Page 1
Author's Accepted Manuscript
The Renal Sinus- Transitional Cell Carcinoma and itsMimickers on CT
Gabriela Gayer MD, Rivka Zissin MD
PII: S0887-2171(14)00021-3DOI: http://dx.doi.org/10.1053/j.sult.2014.02.004Reference: YSULT578
To appear in:Semin Ultrasound CT MRI
Cite this article as: Gabriela Gayer MD, Rivka Zissin MD, The Renal Sinus- TransitionalCell Carcinoma and its Mimickers on CT,Semin Ultrasound CT MRI , http://dx.doi.org/10.1053/j.sult.2014.02.004
This is a PDF file of an unedited manuscript that has been accepted for publication. As aservice to our customers we are providing this early version of the manuscript. Themanuscript will undergo copyediting, typesetting, and review of the resulting galley proofbefore it is published in its final citable form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers that applyto the journal pertain.
www.elsevier.com/locate/enganabound
Page 2
1
The Renal Sinus- Transitional Cell Carcinoma and its Mimickers
on CT
* Gabriela Gayer MD (1,2,3)
Rivka Zissin MD (3,4)
(1) Department of Diagnostic Imaging and Nuclear Medicine,
Sheba Medical Center, Ramat-Gan, Israel
(2) Department of Radiology, Stanford Medical Center, Stanford,
California
(3) Sackler Faculty of Medicine, Tel-Aviv University, Israel
(4) Department of Diagnostic Imaging, Meir Medical Center, Kfar
Saba, Israel
*Corresponding author:
Gabriela Gayer
Email: [email protected]
Page 3
2
Abstract
The renal sinus is a deep recess located at the medial aspect of the kidney
surrounded by the renal parenchyma. It contains within it the collecting
system of the kidney, lymphatics, nerves, and renal blood vessels. The
remainder of the sinus is filled with adipose and fibrous tissue. A variety of
pathological conditions arise from the different tissues in this site. The aim of
this review is to explore and illustrate the common and less common
processes affecting the renal pelvis.
Introduction
A variety of both benign and malignant lesions may affect the renal sinus, the
most common ones being renal sinus cysts and renal sinus lipomatosis.
These, however, rarely pose a diagnostic challenge on CT because of the
typical density of fluid and fat, respectively. Many other conditions that affect
the renal sinus are of soft tissue density and have far less specific imaging
features. While transitional cell carcinoma (TCC) is a relatively common
neoplasm of the renal sinus, many other processes that affect this site have
overlapping imaging findings. Some of these lesions have been mistaken for
TCC, based mainly on their imaging findings, and have lead to unnecessary
nephrectomy.1 The purpose of this review is to highlight the spectrum of
imaging features of a wide array of lesions affecting the renal sinus and to
increase awareness of lesions simulating TCC in this location on CT.
Neoplastic lesions
Malignant tumors
Page 4
3
The most frequent malignant tumors that involve the renal sinus are
transitional cell carcinoma, renal cell carcinoma, lymphoma and metastatic
disease. Superficially, these masses resemble one another on cross-sectional
imaging, but are quite different histologically and clinically. Awareness of
subtle imaging findings may be helpful in the preoperative differentiation of
these masses, which is particularly important since the treatment of each is
substantially different. Transitional cell carcinoma is treated by means of
nephroureterectomy, while infiltrative renal cell carcinoma by nephrectomy,
and lymphoma is treated by systemic chemotherapy. In addition, patients with
upper tract TCC require more intensive surveillance because they have a
lifelong increased risk of developing urothelial tumors in the contralateral
upper urinary tract or bladder.2
• Transitional cell carcinoma
Transitional cell carcinoma (TCC) is the most common tumor of the renal
pelvis (<10% of renal malignancies). TCC arises from the urothelium, the
lining surface epithelium of the renal collecting tubules, calyces, pelvis, ureter,
bladder, and urethra. Hematuria, either gross or microscopic, is the most
common symptom reported in up to 95% of patients.3
On CT, TCC of the renal pelvis may appear as a pelvic filling defect or as
circumferential urothelial wall thickening, distorting the collecting system (Figs.
1,2). The tumor sometimes has a mass-like appearance, similar to that of
renal cell carcinoma (RCC).2 A recent study proved that CT scan is accurate
in distinguishing between intrarenal TCC and centrally located RCC by using
the following six CT features: intrarenal TCC is centered on the collecting
system, appears as a focal filling defect in the pelvicalyceal system,
Page 5
4
preservation of reniform contour is present, cystic or necrotic change is
absent, homogeneous but modest tumor enhancement, and presence of
extension of the tumor towards the ureteropelvic junction.4
It is crucial to differentiate it from other conditions that present as a filling
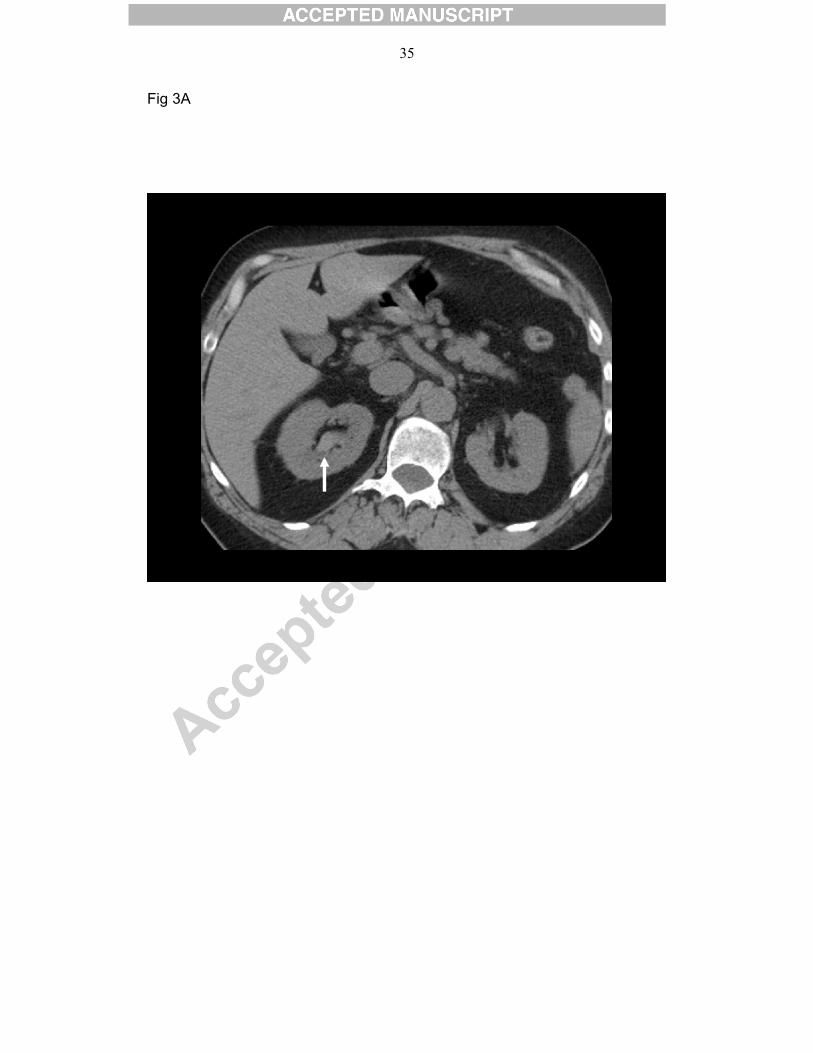
defect - a urinary calculus, blood clot, or sloughed papillae (Fig. 3). The
presence of contrast enhancement of the filling defect is helpful in correctly
diagnosing TCC.5 Biopsy of infiltrative transitional cell carcinoma should be
avoided if possible because of the propensity for seeding.6
• Renal cell carcinoma
RCC is the most common primary renal malignant neoplasm in adults,
accounting for approximately 90% of renal tumors and 2% of all adult
malignancies. In recent years tumors are being discovered at an earlier stage,
likely due to increased use of imaging. RCC is characterized by increased
neovascularization, relatively frequent vascular invasion and early
metastasis.7 RCC is multicentric only in 4%, and bilateral in 0.5–3%.2 Most
renal cell carcinomas grow by expansion and commonly extend into the renal
sinus, leading to focal hydronephrosis or caliceal displacement.1
On un-enhanced CT scans, RCC may appear as isoattenuating,
hypoattenuating, or hyperattenuating relative to the remainder of the kidney.
Calcifications may be present and are usually amorphous and internal. On
contrast-enhanced CT scans, RCC is usually solid, and decreased
attenuation suggestive of necrosis is often present (Fig. 4). RCC is
occasionally a predominantly cystic mass, with thick septa and wall nodularity.
RCC may also appear as a completely solid and highly enhancing mass.
Page 6
5
Renal vein invasion is a feature much more suggestive of centrally located
RCC (Fig. 5), although rarely TCC can invade the renal vein or even the
inferior vena cava. Treatment is surgical and varies according to the size and
stage of the tumor. 4
• Lymphoma
Involvement of the renal sinus by malignant lymphoma usually occurs within
the context of disseminated disease. Renal involvement by lymphoma has
various radiological manifestations: a single renal mass, multiple bilateral
renal masses, a perirenal mass, diffuse infiltration of a kidney and a renal
sinus mass. When the renal sinus is involved by lymphoma, an important clue
to the correct diagnosis is associated retroperitoneal lymphadenopathy.5
Primary lymphomas of the renal sinus are very rare because lymphoid tissue
at this site is scarce. 8 The most common histology of primary renal
lymphoma is diffuse large-cell lymphoma.9 Primary renal lymphoma is
characterized by lymphomatous renal infiltration, unilateral or bilateral
kidney enlargement without ureteral obstruction, and no additional
extrarenal imaging findings. Most patients present with flank pain, and
hematuria, symptoms and signs that are indistinguishable from more
common RCC and TCC.8
Lymphoma affecting the renal sinus usually appears as a homogeneous
mass without hydronephrosis (Fig. 6), quite similar to that of TCC.5,8
Treatment consists of chemotherapy combined with involved-field
Page 7
6
radiation therapy. 8 If the diagnosis of lymphoma is not considered
preoperatively, then the patient might undergo unnecessary
nephroureterectomy for suspected TCC.
• Metastases
Renal metastases are present in approximately 10% to 20% of cancer
patients depending on tumor type and most commonly seen in the setting of
other metastatic diseases. A renal metastasis is the most common malignant
neoplasm of the kidney found at autopsy.10 The most common primary sites
for renal metastases (except hematologic malignancies) are lung, colon and
breast carcinoma, melanoma and reproductive system malignancies.10,11
Spread of metastasis to the kidney is usually hematogenous or lymphatic.
They are usually asymptomatic and discovered incidentally on imaging
studies performed for other purposes. 10 The most common CT appearance of
renal metastases is bilateral, multifocal, small (< 3 cm), hypodense masses.
The nephrographic phase is ideal to detect and characterize renal masses
(Fig. 7). 11,12 The maximal and homogeneous parenchymal enhancement in
this phase facilitates detection of renal metastases, which typically do not
enhance to the same degree as the renal parenchyma. Renal metastases
usually do not change the treatment approach due to the advanced stage of
the disease.10
Benign lesions
• Renal sinus cysts
Page 8
7
Renal sinus cysts are common, with a reported prevalence between of up to
1.5% at autopsy.13
Cysts in the renal pelvis are referred to as parapelvic and peripelvic cysts.
Parapelvic cysts originate in the renal parenchyma and extend into the renal
sinus. Peripelvic cysts originate in sinus structures which presumably
represent mostly lymphatic collections.14 Peripelvic cysts are usually small,
multiple, confluent cysts. They are rarely symptomatic. At US and un-
enhanced CT, these cysts may mimic hydronephrosis. At contrast-enhanced
CT performed during the excretory phase, differentiation of peripelvic cysts
and hydronephrosis is obvious because the enhanced collecting system is
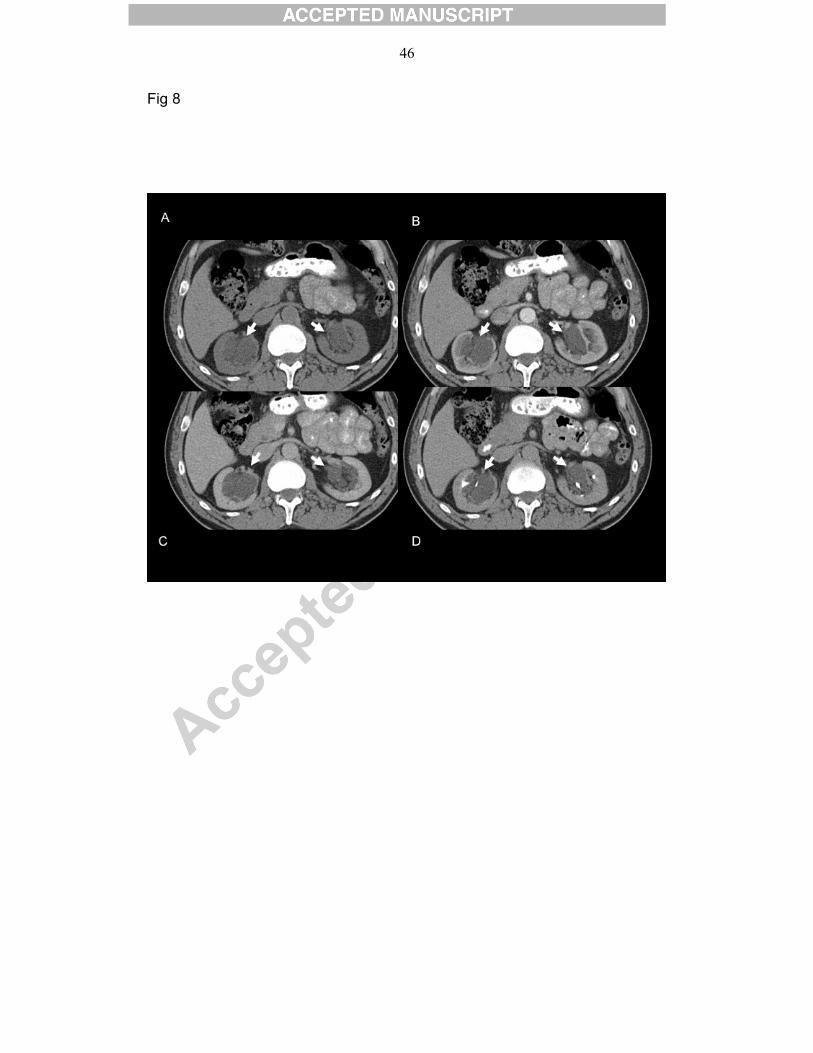
displaced by the water-attenuation sinus cysts (Figs. 7,8). A parapelvic cyst is
usually a single, larger cyst occurring in the sinus and likely originates from
the adjacent parenchyma. Parapelvic cysts exhibit the same imaging features
as simple renal cortical cysts. Neither type of renal sinus cyst is of clinical
importance and does not warrant follow-up or treatment.1, 14
• Renal sinus Lipomatosis
Renal sinus lipomatosis is a benign proliferation of fat that occurs with
advanced age, obesity, and exposure to steroids. Simple renal sinus
lipomatosis is often bilateral. It is asymptomatic because the process does not
cause caliceal obstruction.15 Another form of this process is an advanced or
aggressive form termed replacement renal sinus lipomatosis that usually
occurs unilaterally. The main etiologies of this form include a calculus
disease, chronic hydronephrosis, or infection. Calculus disease is seen in
Page 9
8
70% of cases. Replacement renal sinus lipomatosis results in enlargement of
the kidney with marked proliferation of fat in the sinus and atrophy of the renal
cortex with preservation of the reniform shape of the kidney.16 CT and MR
reveal the fatty nature of sinus lipomatosis (Fig. 9). The main differential
diagnosis is xanthogranulomatous pyelonephritis. 1
• Angiomyolipoma
Angiomyolipoma is the most common mesenchymal renal neoplasm, with a
prevalence of 0.13% in a healthy adult population without tuberous sclerosis
complex.17,18 Angiomyolipoma is a benign tumor that, as the name implies,
typically contains variable proportions of blood vessels, smooth muscle, and
adipose tissue. The presence of macroscopic adipose tissue usually allows
accurate diagnosis with CT or MRI. However, when such neoplasm contains
minimal or no fat, differentiation from renal cell carcinoma on imaging
becomes difficult. Epithelioid angiomyolipoma (EAML) is a rare subtype of
angiomyolipoma, which consists predominately of sheets of epithelioid cells
with granular eosinophilic cytoplasm. It is considered a potentially malignant
neoplasm. On CT EAML usually shows no or very little fat and no calcification.
Tumor enhancement is variable and may be mild, moderate or marked (Fig.
10). EAML can therefore easily be misdiagnosed as renal cell carcinoma
during histologic and imaging examinations. 18
Vascular lesions
Page 10
9
• Renal artery aneurysm
Renal artery aneurysm (RAA) is rare with an incidence of up to 0.9%. RAA
has no gender predilection. The peak incidence occurs in the fifth and sixth
decade. It involves the right artery more frequently than the left and is bilateral
in 10% of cases. More than 90% of true RAAs are extrarenal, typically located
in the renal hilum. RAA is often asymptomatic but may present acutely with
flank/ back pain and hematuria due to spontaneous rupture. 19,20
On CT RAA presents as a well-defined rounded mass in the renal hilum. A
peripheral ring-like calcification is often present (Fig. 11A). On contrast-
enhanced CT the aneurysm undergoes variable enhancement occurs,
depending on technical parameters of the scan (volume of contrast material,
injection rate and phase of acquisition). On arterial phase the aneurysm
shows enhancement similar to that of the abdominal aorta, indicating its
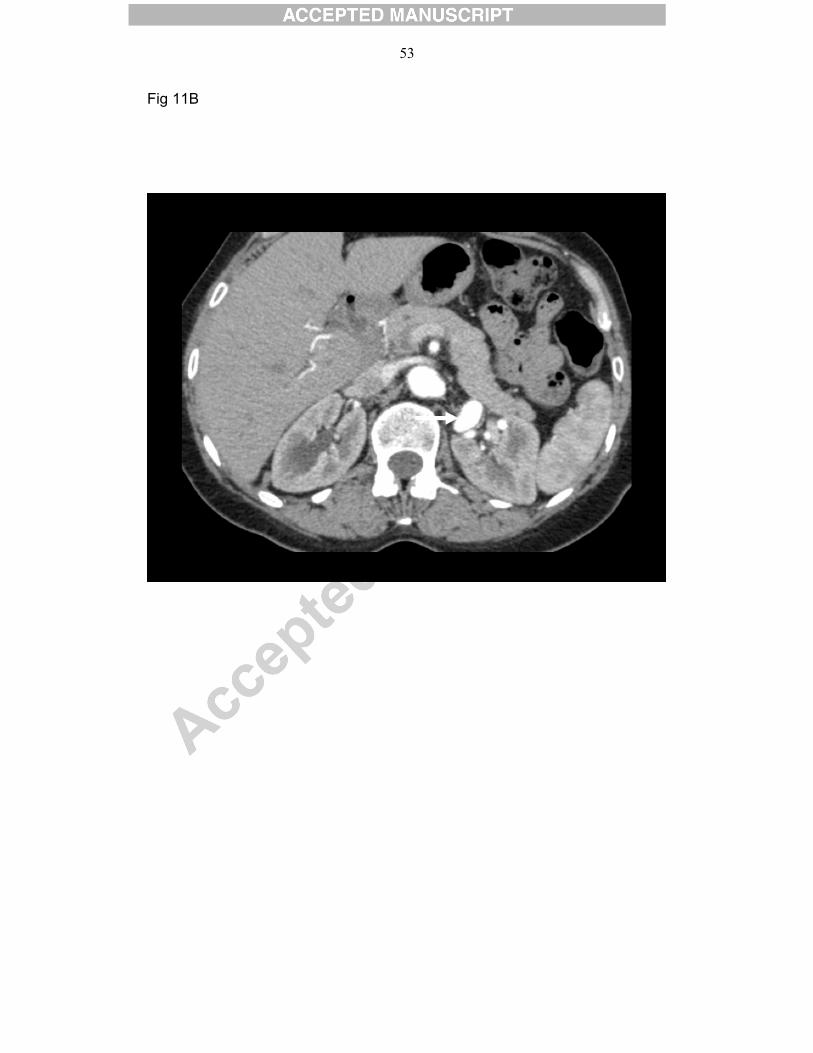
arterial origin (Fig. 11B). 20
Treatment of renal aneurysms is controversial and includes surgery,
endovascular treatment (embolization or stenting) or observation. 21
• Renal arteriovenous malformation
Renal arteriovenous malformations (AVMs) are very rare benign lesions. They
may be congenital or acquired. Most AVMs are acquired, resulting from trauma,
inflammation or percutaneous procedures such as renal biopsy. They are more
common in women and usually affect young people. In some cases they
present with massive hematuria.
AVM may be mistaken for a renal pelvis tumor if the vascular channels do not
opacify densely at the time of scanning. The accurate diagnosis can however
Page 11
10
be made on contrast-enhanced CT performed at the arterial phase. Treatment
consists of transcatheter selective arterial embolization, which leads to
resolution of the hematuria whilst preserving renal parenchyma. 22
Infiltrative lesions:
• Extramedullary hematopoiesis
Extramedullary hematopoiesis (EMH) is the development and growth of
hematopoietic tissue outside of the bone marrow. It is an essential process in
fetal life, but its occurrence after birth is usually considered abnormal and
represents a compensatory mechanism for failure of erythropoiesis. EMH
occurs most frequently in the liver and spleen but has been reported to
involve a myriad of other tissues and organs, mainly intraspinal or paraspinal
in the thoracic region. At one autopsy series lymph nodes were the most
common site of EMH (excluding the liver and spleen) followed by the kidneys.
Most patients with renal EMH are asymptomatic, but may present with
abdominal pain or renal failure due to parenchymal involvement or ureteral
compression. 23
Renal EMH usually affects both kidneys but may be unilateral. It may involve
the renal pelvis, perinephric space or both. Imaging findings on CT and MRI
correspond to the involved compartment. EMH affecting the renal pelvis
appears as soft-tissue infiltration with encasement of the pelvicalyceal
systems, that sometimes involves the proximal ureters (Fig. 12).24 At MRI,
signal intensity on T2-weighted images is typically low owing to the
hemosiderin content. At ultrasound, the perinephric lesions usually appear as
Page 12
11
solid hypoechoic masses. Additional CT findings of hepatosplenomegaly and
paraspinal soft tissue can support the diagnosis of extramedullary
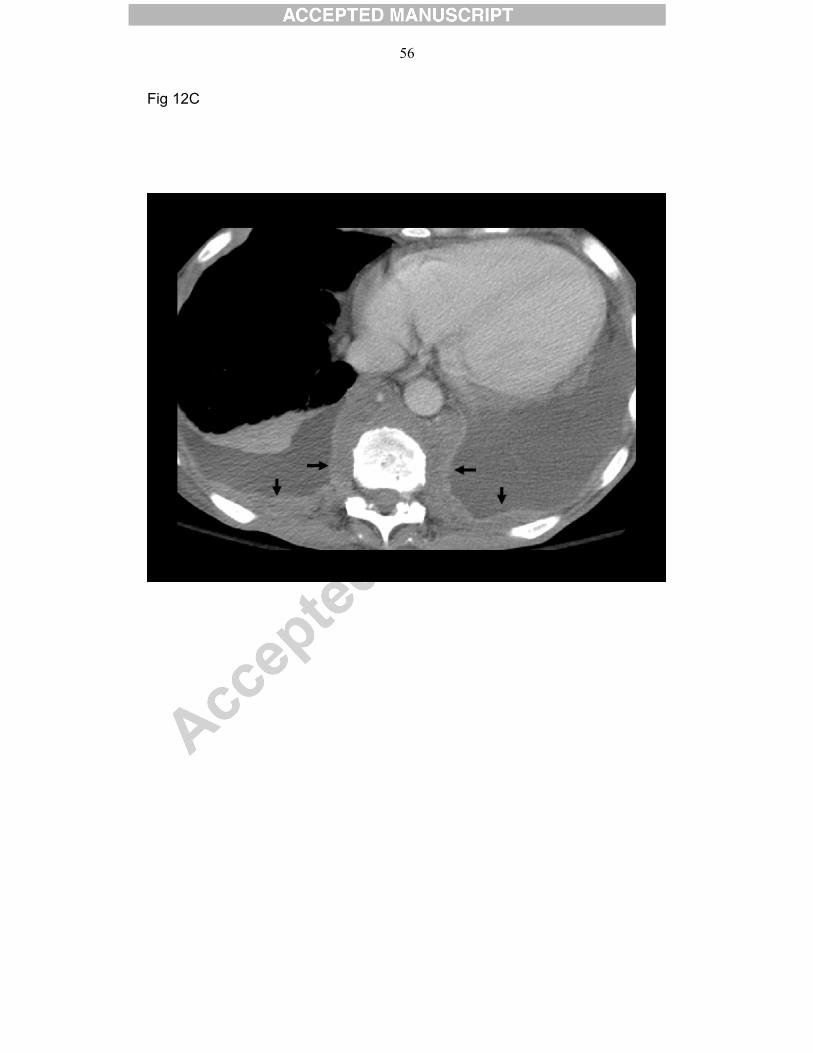
hematopoiesis (Fig. 12C). Treatment for symptomatic cases consists of low-
dose radiation therapy.23
• IgG4-related disease
Immunoglobulin (Ig) G4-related disease is a recently designated benign
clinical entity characterized histopathologically by an extensive IgG4-positive
plasma cells and lymphocyte infiltration. IgG4-related disease has been
described in virtually every organ system including the biliary tree, pancreas.
salivary glands, periorbital tissues, kidneys, lungs, lymph nodes, meninges,
aorta. breast, prostate, thyroid, pericardium, and the skin. 25,26
Renal involvement is quite common and predominantly involves the cortex of
the kidney and less frequently the renal pelvis. The renal lesions manifest as
multiple wedge-shaped or nodular cortical lesions in one or both kidneys.
When the disease affects the renal sinus it will appear as diffuse wall
thickening of the renal pelvis (Fig. 13). 27 Histologic specimen shows
tubulointerstitial nephritis with marked expansion of the interstitium with
fibrosis and an inflammatory cell infiltrate. 26
Most patients with renal IgG4-related disease have involvement of another
organ. The coexistence of similar infiltrative processes affecting other organs
(e.g. pancreas, bile ducts) can support the diagnosis of IgG4-related disease
and serves as an important clue for the differentiation of IgG4-related disease
from RCC or TCC. 28
Glucocorticoids are typically the first line of therapy. Aggressive treatment is
needed when vital organs are involved because IgG4-related disease can
Page 13
12
lead to serious organ dysfunction and failure. However, not all manifestations
of the disease require immediate treatment and watchful waiting has also
been advocated. 25
• Erdheim-Chester Disease
Erdheim-Chester disease is a rare non–Langerhans cell histiocytosis of
unknown etiology that usually affects middle-aged adults with no sex
predilection. 29,30 Patients typically present with lower-extremity bone pain.
Skeletal imaging findings include bilateral symmetric metadiaphyseal cortical
thickening, and medullary sclerosis in the long bones of the appendicular
skeleton, with sparing of the epiphyses and axial skeleton. 31 Extraskeletal
manifestations include central nervous system, lungs, skin, kidneys,
retroperitoneum and heart. 32
Renal involvement is found in about 30% of patients and may be an isolated
site of disease. 33 This involvement is usually asymptomatic but may progress
and lead to renal failure. CT shows hypoattenuated homogeneous tissue
infiltration with weak contrast enhancement. The perirenal infiltration is often
bilateral and symmetric is highly suggestive of the diagnosis. 33,34 The
infiltration may also extend to the renal sinuses and to the proximal and cause
upper urinary tract obstruction (Fig. 14A). On MRI, the soft-tissue infiltration of
the pararenal and perirenal fat appears isointense to muscle on T1- and T2-
weighted spin-echo sequences, with a slight and homogeneous enhancement
in signal intensity after gadolinium injection (Fig. 14B).33
The prognosis for Erdheim-Chester disease is considered poor and depends
on the extent of extraskeletal, mainly pulmonary and cardiac, involvement.
Page 14
13
Treatment usually consists of a combination of steroids, radiotherapy, and
chemotherapy.34
• Suburothelial hemorrhage
Hemorrhage into the suburothelial layer of the collecting system is rare and
occurs mainly secondary to anticoagulant therapy. Because of its rarity
suburothelial hemorrhage is often not clinically suspected, even in a patient
receiving anticoagulant therapy. It presents acutely with flank pain and
hematuria and patients undergo CT for evaluation, mainly to evaluate for renal
calculi or a neoplastic process such as transitional cell carcinoma. 35
Suburothelial hemorrhage appears on CT as mural thickening of the renal
pelvis and sometimes involves also the proximal ureter, sometimes narrowing
their lumen. The hemorrhage is best appreciated on un-enhanced scan, when
the typical high density of the hemorrhage is most conspicuous (Fig. 15 A,B).
35,36 This high density is not as conspicuous on either nephrographic or
pyelographic phases. On the pyelographic phase the mural thickening is the
main abnormality (Fig. 15 C,D). The CT findings mimic those of a neoplasm of
the collecting system. This similarity has resulted in multiple reports of
erroneous nephrectomy.37 It is therefore important to scrutinize the images
obtained prior to intravenous contrast administration and if needed manipulate
the images digitally to search for the linear hyperdensity outlining the
collecting system. In the absence of an un-enhanced scan, a follow-up 2-3
weeks later will usually demonstrate complete resolution of the hemorrhage. 35
Page 15
14
Pitfalls
Excretion of contrast material from an imaging study performed several hours
prior to the current CT may result in errors in interpretation.
Gadolinium, similar to iodinated contrast material, is excreted by the kidneys.
The density of concentrated excreted gadolinium is higher than that of urine,
but lower than that of iodine (Fig. 16). In a patient undergoing an un-enhanced
CT of the abdomen within hours after a gadolinium-enhanced MR study, the
high density of excreted gadolinium may be mistaken for hemorrhage. Such
an error can result in unnecessary additional investigations and anxiety. This
misinterpretation is less likely to occur in a patient scanned after an earlier
contrast-enhanced CT study, because of the typical high density of excreted
iodine. However if the collecting system is dilated the excreted iodine will be
less dense, mixing with low density urine, and may be misinterpreted as a soft
tissue mass (Fig. 17). In both settings, correlation with recent imaging history
is important and helps confirm the diagnosis.
Summary
A wide spectrum of neoplastic and nonneoplastic conditions may involve the
renal sinus. Diagnostic differentiation of these entities can be radiologically
challenging, but distinction is important because management strategies
differ. Several of these lesions have characteristic imaging findings that allow
for a correct diagnosis, while others have overlapping radiologic features, and
a biopsy and histopathologic evaluation are required to establish a definitive
diagnosis.
Page 16
15
Knowledge of clinical information and familiarity with the spectrum of imaging
features of conditions affecting the renal sinus can facilitate accurate
diagnosis and timely treatment.
Legends
Fig. 1
TCC affecting the renal pelves bilaterally.
63-year-old man with history of bladder cancer, status post cystectomy and
ileal neobladder reconstruction, undergoing routine CT follow-up.
A, B. Axial contrast-enhanced CT shows urothelial thickening affecting the
renal pelves bilaterally (arrows). This finding was assumed to represent an
infectious/inflammatory process and follow-up was recommended.
C,D,E. Follow-up contrast-enhanced CT 6 months later shows interval
progression of urothelial thickening.
C. Nephrographic phase at the level of the left renal sinus shows worsening of
circumferential urothelial thickening (long arrows). Note interval progression of
retroperitoneal lymphadenopathy (short arrows).
D. Nephrographic phase at the level of the right renal sinus shows worsening
of circumferential urothelial thickening (white arrow). The left ureteral wall is
now also infiltrated (black arrow, compare to B).
E. Pyelographic phase at the level of the left renal sinus shows an irregular,
narrowed, amputated collecting system resulting from the infiltrative lesion
(arrow).
Fig. 2
Page 17
16
74-year-old man with left-sided centrally located poorly differentiated
transitional cell carcinoma.
A,B. Contrast-enhanced axial images show a heterogeneously enhancing
mass (arrows) in the renal pelvis infiltrating the left upper pole region with
preservation of renal shape. Perinephric fat stranding is present (arrowheads).
C. Coronal image at the pyelographic phase shows amputated collecting
system resulting from the infiltrative lesion (arrow).
Fig. 3.
Blood clot mimicking TCC. 40-year-old man presenting with hematuria for 3
days prior to admission and right flank pain day of admission. He has been on
Coumadin treatment for atrial fibrillation. INR was 3.6, above therapeutic level.
A. Un-enhanced CT scan shows a high-density focus in the upper calyx of the
right kidney (arrow).
B. Contrast-enhanced axial CT at the nephrographic phase at the same level.
The high density focus is much less conspicuous on this phase scan (arrow).
C. Contrast-enhanced axial CT at the pyelographic phase clearly shows the
filling defect in the upper calyx of the right kidney (arrow).
D. Follow up CT 6 weeks later. Contrast-enhanced axial CT at the
pyelographic phase at the same level shows complete resolution of the filling
defect.
Fig. 4
Clear cell RCC affecting the left renal sinus.
43-year-old man presented with hematuria.
Page 18
17
Axial (A) and coronal (B) CT contrast-enhanced CT images at the
corticomedullary phase show a rounded well-defined hetergenously
enhancing mass at the renal pelvis (arrow).
Fig. 5
35-year-old woman with left-sided RCC infiltrating the renal sinus with left
renal vein invasion.
Axial contrast-enhanced CT a shows a large hypodense mass in the left
kidney (black arrow), marked dilatation of the left renal vein (white arrow) with
a large heterogenous filling defect, compatible with invasion of the tumor into
the renal vein, a feature suggestive of RCC.
Fig. 6.
Lymphoma involving the renal pelvis.75-year-old woman presented with left
flank pain and elevated Creatinine level. Ultrasonography showed left-sided
hydronephrosis.
A. Un-enhanced CT shows a round soft tissue mass (white arrow) at the renal
hilum, measuring 25 HU.
B. Contrast-enhanced CT shows mild enhancement of the soft tissue mass
(white arrow) to 57HU. Associated enlarged retroperitoneal and mesenteric
lymph nodes are present, suggestive of metastatic disease.
A percutaneous nephrostomy tube (black arrow) had been inserted and
alleviated the hydronephrosis seen at US.
Fig. 7
Metastatic melanoma of the right renal hilum in a 78-year-old woman with
known melanoma.
Page 19
18
Contrast-enhanced axial CT images at the nephrographic (A) and
pyelographic (B) phases show a well-defined round mass at the right renal
sinus enhancing to a lesser degree than the renal parenchyma (black arrow).
Note additional round masses (arrowheads) in the perirenal fat, suggestive of
metastatic disease. Small nonenhancing fluid-density lesions are seen in the
left renal sinus (white arrow), with an appearance typical of peripelvic cysts.
Fig. 8
Bilateral peripelvic cysts in a 64 -year-old asymptomatic woman. Axial
images on un-enhanced (A), corticomedullary (B), nephrographic (C) and
pyelographic (D) contrast-enhanced phases show multiple small confluent
low-attenuation cystic lesions (arrows) in the renal sinus bilaterally. The
enhanced calices on the pyelographic phase are stretched and attenuated but
not obstructed by the cysts. The latter phase is helpful in differentiating
peripelvic cysts from hydronephrosis.
Fig. 9
Renal pelvic sinus lipomatosis. Abundant fatty tissue occupying the renal
pelvis bilaterally (arrows) in a 88-year-old man with COPD, undergoing CT to
evaluate anemia.
Fig. 10
Epithelioid angiomyolipoma of the renal sinus. 33-year-old male presenting
with intermittent right-sided spine pain. Ultrasound showed a 3 x 4 cm mass in
the interpolar region of the right kidney.
A. Un-enhanced axial CT scan shows a soft tissue mass infiltrating the right
renal pelvis (arrow). Its density is minimally higher than that of the renal
parenchyma and it does not appear to contain any fat.
Page 20
19
B,C. Axial (B) and coronal (C) contrast-enhanced images at nephrographic
phase show mild homogeneous enhancement of the mass (arrow).
D. The mass (arrow) shows no signal loss on fat-saturated gadolinium-
enhanced T1-weighted MR image, because it contains only microscopic fat.
The patient underwent nephrectomy and histologic sections showed an
angiomyolipoma of the renal sinus with epithelioid differentiation and atypia.
Fig. 11
Renal artery aneurysm. 56-year-old woman presenting with microhematuria.
A. Un-enhanced axial CT scan shows a round soft-tissue mass, that is
isodense to the renal parenchyma, with a peripheral linear calcification
(arrow).
B. Contrast-enhanced image at the corticomedullary phase shows marked
enhancement of the lesion (arrow), similar to the enhancement of the adjacent
aorta, indicating the diagnosis of a renal artery aneurysm.
Fig. 12
Extramedullary hematopoiesis. 64-year-old man with myelofibrosis.
A. Contrast-enhanced axial CT image obtained during portal venous phase
shows hypodense, hypovascular mass (long arrow) infiltrating the left renal
sinus. Note also rind-like soft tissue in the perirenal space (short arrows).
B. On pyelographic phase the collecting system is encased but the infiltrative
process (arrow) does not obstruct the calyces.
C. Axial contrast-enhanced CT at the level of the chest shows bilateral
paraspinal and pleural (arrows) soft tissue masses, findings highly suggestive
of EMH.
Page 21
20
Fig. 13
IgG4-related tubulointerstitial nephritis affecting the left kidney in a 63-year-old
man.
A. Un-enhanced axial CT shows an abnormally enlarged left kidney without a
distinct renal pelvis (arrow).
B. Pyelographic phase shows a persistent corticomedullary enhancement of
the left kidney, without excretion of contrast material. The entire left renal
collecting system and medulla appear uniformly infiltrated (arrow).
C. A repeat scan after an additional 30 minutes delay shows excretion of
contrast material from the left kidney. The infiltrative process markedly distorts
the collecting system.
The left perinephric fat is diffusely infiltrated (arrowheads, A-C). The right
kidney is unremarkable.
D. T2-weighted MR image shows the infiltrative process encasing the calyces
(arrow).
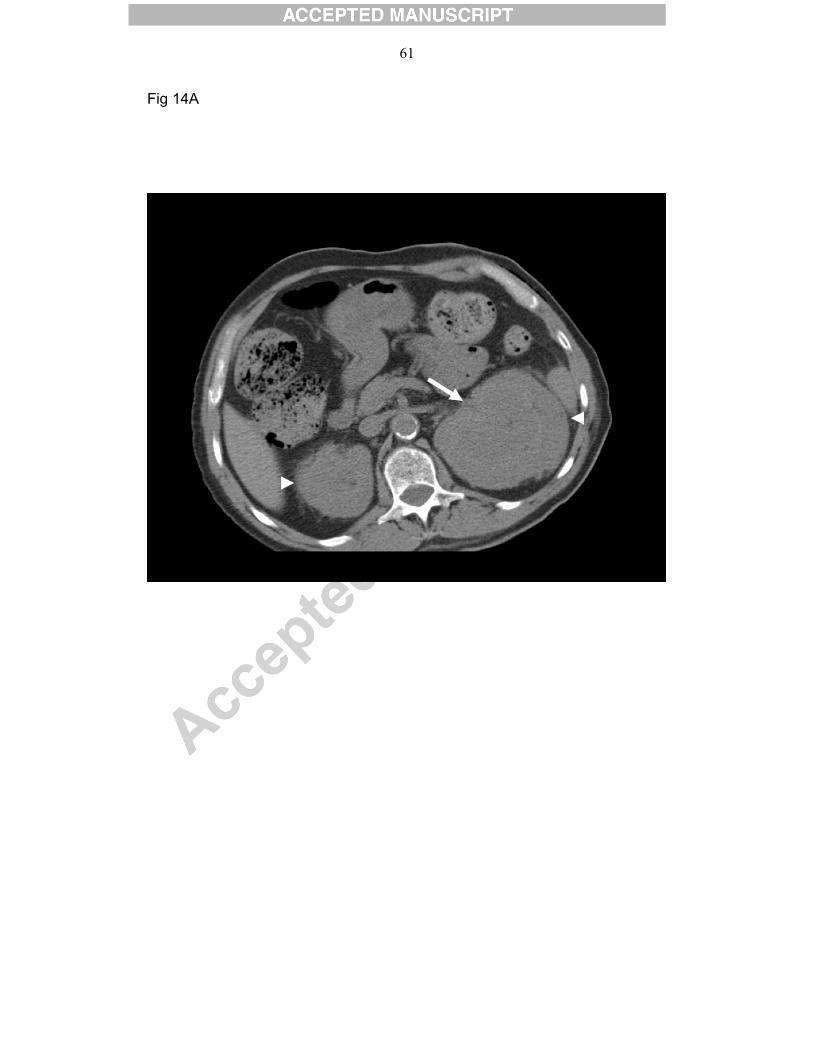
Fig. 14
Erdheim-Chester disease infiltrating the renal sinus.
A 69-year-old man presented with lower extremity bone pain, diabetes
insipidus, chronic renal disease, hyperlipidemia and hypertension.
A. Un-enhanced axial CT shows infiltrative process in the left renal sinus
(arrow) and bilateral homogeneous perirenal soft tissue infiltration
(arrowheads) with attenuation similar to that of muscle.
B. Coronal MR image shows bilateral soft-tissue infiltration of the perirenal
space (black arrows) encasing both kidneys. The infiltrative process involves
also the left renal sinus (white arrow).
Page 22
21
Biopsy of the peri-renal tissue confirmed Erdheim-Chester disease.
Radiograph of the lower extremities (not shown) showed enlarged femora with
metadiaphyseal sclerosis.
Fig. 15
Suburothelial hemorrhage secondary to anticoagulant therapy.
A 60-year-old man presented to the emergency department with left sided
flank pain, right lower quadrant pain and hematuria. The patient had been on
Coumadin treatment due to prior deep venous thrombosis and pulmonary
embolism. An un-enhanced CT of the abdomen and pelvis was initially
obtained to rule out stones.
Un-enhanced CT (A,B) shows high density outlining the left renal pelvis and to
a lesser degree also the right renal pelvis (arrows).
Contrast-enhanced CT at pyelographic phase (C,D) shows marked thickening
of both renal (arrows), extending to the ureters (arrowheads B,D). The
nephrographic phase is prolonged on the left.
Laboratory results showed elevated INR. Patient was treated conservatively
with fresh frozen plasma and Vitamin K with prompt return of INR to
therapeutic levels and resolution of abdominal pain and hematuria.
Fig. 16
Excreted gadolinium from a single left kidney. Un-enhanced CT was
performed several hours after a gadolinium-enhances MR study. The density
of excreted gadolinium (arrow) is higher than that of urine and mimics that of
fresh blood and may therefore be misinterpreted as hemorrhage.
Fig. 17
Page 23
22
Excreted iodinated contrast material in a dilated extra-renal pelvis. Current un-
enhanced CT was performed several hours after a contrast-enhanced CT.
A,B. Un-enhanced axial (A) and coronal (B) CT show homogeneous high
density within the right renal pelvis (arrows). Without a prior CT it is
impossible to establish whether this is a soft tissue lesion or an extra-renal
pelvis containing high-density fluid. Note similarity to figure 10 (epithelioid
angiomyolipoma of the renal sinus).
C. Un-enhanced axial image from a prior study shows a similar dilated extra-
renal pelvis but containing clear fluid density (arrow).
Page 24
23
RFERENCES
1. Rha SE, Byun JY, Jung SE, et al. The renal sinus: pathologic spectrum and
multimodality imaging approach. Radiographics. 2004;24 Suppl 1:S117-31.
2. Bata P, Tarnoki DL, Tarnoki AD, et al. Transitional cell and clear cell renal
carcinoma: differentiation of distinct histological types with multiphase CT.
Acta Radiol. 2013 Nov 15
3. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2009. CA Cancer J Clin
2009;59:225–249.
4. Raza SA, Sohaib SA, Sahdev A, et al. Centrally infiltrating renal masses on
CT: differentiating intrarenal transitional cell carcinoma from centrally located
renal cell carcinoma. Am J Roentgenol 2012;198:846–853.
5. Zhang J, Israel GM, Krinsky GA, et al. Masses and pseudomasses of the
kidney: imaging spectrum on MR. J Comput Assist Tomogr. 2004;28(5):588-
95.
6. Israel GM, Silverman SG. The incidental renal mass. Radiol Clin North Am.
2011;49(2):369-83.
7. Ljungberg B, Hanbury DC, Kuczyk MA, et al. European Association of
Urology Guideline Group for renal cell carcinoma. Renal cell carcinoma
guideline. Eur Urol 2007;51:1502–1510.
8. Bozas G, Tassidou A, Moulopoulos LA, et al. Non-Hodgkin's lymphoma of
the renal pelvis. Clin Lymphoma Myeloma. 2006;6(5):404-6.
9. Dimopoulos MA, Moulopoulos LA, Costantinides C, et al. Primary renal
lymphoma: a clinical and radiological study. J Urol 1996; 155:1865-1867.
Page 25
24
10. Aras M, Dede F, Ones T, et al. Is The Value of FDG PET/CT In Evaluating
Renal Metastasis Underestimated? A Case Report And Review of The
Literature. Mol Imaging Radionucl Ther. 2013;22(3):109-12.
11.Shimko MS, Jacobs SC, Phelan MW. Renal metastasis of malignant
melanoma with unknown primary. Urology. 2007;69(2):384.e9-10.
12. Israel GM, Bosniak MA. Pitfalls in renal mass evaluation and how to avoid
them. Radiographics. 2008;28:1325–1238.
13. Amis ES Jr. Cysts of the renal sinus. In: Pollack HM, McClennan BL, eds.
Clinical urography. 2nd ed. Philadelphia, Pa: Saunders, 2000; 1404– 1412
14. Nahm AM, Ritz E. The renal sinus cyst-the great imitator. Nephrol Dial
Transplant. 2000;15(6):913-4
15. Dogra VS, Bhatt S. Replacement renal sinus lipomatosis of the
kidney.Ultrasound Q. 2009 Jun;25(2):71-3. 16. Kocaoglu M, Bozlar U, Sanal
HT, Guvenc I. Replacement lipomatosis: CT and MRI findings of a rare renal
mass. Br J Radiol. 2007;80(959):e287-9.
17. Fujii Y, Komai Y, Saito K, et al. Incidence of benign pathologic lesions at
partial nephrectomy for presumed RCC renal masses: Japanese dual-center
experience with 176 consecutive patients. Urology 2008; 72:598–602
18. Froemming AT, Boland J, Cheville J, et al. Renal epithelioid
angiomyolipoma: imaging characteristics in nine cases with radiologic-
pathologic correlation and review of the literature. AJR Am J Roentgenol.
2013;200(2):W178-86
19. Bulbul MA, Farrow GA. Renal artery aneurysms. Urology. 1992;40(2):124-
6.
Page 26
25
20. Gayer G, Zissin R, Rimon U et al. Vascular lesions of the renal sinus.
Emerg Radiol. 2003;10(3):135-41.
21 Klausner JQ, Harlander-Locke MP, Plotnik AN, et al. Current treatment of
renal artery aneurysms may be too aggressive. J Vasc Surg. 2014 Jan 22.
22. Sountoulides P, Zachos I, Paschalidis K, et al. Massive hematuria due to
a congenital renal arteriovenous malformation mimicking a renal pelvis tumor:
a case report. J Med Case Rep. 2008 May 5;2:144. doi: 10.1186/1752-1947-
2-144.;
23. Koch CA, Li CY, Mesa RA, et al. Nonhepatosplenic extramedullary
hematopoiesis: associated diseases, pathology, clinical course, and
treatment. Mayo Clin Proc. 2003;78(10):1223-33.
24. Galperin-Aizenberg M, Volchek Y, Even Sapir E, et al. Case report: Renal
extramedullary haematopoiesis mimicking renal lymphoma on computed
tomography. Clin Radiol. 2006;61(10):896-8.
25. Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med.
2012;366(6):539-51
26. Takahashi N, Kawashima A, Fletcher JG, et al. Renal involvement in
patients with autoimmune pancreatitis: CT and MR imaging findings.
Radiology. 2007;242(3):791-801
27. Triantopoulou C, Malachias G, Maniatis P, et al. Renal lesions associated
with autoimmune pancreatitis: CT findings. Acta Radiol. 2010;51(6):702-7.
28. Kawano M, Saeki T, Nakashima H, et al. Proposal for diagnostic criteria
for IgG4-related kidney disease. Clin Exp Nephrol. 2011;15(5):615-26
Page 27
26
29. Yun EJ, Yeh BM, Yabes AP, et al. Erdheim-Chester disease: case report
and review of associated urological, radiological and histological features. J
Urol 2003;169:1470–1471.
30. Sheu SY, Wenzel RR, Kersting C, et al. Erdheim-Chester disease: case
report with multisystemic manifestations including testes, thyroid, and lymph
nodes, and a review of literature. J Clin Pathol 2004;57:1225–1228.
31. Bancroft LW, Berquist TH. Erdheim-Chester disease: radiographic
findings in five patients. Skeletal Radiol 1998;27:127–132.
32. Fortman BJ, Beall DP. Erdheim-Chester disease of the retroperitoneum: a
rare cause of ureteral obstruction. AJR Am J Roentgenol 2001;176:1330–
1331.
33. Dion E, Graef C, Haroche J, et al. Imaging of thoracoabdominal
involvement in Erdheim-Chester disease. AJR Am J Roentgenol 2004;183:
1253e60.
34. Chew HC, Lee CH, Cheah FK, et al. Cardiac tumor and renal involvement
in a nonsmoker with centrilobular pulmonary nodules. Chest.
2009;135(4):1102-6.
35. Gayer G, Desser TS, Hertz M, et al. Spontaneous suburothelial
hemorrhage in coagulopathic patients: CT diagnosis. AJR Am J Roentgenol.
2011;197(5):W887-90
36. Phinney A, Hanson J, Talner LB. Diagnosis of renal pelvis subepithelial
hemorrhage using un-enhanced helical CT. AJR 2000; 174:1023–1024
37. Eccher A, Brunelli M, Gobbo S, et al. Subepithelial pelvic hematoma
(Antopol—Goldman lesion) simulating renal neoplasm: report of a case and
review of the literature. Int J Surg Pathol. 2009;17(3):264-7.