The Schachar Lens: A Two-Year Follow-Up Ronald A. Schachar, MD, PHD Denison, Texas and Les Schachar, MD BY INVITATION Gainesville, Texas The Schachar lens,' a two-loop, two-pin, horizontally mounted iris-clip intraocular lens has been used for the past two years in over 200 patients with excellent success_ It was introduced to the ophthalmological community at the American Academy of Ophthalmology and Otolaryngology in 1976_ 1 The implant has a 5-mm optical zone of polymethylmethacrylate, with two prolene loops and two prolene pins (Fig 1). The implant may be used with intracap- sular or extracapsular surgery and has the major advantage of two-point fixation, al- lowing wide pupillary dilatation without fear of subluxation or dislocation_ METHODS We prefer general anesthesia, although retrobulbar anesthesia may be performed. Our preoperative regimen consists of instil- lation of tropic amide 1%, 1 drop, and Neo- sporin (polymyxin B-neomycin sulfate-gram- icidin), 1 drop, and intramuscular injection of ampicillin, 250 mg, or tetracycline, 250 mg, one hour prior to surgery without any osmotic agents or carbonic anhydrase in- Submitted for publication Jan 8, 1979. From Texoma Eye Institute, Denison, Texas. Presented at tbe poster session of the 1978 Meeting of the American Academy of Ophthalmology, Kansas City, MO, Oct 22·2fi. Reprint requests to Texoma Eye Institute, PO Box 145, Denison, TX 75020 <Dr Ronald A. Schacharl. 'Available from Iolab and Medical Workshop U.S.A., Inc. tAvailable from V. Mueller, fifi()() Touhy Ave, Chicago, II,. Fig l.-Schachar lens, a two-loop, two-pin hori- zontally mounted iris-clip lens. Fig 2.-Schachar blepharostats are attached to rubber bands that are clamped to the drape with mosquito clamps, which in turn are held in posi- tion by towel clips. 1631
Transcript
The Schachar Lens: A Two-Year Follow-Up
Ronald A. Schachar, MD, PHD Denison, Texas
and
Les Schachar, MD BY INVITATION
Gainesville, Texas
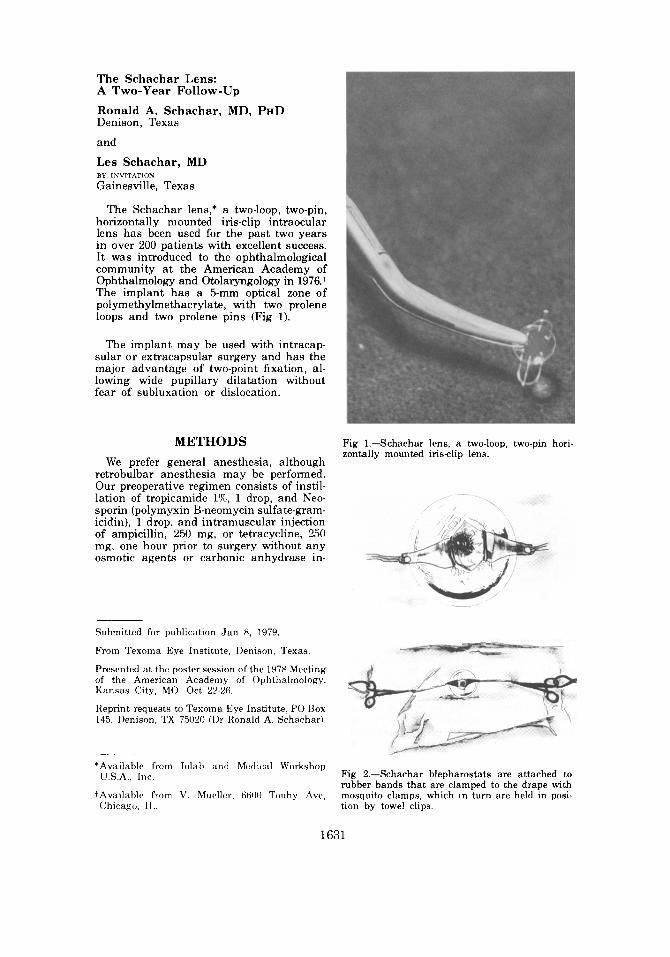
The Schachar lens,' a two-loop, two-pin, horizontally mounted iris-clip intraocular lens has been used for the past two years in over 200 patients with excellent success_ It was introduced to the ophthalmological community at the American Academy of Ophthalmology and Otolaryngology in 1976_ 1
The implant has a 5-mm optical zone of polymethylmethacrylate, with two prolene loops and two prolene pins (Fig 1).
The implant may be used with intracapsular or extracapsular surgery and has the major advantage of two-point fixation, allowing wide pupillary dilatation without fear of subluxation or dislocation_
METHODS
We prefer general anesthesia, although retrobulbar anesthesia may be performed. Our preoperative regimen consists of instillation of tropic amide 1%, 1 drop, and Neosporin (polymyxin B-neomycin sulfate-gramicidin), 1 drop, and intramuscular injection of ampicillin, 250 mg, or tetracycline, 250 mg, one hour prior to surgery without any osmotic agents or carbonic anhydrase in-
Submitted for publication Jan 8, 1979.
From Texoma Eye Institute, Denison, Texas.
Presented at tbe poster session of the 1978 Meeting of the American Academy of Ophthalmology, Kansas City, MO, Oct 22·2fi.
Reprint requests to Texoma Eye Institute, PO Box 145, Denison, TX 75020 <Dr Ronald A. Schacharl.
'Available from Iolab and Medical Workshop U.S.A., Inc.
tAvailable from V. Mueller, fifi()() Touhy Ave, Chicago, II,.
Fig l.-Schachar lens, a two-loop, two-pin horizontally mounted iris-clip lens.
Fig 2.-Schachar blepharostats are attached to rubber bands that are clamped to the drape with mosquito clamps, which in turn are held in position by towel clips.
1631
1632 SCHACHAR AND SCHACHAR OPHTH AAO
Fig 3.-A. Mid-iris iridotomy is made at 3:00, just outside the co\larette, using a Vannas scissors . B. A peripheral iridotomy is made at 1:00. C. Another mid-iris iridotomy is made a t 9:00, just outside the co\larette, using a Vannas scissors. D. The mid-iris iridotomies with the looped 8-0 black sutures in place.
hibitors. Eyelashes are not cut because the Schachar blepharostatst (Fig 2) keep them out of the operating field . The blepharostats are held in place by means of a rubber band, which is clamped to the drape with a mosquito clamp. The mosquito clamp is held in position with a towel clip. The advantages of these blepharostats are that the eyelashes do not have to be cut, the tension on the blepharostats can be easily adjusted by adjusting the rubber bands, and the blepharostats lift the eyelids up and away from the globe without placing any pressure on the globe during surgery. We do not use a superior rectus bridle suture because during general anesthesia the eye remains in the
primary position. Although implant surgery can be performed with loupes, a microscope is preferred with zoom magnification in order to allow for alteration of magnification during the procedure and excellent visualization .
A 1800 corneoscleral incision is performed, using either a limbal- or fornix-based flap or a clear corneal incision. We prefer a clear corneal incision. A keratome is used to enter the anterior chamber through clear cornea at 12 o'clock while fixating the eye with a corneoscleral Colebri forceps at 2 o'clock. A straight corneoscleral scissors with uneven blades is used to complete the corneal sec-
VOLUME 86 SEPTEMBER 1979 SCHACHAR LENS 1633
F
Fig 4.-A. The Schachar implant is held with a Shepard or Schachar intraocular lens forceps by the haptic and the 3:00 loop is placed posterior to the iris . B. The implant is shifted toward 3:00 and with the aid of a closed McPherson microscopic angled tying forceps , the 9:00 loop is placed posterior to the iris. C. Both loops are posterior to the iris in the horizontal meridian. D. The 3:00 pin is bent downward through the 3:00 mid-iris iridotomy and clips the 3:00 loop posterior to the iris. During clipping the implant is held by the haptic steadily with the implantation forceps. E. The 9:00 pin is similarly bent downward through the 9:00 mid-iris iridotomy and clips the 9:00 loop posterior to the iris. F. The implant in place.
tion. This prevents any iris damage since the blade, which is placed in the anterior chamber, is blunt. We bevel the corneal incision by holding the corneoscleral scissors at approximately 45°. The clear corneal incision is made slightly irregular so that the cornea can be easily reapproximated. Beveling the wound allows for easy maintenance of a deep anterior chamber while suturing the wound closed.
Once the corneoscleral incision is completed, the eye should appear soft, with the lens-iris diaphragm appearing backward. If
TABLE 1
REASONS FOR VISUAL ACUITY LEss THAN 20/40
Senile macular disciform degeneration
Cystoid macular edema Optic atrophy Detachment of Descemet's
membrane
16 (7.4%)
5 (2.3%)
2 (0.9%) 1 (0.4%)
the lens-iris diaphragm appears forward, the blepharostats should be adjusted to ensure that they are not exerting pressure on the globe. This is easily done by moving the eye drape and thus adjusting the tension on the rubber bands.
Eight-O black silk, looped sutures are placed through the corneoscleral wound at 10:30 and at 1:30, and a suture is placed just through the cornea at 12:00 to serve for corneal retraction. Mid-iris iridotomies are then performed at 3:00 and 9:00 prior to the lens extraction. Iridotomies are made just outside the collarette. The iris is not grasped with a forceps. A Vannas scissors is used to cut the iris just outside the collarette and to spread the opening apart (Fig 3). If iris bleeding occurs during iridotomy, the iris is further cut in that position and the bleeding will stop. If the iris vessel is partially cut, it will bleed; if it is completely cut, the blood vessel will constrict and stop bleeding. A peripheral iridotomy or iridectomy is performed at 11:00 or LOO, or the peripheral iridectomy may be delayed until after implant insertion.
TABLE 2
COMPLICATIONS
Corneal edema secondary· to 1 detachment of Descemet's membrane
Fig 5.-A. Wide pupillary dilatation with the Schachar implant in place. B. The Schachar implant takes most advantage of the radial structure of the iris for its fixation.
The lens is then extracted intracapsularly or extracapsularly in the usual fashion. We prefer intracapsular extraction using a Douvas self-iris-retracting cryoprobe. The implant is held by a Shepard intraocular lens forceps or the Schachar intraocular lens forceps around the optical portion. The assistant retracts the cornea, using the previously placed retraction suture. If the surgeon is right-handed, the implant is held by the intraocular lens forceps in the left hand. In the right hand is held a closed-angle microscopic McPherson tying forceps. The 3 o'clock loop of the Schachar implant is placed posterior to the iris; then by shifting the lens toward 3:00, the 9 o'clock loop is placed behind the iris with the aid of the closed-angle microscopic McPherson tying forceps (Fig 4). The pin anterior to the 3:00 loop is bent downward through the iridotomy using the closed-angle microscopic McPherson tying forceps and engages the 3:00 loop behind the iris, thus locking the pin, which is passing through the iris iridotomy, behind the loop. This is similarly performed on the other side. During this procedure the cornea is being held up and away from the implant. The implant is held level and steady during clipping. The implant is slightly lifted so that it is above the vitreous face. The loop should be centered around the iridotomy so
that the pins will easily pass through the iridotomy and engage the posterior loops. In order to confirm that the pin is locked behind the loop, the implant is held steadily with the intraocular forceps and the pin is gently lifted upward with the McPherson microscopic angled ties. This will result in the loop raising up against the posterior iris, which is easily visible, and insures proper clipping. Rarely, if the pin is not clipped, the pin will lift up against the posterior iris without raising the loop, signifying that the pin is not clipped. The pin is bent downward again and locking of the pin is reconfirmed. Once both sides are clipped, the cornea is released and the corneoscleral wound is closed with the previously placed 8-0 black silk sutures. Air is placed in the anterior chamber, using a tuberculin syringe attached to a Millipore filter on a 27- or 30-gauge needle, keeping the implant far from the corneal endothelium during wound closure. The 12:00 corneal retraction suture is removed, and the corneal scleral wound is closed with a running 10-0 Prolene suture. The loose strand of the initial knot is left about 2 mm long and is placed under the turns of the running sutures so that the patient will not feel the cut end postoperatively. Every fourth suture is locked. The 8-0 black silk preplaced sutures are removed when the
VOLU ME 86 SEPTEMBER 1979 SCHACHAR LENS 1635
running 10-0 Prolene approaches them. The anterior chamber is constantly maintained with air during suturing. The ends of the last knot are cut short and the knot is buried. The 10-0 Prolene suture offers a tight wound closure. The eye is then dilated with 1% tropicamide (Mydriacyl) and 100/0 phenylephrine (Neo-Synephrine). Neosporin is placed in the eye and the eye is patched and shielded. Note that no miotic agent is needed either intraoperatively or postoperatively. Two-point iris fixation of the Schachar lens allows for immediate pupillary dilatation.
Our routine postoperative regimen consists of maintaining pupillary dilatation with either Mydriacyl 1% and Neo-Synephrine 10% or atropine 1% and applying an antibiotic-steroid ointment daily for one week, which is then followed by topical fluorometholone, 1 drop qid for six to eight weeks postoperatively.
RESULTS Over a two-year period, 216 cases with a minimum of three months follow-up were
treated. Implants with Prolene loops and pins were used in 186, while the other 30 had titanium loops and Supramid pins. The patients ranged in age from 54 to 98 years. Intracapsular surgery was performed in 100% of cases. There were 14 bilateral implantations and one secondary implantation. The visual acuity was 20/40 or better in 89% of cases. The reasons for visual acuity less than 20/ 40 are given in Table 1. Complications are listed in Table 2.
SUMMARY In the past two years, 216 implantations
have been performed with a minimum of a three-month follow-up; visual acuity was better than 20/ 40 in 89% of cases.