THE REPAIR OF THE UNILATERAL CLEFT LIP By DAVID DAVIES, F.R.C.S. Head of the Unit of Plastic Surgery, University of Cape Town, Groote Schuur Hospital IN recent years a large number of ingenious and original repairs for this deformity have been published and the literature has been extensively reviewed. We do not propose to take up the readers' time with a further review of the literature with which they are already familiar. It is with some diffidence, therefore, that I present yet another modification to the fast-growing list. This method follows earlier procedures but, we hope, represents the logical conclusion of those earlier methods. In r955, as a rather puzzled trainee thrust into the complexities of the Le Mesurier repair and all its modifications, I wondered if it would not be possible to devise a simple but satisfactory method of repair which could be applied, unchanged, to all degrees of cleft lip. While analysing the procedures available it appeared that either the procedure is simple and the results variable or the results show a more uniform constancy and the procedure is inordinately complicated. The ideal repair should be easy, predictable, sacrifice the least amount of tissue and the operative result should remain unchanged through the years that follow. When examining these children certain facts are obvious. The markings of the cupid's bow are present ; the defect of the cleft lip is really a linear one with shortening which should be lengthened with a Z-plasty ; and the Creator has been kind enough to give us a normal uncleft side as a standard. We should, therefore, establish the landmarks available to us, measure the height of the normal side and perform a simple calculated Z-plasty on the cleft side, discarding any tissue not covered by the Z-plasty markings. In this way we will find that the same technique can be applied to complete and partial clefts. Little or no tissue is discarded in the complete cleft where the linear shortening on the cleft side is so marked that the Z-plasty markings occupy the entire height of the lip ; whereas in the incomplete cleft it is necessary to discard a small triangle on each side of the cleft in order to maintain the true proportions of the Z-plasty. The plastic surgeon is already familiar with the principles of the Z-plasty (Fig. I). It is simple and allows exact calculation of the final length of the diagonals after imbrication of the triangular flaps. The advantages of a Z-plasty repair are numerous. Straight scars are avoided and thus post-operative contracture does not distort the repaired lip. The flaps in this technique are larger and more easily handled than the smaller flaps in the square-flap and small-triangle techniques. The method satisfies the requirement that the dimple and cupid's bow, present though distorted in the cleft lip, should be rotated downwards into place and maintained there by another flap which gives bulk to the lower half of the lip. This flap from the lateral side of the cleft produces fullness of the lip border, while the upper flap by the direction of its pull tends to maintain a vertical columella and helps in the formation of a sill to the nostril floor (Fig. 2). 254
Transcript
THE REPAIR OF THE UNILATERAL CLEFT LIP
By DAVID DAVIES, F.R.C.S.
Head of the Unit of Plastic Surgery, University of Cape Town, Groote Schuur Hospital
IN recent years a large number of ingenious and original repairs for this deformity have been published and the literature has been extensively reviewed. We do not propose to take up the readers' time with a further review of the literature with which they are already familiar.
It is with some diffidence, therefore, that I present yet another modification to the fast-growing list. This method follows earlier procedures but, we hope, represents the logical conclusion of those earlier methods.
In r955, as a rather puzzled trainee thrust into the complexities of the Le Mesurier repair and all its modifications, I wondered if it would not be possible to devise a simple but satisfactory method of repair which could be applied, unchanged, to all degrees of cleft lip.
While analysing the procedures available it appeared that either the procedure is simple and the results variable or the results show a more uniform constancy and the procedure is inordinately complicated. The ideal repair should be easy, predictable, sacrifice the least amount of tissue and the operative result should remain unchanged through the years that follow.
When examining these children certain facts are obvious. The markings of the cupid's bow are present ; the defect of the cleft lip is really a linear one with shortening which should be lengthened with a Z-plasty ; and the Creator has been kind enough to give us a normal uncleft side as a standard. We should, therefore, establish the landmarks available to us, measure the height of the normal side and perform a simple calculated Z-plasty on the cleft side, discarding any tissue not covered by the Z-plasty markings. In this way we will find that the same technique can be applied to complete and partial clefts. Little or no tissue is discarded in the complete cleft where the linear shortening on the cleft side is so marked that the Z-plasty markings occupy the entire height of the lip ; whereas in the incomplete cleft it is necessary to discard a small triangle on each side of the cleft in order to maintain the true proportions of the Z-plasty.
The plastic surgeon is already familiar with the principles of the Z-plasty (Fig. I). It is simple and allows exact calculation of the final length of the diagonals after imbrication of the triangular flaps. The advantages of a Z-plasty repair are numerous. Straight scars are avoided and thus post-operative contracture does not distort the repaired lip. The flaps in this technique are larger and more easily handled than the smaller flaps in the square-flap and small-triangle techniques. The method satisfies the requirement that the dimple and cupid's bow, present though distorted in the cleft lip, should be rotated downwards into place and maintained there by another flap which gives bulk to the lower half of the lip. This flap from the lateral side of the cleft produces fullness of the lip border, while the upper flap by the direction of its pull tends to maintain a vertical columella and helps in the formation of a sill to the nostril floor (Fig. 2).
254
REPAIR OF THE UNILATERAL CLEFT LIP 255
There should be inherent in any design a possible margin for adjustment. Although we have never found it necessary, the lip could be lengthened by just deepening the V's, and shortened by converting the apices of the V's into Y'so The operation works equally well with all gradations of cleft lip from complete to partial without altering the angles or measurements.
Let us, at this point, summarise our aims in the repair of unilateral cleft lips. We must try to produce well-shaped symmetrical nostrils with the ala: at the
same level, coronally and sagittally, and a normal curve towards the columella. The nostril floor must be closed with, if possible, a sill linking the end of the alar
A
t C.(~
B FIG. I
((9 <9)
FIG. 2 Fig. I . - -The degree of lengthening expected when the equilateral triangles of
a Z-plasty have been transposed.
fold and the base of the columella. The columella itself should be vertical and straight in the midline. The lips should be of the correct height and fullness for the child concerned. This is important as we have found that the normal height of children's lips varies considerably and it would appear wrong to use any method that arbitrarily predetermines the height of the lip.
The philtrum with its central dimple should be preserved, the cupid's bow restored and the repaired lip should have its normal gentle curve of the vermilion border, edged by the vermilion ridge.
Scars should be inconspicuous and so designed that there will be no subsequent contracture--therefore any straight scar should be avoided.
Every plastic surgeon should be an artist but artistry varies from surgeon to surgeon. We have tried, therefore, to devise a technique that, unchanged, will give consistently good results in any degree of cleft lip making an inartistic result impossible. Flap measurements are given solely to ensure the correct height of the lip and the formation of the cupid's bow, but the method leaves ample scope for individual artistry where it is needed most, that is, in the repair of the nostril floor and the positioning of the ala: nasi. The method should allow easy, almost automatic making of flaps and simple operating--not needing more than thirty-five to forty minutes.
This method of repair has been used by us in Cape Town since 1955, and to date over 250 cleft lips have been repaired using this procedure.
256 B R I T I S H J O U RN A L OF P L A S T I C SURGERY
Before discussing the detailed technique of the operation we assume naturally that the child has been well examined beforehand for associated defects such as congenital heart disease, he should have a normal hmmoglobin level and should be 3 to 4 months of age. We prefer to wait until these children are 4 months old as many of the difficulties in any cleft lip operation arise from the presence of wide alveolar clefts. Although we feel that this operation gives a satisfactory result in the repair of the cleft lip, we naturally try to reduce any bony deformity pre- operatively. As a routine, all our patients with a cleft lip associated with a cleft of the alveolar margin are seen by an orthodontic consultant, and if he feels that the arch of the alveolus can be corrected pre-operatively we are only too happy to allow him to treat these cases initially. The method used is that described by McNeil (1956) and Burston (1959). We are convinced that the orthodontist should precede the surgeon if possible.
TECHNIQUE
Our object is to achieve a well-balanced lip, therefore the height of the lip along the philtrum on each side should be equal. To achieve this it is merely necessary to measure the height of the normal side, calculate the size of the triangles needed, interdigitate these, and the repair is completed. We can regard the cleft as the short diagonal of a rhomboid whose diagonals must be switched.
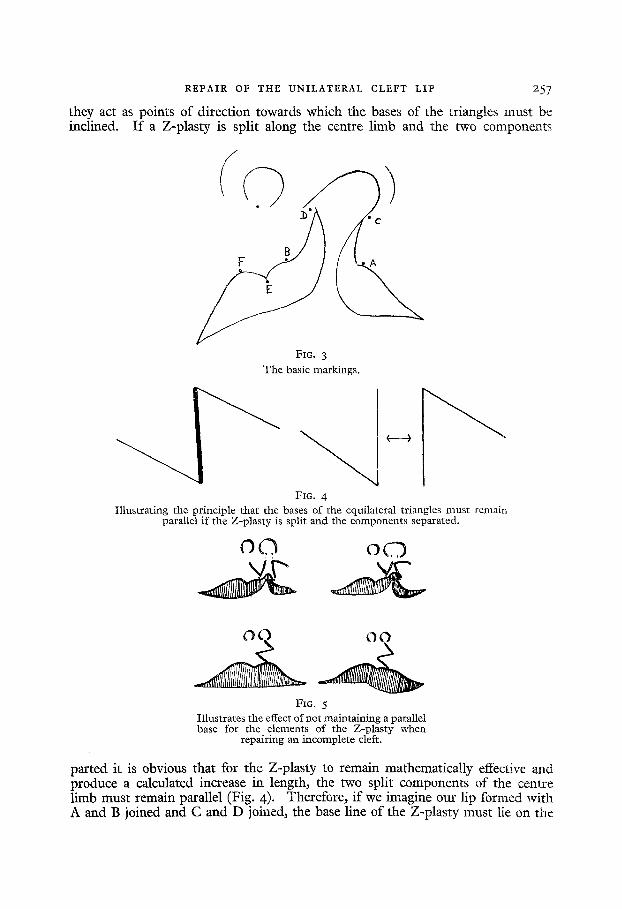
The basic points are shown in Figure 3. As the vermilion border is all important in the final cosmetic result we begin
our markings at this border leaving the nasal floor and nostril to be modified as necessary in the final stages of the operation.
Point A is that point on the lateral side of the cleft at which the mucocutaneous ridge disappears. This will be the peak of the cupid's bow on the lateral side ; it is usually easy to find and more dearly marked than Point B.
Do not hesitate to move this point more laterally if necessary ; whereas Point B must be the same distance from Point E as Point F is from E, there is no disadvantage in moving Point A a millimetre or so laterally along the mucocutaneous ridge. Most trouble arises from an attempt to preserve too much tissue on the lateral element. It is a mistake to attempt to use the attenuated mucosa where the lip narrows into the deft.
Point B is the point at which the mucocutaneous ridge disappears on the medial side of the cleft and should be the apex of the cupid's bow on the medial side of the newly formed lip. A guide to this point, which is not always well marked, is Point F where the normal side of the philtrum joins the vermilion border, and Point E, which is the inverted peak at the centre of the lip. The distance BE should equal EF.
These two points, A and B, are key points in this operation and are the only unchangeable points, acting as they do as the pivots of the Z-plasty limbs. I t is more logical to start one's repair from these easily determined points on the lip, which must be accurately approximated, than from the more variable Points C and D. It is difficult to fix Point C with a grossly flattened and distorted ala, and as this point is often placed too high or too low, it may spoil the remainder of any repair if it is used as a starting point. Points C and D are on the lateral side and medial side of the cleft respectively and when joined should reduce the nostril to its normal diameter. The only importance of these two points is that
REPAIR OF THE U N I L A T E R A L CLEFT LIP 2 5 7
they act as points of direction towards which the bases of the triangles must be inclined. I f a Z-plasty is split along the centre limb and the two components
FIG, 3 The basic markings.
FIG. 4 Illustrating the principle that the bases of the equilateral triangles must remain
parallel if the Z-plasty is split and the components separated.
o O o n
FIG. 5 Illustrates the effect of not maintaining a parallel base for the elements of the Z-plasty when
repairing an incomplete cleft.
parted it is obvious that for the Z-plasty to remain mathematically effective and produce a calculated increase in length, the two split components of the centre limb must remain parallel (Fig. 4). Therefore, if we imagine our lip formed with A and B joined and C and D joined, the base line of the Z-plasty must lie on the
258 BRITISH JOURNAL OF PLASTIC SURGERY
line joining AB and CD. Failure to appreciate this explains early difficulties with the Z-plasty technique in partial cleft lip repairs. The temptation is to run the base line of each triangle along the partial cleft instead of towards C and D, thus making the lip too long when the triangles are interdigitated (Fig. 5).
To be sure of obtaining the correct height any tissue between the upper end of the triangle markings and Points C and D should be sacrificed, and this must be removed in full thickness including skin, muscle and mucosa. In complete clefts it is not usually necessary to sacrifice this tissue, as the triangular markings usually extend the full length of the cleft up to Points C and D. The only tissue sacrificed, therefore, is the attenuated mucosal margin of the cleft which is normally removed in a simple Veau repair. As the severity of the cleft decreases and becomes more incomplete the tissue sacrificed is larger in extent (Figs. 6 and 7).
To simplify the calculations we have had a series of stainless steel triangles made which are marked off in millimetre divisions (Fig. 8). We have also a small stainless steel plate on which is engraved the correct ratio of heights of lips on normal size to the appropriate triangle, e.g., when the height of lips on normal side equals I "75 cm. the triangular markings should have sides I cm. in length. If the lip is I cm. high, the base of the triangle should be o.58 cm. and so forth (see Table).
When the normal height of the lip has been measured (Fig. 9) and the correct triangle selected and the markings of the points and Z-plasty made with Bonney's blue on the lip, a fine dental needle is dipped in Bonney's blue and small punctures are made next to Points A, B, C, and D, to act as a guide in the operation when the other markings have been washed away.
The lip and the nasal mucosa of the anterior palatal defect is now infiltrated on each side with a few millimetres of I : 3oo,ooo solution of adrenaline in saline and the surgeon should wait for seven minutes for this to take effect. One millimetre per pound body weight can safely be used and usually no more than 5 ml. is necessary.
With the operator seated at the head of the table a protected bulldog clamp is gently applied to the lip on each side of the cleft to complete the ha:mostasis. Finger pressure alone can be used but the operator or the assistant should be careful not to rotate the lip between his fingers as the through-and-through incision with a very fine yon Graefe knife may remove too much or too little mucosa. The lip is now held vertically away from the alveolus and the lines of the triangles are followed with a fine yon Graefe knife. At each stage bleeding points are caught with haemostats but not tied. One must make sure at this stage that the flaps are completely free, not only through the skin but also through muscle and mucosa.
Where the cleft is incomplete and it is necessary to sacrifice a small triangle of the lip on each side, this should be removed in full thickness with a yon Graefe knife at the time of dissection of the triangles.
The-incision is carried farther on each side past Points C and D. On the medial side along the junction of nasal and oral mucosa, and on the lateral side along the mucocutaneous junction and the edge of the pyriform fossa. In the case of a complete cleft the mucosa in the lateral sulcus is freed for 3 cm. and if necessary this is repeated in the sulcus on the medial side as well. The lip and ala are freed from the bony edge of the pyriform fossa to allow them to come forward and the skin of the nose is gently freed from its underlying alar cartilage with a flat dissecting scissors. The lip and columella are freed from the nasal spine and the lower end of the septum. Where the cleft is very large it is possible to get still
REPAIR OF THE UNILATERAL CLEFT LIP
ff)(
FIG. 6 FIG. 7
)) 259
A
FIG. 8
A~ Stainless steel triangles used for ease in marking. B, Set of four triangles ranging from I to o'58 cm.
FIG. 9
z6o B R I T I S H JOURNAL OF PLASTIC SURGERY
further advancement of the mucosa by making a small right-angled back cut at the extremities of the sulcal incisions.
With the dissection of the lip completed and the flaps retracted a magnificent view is obtained of the palatal defect in cases of complete clefts of the primary and secondary palates, so it would seem logical to repair this defect in the anterior palate at the same time as the defect of the lip is repaired. The palatal mucosa is not touched, the incision running along the edge of the palate on the cleft side and along the junction of vomerine and palatal mucosa on the uncleft side. The nasal mucosa on each side is freed and dosed, starting posteriorly, with everting sutures of 4/0 chromic catgut. This is continued anteriorly to the sill of the nose and the soft tissues are completely freed from the edge of the pyriform fossa allowing the ala to assume a normal or near normal curve.
TABLE
Conversion Table used for Rapid Calculation of Triangle needed for the Repair. This is engraved on a Small Stainless Steel Sheet for
use at Operation Height of L ip on
Normal Side
I "O CtTI,
l ' I CIIl.
I "2 am.
I" 3 cm. I '4 cm. I '5 cm. I '6 crn. I . 7 cm.
Size of Triangle Necessary
o-58 cm. o'63 cm. o'69 cm. o'75 cm. o-8z cm.
0-87 cm. o - 9 2 c m .
o.98 cm.
The nasal floor is now complete and the repair continues with the advancement of the mucosa and dosing of the sulcal incisions with 4/o chromic catgut. I f this advancement is done it will be found that a fairly large triangle of mucosa is left on the lateral side of the deft, which can be advanced into the gap caused by the freeing of the ala nasi from the edge of the pyriform fossa. At this stage, with the nasal floor dosed and a flap of mucosa available from the lateral element, a bone graft may be used to complete the alveolar arch. We prefer to postpone this to a later stage when the repaired structures have healed unless we are quite sure that the primary cover is adequate. A 3/0 muco-muscular suture is then passed through the lip at the level of the upper triangle and this is tied drawing the upper medial triangle into its position.
There are two words of caution we would like to offer at this stage. The first is not to bring the catgut suture through the muscle too close to the skin edge as this interferes with suturing of the skin and tends to tuck in the apices of the triangles ; in fact, it may be necessary in any case to free the skin on the tips of the triangles from the underlying muscle especially on the lateral triangle where the skin dips sharply towards the cleft. The second is to take an arbitrary measurement, say one and a half centimetres from the vermilion border on each side as the site of entrance and exit of the needle for the lower muco-muscular stitch. This avoids a common fault of pulling down the excess mucosa on the lateral side of the cleft which leaves one with a bulky mucosa on that side in the finished lip. It is
REPAIR OF THE UNILATERAL CLEFT LIP 26I
difficult to compensate for this mistake once it has been made. Continue the closure of the mucosa with fine catgut, then join A and B with 6/0 black silk and suture the point of each flap in place using a subcuticular stitch for the tip. Finish suturing
A
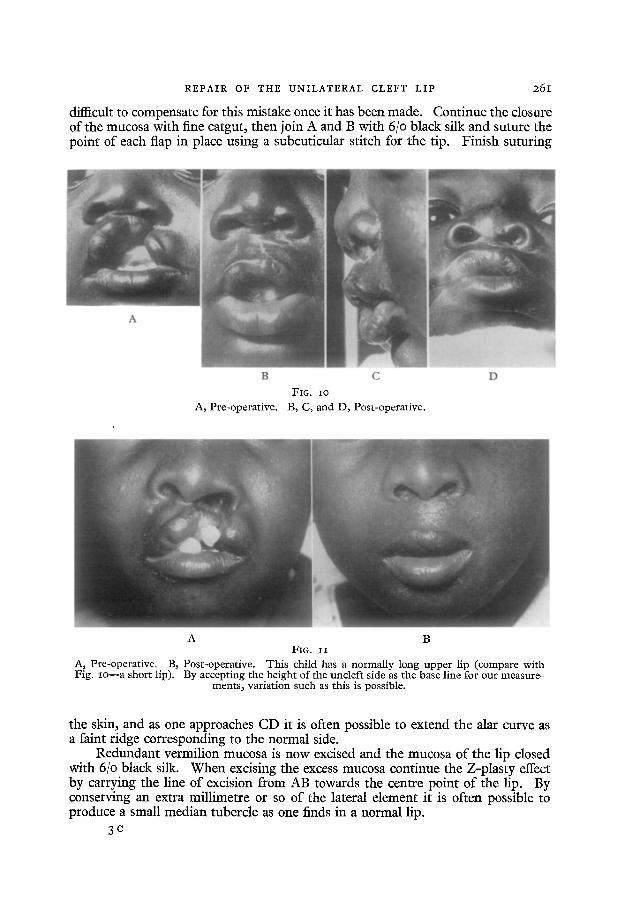
B C FIG. Io
A, Pre-operative. B, C, and D, Post-operative.
D
A B FIG. I I
A, Pre-operative. B, Post-operative. This child has a normally long upper lip (compare with Fig. xo--a short lip). By accepting the height of the uncleft side as the base line for our measure~
ments, variation such as this is possible.
the skin, and as one approaches CD it is often possible to extend the alar curve as a faint ridge corresponding to the normal side.
Redundant vermilion mucosa is now excised and the mucosa of the lip closed with 6/0 black silk. When excising the excess mucosa continue the Z-plasty effect by carrying the line of excision from AB towards the centre point of the lip. By conserving an extra millimetre or so of the lateral element it is often possible to produce a small median tubercle as one finds in a normal lip.
3 c
262 BRITISH JOURNAL OF PLASTIC SURGERY
A
A, Pre-operative.
B C
FIG. I2 B~ One year post-operatively. C, Four years post-operatively.
As Pre-operative. FIG. I3
Be One year post-operatively. C, Three years post-operatively. D, Four years post-operatively. E, Five years post-operatively.
REPAIR OF THE UNILATERAL CLEFT LIP 265
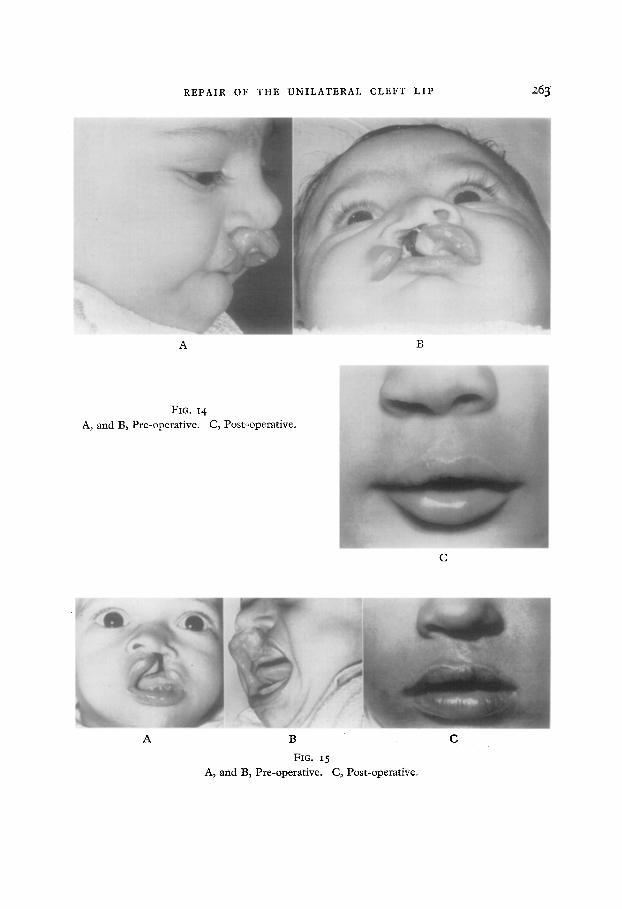
A B
FIe. 14 A, and B, Pre-operative. C, Post-operative.
C
A B
Fro. 15 A, and B, Pre-operative. C, Post-operative.
C
264 BRITISH JOURNAL OF eLASTIC SURGERY
Finally, where the cleft is wide, select a portex tube that fits snugly into the normal nostril and insert it into the repaired nostril. Pass a 2/o Dermalon suture from the alar curve at the edge of the alar fold through the septum to the sound nostril and tie over a small piece of tension tubing. This is just for support of the repaired nostril floor and the nostril must not be distorted through tying this too tightly. Make sure that part of the stitch passes through the tubing to prevent this being inhaled later by the child.
Post-operatively, splints are fixed to the child's arms and the child is spoon- fed. A dressing of Neomycin ointment, dry tulle gras and gauze is fixed with scotch tape to the lip after the operation and this is removed twenty-four hours later. Neomycin ointment is then applied three times a day to the lip in order to prevent any crusting of the serous ooze that may occur. The lip stitches should be removed on the sixth post-operative day and the nasal support on the eighth post-operative day.
The preceding photographs show the results in a series of cases using this method (Figs. io to 15).
A criticism levelled at this method of repair states that although the method leaves one with a satisfactory result at the time of operation, and it is known that immediate post-operative scarring will not distort the lip, over the years there will be an eccentric development of the musculature of the lip and the shape and form of the lip will alter.
We feel that the main bulk of the muscle fibres of the lateral element tend to turn upwards at the cleft margin and are brought down with the lateral triangle to their correct direction in the oral sphincter. Figures 12 and 13 show the progress of a child from the pre-operative cleft to the post-operative state six years later.
SUMMARY
A method is described for marking and utilising two equal flaps of a pure Z-plasty to give a predetermined height of lip on the cleft side.
A series of photographs is appended to illustrate the results in various degrees of cleft.
I would like to thank Dr J. Mostert, Medical Superintendent of the Red Cross War Memorial Children's Hospital, for permission to publish the appended photographs ; Dr B. Binnewald for permitting me to publish Figure 15, one of the first cases done by him as a Registrar ; Mr Todt for his assistance with the illustrations, and finally, Professor J. H. Louw, Head of the Department of Surgery, for his interest and encouragement.
REFERENCES
BURSTON, W. R. (196o). "lYans. int. Soc. plast. Surg. Second Congress, London, p. 28. Edinburgh : E. & S. Livingstone.
McNEIL, C. K. (1956). Brit. dent. ft., ioi, p. I9I.