CARDIAC SONOGRAPHER'S COMMUNICATIONS The Role of the Cardiac Sonographer in the Evaluation of the Heart Transplant Recipient Terry Reynolds, BS, and Marsha Halfinan-Franey, RN, MSN, Phoenix, Ariz. In sixteen years, heart transplantation has changed from a high technology adventure to what has re- cently been described as a "service need." At the end of 1984, there were at least 10 American pro- grams for heart transplantation, with 15 more in preparation. There are currently 72 centers in the United States and at least 27 in other countries that perform cardiac transplantation. 1 Although the introduction of cyclosporine in 1980 has markedly improved survival in heart transplant recipients, early detection.of cardiac allograft rejec- tion remains a major problem. 2 The diagnosis of car- diac rejection has been based on the results of en- domyocardial biopsy, which is considered the only reliable test. 3 Echocardiography combined with car- diac Doppler is an integral part of the follow-up of heart transplant patients and is used to evaluate car- diac function as well as for the detection of acute early rejection. The aim of this review article is to provide an overview of orthotopic cardiac transplantation for the cardiac sonographer, including indications, sur- gical technique, survival rate, complications, electro- cardiographic findings, radiographic findings, "nor- mal" echocardiographic and Doppler findings after transplant surgery, and possible echocardiographic and Doppler findings in acute early rejection. Sug- gestions for a routine echocardiographic and cardiac Doppler examination will be made and, in addition, a sample echocardiographic and cardiac Doppler worksheet will be provided. With this information, the sonographer will be able to thoughtfully ap- proach the echocardiographic and cardiac Doppler examination of the heart transplant patient. From the School of Cardiac Ultrasound and the Cardiovascular Nurse Specialist Program, Arizona Heart Institute Foundation. Reprint requests: Terry Reynolds, BS, Director, School of Cardiac Ultrasound, Ariwna Heart Institute Foundation, 2632 N. 20th Street, Phoenix, AZ 85006. 27/1/16625 INDICATIONS FOR ORTHOTOPIC CARDIAC TRANSPLANT Presently about one half of all cardiac transplan- tations performed have been for dilated cardiomy- opathy with global left ventricular dysfunction of id- iopathic, viral, or postpartum origin. Recent exten- sion of the chronologic age limit has resulted in nearly an equal number of patients with end-stage heart disease caused by extensive coronary artery dis- ease also receiving cardiac transplants. 3 SURGICAL TECHNIQUE Orthotopic cardiac transplantation involves excision of the recipient'S diseased heart and its subsequent replacement with another human donor heart (fig- ure 1). Mter a median sternotomy, dissection, and initiation of cardiopulmonary bypass, the recipient's heart is removed. This cardiectomy requires transec- tion of the main pulmonary artery and aorta, with partial resection of the atria, leaving the posterior walls intact. These portions retain their systemic and pulmonary venous connections and serve for surgical attachment to the donor heart. The donor cardiectomy differs from that of the recipient in that the heart is removed intact. Implan- tation begins after the organ is trimmed to fit the atria and the great vessels. Anastomoses are then made between the recipient and donor left atria, septa, right atria, aorta, and pulmonary arteries. The cardiac transplantation operation itself is usually un- eventful. 3 SURVIVAL Results from the Stanford program indicate that sur- vival is 83% ± 3.6% at 1 year after transplantation and nearly 76% ± 4.5% at 2 years. The registry of 431
Transcript
CARDIAC SONOGRAPHER'S COMMUNICATIONS
The Role of the Cardiac Sonographer in the Evaluation of the Heart Transplant Recipient
Terry Reynolds, BS, and Marsha Halfinan-Franey, RN, MSN, Phoenix, Ariz.
In sixteen years, heart transplantation has changed from a high technology adventure to what has recently been described as a "service need." At the end of 1984, there were at least 10 American programs for heart transplantation, with 15 more in preparation. There are currently 72 centers in the United States and at least 27 in other countries that perform cardiac transplantation. 1
Although the introduction of cyclosporine in 1980 has markedly improved survival in heart transplant recipients, early detection.of cardiac allograft rejection remains a major problem.2 The diagnosis of cardiac rejection has been based on the results of endomyocardial biopsy, which is considered the only reliable test. 3 Echocardiography combined with cardiac Doppler is an integral part of the follow-up of heart transplant patients and is used to evaluate cardiac function as well as for the detection of acute early rejection.
The aim of this review article is to provide an overview of orthotopic cardiac transplantation for the cardiac sonographer, including indications, surgical technique, survival rate, complications, electrocardiographic findings, radiographic findings, "normal" echocardiographic and Doppler findings after transplant surgery, and possible echocardiographic and Doppler findings in acute early rejection. Suggestions for a routine echocardiographic and cardiac Doppler examination will be made and, in addition, a sample echocardiographic and cardiac Doppler worksheet will be provided. With this information, the sonographer will be able to thoughtfully approach the echocardiographic and cardiac Doppler examination of the heart transplant patient.
From the School of Cardiac Ultrasound and the Cardiovascular Nurse Specialist Program, Arizona Heart Institute Foundation.
Reprint requests: Terry Reynolds, BS, Director, School of Cardiac Ultrasound, Ariwna Heart Institute Foundation, 2632 N. 20th Street, Phoenix, AZ 85006.
27/1/16625
INDICATIONS FOR ORTHOTOPIC CARDIAC TRANSPLANT
Presently about one half of all cardiac transplantations performed have been for dilated cardiomyopathy with global left ventricular dysfunction of idiopathic, viral, or postpartum origin. Recent extension of the chronologic age limit has resulted in nearly an equal number of patients with end-stage heart disease caused by extensive coronary artery disease also receiving cardiac transplants. 3
SURGICAL TECHNIQUE
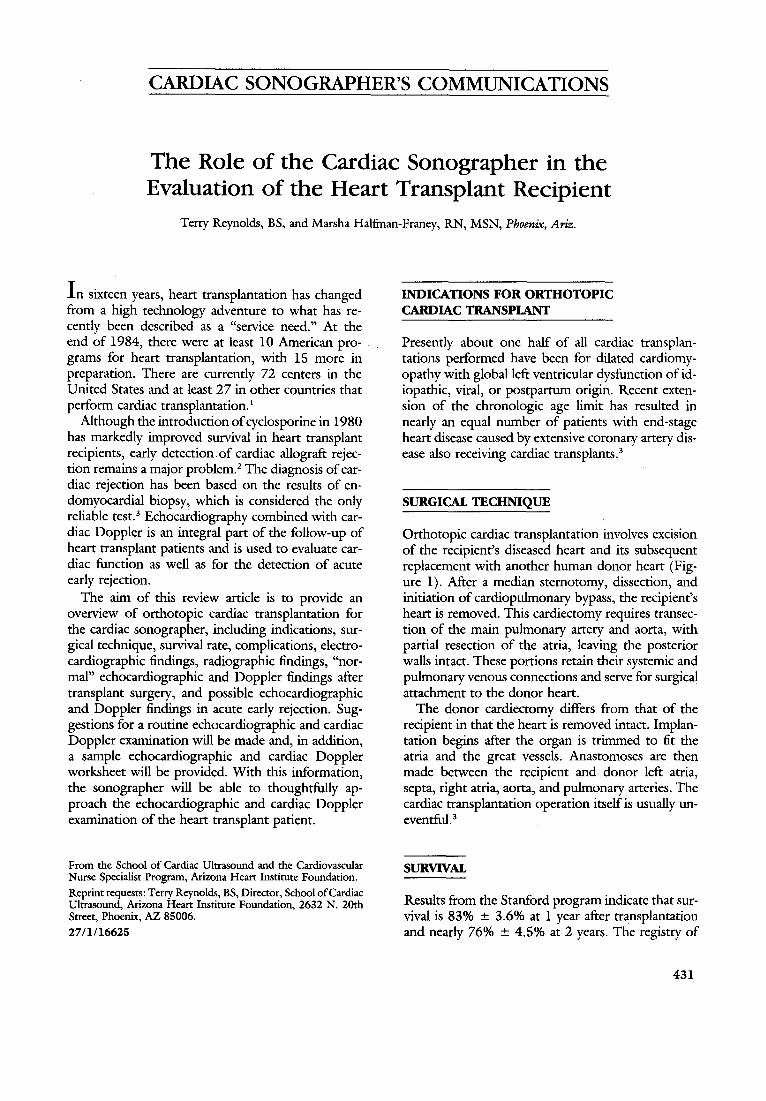
Orthotopic cardiac transplantation involves excision of the recipient'S diseased heart and its subsequent replacement with another human donor heart (figure 1). Mter a median sternotomy, dissection, and initiation of cardiopulmonary bypass, the recipient's heart is removed. This cardiectomy requires transection of the main pulmonary artery and aorta, with partial resection of the atria, leaving the posterior walls intact. These portions retain their systemic and pulmonary venous connections and serve for surgical attachment to the donor heart.
The donor cardiectomy differs from that of the recipient in that the heart is removed intact. Implantation begins after the organ is trimmed to fit the atria and the great vessels. Anastomoses are then made between the recipient and donor left atria, septa, right atria, aorta, and pulmonary arteries. The cardiac transplantation operation itself is usually uneventful. 3
SURVIVAL
Results from the Stanford program indicate that survival is 83% ± 3.6% at 1 year after transplantation and nearly 76% ± 4.5% at 2 years. The registry of
431
432 Reynolds and Halfman-Franey
Figure 1 A, The left atrial anastomosis is commenced at the recipient left superior pulmonary vein and the donor left atrial appendage. B, The left atrial anastomosis is completed, and the right atrial anastomosis is begun. Note that the incision in the donor right atrium begins through the inferior vena cava and then curves anteromedially, to avoid injury to the sinoatrial node. C, The atrial anastomoses are complete, and the aortic anastomosis is near completion. The pulmonary arterial anastomosis is carried out last, after removal of the aortic clamp. SVC, Superior vena cava;IVC, inferior Vena cava; RA, right atrium; LA, left atrium. From Baldwin JC, Stinson EB, Oyer PE, Jamison S, Shumway NE. The Heart. New York: McGraw-Hill, 1986. Reprinted with permission.
the International Society for Heart Transplantation, Minneapolis, Minnesota, reported a survival rate of 80% at 1 year after transplantation and of 70% at 4 years with the use of cyclosporine, excluding death in the first 30 days after the operation.2
ELECTROCARDIOGRAPHIC FINDINGS
Leaving the native sinoatrial node within the remnant right atrium, together with the sinoatrial node
L .." -~ ...r -'" ""
,_A cll .A -Aft..
,
r---A
Journal of the American Society of
Echocardiography
l' v",-, I'-/"'-' --v i-'
J\. J\. A
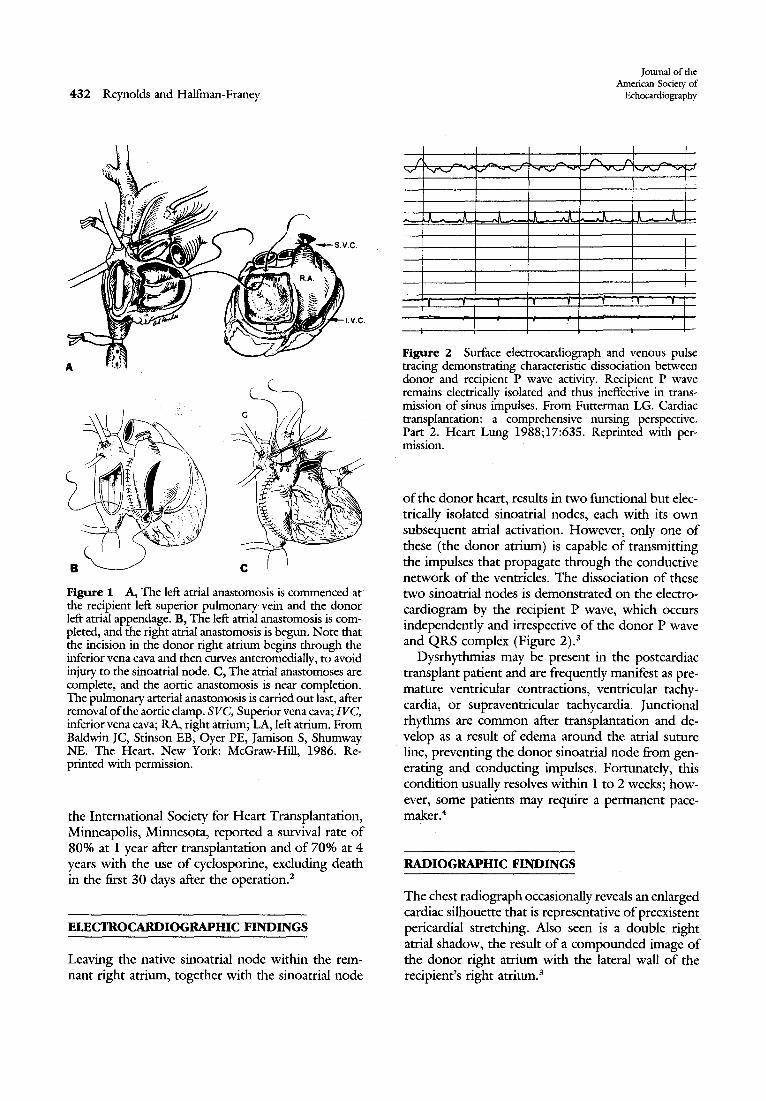
Figure 2 Surface electrocardiograph and venous pulse tracing demonstrating characteristic dissociation between donor and recipient P wave activity. Recipient P wave remains electrically isolated and thus ineffective in transmission of sinus impulses. From Futterman LG. Cardiac transplantation: a comprehensive nursing perspective. Part 2. Heart Lung 1988;17:635. Reprinted with permission.
of the donor heart, results in two functional but electrically isolated sinoatrial nodes, each with its own subsequent atrial activation. However, only one of these (the donor atrium) is capable of transmitting the impulses that propagate through the conductive network of the ventricles. The dissociation of these two sinoatrial nodes is demonstrated on the electrocardiogram by the recipient P wave, which occurs independently and irrespective of the donor P wave and QRS complex (Figure 2).3
Dysrhythmias may be present in the postcardiac transplant patient and are frequently manifest as premature ventricular contractions, ventricular tachycardia, or supraventricular tachycardia. Junctional rhythms are common after transplantation and develop as a result of edema around the atrial suture line, preventing the donor sinoatrial node from generating and conducting impulses. Fortunately, this condition usually resolves within 1 to 2 weeks; however, some patients may require a permanent pacemaker.4
RADIOGRAPHIC FINDINGS
The chest radiograph occasionally reveals an enlarged cardiac silhouette that is representative of preexistent pericardial stretching. Also seen is a double right atrial shadow, the result of a compounded image of the donor right atrium with the lateral wall of the recipient's right atrium. 3
Volume 2 Number 6 November-December 1989
NORMAL ECHOCARDIOGRAPHIC AND DOPPLER FINDINGS IN THE ORTHOTOPIC CARDIAC TRANSPLANT PATIENT
After cardiac transplant surgery, cardiac function needs to be optimized and carefully monitored. Echocardiography and cardiac Doppler are well established tools to use in the evaluation of cardiac function. 5 Because of the approach of the cardiac transplant surgery, certain echocardiographic and Doppler findings will be apparent.
Right and left atrial enlargement. Right and left atrial enlargement is a typical finding and a result of the donor-recipient atrial anastomosis. In addition to a "snowman" appearance of each atrium by twodimensional echocardiography, there is the presence of the atrial suture line. 6
Pericardial effusion. Pericardial effusions of moderate size can occur early after cardiac surgery and are usually related to hemorrhage. Pericardial effusion occurs frequently during the initial three months after heart transplantation, and in the majority of cases it decreases in size in 1 year. 7 Cardiac tamponade occurs in a small proportion of patients after transplantation. The diagnosis of idiopathic dilated cardiomyopathy yields a high probability (86%) of having pericardial effusion during the first three months after heart transplantation. Patients with no pericardial effusion during the first three months after transplantation are unlikely to subsequently develop it during a 1 year follow-up. An increasing, as opposed to stable, pericardial effusion should alert the physician to the possibility of rejection or of an immune-mediated process that may become severe enough to adversely affect ventricular function. 8
Paradoxical or flat interventricular septal motion. This paradoxical septal motion is a fairly characteristic finding in all patients undergoing open heart surgery. 5
Increased left ventricular posterior wall and septal thickness. There is increased left ventricular posterior wall thickness and septal thickness early after transplantation, which decreases over a 3-month period. Hosenpud et al.9 reported that the left ventricular posterior wall thickness descreased from 15 ± 2 to 12 ± 2 mm between studies done at 1 week and at 3 months. No clear explanation can be given for this phenomenon, but the most likely explanation for the increased wall thickness is the presence of myocardial edema caused by prolonged cold ischemia between cardiectomy and resultant ischemic injury (Figure 3).
Evaluation of heart transplant recipients 433
Figure 3 Example of two-dimensional directed M -mode echocardiograms performed 1 week, 1 month, and 3 months after heart transplantation. Note progressive decrease in both posterior wall and septal thickness over three studies. From Hosenpud JD. Serial echocardiographic findings early after heart transplantation: evidence for reversible right ventricular dysfunction and myocardial edema. J Heart Transplant 1987;6:344. Reprinted with permission.
Right ventricular cross-sectional dimension increases. The right ventricular cross-sectional dimension increases from 34 ± 6 to 39 ± 6 mm between I-week and 3-month studies. Again, there is no clear answer for this change in right ventricular size, but the possibilities include an overall increase in right ventricular volume, a change. in the orientation of the right ventricle within the chest cavity caused by adhesions, or a conformational change.9
Early right ventricular dysfunction with improvement. There is early right ventricular dysfunction, which improves by 3 months after cardiac transplantation. Hosenpud et al.9 reported that right ventricular fractional shortening increased from 13% ± 3% to 21 % ± 5% between the echo study done at 1 week and at 3 months. The cause of this early right ventricular dysfunction is unclear, although right ventricular function after routine coronary bypass or valvular surgery can be reduced, presumably because of inadequate preservation. This ischemic injury is presumably reversible.
Left ventricular ejection fraction. The left ventricular ejection fraction is lower in heart transplant patients than that in normal subjects of similar ages,
434 Reynolds and Halfman-Franey
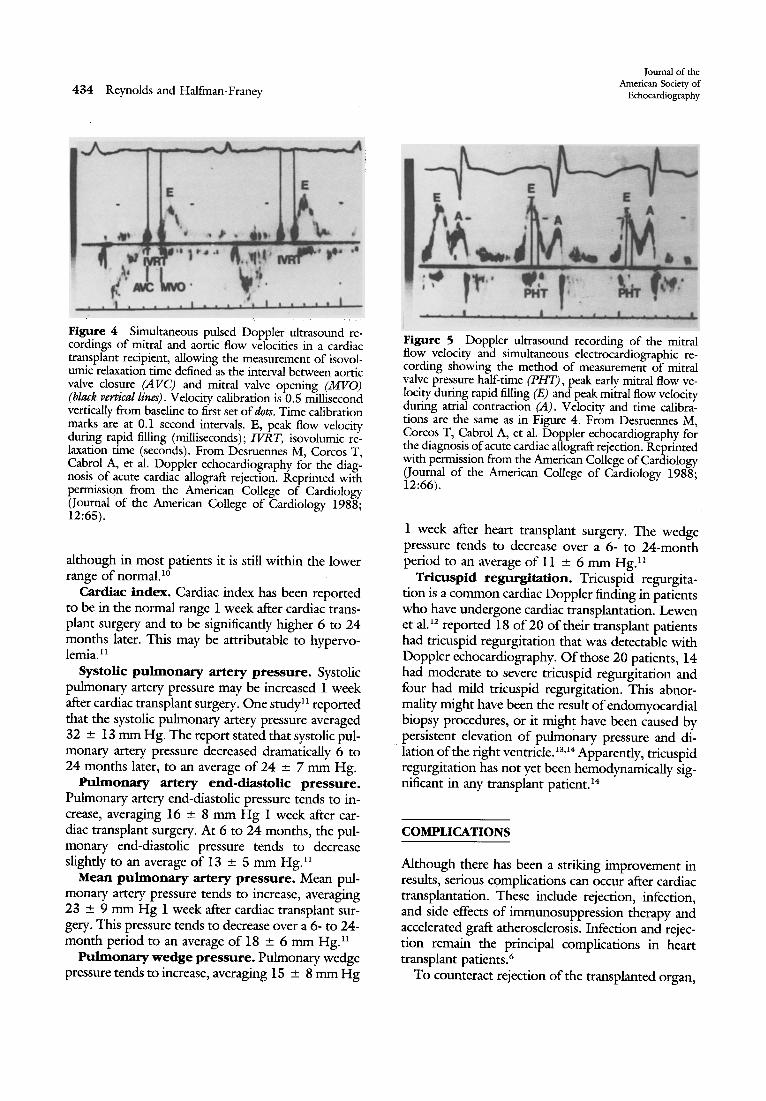
Figure 4 Simultaneous pulsed Doppler ultrasound recordings of mitral and aortic flow velocities in a cardiac transplant recipient, allowing the measurement of isovolumic relaxation time defined as the interval between aortic valve closure (A VC) and mitral valve opening (MVO) (black vertical lines) . Velocity calibration is 0.5 millisecond vertically from baseline to first set of MtS. Time calibration marks are at 0.1 second intervals. E, peak flow velocity during rapid filling (milliseconds) ; IVRT, isovolumic relaxation time (seconds) . From Desruennes M, Corcos T, Cabrol A, et al. Doppler echocardiography for the diagnosis of acute cardiac allograft rejection. Reprinted with permission from the American College of Cardiology (Journal of the American College of Cardiology 1988; 12:65).
although in most patients it is still within the lower range of normal. 10
Cardiac index. Cardiac index has been reported to be in the normal range 1 week after cardiac transplant surgery and to be significantly higher 6 to 24 months later. This may be attributable to hypervolemiaY
Systolic pulmonary artery pressure. Systolic pulmonary artery pressure may be increased 1 week after cardiac transplant surgery. One studyll reported that the systolic pulmonary artery pressure averaged 32 ± 13 mm Hg. The report stated that systolic pulmonary artery pressure decreased dramatically 6 to 24 months later, to an average of 24 ± 7 mm Hg.
Pulmonary artery end-diastolic pressure. Pulmonary artery end-diastolic pressure tends to increase, averaging 16 ± 8 mm Hg 1 week after cardiac transplant surgery. At 6 to 24 months, the pulmonary end-diastolic pressure tends to decrease slightly to an average of 13 ± 5 mm Hg. ll
Mean pulmonary artery pressure. Mean pulmonary artery pressure tends to increase, averaging 23 ± 9 mm Hg 1 week after cardiac transplant surgery. This pressure tends to decrease over a 6- to 24-month period to an average of 18 ± 6 mm Hg.ll
Pulmonary wedge pressure. Pulmonary wedge pressure tends to increase, averaging 15 ± 8 mm Hg
Journal of the American Society of
Echocardiography
Figure 5 Doppler ultrasound recording of the mitral flow velocity and simultaneous electrocardiographic recording showing the method of measurement of mitral valve pressure half-time (PHT), peak early mitral flow velocity during rapid filling (B) and peak mitral flow velocity during atrial contraction (A). Velocity and time calibrations are the same as in Figure 4. From Desruennes M, Corcos T, Cabrol A, et al. Doppler echocardiography for the diagnosis of acute cardiac allograft rejection. Reprinted with permission from the American College of Cardiology (Journal of the American College of Cardiology 1988; 12:66).
1 week after heart transplant surgery. The wedge pressure tends to decrease over a 6- to 24-month period to an average of 11 ± 6 mm HgY
Tricuspid regurgitation. Tricuspid regurgitation is a common cardiac Doppler finding in patients who have undergone cardiac transplantation. Lewen et al. 12 reported 18 of 20 of their transplant patients had tricuspid regurgitation that was detectable with Doppler echocardiography. Of those 20 patients, 14 had moderate to severe tricuspid regurgitation and four had mild tricuspid regurgitation. This abnormality might have been the result of endomyocardial biopsy procedures, or it might have been caused by persistent elevation of pulmonary pressure and di-
"lation of the right ventricle. 13,14 Apparently, tricuspid regurgitation has not yet been hemodynamically significant in any transplant patient. 14
COMPLICATIONS
Although there has been a striking improvement in results, serious complications can occur after cardiac transplantation. These include rejection, infection, and side effects of immunosuppression therapy and accelerated graft atherosclerosis. Infection and rejection remain the principal complications in heart transplant patients. 6
To counteract rejection of the transplanted organ,
Volume 2 Number 6 November·December 1989
immunosuppressive medications are used. These medications include cyclosporine, azathioprine, T cell antibodies, and corticosteroids. The primary purpose of immunosuppressive medications is to blunt the response of the patient to foreign antigens. The major drawback of any immunosuppressive regimen is the crippling of the patient's immunoresponsiveness. This significant immune disarmament predisposes the patient to infection by a multitude of pathogens.6
IUJECTION
The basis of all organ rejection is the reaction of the recipient's immune system to foreign antigens. Because the donor heart is not immunologically identical to that of the recipient, the recipient's body will mount an immunologic attack against the foreign tissue. This immunologic response is termed rejection.6 There are three "types" of rejection; hyperacute, acute and chronic. Hyperacute rejection is an immediate reaction in which damage to the coronary arteries occurs within minutes, causing thrombosis and ischemic organ failure.6 Fortunately, rigorous cytotoxic antibody screening has virtually eliminated hyperacute rejection.
Chronic rejection occurs late in the posttransplantation course. Chronic rejection is a continuous immune-mediated injury process that results in diffuse atherosclerotic changes in the coronary arteries and may necessitate retransplantation.6
Acute rejection occurs with the greatest frequency and severity during the first few weeks after transplantation. Approximately one half of the patients will have an episode of rejection within 1 month after transplant surgery, and 80% of patients will have had rejection within 3 months after transplant surgery.6 Acute rejection is the second leading cause of early postoperative death. This type of rejection is characterized by invasion of the myocardial cells (myocytes) and their surrounding vessels by lymphocytes and other immunoactive cells. Acute rejection, if left untreated, can lead to myocyte necrosis and irreversible graft destruction.6
Although the incidence and severity of rejection have been reduced with cyclosporine, the diagnosis of acute rejection remains a difficult problem. Early in the history of cardiac transplantation, acute rejection was diagnosed by careful observation of certain physiologic (increased heart rate and increased venous pressures) 15 and electrocardiographic (decreased voltage and arrhythmias) alterations.
Evaluation of heart transplant recipients 435
Figure 6 Pulsed Doppler recordings of the mitral flow in a cardiac transplant recipient before rejection (upper panel), during rejection (middle panel), and after therapy (bottom panel), showing the reversible changes in pressure half-time (PHT) associated with acute cardiac rejection. Pressure half-time decreased from 0.055 seconds before rejection to 0.025 seconds during rejection and returned to 0.050 second after therapy. Abbreviations shown in legend of Figure 4. From Desruennes M, Corcos T, Cabrol A, et al. Doppler echocardiography for the diagnosis of acute cardiac allograft rejection. Reprinted with permission from the American College of Cardiology (Journal of the American College of Cardiology 1988; 12:65).
Ultimately, signs of florid heart failure would appear, and the patient would die within 2 to 3 days. 16
Now that cyclosporine is the immunosuppressive agent of choice, clinical signs and symptoms are usually absent. A major milestone in cardiac transplantation was the development of right ventricular endomyocardial biopsy as a means to monitor rejection. 17 Because acute rejection occurs most frequently in the first few weeks after transplant surgery, en-
436 Reynolds and Halfman-Franey
ECHOfDOPPLER WORKSHEET CARDIAC TRANSPLANT
Patient Name: __________ _
Date : _____ _
Date of Transplant Surgery : ______ _
CXR f indings : EKG findings: _____ _
TRICUSPIO VALVE
Journal of the American Society of
Echocardiography
E/A ratio: _______ (Normal 1.1 to 1.5)
Deceleration time: ____ (Nonnal 160 to 240 mi lli seconds)
Systol ic re9urg1 t at i on: ___ Present
Diastolic regurgitation : __ Present
HEPATIC VEIN/SUPERIOR VENA CAVA/PUIJIlIIARY VEINS
_ __ Not present
___ Not present
Degree of left lateral rotation : S wave: em/sec
Degree of upper body elevation : _______ _
Transducer position: PLA IeS PSA I CS
Apical-4 === ICS
ECHO DATA LVIO(d) : ____ ---'cm
LVID(s) : ____ ---'cm
IVS(d) : ______ ,cm
PWLV(d) : _____ ,cm
LV~FS : ______ '
LVEF: _____ _
LV MASS : ____ ---'
RVID(d) : cm
RVWT(d) : cm
Per icardial Effusion: None Minimal Mild Moderare--__ Larg-e --
CARDIAC DOPPlER MITRAL VALVE E/A rat i o: (Normal 1.0 to 1.5)
Deceleration time: (Normal 160 to 240 ml11iseconds.)
Isovolum1c relaxation time : _____ (Normal 73 + 13}
Systolic regurgitation : ___ Present
Diastolic r egurgitation : __ Present
___ Not present
___ Not pr esent
o wave: ____ --'cm/sec
Atrial revers al : _____ cm / sec
MISCRLANEOUS Acceleration time ( ACT) : _____ (Normal >IZO milliseconds)
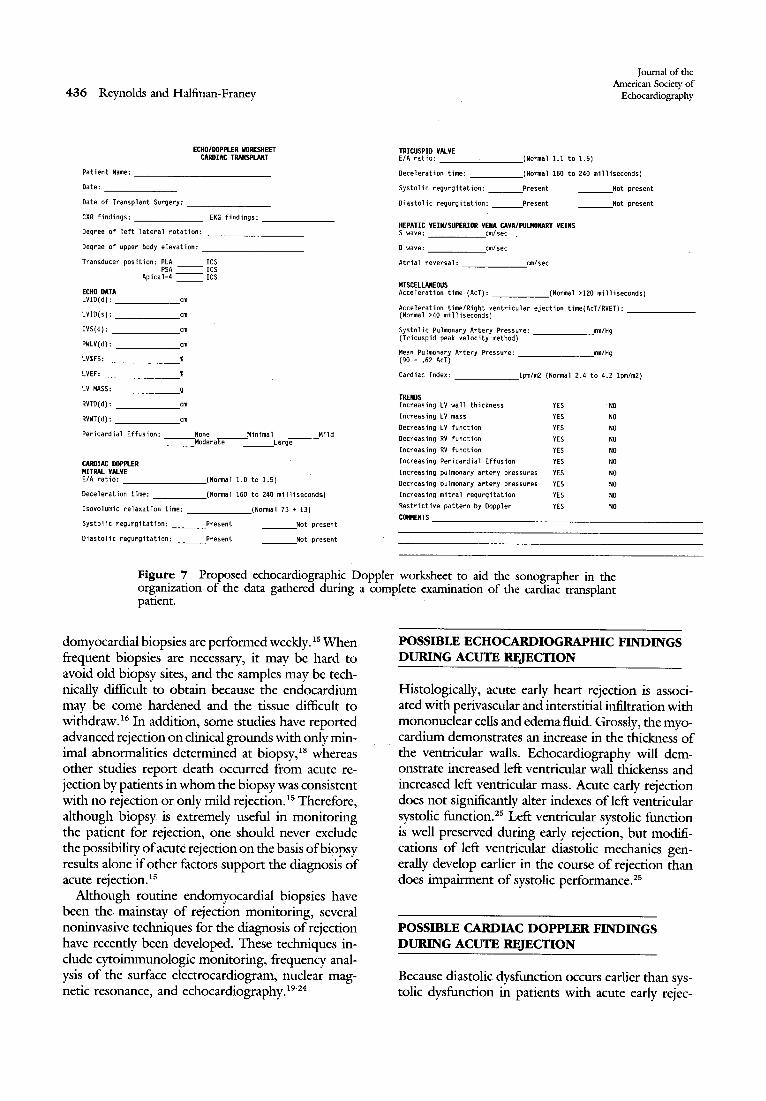
Figure 7 Proposed echocardiographic Doppler worksheet to aid the sonographer in the org.anization of the data gathered during a complete examination of the cardiac transplant patlent.
domyocardial biopsies are performed weekly. 15 When frequent biopsies are necessary, it may be hard to avoid old biopsy sites, and the samples may be technically difficult to obtain because the endocardium may be come hardened and the tissue difficult to withdraw. 16 In addition, some studies have reported advanced rejection on clmical grounds with only minimal abnormalities determined at biopsy,18 whereas other studies report death occurred from acute rejection by patients in whom the biopsy was consistent with no rejection or only mild rejection. 15 Therefore, although biopsy is extremely useful in monitoring the patient for rejection, one should never exclude the possibility of acute rejection on the basis of biopsy results alone if other factors support the diagnosis of acute rejection. 15
Although routine endomyocardial biopsies have been the mainstay of rejection monitoring, several noninvasive techniques for the diagnosis of rejection have recently been developed. These techniques include cytoimmunologic monitoring, frequency analysis of the surface electrocardiogram, nuclear magnetic resonance, and echocardiography.19.24
POSSIBLE ECHO CARDIOGRAPHIC FINDINGS DURING ACUTE RJ;JECTION
Histologically, acute early heart rejection is associated with perivascular and interstitial infiltration with mononuclear cells and edema fluid. Grossly, the myocardium demonstrates an increase in the thickness of the ventricular walls. Echocardiography will demonstrate increased left ventricular wall thickenss and increased left ventricular mass. Acute early rejection does not significantly alter indexes of left ventricular systolic function. 2s Left ventricular systolic function is well preserved during early rejection, but modifications of left ventricular diastolic mechanics generally develop earlier in the course of rejection than does impairment of systolic performance.2S
POSSIBLE CARDIAC DOPPLER FINDINGS DURING ACUTE RJ;JECTION
Because diastolic dysfunction occurs earlier than systolic dysfunction in patients with acute early rejec-
Volume 2 Number 6 November-Dt:cember 1989
tion, the evaluation of diastolic function by cardiac Doppler is important_ Desruennes et al. 26 reported that two cardiac Doppler measurements could be made to detect diastolic dysfunction during acute cardiac allograft rejection_ Isovolumic relaxation time and pressure half-time of the mitral flow velocity can be measured consistently in cardiac transplant patients_ The following may be found in patients suffering acute early rejection:
• Isovolumic relaxation time is shortened_ In the report cited, isovolumic relaxation time decreased from 0.088 ± 0.020 to 0.069 ± 0.021 seconds during acute early rejection (Figure 4).26
• A decrease in pressure half-time of the mitral valve from 0.064 ± 0.016 to 0.309 ± 0.015 seconds (Figures 5 and 6). Deceleration time may be substituted and is measured by simply carrying the E to F velocity line to the baseline and is defined as the time between this point and the time at which the maximal velocity occurred-. The two variables are simply derived from each other by the following equation: Pressure half-time = 0.29 x deceleration time. The normal deceleration time ranges from 160 to 240 milliseconds.26
Hatle et al. 27 reported similar findings in cardiac transplant patients who were experiencing acute early rejection. The group reported that a restrictive cardiac Doppler pattern was found in these patients. This pattern includes an increased mitral E/ A ratio, a decreased deceleration time, and diastolic mitral regurgitation. For the tricuspid valve, the restrictive pattern would include an increased E / A ratio, a decreased deceleration time, and diastolic tricuspid regurgitation. Hepatic veins; superior vena cava, and pulmonary vein flows are also distinctly abnormal, demonstrating a restrictive pattern with decreased systolic and increased diastolic forward filling. In addition, prominent reversal of flow is noted during atrial systole and late ventricular systole. 28
PossmLE CARDIAC DOPPLER FINDINGS IN LONG-TERM CARDIAC ALLOGRAFT RECIPIENTS
Valantine et al. 29 reported the cardiac Doppler findings in long-term (mean, 5 years) cardiac allograft recipients. Of 64 recipient patients, 10 patients were found to have evidence of restrictive-constrictive physiology. In these 10 patients, a shorter isovolumic relaxation time (65 ± 16 milliseconds), a shorter mitral pressure half-time (34 ± 7 milliseconds), and a higher mitral E / A ratio (2.1 ± 0.8) was found. Also, right ventricular pressure half-times were shorter
Evaluation of heart transplant recipients 437
(38 ± 13 milliseconds), and the tricuspid E/ A ratio was higher (2.1 ± 0.9). These Doppler findings are consistent with a restrictive-constrictive physiology and are associated with impared systolic function and may be related to rejection incidence.
SUGGESTIONS FOR ROUTINE ECHOCARDIOGRAPHIC AND DOPPLER EVALUATION OF ORTHOTOPIC CARDIAC TRANSPLANT PATIENTS
The changes caused by acute rejection are subtle findings by echo/Doppler. The sonographer should be prepared to gather a variety of data while examining a cardiac transplant patient. A careful echocardiographic and cardiac Doppler examination is imperative. Serial examinations should be carried out by the same sonographer, if at all possible, to assure consistent data. A worksheet to use in this examination is presented in Figure 7.
SUMMARY
The sonographer should have a basic understanding of the indications, surgical technique, survival rate, electrocardiographic findings, chest radiographic findings, and complications for orthotopic cardiac transplantation. The sonographer should also have a thorough understanding of the normal echocardographic and Doppler findings in these patients and the possible echocardiographic and Doppler findings during acute early rejection. This article has presented those findings in a review form to enable the sonographer to consult the information presented before the echocardiographic and cardiac Doppler examination is carried out. In addition, a sample echocardiographic and cardiac Doppler worksheet has been provided.
2. Braunwald W. Heart disease-a textbook of cardiovascular medicine. Philadelphia: WB Saunders, 1984:88-145.
3. Futtennan LG. Cardiac ttansplantation: a comprehensive nursing perspective. Part 1. Heatt Lung 1988;17:499-510.
4. Whitman GR, Hicks LE. Major nursing diagnoses following cardiac transplantation. J Cardiovasc Nurs 1988;2:1-10.
5. Feigenbaum H. Echocardiography. 4th Ed. Philadelphia: Lea and Febiger, 1986;342.
6. Futtennan LG. Cardiac transplantation: a comprehensive nursing perspective. Part 2. Heart Lung 1988;17:631-9.
438 Reynolds and Halfman-Franey
7. Vendenberg B, Mohany P, Craddock K, et al. Clinical significance of pericardial effusion after heart transplantation. J Heart Transplant 1988;7:128-34.
8. Valantine H, Hunt S, Gibbons R, Billingham M, Stinson E, Popp R. Increasing pericardial effusion in cardiac transplant recipients. Circulation 1989;79:603-9.
9. Hosenpud J, Norman D, Cobanoglu M, Flaten H, Conner R, Start A. Serial echocardiographic findings early after heart transplantation: evidence for reversible right ventricular dysfunction and myocardial edema. J Heart Transplant 1987; 6:343-7.
10. Verani M, George S, Leon C, et al. Systolic and diastolic ventricular performance at rest and during exercise in heart transplant recipients. J Heart Transplant 1988;7: 145-51.
11. Corcos T, Tamburino C, Leger P, et al. Early and late hemodynamic evaluation after cardiac transplantation: a study of 28 cases. J Am Coll Cardiol 1988;11:264-9.
12. Lewen M, Bryg R, Miller L, Williams G, Labovitz A. Tricuspid regurgitation by Doppler echocardiography after orthotopic cardiac transplantation. Am J Cardiol 1987;59: 1371-4.
13. Lewen MK, Bryg RJ, Miller LW, et aI. The development of tricuspid regurgitation after orthotopic cardiac transplantation [Abstract]. J Am Coll CardioI1986;7(suppl):9A.
14. Massin EK. Medical management of the transplant patient: long-term follow-up. Texas Heart Inst J 1987;14:262-7.
15. Murdock DK, Collins EG, Lawless CE, et al. Rejection of the transplanted heart. Heart Lung 1987;16:237-45.
16. Schnee M. Early complications of heart transplantation. Texas Heart Inst J 1987;14:257-61.
17. Caves PK, Stinson EB, Billingham ME, et al. Diagnosis of human cardiac" allograft rejection by serial cardiac biopsy. J Thorac Cardiovasc Surg 1973;66:461-6.
18. Stevenson LW, Lewis W, MacAlpin RN, et al. Acute reversible cardiogenic shock: immunomediated with mild histologic change. Am Heart J 1986;111:611.
19. Hall TS, Baumgartner WA, Borkon AM, et al. Diagnosis of
Journal of the American Society of
Echocardiography
acute cardiac rejection utilizing phosphorus nuclear magnetic resonance, antimyosin monoclonal antibody, 2-D echocardiography and endocardial biopsy. Heart Transplant 1985; 4:595.
20. Hammer C, Riechenspurner H, Ertel W, et al. Cytologial and immunologic monitoring of cyclosporine-treated human heart recipients. Heart Transplant 1984;3:228-32.
21. Dawkins KD, Oldershaw PJ, Billingham ME, et al. Changes in diastolic function as a non-invasive marker of cardiac allograft rejection. Heart Transplant 1985;4:286-92.
22. Lechat P, Eugene M, Hadjiisky P, et al. Nuclear magnetic resonance and detection of rejection in experimental heart transplantation. Heart Transplant 1985;4:593.
23. Reichenspurner H, Haberl R, Angermann C, et al. New methods for non-invasive monitoring of rejection after heart transplantation. Tex Heart Inst J 1988;15:7-11.
24. Chandrasebaran K, Bansal RC, GreenleafJF, et al. Early recognition of heart transplant rejection by backscatter analysis from serial 2D ECHOs in a heterotopic transplant model. J Heart Transplant 1987;6:1-7.
25 . Paulsen W, Magid N, Sagar K, et al. Left ventricular function of heart allografts during acute rejection: an echocardiographic assessment. Heart Transplant 1985;4:525-9.
26. Desruennes M, Corcos T, Cabrol A, et al. Doppler echocardiography for the diagnosis of acute cardiac allograft rejection. J Am Coll Cardiol 1988;12:63-70.
27. Hatle L, Appleton C, Popp R. Differentiation of constrictive pericarditis and restrictive cardiomyopathy by Doppler echocardiography. Circulation 1989;79:357-70.
28. Klein AL, Orr JK, Miller FA, Seward JB, Tajik JA. Twodimensional and Doppler echocardiographic assessment of infiltrative cardiomyopathy. J AM Soc ECHO 1988;1:48-59.
29. Valantine H, Appleton C, Hatle L, et al. A hemodynamic and Doppler echocardiographic study of ventricular function in long-term cardiac allograft recipient. Circulation 1989; 79:66-75.