THE RELATIONSHIP BETWEEN RESPIRATORY SINUS ARRHYTHMIA, AFFECTIVE DECISION-MAKING AND PSYCHOPATHIC TRAITS IN AGGRESSIVE YOUTH by HALEY LAVINDER FORD JOHN E. LOCHMAN, COMMITTEE CHAIR ANSLEY GILPIN JEFF PARKER MARTI RICE MARTIN SELLBOM A DISSERTATION Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Psychology in the Graduate School of The University of Alabama TUSCALOOSA, ALABAMA 2012
Transcript
THE RELATIONSHIP BETWEEN RESPIRATORY SINUS ARRHYTHMIA,
AFFECTIVE DECISION-MAKING AND PSYCHOPATHIC TRAITS
IN AGGRESSIVE YOUTH
by
HALEY LAVINDER FORD
JOHN E. LOCHMAN, COMMITTEE CHAIR ANSLEY GILPIN
JEFF PARKER MARTI RICE
MARTIN SELLBOM
A DISSERTATION
Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy
in the Department of Psychology in the Graduate School of
The University of Alabama
TUSCALOOSA, ALABAMA
2012
Copyright Haley Lavinder Ford 2012 ALL RIGHTS RESERVED
ii
ABSTRACT
The current study, which is a secondary data analysis from a larger grant-funded
intervention research project, attempted to elucidate the relationship between psychopathic traits,
respiratory sinus arrhythmia, and performance on the Iowa Gambling Task. Approximately 120
10- and 11- year-old children were initially assessed at baseline, and 111 participants (67% male)
comprised the final sample. Parents reported on observed behaviors indicative of psychopathic
traits, as measured by the Antisocial Process Screening Device (i.e., impulsivity/conduct
problems, callous-unemotional traits, and boldness). Children also completed the computerized
version of the Iowa Gambling Task, an affective decision-making task with risky and
advantageous decks of cards. During the task, electrodes measured interbeat interval, from
which respiratory sinus arrhythmia was derived. While none of the analyses examining the
influence of RSA, psychopathic traits, and their interaction was significant, a developmental
trend was observed with regard to performance on the IGT and CU traits. Specifically, the
correlation between CU traits and IGT performance in block five was significant for the oldest
third of the sample, which suggests that affective decision-making is influenced by
developmental level. This finding suggests that examining the construct of affective decision-
making in young samples is valid, but perhaps only in older youth (i.e., at least 10.5 years old in
this sample).
iii
LIST OF ABBREVIATIONS AND SYMBOLS
ACC Anterior cingulate cortex
ADHD Attention Deficit/Hyperactivity Disorder
ANS Autonomic nervous system
APSD Antisocial Process Screening Device
BASC Behavioral Assessment System for Children
CBCL Child Behavior Checklist
CD Conduct Disorder
CNS Central nervous system
CU Callous unemotional
DBD Disruptive behavior disorders
DLPFC Dorsolateral prefrontal cortex
HR Heart rate
IBI Interbeat interval
IGT Iowa Gambling Task
IQ Intelligence quotient
IMP/CP Impulsivity/Conduct problems
M Mean
N Sample size
NPIC Narcissism Personality Inventory-Children
ODD Oppositional Defiant Disorder
OFC Orbitofrontal cortex
p Probability associated with the occurrence under the null hypothesis
iv
PCL:R Psychopathy Checklist-Revised
PCL:YV Psychopathy Checklist: Youth Version
PFC Prefrontal cortex
PNS Parasympathetic nervous system
PPI Psychopathic Personality Inventory
r Pearson product-moment correlation
RSA Respiratory sinus arrhythmia
RSA-R Respiratory sinus arrhythmia-reactivity
SC Skin conductance
SCR Skin conductance reactivity
SD Substance dependence
SD Standard deviation
SE Standard error
SNS Sympathetic nervous system
SRP-II Self-Report Psychopathy Scale-II
VPC Ventromedial prefrontal cortex
VT Vagal tone
α Cronbach’s index of internal consistency
< Less than
> Greater than
= Equal to
v
ACKNOWLEDGEMENTS
I would like to express my appreciation to everyone who helped me through the various
stages of completing this dissertation. First, thank you to my dissertation committee. To my
advisor, Dr. John Lochman, you supported my interest in working with physiological data by
funding my attendance at a workshop, helped me navigate the numerous challenges posed by the
physiological data, and provided guidance while also fostering my independence. To the other
members of my committee, Dr. Martin Sellbom, Dr. Ansley Gilpin, Dr. Jeff Parker, and Dr.
Marti Rice, you provided me with invaluable feedback at the different stages of my dissertation.
You helped me to think even more critically about the questions I was asking in my project and
how to better approach the analyses as well as the conceptualization of both the overall project
and specific constructs.
I would also like to thank Dr. Keri Heilman at the University of Illinois at Chicago for
providing guidance on editing the physiological data and giving advice on how to approach my
analyses using respiratory sinus arrhythmia in a meaningful manner. Finally, Dr. Heilman also
provided me with additional resources to answer some of the more technical questions that arose
while working on this project.
Dr. Jim Mintz of the STRONG STAR research consortium at the University of Texas
Health Science Center at San Antonio generously provided several hours of his time to help me
with the numerous challenges I faced with data analysis. He carved out time for me at a very
busy time in our office, and I am incredibly grateful for his advice and input. And, perhaps even
more importantly, Dr. Mintz was a source of much needed humor that helped me to maintain my
focus and determination.
vi
Finally, to my family and friends—To my mother and father, your constant support has
been much needed and appreciated throughout all of graduate school. I am finally done, and I
cannot wait to share graduation day with you. I would not have made it this far without both of
you. To my friends, there are too many of you to list everyone, but you know who you are. I
truly could not have done this without your support, which got me through the toughest phases of
my dissertation. Nonetheless, I do want to mention a few who were there for me at various times
during this process: Marie Moore Channell, Melissa Machac, Tiarney Ritchwood, Sarah Ryan,
Finis Nabors, and “Captain” Keith. In each of your own ways, you provided support and
encouragement that has been incredibly meaningful to me.
vii
CONTENTS
ABSTRACT ……………………………………………………………………….………………….ii
LIST OF ABBREVIATIONS AND SYMBOLS ………………………..……………………...........iii
a. Recruitment and Screening of Participants………………………………………………………...33
b. Procedure…………………………………………………………………………………………..35
c. Screening Measures………………………………………………………………………………..36
d. Time 1 Pre-intervention Measures……………………………………………………………..…..37
e. Missing Data……………………………………………………………………………………….41
f. Power Analysis………………………...………………………………………………………….. 44
3. DATA ANALYSIS AND RESULTS……………………………………………………………..45
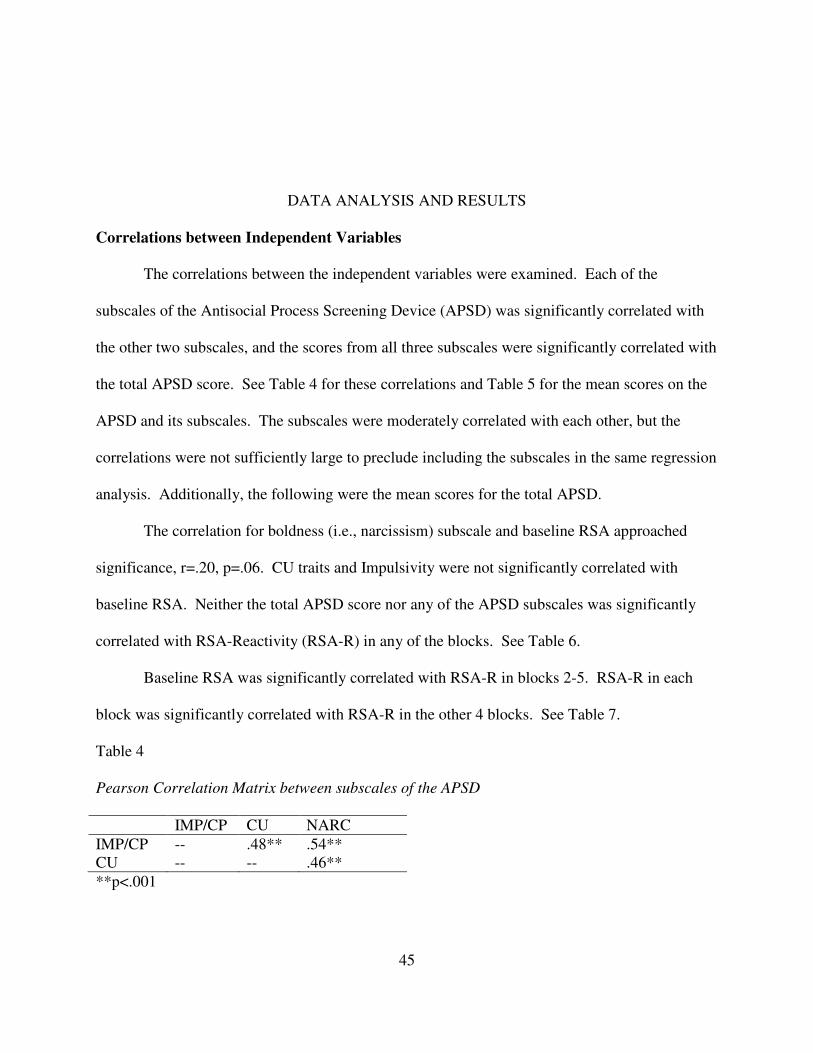
a. Correlations between Independent Variables……………………………………………………...45
b. Correlations between Independent and Dependent Variables………………………………..........46 c. IGT Performance and Correlations by Block……………………………………………………...48 d. Potential Covariates……...…………………………………………………………………...........49
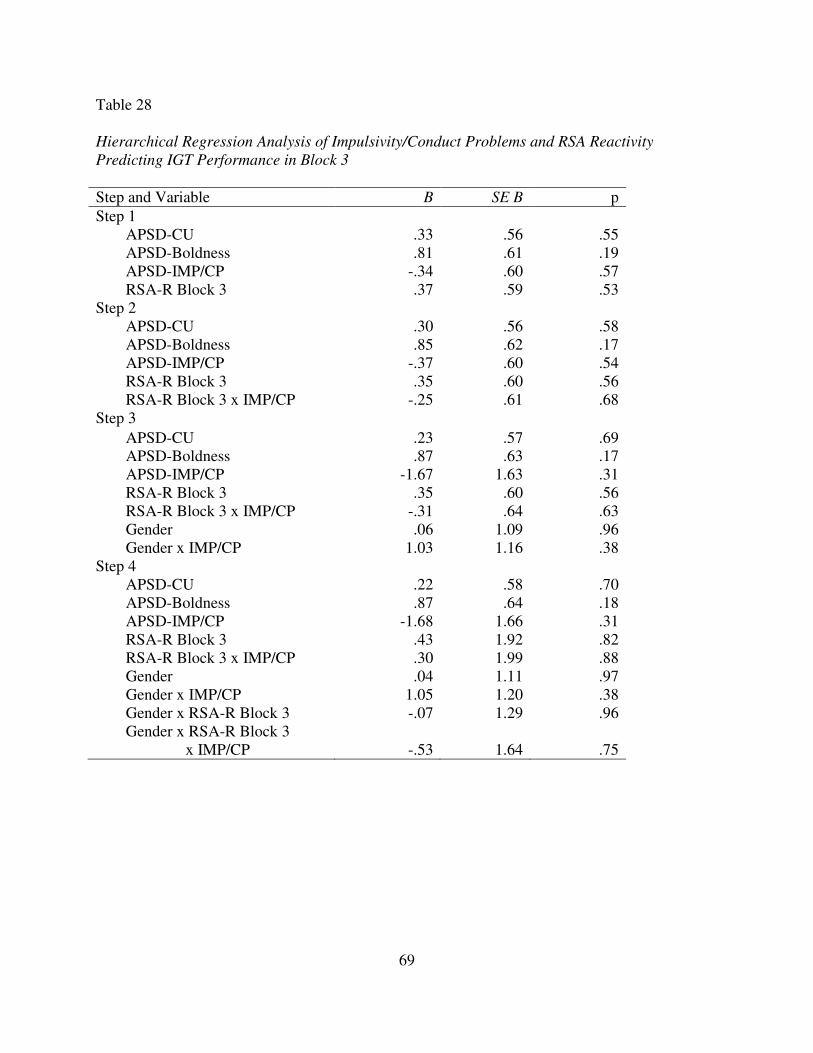
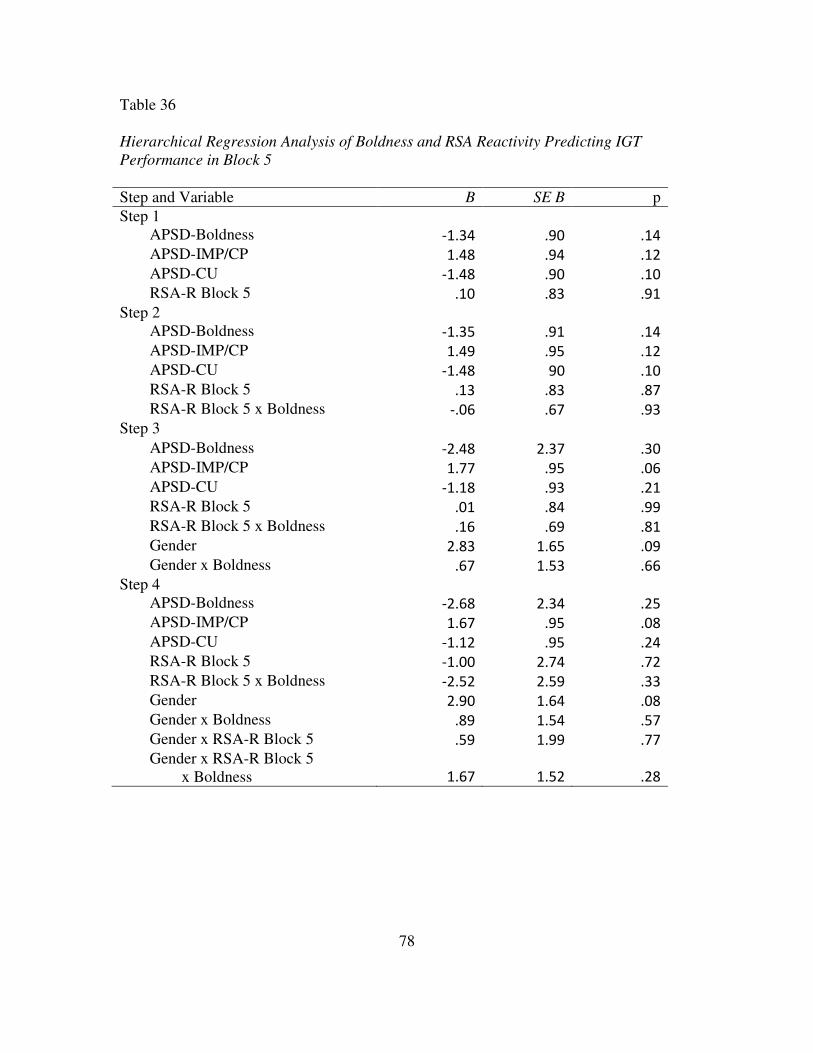
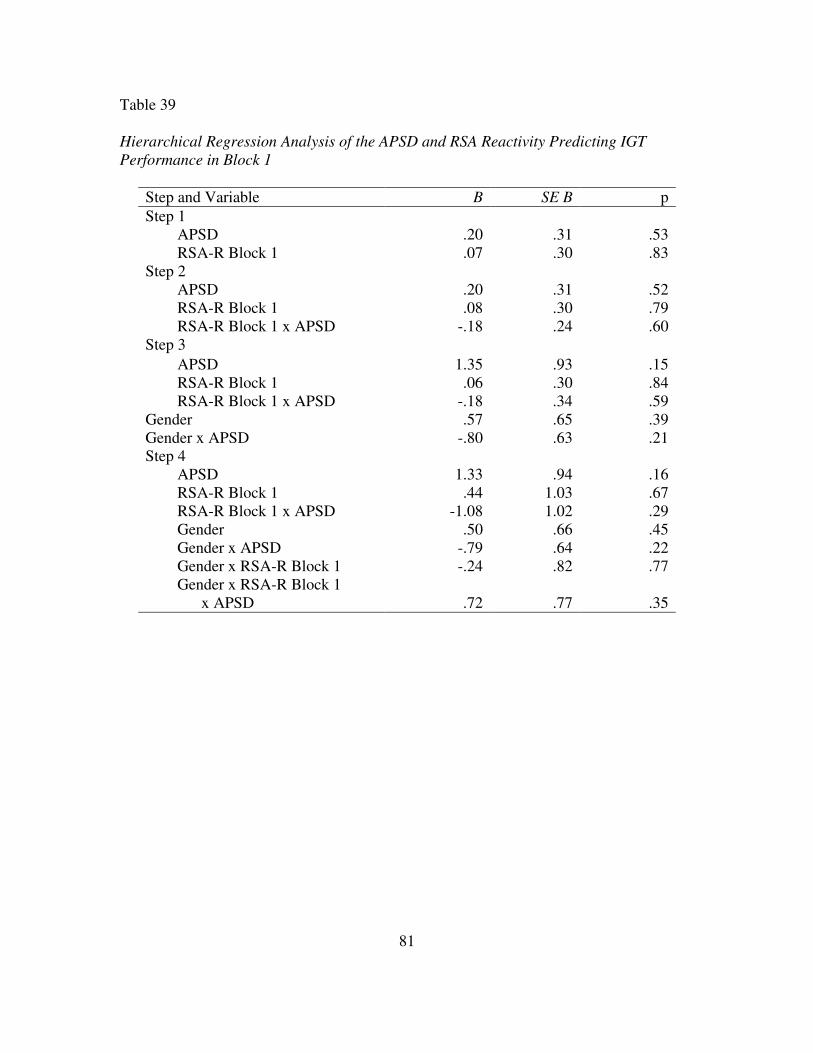
e. Primary Analyses……………………………...……………………………………………...........50
viii
f. Secondary Analyses…………………..………………………………………………………..…. 57
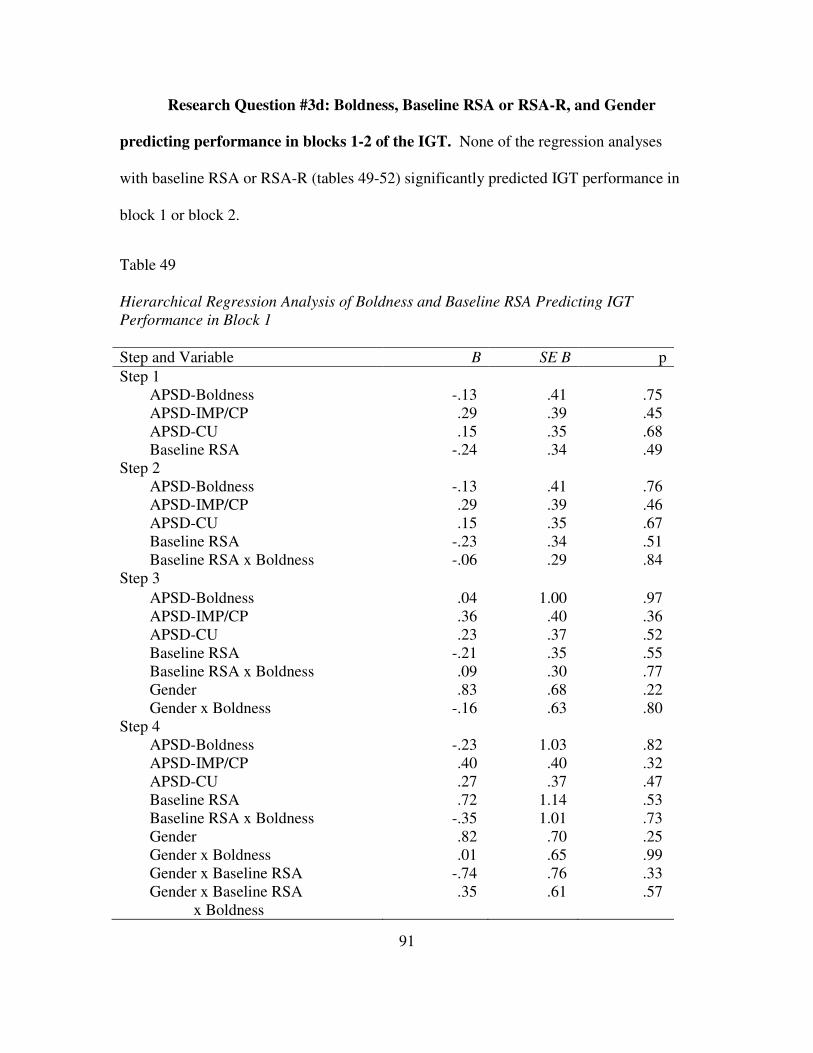
APSD-IMP/CP -.54 .54 .33 APSD-CU .30 .51 .59 RSA-R Block 2 1.19 1.72 .49 RSA-R Block 2 x Boldness -.24 1.75 .89 Gender 1.06 1.00 .29 Gender x Boldness .50 .95 .60 Gender x RSA-R Block 2 -.97 1.32 .47 Gender x RSA-R Block 2 x Boldness .34 1.27 .79
95
DISCUSSION
This section will discuss the findings for psychopathic traits and RSA, physiological
activity and IGT performance, and then psychopathic traits, RSA, and IGT performance. Next,
the themes of developmental and measurement issues (e.g., respirations measurement in
quantifying RSA) is addressed, followed by a discussion on power. The discussion section
concludes with limitations and future directions.
Main Effects of Psychopathy and Respiratory Sinus Arrhythmia
Neither of the hypotheses was supported. No main effects were found for psychopathy
(i.e., total APSD score), baseline RSA, or RSA reactivity when predicting performance in blocks
3-5 of the IGT. Hypothesis 1, which predicted that baseline RSA and the total APSD score
would be negatively correlated, was not supported. The rationale for this hypothesis stemmed
from research that has shown that decreased baseline RSA is associated with several symptoms
of psychopathology, including aggression. It is also possible that the multifaceted nature of the
construct of psychopathy may account for the observed result since the different components
(i.e., boldness, callous unemotional traits, and impulsivity/conduct problems) are associated with
different patterns of physiological activity.
Similarly, hypothesis #2, which examined the influence of psychopathy and RSA (both
baseline and reactivity) on IGT performance, failed to yield significant results. While it was
predicted that psychopathic traits would predict IGT performance, there are a few possibilities
why this hypothesis was not supported. First, the range of scores on the APSD was 2-26 in
96
sample of fourth grade males and females attending mainstream public schools. In a study by
Blair et al. (2001) that found boys with high levels of psychopathic traits as measured by the
APSD performed poorly on the IGT, the range of scores for youth with psychopathic traits was
26-37, while the comparison group’s scores ranged from 0-18. In Blair et al.’s study, a score
greater than 25 on the APSD was considered the cutoff for the psychopathic group, which is
already at the top end of the range in the current study. Additionally, the age range was wider
(9-17 year olds), and older youth simply have had more time to exhibit the behaviors and
personality traits indicative of psychopathy than the youth, with a mean age of 10.3 years, in this
study did. Finally, their sample was drawn from schools for boys with emotional and behavioral
problems, while this study used a community sample, in which the degree of emotional and
behavioral problems associated with psychopathy are typically less severe. In other words, it is
possible that the lack of significant results could be true findings since the degree of psychopathy
was not very severe.
Physiological activity and IGT Performance
Research has shown that low-performing normal individuals (i.e., without brain damage)
did not have anticipatory slowing of heart rate (Drucaroff et al., 2011). Extrapolating this
finding of the absence of heart rate deceleration and poor IGT performance to the current study,
a lack of heart rate deceleration could be reflected by vagal withdrawal, which could be
indicative of greater sympathetic activity that, in turn, is associated with poorer performance on
the IGT. However, this conjecture is speculative, and further research needs to be conducted on
the relationship between parasympathetic activity, sympathetic activity, and IGT performance.
Specifically, the joint activity of the two branches of the autonomic nervous system should be
evaluated simultaneously because there are several possible patterns of activity, including
97
coactivation (e.g., reciprocal activity), coinhibition (e.g., reduced activity in both branches), or
independent activity (Beauchaine, 2009).
Psychopathic traits, RSA, and IGT Performance
As mentioned above, no significant main effects were found for the hypotheses or
secondary analyses examining the effects of baseline RSA and psychopathic traits on IGT
performance. Previous research has found positive, negative, and null findings in studies
examining the relationship between externalizing behaviors and baseline RSA. While no study
to date has specifically addressed the relationship between baseline RSA and psychopathic traits,
such traits are more commonly observed in youth with externalizing difficulties (i.e., aggression,
symptoms of ADHD). The sample in this study was selected based on elevated levels of
aggression, which is more common in non-clinical samples than are psychopathic traits. This
pattern of lower levels of psychopathy was evident in this sample, as the scores obtained on the
APSD were more heavily concentrated at the lower end of the range of possible scores.
Additionally, the lack of a relationship between psychopathy, respiratory sinus arrhythmia, and
the IGT that was found in this study appears to mirror the null findings that have been found in
studies examining RSA in aggressive youth. One possibility is that these youth already have
depressed levels of RSA due to being aggressive, which may explain the non-significant results
for psychopathy and baseline RSA found in this study. Finally, breaking down the APSD to its
three subscales, the scores obtained on the CU subscale had a similar pattern with a small
number of participants scoring in the higher range. Overall, the same pattern held true for the
other two subscales, impulsivity/conduct problems and boldness. Given that the scores on these
subscales are more heavily weighted at the lower end of the possible ranges, the true nature of
the relationships between baseline RSA and psychopathic traits may have been obscured.
98
Research has also found no consistent findings with regard to baseline autonomic activity
(Patrick, 2008), which has been attributed to the different facets of psychopathy. With regard to
CU traits, youth with CU traits have depressed physiological activity. For example, it has been
found that they have lower resting heart rates and less heart rate and skin conductance reactivity
than non-CU youth (Anastassiou-Hadjicharalambous & Warden, 2008). It is possible that the
youth with CU traits in this study experienced less RSA reactivity, which could explain the lack
of significant findings.
Little research has been done on impulsivity alone. Rather, studies have examined
impulsivity in the context of externalizing disorders, which makes discerning the relationship
between impulsivity and baseline RSA difficult. For example, Boyce, Quas, Alkon, Smider, &
Essex’s (2001) externalizing disorders category was comprised of conduct disordered and
oppositional defiant behaviors, impulsivity, hostility, and attention problems. They found that
the externalizing group had low sympathetic and parasympathetic reactivity. Beauchaine et al.
(2001) found that a sample of impulsive youth with conduct disorder also had reduced RSA
activity. These findings suggest that impulsivity alone would also be associated with reduced
RSA reactivity, which, similar to the discussion for CU traits, could be a reason for the absence
of significant results.
Finally, as mentioned in the introduction, comparatively little research has been done on
boldness (i.e., the subscale labeled narcissism on the APSD) and RSA in youth. Narcissism and
boldness are distinct constructs, with the former being traditionally operationalized as having
high but fragile self-esteem and the latter characterized by fearless dominance. Boldness is also
linked with an ability to stay calm in the presence of stressors as well as having tolerance for
uncertainty (Patrick, 2008). Physiologically, these traits may be associated with less
99
physiological reactivity, which may be one reason for the lack of significant findings in this
study.
Developmental Differences
RSA and Developmental Differences. Studies examining RSA have been conducted
with aggressive children as young as two years of age (e.g., Calkins & Dedmon, 2000), 2-5 year
old children at risk for developing externalizing behavioral problems (Calkins, Blandon, et al.,
2007), early school-age children (mean age 7.79 years) with low SES who were from the inner
city (Bubier & Drabick, 2008), 6-7 year old in a community sample (Boyce et al., 2001), as well
as 12-17 year olds males with ADHD or aggressive conduct disorder (Beauchaine et al., 2007).
Significant findings regarding differences in RSA were obtained in these studies, which suggests
that using RSA in this sample was appropriate.
Additionally, research has also shown that depressed sympathetic and parasympathetic
nervous system activity are related to externalizing behavior, but the nature of the relationship is
dependent upon the type of behavior (e.g., ADHD vs. CD) and the age of the participants (Bubier
& Drabick, 2008). For example, only SNS activity is depressed in preschool children with
ADHD and ODD diagnoses while both SNS and PNS activity are depressed in older youth (i.e.,
mid-childhood and adolescence). This pattern of depressed ANS activity has been found in both
middle class and inner-city at risk samples, and it remained significant even after controlling for
race and SES. In summary, the lack of findings regarding RSA is likely not attributable to the
developmental level of the youth in this study, but perhaps could be linked to the nature of
psychopathology examined. While psychopathy shares some similarities with externalizing
behaviors (e.g., conduct problems), it is a distinct cluster of behaviors that has different patterns
100
of physiological activity (i.e., less skin conductance). This study was the first to attempt to
elucidate the relationship between RSA and psychopathic traits in youth.
IGT and Developmental Differences. The IGT measures affective decision-making,
which is influenced by developmental level. As previously discussed, older children typically do
better on the IGT than younger children (Crone & Van der Molen, 2004). The correlation
between CU traits and IGT performance in block five was significant, which suggests that
affective decision-making is influenced by developmental level. In other words, examining the
construct of affective decision-making in young samples is valid, but perhaps only in older youth
(i.e., at least 10.5 years old in this sample).
One possible reason for the differences in performance on the IGT by younger and older
youth is related to brain development. A key task during adolescence is development of parts of
the brain responsible for assessment of risk and reward (Steinberg, 2005). Specifically, the
prefrontal cortex does not fully mature until later in adolescence (Crone & Van der Molen,
2004). Better performance on the IGT depends on the ability to make decisions that are
advantageous in the long-term, which is dependent on the ventromedial prefrontal cortex. In
other words, in younger children, the ventromedial prefrontal cortex is still developing, so their
ability to make advantageous decisions is less developed than that of older children. The
performance of younger children has been likened to that of patients with ventromedial
prefrontal damage, who demonstrate myopia for the future by making more disadvantageous
choices (Crone & van der Molen, 2004).
Measurement Issues
RSA and measurement of respiration. To obtain accurate values of RSA, a minimum
of 30 seconds of data is needed. Given this limitation, it was not possible to measure RSA for
101
the immediate period of time after a decision was made. As a result, RSA was measured over
the average duration of each block on the IGT. Other physiological measures, such as skin
conductance, can be accurately measured in shorter time periods (e.g., Deming, 2009). Because
RSA was measured during each block of the IGT, it is possible that any changes in physiological
activity were not captured due to the participants returning to their baseline levels during the
period of time RSA was measured. In other words, any changes in RSA may have been washed
out or obscured in the 30 seconds of data used to quantify RSA. Future research may benefit
from examining two different forms of physiological activity simultaneously to more accurately
ascertain the influence psychophysiology has on decision-making in the context of psychopathic
traits.
Different methods of quantifying RSA exist, and these approaches sometimes differ on
whether or not respiration frequency needs to be measured (Denver, Reed, & Porges, 2007).
Some methods assume there is a causal relationship between respiration and RSA, and these
approaches make adjustments when quantifying RSA. For example, respiratory parameters can
be included as covariates when quantifying RSA (Denver et al.). In contrast, other approaches
assume there is a parallel relationship between RSA and breathing. These approaches either do
not incorporate respiration frequency at all, or they use a frequency band associated with
respiratory rates for the population of interest (e.g., adolescents).
The method used to measure RSA in this study, a time domain method which was
described earlier, measures heart rate variability within a frequency range of spontaneous
breathing associated with the population of interest (i.e., children in this study). Respiration is
not specifically measured in this approach.
102
Another procedure, spectral analysis, collects respiration (i.e., frequency of breathing)
and heart period data that is then decomposed to identify the peak frequencies, which are
“obtained by locating the frequency at which the maximum spectral density occurred” (Denver,
p. 290). RSA obtained by a time domain method (i.e., using a moving polynomial filter (MPF))
and respiration frequency obtained by the same method were highly correlated, r=.99,
p<.01(Denver et al.). Additionally, to ascertain whether depth of breathing affected this
relationship, Denver and colleagues transformed the respiration data into a binary time series to
remove the influence of respiration depth and then conducted spectral analysis. The correlation
between the frequency of the binary transformed respiration data and the frequency of RSA from
the time domain method remained very high (r=.99, p<.01). Finally, to ensure that the time
domain method did not artificially limit the respiration frequency through the use of filter that
removes variance associated with frequencies lower than those of spontaneous breathing, the
respiration data were detrended with a linear function rather than the moving polynomial
function. Again, results suggested that the correlation between the frequency of RSA obtained
using the MPF and linearly detrended respiration frequency was r= .99, p<.01.
Finally, the RSA amplitudes obtained from spectral analysis were correlated with the amplitudes
obtained from the time domain method. The amplitudes from each method were highly
correlated with each other, r=.99.
Based on these findings, it was concluded that measuring respiration is not a requirement
when quantifying RSA. In further support of this conclusion, Denver et al. summarized research
published in Biological Psychology and Journal of Psychophysiology between 2000-2004 that
included unadjusted and adjusted RSA amplitudes. The results indicated that using correction
procedures (i.e., using respiration frequency, tidal volume, or both as covariates) was not
103
supported, as no differences were found. Thus, in summary, research has shown that there is no
relationship between RSA amplitude and the frequency of respiration, and this pattern remained
even when the respiration data was transformed (e.g., linear, binary) (Denver et al.). This
finding suggests that it is not statistically necessary to include the latter variable as a covariate to
generate an accurate measure of RSA amplitude.
Limitations
This study has a few limitations. First, power was a little low due to IGT data not being
available for a cohort and missing data within the available dataset. Even after multiple
imputation, the sample size remained below the needed sample size of 167 to achieve acceptable
power (i.e., power = .80). However, despite being smaller than needed, the sample used was
sufficient for examining the general direction of relationships as several trends were observed.
Overall, having more participants may not have made a substantial difference for several of the
analyses, as many of the obtained results were clearly not significant.
Second, only parasympathetic nervous system activity was examined. Examining the
activity of both the parasympathetic and sympathetic nervous systems may result in a more
accurate characterization of the psychophysiological activity associated with psychopathic traits
and the influence of these two physiological variables on IGT performance. For example,
Crowell, Beauchaine, Gatzke-Kopp, Sylvers, Mead, & Chipman-Chacon (2006) have used skin
conductance and Keller & El-Sheikh (2009) used salivary alpha-amylase, both of which reflect
sympathetic activity and could be examined in conjunction with RSA.
Additionally, low autonomic nervous system (ANS) arousal is associated with antisocial
behaviors in children and adults. Low ANS arousal can be arrived at by different combinations
of sympathetic and parasympathetic nervous system activity. For example, low sympathetic
104
activity (e.g., sympathetic inhibition) and high PNS activity (e.g., high baseline RSA or RSA
augmentation (higher RSA)) result in less ANS arousal. Raine (2002) proposed that youth with
this profile of ANS activity (i.e., lower sympathetic and higher parasympathetic activity) might
be similar to those who are antisocial and exhibit less fear of punishment or of negative
consequences. Finally, Keller and El-Sheikh (2009) suggest that children with SNS underarousal
alone are not necessarily at risk for externalizing problems and that it is the combination of
sympathetic nervous system underarousal and higher baseline RSA or greater RSA augmentation
that is associated with externalizing symptoms.
Another issue related to study design is that there was no control group of non-aggressive
children. Prior research has shown that low resting heart rate distinguishes between adolescents
who desist from criminal behavior and those who continue to offend (Raine, 2002). This is a
community sample, which is probably more homogeneous in its degree of criminal activity (i.e.,
relatively low level), and thus it likely is substantively different from one characterized by on-
going criminal behavior. Having a control group would allow for examination of differences in
baseline RSA and RSA reactivity between the aggressive and non-aggressive youth. Finally, this
sample is also largely male and African-American. Different findings may emerge in samples
with different demographic characteristics.
Strengths and Future Directions
This study sought to delineate the nature of the relationship between psychopathic traits,
psychophysiological activity, and affective decision-making. One of the primary strengths of
this study is that both behavioral and psychophysiological measures were used to examine
performance on the IGT. According to Boyce et al. (2001), greater understanding of
psychopathology depends on using assessments drawing from different domains, such as
105
physiology and behavior.
A second strength is that this is one of the first studies that has specifically examined the
relationship between psychopathic traits and RSA. The relationship between RSA and
psychopathy should be explored in future studies that use both community and clinical samples,
the latter of which will have greater degrees of psychopathic traits. Additionally, sympathetic
nervous system activity should be examined in conjunction with vagal activity in future research
in an effort to delineate the true relationship between autonomic nervous system activity,
psychopathic traits, and decision-making.
With regard to the constructs of narcissism and boldness, because it appears that these
constructs tap different traits, it is reasonable to suggest that they may be associated with
different patterns of psychophysiological activity. Thus, using a measure that assesses
narcissism may yield different results than were observed in this study, which measured
boldness. There has been some research conducted on the construct of narcissism as
traditionally operationalized (i.e., high but fragile self esteem) in adults and with physiological
measures reflecting sympathetic nervous system activity. Even less research on narcissism and
psychophysiological activity has been carried out with younger samples. Future research should
examine the relationship between RSA and narcissism, as traditionally conceptualized, and
boldness to further characterize these constructs.
Finally, given the developmental differences observed in IGT performance in this study,
future studies should be conducted with older adolescents. It is possible that some of the
relationships examined in this study might differ in an older sample of adolescents, whose brains,
particularly the ventromedial prefrontal cortex, will be more developed.
106
REFERENCES
Achenbach T.M. Integrative guide for the 1991 CBCL/4-18, YSR & TRF profiles. Burlington,
VT: University of Vermont Department of Psychiatry; 1991. Anastassiou-Hadjicharalambous, X. & Warden, D. (2008). Physiologically-indexed and self-
perceived affective empathy in conduct-disordered children high and low on callous-unemotional traits. Child Psychiatry and Human Development, 39, 503-517. doi:10.1007/s10578-008-0104-y
Andershed, H., Gustafson, S.B., Kerr, M., & Stattin, H. (2002). The usefulness of self-reported
psychopathy-like traits in the study of antisocial behavior among non-referred adolescents. European Journal of Personality, 16, 383-402. doi:10.1002/per.455
Andrade, J.T. (2008). The inclusion of antisocial behavior in the construct of psychopathy: A
review of the research. Aggression and Violent Behavior, 13, 328-335. doi:10.1016/j.avb.2008.05.001
Ang, R.P. & Raine, A. (2009). Reliability, validity, and invariance of the narcissistic personality
questionnaire for children-revised (NPQC-R). Journal of Psychopathology and
Barry, C.T., Frick, P.J., DeShazo, T.M., McCoy, M.G., Ellis, M. and Loney, B.R. (2000). The
importance of callous-unemotional traits for extending the concept of psychopathy to children. Journal of Abnormal Psychology, 109(2), 335-340. doi:10.1037/0021-843X.109.2.335
Barry, C. T., & Wallace, M. T. (2010). Current considerations in the assessment of youth
narcissism: Indicators of pathological and normative development. Journal of
Psychopathology and Behavioral Assessment, 32, 479-489. doi:10.1007/s10862-010- 9188-3
Beauchaine, T. P. (2009). Some difficulties in interpreting psychophysiological research with children. Monographs of the Society for Research in Child Development, 74(1), 80-88. doi:10.1111/j.1540-5834.2009.00509.x
Beauchaine, T.P., Gatzke-Kopp, L., & Mead, H.K. (2007). Polyvagal theory and developmental
psychopathology: Emotion dysregulation and conduct problems from preschool to adolescence. Biological Psychology, 74(2), 174-184. doi: 10.1016/j.biopsycho.2005.08.008.
107
Beauchaine, T.P., Hong, J., & Marsh, P. (2008). Sex differences in autonomic correlates of conduct problems and aggression. Journal of the American Academy of Child and
psychopathology in male adolescent: Discriminating conduct disorder from attention-deficit/hyperactivity disorder through concurrent assessment of multiple autonomic states. Journal of Abnormal Psychology, 110(4), 610-624. doi:10.1037/0021-843X.110.4.610
Bechara, A. (2004). The role of emotion in decision-making: Evidence from neurological
patients with orbitofrontal damage. Brain and Cognition, 55, 30-40. doi:10.1016/j.bandc.2003.04.001
Bechara, A., Damasio, H., & Damasio, A. R. (2000). Emotion, Decision-making and the
Orbitofrontal Cortex. Cereb. Cortex, 10, 295-307. doi:10.1093/cercor/10.3.295 Bechara, A., Damasio, H., Damasio, A.R., & Lee, G.P. (1999). Different contributions of the
human amygdala and ventromedial prefrontal cortex to decision-making. The Journal of
Neuroscience, 19(13), 5473-5481. Bechara, A., Damasio, H., Tranel, D., & Damasio, A.R. (1997). Deciding advantageously before knowing the advantageous strategy. Science, 275(5304), 1293-1295.
doi:10.1126/science.275.5304.1293 Bechara, A., Dolan, S., Denburg, N., Hindes, A., Anderson, S.W., & Nathan, P.E. (2001).
Decision-making deficits, linked to a dysfunctional ventromedial prefrontal cortex, revealed in alcohol and stimulant abusers. Neuropsychologia, 39, 376-389. doi:10.1016/S0028-3932(00)00136-6
Blair, R. J. R., (1999). Responsiveness to distress cues in the child with psychopathic
tendencies. Personality and Individual Differences, 27, 135-145. doi:10.1016/S0191-8869(98)00231-1
Blair, R.J.R. (2007). The amygdala and ventromedial prefrontal cortex in morality and
psychopathy. Trends in Cognitive Science, 11, 387-392. doi:10.1016/j.neuron.2007.07.022
Blair, R.J.R., Colledge, E., & Mitchell, D.G.V. (2001). Somatic Markers and Response Reversal: Is there orbitofrontal cortex dysfunction in boys with psychopathic tendencies? Journal
of Abnormal Child Psychology, 29, 499-511. doi:10.1023/A:1012277125119 Blair, R.J.R., Jones, L., Clark, F., & Smith, M. (1997). The psychopathic individual: A lack of
responsiveness to distress cues? Psychophysiology, 34, 192-198. doi:10.1111/j.1469-8986.1997.tb02131.x
108
Blair, R.J.R., Monson, J., & Frederickson, N. (2001). Moral reasoning and conduct problems in children with emotional and behavioural difficulties. Personality and Individual
Differences, 31, 799-811. doi:10.1016/S0191-8869(00)00181-1 Boyce, W. T., Quas, J., Alkon, A., Smider, N. A., Essex, M. J., & Kupfer, D. J. (2001).
Autonomic reactivity and psychopathology in middle childhood. British Journal of
Psychiatry, 179,144-150. doi:10.1192/bjp.179.2.144 Brown, K., Atkins, M. S., Osborne, M. L., & Milnamow, M. (1996). A revised teacher rating
scale for Reactive and Proactive Aggression. Journal of Abnormal Child Psychology,
24(4), 473-480. doi:10.1007/BF01441569 Brown, R.P., Budzek, K., & Tamborski, M. (2009). On the meaning and measure of narcissism.
Personality and Social Psychology Bulletin, 35(7), 951-964. doi:10.1177/0146167209335461
Bubier, J. L., & Drabick, D.A.G. (2008). Affective decision-making and externalizing behaviors:
The role of autonomic activity. Journal of Abnormal Child Psychology, 36, 941-953. doi:10.1007/s10802-008-9225-9
Calkins, S. D., Blandon, A. Y., Williford, A. P., & Keane, S. P. (2007). Biological, behavioral,
and relational levels of resilience in the context of risk for early childhood behavior problems. Development and Psychopathology, 19, 675-700. doi:10.1017/S095457940700034X
Calkins, S.D. & Dedmon, S.E. (2000). Physiological and behavioral regulation in two-year-
old children with aggressive/destructive behavior problems. Journal of Abnormal
Journal of Behavioral Decision-making, 17, 297-311. doi:10.1002/bdm.475
CardioBatch software. Brain-Body Center, University of Illinois at Chicago. 2007. Christian, R. E., Frick, P. J., Hill, N. L., Tyler, L., & Frazer, D. R. (1997). Psychopathy and
conduct problems in children: II. Implications for subtyping children with conduct problems. Journal of the American Academy of Child & Adolescent Psychiatry, 36(2), 233-241. doi:10.1097/00004583-199702000-00014
109
Cohen, M. A. (1998). The monetary value of saving a high-risk youth. Journal of
Quantitative Criminology, 14, 5-33. Cooke, D.J. & Michie, C. (2001). Refining the construct of psychopathy: Towards a hierarchical model. Psychological Assessment, 13(2), 171-188. doi:10.1037/1040-3590.13.2.171 Crider, A. (2008). Personality and electrodermal response lability: An interpretation. Applied
Psychophysiology and Biofeedback, 33, 141-148. doi:10.1007/s10484-008-9057-y Critchley, H.D., Mathias, C.J., & Dolan, R.J. (2002). Fear conditioning in humans: The influence
of awareness and autonomic arousal on functional neuroanatomy. Neuron, 33, 653-663. doi:10.1016/S0896-6273(02)00588-3
Crone, E. A., Somsen, R. J. M., Van Beek, B., & Van Der Molen, M. W. (2004). Heart rate and
skin conductance analysis of antecendents and consequences of decision-making. Psychophysiology, 41, 531-540. doi:10.1111/j.1469-8986.2004.00197.x
Crone, E.A. & van der Molen, M. W. (2004). Developmental changes in real life decision making: Performance on a gambling task previously shown to depend on the
Curran, P.J., West, S.G., & Finch, J.F. (1996). The robustness of test statistics to nonnormality
and specification error in confirmatory factor analysis. Psychological Methods, 1, 16-29. doi:10.1037/1082-989X.1.1.16
DeLisi, M., Umphress, Z.R., & Vaughn, M.G. (2009). The criminology of the amygdala.
Criminal Justice and Behavior, 36, 1241-1252. doi:10.1177/0093854809343119 Deming, A.M. (2009). Anxiety, affective decision-making, and callous-unemotional traits:
Possible predictors and/or moderators of conduct problems over time (Doctoral dissertation). Retrieved from Dissertations and Theses database. (AAT 3385347)
Dietrich, A., Riese, H, Sondeijker, F.E.P.L., Greaves-Lord, K., van Roon, A.M., Ormel, J.,
Neeleman, J., & Rosmalen, J.G.M. (2007). Externalizing and internalizing problems in relation to autonomic function: A population-based study in preadolescents. Journal of
the American Academy of Child and Adolescent Psychiatry, 46(3), 378-386. doi: 10.1097/chi.0b013e31802b91ea
Dodge, K. A., & Coie, J. D. (1987). Social-information-processing factors in reactive and proactive aggression in children's peer groups. Journal of Personality and Social
Psychology, 53(6), 1146-1158. doi:10.1037/0022-3514.53.6.1146 Dolan, M. (2004). Psychopathic personality in young people. Advances in Psychiatric Treatment,
10(6), 466-473. doi:10.1192/apt.10.6.466
110
Dolan, M. (2008). Neurobiological disturbances in callous-unemotional youths. The American
Journal of Psychiatry, 165(6), 668-670. doi:10.1176/appi.ajp.2008.08030393 Dolan, M.C. & Rennie, C.E. (2006). Reliability and validity of the psychopathy checklist: youth version in a UK sample of conduct disordered boys. Personality and Individual
Differences, 40(1), 65-75. doi:10.1016/j.paid.2005.07.001 Doyle, A., Ostrander, R., Skare, S., Crosby, R.D., & August, G.J. (1997). Convergent and
criterion-related validity of the Behavior Assessment System for Children-Parent Rating Scale. Journal of Clinical Child Psychology, 26(3), 276-284. doi:10.1207/s15374424jccp2603_6
Drucaroff, L.J., Kievit, R., Guinjoan, S.M., Gerschcovich, E.R., Cerquetti, D., Leiguarda,
El-Sheikh, M., Keiley, M., & Hinnant, J.B. (2010). Developmental trajectories of skin conductance level in middle childhood: Sex, race, and externalizing behavior problems as predictors of growth. Biological Psychology, 83(2),116-124. doi:10.1016/j.biopsycho.2009.11.009
Essau, C.A., Sasagawa, S., & Frick, P.J. (2006). Callous-unemotional traits in a community sample of adolescents. Assessment, 13(4), 454-469. doi:10.1177/1073191106287354
Falkenbach, D.M., Poythress, N.G., & Heide, K.M., (2003). Psychopathic features in a juvenile
diversion population: reliability and predictive validity of two self-report measures. Behavioral Sciences and The Law, 21(6), 787-805. doi:10.1002/bsl.562
Faul, F., Erdfelder, E., Buchner, A., & Lang, A.G. (2009). Statistical power analyses using
G*Power 3.1: Tests for correlation and regression analyses. Behavior Research Methods,
41, 1149-1160. Forth, A. E., Kosson, D. S., & Hare, R. D. (2003). The Hare Psychopathy Checklist: Youth
Version. North Tonawanda, NY: Multi-Health Systems. Foster, J.D. & Trimm, IV, R.F. (2008). On being eager and uninhibited: Narcissism and
approach-avoidance motivation. Personality and Social Psychology Bulletin, 34(7),1004-1017. doi:10.1177/0146167208316688
Franken, I. H. A., van Strien, J. W., Nijs, I., & Muris, P. (2008). Impulsivity is associated with
Frick, P. J. (1995) Callous-unemotional traits and conduct problems: A two-factor model of psychopathy in children. Issues in Criminological and Legal Psychology, 24, 47-51. doi:10.1007/978-94-011-3965-6_8
Frick, P.J. (2009). Extending the construct of psychopathy to youth: implications for
understanding, diagnosing, and treating antisocial children and adolescents. Canadian
Journal of Psychiatry, 54, 803-812. Frick, P. J., Bodin, S. D., & Barry, C. T. (2000). Psychopathic traits and conduct problems in
community and clinic-referred samples of children: Further development of the Psychopathy Screening Device. Psychological Assessment, 12(4), 382-393. doi:10.1037/1040-3590.12.4.382
Frick, P.J., Cornell, A.H., Bodin, S.D., Dane, H.E., Barry, C.T., & Loney, B. R. (2003). Callous-
unemotional traits and developmental pathways to severe conduct problems. Developmental Psychology 39(2), 246-260. doi:10.1037/0012-1649.39.2.246
Frick, P. J., & Hare, R. D. (2001). The psychopathy screening device. Toronto: Multi-Health
Systems. Frick, P. J., O’Brien, Wootton, & McBurnett. (1994). Psychopathy and conduct problems in
children. Journal of Abnormal Psychology, 103(4), 700-707. doi:10.1037/0021-843X.103.4.700
Frick, P.J. & White, S.F. (2008). Research Review: The importance of callous-unemotional
traits for developmental models of aggressive and antisocial behavior. The Journal of
Child Psychology and Psychiatry, 49(4), 359-375. doi:10.1111/j.1469- 7610.2007.01862.x
Garson, G.D. (2012). Testing statistical assumptions. North Carolina: Statistical Associates
Publishing. Gentzler, A. L., Santucci, A. K., Kovacs, M., & Fox, N. A. (2009). Respiratory sinus arrhythmia
reactivity predicts emotion regulation and depressive symptoms in at-risk and control children. Biological Psychiatry 82(2), 156-163. doi:10.1016/j.biopsycho.2009.07.002
reactivity and respiratory sinus arrhythmia among maltreated and comparison youth: Relations with aggressive behavior. Journal of Pediatric Psychology, 35(5), 547-558. doi:10.1093/jpepsy/jsp113
Gramzow, R. H., Willard, G., & Mendes, W. B. (2008). Big tales and cool heads: Academic
exaggeration is related to cardiac vagal reactivity. Emotion, 8(1), 138-144. doi:10.1037/1528-3542.8.1.138
112
Hastings, P.D., Nuselovici, J.N., Utendale, W.T., Coutya, J. McShane, K.E., & Sullivan, C. (2008). Applying the polyvagal theory to children's emotion regulation: Social context, socialization, and adjustment. Biological Psychology, 79(3), 299-306. doi:10.1016/j.biopsycho.2008.07.005 Herpetz, S. & Sass, H. (2000). Emotional deficiency and psychopathy. Behavioral Sciences and
the Law, 18(5), 567-580. doi:10.1002/1099-0798(200010)18:5<567::AID- BSL410>3.0.CO;2-8
Hill, L.G., Lochman, J.E., Coie, J.D., Greenberg, M.T., & The Conduct Problems Prevention Research Group. (2004). Effectiveness of Early Screening for Externalizing Problems: Issues of Screening Accuracy and Utility. Journal of Consulting and Clinical
Hinson, J. M., Jameson, T. L., & Whitney, P. (2003). Impulsive decision-making and working memory. Journal of Experimental Psychology: Learning, Memory and Cognition 29(2), 298-306. doi:10.1037/0278-7393.29.2.298
Kelsey, R. M., Ornduff, S. R., Reiff, S., & Arthur, C. M. (2002). Psychophysiological correlates
of narcissistic traits in women during active coping. Psychophysiology, 39(3), 322-332. doi:10.1017/S004857720139306X
Keller, P. S. & El-Sheikh, M. (2009). Salivary alpha-amylase as a longitudinal predictor of
children’s externalizing symptoms: Respiratory sinus arrhythmia as a moderator of effects. Psychoneuroendocrinology, 34, 633-643. doi:10.1016/j.psyneuen.2008.12.016
Kempes, M., Matthys, W., Maassen, G., van Goozen, S., & van Engeland, H. (2006). A parent
questionnaire for distinguishing between reactive and proactive aggression in children. European Child & Adolescent Psychiatry, 15(1), 38-45. doi:10.1007/s00787-006-0502-2
Klopf, J., Kofler-Westergren, B., & Mitterauer, B. (2007). Towards action-oriented criteria in
risk assessment. International Journal of Forensic Mental Health., 6(1), 47-56. doi:10.1080/14999013.2007.10471248
Lee, Z., Vincent, G. M., Hart, S. D., & Corrado, R. R. (2003). The validity of the
Antisocial Process Screen Device as a self-report measure of psychopathy in adolescent offenders. Behavioral Sciences and the Law, 21(6), 771-786. doi:10.1002/bsl.561
Lochman, J.E. & The Conduct Problems Prevention Research Group. (1995). Screening of child
behavior problems for prevention programs at school entry. Journal of Consulting and
Clinical Psychology, 63(4), 549-559. doi:10.1037/0022-006X.63.4.549 Loeber, R., Burke, J.D., & Lahey, B.B. (2002). What are the adolescent antecedents to antisocial
personality disorder? Criminal Behaviour and Mental Health, 12(1), 24-36. doi:10.1002/cbm.484
113
Loeber, R., Dishion, T. J., & Patterson, G. R. (1984). Multiple gating: A multistage assessment procedure for identifying youths at risk for delinquency. Journal of Research in Crime
and Delinquency, 21(1), 7-32. doi:10.1177/0022427884021001002 Lorber, M. F. (2004). Psychophysiology of aggression, psychopathy, and conduct problems: A
Marsee, M.A., Silverthorn, P., & Frick, P.J. (2005). The association of psychopathic traits with
aggression and delinquency in non-referred boys and girls. Behavioral Sciences and the
Law, 23(6), 803-817. doi:10.1002/bsl.662
Marsh, P., Beauchaine, T. P., & Williams, B. (2008). Dissociation of sad facial expressions and autonomic nervous system responding in boys with disruptive behavior disorders. Psychophysiology, 45(1), 100-110. doi:10.1111/j.1469-8986.2007.00603.x
(2008). Reduced amygdala response to fearful expressions in children and adolescents with callous-unemotional traits and Disruptive behavior disorders. American Journal of
Psychiatry, 165, 712-720. doi: 10.1176/appi.ajp.2007.07071145 Mathias, C. W., & Stanford, M. S. (2003). Impulsiveness and arousal: Heart rate under
conditions of rest and challenge in healthy males. Personality and Individual Differences,
35(2), 355-371. doi:10.1016/S0191-8869(02)00195-2 Mezzacappa, E., Tremblay, R.E., Kindlon, D., Saul, J.P., Arseneault, L., Seguin, J., Phil, R.O., &
Earls, F. (1997). Anxiety, antisocial behavior, and heart rate regulation in adolescent males. Journal of Child Psychology and Psychiatry, 38(4), 457-469. doi:10.1111/j.1469-7610.1997.tb01531.x
Mitchell, D.G.V., Colledge, E., Leonard, A., & Blair, R.J.R. (2002). Risky decisions and
response reversal: is there evidence of orbitofrontal cortex dysfunction in psychopathic individuals? Neuropsychologia, 40(12), 2013-2022. doi:10.1016/S0028-3932(02)00056-8
Moffitt, T. E. (1993). “Life-course-persistent” and “adolescence-limited” antisocial behavior: A developmental taxonomy. Psychological Review, 100(4), 674– 701. doi:10.1037/0033-295X.100.4.674
Moffitt, T.E & Caspi, A. (2001). Childhood predictors differentiate life-course persistent and
adolescence-limited antisocial pathways among males and females. Developmental
Moffitt, T.E., Caspi, A., Harrington, H., & Milne, B. (2002). Males on the life-course-persistent
and adolescence-limited antisocial pathways: Follow-up at age 26. Development and Psychopathology, 14(1), 179-206. doi:10.1017/S0954579402001104
114
Munoz, L.C., Frick, P.J., Kimonis, E.R., & Aucoin, K.J. (2008). Types of aggression, responsiveness to provocation, and callous-unemotional traits in detained adolescents. Journal of Abnormal Child Psychology 36(1), 15–28. doi:10.1007/s10802-007-9137-0
O'Brien, B. S. & Frick, P. J. (1996). Reward dominance: Associations with anxiety, conduct problems, and psychopathy in children. Journal of Abnormal Child Psychology, 24(2), 223-240. doi:10.1007/BF01441486
Pardini, D. A. & Loeber, R. (2007). Interpersonal and affective features of psychopathy in
children and adolescents: Advancing a developmental perspective. Journal of Clinical
Child & Adolescent Psychology, 36(3), 269-275. doi: 10.1080/15374410701441575 Patrick, C.J. (2008). Psychophysiological correlates of aggression and violence: An integrative
review. Philosophical Transactions of the Royal Society Biological Sciences, 363(1503), 2543-2555. doi:10.1098/rstb.2008.0028
Developmental origins of disinhibition, boldness, and meanness. Development and
Psychopathology, 21, 913-938. doi: http://dx.doi.org/10.1017/S0954579409000492 Pine, D.S., Shaffer, D., Schonfeld, I.S., & Davies, M. (1997). Minor physical anomalies:
Modifiers of environmental risks for psychiatric impairment? Journal of the American
Academy of Child and Adolescent Psychiatry, 36(3), 395-403. doi:10.1097/00004583-199703000-00019
Porges, S.W. (1985). U.S. Patent No. 4,510,944. Washington, DC: U.S. Patent and Trademark
Office. Porges, S.W. & Bohrer, R.E. (1990). Analyses of periodic processes in psychophysiological research. In J.T. Cacioppo and L.G. Tassinary (Eds.), Principles of Psychophysiology:
Physical, Social, and Inferential Elements. 708-753.New York: Cambridge University Press.
Porges, S.W., Doussard-Roosevelt, & Maiti (1994). Vagal tone and the physiological regulation
of emotion. Monographs of the Society for Research in Child Development, 59, 167-186. doi: 10.1111/j.1540-5834.1994.tb01283.x
Poulin, F. & Boivin, M. (2000). Reactive and proactive aggression: Evidence of a two-factor
model. Psychological Assessment, 12(2), 115-122. doi:10.1037/1040-3590.12.2.115 Poythress, N.G., Dembo, R., Wareham, J., & Greenbaum, P.E. (2006). Construct Validity of the
Youth Psychopathic Traits Inventory (YPI) and the Antisocial Process Screening Device (APSD) With Justice-Involved Adolescents. Criminal Justice and Behavior, 33(1), 26- 55. doi:10.1177/0093854805282518
115
Raine, A. (2002). Annotation: The role of prefontal deficits, low autonomic arousal, and early health factors in the development of antisocial and aggressive behavior in children. Journal of Child Psychology and Psychiatry, 43(4), 417-434. doi:10.1111/1469- 7610.00034
Reynolds, C.R. & Kamphaus, R.W. (1992). Behavior Assessment System for Children Manual.
United States: American Guidance Service, Inc. Ronningstam, E. (2010). Narcissistic personality disorder: A current review. Current Psychiatry
Salekin, R.T., Neumann, C.S., Leistico, A.M.R., DiCicco, T.M., & Duros, R.L. (2004). Psychopathy and comorbidity in a young offender sample: Taking a closer look at psychopathy's potential importance over disruptive behavior disorders. Journal of
(2009). Neurobiology of empathy and callousness: Implications for the development of antisocial behavior. Behavioral Sciences & the Law, 27(2), 137-171. doi:10.1002/bsl.862
Silverthorn, P., Frick, P.J,. & Reynolds, R. (2001). Timing of onset and correlates of severe conduct problems in adjudicated girls and boys. Journal of Psychopathology and
Behavioral Assessment, 23(3), 171-181. doi:10.1023/A:1010917304587 Suzuki, A., Hirota, A., Takasawa, N., & Shigemasu, K. (2003). Application of the somatic
marker hypothesis to individual differences in decision-making. Biological Psychology,
65(1), 81-88. doi:10.1016/S0301-0511(03)00093-0 Sylvers, P., Brubaker, N., Alden, S. A., Brennan, P. A., & Lilienfeld, S. O. (2008). Differential
endophenotypic markers of narcissistic and antisocial personality features: A psychophysiological investigation. Journal of Research in Personality, 42(5), 1260-1270. doi:10.1016/j.jrp.2008.03.010
Thomaes, S., Bushman, B.J., De Castro, O., & Stegge, H. (2009). What makes narcissists
bloom? A framework for research on the etiology and development of narcissism. Development and Psychopathology, 21, 1233-1247. doi:10.1017/S0954579409990137
Thomaes, S., Stegge, H., Bush, B.J., Olthof, T., & Denissen, J. (2008). Development and
Validation of the Childhood Narcissism Scale. Journal of Personality Assessment, 90(4), 382–391. doi:10.1080/00223890802108162
Van Lier, P.A.C., Wanner, B., & Vitaro, F. (2007). Onset of antisocial behavior, affiliation with
deviant friends, and childhood maladjustment: A test of the childhood-and adolescent-onset models. Development and Psychopathology, 19(1), 167-185. doi:10.1017/S0954579407070095
116
Vasilev, C.A., Crowell, S.E., Beauchaine, T.P. Mead, H.K., & Gatzke-Kopp, L.M. (2009). Correspondence between physiological and self-report measures of emotion dysregulation: A longitudinal investigation of youth with and without psychopathology. The Journal of Child Psychology and Psychiatry, 50(11), 1357-1364. doi:10.1111/j.1469-7610.2009.02172.x
Vaughn, M.G., Edens, J.F., Howard, M.O., & Smith, S.T. (2009). An investigation of primary
and secondary psychopathy in a statewide sample of incarcerated youth. Youth Violence
and Juvenile Justice, 7(3), 172-188. doi: 10.1177/1541204009333792 Vaughn, M. G. & Howard, M.O. (2005). The construct of psychopathy and its potential
contribution to the study of serious, violent, and chronic youth offending, Youth Violence
and Juvenile Justice, 3(3), 235-252. doi:10.1177/1541204005276320
Vaughn, M.G., Howard, M.O., & DeLisi, M. (2008). Psychopathic personality traits and delinquent careers: An empirical examination. International Journal of Law and
offenders: Affective traits and antisocial behavior patterns. Behavioral Sciences and the
Law, 21(6), 695-712. doi:10.1002/bsl.556 Vitacco, M.J., Rogers, R., & Neumann, C.S. (2003). The Antisocial Process Screening Device:
An examination of its construct and criterion-related validity. Assessment, 10(2), 143-150. doi:10.1177/1073191103010002005
Volavka, J. (1999). The neurobiology of violence: An update. The Journal of Neuropsychiatry
and Clinical Neurosciences, 11(3), 307-314. Washburn, J.J., McMahon, S.D., King, C.A., Reinecke, M.A., & Silver, C. (2004). Narcissistic
Features in Young Adolescents: Relations to Aggression and Internalizing Symptoms. Journal of Youth and Adolescence, 33(3), 247–260. doi:10.1023/B:JOYO.0000025323.94929.d9
Webster-Stratton, C., Reid, M.J., & Hammond, M. (2004). Treating children with early-onset
conduct problems: Intervention outcomes for parent, child, and teacher training. Journal
of Clinical Child and Adolescent Psychology, 33, 105-124. doi:10.1207/S15374424JCCP3301_11
White, J. L., Moffitt, T. E., Caspi, A., Bartusch, D. J., Needles, D. J., & Stouthamer-Loeber, M.
(1994). Measuring impulsivity and examining its relationship to delinquency. Journal of
Wilson, A. C., Lengua, L. J., Tininenko, J., Taylor, A., & Trancik, A. (2009). Physiological profiles during delay of gratification: Associations with emotionality, self-regulation, and adjustment problems. Journal of Applied Developmental Psychology, 30(6), 780-790. doi:10.1016/j.appdev.2009.05.002