3
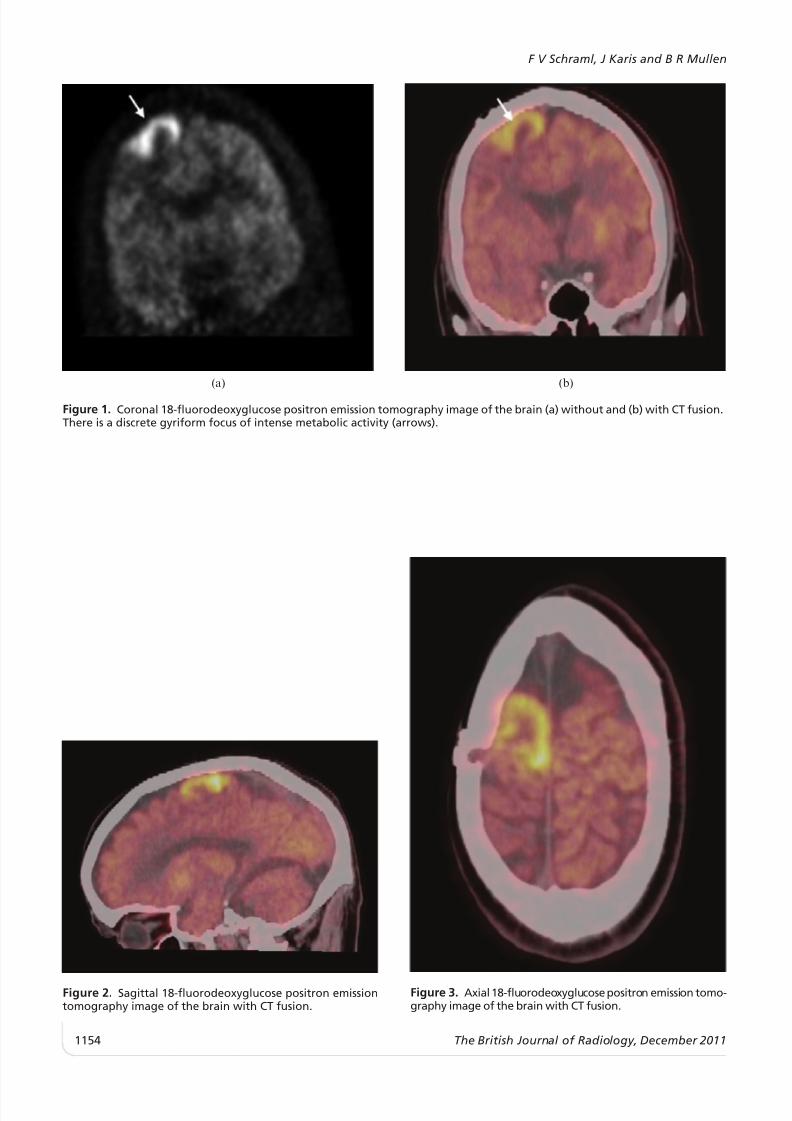
CASE OF THE MONTH The uncontrollable shaking arm F V SCHRAML, MD, J KARIS, MD and B R MULLEN, MD Department of Radiology, Saint Joseph’s Hospital and Medical Center/The Barrow Neurologic Institute, Phoenix, Arizona, USA Received 26 January 2011 Accepted 1 February 2011 DOI: 10.1259/bjr/31 650853 ’ 2011 The British Institute of Radiology Case report A 48 -year- ol d ma le pr es ente d to the emer ge ncy dep art men t wit h the chi ef compla int of intermitt ent unc ont rol lab le sha king of his lef t arm. He repor ted havi ng ha d a brai n tumour rese ct ed from the right frontoparietal region of his brain approximately 5 years earlier. He was admitt ed to hos pit al and underwen t MRI scan of his brain. The MRI demonstrated a right frontoparietal region tumour, which was proven to be a partially resected ( i.e. residual) low-grade astrocytoma. The residual tumour was resected without any apparent motor deficit . Althou gh there was some abatement of seizure activi ty, foc al mot or seizures of the pat ien t’s left upper extremi ty did not complete ly resol ve, des- pit e ant iconvu lsa nt med ica tio n at the rapeutic levels. Brain pos itr on emi ssion tomography (PET)/CT with 18-fl uorod eoxy gluco se (FDG) was perf ormed. Sele cted tomogr aphi c slices wi th and wi thout CT fusion ar e shown in Figures 1, 2 and 3. What is the salient finding? What is the most likely explanation for this pattern of uptake? Discussion ‘‘Inte ricta l’’ imagi ng was the intended proc edur e to demonstrate typical decreased metabolism correspond- ing to the seizure focus in a quiescent state [1, 2]. How- ever, the patient’s left arm was in status epilepticus during radiotracer injection and throughout the 50-min uptake pe ri od. The PET sc an, wi th and wi thout CT fusi on (Figures 1, 2 and 3), revealed a discrete gyriform focus of int ense me taboli c act ivi ty (ar rows in Fig ure 1) in the ant er ior mar gin of the rig ht fro nta l resect ion cav ity , which involved the (somewhat distorted) primary motor cortex. This is the region corresponding to the patient’s con tra lat er al mot ori c activity and the pre sumed ict al focus [3]. As a result of the relatively prolonged uptake period of FDG, FDG PET epilepsy imaging is typically limited to interictal seizure evaluations in which the seizure focus presen ts as an area of relative photope nia, while the 99 Tc m cerebral perfusion tracers, 99 Tc m hexamethylpropylenea- min e oxi me and 99 Tc m ethy l cyst eina te dime r, are typi call y used for ‘‘ictal’’ imaging with injection at the onset of the seizure and visualisation of focally increased uptake indicating the seizure focus [1, 2]. It is not unexpected that FDG would accumulate in seizure foci if the dura- tion of the seizure is sufficiently prolonged ( e.g. status epilepticus) and there are case reports to testify to this phenomen on [4]. As opp ose d to photope nia , which is typi cally asso - ci ate d wit h seiz ur e foci in FDG PET brain imaging , increased uptake is the norm in many FDG PET brain tumour eva lua tion s [5]. Mor eover, the degree of FDG avidity has been useful in assessing brain tumour grade; the degree of uptake serves as a marker of the grade and potential aggressiveness of at least some brain neoplasms. Focally increased FDG uptake in the brain should raise the suspicion of malignancy as a differential diagnosis, particularly where there is a history of a brain tumour. Howe ve r, the his tol ogy of the ma li gnancy in whi ch the re is a well-known lack of significant FDG avidity, the absence of demonstrable residual neoplasm on MRI following the mos t rec ent sur ger y, the mor pho log y of the met abo lic focu s and the cer ebr al cort ical reg iona l-motoric cor res - pondence militate against a tumourous aetiology for this uptak e [6]. Address cor res ponden ce to: Dr Frank Schr aml , Department of Radiology, Saint Joseph’s Hospital and Medical Center/The Barrow Neurol ogic Institute, 350 West Thomas Road, Phoenix, Arizona 85013, USA. E-mail: [email protected] The British Journal of Radiology, 84 (2011), 1153–1155 The British Journal of Radiology, December 2011 1153