The RNR Simulation Tool: Putting RNR to Work to Improve Client Outcomes Michael S. Caudy & Faye S. Taxman Center for Advancing Correctional Excellence (ACE!) George Mason University BJA: 2009-DG-BX-K026; SAMHSA: 202171; Public Welfare Foundation 1
Transcript
The RNR Simulation Tool: Putting RNR to Work to Improve Client Outcomes
Michael S. Caudy & Faye S. Taxman
Center for Advancing Correctional Excellence (ACE!)
George Mason University
BJA: 2009-DG-BX-K026; SAMHSA: 202171; Public Welfare Foundation
1
Faye S. Taxman, Ph.D University Professor
Center for Advancing Correctional Excellence
Criminology, Law and Society
George Mason University
10519 Braddock Road Suite 1900
Fairfax, VA 22032
James M. Byrne, Ph.D. Professor
University of Massachusetts, Lowell
April Pattavina, Ph.D.
Discrete Event Model
Associate Professor
University of Massachusetts, Lowell
Avinash Singh Bhati, Ph.D.
Simulation Model
Maxarth, LLC
Michael S. Caudy, Ph.D. Postdoctoral Research Fellow (ACE!)
Stephanie A. Ainsworth, M.A. Graduate Research Assistant (ACE!)
Erin L. Crites, M.A. Graduate Research Assistant (ACE!)
Joseph, M. Durso, B.S. Graduate Research Assistant (ACE!)
Special Acknowledgements: • Bureau of Justice Assistance
▫ BJA: 2009-DG-BX-K026
• Center for Substance Abuse Treatment
▫ SAMHSA: 202171
• Public Welfare Foundation
• Special Thanks to:
▫ Ed Banks, Ph.D.
▫ Ken Robertson
2
Why Treat CJ Clients?
• Disproportionate rate of SUDs and MH problems
• Public health and public safety benefits
▫ Decreased drug use
▫ Decreased drug-related crime
▫ Reduction in costs related to
Future CJ involvement
Chronic disease and health problems
▫ Improved relationships and employment prospects
• Treatment is effective
▫ Much more effective than sanctions alone
3
The RNR Framework
• Three core principles
▫ Risk – match level of service to individual’s risk to reoffend
▫ Need – target key behaviors we know will have an impact via evidence-based responses
▫ Responsivity – impact maximized when intervention is evidence-based and tailored to offender’s unique learning style
4
What is Risk?
• Risk is the likelihood that an offender will engage in future criminal behavior (recidivate) ▫ Can be static or dynamic or both
• Risk does NOT refer to dangerousness or
likelihood of violence
• Static risk factors have a direct correlation with criminal behavior ▫ Historical – based on criminal history ▫ Cannot be decreased by intervention
5
What are Needs? Criminogenic Needs Destabilizers
• Dynamic factors directly related to offending behavior ▫ Substance Dependence
“Criminogenic” drugs
▫ Criminal Thinking
• Amenable to change ▫ Can be changed ▫ Reduced needs =
reduced offending
• Should be primary focus of programming
• Clinical:
▫ Substance Abuse
▫ Mental Health
• Factors that do NOT have a direct relationship with offending behavior
• Can influence individuals’ ability to benefit from treatment/ programming
6
Risk Principle in Action – High Risk
-34
-18 -17
-15 -14
-10 -8
-6 -5
-2 -2
2 3 3 3
5 7
8 8 8 10 10
12 12 12 13 13
15
19 21
22 24
25 25 27
30 32
33 34
0
10
20
30
40
-10
-20
-30
-40
Ch
an
ge
in R
ecid
ivis
m R
ate
s
Lowenkamp & Latessa, 2005
7
8% Recidivism Reduction
Risk Principle in Action – Low Risk
-36
-32
-29 -29
-21 -21 -21 -21
-16 -15
-11 -11 -11
-7 -7 -6
-5 -4 -4 -4
-2 -2 -2 -1
0 1 1 1
2 3 3
4 4 5
6
8 9
0
10
-10
-20
-30
-40
Ch
an
ge
in R
ecid
ivis
m R
ate
s
Lowenkamp & Latessa, 2005
8
4% Recidivism Increase
3%
-1%
4%
10%
19%
23%
-5%
0%
5%
10%
15%
20%
25%
Risk Need Responsivity
Pe
rc
en
t R
ed
uc
tio
n i
n R
ec
idiv
ism
Recidivism Reduction by RNR Principles
No
Yes
Andrews & Bonta, 2006; 2010; see also Smith, Gendreau, & Swartz, 2009
9
Support for All Three Principles
The RNR Simulation Tool
• Provide decision support tools for the field ▫ Individual Level ▫ Program Feedback ▫ System Building Capability
• Program Tool focuses on: ▫ Classifying Programs ▫ Rating Key Program Features ▫ Linking to meta-analyses/systematic reviews
• Improve the capacity to identify programming that will
address public safety and health needs ▫ Population-level impact
• Reduce recidivism and costs through responsivity
10
Assess an Individual After intake interview
Summarize major findings
Draw from database on offender risk-need profiles
Replaces unknown factors with estimates
Recommends type and level of programming
11
Assess an Individual
• Make programming recommendations for individual offenders
▫ Based on risk level, primary criminogenic needs, and other clinically relevant factors
• Facilitate program matching
▫ Estimate recidivism rate and recidivism reduction associated with matching
• Improve access to treatment
12
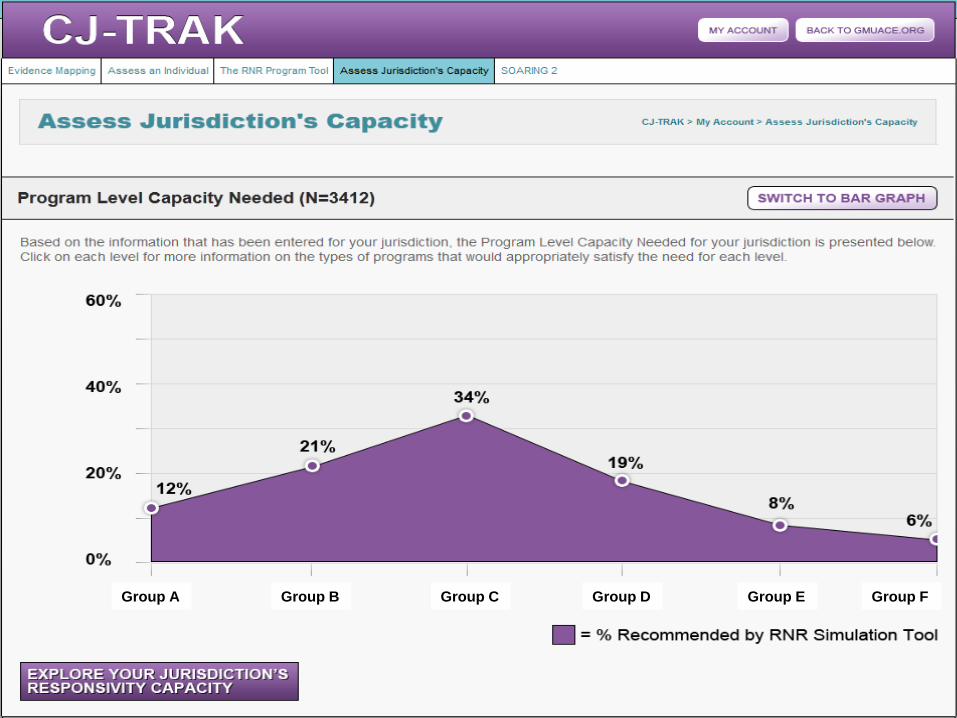
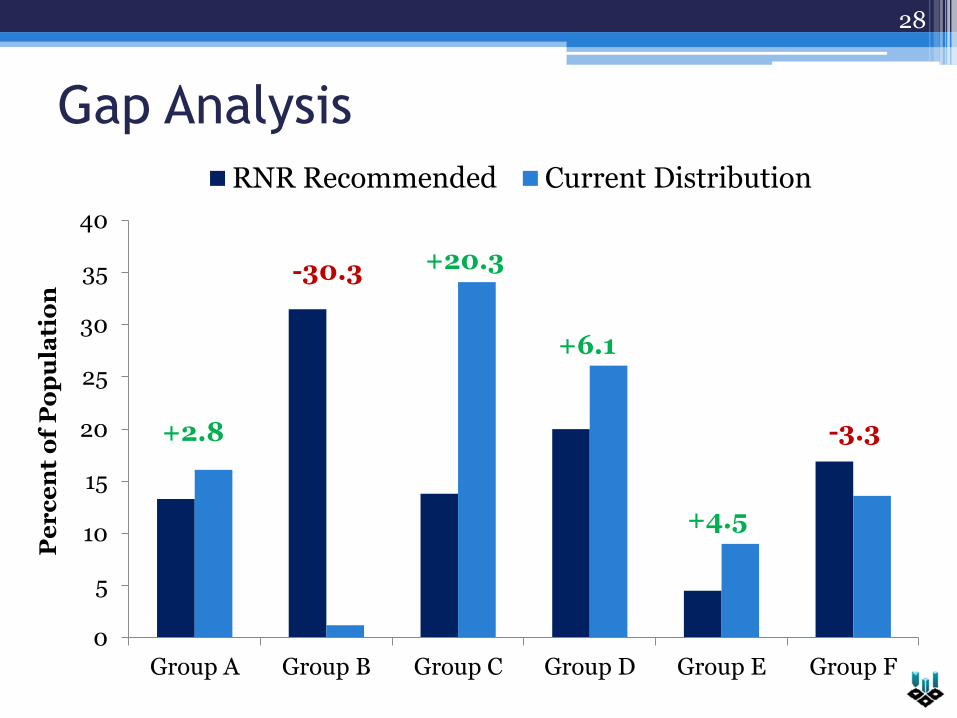
Program Groups
• Six program groups based on specific target behaviors
• Dependence on Criminogenic Drugs Group A
• Criminal Thinking/Cognitive Restructuring Group B
• Self Improvement and Management Group C
• Social/Interpersonal Skills Group D
• Life Skills (e.g. Education, Employment) Group E
• Punishment Only Group F
13
A Case Study
14
• Gender: Male
• Age Group: 28 – 36
• Risk Level: Moderate
• Criminogenic Needs: ▫ Drug Dependence: No ▫ Criminal Thinking: Yes
This project received funding from Bureau of Justice Assistance, Center for Substance Abuse Treatment, and Public Welfare Foundation. Views expressed here are ours and not the positions or policies of the funders.