The Roll-Out of Primary Care Teams in 2011 Practice Managers February 19 Practice Managers February 19 th th 2011 2011 Helen Deely HSE (Regional Helen Deely HSE (Regional Specialist in Primary Care Dublin Specialist in Primary Care Dublin Mid-Leinster) Mid-Leinster)
Transcript
The Roll-Out of Primary Care Teams in 2011Practice Managers February 19Practice Managers February 19thth
20112011
Helen Deely HSE (Regional Helen Deely HSE (Regional Specialist in Primary Care Dublin Specialist in Primary Care Dublin
Mid-Leinster)Mid-Leinster)
Primary Care Health Strategy 2001 Primary Care Strategy Primary Care - 90 – 95% of
all health and social needs Secondary Care – complex
and special needs Central focus of the health
system Team based approach to
health service provision. Shift appropriate activity
from hospitals
GP
PHN Phy
OT SW
Information and Service Flow in the past- Non Integrated Local Service
Information and Service Flow now - Integrated Primary Care Team
Direct Referral
Referral Service Feedback
Direct Referral and Feedback
PHN Phy
OT
GP
SW
Why develop a Primary Care Team?
Formation of PCT’s guided by the following requirements:
To maximise coverage for 100% of population To ensure ease of access to services and
simplify communication and referral processes To support epidemiological population health
monitoring, especially health inequalities To facilitate community involvement in need
assessment To support evidence based decision making To support future management and
governance arrangements within HSE. To facilitate team working amongst health
professionals including GPs
Who’s involved in Primary Care?
Establishing the Team GP Practice
nurse Practice
staff
Primary Care Team
Reconfigure existing staff:PHNRGN
Clerical Admin
Additional staff:Physiotherapy
Occupational TherapySocial Worker
IntegratedServices
PCT ‘A’
• SupportGroups
• Voluntary
PCT ‘E’ PCT ‘B’
PCT ‘C’PCT ‘D’
• Local • PrivateProviders
• Area
MultiAgencies
Hospitals
• Specialist
• Orthodontics
• Other• Home
Help
• Counselling
• Psychiatry • Dietetics
• AlternativeCare
• Child Protection
Network Services & Linkages
Each Primary Care Team is planned to be part of a wider network known as the Health & Social Care Network.
Health & Social Care Network Services Audiology Services Psychology / Counselling Services Podiatry Services Community Health Medical Services (Area Medical Officers) Community Welfare Services Dental Services Dietetic Services Ophthalmology Services Environmental Health Services Civil Registration Services Community Development Services Carers Services
Where we came from? Survey undertaken (August 2008) involving GPs and Public
Health Nurses who were not in Primary Care Teams determined that: 20% of GPs and PHN never had face-to-face contact 29% of GPs indicated that they did not know the PHNs
by name 97% of GPs and 81% of PHNs had no working email
address for each other 56% of GPs and 77% of PHNs did not have each others
mobile phone number Although 45% of GPs and PHNs were in weekly phone
contact, as many 1 in 25 (4%) reported contact on less than an annual basis. PCTs provide multidisciplinary care, which was previously provided in a unidisciplinary manner prior to the establishment of Teams.
Aim of the Primary Care TeamTo provide Primary Care Services that are: Accessible
Anyone who lives in the team geographic area Service users can self-refer
High Quality: Care planning Service planning Continuous education
Meet the needs of the local population Liaison with local community Needs assessment Once off needs & chronic complex needs
What do PCTs do? First point of contact
Defined set of core community-based services
individual care plans for patients with chronic illness or other complex needs.
Link with other community-based professionals such as mental health.
Integrate with acute hospital services - reduce hospital admissions, early discharge of patients and chronic disease management programmes.
Clinical Team meetings Central to Team functioning Feedback from GPs highly positive Business like fashion – agendas, list of
patients etc circulated in advance Leadership within Team required – TDOs
facilitated work to date. Acknowledged there is a myriad of contacts
outside of CTMs. Supporting systems required – Admin and
governance Variances apparent – need to identify reasons
and solutions
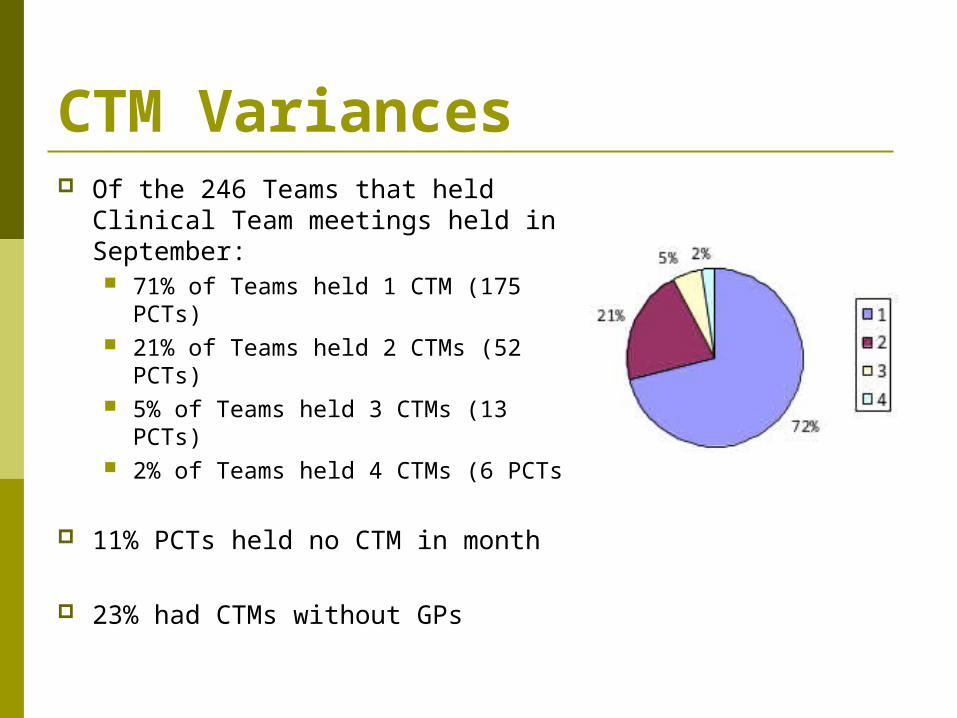
CTM Variances Of the 246 Teams that held Clinical
Team meetings held in September: 71% of Teams held 1 CTM (175
PCTs) 21% of Teams held 2 CTMs (52
PCTs) 5% of Teams held 3 CTMs (13 PCTs) 2% of Teams held 4 CTMs (6 PCTs)
11% PCTs held no CTM in month
23% had CTMs without GPs
PCT Challenges Change from traditional linear working
to multi-disciplinary Different roles & personality
differences Contractual differences Leadership issues For Teams to work well they must be
Challenges cont… CHANGE!! Becoming a team Recruitment & non replacement of staff Capacity: cradle to grave; health & social services Boundaries Accommodation Clinical audit : patient pathways
Lack of systems to record how much we do/how well we do it/ how much it costs us to do it
IT: no single patient record, no secure email
GP Engagement Locally through the TDO Estates for PPPs Primary Care Support Doctors – local &
national forums Exploration of CME Credits for education
element of CTMs (not agreed). Joint initiatives to engage GPs Business like approach to Mtgs – prove the
benefits.
Example of PCT initiatives
Dietitian Clinic & shared Care diabetes Smoking Cessation Falls Prevention Groups Incredible years Antenatal clinics Reduction in outpatient appointments
physio/dietetics clinics, etc. Joint discharge planning between acute &
Primary Care
Pharmacy engagement
Infrastructure PPP progress has been slower than anticipated in
2010 due to the funding difficulties by developers HSE Board approved 210 locations under the PPP
initiative. HSE has signed 12 lease agreements, 23
Agreements to Lease and 82 letters of intent.
12 locations have been completed within the past 12 months accommodating 17 PCTs
A further 42 have been identified to be completed in 2011
By 2013 - 115 PCCs operational supported by 160 PCTs
Integrated Working with Acute
Essential that Acute and Primary Care Services are a seamless service –
PCT first point of contact with patient Acute Hospital Service Post Admission
Chronic Disease Management Shift from episodic acute hospital care integrated care focused on primary care.
Hospital Integration Discharge planning Shared care – diabetes, asthma Current hospital care to be provided in the community e.g. cancer
initiative, minor surgery Access to Diagnostics OPD direct access to hospital
Primary Care Team Development
Target to have 527 Teams in place by end of 2011
Plan to create 134 Health and
Social Care Networks
Steps to Primary Care Development… Step 1 – Develop PCTs Foundations
(complete by end 2011) Step 2 – Strengthen functionality of Teams
Identify and address staffing deficits Strengthen team working though training or
otherwise Implement standard business processes Complete health needs assessment &
strengthen community participation Hold regular CTMs with log of care plans
Steps to PC Development…(cont’d) Step 3 – Development of Network Services
Implementation of governance and management structures.
Alignment of specialist and care group services. Implementation of general principles of referral and
shared care arrangements with secondary care, care group and specialist services.
Step 4 - Develop health promotion and proactive services within the team Roll out of Chronic Disease Management Falls prevention programmes Locally targeted programmes
Supporting Developments Management and Clinical Governance ICT Chronic Disease Management Community Needs Assessments – guidance doc
nearing completion Reconfiguration of Admin staff Plan Resource Pack for PCTs DVD Community Engagement Guidelines Pharmaceutical Engagement Guidelines (draft)
Primary Care Performance Activity
350 Teams in operation at end of December 2010 (89% of 2010 target)
Additional 31 Teams holding multi-disciplinary clinical meetings between HSE staff without GPs
2,615 Staff assigned to functioning Teams
Over 1,309 GPs participating on Teams
Primary Care Performance Activity & Performance Indicators cont… ICT Supports – Hardware requirements, work with GPIT
group to progress secure e-mail
Enhancement of Primary Care Services – Community Intervention Teams IV Therapy Falls Prevention CMHTs Smoking cessation Breast feeding training for PHNs
Primary Care Performance Activity & Performance Indicators cont… Cancer Services
training for practice nurses in cancer prevention care, community nurse education programme further developed, information/training sessions for GPs and electronic referral cancer systems developed within the GP
software packages
Chronic Disease Management (QCCD) – Commencement of Clinical Leadership for primary care & Guidelines for disease management for 7 priority programmes pertinent to Primary Care – Stroke Heart Failure Asthma Diabetes COPD Dermatology/Rheumatology Care of the Elderly
Chronic Disease Management in Primary Care Most of the care of patients with chronic conditions takes
places within the primary healthcare sector. This includes: Diagnosis, treatment and rehabilitation of patients with chronic
conditions; Early detection, assessment and follow-up comprehensive
medical treatment Preventive activities including smoking cessation, dietary
advise and support of patients’ self care.
Estimated 15-16 million consultations in general practice while approximately 1.9 million consultations take place in out-patient departments each year.
Why focus on Chronic Disease 80% of GP consultations 60% of hospital bed days 2/3rds of emergency medical admissions to hospitals. 8 of the top 11 causes of hospital admissions are due to
chronic diseases 5% of inpatients with a long-term condition account for 42%
of all acute bed days. CDMP - 50% reduction in unplanned hospital admissions as
well as a 50% reduction in bed day rates
Falls Prevention 34,000 treated per year due
to falls = 703,000 bed days Hip fractures – €35m per year 2 out of 3 over 65 who
fracture hip never return home
Falls Prevention PCT delivered >25 PCT’s delivering Fall
Programmes Programmes reduce falls
by 15 – 30 % Potential savings: €17.5 m
Diabetes 10% total healthcare
budget -700m per year
Complications of DM cost €696m per year
4.1% reduction in Stroke/ MI in a 3 year structured DM programme
Heart FailureA structured shared care model
between Primary Care/ Hospital would prevent:
> 4,000 hospitalisations per year
free up 50,000 bed days.
Equivalent to building a small to medium size hospital at a cost of €27m.
Asthma 5,000 admissions
per annum
Structured Primary Care Model (Finland)
54% reduction in hospital bed days
90% reduction in deaths
COPD
Estimated by 2020 COPD will be third leading cause of death worldwide.
2003 - COPD caused 4.9% of all deaths in the UK At least 10% of emergency admissions to hospital are COPD
related Average hospital stay of nine days per exacerbation, three
to four times a year Integrated care intevertion including education, co-
ordination among levels of care and improved accessibility, reduced hospital readmissions in COPD after 1 year.
Stroke Rates in Irish Population
Stroke: 1.93/1,000 pop. (NDPSS)/ TIA: 0.62/1,000 pop. (NDPSS) 10,817 new stroke/TIA nationally per year- 1 every hour
Stroke/TIA Hospital Bed Use 9,570 hospital admissions/yr (2000-06, HIPE)
Stroke/TIA Combined: 5% of all hospital bed days (HIPE, 2000-06)
Estimated 2009 Total Direct Costs - €405m
Atrial fibrillation Atrial fibrillation (irregular heartbeat) in 10-20% of over-70s Extensive brain injury disability, NH care common 30% of all stroke (NDPSS, INASC) Easy and inexpensive to detect (pulse, ECG) 70% preventable (blood-thinning anticoagulation) Only 25% of known AF treated (NDPSS) 600 missed opportunities - potentially-preventable severe strokes in 2006
Benefits of Primary Care TeamImproved service to the client Safer more co-ordinated care Clearly identifiable for patients Named Nurses, physiotherapists, occupational therapists, social
worker on the team, relationship building Shorter waiting times for Occupational Therapy, Physiotherapy,
Social Work Range of services provided increased Increased clinical contacts with clinical rooms Single referral form/self referral More focus on:
health promotion disease prevention
Improved communication and information sharing Communication with other agencies e.g. hospitals, voluntary
groups and community groupsBenefits to staff: high staff retention levels
Benefits of PCTs cont… Local personal relationships with clients/patients Community-based services near patients’ home Better use of the clinical skills of the various professionals; Identify and tackle critical local health issues e.g. suicide prevention; Less duplication and fragmentation in the health system due to better
communication structures; Decrease hospital attendance through the delivery of chronic disease
management programmes Transfer services from acute hospitals to the community e.g. diagnostics,
minor surgery, wound management, IV therapy in the community; Facilitate early discharge through the delivery of CITs, pre-hospital and
discharge planning, timely access to appropriate multi-disciplinary services in the PCTs;
Support patients in the community e.g. falls prevention programme; Offer multidisciplinary health promotion initiatives De-stigmatise the provision of Mental Health services in the community In complex cases a Key Worker navigates health system on behalf of the
patient
Feedback on Development to date….. Lack of Resources: Those teams without
premises feel very strongly about this position and feel they will not work as a “team” until this is rectified.
The moratorium is leaving teams without resources and this has been identified as a key risk in a number of teams.
Lack of basic IT equipment coupled with no administrative support is impinging on team effectiveness.
Next Steps… Continue roll out of PCTs
Staff reconfiguration Engagement with GPs
Strengthen exiting Primary Care Teams Implementation of governance arrangements Strengthen team working though training or otherwise Implement standard business processes Complete health needs assessment
Primary Care Centre Developments Development of Performance Metrics PCT Needs Assessments Progress Engagement with Acute Develop Health and Social Care Networks Roll out of Chronic Disease Management Programmes Updated and clear information needs to be communicated to the
public, PCT members, and HSE literature and websites.
We know
Patients feel they get a better service from a multi-disciplinary team
Staff are happier working in well functioning teams
Happier staff deliver better services Countries with advanced health systems are