed to recruit a physician on a visa
– Treat them the same as all other physician recruits
• Specialty• Advanced practitioners (NP/PA in our top 10)• Primary Care (IM, FP, PED, HOSP) are 4 of the top
most frequently requested specialties in our 2014 survey.
ARE PA’S AND NP’s THE ANSWER?
83,000 Physicians Assistants 2/3 in specialties 1/3 in primary careMedian salary: $91,000
155,000 Nurse practitioners75% in primary care25% in specialtiesMean salary: $93,310
A 20% deficit of by 2025
Source: American Academy of Physician Assistants, American Academy of Nurse Practitioners, “Physician shortage isn’t the only looming one,” Advance for Nurse Practitioners & Physician Assistants, July 28, 2011

BECOMING A DOCTOR MAGNET: A SOUND MODEL IS A GOOD BEGINNING
A SENSE OF URGENCY
Hospitals, medical groups, CHCs – all are looking for the same doctor you are
LEAVE NO STONE UNTURNED
Physician conventions
Networking with staff/community/residencies
The Internet (your site, employment sites, the Chamber site)
Direct mail (for “passive” candidates)
Journal ads (focus on residents)
High-need doctors (residents, military, J-1s)
SOURCING CANDIDATES

MEASURABLE ACTIVITY =
MEASURABLE RESULTS
SOURCING CANDIDATES

SOMEONE HAS TO GET ON THE PHONE
Usually after hours or on weekends
Suggested Telephone Metrics/In-House Recruiters
100 dials per week10 physician contacts per week3 Healthcare Center opportunity presentations1-2 candidate referrals from physicians contacted1 potential candidate sourced per week
SOURCING CANDIDATES

SCREENING
“Leave your practice, Doctor, take your kids out of school, sell your home, and quit the country club,
because have I got the deal for you. Trust me.”
HOW DO YOU GO FROM STRANGER TO CONFIDANT?

A CANDIDATE IS ON THE PHONE
THE “SCREEN” IS THE “ART” OF PHYSICIAN RECRUITING, AND A KEY PART OF THE “ICEBERG”
SCREENING
NOW, WHAT DO YOU SAY?

Footer Text: Detail/Disclaimer 01/07/10
Screening/Qualifying Physicians
• Motivation(s) for change– Why are they leaving their current position?
• Is it personal? Professional? Both?
• Candidate professional & personal goals– Spouse goals– Family goals
• What follows the physician screen?– Opportunity presentation

Objectives Of The Screen
Build relationship/rapport with
candidate
Identify motivations (personal or
professional)
Understand candidate’s priorities/goals
Consultatively address needs vs. wants
Determine whether candidate is a
good long-term fit for you
Screening, Know the Roles

WHO THEY ARE: Understanding each physician is the key to retention, and they won’t care how much you know, until they know how much you care:
• Family Considerations• Hobbies & Non-Practice Activities• Training & Previous Experience • Research & Subspecialty Interests• Work Ethic & Desired Schedule• Patient Encounter & Volume Preferences• Practice Management Involvement• Income Expectations• Professional Goals• Personal Goals
37
Screening, Know the Roles
Family Considerations• Where were they born and raised?• Are their parents still living? • Do they have any siblings? What are their siblings
professions? • Where do their extended family members live?• How often do they travel to spend time with family?• Are they married? • Does their spouse work outside the home?• Do they have any children? • What are their children’s interests?
38
Screening, Know the Roles

Hobbies & Non-Practice Activities• Do they exercise?• Where do they vacation?• Do they play a musical instrument?• What do they do during evenings and weekends?• What are their favorite television shows?• Where do they live? How is that neighborhood?• Is their commute reasonable?• Are they a member of a local religious institution or
social organization?• Is the physician rooted in the community?
39
Screening, Know the Roles
Training & Previous Experience • Where did they go to medical school?• What program provided their Residency and/or
Fellowship training?• Are there other members of the medical staff that also
attended these schools?• What other positions have they previously held?• Do they have skills developed in prior opportunities that
could benefit this current role?• Why did they relocate from any earlier practices?• Is their present job fulfilling prior unmet needs?
40
Screening, Know the Roles

Research & Subspecialty Interests• Do they have Fellowship training which is being under
utilized?• What research projects and/or clinical studies are listed
on their CV?• Have they expressed interest in developing programs or
niche services (for which they’re qualified) within the local market?
• Is there an opportunity for them to provide these services or does supply/demand and demographics preclude success in this style of practice?
41
Screening, Know the Roles

Work Ethic & Desired Schedule• Are they intent on building a practice or just in being
paid for their time? Are their expectations reasonable?• Have they requested scaling back to part-time?• How many hours would they like to work?• What are the needs of the community relative to the
physician’s desired contributions?• How can on-call responsibilities be structured in a
tolerable manner?• Do they tend to stay until the last patient is seen, or
make sure to get home on time for personal reasons?• Are they open to the recruitment of additional doctors?
42
Screening, Know the Roles

Patient Encounter & Volume Preferences• What is the health system’s expectation for productivity,
and does the physician believe this is both realistic and commensurate with the compensation model?
• How many patients would the physician like to see per (day, week, year, etc.) in clinic and/or the hospital?
• Would the physician like a slower patient flow and correspondingly lower income?
• Is there adequate consideration for patient appointment times relative to new patients vs. return visits?
• Are satellite locations, and trips back and forth from the office to the hospital causing logistical difficulties and decreasing available time to see patients?
43
Screening, Know the Roles
Practice Management Involvement• How much involvement would the physician like in the
day to day operations of the practice?• Does the physician possess the necessary business
acumen to run an office with staff, or lead a team with other doctors?
• Do they expect to show up at a designated location, at a set time, and simply see the patients that have been scheduled for them?
• If this physician has run a successful practice previously, are their ideas and suggestions being solicited, appreciated and implemented?
44
Screening, Know the Roles

Income Expectations• Is the originally agreed upon base remuneration still in effect? Is the
physician exceeding the guarantee?• Does the physician feel the financial potential of the practice was
honestly represented during recruitment?• Is there adequate demand in the service area for the physician to earn
the income they would like? • Does the physician have an accurate sense of financial benchmarking
data, and are they able to determine if their current productivity is being appropriately compensated relative to national norms?
• Is the demography and payer mix in the market able to accommodate a normal income range, and if not, are both the employer and physician open to exploring alternative compensation models?
• When assessing the impact of the practice, are both the physician and hospital cognizant of factors beyond the doctor’s Professional Charges (i.e. non-physician providers, ancillaries, inpatient revenue, etc.)?
45
Screening, Know the Roles
Professional Goals• Does the doctor aspire to a Medical Director role or a “C”
level position within the health system? • Is the physician content with their current practice style
and apprehensive about additional responsibilities?• Do they want to continue working in the community but
run their practice privately?• Is it possible to build a hospital employed group around
this physician leader? • Will the physician likely need to pursue opportunities
elsewhere to achieve this perceived advancement? • Would the physician like to change their position, to slow
down nearing retirement, or have more time for family?
46
Screening, Know the Roles

Personal Goals• Would the physician like to move to be closer to family?• Do they have significant student loans or other personal
obligations motivating them to earn greater income?• Are there changes in their marital status or children
altering their professional focus and commitments? • Does the physician need training or support in
developing their interpersonal communication skills?• Is there a negative relationship with a colleague,
administrator or staff that needs to be addressed? • What are the goals of the physician’s spouse and how
are these impacting the families professional decisions?
47
Screening, Know the Roles

Opportunity Presentation
– This is your one shot!– Comprehensive presentation
• Community– Broad to narrow focus on region
• Opportunity• Hospital• Financial package
– Salary + realistic financial expectations
– Email follow up that day with supporting documents/web links / presentation summary
– Telephone follow up within 4-5 days with confirmed next steps
Edit Footer Text 01/07/1048
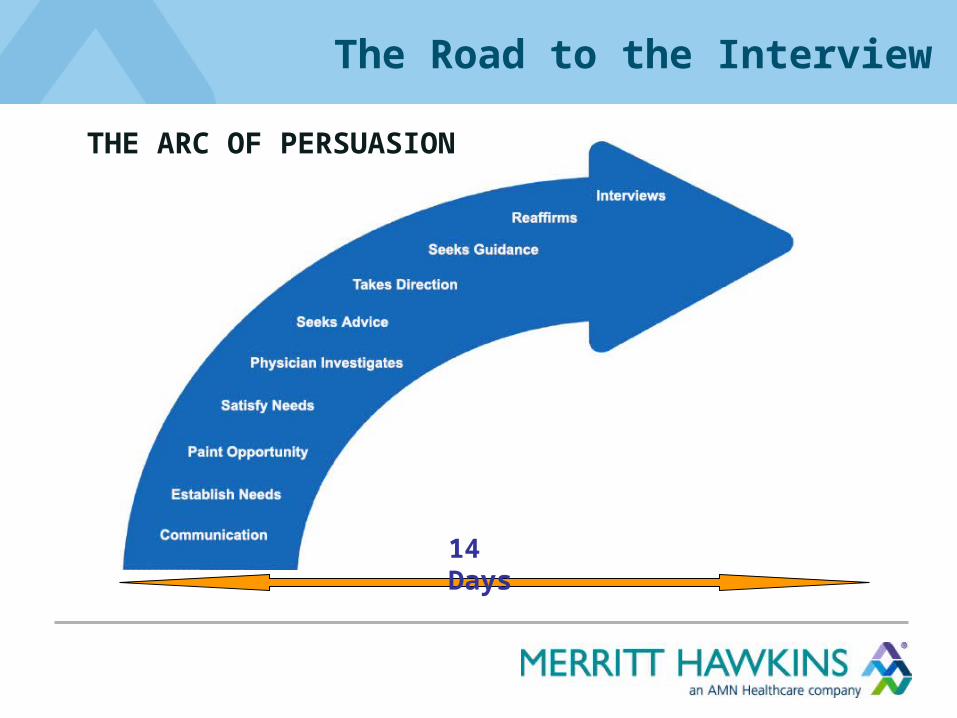
14 Days
THE ARC OF PERSUASION
The Road to the Interview

Footer Text: Detail/Disclaimer 01/07/10
Candidate Interview
• One interview process with Physician and spouse
• 70% Social• Recruitment team to include community
members of similar age and station in life
• Separate spouse interview• Confirmation, not exploration• Goal is to secure physician

NOW, THE STAGE IS SET
You know your candidate (written profile, professional and personal)
The candidate knows you (setting, hours, finances, mission, etc.)
Your offer is readyYour team is readyThe interview itinerary is ready
THE INTERVIEW
You’ve got a lot of sweat equity in this search, BUT…
EXPECTATIONS ARE CLEAR on both sides.

THE PYRAMID OF INTEREST
THE DECISION

Footer Text: Detail/Disclaimer 01/07/10
Educational loan repayment
• http://nhsc.hrsa.gov/loanrepayment/• National Health Scholarship Program
– Become an NHSC site– $30,000 - $50,000 loan repayment over a
two year period

THE VALUE OF PHYSICIANS TO HOSPITALS
2014 Physician Inpatient/
Outpatient Revenue Survey
PHYSICIAN GENERATED REVENUE
• All Physicians………… $1,448,458• Primary Care………….$1,566,165• Specialists……………..$1,424,917
According to the Lewin Group, the economic value of a physician is $2.2 million

COST/BENEFITS

RETENTION
RETENTION AND RECRUITMENT ARE TWO SIDES OF THE SAME COIN
Basic Recruiter Truth 101
Physicians are not pulled
from their practices…
They are pushed.
Footer Text: Detail/Disclaimer 01/07/10
Candidate Retention
• Two years is the magic number– If a physician remains for 2-3 years, he/she
will establish roots in your community• Established retention program
– Spouse program– Formal process to monitor physician
onboarding for the first two years

SUCCESS!
Now, it is time to incorporate the new physician into the Retention
Program while the Recruitment Cycle begins again.

If you have any questions, please contact Mark Conley at:
Follow Us:

THE PHYSICIAN RECRUITING MAKEOVER:
HOW TO MAKE YOUR FACILITY A DOCTOR MAGNET
Presented to:

















