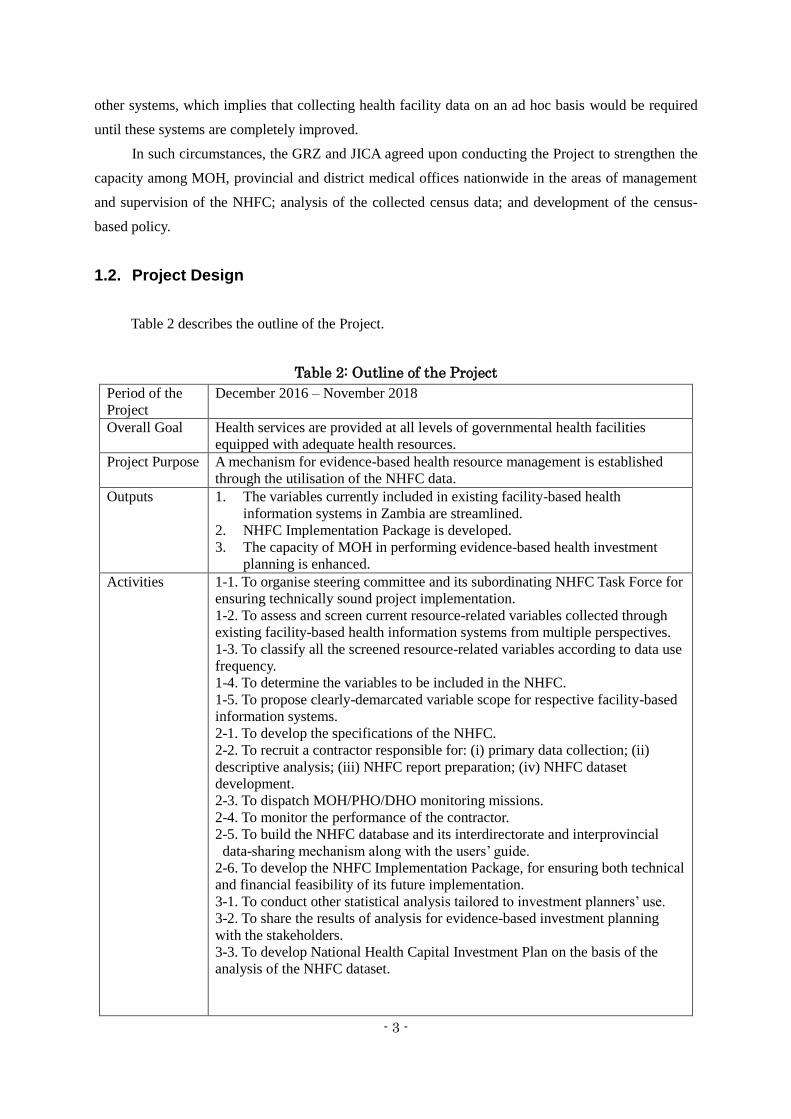
The Republic of Zambia Ministry of Health The Project for Strengthening the Capacity of Facility-Census-Based Health Investment Planning in The Republic of Zambia Project Completion Report March 2019 Japan International Cooperation Agency (JICA) TA Networking Corp. HM JR 19-012
The latest list of facilities and the most time efficient
route should be advised by PHOs and DHOs.
Water transport was not estimated regardless of
the fact that there are facilities that are not
reachable without water transport.
It was allocated from other expense items.
Facilities only accessible via water or air transport
should be counted in advance and budgeted for. If
budget is limited, other mean of collecting data (i.e.
phone interview) should be considered.
- 23 -
Challenges Countermeasures Recommendations
Responsible personnel was absent from the
facility at the time of visit.
Appointment was made through phone calls and
enumerators revisited the facilities.
DHOs should share the phone numbers of responsible
personnel at facilities. Enumerators should then make
appointment in advance.
Responsible personnel was too busy to receive
interviews.
Ditto Ditto
Some facilities refused to acknowledge the
enumerators.
Enumerators asked DHOs to call personnel at the facility
to allow access for enumeration.
MOH should announce the NHFC implementation
and its purpose at national, provincial and district
level meetings or through media.
Both application and tablet tended to crash. Paper based questionnaire was provided as back-up.
Supervisors brought tablets to the field at the timing of
supervision and exchanged.
Application should be carefully selected and
programmed to accommodate the heaviest data such
as infrastructure.
It took more time than estimated to collect data. Enumerators worked in groups of 2: while 1 enumerator
did the interview, the other enumerator took
measurements.
Dashboard was created to monitor performance of each
team and enumerator and shared with the entire team.
Team structures and car allocations should be
arranged for enumerators to work in groups of 2.
Dashboard for monitoring the performance should be
utilised from the beginning of data collection to
manage operational progress and to motivate
enumerators.
It took more time than planned to measure the plot
and buildings.
Measuring tape was utilised at the beginning but
distometers were procured and allocated for each team.
Distometers should be utilised from the beginning.
- 24 -
Challenges Countermeasures Recommendations
Some enumerators were not familiar with basic
health related knowledge.
Team members were changed based on basic health
related knowledge and performance level.
Data collection tools were revised to include the pictures
of each medical equipment.
Preparation period before commencing the data
collection should be secured in order to recruit well
qualified enumerators. Especially, each team should
have at least one enumerator who is conversant with
medical equipment.
Data collection should be started from Lusaka
province so that it is easier to monitor and supervise
the enumerators together with MOH officers.
Some team leaders did not play their role and the
team performance degraded in some cases.
TOR of field team leaders was created and shared with all
teams.
Team leader should be selected in advance and the
training for team leaders should be conducted
additionally.
Some enumerators left the team because they got
a new full-time job or enrolled in the school.
Additional training was conducted for 8 enumerators and
deployed to the field.
More enumerators should be trained as substitutes at
the beginning because these circumstances are likely
to occur.
Some enumerators got sick (e.g. malaria). Others
experienced burnout and left the team.
Malaria preventive medicine was distributed.
Insurance package was provided to enumerators.
As soon as completing the enumeration at the first
province, enumerators were given one-week break.
Ditto
- 25 -
Challenges Countermeasures Recommendations
Enumeration at Military or Police operating
facilities was restricted.
UNZA team asked Ministry of Defence and Ministry of
Home Affairs to produce a letter for permission to
enumerate the facilities.
Enumerators visited the facilities twice; first visit for
making appointment and second visit for enumeration.
MOH should spearhead to obtain security clearance
from other Ministries.
Accommodation allowance was more than it was
budgeted for.
It was allocated from other expense items. Higher rate should be applied to Solwedi, Kitwe,
Ndola and other urban cities as well as Lusaka and
Livingstone.
There was missing information. Follow-ups by phone calls
Skip function of the data collecting tool was improved
during the field work.
At the early stage of data collection, data should be
validated against what is observed on the ground.
MOH should cooperate in this exercise.
Data collecting application with skip functions
should be carefully selected.
Pre-tests should be conducted until missing
information is not recorded.
Two variables were omitted. Data was collected through phone interviews Pre-tests should be repeatedly conducted until data
collecting tools are finalised. Enumerators should
not be deployed until the tools are finalised.
- 26 -
Challenges Countermeasures Recommendations
Post-Data Collection Period
Data cleaning required more time than planned. MOH and JICA Experts gave the Contractor detailed
feedback.
Submission was extended.
Data cleaning should be planned for at least one
month
Data clashed on the main server. Enumerators visited the same facility when it was
possible. Otherwise it was considered as missing
information.
There should be a backup server prepared before the
census commences.
Structure of dataset was too complicated to run
analyses in the statistical software.
It was required to restructure the dataset in order to put
the data into the statistical software.
Utilising the pre-test data, basic analyses should be
conducted at the earliest stage so that the necessary
structure of dataset or design of data collecting tools
can be revised accordingly.
- 27 -
Termination of the Contract with the Data Collecting Contractor
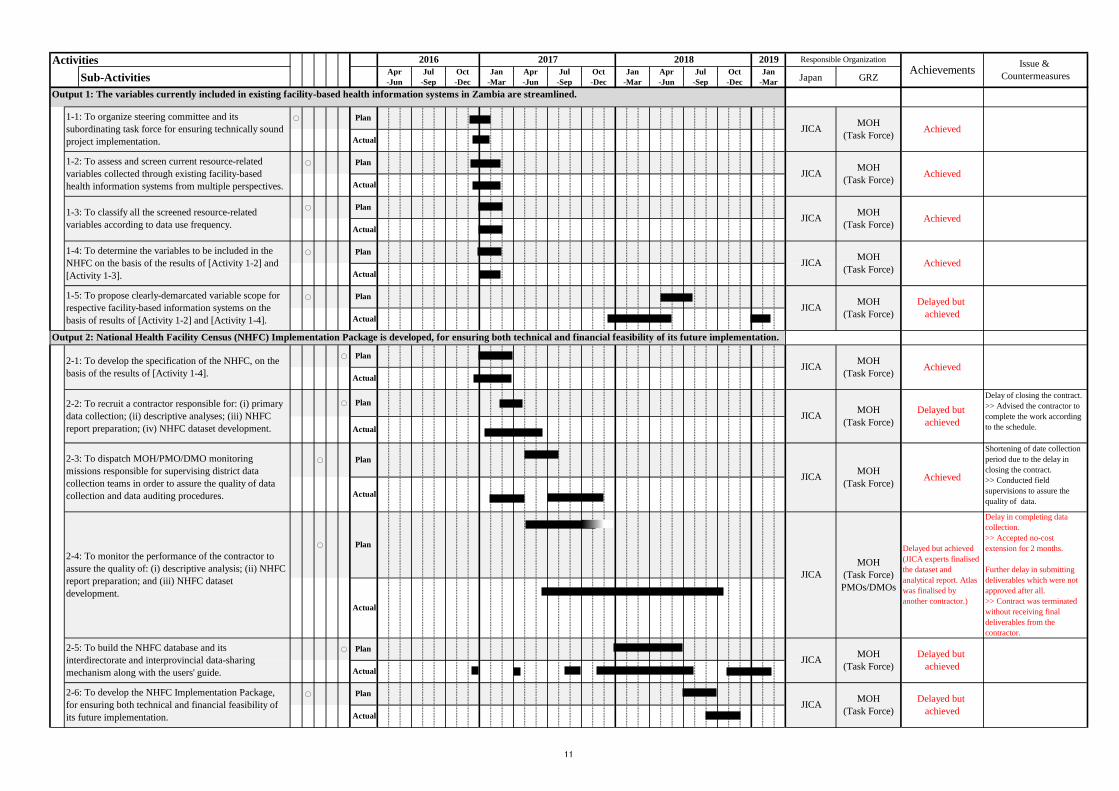
Although UNZA completed the data collection and submitted the draft of dataset, descriptive
report and the final report, these were not approved by the MOH. Especially, the dataset needed to be
further cleaned. In October 2018, Consensus Workshop was held in Lusaka, inviting Provincial Health
Officers from all ten provinces and further verified the data. UNZA was supposed to reflect those
verified and finalised data to the final deliverables, however, it was agreed that the contract would be
terminated in October 2018 and the Project would reflect the changes made during the Consensus
Workshop. The Project further conducted the analyses and compiled the NHFC Analytical Report. The
Project also engaged another Contractor which had GPS specialists to finalise the National Health
Facility Atlas. It is recommended that the atlas could be developed by the different Contractor than the
data collecting Contractor whose expertise is more focused on GPS.
3.3. Opportunity to Share the NHFC Results
NHFC Conference was initially designed in the project scope to share the analytical results with
PHOs and CPs. However, Consensus Workshop was held instead because the quality of data collected
by the Contractor had some more room to improve. The Project prioritised to share the data with PHOs
to further verify it at the Consensus Workshop. Details of this workshop is described in “2.5. Activities
Related to [Output 3: To develop Capital Investment Plan]”.
3.4. Approach Taken to Achieve [Output 3: The capacity of MOH in performing
evidence-based health investment planning is enhanced]
As the name of the Project “Strengthening the capacity of facility-census-based capital
investment planning” indicates, capacity building of MOH is one of the main aims of the Project. Based
on the “Capacity Assessment Handbook” published by JICA in 2008, the Project considered “Capacity”
as “Individual capacity”, “Organisational capacity” and “Systems and environment”.
As soon as the Project was commenced, JICA Experts reviewed the mid-term and long-term
policies developed by the MOH, which includes NHSP 2017-2021 and National Human Resources for
Health Strategic Plan (NHRHSP) 2018-2022. It was found that the consultants are often out-sourced to
draft these mid to long term policies and the MOH plays roles in supervising the consultants and
commenting on the drafts. On the other hand, it was found that the MOH officers are required to develop
the annual plan for infrastructure and medical equipment which are the two main components of the CIP.
As the Project was not designed to feature the “Individual capacity” in terms of pre-determined
activities and the budget, the focus was made on “Organisational capacity” and “Systems and
environment”. Although the Project still conducted on-the-job trainings to contribute to the “Individual
capacity” building, it was not possible to conduct more intense trainings due to the time and budget
constraints. Instead, “Organisational capacity” was strengthened through the Project by organising the
- 28 -
CITC as the responsible technical committee to develop the CIP, which was related to [Activity 3-1: To
conduct other statistical analyses tailored investment planners’ use]. NHFC 2017 database was created
as “Systems” to provide necessary information for developing the CIP, which was related to [Activity
2-5: To build the NHFC database]. Also, the “Environment” was prepared to draw up the annual plan
by providing the framework of mid to long term CIP, which was related to [Activity 3-3: To develop
five-year NHCIP on the basis of the analyses of the NHFC dataset]. Achievements of these activities are
described in “4. Achievements of the Project”.
3.5. Project Implementation Structure
Figure 4 shows the MOH organisational chart at the time when the R/D was signed in July 2016.
When the Project was officially launched in December 2016, MOH operated in newly restructured
departments and units as shown in Figure 5. The Project, therefore, formed the implementation structure
as follows:
- The Permanent Secretary – Administration as the Project Director,
- Director of Department of Policy and Planning (DPP) as the Project Manager, and
- Each unit under DPP as the main counterpart.
Figure 4 : Ministry of Health Organisational Chart as of July 2016 (When R/D was signed)
- 29 -
Figure 5 : Ministry of Health Organisational Chart as of December 2016 (When the Project was
officially launched)
In November 2018, MOH experienced another restructure of the departments and units as shown
in Figure 6. M&E Unit which used to fall under DPP and played the main role in conducting the Project
at the time became an independent department, whereas Infrastructure Unit which used to fall under
DPP and Medical Equipment Unit which used to fall under Department of Clinical Care and Diagnostic
Services became integrated as Department of Physical Planning and Medical Technologies. This new
department became the most important department for the second phase of the Project when the
development of CIP was commenced. Director, Assistant Director and Chiefs of this department, all of
whom are CITC members, spearheaded the discussion with JICA Experts to develop the CIP.
- 30 -
Source: Ministry of Health Organisation Structure Report for the Ministry of Health 2018
Figure 6 : Ministry of Health Organisational Chart as of February 2018
- 31 -
3.6. Co-Financing
It was agreed through the MM signed in April 2016 that MOH would fully finance the dispatch
of Monitoring Missions, which was also confirmed at the 1st JCC meeting in January 2017. However,
upon request from the Project Manager, Director of DPP, it was agreed during the 1st SC meeting in
March 2017 that the Japanese side would provide DSA at JICA rate and MOH would cover the shortfalls.
MOH eventually coordinated this expense through the initiative support by the GF. Similarly, the
expense of the Consensus Workshop in October 2018 was co-financed with the GF.
3.7. Delay in the First Dispatch of Chief Advisor / Health Survey 1
First dispatch of Chief Advisor was initially planned in January 2017. However, his dispatch was
postponed to November 2017 due to some medical concerns. Deputy Chief Advisor was instead
dispatched longer period to take over Chief Advisor’s main task which was to organise SC and its
subordinating TF. By the 1st JCC meeting in January 2017, the Project finalised the TORs of SC and TF,
which were also endorsed at the same meeting. Moreover, the 1st SC meeting was held as planned in
March 2017.
3.8. Collaboration with Other Projects
MOH and JICA have implemented the “Project for Strengthening Basic Health Care Services
Management for Universal Health Coverage” since 2015. This project mainly aims to strengthen the
capacity of service providing management at DHO, health centre and health post level by collecting
data. As the NHFC data could be also a valuable data source for these pilot areas, the Project shared the
data and atlas for collaboration.
Similar activities to the NHFC project are conducted in Zambia such as initiative of Master
Facility List (MFL) development by MOH and EQUIP Consortium’s programme to increase HIV testing,
care and treatment with support from USAID. The Project often discussed with the teams working on
such similar activities in order to share lessons learnt from each other for sound implementation. The
Project agreed to contribute to the MFL development by providing general facility information as its
initial data. The EQUIP Consortium shared useful lessons learnt in logistics of data collection. Also, the
Project invited relevant departments of MOH and other cooperating partners at tools and methodology
finalisation workshop in July 2017 and optimised opportunities to collaborate with other stakeholders.
- 32 -
4. Achievements of the Project
Achievements of each output and the project purpose is described in this chapter. Details are
indicated in the PDM attached as Annex 1.
4.1. Achievements by Output
PDM designated 3 outputs with 7 indicators for this Project. Although some indicators were
achieved later than planned, all 7 indicators were thoroughly achieved.
[Output 1: The variables currently included in existing Facility-based Health Information Systems
in Zambia are streamlined]
[Indicator 1-1: By February 2017, classification of the variables from data use frequency viewpoint is
completed]
Achieved: HISs were screened and their variables were classified by data user and data use frequency
in the matrix. This matrix contributed to streamline and determine the variables of NHFC at the NHFC
Preparation Workshop held in February 2017. The “Report on Variables for Future NHFC and Further
Development of NHFC 2017 Database” was produced as [Activity 1-5: To propose clearly-demarcated
variable scope], which includes the revised and updated matrix for future use.
[Indicator 1-2: By July 2018, a report of recommendations on variable scoping for respective HISs is
shared with the stakeholders.]
Delayed but achieved: The “Report on Variables for Future NHFC and Further Development of NHFC
2017 Database” was produced after CIP was finalised. Main recommendations made in this report are
variables for the future NHFC and prospect of the NHFC database developed through the Project. The
report was shared with relevant departments of MOH such as Physical Planning and Medical
Technologies and M&E.
[Output 2: NHFC Implementation Package is developed.]
[Indicator 2-1: By April 2017, the preparation work of the specification of NHFC is completed]
Achieved: Members of TF and JICA Experts together with the Monitoring Mission from Japan finalised
the specification of NHFC at the NHFC Preparation Workshop held in February 2017, which was
endorsed at the 1st SC meeting held in March 2017.
[Indicator 2-2: By May 2017, data collection activities are commenced]
Delayed but achieved: Because of the delay in [Activity 2-2: To recruit a contractor], data collection
activities were commenced in August 2017. “3.2. Delay in Completion of NHFC and Termination of the
Contract with Out-sourced Contractor” can be referred for details.
- 33 -
[Indicator 2-3: By September 2018, the draft of NHFC implementation package is readily available.]
Delayed but achieved: NHFC implementation package was finalised and shared with MOH in
December 2018. In order to reflect all the lessons learnt from the 2017 NHFC, this package was not
compiled until all data collection activities were completed.
[Output 3: The capacity of MOH in performing evidence-based health investment planning is
enhanced]
[Indicator 3-1: By January 2018, the preparatory work for the NHFC reports s completed.]
Delayed but achieved: Due to the delay in completion of NHFC 2017, the preparatory work for the
NHFC report was commenced later than planned. However, the report was finalised in January 2019.
Details can be referred to “3.2. Delay in Completion of NHFC and Termination of the Contract with
Out-sourced Contractor”.
[Indicator 3-2: By March 2018, the NHFC report launching conference is held.]
Delayed but achieved: As described above, due to the delay in completion of NHFC 2017, the
completion of the NHFC report was delayed accordingly. Although the NHFC report launching
conference was not held, data was shared with MOH and PHOs and further verified at the Consensus
Workshop held in October 2018. Details of this change in launching conference is described in “3.3.
Opportunity to Share the NHFC Results”.
4.2. Achievement of Project Purpose
PDM indicates the project purpose as “A mechanism for evidence-based health resource
management is established through the utilisation of the NHFC data” with 2 indicators. Although it was
delayed than planned, both indicators were achieved.
[Indicator 1: By September 2018, the NHFC implementation package is endorsed by MOH]
Delayed but achieved: NHFC implementation package was finalised and submitted to the MOH in
December 2018. In order to reflect all the lessons learnt from the 2017 NHFC, this package was not
compiled until all data collection activities were completed. Details are described in “2.4. Activities
Related to [Output 2: NHFC Implementation Package is developed]”.
[Indicator 2: By September 2018, the National Health Capital Investment Plan is endorsed and
disseminated by MOH]
Delayed but achieved: Due to the delay in completion of NHFC 2017, the CIP was finalised later than
planned. However, it was endorsed by the MOH in February 2019. Details are described in “2.5.
Activities Related to [Output 3: NHCIP is developed]”.
- 34 -
5. Recommendations for Achieving Overall Goal
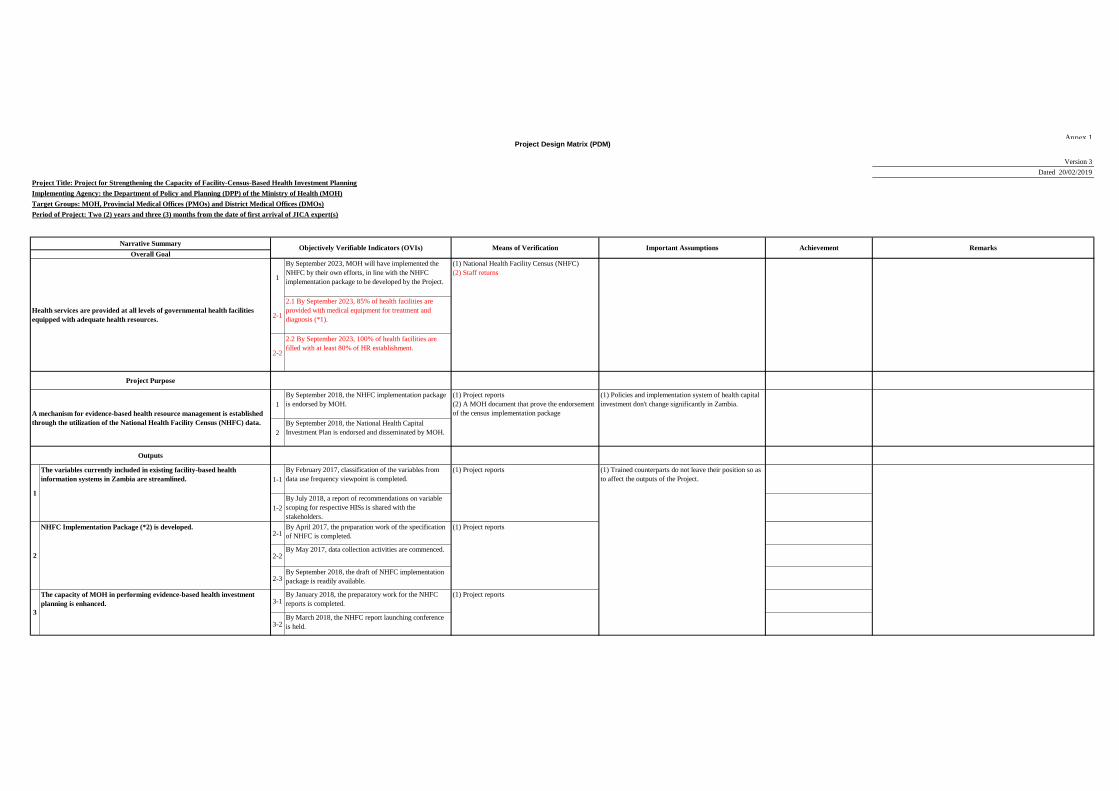
PDM indicates the overall goal as “Health services are provided at all levels of governmental health
facilities equipped with adequate health resources”. Two indicators are provided to verify the
achievements of this goal, one of which [Indicator 1: MOH will have implemented the NHFC by their
own efforts] is likely to be achieved. On the other hand, in order to achieve [Indicator 2-1: By September
2023, 85% of health facilities are provided with medical equipment for treatment and diagnosis] and
[Indicator 2-2: By September 2023, 100% of health facilities are filled with at least 80% of HR
establishment], further budgetary measures will be required.
[Indicator 1: By September 2023, MOH will have implemented the NHFC by their own efforts, in line
with the NHFC implementation package to be developed by the Project]
Likely to achieve: It is recognised by most stakeholders including MOH that the evidence-based
approach is crucial in planning capital investment and other planning exercises. As a result of this Project
which completed a full cycle of “Evidence-based health resource management” as shown in Figure 2,
this has been more widely recognised. As the 2017 NHFC did not include private health facilities, MOH
has started planning to conduct the similar census targeted private facilities. The Project shared the
specifications of the NHFC, data collecting tools, variables and other documents with the MOH. This
indicates that the NHFC implementation package has been already utilised partially for the similar
exercise. It is therefore likely that the MOH will achieve this indicator.
In an ideal situation, health information systems should be updated in a routine basis with accurate
quality of data so that the big survey like NHFC in an ad-hoc basis would not be necessary. The MOH
recently started preparing for building the MFL which offers health facility information to be updated
in a routine basis. It was agreed that the NHFC 2017 data would be imported in this system as the
baseline information. In addition, the Project proposed the MOH recommendations on the MFL
variables and frequency to be updated based on the experience in conducting the NHFC 2017 and
developing the CIP. It was therefore acknowledged that the Project contributed not only to conducting
the future NHFC but also to improving the routine basis health facility information system.
[Indicator 2-1: By September 2023, 85% of health facilities are provided with medical equipment for
treatment and diagnosis] and [Indicator 2-2: By September 2023, 100% of health facilities are filled with
at least 80% of HR establishment]
Requires more efforts to achieve: Specific proportion of health facilities was not indicated in the initial
PDM when the Project was commenced. It was agreed in February 2019 that the specific proportion of
health facilities should be set in line with NHSP 2017-2021.
[Indicator 2-2: By September 2023, 100% of health facilities are filled with at least 80% of HR
establishment] is likely to be achieved based on the past few years’ deployment record. On the other
hand, [Indicator 2-1: By September 2023, 85% of health facilities are provided with medical equipment
- 35 -
for treatment and diagnosis] will require MOH much more efforts and budgetary measures to achieve.
The Permanent Secretary –Administration appreciated the development of NHCIP 2019-2021
through the Project as this could provide evidence to convince the Ministry of Finance how much budget
the MOH requires to attain the legacy goals. In such a way, the MOH is expected to utilise the NHCIP
to take budgetary measures through the Ministry of Finance and CPs so as to achieve these indicators.
Annex
Annex 1
Project Design Matrix (PDM)
Annex 1
Version 0
Dated 06/07/2016
Project Title: Project for Strengthening the Capacity of Facility-Census-Based Health Investment Planning
Implementing Agency: the Department of Policy and Planning (DPP) of the Ministry of Health (MOH)
Target Groups: MOH, Provincial Medical Offices (PMOs) and District Medical Offices (DMOs)
Period of Project: Two (2) years from the date of first arrival of JICA expert(s)
1
2
1
2
1-1
1-2
2-1
2-2
2-3
3-1
3-2
(1) Project reports
By March 2018, the NHFC report launching conference
is held.
(1) Trained counterparts do not leave their position so as
to affect the outputs of the Project.
By July 2018, a report of recommendations on variable
scoping for respective HISs is shared with the
stakeholders.
2
NHFC Implementation Package (*2) is developed. By March 2017, the preparation work of the specification
of NHFC is completed.
(1) Project reports
By April 2017, data collection activities are commenced.
By April 2018, the draft of NHFC implementation
package is readily available.
(1) Project reports
3
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
By January 2018, the preparatory work for the NHFC
reports is completed.
Outputs
1
The variables currently included in existing facility-based health
information systems in Zambia are streamlined.
By January 2017, classification of the variables from data
use frequency viewpoint is completed.
By September 2018, the National Health Capital
Investment Plan is endorsed and disseminated by MOH.
Health services are provided at all levels of governmental health facilities
equipped with adequate health resources.
By September 2023, MOH will have implemented the
NHFC by their own efforts, in line with the NHFC
implementation package to be developed by the Project.
(1) National Health Facility Census (NHFC)
By September 2023, the proportion of health facilities
that meet the standards of facility, equipment and staffing
is XX% or greater (*1).
Project Purpose
A mechanism for evidence-based health resource management is established
through the utilization of the National Health Facility Census (NHFC) data.
By September 2018, the NHFC implementation package
is endorsed by MOH.
(1) Project reports
(2) A MOH document that prove the endorsement
of the census implementation package
(1) Policies and implementation system of health capital
investment don't change significantly in Zambia.
Project Design Matrix (PDM)
Narrative SummaryObjectively Verifiable Indicators (OVIs) Means of Verification Important Assumptions Achievement Remarks
Overall Goal
1
Pre-conditions
1
1-1
1-2
1-3
1-4
1-5 <Issues and countermesures>
2
2-1
2-2
2-3
2-4
2-5
2-6
3
3-1
3-2
3-3
Notes
(*1) : This target level is considered and endorsed in 2nd JCC because accurate situation at health facilities is supposed to be presented after the Project conducts the NHFC.
(*2) : Implementation Package is composed of: (i) implementation guidelines; (ii) data collection tools; (iii) training materials; (iv) census financial requirement estimation tool; and (v) others.
(*3) : E.g. previous National Health Facility Census (NHFC) dataset, Health Management Information System (HMIS), and Performance Assessment (PA) dataset
(*4) : E.g. definition clarity, measurability, accuracy, relevance
(*5) : E.g. every five years and annually
(*6) : Specification is composed of: (i) operational procedures; (ii) basic analysis framework; and (iii) structure of NHFC report.
(*7) : E.g. research institute, university or consulting firm.
(*8) : E.g. relevant directorates of MOH, PMOs, and development partners.
NHFC Implementation Package (*2) is developed.
To develop the specification (*6) of the NHFC, on the basis of the results
of [Activity 1-4].
To share the results of analyses for evidence-based investment planning
with the stakeholders (*8).
To develop five-year National Health Capital Investment Plan on the
basis of the analyses of the NHFC dataset.
To dispatch MOH/PMO/DMO monitoring missions responsible for
supervising district data collection teams in order to assure the quality of
data collection and data auditing procedures.
To monitor the performance of the contractor to assure the quality of: (i)
primary data collection; (ii) descriptive analysis; (iii) NHFC report
preparation; and (iv) NHFC dataset development.
To build the NHFC database and its interdirectorate and interprovincial
data-sharing mechanism along with the users' guide.
To develop the NHFC Implementation Package, for ensuring both
technical and financial feasibility of its future implementation.
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
To conduct other statistical analyses tailored to investment planners' use
(e.g. bivariate analysis, and multivariate analysis).
To organize the steering committee and its subordinating NHFC Task
Force for ensuring technically sound project implementation.
1. Dispatch of JICA experts
1. Allocation of Counterpart Personnel
(1) Project Director
(2) Project Manager(s)
(3) Other counterpart personnel
To assess and screen current resource-related variables collected through
existing facility-based health information systems (*3) from multiple
perspectives (*4).
To recruit a contractor (*7) responsible for: (i) primary data collection;
(ii) descriptive analysis; (iii) NHFC report preparation; (iv) NHFC
dataset development.
The variables currently included in existing facility-based health
information systems in Zambia are streamlined. The Japanese Side The Zambian Side(1) MOH expresses its clear commitment to conducting
the NHFC every five years after the Project's completion
by budgeting for the NHFC, unless/until routine health
information systems enable quality of resource-related
variables to be collected on a sustainable basis.
To classify all the screened resource-related variables according to data
use frequency (*5).
To determine the variables to be included in the NHFC on the basis of the
results of [Activity 1-2] and [Activity 1-3].
To propose clearly-demarcated variable scope for respective facility-
based information systems on the basis of results of [Activity 1-2] and
[Activity 1-4].
Activities Inputs
2
Annex 1
Version 1
Dated 13/01/2017
Project Title: Project for Strengthening the Capacity of Facility-Census-Based Health Investment Planning
Implementing Agency: the Department of Policy and Planning (DPP) of the Ministry of Health (MOH)
Target Groups: MOH, Provincial Medical Offices (PMOs) and District Medical Offices (DMOs)
Period of Project: Two (2) years from the date of first arrival of JICA expert(s)
1
2
1
2
1-1
1-2
2-1
2-2
2-3
3-1
3-2
(1) Project reports
By March 2018, the NHFC report launching conference
is held.
(1) Trained counterparts do not leave their position so as
to affect the outputs of the Project.
By July 2018, a report of recommendations on variable
scoping for respective HISs is shared with the
stakeholders.
2
NHFC Implementation Package (*2) is developed. By April 2017, the preparation work of the specification
of NHFC is completed.
(1) Project reports
By May 2017, data collection activities are commenced.
By September 2018, the draft of NHFC implementation
package is readily available.
(1) Project reports
3
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
By January 2018, the preparatory work for the NHFC
reports is completed.
Outputs
1
The variables currently included in existing facility-based health
information systems in Zambia are streamlined.
By February 2017, classification of the variables from
data use frequency viewpoint is completed.
By September 2018, the National Health Capital
Investment Plan is endorsed and disseminated by MOH.
Health services are provided at all levels of governmental health facilities
equipped with adequate health resources.
By September 2023, MOH will have implemented the
NHFC by their own efforts, in line with the NHFC
implementation package to be developed by the Project.
(1) National Health Facility Census (NHFC)
By September 2023, the proportion of health facilities
that meet the standards of facility, equipment and staffing
is XX% or greater (*1).
Project Purpose
A mechanism for evidence-based health resource management is established
through the utilization of the National Health Facility Census (NHFC) data.
By September 2018, the NHFC implementation package
is endorsed by MOH.
(1) Project reports
(2) A MOH document that prove the endorsement
of the census implementation package
(1) Policies and implementation system of health capital
investment don't change significantly in Zambia.
Project Design Matrix (PDM)
Narrative SummaryObjectively Verifiable Indicators (OVIs) Means of Verification Important Assumptions Achievement Remarks
Overall Goal
3
Pre-conditions
1
1-1
1-2
1-3
1-4
1-5 <Issues and countermesures>
2
2-1
2-2
2-3
2-4
2-5
2-6
3
3-1
3-2
3-3
Notes
(*1) : This target level is considered and endorsed in 2nd JCC because accurate situation at health facilities is supposed to be presented after the Project conducts the NHFC.
(*2) : Implementation Package is composed of: (i) implementation guidelines; (ii) data collection tools; (iii) training materials; (iv) census financial requirement estimation tool; and (v) others.
(*3) : E.g. previous National Health Facility Census (NHFC) dataset, Health Management Information System (HMIS), and Performance Assessment (PA) dataset
(*4) : E.g. definition clarity, measurability, accuracy, relevance
(*5) : E.g. every five years and annually
(*6) : Specification is composed of: (i) operational procedures; (ii) basic analysis framework; and (iii) structure of NHFC report.
(*7) : E.g. research institute, university or consulting firm.
(*8) : E.g. relevant directorates of MOH, PMOs, and development partners.
NHFC Implementation Package (*2) is developed.
To develop the specification (*6) of the NHFC, on the basis of the results
of [Activity 1-4].
To share the results of analyses for evidence-based investment planning
with the stakeholders (*8).
To develop five-year National Health Capital Investment Plan on the
basis of the analyses of the NHFC dataset.
To dispatch MOH/PMO/DMO monitoring missions responsible for
supervising district data collection teams in order to assure the quality of
data collection and data auditing procedures.
To monitor the performance of the contractor to assure the quality of: (i)
primary data collection; (ii) descriptive analysis; (iii) NHFC report
preparation; and (iv) NHFC dataset development.
To build the NHFC database and its interdirectorate and interprovincial
data-sharing mechanism along with the users' guide.
To develop the NHFC Implementation Package, for ensuring both
technical and financial feasibility of its future implementation.
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
To conduct other statistical analyses tailored to investment planners' use
(e.g. bivariate analysis, and multivariate analysis).
To organize the steering committee and its subordinating NHFC Task
Force for ensuring technically sound project implementation.
1. Dispatch of JICA experts
1. Allocation of Counterpart Personnel
(1) Project Director
(2) Project Manager(s)
(3) Other counterpart personnel
To assess and screen current resource-related variables collected through
existing facility-based health information systems (*3) from multiple
perspectives (*4).
To recruit a contractor (*7) responsible for: (i) primary data collection;
(ii) descriptive analysis; (iii) NHFC report preparation; (iv) NHFC
dataset development.
The variables currently included in existing facility-based health
information systems in Zambia are streamlined. The Japanese Side The Zambian Side(1) MOH expresses its clear commitment to conducting
the NHFC every five years after the Project's completion
by budgeting for the NHFC, unless/until routine health
information systems enable quality of resource-related
variables to be collected on a sustainable basis.
To classify all the screened resource-related variables according to data
use frequency (*5).
To determine the variables to be included in the NHFC on the basis of the
results of [Activity 1-2] and [Activity 1-3].
To propose clearly-demarcated variable scope for respective facility-
based information systems on the basis of results of [Activity 1-2] and
[Activity 1-4].
Activities Inputs
4
Annex 1
Version 2
Dated 12/11/2018
Project Title: Project for Strengthening the Capacity of Facility-Census-Based Health Investment Planning
Implementing Agency: the Department of Policy and Planning (DPP) of the Ministry of Health (MOH)
Target Groups: MOH, Provincial Medical Offices (PMOs) and District Medical Offices (DMOs)
Period of Project: Two (2) years and three (3) months from the date of first arrival of JICA expert(s)
1
2
1
2
1-1
1-2
2-1
2-2
2-3
3-1
3-2
(1) Project reports
By March 2018, the NHFC report launching conference
is held.
(1) Trained counterparts do not leave their position so as
to affect the outputs of the Project.
By July 2018, a report of recommendations on variable
scoping for respective HISs is shared with the
stakeholders.
2
NHFC Implementation Package (*2) is developed. By April 2017, the preparation work of the specification
of NHFC is completed.
(1) Project reports
By May 2017, data collection activities are commenced.
By September 2018, the draft of NHFC implementation
package is readily available.
(1) Project reports
3
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
By January 2018, the preparatory work for the NHFC
reports is completed.
Outputs
1
The variables currently included in existing facility-based health
information systems in Zambia are streamlined.
By February 2017, classification of the variables from
data use frequency viewpoint is completed.
By September 2018, the National Health Capital
Investment Plan is endorsed and disseminated by MOH.
Health services are provided at all levels of governmental health facilities
equipped with adequate health resources.
By September 2023, MOH will have implemented the
NHFC by their own efforts, in line with the NHFC
implementation package to be developed by the Project.
(1) National Health Facility Census (NHFC)
By September 2023, the proportion of health facilities
that meet the standards of facility, equipment and staffing
is XX% or greater (*1).
Project Purpose
A mechanism for evidence-based health resource management is established
through the utilization of the National Health Facility Census (NHFC) data.
By September 2018, the NHFC implementation package
is endorsed by MOH.
(1) Project reports
(2) A MOH document that prove the endorsement
of the census implementation package
(1) Policies and implementation system of health capital
investment don't change significantly in Zambia.
Project Design Matrix (PDM)
Narrative SummaryObjectively Verifiable Indicators (OVIs) Means of Verification Important Assumptions Achievement Remarks
Overall Goal
5
Pre-conditions
1
1-1
1-2
1-3
1-4
1-5 <Issues and countermesures>
2
2-1
2-2
2-3
2-4
2-5
2-6
3
3-1
3-2
3-3
Notes
(*1) : This target level is considered and endorsed in 2nd JCC because accurate situation at health facilities is supposed to be presented after the Project conducts the NHFC.
(*2) : Implementation Package is composed of: (i) implementation guidelines; (ii) data collection tools; (iii) training materials; (iv) census financial requirement estimation tool; and (v) others.
(*3) : E.g. previous National Health Facility Census (NHFC) dataset, Health Management Information System (HMIS), and Performance Assessment (PA) dataset
(*4) : E.g. definition clarity, measurability, accuracy, relevance
(*5) : E.g. every five years and annually
(*6) : Specification is composed of: (i) operational procedures; (ii) basic analysis framework; and (iii) structure of NHFC report.
(*7) : E.g. research institute, university or consulting firm.
(*8) : E.g. relevant directorates of MOH, PMOs, and development partners.
NHFC Implementation Package (*2) is developed.
To develop the specification (*6) of the NHFC, on the basis of the results
of [Activity 1-4].
To share the results of analyses for evidence-based investment planning
with the stakeholders (*8).
To develop five-year National Health Capital Investment Plan on the
basis of the analyses of the NHFC dataset.
To dispatch MOH/PMO/DMO monitoring missions responsible for
supervising district data collection teams in order to assure the quality of
data collection and data auditing procedures.
To monitor the performance of the contractor to assure the quality of: (i)
primary data collection; (ii) descriptive analysis; (iii) NHFC report
preparation; and (iv) NHFC dataset development.
To build the NHFC database and its interdirectorate and interprovincial
data-sharing mechanism along with the users' guide.
To develop the NHFC Implementation Package, for ensuring both
technical and financial feasibility of its future implementation.
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
To conduct other statistical analyses tailored to investment planners' use
(e.g. bivariate analysis, and multivariate analysis).
To organize the steering committee and its subordinating NHFC Task
Force for ensuring technically sound project implementation.
1. Dispatch of JICA experts
1. Allocation of Counterpart Personnel
(1) Project Director
(2) Project Manager(s)
(3) Other counterpart personnel
To assess and screen current resource-related variables collected through
existing facility-based health information systems (*3) from multiple
perspectives (*4).
To recruit a contractor (*7) responsible for: (i) primary data collection;
(ii) descriptive analysis; (iii) NHFC report preparation; (iv) NHFC
dataset development.
The variables currently included in existing facility-based health
information systems in Zambia are streamlined. The Japanese Side The Zambian Side(1) MOH expresses its clear commitment to conducting
the NHFC every five years after the Project's completion
by budgeting for the NHFC, unless/until routine health
information systems enable quality of resource-related
variables to be collected on a sustainable basis.
To classify all the screened resource-related variables according to data
use frequency (*5).
To determine the variables to be included in the NHFC on the basis of the
results of [Activity 1-2] and [Activity 1-3].
To propose clearly-demarcated variable scope for respective facility-
based information systems on the basis of results of [Activity 1-2] and
[Activity 1-4].
Activities Inputs
6
Annex 1
Version 3
Dated 20/02/2019
Project Title: Project for Strengthening the Capacity of Facility-Census-Based Health Investment Planning
Implementing Agency: the Department of Policy and Planning (DPP) of the Ministry of Health (MOH)
Target Groups: MOH, Provincial Medical Offices (PMOs) and District Medical Offices (DMOs)
Period of Project: Two (2) years and three (3) months from the date of first arrival of JICA expert(s)
1
2-1
2-2
1
2
1-1
1-2
2-1
2-2
2-3
3-1
3-2
(1) Trained counterparts do not leave their position so as
to affect the outputs of the Project.
By July 2018, a report of recommendations on variable
scoping for respective HISs is shared with the
stakeholders.
2
NHFC Implementation Package (*2) is developed. By April 2017, the preparation work of the specification
of NHFC is completed.
(1) Project reports
By May 2017, data collection activities are commenced.
By September 2018, the draft of NHFC implementation
package is readily available.
3
(1) Project reports
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
By January 2018, the preparatory work for the NHFC
reports is completed.
(1) Project reports
By March 2018, the NHFC report launching conference
is held.
Outputs
1
The variables currently included in existing facility-based health
information systems in Zambia are streamlined.
By February 2017, classification of the variables from
data use frequency viewpoint is completed.
By September 2018, the National Health Capital
Investment Plan is endorsed and disseminated by MOH.
Health services are provided at all levels of governmental health facilities
equipped with adequate health resources.
By September 2023, MOH will have implemented the
NHFC by their own efforts, in line with the NHFC
implementation package to be developed by the Project.
(1) National Health Facility Census (NHFC)
(2) Staff returns
2.1 By September 2023, 85% of health facilities are
provided with medical equipment for treatment and
diagnosis (*1).
2.2 By September 2023, 100% of health facilities are
filled with at least 80% of HR establishment.
Project Purpose
A mechanism for evidence-based health resource management is established
through the utilization of the National Health Facility Census (NHFC) data.
By September 2018, the NHFC implementation package
is endorsed by MOH.
(1) Project reports
(2) A MOH document that prove the endorsement
of the census implementation package
(1) Policies and implementation system of health capital
investment don't change significantly in Zambia.
Project Design Matrix (PDM)
Narrative SummaryObjectively Verifiable Indicators (OVIs) Means of Verification Important Assumptions Achievement Remarks
Overall Goal
Pre-conditions
1
1-1
1-2
1-3
1-4
1-5
2
2-1
2-2
2-3
2-4
2-5
2-6
3
3-1
3-2
3-3
Notes
(*1) : Medical equipment for treatment and diagnosis stands for 11 essencial items described in National Health Capital Investment Plan 2019-2021.
(*2) : Implementation Package is composed of: (i) implementation guidelines; (ii) data collection tools; (iii) training materials; (iv) census financial requirement estimation tool; and (v) others.
(*3) : E.g. previous National Health Facility Census (NHFC) dataset, Health Management Information System (HMIS), and Performance Assessment (PA) dataset
(*4) : E.g. definition clarity, measurability, accuracy, relevance
(*5) : E.g. every five years and annually
(*6) : Specification is composed of: (i) operational procedures; (ii) basic analysis framework; and (iii) structure of NHFC report.
(*7) : E.g. research institute, university or consulting firm.
(*8) : E.g. relevant directorates of MOH, PMOs, and development partners.
To develop five-year National Health Capital Investment Plan on the
basis of the analyses of the NHFC dataset.
To dispatch MOH/PMO/DMO monitoring missions responsible for
supervising district data collection teams in order to assure the quality of
data collection and data auditing procedures.
To monitor the performance of the contractor to assure the quality of: (i)
primary data collection; (ii) descriptive analysis; (iii) NHFC report
preparation; and (iv) NHFC dataset development.
To build the NHFC database and its interdirectorate and interprovincial
data-sharing mechanism along with the users' guide.
To develop the NHFC Implementation Package, for ensuring both
technical and financial feasibility of its future implementation.
The capacity of MOH in performing evidence-based health investment
planning is enhanced.
NHFC Implementation Package (*2) is developed.
To develop the specification (*6) of the NHFC, on the basis of the results
of [Activity 1-4].
To recruit a contractor (*7) responsible for: (i) primary data collection;
(ii) descriptive analysis; (iii) NHFC report preparation; (iv) NHFC
dataset development.
To conduct other statistical analyses tailored to investment planners' use
(e.g. bivariate analysis, and multivariate analysis).
To share the results of analyses for evidence-based investment planning
with the stakeholders (*8).
Activities Inputs
To organize the steering committee and its subordinating NHFC Task
Force for ensuring technically sound project implementation.
1. Dispatch of JICA experts
1. Allocation of Counterpart Personnel
(1) Project Director
(2) Project Manager(s)
(3) Other counterpart personnel
To assess and screen current resource-related variables collected through
existing facility-based health information systems (*3) from multiple
perspectives (*4).
The variables currently included in existing facility-based health
information systems in Zambia are streamlined. The Japanese Side The Zambian Side(1) MOH expresses its clear commitment to conducting
the NHFC every five years after the Project's completion
by budgeting for the NHFC, unless/until routine health
information systems enable quality of resource-related
variables to be collected on a sustainable basis.
To classify all the screened resource-related variables according to data
use frequency (*5).
To determine the variables to be included in the NHFC on the basis of the
results of [Activity 1-2] and [Activity 1-3].
To propose clearly-demarcated variable scope for respective facility-
based information systems on the basis of results of [Activity 1-2] and
[Activity 1-4].
Annex 2
Plan of Operation
Annex 2
Version 0
Dated 06/07/2016
Project Title: Project for Strengthening the Capacity of Facility-Census-based Health Investment Planning
Implementing Agency: the Directorate of Policy and Planning (DPP) of the Ministry of Health (MOH)
Target Groups: MOH, Provincial Medical Offices (PMOs) and District Medical Offices (DMOs)
Period of Project: Two (2) years from the date of first arrival of JICA expert(s)
Equipment
Training in Japan
In-country/Third country Training
Plan of Operation (PO)
Monitoring
Inputs 2016 2017 2018
Remarks Issue Solution
Chief Advisor / Health SurveyPlan
Actual
Project Coordinator / NHFC Operational Management
Apr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Apr
-Jun
Jul
-Sep
Jan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Plan
Actual
Health Statistics / Evidence-based Investment PlanningPlan
Actual
Other persons with necessary expertise for the project
activities
Plan
Actual
Oct
-Dec
Expert
Plan
Actual
Plan
Actual
Plan
Actual
Plan
Actual
Activities
Sub-Activities Japan GRZJul
-Sep
Oct
-Dec
Output 1: The variables currently included in existing facility-based health information systems in Zambia are streamlined.
1-1: To organize steering committee and its
subordinating task force for ensuring technically sound
project implementation.
Plan
JICAMOH
(Task Force)
Issue &
CountermeasuresJan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
2016 2017 2018 Responsible Organization
AchievementsJan
-Mar
Apr
-Jun
Actual
1-2: To assess and screen current resource-related
variables collected through existing facility-based health
information systems from multiple perspectives.
Plan
JICAMOH
(Task Force)Actual
1-3: To classify all the screened resource-related
variables according to data use frequency.
Plan
JICAMOH
(Task Force)Actual
1-5: To propose clearly-demarcated variable scope for
respective facility-based information systems on the
basis of results of [Activity 1-2] and [Activity 1-4].
Plan
JICAMOH
(Task Force)Actual
1-4: To determine the variables to be included in the
NHFC on the basis of the results of [Activity 1-2] and
[Activity 1-3].
Plan
JICAMOH
(Task Force)Actual
Output 2: National Health Facility Census (NHFC) Implementation Package is developed, for ensuring both technical and financial feasibility of its future implementation.
2-1: To develop the specification of the NHFC ,on the
basis of the results of [Activity 1-4].
Plan
JICAMOH
(Task Force)Actual
2-2: To dispatch MOH/PMO/DMO monitoring
missions responsible for supervising district data
collection teams in order to assure the quality of data
collection and data auditing procedures.
Plan
JICAMOH
(Task Force)Actual
2-3: To recruit a contractor responsible for: (i) primary
data collection; (ii) descriptive analyses; (iii) NHFC
Health Statistics / Evidence-based Investment PlanningPlan
Actual
Expert
Plan
Actual
4WD carPlan
Actual
Desktop PC, Laptop PC, Projector, UPS and PrinterPlan
Actual
Plan
Actual
4
Activities
Sub-Activities Japan GRZ
○
○
○
○
○
○
○
○
○
○
○
○
Jul
-Sep
Oct
-Dec
Output 1: The variables currently included in existing facility-based health information systems in Zambia are streamlined.
1-1: To organize steering committee and its
subordinating task force for ensuring technically sound
project implementation.
Plan
JICAMOH
(Task Force)
Issue &
CountermeasuresJan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
2016 2017 2018 Responsible Organization
AchievementsJan
-Mar
Apr
-Jun
Actual
1-2: To assess and screen current resource-related
variables collected through existing facility-based
health information systems from multiple perspectives.
Plan
JICAMOH
(Task Force)Actual
1-3: To classify all the screened resource-related
variables according to data use frequency.
Plan
JICAMOH
(Task Force)Actual
1-5: To propose clearly-demarcated variable scope for
respective facility-based information systems on the
basis of results of [Activity 1-2] and [Activity 1-4].
Plan
JICAMOH
(Task Force)Actual
1-4: To determine the variables to be included in the
NHFC on the basis of the results of [Activity 1-2] and
[Activity 1-3].
Plan
JICAMOH
(Task Force)Actual
Output 2: National Health Facility Census (NHFC) Implementation Package is developed, for ensuring both technical and financial feasibility of its future implementation.
2-1: To develop the specification of the NHFC, on the
basis of the results of [Activity 1-4].
Plan
JICAMOH
(Task Force)Actual
2-2: To recruit a contractor responsible for: (i) primary
data collection; (ii) descriptive analyses; (iii) NHFC
Health Statistics / Evidence-based Investment Planning
Plan
Actual
Medical Equipment Management and MaintenancePlan
Actual
Evidence-based Public Health Planning
Capacity Development on Health Systems Planning
Plan
Actual
Plan
Actual
7
Activities
Sub-Activities Japan GRZ
〇
〇
〇
〇
〇
〇
〇
〇
〇
〇
〇
Issue &
CountermeasuresApr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
2016 2017 2018 2019 Responsible Organization
1-1: To organize steering committee and its
subordinating task force for ensuring technically sound
project implementation.
Plan
JICAMOH
(Task Force)
Jan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Output 1: The variables currently included in existing facility-based health information systems in Zambia are streamlined.
Achievements
Actual
1-2: To assess and screen current resource-related
variables collected through existing facility-based
health information systems from multiple perspectives.
Plan
JICAMOH
(Task Force)Actual
1-3: To classify all the screened resource-related
variables according to data use frequency.
Plan
JICAMOH
(Task Force)Actual
1-5: To propose clearly-demarcated variable scope for
respective facility-based information systems on the
basis of results of [Activity 1-2] and [Activity 1-4].
Plan
JICAMOH
(Task Force)Actual
1-4: To determine the variables to be included in the
NHFC on the basis of the results of [Activity 1-2] and
[Activity 1-3].
Plan
JICAMOH
(Task Force)Actual
Output 2: National Health Facility Census (NHFC) Implementation Package is developed, for ensuring both technical and financial feasibility of its future implementation.
2-1: To develop the specification of the NHFC, on the
basis of the results of [Activity 1-4].
Plan
JICAMOH
(Task Force)Actual
2-2: To recruit a contractor responsible for: (i) primary
data collection; (ii) descriptive analyses; (iii) NHFC
subordinating task force for ensuring technically sound
project implementation.
Plan
JICAMOH
(Task Force)Achieved
Jan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Output 1: The variables currently included in existing facility-based health information systems in Zambia are streamlined.
Achievements
Actual
1-2: To assess and screen current resource-related
variables collected through existing facility-based
health information systems from multiple perspectives.
Plan
JICAMOH
(Task Force)Achieved
Actual
1-3: To classify all the screened resource-related
variables according to data use frequency.
Plan
JICAMOH
(Task Force)Achieved
Actual
1-5: To propose clearly-demarcated variable scope for
respective facility-based information systems on the
basis of results of [Activity 1-2] and [Activity 1-4].
Plan
JICAMOH
(Task Force)
Delayed but
achievedActual
1-4: To determine the variables to be included in the
NHFC on the basis of the results of [Activity 1-2] and
[Activity 1-3].
Plan
JICAMOH
(Task Force)Achieved
Actual
Output 2: National Health Facility Census (NHFC) Implementation Package is developed, for ensuring both technical and financial feasibility of its future implementation.
2-1: To develop the specification of the NHFC, on the
basis of the results of [Activity 1-4].
Plan
JICAMOH
(Task Force)Achieved
Actual
2-2: To recruit a contractor responsible for: (i) primary
data collection; (ii) descriptive analyses; (iii) NHFC
Health Statistics / Evidence-based Investment PlanningPlan
Actual
1) Delay of dispatch of
Chief Advisor.
2) Shortening of date
collection period
ExpertTask of evidence-based
investment planning was
added to Project
Coordinator 1 / NHFC
Operational Management
as Evidence-based
Investment Planning 2.
Chief Advisor / Health Survey 1Plan
Actual
Deputy Chief Advisor / Health Survey 2
4WD carPlan
Actual
Desktop PC, Laptop PC, Projector, UPS and PrinterPlan
Actual
Evidence-based Public Health Planning
Capacity Development on Health Systems Planning
Plan
Actual
Medical Equipment Management and MaintenancePlan
Actual
Oct
-Dec
2018 2019
Plan
Actual
Plan
Actual
Activities
Sub-Activities Japan GRZOct
-Dec
Output 1: Output 1: The variables currently included in existing facility-based health information systems in Zambia are streamlined.
1-1: To organize steering committee and its
subordinating task force for ensuring technically sound
project implementation.
Plan
Issue &
CountermeasuresActualApr
-Jun
Jul
-Sep
Oct
-Dec
Jan
-Mar
Apr
-Jun
Jul
-Sep
Oct
-Dec
Plan 2016 2017 Responsible Organization
AchievementsJan
-Mar
Apr
-Jun
Jul
-Sep
Jan
-Mar
AchievedActual
1-1-1: To make a staff list and confirm their TORPlan
Kuramata -Actual
1-2: To assess and screen current resource-related
variables collected through existing facility-based
health information systems from multiple perspectives.
Plan
AchievedActual
1-1-3: To finalize and confirm TOR of steering
committee and task force
Plan
Actual
1-2-2: To collect information from relating units of
MOH and Cooperating Partners
Plan Mochida Task Force
Actual
1-2-1: To make tools such as screen and
classification matrix
Plan Mochida Task Force
Actual
1-3: To classify all the screened resource-related
variables according to data use frequency.
Plan
AchievedActual
1-2-3: To have interviews with stakeholders to
assess existing HISs
Plan Mochida Task Force
Actual
1-4: To determine the variables to be included in the
NHFC on the basis of the results of [Activity 1-2] and
[Activity 1-3].
Plan
AchievedActual
1-3-1: To classify variables by reviewing annual
plans & mid-term plans / policies of relating units of
Plan Mochida Task Force
Actual
1-4-3: To compile discussion contents such as
reasons for inclusion / exclusion of variable in a
Plan Mochida /
KuramataTask Force
Actual
1-4-1: To hold a workshop / meeting in order to
discuss variables for NHFC
Plan Mochida Task Force
Actual
1-5-1: To reconfirm variable by reflecting NHFC
data analysis and NHCI plan development
Plan Mochida Task Force
Actual
1-5: To propose clearly-demarcated variable scope for
respective facility-based information systems on the
basis of results of [Activity 1-2] and [Activity 1-4].
Plan Delayed but
achievedActual
Actual
1-5-2: To discuss variables to be included in other
facility-based information system
Plan Mochida Task Force
Actual
1-5-3: To compile discussion contents such as
reasons for inclusion / exclusion of variable in a
Plan Mochida,
TatenoTask Force
1-1-2: To draft TOR of steering committee and task
force
Plan Mochida Task Force
Actual
JCC / SC
1-4-2: To finalize and onfirm variables for NHFC
2017
Plan
ActualSC
2018 2019
Output 2: National Health Facility Census (NHFC) Implementation Package is developed, for ensuring both technical and financial feasibility of its future implementation.
2-1: To develop the specification of the NHFC, on the
basis of the results of [Activity 1-4].
Plan
AchievedActual
2-1-1: To review past similar procurement cases by
JICA Zambia Office
Plan Kuramata,
Kaneko-
Actual
Actual
2-1-2: To draft the specificationPlan Kuramata,
KanekoTask Force
Actual
Actual
2-2: To recruit a contractor responsible for: (i) primary
data collection; (ii) descriptive analyses; (iii) NHFC
26 Patrick Phiri Provincial Infrastructure Officer PHO - Luapula
27 Patrick Phiri Provincial Infrastructure Officer PHO - Luapula
28 Mulambya Jairos (Dr.) PHS PHO - Eastern
29 Francis Liywali (Dr.) Provincial Health Director PHO - Western
30 Moses Chabala Senior Human Resources Officer PHO - North Western
Annex 8
7
31 Mwenya S. Soko Provincial Planner MOH HQ - Lusaka
32 Paul C. Ngwenyufu Principal Planner MOH HQ - Lusaka
33 Kennedy Bwalya Medical Equipment Officer MOH HQ - Lusaka
34 Luhana Elias Principal Equipment Officer PHO - Western
35 Patrick Mumba Medical Equipment Officer PHO - Copperbelt
36 Fabian Habeenzu Senior Human Resource Officer PHO - Muchinga
37 George Chipulu (Dr.) CCS PHO - Central
38 Timothy Mukoko Medical Equipment Officer PHO - Central
39 Chishimba
Kalandanya (Dr.)
Ag. Provincial Health Director PHO - Northern
40 Hilda Chilufya Human Resources Officer PHO - Lusaka
41 Christopher Sinkala Medical Equipment Officer PHO - Lusaka
42 Muleya Muchanga Provincial Infrastructure Officer PHO - North Western
43 Lawrence Mukombo Provincial ICT Officer PHO - North Western
44 Gift Lupenga Medical Equipment Officer PHO - North Western
45 Emmanuel Mwambazi Senior Human Resource Officer PHO - Luapula
46 Mhone F. Simon Biomedical Engineer PHO - Luapula
47 Allan Simakai Senior Human Resource Officer PHO - Western
48 Edward Phiri Planner PHO - Northern
49 Jason Wamulume Assistant Director - DPPMT MOH HQ - Lusaka
50 Keiji Mochida JICA Expert JICA Team
51 Michiru Kuramata JICA Expert JICA Team
52 Rafael Nkandu Project Officer JICA Team
53 Tatsuhiko Tsukakoshi JICA Project Advisor – Health JICA Zambia
Annex 9
List of Procured Equipment
Annex 9
LIST OF PROCURED EQUIPMENT
The Project for Strengthening the Capacity of Facility-Census-Based Health Investment Planning
No. Item Maker/ Model/
Accessories Quantity
Present
Location
Usage
Situation
JICA
Registration
No.
1 Colour Copier
Machine
SHARP/ DX-2500N
(MFP) 1
Annex Bld.
Room 203 In Use
16-3-
001260
2 Desktop
Computer
HP/ CZC6298CD3/
APC UPS back up,
MS office
1 Annex Bld.
Room 203 In Use
16-3-
001261
3 Desktop
Computer
HP/ CZC6298CH5/
APC UPS back up,
MS office
1 Annex Bld.
Room 203 In Use
16-3-
002219
4 Laptop HP/ CND5256R19/
MS office 1
Annex Bld.
Room 203 In Use
16-3-
001262
5 Portable
Projector Epson/ EB-S31 1
Annex Bld.
Room 203 In Use
16-3-
001263
6 Air conditioner LG/ SSH126THA1 1 Annex Bld.
Room 203 In Use
16-3-
001264
Annex 10
List of Counterparts Training in Japan
Annex 10
List of Counter Part Participated in the Training Programs in Japan
1)
Name Mildred Tolosi KAUNDA (Ms)
Job Title Senior Monitoring and Evaluation Officer
Course Period 5 – 27 July, 2017
Course Title Evidence-Based Public Health Planning
Training Institutes
1) TA Networking Corp.
2) Ryukyu University
3) Tokyo University
Course Objective
Participants will introduce and use evidence-based public
health approaches, with quantitative and qualitative
analysis, in health planning and health policy development,
as indicated by reports, case analyses, and/or planning and
policy documents.
Overall Goal Evidence-based public health policies and health service plans
will be formulated, approved, and implemented.
2)
Name Jason Wamulume (Mr)
Job Title Assistant Director, Department of Physical Planning and
Medical Techonologies
Course Period 18 February – 17 March, 2018
Course Title Capacity Development on Health Systems Planning
Training Institutes 1) JICA Yokohama
2) Tokai University
Course Objective
To strengthen the capacity of policy development and planning
through acquisition of visioning methodologies, understanding
of Japanese health policy and international trends in global
health, analyzing and having discussions on health issues of
each country.
Overall Goal Practical ‘health’ policy/ planning is developed based on
evidence.
Annex 10
3)
Name Mannix Ngabwe (Mr)
Job Title Principal Planner, Department of Policy and Planning
Course Period 27 June – 19 July, 2018
Course Title Evidence-Based Public Health Planning
Training Institutes
1) JICA Okinawa International Center
2) Ryukyu University
3) TA Networking Corp.
Course Objective
To introduce and to use evidence-based public health
approaches, with quantitative and qualitative analysis, in
health planning and health policy development, as indicated by
reports, case analyses, and/ or planning and policy documents.
Overall Goal Evidence-based public health policies and health service plans
will be formulated, approved, and implemented.
4)
Name Kaleya Mbewe (Mr)
Job Title Chief Medical Equipment, Department of Physical Planning
and Medical Technologies
Course Period 6 September – 15 November, 2018
Course Title Medical Equipment Management and Maintenance
Training Institutes 1) JICA Tohoku
2) Tohoku Air Water Inc. (Medisun)
Course Objective
To improve knowledge and skills of government officers who are
engineers and are responsible for purchasing, managing and
maintaining medical equipment, so that an appropriate level of
medical equipment management and maintenance services can
be achieved and maintained in the target countries.
Overall Goal
An appropriate level of medical equipment management and
maintenance are continuously provided in the target countries,
and the quality of medical services is improved.
Annex 11
Recommendation on Variables for Future National Health Facility Census and
Further Development of National Health Facility Census 2017 Database
THE PROJECT FOR STRENGTHENING THE CAPACITY OF FACILITY-
CENSUS-BASED CAPITAL INVESTMENT PLANNING
Recommendations on Variables for Future National Health Facility Census and Methods to Update National Health Facility Census 2017 Database
Contents Purpose of This Report ......................................................................................................................... 1 I. Recommendations on Variables for Future National Health Facility Census ............................... 1
1. Overview of Existing Facility-Based Information Systems and Surveys ................................. 1 2. Analysis and Variables Used to Develop Past National Health Capital Investment Plan and
Other Plans ........................................................................................................................................ 3 3. Variables Used in National Health Facility Census 2017 ......................................................... 4
3.1. Assessment of Variables on Existing Facility-Based Information Systems and Surveys . 4 3.2. Process to Determine Variables for National Health Facility Census 2017 ...................... 4
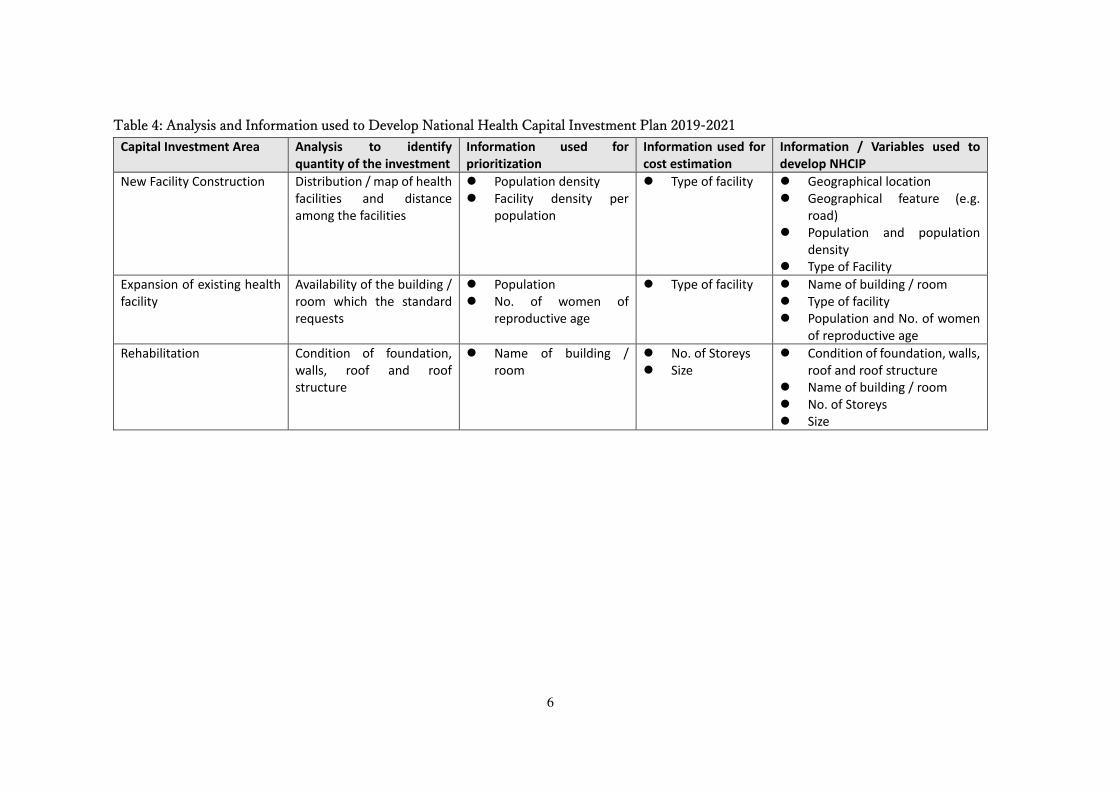
4. Variables for Future National Health Facility Census ............................................................... 5 4.1. Analysis and Information used to Develop National Health Capital Investment Plan 2019-
2021 5 4.2. Recommendations on Variables for Future National Health Facility Census ................... 8
II. Recommendations on methods to update National Health Facility Census 2017 Database ....... 10
Annex 1. Matrix of Variables
2. District Capital Investment Prioritization and Situation Analysis Guidelines
3. Hospital Capital Investment Prioritization and Situation Analysis Guidelines
4. Finalized Variables
1
Purpose of This Report
I. Recommendations on Variables for Future National Health Facility Census
It will contribute to improvement of data quality, and feasibility and sustainability of future
National Health Facility Census (NHFC) to exclude unnecessary variables and determine appropriate
variables for enumerators to concentrate on smaller number of variables and therefore will result in
saving implementation costs. In this report, the Project recommends variables for future NHFC from
experiences of NHFC 2017 implementation and development of National Health Capital Investment
Plan (NHCIP) 2019-2021. However, it is difficult to determine perfect variables for future
implementation in an environment where the health sector and society in general are rapidly changing.
It is requested that the variables should be revised based on the future situation, rather than simply
adapt variables recommended in this report. Therefore, this report devotes pages to explain the process
and approaches how the Project determined the variables for NHFC 2017. The Project recommends
that the future NHFC implementer should review and re-assess these variables with the process and
approaches used by the Project.
II. Further Development of National Health Facility Census 2017 Database
The Project developed NHFC 2017 database by using the platform of District Health Information
System (DHIS) 2. It is ideal to acquire health capital information though routine health information
systems such as Health Management Information System (HMIS). However, it would most likely take
a long time to integrate health capital variables into HMIS and other systems, which implies that data
of NHFC 2017 database would be required for updating until these systems are completely improved.
Therefore, the Project proposes methods to update data of the database.
I. Recommendations on Variables for Future National Health Facility
Census
1. Overview of Existing Facility-Based Information Systems and Surveys
To avoid duplication with other information systems or surveys, the Project screened the variables
used in existing facility-based information systems and ad hock surveys. Characteristics of the systems
and surveys are summarized in Table 1 and results of reviewing are shown in Annex 1: Matrix of
Variables.
2
Table 1: Overview of Existing Facility-Based Information Systems and Surveys
Name of System / Survey
Frequency of Data
Collection /
Update
Target / Sampling Main Information Area Responsible
Department of MOH
Health Information System /
District Health Information
System 2
Routine (monthly1) All public and private health facilities
across the country
Epidemiological and administrative (resource inputs and
service utilization) information
Monitoring and
Evaluation
Human Resources
Information System
Routine (daily) All health workers at public health
facilities across the country
HR supply (training, registration) and deployment (facility
of deployment, date of appointment)
Human Resource and
Administration
Performance Assessment Routine
(biannually)
All PHO, DHO, and public & private
health facilities across the country
Progress of activities and compliance of standard across
thematic area (governance, HR, Medical supplies,
equipment and infrastructure, information, service etc.)
Monitoring and
Evaluation
National Health Facility
Census
Ad hock (2004-05
and 2017-18)
All public health facilities across the
country
Geographical location and comprehensive health capital
(infrastructure, medical equipment, transport, utility, HR
and service delivery)
Policy and Planning
(at that time)
Health Facility List Ad hock (2002,
2010, 2014 and
2017)
All public and private health facilities
across the country
Basic service availability and utility Monitoring and
Evaluation
Service Availability and
Readiness Assessment 2010
Ad hock (2010) All public and private health facilities in
18 districts
Comprehensive service availability Policy and Planning
(at that time)
GIS Facilities Mapping and
Laboratories Assessment
Ad hock (2017) All public and private health facilities
across the country (650 facilities across
the country for lab. equipment)
Geographical location, laboratory equipment, utility and
specimen transportation routes
-
Source. Health Information System / District Health Information System 2: Health Service Delivery Aggregation Form
Human Resources Information System: Microsoft Access-base database
National Health Facility Census 2004: National Health Facility Census questionnaires
Health Facility List: The 2017 List of Health Facilities in Zambia
Service Availability and Readiness Assessment 2010: Service Availability and Readiness Assessment Reference Manual
GIS Facilities Mapping and Laboratories Assessment: GIS Mapping Assessment Tool
1 Some organizations and variables are requested to collect / update information daily and monthly.
3
2. Analysis and Variables Used to Develop Past National Health Capital
Investment Plan and Other Plans
To choose necessary variables for Health Capital Investment Plans, the Project screened the
information used to develop past NHCIP and other plans. Past NHCIP was developed though “District
Capital Investment Prioritization Planning Workshop” and “Hospital Capital Investment Prioritization
Planning Workshop” and the main analysis and information used during the workshops are
summarized in Table 2. Details of these workshops are shown in Annex 2: District Capital Investment
Prioritization and Situation Analysis Guidelines and Annex 3: Hospital Capital Investment
Prioritization and Situation Analysis Guidelines, which were developed by past cooperation between
MOH and JICA. Results of reviewing past NHCIP and other plans are shown in Annex 1: Matrix of
Variables.
Table 2: Main Analysis and Information / Variables Used to Develop Past National Health Capital Investment Plan
Main Analysis Information / Valuables
Facility density per population Geographical location (GPS)
Population
Distribution / map of health facilities and
distance among the facilities
Geographical location (GPS)
Distribution / map of delivery points of kinds of
health services, medical equipment and HR
Geographical location (GPS)
Service availability
Number and functional status of medical
equipment
Number of HR
Disease burden (e.g. malaria and respiratory
infection) per population
Epidemiology data (e.g. No. of ne malaria
cases)
Population
Distribution / map of availability of utility and
transport, and distance among the points
Geographical location (GPS)
Availability and functional status of utility
Availability and functional status of
transport
Condition (e.g. poor and good) of buildings /
rooms
Condition of buildings / rooms
Source: “District Capital Investment Prioritization and Situation Analysis Guidelines” and
“Hospital Capital Investment Prioritization and Situation Analysis Guidelines”
Note: All information / variables obtained from NHFC 2004 except that population information
from Central Statistical Office of Zambia and Epidemiology data from Health Management
Information System / District Health Information System 2.
4
3. Variables Used in National Health Facility Census 2017
3.1. Assessment of Variables on Existing Facility-Based Information Systems and
Surveys
As it is summarized in Chapter 1 and 2, the Project screened capital-related variables collected
through existing facility-based health information systems and surveys, and classified the variables
according to data use frequency in capital investment planning. This work is shown in Annex 1: Matrix
of Variables.
NHFC 2004, and Service Availability and Readiness Assessment 2010 collected capital-
related information on the largest number of variables. However, all of these variables were not always
used for capital investment planning as long as the project reviewed some capital investment plans.
3.2. Process to Determine Variables for National Health Facility Census 2017
The project organized “NHFC Preparation Workshop” in February 2017 and variables for
NHFC 2017 were proposed through participatory approach. The workshop participants from relevant
departments from MOH discussed necessary variables to develop NHCIP and duplication with other
information system or surveys by referring to Annex 1: Matrix of Variables. Variables, which are
needed for the planning and not collected in other information systems, were extracted. Table 3 shows
the basic strategy to determine the variable and “Variable C” was proposed for NHFC 2017 in this
case. After review by senior officials, the variables were finally determined as it is shown in Annex 4:
Finalized Variables
Table 3: 2 by 2 Table to Determine Variables for National Health Facility Census 2017
Source: The Project
5
4. Variables for Future National Health Facility Census
4.1. Analysis and Information used to Develop National Health Capital Investment
Plan 2019-2021
The Project developed NHCIP 2019-2021 as a mid-term plan at national level. Table 4 shows
analysis and information used to develop NHCIP 2019-2021. Details of analysis, prioritization and
cost estimation are shown in NHCIP 2019-2021.
6
Table 4: Analysis and Information used to Develop National Health Capital Investment Plan 2019-2021 Capital Investment Area Analysis to identify
quantity of the investment
Information used for
prioritization
Information used for
cost estimation
Information / Variables used to
develop NHCIP
New Facility Construction Distribution / map of health
facilities and distance
among the facilities
Population density
Facility density per
population
Type of facility Geographical location
Geographical feature (e.g.
road)
Population and population
density
Type of Facility
Expansion of existing health
facility
Availability of the building /
room which the standard
requests
Population
No. of women of
reproductive age
Type of facility Name of building / room
Type of facility
Population and No. of women
of reproductive age
Rehabilitation Condition of foundation,
walls, roof and roof
structure
Name of building /
room
No. of Storeys
Size
Condition of foundation, walls,
roof and roof structure
Name of building / room
No. of Storeys
Size
7
Table 4: Analysis and Information used to Develop National Health Capital Investment Plan 2019-2021 (Cont.) Capital Investment Area Analysis to identify
quantity of the investment
Information used for
prioritization
Information used for
cost estimation
Variables used to develop NHCIP
Utility Availability of water supply
resource and electrical
power resource
- Type of facility Type of water supply resource
and working status
Type of electrical power
resource and working status
Type of facility
Availability of the transport
which the standard
requests
Distance from HF to the
furthest outreach site
Population at
catchment area
Type of facility Means of transport for patient
Means of transport for staff
and other purposes
Type of facility
Distance from HF to the
furthest outreach site
Population at catchment area
Medical Equipment Availability of the
equipment which the
standard requests
Epidemiology data (e.g.
No. of new malaria
cases)
Service utilization data
(e.g. No. of at least 4-
time ANC visits)
Population
Type of facility No. of equipment
Functional status
Epidemiology data (e.g. No. of
new malaria cases)
Service utilization data (e.g.
No. of at least 4-time ANC
visits)
Population
Source: The Project
Note: All information / variables obtained from NHFC 2017 except that population information and geographical feature from Central Statistical Office of
Zambia, and Epidemiology data and Service utilization data from Health Management Information System / District Health Information System 2.
8
4.2. Recommendations on Variables for Future National Health Facility Census
To streamline its variables enhances feasibility and sustainability of future NHFC. The Project
determined the variables NHFC 2017 in two approaches as summarized in Table 3: 1) to avoid
duplication with variables of other health information systems and 2) to select only necessary variables
to develop investment plans. Based on same two approaches and experience to develop NHCIP 2019-
2021, variables for the future NHFC are suggested. However, the Project recommends that the future
NHFC implementer should review and re-assess these variables with the process and approaches used
by the Project.
1) To avoid duplication with variables of other health information systems
Variables of Human Resources and Service Delivery should be less prioritized because the
information of these thematic areas is available from “Staff Return” records and HMIS/DHIS2.
Moreover, data from these 2 resources are routinely updated and was reliable enough to use for NHCIP
2019-2021 development.
2) To select only necessary variable to develop investment plans
NHCIP 2019-2021 as a mid-term plan at national level shows investment framework and
subsystem such as District Health Offices are requested to make annual plans based on the framework.
It needs more detailed information and more various variables to develop annual plans at subsystem
level than the mid-term plan at national level. However, in case the resources are limited, variables
should be prioritized based on necessity for planning. Table 5 shows variables recommended for future
NHFC. Variables highlighted with gray should be prioritized because they were used to develop
NHCIP 2019-2021 and are likely to be needed for future mid-term NHCIP.
Table 5: Recommendations on Variables for Future National Health Facility Census Category of
Variables Variables
General Name of facility
Facility code
Location of facility (province, district)
GPS / GIS
Type of facility
Managing authority
No. inpatient beds
No. maternity beds
Distance from HF to the furthest outreach site
Distance of facility from DMO
Population at catchment area
9
Table 5: Recommendations on Variables for Future National Health Facility Census (Cont.) Category of Variables Variables
Utility Plot size
Is there a space for future expansion?
Size of a space for future expansion
Type of water supply resource and working status
Type of electrical power resource and working status
Type of general waste disposal system
Type of medical waste disposal system
Means of transport for patient
Means of transport for staff and other purposes
Toilet / latrine
Infrastructure Name of building & rooms (e.g. clinic, staff house)
Sketch
Permanent or temporary
No. of Storeys
Size building & room
Year built
Rehabilitation year
Availability of fire alarm
Condition of foundation
Condition of walls
Condition of roof
Condition of roof structure
Function of water system
Function of power system
Function of sewage system
Function of storm water drain
Construction material of foundations
Construction material of walls
Construction material of floors
Construction material of ceiling
Construction material of roof
Construction material of trusses
Medical Equipment Type of equipment
Number of units
Functional status
Country of origin
Manufacturing year
Source: The Project
Note: Variables highlighted with gray should be prioritized
10
II. Recommendations on methods to update National Health Facility
Census 2017 Database
It is ideal to acquire health capital information through routine health information systems such
as HMIS. However, it would most likely take a long time to integrate health capital variables into
HMIS and other systems, which implies that the data of NHFC 2017 database would be required to be
frequently updated until these systems are completely improved.
The Project organized NHFC 2017 Database Deployment Training in February 2019 to
handover the database to MOH and orient MOH officials to get familiar with basic use of it. Table 6
shows summary of the training.
Table 6: Summary of NHFC 2017 Database Deployment Training Date 13-14 February 2019 (2 days)
Venue Nomad’s Court Lodge in Lusaka
Participants
9 officers from MOH and 1 adviser from cooperating partner:
<MOH>
Department of Physical Planning and Medical Technologies
Assistant Director, Chief Medical Equipment Officer, Principal Planners
Department of Policy and Planning
Planning & Budgeting Officers
Department of Monitoring and Evaluation
Principal Monitoring & Evaluation Officer, Monitoring and Evaluations
Officer
ICT Unit
Principal ICT Officer, Senior ICT Officer
<Cooperating Partner>
Tropical Health & Education Trust (THET)
Health Technology Management Consultant
Main Agenda Training on basic use of the database (data entry, analysis and
visualization etc.)
Discussion about methods to update data and user management
During the group discussion, methods to update data of the NHFC 2017 Database was considered
in the points of; 1) necessity of updating, 2) frequency of updating, and 3) responsible organization of
updating. Table 7 shows methods to update data of the NHFC 2017 Database. All participants agreed
that data of human resources and service delivery are not needed for updating because information
from HRIS / Staff Returns and HMIS / DHIS2 provide routinely updated information. It is suggested
that the data should be updated only in case any changes are created.
11
Table 7: Methods to update data of the National Health Facility Census 2017 Database
Category of Variables Variables for NHFCNecessity of
UpdatingFrequency of
UpdatingResponsibility
of updatingNote
Name of facility Yes Quarterly MOH HQs- M&EFacility code NoLocation of facility (province, district) Yes Quarterly MOH HQs- M&EGPS / GIS Yes Quarterly MOH HQs- M&EType of facility Yes Quarterly MOH HQs- M&EManaging authority Yes Quarterly MOH HQs- M&ENo. inpatient beds Yes Quarterly DHONo. maternity beds Yes Quarterly DHODistance from HF to the furthest out reach site Yes Quarterly MOH HQs- M&EDistance of facility from DMO Yes Quarterly MOH HQs- M&EPopulation at cathment area Yes Quarterly MOH HQs- M&EPlot size Yes Annually DHOIs there a space for future expansion? Yes Annually DHOSize of a space for future expansion Yes Annually DHOType of water supply resource Yes Annually DHOType of electrical power resource Yes Annually DHOType of general waste disposal system Yes Annually DHOType of medical waste disposal system Yes Annually DHOMeans of transportation for patient Yes Annually DHOMeans of transportation for staff and other purposes Yes Annually DHOToilet / latrine Yes Annually DHO
Chan
ges a
re le
ss li
kely
to b
ecr
eate
d th
an o
ther
them
atic
area
s.
Chan
ges a
re le
ss li
kely
to b
e cr
eate
dbu
t the
chan
ges h
ave
larg
e im
pact
and
easy
to vi
ew.
General
Utility
12
Table 7: Methods to update data of the National Health Facility Census 2017 Database (Cont.)
2 Information of these variables will be collected only if new buildings are constructed or new equipment is provided.
Category of Variables Variables for NHFCNecessity of
UpdatingFrequency of
UpdatingResponsibility
of updatingNote
Name of building & rooms (e.g. clinic, staff house) Yes Annually DHOSketch NoPermanent or temporary No(2)
No. of Storeys No(2)
Size building & room Yes Annually DHOYear built No(2)
Rehabilitation year Yes Annually DHOAvailability of fire alarm Yes Annually DHOCondition of foundation Yes Annually DHOCondition of walls Yes Annually DHOCondition of roof Yes Annually DHOCondition of roof structure Yes Annually DHOFunction of water system Yes Annually DHOFunction of power system Yes Annually DHOFunction of sewage system Yes Annually DHOFunction of storm water drain Yes Annually DHOConstruction material of foundations Yes Annually DHOConstruction material of walls Yes Annually DHOConstruction material of floors Yes Annually DHOConstruction material of ceiling Yes Annually DHOConstruction material of roof Yes Annually DHOConstruction material of trusses Yes Annually DHO
Chan
ges a
re le
ss li
kely
to b
e cr
eate
d th
an o
ther
them
atic
area
s.
Infrastructure
13
Table 7: Methods to update data of the National Health Facility Census 2017 Database (Cont.)
3 Though "Serial Number" was not included in variables for NHFC 2017, it was recommended to be added to future database
Category of Variables Variables for NHFCNecessity of
UpdatingFrequency of
UpdatingResponsibility
of updatingNote
Type of equipment Yes Quarterly DHONumber of unit Yes Quarterly DHOFunctional status Yes Quarterly DHOCountry of origin No(2)
Manufacturing year No(2)
Human Resources Recorded No. on registerService delivery Availability of each service (Yes or not)
Chan
ges a
relik
ely t
o be
crea
ted
mor
efre
quen
tly th
anot
her t
hem
atic
area
s.
Medical Equipment(3)
Annex 1: Matrix of Variables
HMIS/DHIS2
HRIS PANHFC2004
HealthFacility
ListSARA
GISFacilitiesMapping
Health Infra.OperationalPlan 2016
(Draft)
MedicalEquipment
Procurementplan 2017
HealthSectorCapital
InvestmentPlan
NationalHealth
StrategicPlan 2017-
2021
Name of facility ✓ ✓ ✓ ✓ ✓ ✓Facility code ✓ ✓ ✓ ✓ ✓ ✓Location of facility (province,district)
✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓
GPS / GIS ✓ ✓ ✓ ✓ ✓Type of facility ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓ ✓Managing authority ✓ ✓ ✓ ✓ ✓ ✓Urban / rural ✓ ✓Outpatient only ✓Road access ✓No. inpatient beds ✓ ✓No. maternity beds ✓No. outreach site ✓Distance from facility to thefurthest out reach site
✓
Distance of facility from DHO ✓Surroundings Plot size ✓
Is the facility fenced? ✓ ✓Is there a public gate? ✓Is there a parking space? ✓Is there a space for futureexpansion?
✓ ✓
Operational water Type of water supply resource ✓ ✓ ✓ ✓ ✓ ✓Operational power Type of electrical power resource ✓ ✓ ✓ ✓ ✓Communications Type of communication tools ✓ ✓ ✓ ✓ ✓ ✓Waste disposal Type of waste disposal system ✓ ✓ ✓ ✓ ✓Fire equipment Type of fire equipment ✓ ✓ ✓Transportation Means of transportation ✓ ✓ ✓ ✓ ✓Toilet / latrine ✓ ✓Availability of SMARTCARE ✓
Variables Health Information Systems Data use frequency
Largecategory
Medium category Small category
Routine Ad hoc Annually Every 3-5 yearsGe
nera
lUt
ility
1
Annex 1: Matrix of Variables
HMIS/DHIS2
HRIS PANHFC2004
HealthFacility
ListSARA
GISFacilitiesMapping
Health Infra.OperationalPlan 2016
(Draft)
MedicalEquipment
Procurementplan 2017
HealthSectorCapital
InvestmentPlan
NationalHealth
StrategicPlan 2017-
2021
Variables Health Information Systems Data use frequency
Largecategory
Medium category Small category
Routine Ad hoc Annually Every 3-5 years
Name of building & rooms (e.g.clinic, staff house)
✓ ✓ ✓
SketchBuilding Permanent or temporary
No. of Storeys ✓Area (M2) ✓Year built ✓Funded by (e.g. MOH) ✓Rehabilitation by (e.g. MOH) ✓Rehabilitation year ✓Condition of foundation ✓ ✓ ✓Condition of walls ✓ ✓ ✓Condition of roof ✓ ✓ ✓Condition of roof structure ✓ ✓ ✓Function of water system ✓Function of power system ✓Function of sewage system ✓ ✓Function of storm water drain ✓Construction material offoundationsConstruction material of wallsConstruction material of floorsConstruction material of Ceiling ✓Construction material of Roof ✓Construction material of trusses ✓
Infra
stru
ctur
e
2
Annex 1: Matrix of Variables
HMIS/DHIS2
HRIS PANHFC2004
HealthFacility
ListSARA
GISFacilitiesMapping
Health Infra.OperationalPlan 2016
(Draft)
MedicalEquipment
Procurementplan 2017
HealthSectorCapital
InvestmentPlan
NationalHealth
StrategicPlan 2017-
2021
Variables Health Information Systems Data use frequency
Largecategory
Medium category Small category
Routine Ad hoc Annually Every 3-5 years
Room Size ✓Condition of walls ✓Condition of windows ✓Condition of doors ✓Condition of ceiling ✓Condition of floor ✓Function of power system ✓Function of sanitation system ✓Function of lighting ✓Function of ventilation ✓
Equipment Number ✓ ✓ ✓ ✓ ✓ ✓Functional status ✓ ✓ ✓ ✓ ✓Manufacture ✓Country of origin ✓Model ✓Serial No. ✓Manufacturing year ✓Commission year ✓Availability of Manual ✓
Med
ical
Equ
ipm
ent
3
Annex 1: Matrix of Variables
HMIS/DHIS2
HRIS PANHFC2004
HealthFacility
ListSARA
GISFacilitiesMapping
Health Infra.OperationalPlan 2016
(Draft)
MedicalEquipment
Procurementplan 2017
HealthSectorCapital
InvestmentPlan
NationalHealth
StrategicPlan 2017-
2021
Variables Health Information Systems Data use frequency
Largecategory
Medium category Small category
Routine Ad hoc Annually Every 3-5 years
No. of qualified staff at each dep./ward ✓ ✓ ✓Each cadre Recorded No. on register ✓ ✓
Headcount No. ✓No. of duty roster ✓ ✓ ✓
Each individual General ✓Position and compensation ✓Contact information ✓Dependants and emergencycontacts
✓
Training and education ✓Leave and attendance ✓Provided equipment ✓Performance appraisal ✓Debt ✓Discipline ✓Assignments ✓License and vehicle ✓Award ✓
No. OPD first attendance (each disease / service) ✓ ✓ ✓No. IPD discharge (each disease / service) ✓ ✓No. deaths (each disease / service) ✓ ✓No. bed utilisation ✓Availability of each service (Yes or not) ✓ ✓ ✓ ✓ ✓Availability of each service (No. of day per week) ✓Availability of trained personnel for each service ✓ ✓ ✓Referral system Communication ✓
Transportation ✓Referred facilities ✓
Progress of action plan ✓Availability of treatment / service guidelines ✓ ✓Compliance to guideline / standards ✓
Serv
ice
deliv
ery
Hum
an R
esou
rces
4
Annex 1: Matrix of Variables
HMIS/DHIS2
HRIS PANHFC2004
HealthFacility
ListSARA
GISFacilitiesMapping
Health Infra.OperationalPlan 2016
(Draft)
MedicalEquipment
Procurementplan 2017
HealthSectorCapital
InvestmentPlan
NationalHealth
StrategicPlan 2017-
2021
Variables Health Information Systems Data use frequency
Largecategory
Medium category Small category
Routine Ad hoc Annually Every 3-5 years
HMIS/DHIS2: Health Information System / District Health Information System 2HRIS: Human Resources Information SystemPA: Performance AssessmentNHFC 2004: National Health Facility Census 2004SARA 2010: Service Availability and Readiness Assessment 2010GIS Facilities Mapping: GIS Facilities Mapping and Laboratories AssessmentDHO: District Health Office
5
Annex 4: Finalized Variables
Category of Variables Finalized Variables for NHFCName of facilityFacility codeLocation of facility (province, district)GPS / GISType of facilityManaging authorityNo. inpatient bedsNo. maternity bedsDistance from HF to the furthest out reach siteDistance of facility from DMOPopulation at cathment areaPlot sizeIs there a space for future expansion?Size of a space for future expansionType of water supply resourceType of electrical power resourceType of general waste disposal systemType of medical waste disposal systemMeans of transportation for patientMeans of transportation for staff and other purposesToilet / latrineName of building & rooms (e.g. clinic, staff house)SketchPermanent or temporaryNo. of StoreysSize building & roomYear built
General
Utility
1
Annex 4: Finalized Variables
Category of Variables Finalized Variables for NHFCRehabilitation yearAvailability of fire alarmCondition of foundationCondition of wallsCondition of roofCondition of roof structureFunction of water systemFunction of power systemFunction of sewage systemFunction of storm water drainConstruction material of foundationsConstruction material of wallsConstruction material of floorsConstruction material of ceilingConstruction material of roofConstruction material of trussesNumberFunctional statusCountry of originManufacturing year
Human Resources Recorded No. on registerService delivery Availability of each service (Yes or not)