ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2019 Digital Comprehensive Summaries of Uppsala Dissertations from the Faculty of Medicine 1556 The role of PDGF-B in brain blood vessels KHAYRUN NAHAR ISSN 1651-6206 ISBN 978-91-513-0607-0 urn:nbn:se:uu:diva-380088
Transcript
ACTAUNIVERSITATIS
UPSALIENSISUPPSALA
2019
Digital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1556
Dissertation presented at Uppsala University to be publicly examined in Rudbecksalen, DagHammarskjölds väg 20, Uppsala, Wednesday, 15 May 2019 at 09:00 for the degree of Doctorof Philosophy (Faculty of Medicine). The examination will be conducted in English. Facultyexaminer: Professor Jean-Baptiste Demoulin (De Duve Institute, Université Catholique deLouvain, Brussels, Belgium).
AbstractNahar, K. 2019. The role of PDGF-B in brain blood vessels. Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty of Medicine 1556. 48 pp. Uppsala: ActaUniversitatis Upsaliensis. ISBN 978-91-513-0607-0.
The development of blood vessels is dependent on several molecular cues to form properly.A functional PDGF-B/PDGFR-b signaling is paramount for the investment of mural cells, thatprovide with support, to the developing vasculature. Mutations in PDGFB and PDGFRB arelinked to PFBC, an age-dependent neurodegenerative condition manifested by vessel associatedcalcifications in the brain. The overall aim of the work presented in here was to investigatePFBC related calcifications and analyze the effects of impaired PDGF-B/PDGFR-b signalingon the formation of brain calcifications in different mouse models.
In paper I, we functionally analyzed PFBC-related PDGFB and PDGFRB mutations in vitro.While all PDGFB mutations lead to abolished protein function, PDGFRB mutations have morediverse consequences. We also show that reduced Pdgfb and Pdgfrb levels are insufficientfor the formation of brain calcifications in several mouse strains. Moreover, region-specificsusceptibility factors seem to reside in PFBC pathogenesis that are distinct from pericytecoverage and BBB deficiency.
In paper II, we described the molecular composition and cellular association of calcifiednodules that develop in two mouse models of PFBC, Pdgfbret/ret and Slc20a2-/- mice. We showthat the nodules are composed of pro- and anti-mineralization proteins and that they are in directassociation with astrocytes and microglia
In paper III, we analyzed the effects of EC-specific ablation of PDGF-B in adult brainvasculature. We report a substantial decrease of pericyte coverage and altered VSMCmorphology and that this phenotype is inadequate to trigger the formation of calcifications oraffect BBB integrity.
The aim of paper IV was to molecularly define the adult mouse brain vasculature by takingadvantage of the scRNAseq technique. Here, we describe a gradual change in expression profilealong the arteriovenous axis: ECs present a continuum along the axis while mural cell expressionprofile is punctuated.
In summary, this thesis present detailed description of calcifications formed in mouse modelsof PFBC and address the role of impaired PDGF-B/PDGFR-b signaling for the formationof nodules in mice. Furthermore, the scRNaseq analysis performed on healthy adult brainvasculature has paved the way for future analysis in mouse models of PFBC.
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Vanlandewijck, M., Lebouvier, T., Mäe, MA., Nahar, K., Horne-
mann, S., Kenkel, D., Cunha, SI., Lennartsson, J., Boss, A., Heldin, C-H., Keller, A., Betsholtz, C. (2015) Functional Char-acterization of Germline Mutations in PDGF-B and PDGFRB in Primary Familial Brain Calcification. PLoS One, 10 (11): e0143407
II Nahar, K., Lebouvier, T., Mäe, MA., Konzer, A., Bergquist, J., Zarb, Y., Johansson, B., Vanlandewijck, M., Betsholtz, C. Astro-cyte – microglial association and matrix deposition define com-mon pathogenic events in primary familial brain calcification. Manuscript
III Nahar, K., Bertuzzi, G., Vanlandewijck, M., Keller, A., Bets-
holtz, C., Mäe, MA. Endothelium-derived PDGF-B is essential for adult brain pericyte and vascular smooth muscle cell mainte-nance. Manuscript
IV Vanlandewijck, M., He, L., Mäe, MA., Andrae, J., Ando, K., Del Gaudio, F., Nahar, K., Lebouvier, T., Laviña, B., Gouveia, L., Sun, Y., Raschperger, E., Räsänen, M., Zarb, Y., Mochizuki, N., Keller, A., Lendahl, U., Betsholtz, C. (2018) A molecular atlas of cell types and zonation in the brain vasculature. Nature 554 (7693): 475–480
Reprints were made with permission from the respective publishers.
Other papers by the author
Mäe, MA., Li, T., Bertuzzi, G., Raschperger, E., Vanlandewijck, M., He, L., Nahar, K., Dalheim, A., Hofmann, JJ., Laviña, B., Keller, A., Betsholtz, C., Genové, G. Prolonged systemic hyperglycemia does not cause pericyte loss and permeability at the mouse blood-brain barrier. (2018) Scientific Report. 8(1):17462
He, L., Vanlandewijck, M., Mäe, MA., Andrae, J., Ando, K., Del Gaudio, F., Nahar, K., Lebouvier, T., Laviña, B., Gouveia, L., Sun, Y., Raschperger, E., Segerstolpe, Å., Liu, J., Gustafsson, S., Räsänen, M., Zarb, Y., Mochizuki, N., Keller, A., Lendahl, U., Betsholtz, C. (2018) Single-cell RNA sequencing of mouse brain and lung vascular and vessel-associated cell types. Scientific Data. 5:180160 Zarb, Y., Weber-Stadlbauer, U., Kirschenbaum, D., Kindler, DR., Richetto, J., Keller, D., Rademakers, R., Dickson, DW., Pasch, A., Byzova, T., Nahar, K., Voigt, FF., Helmchen, F., Boss, A., Aguzzi, A., Klohs, J., Keller, A. (2019) Ossified blood vessels in primary familial brain calcification elicit a neuro-toxic astrocyte response. Brain. pii: awz032
Contents
The vascular network.................................................................................11The cerebrovascular system ...................................................................11Properties of the BBB ...........................................................................12The neurovascular unit (NVU) ..............................................................13
Platelet-derived growth factors (PDGFs) and PDGF receptors (PDGFRs) ..16The role of PDGF-B and PDGFR-b in blood vessel formation ...............20Pathological roles of PDGF-B and PDGFR-b ........................................22
Primary familial brain calcifications (PFBC)..............................................22Intracranial calcifications ......................................................................23Pathophysiology of PFBC .....................................................................23
Diagnosis and clinical features ..........................................................24The genetic mutations causing PFBC ....................................................23Mouse models of PFBC ........................................................................27
Present investigations ................................................................................30Paper I ..................................................................................................30Paper II .................................................................................................31Paper III ................................................................................................32Paper IV................................................................................................33
The blood vascular network, also known as the cardiovascular system, is a circulatory system essential to sustain physiological functions of all other or-gans and cells in the vertebrate organisms. In a simplified view, the blood vasculature can schematically be visualized as vessels of different sizes, giv-ing rise to a closed and fluid-filled tubular network driven by the contractions of a muscular pump, the heart. Some of the main functions of blood vessels are to transport necessary substances (e.g. oxygen, nutrients) to the organs to maintain normal physiological functions, regulate body heat, filtration and re-move waste products and deliver immune cells to their final destination (Mo-nahan-Earley et al., 2013).
Blood vessels are arranged in a hierarchical manner, comprised of pressur-ized large arteries that carry oxygenated blood from the heart and feed into smaller arterioles (Potente and Mäkinen, 2017). Arterioles ultimately branch into a network of small sized capillaries and it is here, at the surface of the capillary network, where the exchange of nutrients and gases between the blood stream and the surrounding tissue occur. In the majority of organs, non-oxygenated blood then flows back through venules and larger veins in order to get rid of waste products and become re-oxygenated in the lungs, eventually closing the loop in the heart and re-circulating the blood.
The innermost lining of blood vessels, the endothelium, is composed of endothelial cells (ECs) that are enwrapped by a basement membrane (BM) and also supported by mural cells. Mural cell is a collective term for vascular smooth muscle cells (VSMCs) that wrap ECs of larger caliber vessels, and pericytes that cover ECs on capillaries and venules (Betsholtz, 2018).
Every organ has its own demands and requirements to fulfill their specific physiological functions. Accordingly, this has resulted in the adaptation and specialization of different vascular beds in different organs leading to vascular heterogeneity/vascular organotypicity (Betsholtz, 2018; Potente and Mäkinen, 2017). Heterogeneity can also be found within the same vascular bed of an organ. For instance, zonation of liver ECs displaying a gradual change in marker expression according to their anatomical location and functional prop-erties exists (Halpern et al., 2018).
Gaining more insight into how the vascular system and all its components function has been under the scope of intense research for a very long time (and still is). In fact, a dysfunctional vascular system has been implicated in several human conditions, ranging from cardio- and cerebrovascular diseases to
12
cancer. Although our knowledge of how such an intricate system, in both health and disease, is expanding it wouldn’t be excessive to claim that we have only just began to understand the broadness of its complexity.
The cerebrovascular system The human brain receives up to 20% of all the cardiac output, making it one of the highest demanding organs when it comes to total energy consumptions (Andreone et al., 2015). A rough estimation of the total capillary length in the average human brain is an astonishing 644 km and can cover a surface area of up to 20 m2 (Begley and Brightman, 2003)! To put things into perspective, if cerebral blood flow (CBF) comes to a halt the brain stops to function within seconds and neuronal damage can occur in just a few minutes. Disruption of CBF, and the subsequent perturbation in substance delivery and removal of by-products to and from brain cells respectively, has been implicated in neu-rodegenerative diseases such as Alzheimer’s disease (Zlokovic, 2008).
Arterial blood is supplied to the brain through the internal carotid artery and distal vertebral artery that forms the ring structure of the circle of Willis (Prince and Ahn, 2013). Large arteries are spread out on the surface of the subarachnoid space and divide into smaller pial arteries and arterioles that subsequently penetrate inwards and enter the brain tissue (Girouard and Iadecola, 2006) (Figure 1A). These vessels consist of ECs, VSMCs and astro-cyte end feet. As the arteries and arterioles gradually become smaller they lose the smooth muscle cell layer and turn into capillaries covered by pericytes and astrocyte end feet. In addition, brain blood vessels are in contact with nerve endings and other resident cells of the brain (see below, section on NVU) (Fig-ure 1B). It has been demonstrated that the capillary density in rat brain varies between the grey and white matter, reflecting local activity and metabolic de-mands (Borowsky and Collins, 1989).
Properties of the BBB The observation that the central nervous system (CNS) regulate the passage of molecules between the blood and different CNS tissues was made already in 1885 by Paul Ehrlich (Ehrlich, 1885). He performed experiments with sub-cutaneous injections of water-soluble dyes and noticed that it stained almost all organs except for the brain and spinal cord. Subsequent studies performed in similar manners and with electron microscopy studies confirmed the exist-ence of CNS barriers in the retina (Cunha-Vaz et al., 1966; PALM, 1947) and brain (Reese and Karnovsky, 1967). Regulated passage of substances have also been described for blood-nerve barrier, blood-spinal cord barrier and
13
blood-cerebrospinal fluid (CSF) barrier, encompassing different molecular signatures and functions (Reinhold and Rittner, 2017).
Figure 1. (A) Overview of the cerebral vasculature. Larger pial arteries of the sub-arachnoid space penetrate into the brain tissue and subsequently become smaller sized blood vessels. Dashed insert is magnified in (B) where the transition from larger artery and arteriole to smaller capillaries is illustrated. There is shift in associated cell types and mural cell coverage along the vascular tree. Within the brain parenchyma, neurons signal through chemical and electrical cues and require a homoeostatic microenvironment that is favorable for their communication. Maintenance of a homoeostatic microenvironment and pro-tection against neurotoxic insult is fundamental and obtained by the blood-
14
brain barrier (BBB), which is formed by specialized capillary ECs that regu-late the transport of molecules between the blood and brain. These ECs are tightly connected to one another by adherens junction (AJ) and tight junction (TJ) proteins (Dejana et al., 2009; Reese and Karnovsky, 1967). Functionally, AJs are involved in the initiation of cell-cell contacts which provides the tissue with structural support, while TJs regulate the paracellular transport of solutes. Vascular endothelial cadherin (VE-Cadherin) is a transmembrane AJ that spans the cleft between adjacent cells and is connected to intracellular actin cytoskeleton proteins. Occludins and claudins are transmembrane TJ proteins that also span the extracellular space between adjacent cells (Furuse et al., 1993; Morita et al., 1999). In addition, TJs are connected to the actin cytoskel-eton via regulatory scaffolding cytoplasmic proteins such as zonula occludens proteins. Among the TJ proteins, claudin-5 is expressed by ECs at the BBB (Liebner et al., 2000) and for long, it was believed that claudin-3 is also ex-pressed there. However, it was recently demonstrated that ECs at the BBB lack expression of claudin-3 in mice (Castro Dias et al., 2019).
The properties of the tight barrier require alternative ways of delivering essential molecules to brain cells and also to rapidly remove toxic substances from the brain tissue. Lipid-soluble molecules can cross the barrier by passive diffusion through complex physiochemical modes while the transport of gases such as oxygen and carbon dioxide occur via passive diffusion that is depend-ent on blood flow (Abbott et al., 2010). Furthermore, ECs at the BBB are equipped with transmembrane influx and efflux proteins that selectively al-lows for the passage of molecules. One such influx protein that is highly ex-pressed by brain ECs is the glucose transporter 1 (GLUT1) that belongs to the solute carrier (SLC) family of transporters. This transporter is critical to ac-commodate for the high glucose requirement of the brain (Brockmann, 2009; Crone, 1965) and the transport of lipids across the BBB is facilitated by the lipid transporter MFSD2A (Nguyen et al., 2014). The ATP-binding cassette (ABC) transporters consist of a large family of efflux proteins whose main functions are to actively pump out lipid-soluble compounds out of the brain parenchyma (Abbott et al., 2010).
Another route for macro-molecules across the endothelium of the BBB is transcytosis, the transport of substances in vesicles through endocytosis from the luminal to abluminal side of the vasculature (Nag, 2011). There are two types of transcytosis, receptor-mediated and adsorptive-mediated. An exam-ple of receptor-mediated transcytosis is the uptake of iron-containing transfer-rin by the Transferrin receptor from blood to brain (Jefferies et al., 1984; Moos and Morgan, 2000). Caveolae-facilitated uptake of positively charged mole-cules, such as cationic lipids and albumin, are internalized by adsorptive-me-diated endocytosis (Pulgar, 2018).
15
The neurovascular unit (NVU) The intimate cell-cell interactions between the components of the neurovas-cular unit (NVU) is essential to maintain the properties of the BBB. The func-tional units of the NVU (other than ECs) are mural cells, astrocyte end feet, microglia, BM and nerve endings (Figure 2). The constituents of the NVU contribute to the regulation and coupling of local neuronal requirements to changes in CBF (Girouard and Iadecola, 2006). Short descriptions of some of the NVU components are listed below.
Mural cells: the distinction between the two mural cell types, pericytes and VSMCs, has mainly focused on their morphology and anatomical lo-cations. They share many of the gene expression in mice (e.g. Pdgfrb, Cspg4, Des and Anpep) and are believed to derive from the same cell lin-eage (Armulik et al., 2005). VSMCs constitute a separate layer in the ves-sel wall and tightly wrap the vasculature with alpha-smooth muscle actin (a-SMA) fibers on arteries and arterioles. In contrast, pericytes do not ex-press a-SMA, share their BM with ECs and extend long primary pro-cesses with secondary thin processes along smaller vessels. Brain peri-cytes have been attributed to maintain and regulate transport across the BBB (Armulik et al., 2010; Daneman et al., 2010). The identity of a peri-cyte is still poorly understood and their proposed functional roles are var-ious - contractile abilities and regulation of vascular tone (Hall et al., 2014; Hill et al., 2015), stem cell properties (Crisan et al., 2008; Guimarães-Camboa et al., 2017), their role in pathological scarring (Gö-ritz et al., 2011; Soderblom et al., 2013) and the presence of different sub-populations have been reported in the literature (Göritz et al., 2011). How-ever, it is worth mentioning that many of the assigned pericyte properties have sparked controversy in the field with publications of conflicting data.
• Astrocytes: these are the most abundant glial cells in the adult CNS and acquire a spectrum of functions ranging from uptake and recycling of neu-rotransmitters to maintaining the properties of the BBB (Rothstein et al., 1996). Regional specific differences, where astrocytes perform distinct functions, have been reported to give rise to different subsets of cell iden-tities that gradually changes with age (Clarke et al., 2018). At the NVU, astrocytes are located on the abluminal side of blood vessels through their slender “foot processes” (also called astrocyte end feet) and cover the en-tire cerebral vasculature (Stewart and Wiley, 1981). These processes are highly enriched with water channels (e.g. aquaporin 4 (AQP4)) and plays a fundamental role in controlling water homeostasis at the barrier (Jung et al., 1994). In addition, astrocyte end feet are believed to regulate CBF through vessel constriction and dilation, thereby adjusting CBF to local neuronal activity and demand (Attwell et al., 2010).
16
Figure 2. Cellular and basement membrane contribution to the neurovascular unit (NVU) complex. The NVU is an extension of the blood-brain barrier (BBB) and the intimate cell-cell interaction between the components of the complex maintains the properties of the BBB.
• Microglia: often referred to as the resident immune cells of the CNS.
Resting microglia are equipped with long, thin processes radiating out from a small cell body (Helmut et al., 2011). During pathological situa-tions such as in Alzheimer’s disease, microglial gets activated, change ap-pearance to an amoeboid-like structure and become phagocytotic (Griciuc et al., 2013). The changes in morphology and function in activated mi-croglia is accompanied by the release of cytokines and changes in surface antigen expression (Berg et al., 2012).
• Basement membrane: a structural support and integral part of the extra-cellular matrix that connects and holds the separate building blocks of the NVU together. The BM is mainly comprised of proteoglycans, different collagen isoforms, laminins and nidogens (Engelhardt and Sorokin, 2009;
17
Sorokin et al., 1994). These components are produced and maintained by endothelial cells, pericytes and astrocyte end feet (Gautam et al., 2016; Sorokin et al., 1994; Y. Yao et al., 2014).
18
Platelet-derived growth factors (PDGFs) and PDGF receptors (PDGFRs)
Platelet-derived growth factors (PDGFs), first identified as a constituent of whole blood serum and purified from human platelets, is a family composed of disulfide-linked homo- and heterodimer polypeptide chains (Heldin and Westermark, 1999; Westermark and Wasteson, 1976). The growth factors were originally described as major mitogens for fibroblasts, smooth muscle cells and glia cells in culture (Kohler and Lipton, 1974; Ross et al., 1974; Westermark and Wasteson, 1976).
Four polypeptide chains (PDGF-A, PDGF-B, PDGF-C and PDGF-D), en-coded by four different genes, have been discovered to form five different dimeric isoforms; PDGF-AA, PDGF-BB, PDGF-CC, PDGF-DD and PDGF-AB (Andrae et al., 2008; Fredriksson et al., 2004). Whereas human PDGFA and PDGFB genes, carrying seven exons each, are located on chromosomes 7 (Betsholtz et al., 1986) and 22 (Dalla-Favera et al., 1982; Swan et al., 1982) respectively, PDGFC and PDGFD are expressed on chromosomes 4 and 11 (Uutela et al., 2001). For both PDGFA and PDGFB, exon 1 encodes the signal peptide while exons 2 and 3 encode the N-terminal precursor sequence that gets intracellularly processed and removed before secretion (Fredriksson et al., 2004). The mature part of the growth factor core domain is encoded by exons 4 and 5 whereas exon 6 encodes the C-terminal extension (also known as C-terminal retention motif) that is crucial for extracellular matrix (ECM) binding (Figure 3). Structurally, all PDGFs share a highly conserved growth factor core domain essential for peptide dimerization, receptor binding and receptor activation.
The PDGF ligands exert their biological effects on PDGF receptor -a (PDGFRa) and -b (PDGFRb) (Andrae et al., 2016; Gladh et al., 2016; Hell-ström et al., 1999; Lindahl et al., 1997b). These two receptors belong to the superfamily of receptor tyrosine kinases and are structurally composed of five extracellular immunoglobulin domains and two divided intracellular tyrosine kinase domains (Andrae et al., 2008) (Figure 4). In their inactive state, the receptors occur as monomers. However, upon ligand binding they undergo dimerization and transphosphorylation occurs at cytoplasmic kinase residues (Kazlauskas and Cooper, 1989; Kelly et al., 1991). This in turn creates dock-ing sites for Src homology 2 (SH2) domain containing molecules to bind to phosphotyrosine residues on the receptor (Claesson-Welsh, 1996), allowing
19
for further downstream signaling cascade events. The activation of the PDG-FRs engage several signaling pathways, including PI3K (Kazlauskas and Cooper, 1989), Ras-MAPK(Heldin et al., 1998) and PLCg (Sultzman et al., 1991). Cellular responses activated by the different signaling pathways in-volve cell motility and actin cytoskeleton rearrangement (Wennström et al., 1994), cell growth and cell differentiation (Heldin et al., 1998).
The dimerized receptors can appear in one out of the three following con-stellations: PDGFR-a, PDGFR-b and PDGFR-ab (Heldin and Westermark, 1999). Whereas PDGFR-a has been demonstrated to interact with PDGF-AA (Lindahl et al., 1997b) and PDGF-CC (Andrae et al., 2016) in vivo, PDGFR-b interacts with PDGF-BB (Hellström et al., 1999) and PDGF-DD (Gladh et al., 2016). PDGFR-ab is believed to interact with the heterodimer PDGF-AB (Heldin and Westermark, 1999). However, these observations are based on on in vitro studies.
Figure 3. Schematic drawing of human PDGFB gene, located on chromosome 22. The gene is composed of 7 exons where exons 4 and 5 encodes the growth factor core domain that interacts through dimerization with the receptor. Exon 6 encodes the C-terminal retention motif required for the interaction with extracellular matrix compo-nents. This thesis will from this point onwards focus on the roles of PDGF-B and PDGFRb under physiological and pathophysiological conditions. The tissue expression of the ligand and receptor vary and the physiological roles of their interactions have mainly been attributed to developmental processes. Mapping of the brain vasculature in adult mice using single cell RNA sequencing (scRNASeq) analysis shows that Pdgfb is mainly expressed by ECs, although lower expression is also seen in neurons (Sasahara et al., 1991), VSMCs and microglia (Vanlandewijck et al., 2018; Zeisel et al., 2018). EC-restricted Pdgfb expression is also found in the lung and other (but not all) organs (Tab-ula Muris Consortium et al., 2018). The expression of the receptor is confined to pericytes, VSMCs and fibroblasts in the mouse adult brain vasculature (Vanlandewijck et al., 2018) and different cell types (e.g. pericytes, VSMCs,
20
fibroblasts, stromal cells) in several other organs (Tabula Muris Consortium et al., 2018).
Figure 4. Schematic representation of PDGFR-b protein. The receptor is composed of five extracellular Ig domains, a transmembrane domain and two split intracellular tyrosine kinase domains. Upon ligand binding, the receptor dimerizes and becomes phosphorylated on tyrosine residues, which in turn triggers downstream signaling cas-cades and diverse biological effects.
The role of PDGF-B and PDGFR-b in blood vessel formation The development of blood vasculature can be divided in vasculogenesis, the de novo formation of tubular vessels by ECs, and angiogenesis, the formation of new blood vessels through remodeling and sprouting of pre-existing ones. Numerous molecular cues in the form of paracrine, juxtacrine and endocrine ligands play vital roles and are required for cell-cell communications during both vasculogenesis and angiogenesis. The main regulator of vascular devel-opment is vascular endothelial growth factor-A (VEGF-A) (Connolly, 1991; Gospodarowicz et al., 1989), a ligand that is produced by neural cells in the CNS and upregulated by hypoxia (Stone et al., 1995) .
The recruitment of mural cells, facilitated by PDGF-B/PDGFR-b signaling is also paramount for the development and stability of blood vessels (Armulik et al., 2010; Daneman et al., 2010). PDGF-B, produced and secreted by en-dothelial tip cells at the leading position of the angiogenic sprout, binds
21
through the retention motif to heparan sulfate proteoglycans (HSPG) in the ECM and creates a gradient of signaling cue along the developing vasculature (Abramsson et al., 2007; Hellström et al., 1999; Lindahl et al., 1997a; Lind-blom et al., 2003) (Figure 5). The ligand exerts its effect through paracrine signaling on PDGFRb positive VSMCs and pericytes and allows for their pro-liferation and migration and eventually guides them along the newly formed vessel.
The physiological roles of PDGF-B/PDGFR-b signaling were established in early studies where either the ligand or receptor were ablated in mice (Levéen et al., 1994; Soriano, 1994). Complete loss of PDGF-B or PDGFR-b in mice results in perinatal lethality. The pups die during late gestation due to widespread hemorrhage, general edema and organ failure. Subsequent find-ings report the failure of mural cell recruitment and the enlargement of blood vessels in these mice, linking PDGF-B/PDGFRb signaling to blood vessel for-mation during embryonic development (Hellström et al., 1999; Lindahl et al., 1997a).
Figure 5. The physiological role of PDGF-B/PDGFR-b signaling in blood vessel for-mation. During angiogenesis, PDGF-B is produced and secreted by endothelial tip cells at the sprouting front. The ligand exerts its effect on PDGFR-b positive mural cells and allows for their proliferation, migration and ultimately for their investment in the vessel wall. The binding of PDGF-B to extracellular matrix components, through the retention motif, is crucial for the formation of a growth factor gradient that acts as signaling cue for mural cells.
Using constitutive knockout (KO) approaches to specifically delete PDGF-B from ECs results in mice that are viable and reach adulthood (Bjarnegård et al., 2004; Enge, 2002). However, these mutants have impaired pericyte re-cruitment to brain capillaries, with 50-90% pericyte loss (Enge, 2002). In ad-dition, they exhibit kidney, placental and cardiac abnormalities, confirming the importance of PDGF-B signaling during embryonic development (Bjarnegård et al., 2004; Enge, 2002). Additionally, postnatal deletion of EC-
22
derived PDGF-B using tamoxifen inducible Cre-loxP system lead to pericyte drop-out on retinal capillaries and increased blood-retinal barrier permeability (Park et al., 2017; Pitulescu et al., 2010). Interestingly, neuron-specific abla-tion of PDGF-B result in viable mice which display no apparent effect on be-havior, pericyte loss or other vascular abnormalities (Enge et al., 2003).
The Pdgfb retention motif KO (Pdgfbret/ret) mouse model, where a stop co-don in exon 6 of the Pdgfb gene results in the deletion of the retention motif, has been extensively used to study the postnatal effects of impaired PDGF-B signaling (Lindblom et al., 2003). The mutation renders a biologically active PDGF-B protein that due to its inability to bind HSPG fails in proper recruit-ment of pericytes to the developing brain capillaries. The Pdgfbret/ret mice are adult viable and present two hallmarks of reduced brain pericyte coverage (25% as compared to control): capillary diameter enlargement and increased BBB permeability (Armulik et al., 2010).
Pathological roles of PDGF-B and PDGFR-b Although the pathological roles of PDGF-B and PDGFR-b are still poorly un-derstood, mutations in their respective genes have been linked to some rare tumors and leukemias (Demoulin and Essaghir, 2014; Östman and Heldin, 2007). The tumors associated with PDGFB and PDGFRb are of mesenchymal and glial origin (sarcomas and gliomas, respectively), reflecting the expres-sion patterns of the ligand and receptor.
Chromosomal translocation affecting the PDGFB gene is seen in a rare form of skin tumor of intermediate malignancy, dermatofibrosarcoma protu-berans (DFSP). In DFSP the translocation affects exon 2 of the PDGFB gene on chromosome 22, which fuses with the high expressing collagen 1 alpha 1 (COL1A1) gene on chromosome 17 (SIMMON, 1997). The fused gene en-codes a mature and functional PDGF-B protein that activates PDGFR-b through paracrine and autocrine signaling (Shimizu et al., 1999). Treatment with the tyrosine kinase inhibitor, imatinib, has shown clinical effects in pa-tients diagnosed with DFSP (McArthur et al., 2005).
Infantile myofibromatosis (IM) is a proliferative fibrous tumor affecting infants and children and found in soft tissue that has been linked to missense mutations in genes including PDGFRB and NOTCH3 (Cheung et al., 2013; J. Lee, 2013; Martignetti et al., 2013). The causative PDGFRB mutations ren-ders a receptor that is constitutively active in the absence of ligand and sensi-tive to tyrosine kinase inhibitors such as imatinib and nilotinib (Arts et al., 2016).
Interestingly, loss-of-function (LoF) mutations in both PDGFB and PDG-FRB were simultaneously discovered to be causative for primary familial brain calcification (PFBC) (Keller et al., 2013; Nicolas et al., 2013b).
23
Primary familial brain calcifications (PFBC)
Intracranial calcifications The findings of intracranial ectopic calcifications unaccompanied by any clin-ical manifestations are common in patients undergoing computed tomography scan (CT) (Kiroglu et. al., 2010). Incidents of non-pathological calcifications are discovered during routine CT scans in approximately 20% of the popula-tion and different brain regions are affected to different extent(Yamada et al., 2013). In the vast majority of cases, the calcifications develop in an aged-dependent manner and are detected in adults or elderly patients.
Rare congenital conditions associated with brain calcifications occur in diseases like Sturge-Weber syndrome (SWS) (Maton et al., 2010) and tuber-ous sclerosis (TS) (Thibaut et al., 1993). SWS results from cerebral vascular malformations in the cerebral cortex causing venous hypertension and subse-quent hyperfusion of the underlying tissue and chronic cerebral ischemia. TS is an autosomal dominant disease characterized by epilepsy and mental retar-dation where calcified lesions are found in the white matter (Kiroglu et. al., 2010).
In 1850, Delacour first documented the findings on vascular calcifications in the basal ganglia after pathological examination of a deceased patient that had shown clinical symptoms of tremors and weaknesses in lower extremities (Delacour, 1850). Later, Bamberger and Fahr also reported discoveries of bi-lateral calcifications in different brain regions of patients whom had been pre-sented with neurological symptoms (Manyam, 2005). Following his reports, Fahr’s name became associated with bilateral brain calcifications. In fact, one of the many names that has been used for the condition is Fahr’s syndrome. In recent years, the linking of mutations in specific genes to the disease, has been reflective in the terminology and nowadays the preferred nomenclature is PFBC. Prior to that, it was often referred to idiopathic basal ganglia calcifica-tions.
Pathophysiology of PFBC PFBC, a rare and age-dependent neurodegenerative condition, is manifested by the formation of bilateral calcium deposits primarily in the basal ganglia, thalamus brainstem and cerebellum (Manyam et al., 2001; Norman and
24
URICH, 1960; Westenberger and Klein, 2014). Although the prevalence of the disease remains mostly unknown, some reports have estimated it to be <1/1 000 000 in the population (Nicolas et al., 2018). The ambiguity to ascer-tain a precise number may stem from the fact that relatively few cases have been reported.
The deposits are composed of calcium (hydroxyapatite) but traces of silver, aluminum, arsenic, copper, cobalt, magnesium, silver, molybdenum, iron, lead, phosphorus, manganese and zinc has also been reported to be present (Duckett et al., 1977; Smeyers-Verbeke et al., 1975). Levels of calcium, phos-phorous and parathyroid hormones are normal and the systemic mineral me-tabolism is unaltered (Betsholtz and Keller, 2014; Samuels et al., 2018).
Bilateral calcifications in PFBC form along capillaries, arterioles and ven-ules along with associated gliosis from reactive astrocytes and microglia (Kozik and Kulczycki, 1978; Miklossy et al., 2005). Moreover, electron mi-croscopy (EM) analysis revealed the presence of mineral deposits within peri-vascular cells surrounding the blood vessels in samples from patients (Koba-yashi et al., 1987). Although signs of neuroinflammation and extravasation of plasma proteins have been reported, the general physiological state of neurons seems to be conserved (Miklossy et al., 2005). Other pathological findings in PFBC patients include vasogenic edema, dilation of lateral ventricles, reduc-tion in glucose metabolism and regional blood flow changes (Gomez et al., 2016; Kozik and Kulczycki, 1978; Shouyama et al., 2005).
It is, however, import to stress that many of these case reports were pub-lished before the genetic component of the disease was known. The hetero-genous pathologies of the reports associated with brain calcifications may as well have represented different disease etiologies.
Diagnosis and clinical features Diagnosis of PFBC is based on neuroimaging techniques, signs of progressive neurological dysfunction, absence of infectious or toxic agents in CSF and normal levels of minerals (e.g. calcium, magnesium, phosphorous), serum parathyroid hormone and heavy metal concentrations in urine and blood (Bonazza et al., 2011). Visualization of calcifications using brain CT scans appear more progressive in older individuals and calcified areas give a low signal intensity on magnetic resonance imaging (MRI) (Avrahami et al., 1994). While CT scans provide more sensitive detection of calcifications (Yamada et al., 2013), MRI offers a more detailed anatomical imaging (Av-rahami et al., 1994). To distinguish PFBC-related calcifications from other causes of calcifications using imaging techniques is generally not possible. However, the localization and appearance may be useful guidelines in the di-agnostics (Livingston et al., 2013). After the discoveries of the genetic contri-butions to the disease, genomic tests are performed to determine the diagnose.
25
The clinical manifestations of PFBC, albeit presented in a heterogenous manner, are restricted to the nervous system. Findings of bilateral calcifica-tions in asymptomatic individuals have been reported in ~30% of the cases (Huang et al., 2018; Manyam et al., 2001; Samuels et al., 2018). The relatively high frequency of asymptomatic cases may be a contributing factor to the un-derreporting nature of PFBC. Although most of the incidences have been re-ported in adults, the clinical onset ranges from early childhood to ~80 years of age (Nicolas et al., 2015) and the male:female ratio is estimated to be 2:1 (Manyam, 2005). The most frequent clinical symptoms accompanying the condition are neuropsychiatric symptoms (including behavioral disturbances, psychosis and cognitive impairment) (Adam et al., 1993; Chiriaco et al., 2018) and movement disorders (such as parkinsonism and tremor) (Rohani et al., 2017). Other less frequent signs are speech impairments, seizures, headache and vertigo (Guo et al., 2019; Y. J. Lee et al., 2018). It has been proposed that symptomatic patients are presented with higher calcification scores compared to asymptomatic patients (Nicolas et al., 2013a) and the correlation of specific phenotypes to the different genetic mutations have been observed (Batla et al., 2017).
The genetic mutations causing PFBC Although sporadic cases have been reported for the condition, a growing num-ber of studies have associated PFBC to pathogenic mutations in five different genes (below listed). Whereas mutations in four of the causative genes (SLC20A2, PDGFB, PDGFRB and XPR1) are inherited in an autosomal dom-inant manner, the latest one (MYORG) follows an autosomal recessive fashion (Figure 6).
• Solute carrier family 20 member 2 (SLC20A2): mutations in SLC20A2
were the first ones to be described as causative for the disease (Wang et al., 2012). Seven LoF mutations (five missense, one frameshift and one deletion) were discovered in seven families of different ancestry. Since that first discovery, more than 60 different variants have been reported in the literature and SLC20A2 mutations account for the most frequent ones in PFBC incidences (Oliva et al., 2019). The gene is located on chromo-some 8 and encodes the type III sodium-dependent inorganic phosphate (Pi) transporter 2 (PiT2), a transmembrane protein involved in phosphate homeostasis in various cell types and tissues including the brain (Ka-vanaugh and Kabat, 1996; Lagrue et al., 2010). A dysfunctional PiT2 protein may lead to inadequate uptake of Pi by cells, consequently leading to buildup of calcium phosphates in the tissue and subsequent formation of calcifications (Wang et al., 2012).
26
• PDGFRß: one missense mutation in the PDGFRß gene was discovered in two related French patients with a family history of PFBC (Nicolas et al., 2013b). Additional screening in 19 patients revealed one more mis-sense mutation in a sporadic case. Later, two more missense mutations in patients without a family history of PFBC were discovered to be patho-genic (Nicolas et al., 2013a; Sanchez-Contreras et al., 2014). All muta-tions have been predicted to be LoF and disease-causing due to conserved amino acid substitutions leading to reduced autophosphorylation and re-ceptor levels (Sanchez-Contreras et al., 2014).
• PDGFB: two pathogenic mutations, one nonsense and one missense,
were detected by genome sequencing in two different families (Keller et al., 2013). Sanger sequencing revealed the presence of four more addi-tional variants in families of mainly European ancestry. Two more spo-radic cases with new variants were discovered in French patients, one being a de-novo mutation (Nicolas et al., 2014a) and the other being a re-arraignment, deleting exons 3-6 of the PDGFB gene (Nicolas et al., 2014b).
• Xenotrpic and polytropic retrovirus receptor 1(XPR1): out of six de-
tected mutations, four deleterious missense variants in the XPR1 gene, were detected in five PFBC patients from unrelated families (Legati et al., 2015). One more variant was identified in a patient not long after (Anheim et al., 2016). The gene encodes a multi-pass transmembrane protein involved in Pi export and is conserved among most species (Ka-vanaugh et al., 1994). The mutations were identified to be located in a regulatory domain of the protein, leading to insufficient cellular phos-phate export (Legati et al., 2015). Gene expression analysis of XPR1 re-vealed a wide distribution in the mouse brain and functional analysis in-dicated a potential interaction of the protein with PDGFR-ß (X.-P. Yao et al., 2017).
• MYORG: the most recent identification of gene-specific mutations asso-
ciated with PFBC was found in MYORG (X.-P. Yao et al., 2018). Unlike the mutations in the previously described genes, mutations in MYORG are inherited in an autosomal recessive manner in patients. Nine variants were found and among those four were classified as missense mutations in highly conserved regions, three nonsense mutations and two were re-arrangement mutations. The gene encodes a lamina-associated trans-membrane protein, located in the nuclear envelope, that belongs to the glycosidase family 31 (Datta et al., 2009). Specific expression was found in astrocytes in the brain and inactivation of the enzyme was predicted to
27
lead to insufficient protein glycosylation and metabolism, ultimately trig-gering the formation of calcifications (X.-P. Yao et al., 2018).
Figure 6. Physiological roles of the PFBC-causative genes in humans. While SLC20A2, XPR1, PDGFB and PDGFB and PDGFRB all have shown to be inherited in an autosomal dominant fashion, MYORG is inherited in an autosomal recessive manner. The products of the five genes are structurally and functionally diverse and the mechanism by how pathogenic mutations in them causes PFBC is currently not known.
Mouse models of PFBC A few mouse models of PFBC, mimicking the human condition, have been established over the years in order to increase the understanding of the disease etiology. Slc20a2 homozygous KO mice were demonstrated to develop bilat-eral brain calcifications in agreement with reported findings in humans (Jen-sen et al., 2013). The authors used histological approaches to identify mineral nodules associated with blood vessels and macrophage/microglial reactivity, mainly in the thalamus along with a few findings in the cortex and basal gan-glia. Subsequent analysis of the Slc20a2-/- mice revealed the presence of ele-vated levels of inorganic phosphates in the CSF (Jensen et al., 2016; Walling-ford et al., 2016) and placental calcifications accompanied by abnormal pla-cental vasculature and increased BM deposition. Wallingford et. al. also re-ported the findings of nodules in adult heterozygous Slc20a+/- mice, formation
28
of ocular calcifications, intact BBB integrity, high expression of Slc20a2 in VSMCs and the formation of calcifications in arteriolar VSMCs in the glym-phatic-pathway (Wallingford et al., 2016). In sharp contrast, a more recent study failed in detecting nodules in heterozygous mice (Jensen et al., 2018). Moreover, the study suggest that the calcifications had an intracellular origin in pericytes and astrocytes and reported an increase in endogenous IgG around the calcifications, signs of dysfunctional BBB properties.
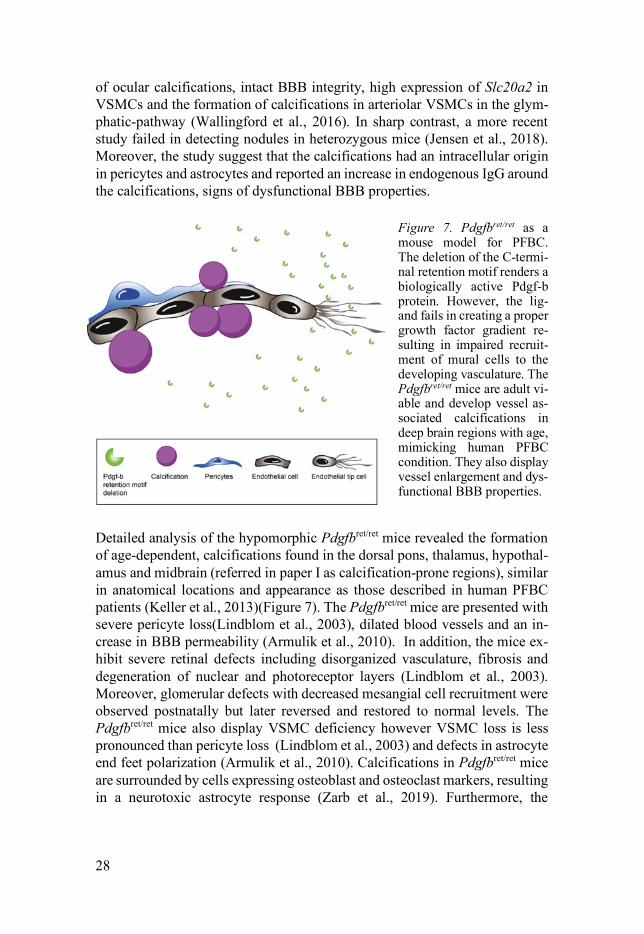
Figure 7. Pdgfbret/ret as a mouse model for PFBC. The deletion of the C-termi-nal retention motif renders a biologically active Pdgf-b protein. However, the lig-and fails in creating a proper growth factor gradient re-sulting in impaired recruit-ment of mural cells to the developing vasculature. The Pdgfbret/ret mice are adult vi-able and develop vessel as-sociated calcifications in deep brain regions with age, mimicking human PFBC condition. They also display vessel enlargement and dys-functional BBB properties.
Detailed analysis of the hypomorphic Pdgfbret/ret mice revealed the formation of age-dependent, calcifications found in the dorsal pons, thalamus, hypothal-amus and midbrain (referred in paper I as calcification-prone regions), similar in anatomical locations and appearance as those described in human PFBC patients (Keller et al., 2013)(Figure 7). The Pdgfbret/ret mice are presented with severe pericyte loss(Lindblom et al., 2003), dilated blood vessels and an in-crease in BBB permeability (Armulik et al., 2010). In addition, the mice ex-hibit severe retinal defects including disorganized vasculature, fibrosis and degeneration of nuclear and photoreceptor layers (Lindblom et al., 2003). Moreover, glomerular defects with decreased mesangial cell recruitment were observed postnatally but later reversed and restored to normal levels. The Pdgfbret/ret mice also display VSMC deficiency however VSMC loss is less pronounced than pericyte loss (Lindblom et al., 2003) and defects in astrocyte end feet polarization (Armulik et al., 2010). Calcifications in Pdgfbret/ret mice are surrounded by cells expressing osteoblast and osteoclast markers, resulting in a neurotoxic astrocyte response (Zarb et al., 2019). Furthermore, the
29
nodules are restricted to the brain and the mice display some behavioral alter-ations also reported in a subset of human PFBC cases.
In conjunction with the identification of recessive mutations in the MY-ORG gene causing PFBC in humans, it was also discovered that brain calcifi-cations develop in 9 month old Myorg KO mice in the thalamus region (X.-P. Yao et al., 2018). Taking into consideration that these mouse models represent mutations in genes that are structurally and functionally diverse, it is currently unclear to what extent they present the same disease etiology. Nevertheless, they are im-portant tools in taking us further in understanding PFBC.
30
Present investigations
Paper I Functional characterization of germline mutations in PDGFB and PDG-FRB in primary familial brain calcification The discovery that mutations in PDGFB and PDGFRb are causative for PFBC has assigned new pathogenic roles for the ligand and receptor. Therefore, we aimed to functionally analyze several of the known PFBC-related PDGFB and PDGFRb mutations in vitro in paper I. Our investigation showed that all six analyzed PDGFB mutations lead to complete loss of PDGFB function, either through abolished protein synthesis or through defective binding and/or stim-ulation of PDGFRβ.
By functionally assessing three PDGFRB mutations, we found that they had more diverse consequences, ranging from almost totally abolished auto-phosphorylation to reductions in protein levels and specific changes in PLCγ activation.
We also explored the outcomes of reduced Pdgfb or Pdgfrb transcript and protein levels in Pdgfb+/-, Pdgfrb+/- and Pdgfb+/-;Pdgfrb+/- mice on the for-mation of calcifications. Calcified nodules were neither detected in any of the abovementioned genetic models, nor did they develop in Pdgfrbredeye/redeye
mice, which show a 90% reduction of PDGFRβ protein levels. Analysis of pericyte coverage in calcification- prone and non-calcification-
prone brain regions in Pdgfbret/ret mice revealed that calcification-prone brain regions in Pdgfbret/ret mice had a higher pericyte coverage and a more intact BBB compared to non-calcification-prone brain regions. This suggest that re-gion-specific susceptibility factors may reside in PFBC pathogenesis that are distinct from pericyte coverage and BBB deficiency.
31
Paper II Astrocyte – microglial association and matrix deposition define common pathogenic events in primary familial brain calcification While the genes causing PFBC have diverse physiological functions, the de-velopment of brain calcifications have been reported for Slc20a2, Pdgfb and Myorg mutants, recapitulating the human condition. The aim of paper II was to perform an in-depth analysis of the calcifications formed in two of the abovementioned models, namely the Pdgfbret/ret and Slc20a2-/- mice.
By use of transmission electron microscopy and immunofluorescence we could show that the nodules display a multi-layered ultrastructure and that they are in direct contact with reactive astrocytes and microglia in both mod-els.
Through proteomic and immunofluorescence analysis, we found a com-mon molecular composition of the nodules, with the presence of proteins im-plicated in bone homeostasis. We also found that the nodules were composed of proteins that previously have not been linked to tissue mineralization. In addition, with immunofluorescence analysis, we could confirm the close as-sociation of astrocytes and microglia to the calcifications.
We also detected clear differences between the two models. While Pdgfbret/ret mice developed large, solitary nodules, the deposits in Slc20a2-/- mice were multi-lobulated and occurred in clusters. Moreover, the nodular distribution in Pdgfbret/ret mice were concentrated to the dorsal pons, thalamus, hypothalamus and midbrain. In contrast, they were more spread out in deeper brain regions in Slc20a2-/- mice and in few cases even detected in the cerebral cortex. This observation might reflect local anatomical differences leading to differences in mineral deposition susceptibility.
Assessment of pericyte coverage and blood-brain barrier integrity in Slc20a2-/- revealed both to be intact, suggesting that these two features, both compromised in Pdgfbret/ret mice, are likely not the causal triggers of PFBC pathogenesis. Instead, we propose that gene expression and spatial correla-tions point to astrocytes as culprit cells in PFBC.
32
Paper III Endothelium-derived PDGF-B is essential for adult brain pericyte and vascular smooth muscle cell maintenance The role of PDGF-B has mainly been attributed to mural cell recruitment and vessel maturation during developmental stages in the brain. However, what role endothelial sources of PDGF-B has on mural cell stability and mainte-nance in adult, quiescent vasculature is still not known.
In paper III, we sought to investigate the role of endothelium restricted PDGFB on mural cell maintenance in fully developed and quiescent adult brain vasculature. In addition, we studied whether the adult loss of Pdgfb is sufficient to cause increased BBB permeability and development of brain cal-cifications in mice.
For that, we took a tamoxifen-inducible approach to delete Pdgfb specifi-cally in endothelial cells by crossing either Pdgfbflox/flox or Pdgfbflox/- mice with Cdh5-CreERT2 mice (Pitulescu et al., 2010). This breeding strategy gave rise to litters with Cre negative offspring analyzed as controls (Ctrl) and Cre pos-itive mice with either two floxed alleles or one floxed and one null allele ana-lyzed as endothelial cell PDGF-B knock-outs (PdgfbECKO). We induced 2-month-old mice and sacrificed at 4 months for early time- point analysis and 12- and 18-months for late time-point analysis.
In paper I we showed that 50% loss of Pdgfb gene is not sufficient to sig-nificantly alter pericyte numbers or lead to the formation of calcifications in mice. In order to confirm sufficient gene deletion efficiency, we performed qPCR on isolated microvascular fragments from one brain hemisphere. The other hemisphere was utilized for either permeability studies or mural cell coverage studies by immunofluorescence. We also screened several late time-point litters for the appearance of calcification by staining with two of the calcification markers we found in paper II.
In this study, we demonstrate that endothelium-derived PDGFB is crucial for mural cell maintenance also in adult mouse brain. Deletion of endothelial Pdgfb (>80% downregulation in early time point and >95% in late time point) resulted in nearly 50% pericyte loss, as evident by pericyte coverage quantifi-cations and decreased expression levels of pericyte/mural cell genes. Although VSMC morphology was altered, they seemed affected to a lesser degree than the pericytes, an observation also made in constitutive Pdgfb and Pdgfrb mu-tants (Hellström et al., 1999). We did not detect any signs of vessel enlarge-ment, BBB disruption (assessed by intravenously injected Alexa Flour 555 cadaverine accumulation and Fibrinogen staining) or formation of calcifica-tions.
33
Paper IV A molecular atlas of cell types and zonation in the brain vasculature A dysfunctional brain vasculature in several cerebrovascular disorders is a major cause of death in many parts of the world. However, in order to under-stand how the vasculature changes under disease conditions, it is fundamental to define the molecular signature of brain vascular cells in a normal physio-logical state.
In paper IV, we used single-cell transcriptomics to provide molecular def-initions for the principal types of blood vascular and vessel-associated cells in the adult mouse brain. For this, we took advantage of the following reporter mice to capture major vascular and vessel-associated cell types from the adult brain: Cldn5-GFP, Pdgfrb-GFP; Cspg4-DsRed, Tagln-Cre; R26-stop-tdTomato and Pdgfra-H2BGFP. We sorted single cells in 384-well plates and created sequencing libraries with Smart-seq2 chemistry. After sequencing and alignment, the data was clustered using the BackSPIN algorithm and trans-formed in an online searchable database (http://betsholtzlab.org/Vascu-larSingleCells/database.html).
Through this investigation, we found a gradual phenotypic change (zona-tion) along the arteriovenous axis. While the endothelial cells present a tran-scriptomic continuum along the anatomical axis, mural cells displayed a punc-tuated expression profile along the axis, with an abrupt transition from VSMC to pericyte. We also establish that pericytes possess a single identity in the healthy adult mouse brain and that they are organotypic by comparing the vas-culature between brain and lung. Noticeably, brain pericytes abundantly ex-press SLC, ABC and ATP transporters while the same markers are absent or low expressed in lung pericytes. This shows that pericytes play an integral part in BBB transport. Moreover, we define a population of perivascular fibroblast-like cells that are present on all vessel types except capillaries.
34
Future perspectives
Our understanding of how the vasculature and vessel associated cells function in health and disease is significantly improving. Nevertheless, it is evident that with increasing knowledge, further questions arise that need to be addressed. The work presented herein has mainly focused on exploring the specific cir-cumstances resulting in the formation of vessel associated pathological brain calcifications in mouse models of PFBC.
With the aid of techniques such as scRNAseq, it is now possible to profile individual cells on a molecular level. This paves the way for future investiga-tions to unravel what happens to those same cell types under pathological con-ditions that might explain disease mechanisms. As a continuation of the study performed in paper IV, the lab is currently undertaking a similar approach to transcriptomically define endothelial cells and mural cells in Pdgfbret/ret mice. Interestingly, in paper I we discovered that pericyte drop-out and BBB impair-ment is more pronounced in non-calcification prone regions compared to cal-cification-prone regions. This particular finding raises the question to whether the mural cells and underlying ECs associated with nodules are dysfunctional to certain degrees in Pdgfbret/ret mice, and scRNAseq has the potential to pro-vide us an insight.
In contrast, pericyte coverage and BBB functions were found to be intact in Slc20a-/- mice and this might suggest that these two factors are less signifi-cant for the formation of calcifications. A more probable scenario is that as-trocytes and microglia play crucial roles in the calcification forming process. The two cell types were consistently observed to oppose the calcified nodules in paper II. Moreover, given that astrocytes express four out of the five PFBC-causing genes (to varying degrees) is intriguing enough to assign them a cen-tral role. These particular observations encouraged us to follow up on paper II by assessing the expression profiles of astrocytes and microglia in Pdgfbret/ret
mice using scRNAseq. We have isolated single cells from both calcification prone and non-calcification prone regions and sorted them in 384-well plates from the following transgenic lines: astrocytes from Pdgfbret/ret; Aldh1l1-tdTomato and microglia from Pdgfbret/ret; Cx3cr1-GFP. These experiments may provide insight into whether astrocytes and microglia in a brain calcifi-cation model express genes that are otherwise associated with osteoblasts and osteoclasts.
The findings in paper III suggests that loss of PDGF-B proteins is required during developmental stages in order to have a negative impact on BBB
35
integrity and for the formation of calcifications. However, we found that per-icyte coverage and mural cell phenotype were significantly altered in adult induced PdgfbECKO mice. Although the underlying vasculature seems normal in size, shape and density in PdgfbECKO, it would be of great interest to explore whether pericyte loss in this model affects other vascular properties such as blood flow, vascular tone and increased immune cell infiltration.
36
Acknowledgements
I have many people to express my gratitude towards. First and foremost, I would like to thank Christer Betsholtz, my main supervisor, for giving me the opportunity to do a PhD in a lab full of curios and sharp minds. Christer himself is a role model for many of us and inspiring in so many ways. His enthusiasm and passion for science is contagious and it is always very exciting to hear him discuss science stuff.
My journey here at Rudbeck lab started in the fall of 2014, with a nervous and somewhat shaky (from my side) interview with two people who intro-duced me to the world of PFBC. Those two are Michael Vanlandewijck and Thibaud Lebouvier, my two co-supervisors at the time. Thibaud left us too soon (to pursue his career in France), leaving an empty gap where his intelli-gent and warm-hearted personality used to fill. Michael, now without his other lab-half and my only co-supervisor, got stuck with me for four more years. For that, and all his wisdom, guidance and feedback I am tremendously thankful. I hope one day I can become as relaxed, confident and funny as he already is. Fun fact: all his boxes in the lab are marked as “Box 1”.
Along the way, I was introduced to people in the lab that came to play a major part in my work and personal life. Maarja Andaloussi Mäe is one of them. We ended up working closely together for the third paper in this thesis and I can honestly say that it was very exciting times. She has encouraged me to think more critically and helped me in so many aspects, both in the lab and outside. She also believes that she is a despot but has no idea what a lousy one she would make. Kind and thoughtful people make terrible despots.
I am also very grateful towards all our other CBZ lab members, both past (Colin, Bong, Koji, Nebojsa, Priya, Rajesh, Jen, Lwaki, Elisa) and present. I would specially like to thank Jana, Pia and Cissi for being patient and help-ing me all those times in the animal house and in the lab. Johanna, Kon, Marie, Riika, Barbara, Liqun, Ying, Jantine and Helene (everyone ought to have a Helene in their lives) have all helped me many times and made the working and social environment in the lab enjoyable and fun. Alberto can sometimes drive me crazy but I am happy that he ended up coming back to our group after that weird detour he made to BMC for his master thesis. Don’t trust him when he says that he is better than me at pipes (a big fat lie) and if you get an opportunity, ask him how Yosemite is pronounced. Leonor, Marco and Yang are the three, now all with their PhDs and flown out of the nests, former PhD-students that I had to live up to. They did not make it easy
37
for me and I miss you all! Tove, is the best office mate you can have and probably the most structured and organized person I have met. I am happy she has become an adopted member of the CBZ social activities. Her positive and cheerful personality spreads like rays of sunlight in her surroundings.
I would like to take the opportunity to thank people at Rudbeck and the vascbio community, with whom I have had the opportunity to interact with in one way or another: Maria Ulvmar, Peetra, Lena, Taija, Pontus, Milena, Sara, Miguel, Simon, Nina, Yan, Mark, Ross, Eric, Tor, Elin, Dom, Ve-ronica R, Svea, Kalyani, Maria Globish, Joppe, Emelie, Alessandra, Abdalla, Veronica S, Alba, Kiki, Marcus, Matko, Luz, Di, Dijana, Cherno and Abir. There are some remarkable people outside of work that have supported me in vått and torrt! I am so lucky to have these people in my life, although I know they would all agree that I am the worst at keeping in touch. You know who you are Sharzad, Canda, Shakia, Tusy, Regina, Dhifaf, Clarissa, Samira, Senait and Aylin. Sending you all some environmentally friendly Sist, men inte minst, vill jag tacka min familj. De är kärnan i min tillvaro och de personer som jag känner mig allra mest bekväm med. Utan min familj vet jag inte riktigt vad jag skulle tagit mig till många gånger och jag är så tacksam för att de finns närvarande i mitt liv. Mina systrar, Mamma Syd (med sin barnsliga humor och goda matlagning), Borris (med sitt pedantiska styre men oerhörda generositet) och Da (med allt sitt planerande och sin hjälpsamhet), ställer upp i alla väder och lägen. Jag skulle inte vilja byta ut mina systrar mot några andra i helaste världen! Mina bröder, Palle, Affe och Lutte som på olika sätt och nivåer är delaktiga i mitt liv. Har haft många diskussioner med dem och trots att de älskar att driva med mig så vet jag att de menar väl (hoppas jag). Även om de två sistnämnda är ingifta bröder så delar vi många starka band. Mina älskade syskonbarn (mina små börds), vad skulle jag göra utan er! Samantha är en riktig slarvpotta och latmask, men äger ett hjärta av guld. Simon har knappt sagt 1500 ord i hela sitt 16 år långa liv men det finns ingen snällare person här på jorden. Aaliyah, den lilla bråkstaken i familjen, visar och delar ut mer kärlek än någon annan av oss. Minstingen, Yosse-Bosse, är bara en så himla gullig och snäll liten pojke. Man vill typ bara nypa honom i kinderna hela tiden. Mamma, Pappa och mina växter, ni betyder allt!
38
References
Abbott, N.J., Patabendige, A.A.K., Dolman, D.E.M., Yusof, S.R., Begley, D.J., 2010. Structure and function of the blood-brain barrier. Neurobiology of Disease 37, 13–25. doi:10.1016/j.nbd.2009.07.030
Abramsson, A., Kurup, S., Busse, M., Yamada, S., Lindblom, P., Schallmeiner, E., Stenzel, D., Sauvaget, D., Ledin, J., Ringvall, M., Landegren, U., Kjellén, L., Bondjers, G., Li, J.-P., Lindahl, U., Spillmann, D., Betsholtz, C., Gerhardt, H., 2007. Defective N-sulfation of heparan sulfate proteoglycans limits PDGF-BB binding and pericyte recruitment in vascular development. Genes & Development 21, 316–331. doi:10.1101/gad.398207
Andrae, J., Gallini, R., Betsholtz, C., 2008. Role of platelet-derived growth factors in physiology and medicine. Genes & Development 22, 1276–1312. doi:10.1101/gad.1653708
Andrae, J., Gouveia, L., Gallini, R., He, L., Fredriksson, L., Nilsson, I., Johansson, B.R., Eriksson, U., Betsholtz, C., 2016. A role for PDGF-C/PDGFRα signaling in the formation of the meningeal basement membranes surrounding the cerebral cortex. Biol Open 5, 461–474. doi:10.1242/bio.017368
Anheim, M., López-Sánchez, U., Giovannini, D., Richard, A.-C., Touhami, J., N'Guyen, L., Rudolf, G., Thibault-Stoll, A., Frébourg, T., Hannequin, D., Cam-pion, D., Battini, J.-L., Sitbon, M., Nicolas, G., 2016. XPR1 mutations are a rare cause of primary familial brain calcification. Journal of Neurology 263, 1559–1564. doi:10.1007/s00415-016-8166-4
Armulik, A., Abramsson, A., Betsholtz, C., 2005. Endothelial/Pericyte Interactions. Circulation Research 97, 512–523. doi:10.1161/01.RES.0000182903.16652.d7
Armulik, A., Genové, G., Mäe, M., Nisancioglu, M.H., Wallgard, E., Niaudet, C., He, L., Norlin, J., Lindblom, P., Strittmatter, K., Johansson, B.R., Betsholtz, C., 2010. Pericytes regulate the blood-brain barrier. Nature 468, 557–561. doi:10.1038/na-ture09522
Arts, F.A., Chand, D., Pecquet, C., Velghe, A.I., Constantinescu, S., Hallberg, B., Demoulin, J.-B., 2016. PDGFRB mutants found in patients with familial infantile myofibromatosis or overgrowth syndrome are oncogenic and sensitive to imatinib. Oncogene 1998 17:10 35, 3239–3248. doi:10.1038/onc.2015.383
Attwell, D., Buchan, A.M., Charpak, S., Lauritzen, M., Macvicar, B.A., Newman, E.A., 2010. Glial and neuronal control of brain blood flow. Nature 468, 232–243. doi:10.1038/nature09613
Avrahami, E., Cohn, D.-F., Feibel, M., Tadmor, R., 1994. MRI demonstration and CT correlation of the brain in patients with idiopathic intracerebral calcification. Jour-nal of Neurology 241, 381–384. doi:10.1007/BF02033355
39
Batla, A., Tai, X.Y., Schottlaender, L., Erro, R., Balint, B., Bhatia, K.P., 2017. De-constructing Fahr's disease/syndrome of brain calcification in the era of new genes. Parkinsonism & Related Disorders 37, 1–10. doi:10.1016/j.parkreldis.2016.12.024
Begley, D.J., Brightman, M.W., 2003. Structural and functional aspects of the blood-brain barrier, in: Peptide Transport and Delivery Into the Central Nervous System. Birkhäuser, Basel, Basel, pp. 39–78. doi:10.1007/978-3-0348-8049-7_2
Betsholtz, C., 2018. Cell-cell signaling in blood vessel development and function. EMBO Mol Med 10, e8610. doi:10.15252/emmm.201708610
Betsholtz, C., Johnsson, A., Heldin, C.H., Westermark, B., Lind, P., Urdea, M.S., Eddy, R., Shows, T.B., Philpott, K., Mellor, A.L., 1986. cDNA sequence and chromosomal localization of human platelet-derived growth factor A-chain and its expression in tumour cell lines. Nature 320, 695–699. doi:10.1038/320695a0
Betsholtz, C., Keller, A., 2014. PDGF, Pericytes and the Pathogenesis of Idiopathic Basal Ganglia Calcification (IBGC). Brain Pathology 24, 387–395. doi:10.1111/bpa.12158
Bjarnegård, M., Enge, M., Norlin, J., Gustafsdottir, S., Fredriksson, S., Abramsson, A., Takemoto, M., Gustafsson, E., Fässler, R., Betsholtz, C., 2004. Endothelium-specific ablation of PDGFB leads to pericyte loss and glomerular, cardiac and placental abnormalities. Development (Cambridge, England) 131, 1847–1857. doi:10.1242/dev.01080
Bonazza, S., La Morgia, C., Martinelli, P., Capellari, S., 2011. Strio-pallido-dentate calcinosis: a diagnostic approach in adult patients. Neurol Sci 32, 537–545. doi:10.1007/s10072-011-0514-7
Borowsky, I.W., Collins, R.C., 1989. Metabolic anatomy of brain: a comparison of regional capillary density, glucose metabolism, and enzyme activities. The Jour-nal of Comparative Neurology 288, 401–413. doi:10.1002/cne.902880304
Brockmann, K., 2009. The expanding phenotype of GLUT1-deficiency syndrome. Brain Dev. 31, 545–552. doi:10.1016/j.braindev.2009.02.008
Castro Dias, M., Coisne, C., Lazarevic, I., Baden, P., Hata, M., Iwamoto, N., Fran-cisco, D.M.F., Vanlandewijck, M., He, L., Baier, F.A., Stroka, D., Bruggmann, R., Lyck, R., Enzmann, G., Deutsch, U., Betsholtz, C., Furuse, M., Tsukita, S., Engelhardt, B., 2019. Claudin-3-deficient C57BL/6J mice display intact brain barriers. Sci Rep 9, 203. doi:10.1038/s41598-018-36731-3
Cheung, Y.H., Gayden, T., Campeau, P.M., LeDuc, C.A., Russo, D., Nguyen, V.-H., Guo, J., Qi, M., Guan, Y., Albrecht, S., Moroz, B., Eldin, K.W., Lu, J.T., Schwartzentruber, J., Malkin, D., Berghuis, A.M., Emil, S., Gibbs, R.A., Burk, D.L., Vanstone, M., Lee, B.H., Orchard, D., Boycott, K.M., Chung, W.K., Jabado, N., 2013. A recurrent PDGFRB mutation causes familial infantile myo-fibromatosis. American Journal of Human Genetics 92, 996–1000. doi:10.1016/j.ajhg.2013.04.026
Chiriaco, C., Novellino, F., Salsone, M., Gagliardi, M., Morelli, M., Quattrone, A., 2018. Neuropsychological heterogeneity in patients with primary familial brain calcification due to a novel mutation in SLC20A2. Neurological Sciences: Offi-cial Journal of the Italian Neurological Society and of the Italian Society of Clin-ical Neurophysiology 39, 379–380. doi:10.1007/s10072-017-3125-0
40
Claesson-Welsh, L., 1996. Mechanism of action of platelet-derived growth factor. The International Journal of Biochemistry & Cell Biology 28, 373–385. doi:10.1016/1357-2725(95)00156-5
Clarke, L.E., Liddelow, S.A., Chakraborty, C., Münch, A.E., Heiman, M., Barres, B.A., 2018. Normal aging induces A1-like astrocyte reactivity. Proceedings of the National Academy of Sciences of the United States of America 115, E1896–E1905. doi:10.1073/pnas.1800165115
Connolly, D.T., 1991. Vascular permeability factor: A unique regulator of blood ves-sel function. Journal of Cellular Biochemistry 47, 219–223. doi:10.1002/jcb.240470306
Crisan, M., Yap, S., Casteilla, L., Chen, C.-W., Corselli, M., Park, T.S., Andriolo, G., Sun, B., Zheng, B., Zhang, L., Norotte, C., Teng, P.-N., Traas, J., Schugar, R., Deasy, B.M., Badylak, S., Bűhring, H.-J., Giacobino, J.-P., Lazzari, L., Huard, J., Péault, B., 2008. A Perivascular Origin for Mesenchymal Stem Cells in Multiple Human Organs. Cell Stem Cell 3, 301–313. doi:10.1016/j.stem.2008.07.003
Crone, C., 1965. Facilitated transfer of glucose from blood into brain tissue. J. Physiol. (Lond.) 181, 103–113. doi:10.1111/(ISSN)1469-7793
Cunha-Vaz, J.G., Shakib, M., Ashton, N., 1966. Studies on the permeability of the blood-retinal barrier. I. On the existence, development, and site of a blood-retinal barrier. Br J Ophthalmol 50, 441–453.
Dalla-Favera, R., Gallo, R.C., Giallongo, A., Croce, C.M., 1982. Chromosomal local-ization of the human homolog (c-sis) of the simian sarcoma virus onc gene. Sci-ence 218, 686–688.
Daneman, R., Zhou, L., Kebede, A.A., Ben A Barres, 2010. Pericytes are required for blood-brain barrier integrity during embryogenesis. Nature 468, 562–566. doi:10.1038/nature09513
Datta, K., Guan, T., Gerace, L., 2009. NET37, a Nuclear Envelope Transmembrane Protein with Glycosidase Homology, Is Involved in Myoblast Differentiation. The Journal of Biological Chemistry 284, 29666–29676. doi:10.1074/jbc.M109.034041
Dejana, E., Tournier-Lasserve, E., Weinstein, B.M., 2009. The control of vascular integrity by endothelial cell junctions: molecular basis and pathological implica-tions. Dev. Cell 16, 209–221. doi:10.1016/j.devcel.2009.01.004
Delacour, A., 1850. Ossification des capillaries du cerveau. Ann Med Psychol (Paris) 2:458-461
Demoulin, J.-B., Essaghir, A., 2014. PDGF receptor signaling networks in normal and cancer cells. Cytokine & Growth Factor Reviews 25, 273–283. doi:10.1016/j.cy-togfr.2014.03.003
Duckett, S., Galle, P., Escourolle, R., Poirier, J., Hauw, J.-J., 1977. Presence of zinc, aluminum, magnesium in striopalledodentate (SPD) calcifications (Fahr's dis-ease): Electron probe study. Acta Neuropathol. 38, 7–10. doi:10.1007/BF00691269
Ehrlich, M., 1885. Königthum und staatswesen der alten Hebräer: nach biblischen und talmudischen Quellen bearbeitet, eine populärwissenschaftliche Studie.
Enge, M., 2002. Endothelium-specific platelet-derived growth factor-B ablation mim-ics diabetic retinopathy. The EMBO Journal 21, 4307–4316. doi:10.1093/em-boj/cdf418
Enge, M., Wilhelmsson, U., Abramsson, A., Stakeberg, J., Kühn, R., Betsholtz, C., Pekny, M., 2003. Neuron-specific ablation of PDGF-B is compatible with normal central nervous system development and astroglial response to injury. Neuro-chem. Res. 28, 271–279.
41
Engelhardt, B., Sorokin, L., 2009. The blood-brain and the blood-cerebrospinal fluid barriers: function and dysfunction. Semin Immunopathol 31, 497–511. doi:10.1007/s00281-009-0177-0
Fredriksson, L., Li, H., Eriksson, U., 2004. The PDGF family: four gene products form five dimeric isoforms. Cytokine & Growth Factor Reviews 15, 197–204. doi:10.1016/j.cytogfr.2004.03.007
Furuse, M., Hirase, T., Itoh, M., Nagafuchi, A., Yonemura, S., Tsukita, S., 1993. Oc-cludin: a novel integral membrane protein localizing at tight junctions. J. Cell Biol. 123, 1777–1788.
Gautam, J., Zhang, X., Yao, Y., 2016. The role of pericytic laminin in blood brain barrier integrity maintenance. Sci Rep 6, 36450. doi:10.1038/srep36450
Girouard, H., Iadecola, C., 2006. Neurovascular coupling in the normal brain and in hypertension, stroke, and Alzheimer disease. J. Appl. Physiol. 100, 328–335. doi:10.1152/japplphysiol.00966.2005
Gladh, H., Folestad, E.B., Muhl, L., Ehnman, M., Tannenberg, P., Lawrence, A.-L., Betsholtz, C., Eriksson, U., 2016. Mice Lacking Platelet-Derived Growth Factor D Display a Mild Vascular Phenotype. PLoS ONE 11, e0152276. doi:10.1371/journal.pone.0152276
Gomez, C.R., Luque, A., Horenstein, S., 2016. Microvasculopathy May Precede Idi-opathic Cerebral Calcifications — Case Report:. Angiology 40, 67–72. doi:10.1177/000331978904000113
Gospodarowicz, D., Abraham, J.A., Schilling, J., 1989. Isolation and characterization of a vascular endothelial cell mitogen produced by pituitary-derived folliculo stel-late cells. Proceedings of the National Academy of Sciences 86, 7311–7315. doi:10.1073/pnas.86.19.7311
Göritz, C., Dias, D.O., Tomilin, N., Barbacid, M., Shupliakov, O., Frisén, J., 2011. A Pericyte Origin of Spinal Cord Scar Tissue. Science 333, 238–242. doi:10.1126/science.1203165
Griciuc, A., Serrano-Pozo, A., Parrado, A.R., Lesinski, A.N., Asselin, C.N., Mullin, K., Hooli, B., Choi, S.H., Hyman, B.T., Tanzi, R.E., 2013. Alzheimer's disease risk gene CD33 inhibits microglial uptake of amyloid beta. Neuron 78, 631–643. doi:10.1016/j.neuron.2013.04.014
Guimarães-Camboa, N., Cattaneo, P., Sun, Y., Moore-Morris, T., Gu, Y., Dalton, N.D., Rockenstein, E., Masliah, E., Peterson, K.L., Stallcup, W.B., Chen, J., Ev-ans, S.M., 2017. Pericytes of Multiple Organs Do Not Behave as Mesenchymal Stem Cells In Vivo. Cell Stem Cell 20, 345–359.e5. doi:10.1016/j.stem.2016.12.006
Guo, X.-X., Zou, X.-H., Wang, C., Yao, X.-P., Su, H.-Z., Lai, L.-L., Chen, H.-T., Lai, J.-H., Liu, Y.-B., Chen, D.-P., Deng, Y.-C., Lin, P., Lin, H.-S., Hong, B.-C., Yao, Q.-Y., Chen, X.-J., Huang, D.-Q., Fu, H.-X., Peng, J.-D., Niu, Y.-F., Zhao, Y.-Y., Zhu, X.-Q., Lu, X.-P., Lin, H.-L., Li, Y.-K., Liu, C.-Y., Huang, G.-B., Wang, N., Chen, W.-J., 2019. Spectrum of SLC20A2, PDGFRB, PDGFB, and XPR1 mutations in a large cohort of patients with primary familial brain calcification. Human Mutation 7, 248. doi:10.1002/humu.23703
Hall, C.N., Reynell, C., Gesslein, B., Hamilton, N.B., Mishra, A., Sutherland, B.A., O’Farrell, F.M., Buchan, A.M., Lauritzen, M., Attwell, D., 2014. Capillary peri-cytes regulate cerebral blood flow in health and disease. Nature 508, 55–60. doi:10.1038/nature13165
Halpern, K.B., Shenhav, R., Massalha, H., Toth, B., Egozi, A., Massasa, E.E., Medgalia, C., David, E., Giladi, A., Moor, A.E., Porat, Z., Amit, I., Itzkovitz, S., 2018. Paired-cell sequencing enables spatial gene expression mapping of liver endothelial cells. Nat. Biotechnol. 36, 962–970. doi:10.1038/nbt.4231
42
Heldin, C.-H., Östman, A., Rönnstrand, L., 1998. Signal transduction via platelet-de-rived growth factor receptors. Biochimica et Biophysica Acta (BBA) - Reviews on Cancer 1378, F79–F113. doi:10.1016/S0304-419X(98)00015-8
Heldin, C.H., Westermark, B., 1999. Mechanism of action and in vivo role of platelet-derived growth factor. Physiological Reviews 79, 1283–1316. doi:10.1146/an-nurev.ph.57.030195.001501
Hellström, M., Kalén, M., Lindahl, P., Abramsson, A., Betsholtz, C., 1999. Role of PDGF-B and PDGFR-beta in recruitment of vascular smooth muscle cells and pericytes during embryonic blood vessel formation in the mouse. Development (Cambridge, England) 126, 3047–3055.
Helmut, K., Hanisch, U.K., Noda, M., Verkhratsky, A., 2011. Physiology of micro-glia. Physiological Reviews 91, 461–553. doi:10.1152/physrev.00011.2010
Hill, R.A., Tong, L., Yuan, P., Murikinati, S., Gupta, S., Grutzendler, J., 2015. Re-gional Blood Flow in the Normal and Ischemic Brain Is Controlled by Arteriolar Smooth Muscle Cell Contractility and Not by Capillary Pericytes. Neuron 87, 95–110. doi:10.1016/j.neuron.2015.06.001
Huang, Y.-T., Zhang, L.-H., Li, M.-F., Cheng, L., Qu, J., Cheng, Y., Li, X., Zou, G.-Y., Zhou, H.-H., 2018. Clinical Features of Primary Familial Brain Calcification in 17 Families. Chin. Med. J. 131, 2997–3000. doi:10.4103/0366-6999.247218
Jensen, N., Autzen, J.K., Pedersen, L., 2016. Slc20a2 is critical for maintaining a physiologic inorganic phosphate level in cerebrospinal fluid. Neurogenetics 17, 125–130. doi:10.1007/s10048-015-0469-6
Jensen, N., Schrøder, H.D., Hejbøl, E.K., Füchtbauer, E.-M., de Oliveira, J.R.M., Pedersen, L., 2013. Loss of Function of Slc20a2 Associated with Familial Idio-pathic Basal Ganglia Calcification in Humans Causes Brain Calcifications in Mice. Journal of Molecular Neuroscience 51, 994–999. doi:10.1007/s12031-013-0085-6
Jensen, N., Schrøder, H.D., Hejbøl, E.K., Thomsen, J.S., Brüel, A., Larsen, F.T., Vinding, M.C., Orlowski, D., Füchtbauer, E.-M., Oliveira, J.R., Pedersen, L., 2018. Mice knocked out for the primary brain calcification associated gene Slc20a2 show unimpaired pre-natal survival but retarded growth and nodules in the brain that grow and calcify over time. Am. J. Pathol. doi:10.1016/j.aj-path.2018.04.010
Jung, J.S., Bhat, R.V., Preston, G.M., Guggino, W.B., Baraban, J.M., Agre, P., 1994. Molecular characterization of an aquaporin cDNA from brain: candidate osmore-ceptor and regulator of water balance. Proceedings of the National Academy of Sciences 91, 13052–13056.
Kavanaugh, M.P., Kabat, D., 1996. Identification and characterization of a widely expressed phosphate transporter/retrovirus receptor family. Kidney Int. 49, 959–963.
Kavanaugh, M.P., Miller, D.G., Zhang, W., Law, W., Kozak, S.L., Kabat, D., Miller, A.D., 1994. Cell-surface receptors for gibbon ape leukemia virus and ampho-tropic murine retrovirus are inducible sodium-dependent phosphate symporters. Proceedings of the National Academy of Sciences of the United States of America 91, 7071–7075. doi:10.1073/pnas.91.15.7071
Kazlauskas, A., Cooper, J.A., 1989. Autophosphorylation of the PDGF receptor in the kinase insert region regulates interactions with cell proteins. Cell 58, 1121–1133. doi:10.1016/0092-8674(89)90510-2
43
Keller, A., Westenberger, A., Sobrido, M.J., García-Murias, M., Domingo, A., Sears, R.L., Lemos, R.R., Ordoñez-Ugalde, A., Nicolas, G., da Cunha, J.E.G., Rushing, E.J., Hugelshofer, M., Wurnig, M.C., Kaech, A., Reimann, R., Lohmann, K., Do-bricić, V., Carracedo, Á., Petrović, I., Miyasaki, J.M., Abakumova, I., Mäe, M.A., Raschperger, E., Zatz, M., Zschiedrich, K., Klepper, J., Spiteri, E., Prieto, J.M., Navas, I., Preuss, M., Dering, C., Janković, M., Paucar, M., Svenningsson, P., Saliminejad, K., Khorshid, H.R.K., Novaković, I., Aguzzi, A., Boss, A., Le Ber, I., Defer, G., Hannequin, D., Kostić, V.S., Campion, D., Geschwind, D.H., Cop-pola, G., Betsholtz, C., Klein, C., Oliveira, J.R.M., 2013. Mutations in the gene encoding PDGF-B cause brain calcifications in humans and mice. Nature Genet-ics 45, 1077–1082. doi:10.1038/ng.2723
Kelly, J.D., Haldeman, B.A., Grant, F.J., Murray, M.J., Seifert, R.A., Bowen-Pope, D.F., Cooper, J.A., Kazlauskas, A., 1991. Platelet-derived growth factor (PDGF) stimulates PDGF receptor subunit dimerization and intersubunit trans-phosphor-ylation. The Journal of Biological Chemistry 266, 8987–8992.
Kobayashi, S., Yamadori, I., Miki, H., Ohmori, M., 1987. Idiopathic nonarterioscle-rotic cerebral calcification (Fahr's disease): an electron microscopic study. Acta Neuropathol. 73, 62–66. doi:10.1007/BF00695503
Kohler, N., Lipton, A., 1974. Platelets as a source of fibroblast growth-promoting ac-tivity. Experimental Cell Research 87, 297–301.
Kozik, M., Kulczycki, J., 1978. Laser-spectrographic analysis of the cation content in Fahr's syndrome. Arch. Psychiat. Nervenkr. 225, 135–142. doi:10.1007/BF00343397
Lagrue, E., Abe, H., Lavanya, M., Touhami, J., Bodard, S., Chalon, S., Battini, J.-L., Sitbon, M., Castelnau, P., 2010. Regional characterization of energy metabolism in the brain of normal and MPTP-intoxicated mice using new markers of glucose and phosphate transport. Journal of Biomedical Science 17, 91. doi:10.1186/1423-0127-17-91
Lee, J., 2013. Mutations in PDGFRB and NOTCH3 are the first genetic causes iden-tified for autosomal dominant infantile myofibromatosis. Clinical Genetics 84, 340–341. doi:10.1111/cge.12238
Lee, Y.J., Park, S., Kim, Y.W., Park, K.M., Hwan Kim, Il, Park, J.H., Park, B.S., 2018. A Case of Seizure Revealing Fahr’s Syndrome with Primary Hypoparathy-roidism. The American Journal of Case Reports 19, 1430–1433. doi:10.12659/AJCR.913382
Legati, A., Giovannini, D., Nicolas, G., López-Sánchez, U., Quintáns, B., Oliveira, J.R.M., Sears, R.L., Ramos, E.M., Spiteri, E., Sobrido, M.-J., Carracedo, Á., Cas-tro-Fernández, C., Cubizolle, S., Fogel, B.L., Goizet, C., Jen, J.C., Kirdlarp, S., Lang, A.E., Miedzybrodzka, Z., Mitarnun, W., Paucar, M., Paulson, H., Pariente, J., Richard, A.-C., Salins, N.S., Simpson, S.A., Striano, P., Svenningsson, P., Ti-son, F., Unni, V.K., Vanakker, O., Wessels, M.W., Wetchaphanphesat, S., Yang, M., Boller, F., Campion, D., Hannequin, D., Sitbon, M., Geschwind, D.H., Bat-tini, J.-L., Coppola, G., 2015. Mutations in XPR1 cause primary familial brain calcification associated with altered phosphate export. Nature Genetics 47, 579–581. doi:10.1038/ng.3289
Levéen, P., Pekny, M., Gebre-Medhin, S., Swolin, B., Larsson, E., Betsholtz, C., 1994. Mice deficient for PDGF B show renal, cardiovascular, and hematological abnormalities. Genes & Development 8, 1875–1887.
44
Liebner, S., Kniesel, U., Kalbacher, H., Wolburg, H., 2000. Correlation of tight junc-tion morphology with the expression of tight junction proteins in blood-brain bar-rier endothelial cells. Eur. J. Cell Biol. 79, 707–717. doi:10.1078/0171-9335-00101
Lindahl, P., Johansson, B.R., Levéen, P., Betsholtz, C., 1997a. Pericyte loss and mi-croaneurysm formation in PDGF-B-deficient mice. Science 277, 242–245.
Lindahl, P., Karlsson, L., Hellström, M., Gebre-Medhin, S., Willetts, K., Heath, J.K., Betsholtz, C., 1997b. Alveogenesis failure in PDGF-A-deficient mice is coupled to lack of distal spreading of alveolar smooth muscle cell progenitors during lung development. Development 124, 3943–3953. doi:10.1002/jez.1401500202
Lindblom, P., Gerhardt, H., Liebner, S., Abramsson, A., Enge, M., Hellström, M., Bäckström, G., Fredriksson, S., Landegren, U., Nyström, H.C., Bergström, G., Dejana, E., Östman, A., Lindahl, P., Betsholtz, C., 2003. Endothelial PDGF-B retention is required for proper investment of pericytes in the microvessel wall.
Livingston, J.H., STIVAROS, S., van der KNAAP, M.S., Crow, Y.J., 2013. Recog-nizable phenotypes associated with intracranial calcification. Developmental Medicine & Child Neurology 55, 46–57. doi:10.1111/j.1469-8749.2012.04437.x
Manyam, B.V., 2005. What is and what is not “Fahr's disease.” Parkinsonism & Re-lated Disorders 11, 73–80. doi:10.1016/j.parkreldis.2004.12.001
Manyam, B.V., Walters, A.S., Narla, K.R., 2001. Bilateral striopallidodentate calcin-osis: clinical characteristics of patients seen in a registry. Mov. Disord. 16, 258–264.
Martignetti, J.A., Tian, L., Li, D., Ramirez, M.C.M., Camacho-Vanegas, O., Camacho, S.C., Guo, Y., Zand, D.J., Bernstein, A.M., Masur, S.K., Kim, C.E., Otieno, F.G., Hou, C., Abdel-Magid, N., Tweddale, B., Metry, D., Fournet, J.-C., Papp, E., McPherson, E.W., Zabel, C., Vaksmann, G., Morisot, C., Keating, B., Sleiman, P.M., Cleveland, J.A., Everman, D.B., Zackai, E., Hakonarson, H., 2013. Mutations in PDGFRB Cause Autosomal-Dominant Infantile Myofibroma-tosis. The American Journal of Human Genetics 92, 1001–1007. doi:10.1016/j.ajhg.2013.04.024
Maton, B., Krsek, P., Jayakar, P., Resnick, T., Koehn, M., Morrison, G., Ragheb, J., Castellano-Sanchez, A., Duchowny, M., 2010. Medically intractable epilepsy in Sturge-Weber syndrome is associated with cortical malformation: implications for surgical therapy. Epilepsia 51, 257–267. doi:10.1111/j.1528-1167.2009.02304.x
McArthur, G.A., Demetri, G.D., Van Oosterom Journal of clinical oncology, A., 2004, 2005. Molecular and clinical analysis of locally advanced dermatofibrosarcoma protuberans treated with imatinib: Imatinib target exploration consortium study B ….
Miklossy, J., Mackenzie, I.R., Dorovini-Zis, K., Calne, D.B., Wszolek, Z.K., Klegeris, A., McGeer, P.L., 2005. Severe vascular disturbance in a case of familial brain calcinosis. Acta Neuropathol. 109, 643–653. doi:10.1007/s00401-005-1007-7
Monahan-Earley, R., Dvorak, A.M., Aird, W.C., 2013. Evolutionary origins of the blood vascular system and endothelium. J. Thromb. Haemost. 11 Suppl 1, 46–66. doi:10.1111/jth.12253
Moos, T., Morgan, E.H., 2000. Transferrin and Transferrin Receptor Function in Brain Barrier Systems. Cell Mol Neurobiol 20, 77–95. doi:10.1023/A:1006948027674
Morita, K., Sasaki, H., Furuse, M., Tsukita, S., 1999. Endothelial claudin: claudin-5/TMVCF constitutes tight junction strands in endothelial cells. J. Cell Biol. 147, 185–194.
45
Nag, S., 2011. Morphology and Properties of Brain Endothelial Cells, in: The Blood-Brain and Other Neural Barriers, Methods in Molecular Biology. Humana Press, Totowa, NJ, pp. 3–47. doi:10.1007/978-1-60761-938-3_1
Nguyen, L.N., Ma, D., Shui, G., Wong, P., Cazenave-Gassiot, A., Zhang, X., Wenk, M.R., Goh, E.L.K., Silver, D.L., 2014. Mfsd2a is a transporter for the essential omega-3 fatty acid docosahexaenoic acid. Nature 509, 503–506. doi:10.1038/na-ture13241
Nicolas, G., Charbonnier, C., Campion, D., Veltman, J.A., 2018. Estimation of mini-mal disease prevalence from population genomic data: Application to primary familial brain calcification. Am. J. Med. Genet. B Neuropsychiatr. Genet. 177, 68–74. doi:10.1002/ajmg.b.32605
Nicolas, G., Charbonnier, C., de Lemos, R.R., Richard, A.-C., Guillin, O., Wallon, D., Legati, A., Geschwind, D., Coppola, G., Frébourg, T., Campion, D., de Oliveira, J.R.M., Hannequin, D., collaborators from the French IBGC study Group, 2015. Brain calcification process and phenotypes according to age and sex: Lessons from SLC20A2, PDGFB, and PDGFRB mutation carriers. Am. J. Med. Genet. B Neuropsychiatr. Genet. 168, 586–594. doi:10.1002/ajmg.b.32336
Nicolas, G., Jacquin, A., Thauvin-Robinet, C., Rovelet-Lecrux, A., Rouaud, O., Pot-tier, C., Aubriot-Lorton, M.-H., Rousseau, S., Wallon, D., Duvillard, C., Béjot, Y., Frébourg, T., Giroud, M., Campion, D., Hannequin, D., 2014a. A de novo nonsense PDGFB mutation causing idiopathic basal ganglia calcification with lar-yngeal dystonia. Eur. J. Hum. Genet. 22, 1236–1238. doi:10.1038/ejhg.2014.9
Nicolas, G., Pottier, C., Charbonnier, C., Guyant-Maréchal, L., Ber, I.L., Pariente, J., Labauge, P., Ayrignac, X., Defebvre, L., Maltête, D., Martinaud, O., Lefaucheur, R., Guillin, O., Wallon, D., Chaumette, B., Rondepierre, P., Derache, N., Fro-mager, G., Schaeffer, S., Krystkowiak, P., Verny, C., Jurici, S., Sauvée, M., Vérin, M., Lebouvier, T., Rouaud, O., Thauvin-Robinet, C., Rousseau, S., Rov-elet-Lecrux, A., Frébourg, T., Campion, D., Hannequin, D., Group, T.F.I.S., 2013a. Phenotypic spectrum of probable and genetically-confirmed idiopathic ba-sal ganglia calcification. Brain 136, 3395–3407. doi:10.1093/brain/awt255
Nicolas, G., Pottier, C., Maltête, D., Coutant, S., Rovelet-Lecrux, A., Legallic, S., Rousseau, S., Vaschalde, Y., Guyant-Maréchal, L., Augustin, J., Martinaud, O., Defebvre, L., Krystkowiak, P., Pariente, J., Clanet, M., Labauge, P., Ayrignac, X., Lefaucheur, R., Le Ber, I., Frébourg, T., Hannequin, D., Campion, D., 2013b. Mutation of the PDGFRB gene as a cause of idiopathic basal ganglia calcification. Neurology 80, 181–187. doi:10.1212/WNL.0b013e31827ccf34
Nicolas, G., Rovelet-Lecrux, A., Pottier, C., Martinaud, O., Wallon, D., Vernier, L., Landemore, G., Chapon, F., Prieto-Morin, C., Tournier-Lasserve, E., Frébourg, T., Campion, D., Hannequin, D., 2014b. PDGFB partial deletion: a new, rare mechanism causing brain calcification with leukoencephalopathy. J. Mol. Neuro-sci. 53, 171–175. doi:10.1007/s12031-014-0265-z
Norman, R.M., URICH, H., 1960. The influence of a vascular factor on the distribu-tion of symmetrical cerebral calcifications. Journal of Neurology, Neurosurgery, and Psychiatry 23, 142–147.
Oliva, M., Capaldo, G., D'Amico, A., Colavito, D., Elefante, A., Straccia, G., Ugga, L., Puoti, G., 2019. A novel SLC20A2 gene mutation causing primary familial brain calcification in an Ukrainian patient. Neurological Sciences: Official Jour-nal of the Italian Neurological Society and of the Italian Society of Clinical Neu-rophysiology 36, 787–3. doi:10.1007/s10072-018-3684-8
Östman, A., Heldin, C.-H., 2007. PDGF Receptors as Targets in Tumor Treatment. Advances in Cancer Research 97, 247–274. doi:10.1016/S0065-230X(06)97011-0
46
PALM, E., 1947. On the occurrence in the retina of conditions corresponding to the blood-brain barrier. Acta Ophthalmol (Copenh) 25, 29–35.
Park, D.Y., Lee, J., Kim, J., Kim, K., Hong, S., Han, S., Kubota, Y., Augustin, H.G., Ding, L., Kim, J.W., Kim, H., He, Y., Adams, R.H., Koh, G.Y., 2017. Plastic roles of pericytes in the blood-retinal barrier. Nat Commun 8, 15296. doi:10.1038/ncomms15296
Pitulescu, M.E., Schmidt, I., Benedito, R., Adams, R.H., 2010. Inducible gene target-ing in the neonatal vasculature and analysis of retinal angiogenesis in mice. Nat Protoc 5, 1518–1534. doi:10.1038/nprot.2010.113
Potente, M., Mäkinen, T., 2017. Vascular heterogeneity and specialization in devel-opment and disease. Nat. Rev. Mol. Cell Biol. doi:10.1038/nrm.2017.36
Prince, E.A., Ahn, S.H., 2013. Basic vascular neuroanatomy of the brain and spine: what the general interventional radiologist needs to know. Semin Intervent Radiol 30, 234–239. doi:10.1055/s-0033-1353475
Pulgar, V.M., 2018. Transcytosis to Cross the Blood Brain Barrier, New Advance-ments and Challenges. Front Neurosci 12, 1019. doi:10.3389/fnins.2018.01019
Reese, T.S., Karnovsky, M.J., 1967. Fine structural localization of a blood-brain bar-rier to exogenous peroxidase. J. Cell Biol. 34, 207–217.
Reinhold, A.K., Rittner, H.L., 2017. Barrier function in the peripheral and central nervous system-a review. Pflügers Archiv: European Journal of Physiology 469, 123–134. doi:10.1007/s00424-016-1920-8
Rohani, M., Poon, Y.-Y., Naranian, T., Fasano, A., 2017. SCL20A2 mutation mim-icking fluctuating Parkinson's disease. Parkinsonism & Related Disorders 39, 93–94. doi:10.1016/j.parkreldis.2017.03.019
Ross, R., Glomset, J., Kariya, B., Harker, L., 1974. A platelet-dependent serum factor that stimulates the proliferation of arterial smooth muscle cells in vitro. Proceed-ings of the National Academy of Sciences of the United States of America 71, 1207–1210.
Rothstein, J.D., Dykes-Hoberg, M., Pardo, C.A., Bristol, L.A., Jin, L., Kuncl, R.W., Kanai, Y., Hediger, M.A., Wang, Y., Schielke, J.P., Welty, D.F., 1996. Knockout of glutamate transporters reveals a major role for astroglial transport in excitotox-icity and clearance of glutamate. Neuron 16, 675–686.
Samuels, C.R., Khanni, J.L., Barkley, K., Azhar, M., Espinosa, P.S., 2018. Case Re-port: An Incidental Finding of Fahr's Disease in a Patient with Hypochondria. Cureus 10, e3668. doi:10.7759/cureus.3668
Sanchez-Contreras, M., Baker, M.C., Finch, N.A., Nicholson, A., Wojtas, A., Wszolek, Z.K., Ross, O.A., Dickson, D.W., Rademakers, R., 2014. Genetic screening and functional characterization of PDGFRB mutations associated with basal ganglia calcification of unknown etiology. Human Mutation 35, 964–971. doi:10.1002/humu.22582
Sasahara, M., Fries, J.W., Raines, E.W., Gown, A.M., Westrum, L.E., Frosch, M.P., Bonthron, D.T., Ross, R., Collins, T., 1991. PDGF B-chain in neurons of the cen-tral nervous system, posterior pituitary, and in a transgenic model. Cell 64, 217–227.
Shimizu, A., O'Brien, K.P., Sjöblom, T., Pietras, K., Buchdunger, E., Collins, V.P., Heldin, C.H., Dumanski, J.P., Ostman, A., 1999. The dermatofibrosarcoma pro-tuberans-associated collagen type Ialpha1/platelet-derived growth factor (PDGF) B-chain fusion gene generates a transforming protein that is processed to func-tional PDGF-BB. Cancer Res. 59, 3719–3723.
Shouyama, M., Kitabata, Y., Kaku, T., Shinosaki, K., 2005. Evaluation of Regional Cerebral Blood Flow in Fahr Disease with Schizophrenia-Like Psychosis: A Case Report. American Journal of Neuroradiology 26, 2527–2529.
47
SIMMON, M.-P., 1997. Deregulation of the platelet-derived growth factor B-chain gene via fusion with collagen gene COL1A1 in dermatofirosarcoma protuberans and giant-cell fibroblastoma. Nature Genet 15, 95–98.
Smeyers-Verbeke, J., Michotte, Y., PELSMAECKERS, J., LOWENTHAL, A., MASSART, D.L., DEKEGEL, D., KARCHER, D., 1975. The chemical compo-sition of idiopathic nonarteriosclerotic cerebral calcifications. Neurology 25, 48–48. doi:10.1212/WNL.25.1.48
Soderblom, C., Luo, X., Blumenthal, E., Bray, E., Lyapichev, K., Ramos, J., Krishnan, V., Lai-Hsu, C., Park, K.K., Tsoulfas, P., Lee, J.K., 2013. Perivascular Fibroblasts Form the Fibrotic Scar after Contusive Spinal Cord Injury. J. Neurosci. 33, 13882–13887. doi:10.1523/JNEUROSCI.2524-13.2013
Soriano, P., 1994. Abnormal kidney development and hematological disorders in PDGF beta-receptor mutant mice. Genes & Development 8, 1888–1896. doi:10.1101/gad.8.16.1888
Sorokin, L., Girg, W., Göpfert, T., Hallmann, R., Deutzmann, R., 1994. Expression of novel 400-kDa laminin chains by mouse and bovine endothelial cells. Eur. J. Biochem. 223, 603–610.
Stewart, P.A., Wiley, M.J., 1981. Developing nervous tissue induces formation of blood-brain barrier characteristics in invading endothelial cells: a study using quail--chick transplantation chimeras. Dev. Biol. 84, 183–192.
Stone, J., Itin, A., Alon, T., Pe'er, J., Gnessin, H., Chan-Ling, T., Keshet, E., 1995. Development of retinal vasculature is mediated by hypoxia-induced vascular en-dothelial growth factor (VEGF) expression by neuroglia. J. Neurosci. 15, 4738–4747. doi:10.1523/JNEUROSCI.15-07-04738.1995
Sultzman, L., Ellis, C., Lin, L.L., Pawson, T., Knopf, J., 1991. Platelet-derived growth factor increases the in vivo activity of phospholipase C-gamma 1 and phospho-lipase C-gamma 2. Molecular and Cellular Biology 11, 2018–2025. doi:10.1128/MCB.11.4.2018
Swan, D.C., McBride, O.W., Robbins, K.C., Keithley, D.A., Reddy, E.P., Aaronson, S.A., 1982. Chromosomal mapping of the simian sarcoma virus onc gene ana-logue in human cells. Proceedings of the National Academy of Sciences 79, 4691–4695. doi:10.1073/pnas.79.15.4691
Tabula Muris Consortium, Overall coordination, Logistical coordination, Organ col-lection and processing, Library preparation and sequencing, Computational data analysis, Cell type annotation, Writing group, Supplemental text writing group, Principal investigators, 2018. Single-cell transcriptomics of 20 mouse organs cre-ates a Tabula Muris. Nature 562, 367–372. doi:10.1038/s41586-018-0590-4
Thibaut, H., Parizel, P.M., Van Goethem, J., De Schepper, A.M., 1993. Tuberous scle-rosis: CT and MRI characteristics. Eur J Radiol 16, 176–179.
Uutela, M., Lauren, J., Bergsten, E., Li, X., Horelli-Kuitunen, N., Eriksson, U., Alitalo, K., 2001. Chromosomal location, exon structure, and vascular expression patterns of the human PDGFC and PDGFD genes. Circulation 103, 2242–2247. doi:10.1161/01.CIR.103.18.2242
Vanlandewijck, M., He, L., Mäe, M.A., Andrae, J., Ando, K., Del Gaudio, F., Nahar, K., Lebouvier, T., Laviña, B., Gouveia, L., Sun, Y., Raschperger, E., Räsänen, M., Zarb, Y., Mochizuki, N., Keller, A., Lendahl, U., Betsholtz, C., 2018. A mo-lecular atlas of cell types and zonation in the brain vasculature. Nature 554, 475–480. doi:10.1038/nature25739
Wallingford, M.C., Chia, J., Leaf, E.M., Borgeia, S., Chavkin, N.W., Sawangmake, C., Marro, K., Cox, T.C., Speer, M.Y., Giachelli, C.M., 2016. SLC20A2 defi-ciency in mice leads to elevated phosphate levels in cerbrospinal fluid and glym-phatic pathway-associated arteriolar calcification, and recapitulates human
Wennström, S., Hawkins, P., Cooke, F., Hara, K., Yonezawa, K., Kasuga, M., Jack-son, T., Claesson-Welsh, L., Stephens, L., 1994. Activation of phosphoinositide 3-kinase is required for PDGF-stimulated membrane ruffling. Current Biology 4, 385–393. doi:10.1016/S0960-9822(00)00087-7
Westenberger, A., Klein, C., 2014. The genetics of primary familial brain calcifica-tions. Current Neurology and Neuroscience Reports 14, 490. doi:10.1007/s11910-014-0490-4
Westermark, B., Wasteson, P., 1976. A platelet factor stimulating human normal glial cells. Experimental Cell Research 98, 170–174. doi:10.1016/0014-4827(76)90476-6
Yamada, M., Asano, T., Okamoto, K., Hayashi, Y., Kanematsu, M., Hoshi, H., Akaiwa, Y., Shimohata, T., Nishizawa, M., Inuzuka, T., Hozumi, I., 2013. High frequency of calcification in basal ganglia on brain computed tomography images in Japanese older adults. Geriatrics \& Gerontology International 13, 706–710. doi:10.1111/ggi.12004
Zarb, Y., Weber-Stadlbauer, U., Kirschenbaum, D., Kindler, D.R., Richetto, J., Kel-ler, D., Rademakers, R., Dickson, D.W., Pasch, A., Byzova, T., Nahar, K., Voigt, F.F., Helmchen, F., Boss, A., Aguzzi, A., Klohs, J., Keller, A., 2019. Ossified blood vessels in primary familial brain calcification elicit a neurotoxic astrocyte response. Brain 116, 2841. doi:10.1093/brain/awz032
Zeisel, A., Hochgerner, H., Lönnerberg, P., Johnsson, A., Memic, F., van der Zwan, J., Häring, M., Braun, E., Borm, L.E., La Manno, G., Codeluppi, S., Furlan, A., Lee, K., Skene, N., Harris, K.D., Hjerling-Leffler, J., Arenas, E., Ernfors, P., Marklund, U., Linnarsson, S., 2018. Molecular Architecture of the Mouse Nerv-ous System. Cell 174, 999–1014.e22. doi:10.1016/j.cell.2018.06.021
Zlokovic, B.V., 2008. The Blood-Brain Barrier in Health and Chronic Neurodegener-ative Disorders. Neuron 57, 178–201. doi:10.1016/j.neuron.2008.01.003
Acta Universitatis UpsaliensisDigital Comprehensive Summaries of Uppsala Dissertationsfrom the Faculty of Medicine 1556
Editor: The Dean of the Faculty of Medicine
A doctoral dissertation from the Faculty of Medicine, UppsalaUniversity, is usually a summary of a number of papers. A fewcopies of the complete dissertation are kept at major Swedishresearch libraries, while the summary alone is distributedinternationally through the series Digital ComprehensiveSummaries of Uppsala Dissertations from the Faculty ofMedicine. (Prior to January, 2005, the series was publishedunder the title “Comprehensive Summaries of UppsalaDissertations from the Faculty of Medicine”.)