68
The public perceives widespread problems with quali The public perceives widespread problems with quali -- Dr. Robert Johnstone -- Dr. Robert Johnstone
| Date post: | 28-Dec-2015 |
| Category: |
Documents |
| Upload: | clara-ball |
| View: | 216 times |
| Download: | 0 times |

The public perceives widespread problems with qualityThe public perceives widespread problems with quality-- Dr. Robert Johnstone-- Dr. Robert Johnstone

Anesthesia Quality in the Perfect Digital Future
June 16, 2012
Richard P. Dutton, MD MBA
Executive Director
Anesthesia Quality Institute

Disclosure
• I am the Executive Director of the Anesthesia Quality Institute, a public charity devoted to creating a national registry. The AQI pays my salary.
• I am strongly biased on this topic:

04/19/234
The Challenge
The government wants to know that Ma and Pa are getting the healthcare they deserve … and that our taxes pay for.

W
Quality in Healthcare

Quality in Healthcare?
“I shall not today attempt further to define the kinds of material I understand to be embraced within that shorthand description; and perhaps I could never succeed in intelligibly doing so.But I know it when I see it …”
— Supreme Court Justice Potter Stewart in Jacobellis v.
Ohio, 1964, regarding possible obscenity in The Lovers
Some Characteristics of Quality in Healthcare
• Accessibility
• Affordability
• Efficiency
• Modernity
• Adaptability
• Humanity
EffectivenessEffectiveness Prevention of Prevention of
diseasedisease Avoidance of Avoidance of
complicationscomplications Improved survivalImproved survival

Case #1Is This Quality?
Case #1


Is this Quality?
• It’s modern!
• It’s accessible!
• It’s adaptable!
It’s not cheapIt’s not cheap It’s not humaneIt’s not humane It’s not efficientIt’s not efficient
It’s not effective (not It’s not effective (not this time)this time)

Case #1Is This Quality?
Case #2

Patient L.C.
• Young adult female
• Works in a large factory
• “Not feeling well”
• Reduced productivity over two shifts – monitored in real time
• Referred by supervisor to physician
• Same day appointment

L.C.
• Febrile
• Distended, tympanitic abdomen
• Diagnosed with bowel obstruction
• Surgery that same day
• Regional anesthesia with sedation
• Brief exploratory laparotomy, relief of volvulus
• Antibiotics, fluids

L.C.
• Rapid convalescence (1-2 hours)
• Normal appetite at dinner time
• Returned to work on evening shift
• Productivity restored < 36 hours after onset of symptoms

Is this Quality?
• It’s accessible!
• It’s adaptable!
• It’s efficient!
• It’s modern!
• It’s inexpensive!
• It’s Effective!
It’s not humanIt’s not human

Elsie

W
Quality in Anesthesiology




Prehistoric AIMS



25







04/19/2333


The Future As It Used To Be

We live in the Information Age…
“Your data is going to be collected. Do you want it to be gathered by your friends or by your enemies?”
-- Keith Ruskin, MD
* Goofy picture of Keith obtained in 5.4 seconds of internet search.
*

• A non-profit 501(c)3 corporation
• Vision: To become the primary source for quality improvement in the clinical practice of anesthesiology
• Mission: To establish and maintain the National Anesthesia Clinical Outcomes Registry
The AQI
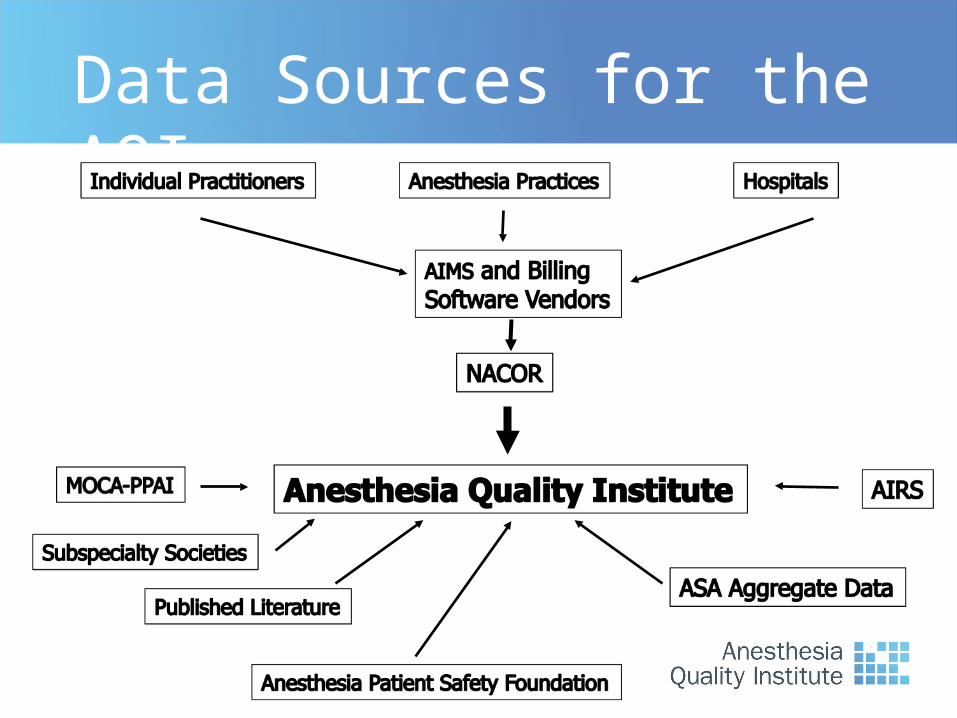
Data Sources for the AQI

AQI Registries
• NACOR
• AIRS
• PPAI
04/19/2339

NACOR: the National Anesthesia Clinical Outcomes Registry
• Electronic capture
• All cases (no bias)
• All available data
• De-identified, but with context
• Automated reporting
• Automated validation
• Analysis and reporting

AQI Reporting
Practice Recruitment Process
• Legal agreements
• Practice Demographic Survey
• Technical assessment
• Data transmission
04/19/2342

What to Collect?
• Quality Improvement data
• Hospital EHR / EMR data
• AIMS data
• Administrative / Billing data

“Knowledge is Power”
-- Sir Francis Bacon, 1597
“Let’s Dance!”
-- Kevin Bacon, Footloose, 1984

NACOR to date
• > 800 interested groups
• 160 participating practices
• Case data from:– 100 groups– 1100 facilities– 8,500 providers
–4,500,000 cases
04/19/2345

Age and ASA Physical Status
04/19/2346

Patient Age
04/19/2347

Anesthesia Type
04/19/2348

Carpal Tunnel Release

Reporting Drill-Down

Measure Group
Description (n=814,890 cases) Events Incident Rate
Process Process outcomes 11,201 1.37%
Major Serious adverse events; actual patient harm or significant risk 3,539 0.43%
Minor Minor adverse event; without long-term impact 85,210 10.46%
Admin Administrative outcomes; such as case cancel, extended PACU, unexpected admission 11,420 1.40%
Mortality Patient death; excluding patients presenting for organ harvesting 293 0.04%
Outcomes

Mortality
Easy to define
Easy to count
Should be a good way to define effectiveness …
…right?

Anesthesia Mortality Estimates
Mortality in elective outpatient surgery:
7.8/million in ASCs (92/million in offices)
(Vila et al. Arch Surg 2003)
Mortality within 30 days of admission:
4/hundred at the Shock Trauma Center
(Dutton et al. J Trauma 2010)

12
8
16
24
32
36
40
44
28
20
4
1
12
8
16
24
32
36
40
28
20
4
44
1
Changes in Hospital Ranks After Risk Adjustment for 30-day Mortality
Rank by unadjustedmortality rate (%)(1 = lowest rate)
Risk Adjustment from NSQIP

Risk Adjustment of Trauma Mortality
0
1000
2000
3000
4000
5000
6000
7000
0
1
2
3
4
5
6
7
8
9
10
Admissions
Deaths
z-score

Utopia Principle #1
Align the Incentives
•Pursue capitation
•Share the incentives with all providers

Utopia Principle #2
Get the most out of expensive resources
•Beds should be filled
•ORs should be utilized
•Physicians should do physician stuff

Utopia Principle #3
Healthcare is an Information Business*
*Invest accordingly!

Utopia Principle #4
Software
Requires
Liveware

Utopia Principle #5
Quality, Safety and Efficiency are the
same thing
•Re-work takes time and costs money
•The best care is usually the most efficient

Utopia Principle #6
What isn’t measured, can’t be improved

Utopia Principle #7
Patients do the Darndest Things

“Bottom-up QM”
• Sometimes, strange stuff happens
• Learning from these episodes is critical
• Never make the same mistake twice!

The Anesthesia Incident Reporting System (AIRS)
• Maintained by AQI• Separate registry
from NACOR• Designed for detailed
individual reports• Some practices enter
everything• Co-reporting to
hospital QM program

“The unexamined life is not worth living.”
-- Socrates, Apology 38a

Have I forgotten anything?


















