Annual Meeting Therapeutic Frontiers Award Lecture—Therapeutic Frontiers In Health Services Research: Methods and Intervention Models Activity No. 0217-0000-11-065-L04-P (Knowledge-Based Activity) Sunday, October 16 10:30 a.m.–11:30 a.m. Convention Center: Spirit of Pittsburgh Ballroom A Moderator: William A. Kehoe, Pharm.D., FCCP, BCPS ACCP President, Professor of Clinical Pharmacy and Psychology; Chair, Department of Pharmacy Practice, University of the Pacific Stockton, California Speaker: Barry L. Carter, Pharm.D., FCCP, BCPS Professor, College of Pharmacy, University of Iowa, Iowa City, Iowa Faculty Conflict of Interest Disclosures Barry L. Carter: no conflicts to disclose. Learning Objectives 1. Briefly review rigorously designed controlled clinical trials on team-based care for the management of hypertension. 2. Discuss various methodologies for conducting prospective interventional studies. 3. Describe new methodologies to evaluate technology, implementation, dissemination and/or sustainability. Self-Assessment Questions Self-assessment questions are available online at www.accp.com/am
Transcript
Annual Meeting
Therapeutic Frontiers Award Lecture—Therapeutic Frontiers In Health Services Research: Methods and Intervention Models Activity No. 0217-0000-11-065-L04-P (Knowledge-Based Activity) Sunday, October 16 10:30 a.m.–11:30 a.m. Convention Center: Spirit of Pittsburgh Ballroom A Moderator: William A. Kehoe, Pharm.D., FCCP, BCPS ACCP President, Professor of Clinical Pharmacy and Psychology; Chair, Department of Pharmacy Practice, University of the Pacific Stockton, California Speaker: Barry L. Carter, Pharm.D., FCCP, BCPS Professor, College of Pharmacy, University of Iowa, Iowa City, Iowa Faculty Conflict of Interest Disclosures Barry L. Carter: no conflicts to disclose. Learning Objectives
1. Briefly review rigorously designed controlled clinical trials on team-based care for the
management of hypertension. 2. Discuss various methodologies for conducting prospective interventional studies. 3. Describe new methodologies to evaluate technology, implementation, dissemination and/or
sustainability.
Self-Assessment Questions Self-assessment questions are available online at www.accp.com/am
Therapeutic Frontiers In Health Services Therapeutic Frontiers In Health Services Research: Methods and Intervention Research: Methods and Intervention
Therapeutic Frontiers In Health Services Therapeutic Frontiers In Health Services Research: Methods and Intervention Research: Methods and Intervention
ModelsModelsModelsModels
Barry L. Carter, Pharm.D., FCCP, FAHA, FASHDepartment of Pharmacy Practice and Science
Patrick E. Keefe Professor in PharmacyCollege of Pharmacy and
Professor and Associate Head for ResearchDepartment of Family Medicine
Roy J. and Lucille A. Carver College of MedicineRoy J. and Lucille A. Carver College of MedicineUniversity of Iowa
Our Research TeamOur Research Team
Thanks to my family…..Thanks to my family…..
Thank you to the ACCP Research Thank you to the ACCP Research InstituteInstitute
1.1. 1990 ACCP1990 ACCP--Mead Johnson Family Medicine Mead Johnson Family Medicine
InstituteInstitute
yyClinical Pharmacy Research Award. Clinical Pharmacy Research Award.
2. 19972. 1997--1998 ACCP 1998 ACCP -- Merck Merck PharmacoeconomicsPharmacoeconomicsll h ( hll h ( h llll ))Fellowship (Sarah Fellowship (Sarah BillupsBillups).).
All investigators who have yet to beAll investigators who have yet to beAll investigators who have yet to be All investigators who have yet to be federally funded should definitely federally funded should definitely consider applying for the ACCP FITconsider applying for the ACCP FITconsider applying for the ACCP FIT consider applying for the ACCP FIT program!!!program!!!
ObjectivesObjectives
1. Briefly review rigorously designed, y g y g ,controlled clinical trials on team-based care for the management of hypertension.
i i h d l i f2. Discuss various methodologies for conducting prospective interventional studiesstudies.
3. Describe new methodologies to evaluate technology, implementation,technology, implementation, dissemination and/or sustainability.
Important Concepts that Determine Important Concepts that Determine Various Study MethodologiesVarious Study MethodologiesVarious Study MethodologiesVarious Study Methodologies
Diff i th i t t d l d dDiffusion: the passive, untargeted, unplanned and uncontrolled spread of new interventions. See later CAPTION study example…..later CAPTION study example…..
Implementation: is the process of putting to use p p p gor integrating evidence-based interventions within a specific setting. See later CAPTION study…..
Rabin BA et al. A glossary for dissemination and implementation Rabin BA et al. A glossary for dissemination and implementation research in health. J Public Health Management Practice research in health. J Public Health Management Practice 2008;14:1172008;14:117--123.123.
Important Concepts that Determine Important Concepts that Determine Various Study MethodologiesVarious Study Methodologies
Sustainability: describes to what extent an id b d i i d li ievidence-based intervention can deliver its
intended benefits over an extended period of time after external support from the donor agency isafter external support from the donor agency is terminated. See two later examples….
Rabin BA et al. A glossary for dissemination and implementation Rabin BA et al. A glossary for dissemination and implementation research in health. J Public Health Management Practice research in health. J Public Health Management Practice 2008;14:1172008;14:117--123.123.
Types of Designs:Types of Designs:
Efficacy trial: conducted under ideal circumstances with tight inclusion criteria Good internal validity butwith tight inclusion criteria. Good internal validity but low external validity (generalization). Example outcome measure: multiple BPs measured frequently ( thl ) b bli d d h(e.g. monthly) by a blinded research nurse.
Effectiveness trial: conducted under usual practiceEffectiveness trial: conducted under usual practice conditions and often using databases or retrospective designs. Prospective trials have few exclusions and less internal validity but high external validityless internal validity but high external validity. Example outcome measure: routine office-measured BPs measured whenever…..
Types of Designs Continued:Types of Designs Continued:
Combination trial: attempts to use features of both pefficacy and effectiveness trials. Example outcome measure: research measured BP but limit the frequency to reduce the effect on patient behaviorfrequency to reduce the effect on patient behavior.
T i l M th d f R d i tiT i l M th d f R d i tiTypical Method of Randomization:Typical Method of Randomization:
• By Patient: typical approach for randomized controlled drug trials but will inject g jcontamination for a behavioral intervention at MD level.
Gold Standard for HSR: Gold Standard for HSR: Cl R d i d D iCl R d i d D iCluster Randomized DesignsCluster Randomized Designs
• By Physician (MD clusters): reduces y ys c a ( c uste s) educescontamination since a given MD only has patients in one group. However, if MDs cover for one another or interact thencover for one another or interact, then contamination still occurs.
• By Clinic or Hospital (cluster randomized trial): The strongest design for behavioral interventions but requires many clinics or hospitals (usually no less than 10 for 2-arm study)study).
Limitations with many studies evaluating team based careevaluating team-based care
Small sample sizes (low power or limited generalizability)Small sample sizes (low power or limited generalizability)Single site and single intervention pharmacist or nurseBias in BP measurementL k f t l ( t d i l )Lack of control groups (pre- post- design only)No evaluation of key covariatesFew were intention-to-treat analysesFew were intention to treat analysesDid not adequately evaluate missing data (last value
carried forward versus more sophisticated modeling or l )sensitivity analysis).
Carter BL, Bosworth HB, Green BB. State of the Art Review: The Carter BL, Bosworth HB, Green BB. State of the Art Review: The Hypertension Team: The role of the pharmacist, nurse and Hypertension Team: The role of the pharmacist, nurse and teamwork in hypertension therapy. J Clin teamwork in hypertension therapy. J Clin HypertensHypertens (in press).(in press).
Examples of Clinical Trials with pDifferent Methodologies and
InterventionsInterventions
Contemporary and rigorously designed trialsdesigned trials
Efficacy study that evaluates sustainabilityEfficacy study that evaluates sustainability
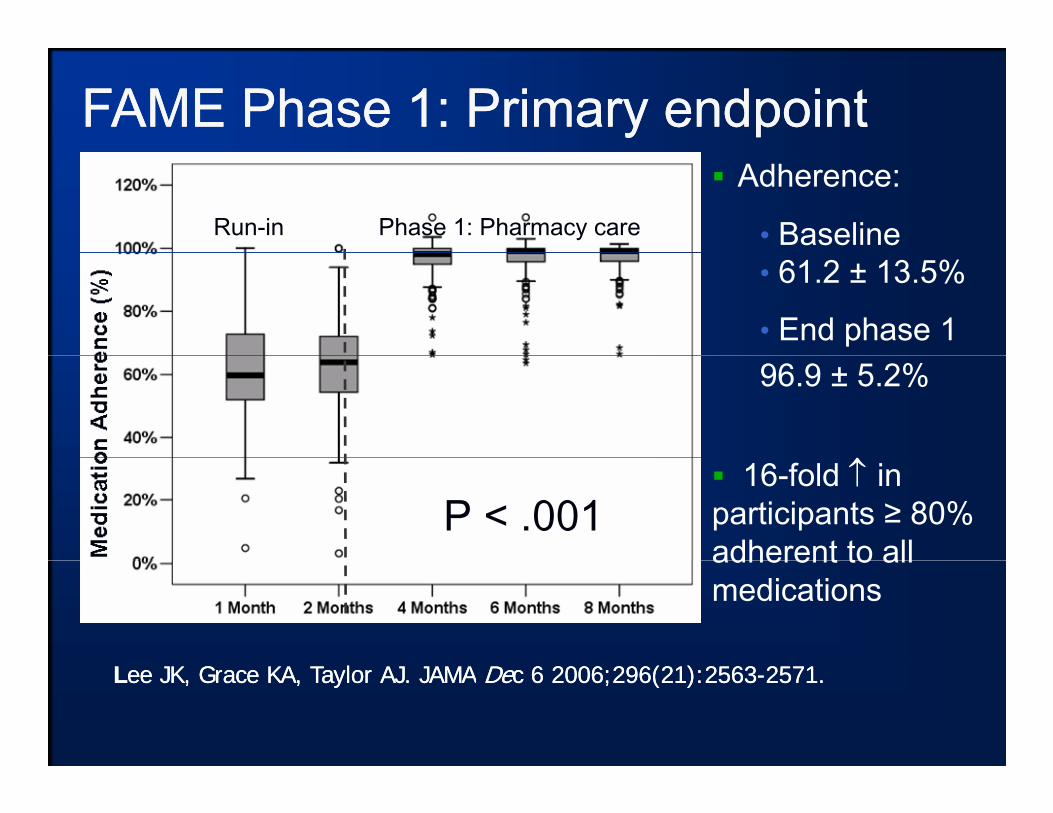
Federal Study of Adherence to Medications in the ElderlyMedications in the Elderly
(FAME)Cli i l h i t l ti d d ti•Clinical pharmacist evaluation and education:
Medication names, indications, doses, frequency, side effects, and properfrequency, side effects, and proper medication-taking behavior
LLee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication ee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication dh d i t bl d d ldh d i t bl d d l d it li t id it li t i
Custom blister-packed medications
adherence and persistence, blood pressure, and lowadherence and persistence, blood pressure, and low--density lipoprotein density lipoprotein cholesterol: a randomized controlled trial. JAMAcholesterol: a randomized controlled trial. JAMA DeDec 6 2006;296(21):2563c 6 2006;296(21):2563--2571.2571.
FAME Phase 2: BP and LDLFAME Phase 2: BP and LDL--CCPre-specified analyses
Systolic BP Change SBP 95% CI P (within group)
P (between group)group) group)
Usual care -1.0 mm Hg -5.9 to 3.9 .69 .04
Pharmacy care -6.9 mm Hg -10.7 to -3.1 .001
Cluster, Randomized Efficacy Trial
O r i g i n a l P a p e r
A Cluster Randomized Trial to EvaluateA Cluster Randomized Trial to Evaluate Physician/Pharmacist Collaboration toI Bl d P C t lImprove Blood Pressure ControlBarry L. Carter, PharmD; George R. Bergus, MD; Jeffrey D. Dawson, ScD;
Karen B. Farris, PhD; William R. Doucette, PhD; Elizabeth A. , ; , ;Chrischilles, PhD; Arthur J. Hartz, MD, PhD
Funded by NHLBI: RO1 HL69801Funded by NHLBI: RO1 HL69801Journal of Clinical Hypertension 2008;10:260Journal of Clinical Hypertension 2008;10:260--271271
Collaborative Management of Collaborative Management of H t iH t i St dSt d Effi T i lEffi T i lHypertension Hypertension StudyStudy: Efficacy Trial: Efficacy Trial
• Only faculty / private physicians involved in the study.P ti t 21 85 ith di i f h t i• Patients 21-85 years with diagnosis of hypertension.
• Baseline BP: 145-179 SBP or 95-109 DBP for uncomplicated.• 135-179 SBP or 85-109 DBP for diabetes.135 179 SBP or 85 109 DBP for diabetes.
• Clinic BP at 0, 2, 4, 6, 8, 9 months• 24-hour BP at baseline and 9 months
Journal of Clinical Hypertension 2008;10:260Journal of Clinical Hypertension 2008;10:260--271271
• Pharmacist conducted interview and assessed patient for strategies to improve BP controlpatient for strategies to improve BP control.
• Pharmacist made recommendations to MD and patient to improve BP control.patient to improve BP control.
• Pharmacists and physicians worked to overcome/prevent sub-optimal treatment, clinical inertia, poor adherence, adverse reactions, drug interactions
• Pharmacists saw patients at least every 2 months x• Pharmacists saw patients at least every 2 months x 9 months.
NHLBI: RO1 HL69801
Data AnalysisData Analysis
• Continuous variables – likelihood-based mixed models with random patient effects fit to SAS pProc Mixed in an intention-to-treat analysis.
• Models adjusted for baseline BP, age, gender, race, education, insurance status, household income marital status smoking status alcoholincome, marital status, smoking status, alcohol intake, BMI, number of co-existing conditions, baseline medication adherence and total number of visits during the study.
Dealing with Missing DataDealing with Missing Data
• Common methods are to use the baseline BP or the last value carried forward, these are now ,considered inferior approaches.
• We used statistical modeling for missing data.• We then performed as sensitivity analysis
under worst-case scenario to demonstrate the effect was robust:effect was robust:– Missing data for subjects in the control group all
assumed to have controlled BP– Missing data for subjects in the intervention groups
When adjusting for the intervention effect the• When adjusting for the intervention effect, the within-clinic Intercluster Correlation Coefficient (ICC) is needed to determine the variability(ICC) is needed to determine the variability within office or within physician cluster.
• Measuring patient level data without accounting for clustering will potentially bias g g p ythe results.
Results of Clustering AnalysesResults of Clustering Analyses
• ICC for SBP at 9 months was 0.0084 (<1%). Th ithi li i i 139 dThe within clinic variance was 139 and between clinic variance of 1.2 (NS). When adjusting for all relevant baseline covariatesadjusting for all relevant baseline covariates, ICC dropped to 0.0010.
• Within-physician ICC was 0.0097 (NS), within-physician variance was 138.4, between-physician variance was 138.4, betweenphysician variance was 1.4. When adjusting for covariates, ICC dropped to 0.0005.
ResultsResults• Mean difference (control group minus the
intervention group) in SBP was -8.7 (95% g p) (CI: -4.4, -12.9) mm Hg
• Mean difference in DBP was -5.4 (CI: -2.8, 8 0) mm Hg-8.0) mm Hg.
• 24-hour BP levels mean difference in SBP of -8.8 (CI: -5.0, -12.6) mm Hg -4.6(CI: -2.4, -6.8) mm Hg for DBP.
ResultsS li BP Ti
Intervention - CMH (n=101)
C t l CMH ( 78)
155
160Systolic BP vs. Time Control - CMH (n=78)
Intervention - post-study (n=64)
Control - post-study (n=39)
140
145
150
Hg
)
Sustainability
** ** **125
130
135
SB
P m
m H
*** *******
**********
** **
115
120
125
**************
1100 2 4 6 8 10 12 14 16 18 20 22 24 26
Time in Months
* p<0.05, ** p<0.01, *** p<0.001, * p<0.05, ** p<0.01, *** p<0.001, Carter BL, Bergus GR, Dawson et al. Journal of Clinical Hypertension 2008;10:260Carter BL, Bergus GR, Dawson et al. Journal of Clinical Hypertension 2008;10:260--271.271.Carter BL, Doucette WR. Franciscus CL, et al. Pharmacotherapy 2010;30:228Carter BL, Doucette WR. Franciscus CL, et al. Pharmacotherapy 2010;30:228--235.235.
Results: BP Control RatesResults: BP Control RatesMain Finding: The major reason for the high control was due to intensification of medications.
Control Interven-tion
Adjusted OR
CI; p valuep
All patients
52.9% 89.1% 8.9 3.8-20.7P<0 001patients P<0.001
Diabetes 23.5% 81.8% 40.1 4.1-394.7P=0.002
-- Carter BL, Bergus GR, Dawson et al. Journal of Clinical Carter BL, Bergus GR, Dawson et al. Journal of Clinical H t i 2008 10 260H t i 2008 10 260 271271Hypertension 2008;10:260Hypertension 2008;10:260--271.271.
-- Von Muenster SJ, et al. Pharmacy World & Science Von Muenster SJ, et al. Pharmacy World & Science 2008:30:1282008:30:128--135.135.
Physician and Pharmacist Collaboration to Improve Blood Pressure Controlto Improve Blood Pressure Control
Barry L. Carter, PharmD; Gail Ardery, PhD; Jeffrey D. Dawson, ScD; Paul A. y y yJames, MD; George R. Bergus, MD; William R. Doucette, PhD; Elizabeth A. Chrischilles, PhD; Carrie L. Franciscus, MA; Yinghui Xu, MS
Adherence Study: Combination of Adherence Study: Combination of Efficacy and EffectivenessEfficacy and Effectiveness
Adherence Study: Combination of Adherence Study: Combination of Efficacy and EffectivenessEfficacy and EffectivenessEfficacy and EffectivenessEfficacy and EffectivenessEfficacy and EffectivenessEfficacy and Effectiveness
• Prospective, cluster-randomized controlled trial inProspective, cluster randomized controlled trial in 6 community-based family medicine residency clinics all with clinical pharmacist faculty in the medical office.
• Research nurse in each clinic measured BP at baseline, 3 and 6 months and 24-hour BP at b li d 6 hbaseline and 6 months.
InterventionIntervention
• Pharmacist conducted interview and assessed patient for strategies to improve BP controlpatient for strategies to improve BP control.
• Pharmacist made recommendations to MD and patient to improve BP control.patient to improve BP control.
• Pharmacists and physicians worked to overcome/prevent sub-optimal treatment, clinical inertia, poor adherence
• Pharmacists only encouraged to see patients at baseline and 1 month with a telephone call at 3baseline and 1 month with a telephone call at 3 months with a goal to achieve BP control by 6 months (but they could see patients more often).( y p )
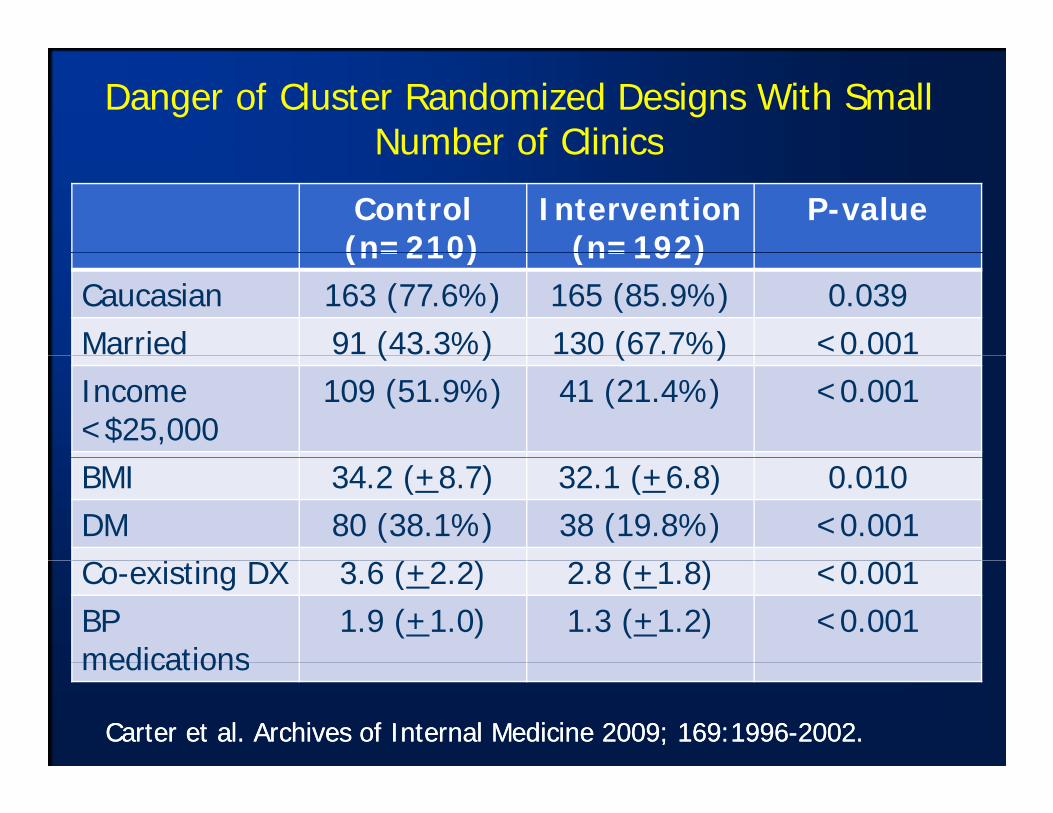
Danger of Cluster Randomized Designs With Small Number of ClinicsNumber of Clinics
Department of Pharmacy Practice and Science, Department of Pharmacy Practice and Science, College of Pharmacy andCollege of Pharmacy and
Professor and Associate Head for ResearchProfessor and Associate Head for ResearchDepartment of Family MedicineDepartment of Family Medicine
Principal Investigator, DCCPrincipal Investigator, DCCProfessor and Director, Clinical Trials DataProfessor and Director, Clinical Trials Data
Management CenterManagement Center
College of Public HealthCollege of Public HealthDepartment of Family MedicineDepartment of Family MedicineRoy J. and Lucille A. Carver College of Roy J. and Lucille A. Carver College of MedicineMedicine
* The study is being funded y gby NHLBI/NIH, R01 HL091841-01A1.
Participating Locationsp g
CAPTION Study Design:CAPTION Study Design: Cluster Randomized Trial
1.1. One goal is to determine if the intervention One goal is to determine if the intervention is effective in minorities so goal is to enrollis effective in minorities so goal is to enrollis effective in minorities so goal is to enroll is effective in minorities so goal is to enroll 40% minorities.40% minorities.
2.2. Clinics stratified based on the percent Clinics stratified based on the percent ppAfrican Americans or Hispanics (high or African Americans or Hispanics (high or low), and the score of a pharmacy services low), and the score of a pharmacy services provided by the clinical pharmacists (high or provided by the clinical pharmacists (high or low).low).
33 DCC then randomized the medical officesDCC then randomized the medical offices3.3. DCC then randomized the medical offices.DCC then randomized the medical offices.
Site Randomization to 3 ArmsSite Randomization to 3 Arms
Active Observation Group 1Active Observation Group 1 9 month BP intervention (n=24/site)
Active Observation Group 2 24 month BP intervention (n=24/site)
Usual Care/Practice Diversion Group Control arm for the hypertension study Control arm for the hypertension study
Every site will also identify 18 patients withEvery site will also identify 18 patients with uncontrolled HTN who are not consented into the study (passive observation BPinto the study (passive observation BP group) who will undergo med record review to test whether the effect of thereview to test whether the effect of the intervention diffuses throughout the medical officemedical office.
32 clinics stratified
32 clinics randomized
BP 9 month Intervention
Group:
BP 24 month Intervention
BP Usual Care/ Asthma PPCM
(9 clinics)
BP Control Group: (n=216)
Group: (9 clinics, n=216)
Group: (9 clinics, n=216)
9-month asthma
intervention
BP Observational Cohort: 3 BP Arms (n=216)
9 month Intervention, then stopped
Intervention for 24
months
(n=100) (n=486)
Clinic BPs via
BP at baseline, 6, 9, 12, 18, 24
BP at baseline, 6, 9, 12, 18,
BP at baseline, 6, 9, 12, 18, 24
chart review for
Observational Cohort
24-month evaluation of BP and covariates (all HTN
9, 12, 18, 24 mos.
, , ,24 mos.
9, 12, 18, 24 mos.
patients)
The Electronic Communications and Home Blood Pressureand Home Blood Pressure
Monitoring Trial (e-BP)g ( )Comparison of 2 Interventions to Usual Care:• Home BP monitor and use of an existing patient g pWeb site
• This plus pharmacist care management (delivered via the patient Web site)
Green BB Cook AJ Ralston JD et al Effectiveness of home bloodGreen BB, Cook AJ, Ralston JD, et al. Effectiveness of home blood pressure monitoring, Web communication, and pharmacist care on hypertension control: a randomized controlled trial. JAMA. Jun 25 2008;299(24):2857-28672008;299(24):2857 2867.
Funded by NHLBI: 5R01HL075263-04
BP control at 12 monthsControl BPM-Web
OnlyBPM-Web-Only Web
PharmAll 31% 36% 56%**
Systolic BP 20% 26% 54%**Systolic BP at baseline >160 mm
20% 26% 54%
**P < 0.001 compared to UC and BPM**P < 0.001 compared to UC and BPM--WebWeb
Conclusion: the addition of the pharmacist intervention to the web was necessary to achieve good BP control.
Green BB, et al. Green BB, et al. JAMA. JAMA. 2008;299(24):28572008;299(24):2857--2867.2867.
Numerous Meta-analyses of Team-Based Care in BPBased Care in BP
1. Walsh JM, et al. Med Care. Jul 2006;44(7):646-657.2 Carter BL et al Arch Intern Med 2009;169(19):17482. Carter BL, et al. Arch Intern Med. 2009;169(19):1748-
1755.3. Chisholm-Burns MA, et al. Med Care. 2010;48(10):923-
933.4. Machado M, et al. Ann Pharmacother. 2007;41(11):1770-
1781.5. Glynn LG, et al. Cochrane Database Syst Rev.
2010(3):CD005182.6 Fahey T et al Cochrane Database Syst Rev6. Fahey T, et al.. Cochrane Database Syst Rev.
2006(4):CD005182.7. Clark CE, et al.. BMJ. 2011;341:c3995.
Meta-Analysis: Potency of individual components of team-based care
Median reduction in SBP(mm Hg)
Pharmacist recommended medication to physician -9.3*
Education on BP medications -8.75*
Pharmacist did the intervention -8 44Pharmacist did the intervention -8.44
Assessed medication compliance -7.9
Counseling on lifestyle modification -7.59Counseling on lifestyle modification 7.59
Carter BL, Rogers M, Daly J, Zheng S, James JA. Quality Improvement Strategies for Hypertension: The Potency of Team-based Care Interventions. Archives of Internal Medicine 2009; 169:1748-1755. Adapted from the methods of:W l h J t l H t i C Cl i th Q lit G A iti l l i f lit
Walsh J et al. Hypertension Care. Closing the Quality Gap: A critical analysis of quality improvement strategies. (Prepared by Stanford -UCSF Evidence-based Practice Center, Contract No. 290-02-0017). AHRQ publication No. 04-0051-3, Rockville, MD. January 2005.
Meta-analysis of Potency of individual components of team-based carebased care
Odds that BP was controlled (95% confidence Interval)
Studies involving nurses 1.69 (1.48-1.93)
[69% increased chance]
Studies involving pharmacists within physician offices or clinics
2.48 (2.05-2.99)
[148% increased chance]
Studies done in community pharmacies
2.89 (1.83-4.55)
[189% increased chance]
Conclusion: All were effective but interventions by pharmacists appear to be more potent than by nurses
47Carter BL, et al. Archives of Internal Medicine 2009; 169:1748-1755.
nurses.
The Therapeutic Frontiers in The Therapeutic Frontiers in Health Services Research:Health Services Research:
The Therapeutic Frontiers in The Therapeutic Frontiers in Health Services Research:Health Services Research:Health Services Research: Health Services Research:
QuestionsQuestionsHealth Services Research: Health Services Research:
QuestionsQuestionsb d h l lb d h l l1.1. TeamTeam--based care interventions have clearly based care interventions have clearly
been shown to be effective for a variety of been shown to be effective for a variety of chronic conditions but many questions remainchronic conditions but many questions remainchronic conditions but many questions remain chronic conditions but many questions remain and and NIH will fund such studiesNIH will fund such studies::a.a. Can the models be scaled up andCan the models be scaled up anda.a. Can the models be scaled up and Can the models be scaled up and
implemented in large numbers of diverse implemented in large numbers of diverse and very busy practices?and very busy practices?
b.b. Can the effect be sustained in the longCan the effect be sustained in the long--term? Are “booster” interventions needed?term? Are “booster” interventions needed?
cc Is there a viable business model for currentIs there a viable business model for currentc.c. Is there a viable business model for current Is there a viable business model for current and future payment structures?and future payment structures?
The Therapeutic Frontiers in The Therapeutic Frontiers in Health Services Research:Health Services Research:
The Therapeutic Frontiers in The Therapeutic Frontiers in Health Services Research:Health Services Research:Health Services Research: Health Services Research:
Summary of Key PointsSummary of Key PointsHealth Services Research: Health Services Research:
Summary of Key PointsSummary of Key Points1. Health-care reform, the patient-centered
medical home and technology will require much more health services research studies in team-based care.
2. Studies must be rigorously designed, tested and analyzed which will likely require federallyand analyzed which will likely require federally funded grants.
The Therapeutic Frontiers in The Therapeutic Frontiers in Health Services Research:Health Services Research:
The Therapeutic Frontiers in The Therapeutic Frontiers in Health Services Research:Health Services Research:Health Services Research: Health Services Research:
Summary of Key PointsSummary of Key PointsHealth Services Research: Health Services Research:
Summary of Key PointsSummary of Key Points
3. Clinical pharmacy scientists must have strong training in grant writing Should attend astraining in grant writing. Should attend as many grant writing workshops as possible.
4. You must consider the ACCP FIT program if you are a clinical pharmacy researcher desiring federal funding.
Comments and QuestionsComments and QuestionsComments and QuestionsComments and QuestionsComments and QuestionsComments and QuestionsComments and QuestionsComments and Questions
Suggested readings:
1. Okonofua EC, Simpson KN, Jesri A, Rehman SU, Durkalski VL, Egan BM. Therapeutic inertia is an impediment to achieving the Healthy People 2010 blood pressure control goals. Hypertension. Mar 2006;47(3):345-351.
2. Walsh JM, McDonald KM, Shojania KG, et al. Quality improvement strategies for hypertension management: a systematic review. Med Care. Jul 2006;44(7):646-657.
3. Carter BL, Rogers M, Daly J, Zheng S, James PA. The potency of team-based care interventions for hypertension: a meta-analysis. Arch Intern Med. Oct 26 2009;169(19):1748-1755.
4. Chisholm-Burns MA, Kim Lee J, Spivey CA, et al. US pharmacists' effect as team members on patient care: systematic review and meta-analyses. Med Care. Oct 2010;48(10):923-933.
5. McKenney JM, Slining JM, Henderson HR, Devins D, Barr M. The effect of clinical pharmacy services on patients with essential hypertension. Circulation. Nov 1973;48(5):1104-1111.
6. Bogden PE, Abbott RD, Williamson P, Onopa JK, Koontz LM. Comparing standard care with a physician and pharmacist team approach for uncontrolled hypertension. J Gen Intern Med. Dec 1998;13(11):740-745.
7. Borenstein JE, Graber G, Saltiel E, et al. Physician-pharmacist comanagement of hypertension: a randomized, comparative trial. Pharmacotherapy. Feb 2003;23(2):209-216.
8. Logan AG, Milne BJ, Achber C, Campbell WP, Haynes RB. Work-site treatment of hypertension by specially trained nurses. A controlled trial. Lancet. 1979;2(8153):1175-1178.
9. Rudd P, Miller NH, Kaufman J, et al. Nurse management for hypertension. A systems approach. Am J Hypertens. Oct 2004;17(10):921-927.
10. Machado M, Bajcar J, Guzzo GC, Einarson TR. Sensitivity of patient outcomes to pharmacist interventions. Part II: Systematic review and meta-analysis in hypertension management. Ann Pharmacother. Nov 2007;41(11):1770-1781.
11. Glynn LG, Murphy AW, Smith SM, Schroeder K, Fahey T. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database Syst Rev. 2010(3):CD005182.
12. Fahey T, Schroeder K, Ebrahim S. Interventions used to improve control of blood pressure in patients with hypertension. Cochrane Database Syst Rev. 2006(4):CD005182.
13. Clark CE, Smith LF, Taylor RS, Campbell JL. Nurse led interventions to improve control of blood pressure in people with hypertension: systematic review and meta-analysis. Bmj. 2011;341:c3995.
14. Carter BL. Designing quality health services research: why comparative effectiveness studies are needed and why pharmacists should be involved. Pharmacotherapy. Aug 2010;30(8):751-757.
15. Carter BL, Foppe van Mil JW. Comparative Effectiveness Research: Evaluating Pharmacist Interventions and Strategies to Improve Medication Adherence. Am J Hypertens. Jul 22 2010.
16. Lee JK, Grace KA, Taylor AJ. Effect of a pharmacy care program on medication adherence and persistence, blood pressure, and low-density lipoprotein cholesterol: a randomized controlled trial. Jama. Dec 6 2006;296(21):2563-2571.
17. Carter BL, Bergus GR, Dawson JD, et al. A cluster randomized trial to evaluate physician/pharmacist collaboration to improve blood pressure control. J Clin Hypertens (Greenwich). Apr 2008;10(4):260-271.
18. Von Muenster SJ, Carter BL, Weber CA, et al. Description of pharmacist interventions during physician-pharmacist co-management of hypertension. Pharm World Sci. Jan 2008;30(1):128-135.
19. Carter BL, Doucette WR, Franciscus CL, Ardery G, Kluesner KM, Chrischilles EA. Deterioration of blood pressure control after discontinuation of a physician-pharmacist collaborative intervention. Pharmacotherapy. Mar 2010;30(3):228-235.
20. Carter BL, Ardery G, Dawson JD, et al. Physician and pharmacist collaboration to improve blood pressure control. Arch Intern Med. Nov 23 2009;169(21):1996-2002.
21. Wentzlaff DM, Carter BL, Ardery G, et al. Sustained blood pressure control following discontinuation of a pharmacist intervention. J Clin Hypertens (Greenwich). Jun 2011;13(6):431-437.
22. Allen JK, Dennison CR. Randomized trials of nursing interventions for secondary prevention in patients with coronary artery disease and heart failure: systematic review. J Cardiovasc Nurs. May-Jun 2010;25(3):207-220.
23. Hill MN, Han HR, Dennison CR, et al. Hypertension care and control in underserved urban African American men: behavioral and physiologic outcomes at 36 months. Am J Hypertens. 2003;16(11):906-913.
24. Bosworth HB, Olsen MK, Dudley T, et al. Patient education and provider decision support to control blood pressure in primary care: a cluster randomized trial. Am Heart J. Mar 2009;157(3):450-456.
25. Bosworth HB, Olsen MK, Grubber JM, et al. Two self-management interventions to improve hypertension control: a randomized trial. Ann Intern Med. Nov 17 2009;151(10):687-695.
26. Bosworth H, Powers BJ., Olsen MK., McCant F., Grubber J., Smith V., Gentry P., Rose, C., Van Houtven C., Wang V., Goldstein MK., Oddone EZ. . Can Home Blood Pressure Management Improve Blood Pressure Control: Results from a Randomized Controlled Trial. . Archives of Internal Medicine. in press.
27. Bosworth HB, Olsen MK, Gentry P, et al. Nurse administered telephone intervention for blood pressure control: a patient-tailored multifactorial intervention. Patient Educ Couns. Apr 2005;57(1):5-14.
28. Smith M, Bates DW, Bodenheimer T, Cleary PD. Why pharmacists belong in the medical home. Health Aff (Millwood). May 2010;29(5):906-913.
29. Artinian NT, Flack JM, Nordstrom CK, et al. Effects of nurse-managed telemonitoring on blood pressure at 12-month follow-up among urban African Americans. Nurs Res. Sep-Oct 2007;56(5):312-322.
30. Bosworth HB, Powers BJ, Olsen MK, et al. Home blood pressure management and improved blood pressure control: results from a randomized controlled trial. Archives of Internal Medicine. Jul 11 2011;171(13):1173-1180.
31. Magid DJ, Ho PM, Olson KL, et al. A multimodal blood pressure control intervention in 3 healthcare systems. Am J Manag Care. 2011;17(4):e96-e103.
32. Shea S, Weinstock RS, Teresi JA, et al. A randomized trial comparing telemedicine case management with usual care in older, ethnically diverse, medically underserved patients with diabetes mellitus: 5 year results of the IDEATel study. J Am Med Inform Assoc. Jul-Aug 2009;16(4):446-456.
33. Green BB, Cook AJ, Ralston JD, et al. Effectiveness of home blood pressure monitoring, Web communication, and pharmacist care on hypertension control: a randomized controlled trial. Jama. Jun 25 2008;299(24):2857-2867.
34. Okamoto MP, Nakahiro RK. Pharmacoeconomic evaluation of a pharmacist-managed hypertension clinic. Pharmacotherapy. Nov 2001;21(11):1337-1344.
35. Zillich AJ, Sutherland JM, Kumbera PA, Carter BL. Hypertension outcomes through blood pressure monitoring and evaluation by pharmacists (HOME study). J Gen Intern Med. Dec 2005;20(12):1091-1096.
36. Carter BL, Barnette DJ, Chrischilles E, Mazzotti GJ, Asali ZJ. Evaluation of hypertensive patients after care provided by community pharmacists in a rural setting. Pharmacotherapy. Nov-Dec 1997;17(6):1274-1285.