The Prescription Project: Ending Conflicts of Interest; Promoting Evidence-Based Prescribing Marcia Hams, Director of Prescription Policy Initiatives The Prescription Project National State Attorneys General Program Columbia Law School, 5/10/07
Transcript
The Prescription Project:Ending Conflicts of Interest;
Promoting Evidence-Based Prescribing
Marcia Hams, Director of Prescription Policy Initiatives
The Prescription Project
National State Attorneys General ProgramColumbia Law School, 5/10/07
The Prescription Project is a collaboration of
Community Catalyst andThe Institute on Medicine as a
Profession Funded by Pew Charitable Trusts
3
Community Catalyst is a national non-profit advocacy organization established in 1997 to increase consumer participation in shaping the U.S. health care system to ensure quality, affordable health care for all. It works in numerous states with state and local organizations as well as other national organizations.
Community CatalystCommunity Catalyst
4
The Institute on Medicine as a Profession seeks to shape a world inside and outside of medicine that is responsive to the ideals of professionalism. IMAP supports research on the past, present, and future roles of professionalism in guiding individual and collective behavior. It aims to make professionalism relevant to physicians, leaders of medical organizations, policy analysts, public officials, and consumers. IMAP’s programmatic agenda is carried out through the Center on Medicine as a Profession of Columbia University.
Institute on Medicine Institute on Medicine
as a Profession as a Profession
5
www.prescriptionproject.org
6
• Out of control industry marketing
• Industry influence in government
• Quality of care compromised
• Pharmaceutical costs out of control
• Consumers can’t afford their drugs
The ProblemThe Problem
7
• Industry spends $12B/year on drug marketing to MDs ($13,000/MD)
Advance practical public and private policy solutions to meet these goals among: – academic medical centers – medical professional societies– public and private purchasers – providers– policy makers/regulators– consumers and advocates
12
Drivers of Prescription ReformDrivers of Prescription Reform
• Consumers want access & affordability • Media and public opinion• Public and private payers seek to preserve programs and
benefits • States seek to sustain expansions of coverage/benefits • MDs and other providers who seek to reestablish trust in
medicine• The Quality Movement
13
Reducing Conflicts of Interest:Reducing Conflicts of Interest:Self-RegulationSelf-Regulation
• Academic Medical Centers• Professional Medical Societies
(which also publish Clinical Practice Guidelines)
• Hospitals and group practices
14
Journal of the American Medical Association January 25, 2006
(2006; 295: 429-433)
15
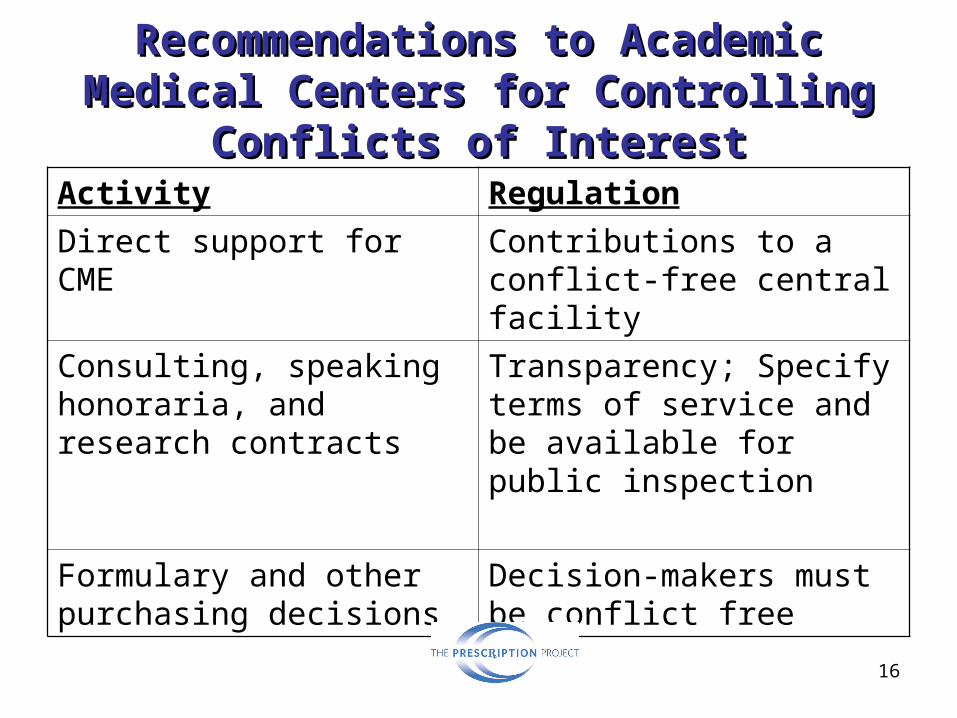
Recommendations to Academic Recommendations to Academic Medical Centers for Controlling Medical Centers for Controlling
Conflicts of InterestConflicts of InterestActivity Regulation
Gifts, meals directly to physician from industry
Eliminate
Provision of free samples, other patient-use products
Vouchers, other indirect distribution system
Speakers’ Bureaus and Ghostwriting
Eliminate
Payment for physician and trainee travel
Contributions to a conflict-free central facility
16
Recommendations to Academic Recommendations to Academic Medical Centers for Controlling Medical Centers for Controlling
Conflicts of InterestConflicts of InterestActivity Regulation
Direct support for CME Contributions to a conflict-free central facility
Consulting, speaking honoraria, and research contracts
Transparency; Specify terms of service and be available for public inspection
Formulary and other purchasing decisions
Decision-makers must be conflict free
17
Conflicts of Interest: Conflicts of Interest: Public Policy Solutions Public Policy Solutions
• Vermont statute (2002): Disclosure. Reports by AG on amounts to MDs (by specialty, not name)
• Minnesota statute (1993): $50 limit for gifts but many exemptions; disclosures published by Board of Pharmacy
• Maine (2003): disclosure of expenses>$25• West Virginia (2004): Broad disclosure but no individual
MD names
18
Evidence-based prescribing
• Expand reliance on evidence-based systematic reviews
• Expand use of generics• Implement academic/counter detailing • Prohibit sale of prescriber data for
industry marketing
19
Promote evidence-based Promote evidence-based reviews to shape reviews to shape
prescribing: public sectorprescribing: public sector
• Expand use of Drug Effectiveness Review Project to shape Preferred Drug Lists; now in13 states
• Statutory requirements to use EBM as basis for public purchasing (WA ’05; proposed in VT and MA ‘07)
20
Promote evidence-based Promote evidence-based reviews to shape prescribing: reviews to shape prescribing:
private sectorprivate sector • Create standards for accountability
• Minnesota Coalition utilizing DERP based CRBestBuyDrugs
• Health plan/insurer/employer interest
• Public/Private partnerships: Puget Sound Health Alliance
• Kaiser, Health Partners in-house• Potential for employer interest• Minnesota Coalition/payers using CRBest
BuyDrugs for MD education• Proposed ME and MA bills allows for
private plans to subscribe to public initiative
23
Academic Detailing: Academic Detailing: Evaluation and Best PracticesEvaluation and Best Practices
• Show Me the Evidence: Best practices for using educational visits to promote evidence-based prescribing A two-year evaluation program from
May 2004 to April 2006By the Canadian Academic Detailing
Collaboration and Drug Policy Futures
24
Programs Evaluated in the Programs Evaluated in the U.S. and CanadaU.S. and Canada
• Kaiser Permanente, Colorado; Brigham and Women’s Hospital, Harvard Medical School; Accessible Intelligent Medication Strategies, West Virginia; Veterans Administration, Greater Los Angeles
• B.C. Community Drug Utilization Program; Alberta Drug Utilization Program; RxFiles Academic Detailing Program, Saskatchewan; Prescription Information Services of Manitoba; Dalhousie Academic Detailing Service, Nova Scotia
• Will establish a preferred drug list based on Evidence Based Medicine and a prior authorization system for state programs
• Bans the sale of prescriber information unless the physician explicitly “opts-in”
• Requires PBM transparency and establishes required practices
31
Vermont S.115 Vermont S.115 cont.cont.
• Establishes an annual $1,000 manufacturer fee for each pharmaceutical company selling prescription drugs to state programs
• Establishes a pharmacy discount plan for certain seniors and individuals below a specified income threshold
• Prohibits “unconscionable pricing”
32
Vermont S.115Vermont S.115 cont. cont.
• Establishes an evidence-based prescription drug education program for state program health care professionals There may be collaboration with other states
in establishing the programIncludes establishment of a pilot program to