25
Theoretical Explanations for the Importance of Using NANDA/NIC/NOC Margaret Lunney, RN, PhD
| Date post: | 29-Dec-2015 |
| Category: |
Documents |
| Upload: | dortha-nelson |
| View: | 216 times |
| Download: | 1 times |
Theoretical Explanations for the Importance of Using
NANDA/NIC/NOC
Margaret Lunney, RN, PhD
Who Needs Theoretical Explanations?
Nurses and others who:• value research-theory-practice
relationship• reject standardization • reject the complexity of N/N/N• feel the “power of nursing” without
N/N/N
Explanations Currently Used1. Need for documentation of nursing
diagnoses, interventions, and outcomes
2. Visibility of nursing’s contributionNote: 1 & 2 are viewed by critics as self-serving
3. Improved quality & manageable costs
Problem: Pervasive Criticisms
• Covert response (most common)– N/N/N are ignored & avoided
• Overt responses:– Articles: Shamansky & Yanni (1983);
Hagey & McDonough (1984); Leininger (1990); Mitchell (1991);
– Negative comments on listservs; negative reviews of manuscripts & research
Effects of Criticisms
• N/N/N not included in education • N/N/N not required for
documentation• N/N/N not in HIS/EHR • Research proposals & manuscripts
not approved for funding/publication
Solution: Theoretical Explanations Theories to describe, explain and predict reasons
touse N/N/N:
– Linguistic TheoryHayakawa (1990). Language in thought and action.
– Critical thinking theory/conceptsScheffer & Rubenfeld (2000). Consensus statementon CT
– Concept of AccuracyLunney (2000). Critical thinking and nursing
diagnosis
Linguistic Theory Languages are:• fundamental mechanism of survival• most highly developed symbolic
processes• tools for communication with self &
others• sources of cooperative actions with
others• tools to improve human experiences
Linguistic Theory
• Scientific names are needed because word usage varies
• Naming is a “great” step forward; it makes discussion possible
• There are no “right” names for anything
• Definitions are statements of linguistic habits; not law
Linguistic Theory• Naming is classifying• Classifications are developed for specific
purposes • Classifications =pooled knowledge• Pooled knowledge helps us to deal with
the physical world• Science seeks generally useful
classifications, ones that produce results• Results in nursing = quality of nursing
care
Maps to the Territory
• Many maps needed to “know” a territory
• No maps “fully” represent the territory• All maps do not “equal” the territory • Goal- Make “good maps” of the
territory • NANDA, NIC and NOC are the “good
maps”
Meaning, Context, Experience• Meanings known through context• Context gained through experience• Using N/N/N increases experience
by: – depicting interrelationships– reducing complexity– available in one source
Extensional/Intensional Meanings
• Extensional– relates to the physical world
• Intensional– relates to individual connotations– focus on intensional = Prejudice
• N/N/N - extensional & intensional
How We Know What We Know• We experience a small fraction of
phenomena• We abstract the objects of our experiences • It makes no sense to distrust abstractions• We need to be AWARE of abstracting• Words always need to be connected with
what they stand for.Avoid this:
words defining words
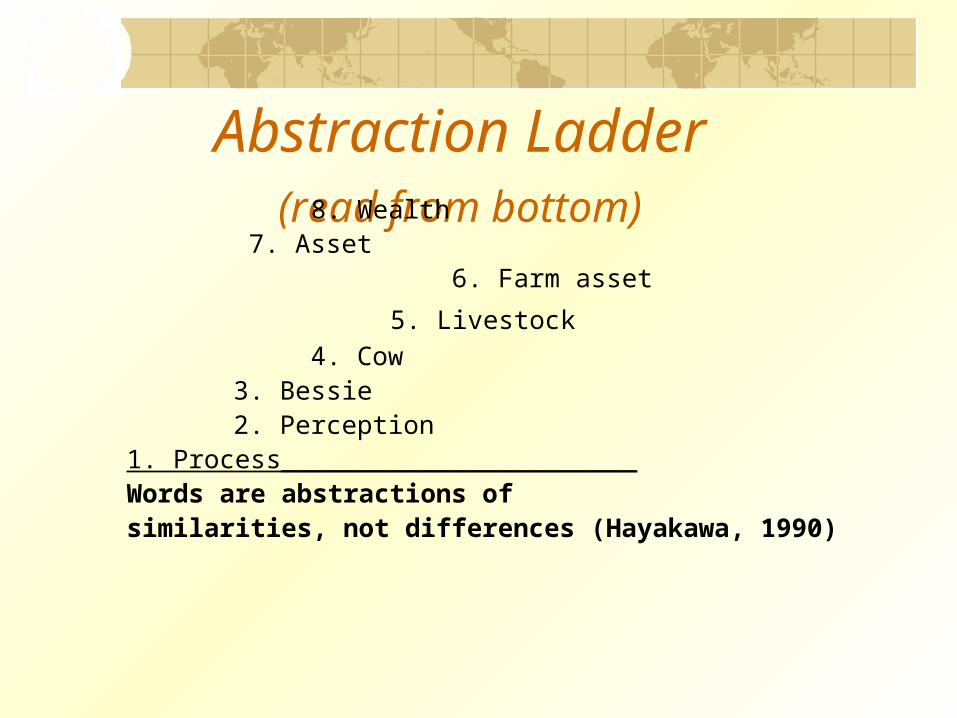
Abstraction Ladder (read from bottom) 8. Wealth 7. Asset
6. Farm asset
5. Livestock 4. Cow
3. Bessie 2. Perception 1. Process_______________________Words are abstractions ofsimilarities, not differences (Hayakawa, 1990)
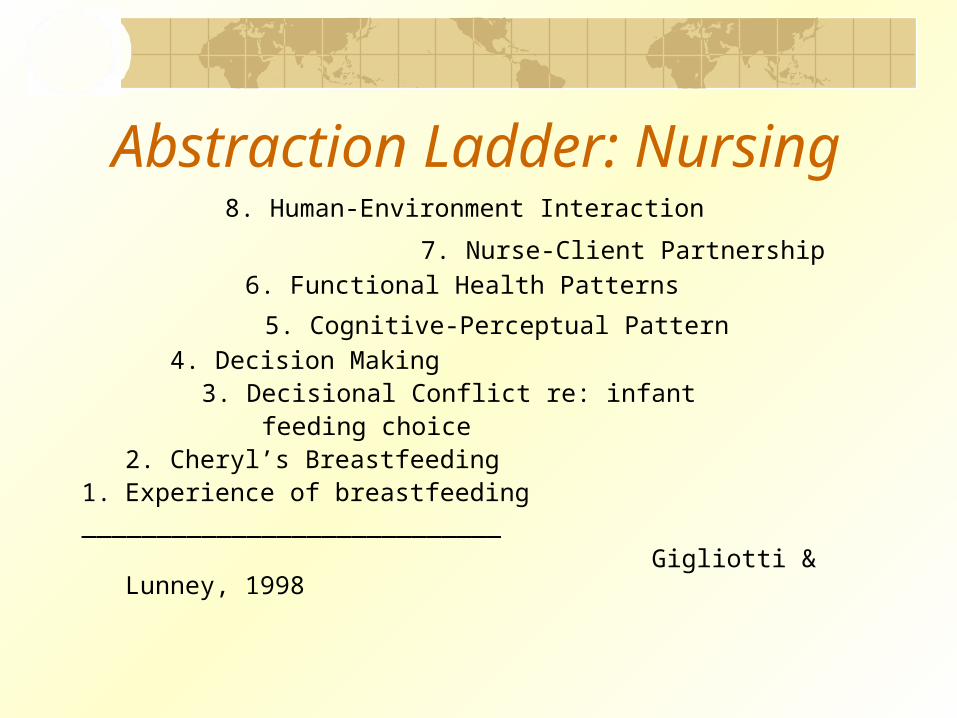
Abstraction Ladder: Nursing 8. Human-Environment Interaction
7. Nurse-Client Partnership 6. Functional Health Patterns
5. Cognitive-Perceptual Pattern 4. Decision Making
3. Decisional Conflict re: infant feeding choice
2. Cheryl’s Breastfeeding 1. Experience of breastfeeding____________________________ Gigliotti & Lunney, 1998
Application to N/N/N• Explain relation of naming to
knowing • Acknowledge reality of naming• Describe essential nature of
abstraction & levels of abstraction• Demonstrate connections to the
extensional world through case studies
Complexity of NNN and Theory
• Indicators of Complexity: – ~1000 concepts with related
information/knowledge– Ambiguous relationships among concepts– Extreme # of choices
• Reducing complexity of N/N/N improves:– Efficiency and effectiveness of thinking– Accuracy of diagnoses– Discernment of best interventions and outcomes
What is Critical thinking (CT)?
Consensus of 57 Nurse Experts:• Cognitive Skills (7)
– Analyzing– Applying Standards– Discriminating– Information Seeking– Logical Reasoning– Predicting
• Habits of mind (10) Scheffer & Rubenfeld,
2000 Lunney, 2001, Ch 1
Why Critical Thinking?
• Thinking abilities of adults vary from low to high
• The thinking processes needed for the nursing process are complex
• Each clinical case requires specific types of thinking abilities
• Thinking affects choices of diagnoses, interventions and outcomes
What is Accuracy of NDx?• Definition
“A rater’s judgment of the degree to which a diagnostic statement matches the cues in a client situation.” (Lunney, 1990)
• Characteristics– Ranges from high to low– Relative to interactive elements– Simple to complex according to # of cues, types
of cues, characteristics of cues– Includes supporting and conflicting cues– Relative to the whole situation
Why Accuracy of NDx?• Accuracy is an outcome of CT• Client data lead to many possible
dx choices, including etiologies• Research findings show that low
accuracy is a reality• Diagnoses are the foundation of
interventions and outcomes
Why discernment of outcomes/interventions?
• Clinical situations differ based on contextual factors (e.g., culture, age, history)
• Many outcomes and interventions are possible
• The most appropriate outcomes and interventions need to be selected through CT
Using N/N/N Improves CT for Accuracy/Discernment
• More efficient and effective:Analyzing DiscriminatingInformation seeking Applying standards Logical reasoningPredicting

Effects on Quality Words & Critical Accuracy & Phrases + Thinking + Discernment
Communication & Cooperation
Improved Actions
Improved Quality Lunney, 1999,
2001
Using N/N/N• Mitigate criticisms, e.g.,
– Be conscious that the labels of N/N/N/ are NOT nursing
• Show connections of N/N/N to thinking & actions through case studies
• Demonstrate through theories andresearch that using N/N/N improves quality

















