144
| Date post: | 23-Jul-2016 |
| Category: |
Documents |
| Upload: | dominic-feng |
| View: | 232 times |
| Download: | 1 times |


Student: Dominic FengChair Instructor: Bradley Walters, RA, AIA, NCARBCo-chair Instructor: Nawari Nawari, Ph.D., P.E., M.ASCE
2015 Master Research Project (Degree Research Project)MASTER OF ARCHITECTURE PROGRAMSchool of ArchitectureCollege of Design, Construction and PlanningUniversity of Florida
Copyright at School of ArchitectureUF School of Architecture, POB 115702Gainesville FL, 32611-5702Tel: (352) 392-0205Fax: (352) 392-4606
1 H21

HOSPITAL FOR 21ST CENTURY
H21
2015 MASTER’S RESEARCH PROJECT 2

01PrincipiaCONTENTS
3 H21

PrincipiaInitiativeManifestoForegroundEvolutionTrackScopeCrisis
ExamplesTempleSanctuaryWardPavilionSkyscraperModernismComplexityMobilityEfficiencySustainabilityElements
DisruptionRealityBusinessProgression
ProcessThesisPractice
AssumptionStrategemPossibilities
LinksCredits
PART 1
PART 2
PART 3
PART 4
ContentsAcknowledgementsPrefaceIntroductionHistoryAlmanacStatisticsChallenges and Dilemmas
Ten Canonical HospitalsGreek AsklepieiaInfirmary of Monastery in ClunySt Thomas’s and Guy’s HospitalHôtel-Dieu de ParisJohns Hopkins HospitalPaimio SanatoriumBeaujon Hospital at ClichyUSS MercyYale-New Haven HospitalH3C Massachusetts General HospitalThe Formation Patterns of Hospitals
Business Model on ChangingThe Innovator’s PrescriptionThe Innovator’s Healthcare IndustryThe Innovator’s Hospital Design
Practical Synthesis of AdvancementsMaking Twenty-First Century HospitalUF Health Shands Cardiovascular Hospital
Emphasis on New Paradigms in Twenty-First CenturyChanging Needs, Changing DirectionsFindings and Conclusion from H21
BibliographyList of Illustrations
0306072729334145
484951535557596163656771
76777981
848587
132133137
139141
2015 MASTER’S RESEARCH PROJECT 4

In 2008, I survived from the devastating earthquake in Sichuan of China after witnessing to the vulnerability of built environment and its makers in front of a disaster. Hundreds of thousands of people were obliterated or maimed as the con-sequence of massive collapsing of buildings. Thus I dedicate hereupon my master research project to this type of the building which can protect and help the lives in most - hospitals, for those who were cherished and lost in that disaster.
5 H21

02
This book —in such a complex subject regarding healthcare facility design—can never be real without help from others, and I wish to recognize all those who par-ticipated in producing this master’s research project, as well as those who helped in the final year of my Master of Architecture program.
First and foremost, it was the invaluable encouragement and support from my parents—Yangchun Feng and Dongmei Mao—who sustained me the strength to obtain those academic achievements in architecture filed and to create this work of which I am proud. In all the years of my life, they instilled to me by their own actions about the very concept of benevolence and sincerity, which I establish all the time as my principles in designing buildings, particularly when it is involved with healthcare. For this project, they provided me not only with their enthusiasm as my friends on my road of growing up, but they also once again deployed their patience for listening to my aspiration, the patience essential to ground my ideas onto the drafting board.
I would also like to thank all these professors in School of Architecture at Univer-sity of Florida, who has honored me with an elegant and inspiring instruction for this challenging project. At first there is Professor Bradley Walters, he is one of my greatest teachers who taught me as well in my lower division design studio when I started in architecture. It was he who helped me string thoughts together and structuring the parts for clarity and precision, coordinated the project from start to finish. The wisdom and strictness that I learned from him keep my mind-set being refreshed in the whole project. In accomplishing this project, the generosity of the knowledge of Professor Nawari Nawari is also to be appreciated. The skills and perseverance that I fostered when I was working with him concerning Building Information Technology are critical to this complex project. In the working process, his wishes sent from Kuwait fuel me match ahead.
In all the incremental progresses, it was also the encouraging discussions and inspiring working environment which is constructed by my fierce colleagues in School of Architecture that allows this work to grow. There, they included: Jefrall Betancourt, David J Catanach, Yixuan Chen, Joel Corazon, Junda He, Felipe Lop-era, Eleanor F McKenna, Juan C Monsalve, Stefan R Oliver, Timothy J O’Neill, Nicole M Paul, Christian N Poppell, Ling Qiu, Maria E Riveros, Jennifer E Russell, Alyson P Silva, Samantha F Spaniak.
At last, I thank all others from my old and new acquaintances, too numerous to mention in here, for helping me to create this work. The discussions they partici-pated in, the criticisms they provided, the general information they offered, and the concerns and issues they held were key to the success of the project, and they are a large part of the reason it has been done. What you will find of the bright and the true in the following pages is in big part of previous endeavors of countless people in healthcare industry—only the errors and mistakes do me alone assume as my own.
Dominic Feng
InitiativeACKNOWLEDGEMENT
2015 MASTER’S RESEARCH PROJECT 6

03ManifestoPREFACE
7 H21
Hospital is the ultimate housing.
Housing birthplaces, housing souls, housing hopes, housing equality and dignity, housing the opportunities to achieve common welfare; hospital is the contemporary temple for physical and mental health. It is of vital importance to a society in both street and global scale.
Hospital projects receive only marginal attention in architectural aca-demia, periodicals, websites, practice, architectural awards and in the oeuvre of super star architects. Hence the intention of this project is the “liberating divergence” of an architecture’s insignificant and conspicuously minor realm.
Fortunately, innovation always occurs when the preceding marginal is accepted into the discipline, sparking adjustments to the logic with-in; just like alchemy to chemistry, astrology to astrophysics, folklore to history, Behrens and Gropius’ industrial factories to modern ar-chitecture. This project will be an experimental attempt to evoke the new paradigm of hospital, which is the most important atherogenic artifact to maintain the survival.
The places of healing can be considered as hospital’s fundamental existence, or in other words, a facility that caters to patients’ well-being. Challenged by the rapid changes of modern society, a redefi-nition and an update of very long-established concept of hospital seems needed. When raw birth rate hits 4.3 births/second for the world, hospital reaches the moment of H21.
2015 MASTER’S RESEARCH PROJECT 8

Epidauros 350 BCEAsklepieion at Epidauros, in ancient Greece, fifth century BCE, as undeni-ably places for inpatient nursing, including bed rest, treatments, medica-tion, baths. By the time of Hippocrates, the temples of Asclepios offered a place of worship and shelter for the sick. It established the earliest arche-type of healthcare facilities according to modern archeology.
9 H21

2015 MASTER’S RESEARCH PROJECT 10

Vercovicium 55Known as Housesteads Roman Fort, was an auxiliary fort on Hadrian’s Wall. Roman Valetudinarium (Military Hospital) in England (first century CE). A Roman military hospital is one designed by the Roman State for its soldiers in the field.
11 H21

2015 MASTER’S RESEARCH PROJECT 12

Angers 1153Interior of the Hôtel-Dieu of St. Jeans in Angers, France (founded in 1153) in the nineteenth century. Well-built stone hospitals, if properly maintained, survive as long as cathedrals.
13 H21

2015 MASTER’S RESEARCH PROJECT 14

Bruges 1778Johnnaes Beerblock’s painting, View of the Sick Ward of St. John’s Hos-pital (Bruges), 1778. This picture conveys the conservation that preserved the forms of the great hall for 600 years that never changed in a radical way until 19th century.
15 H21

2015 MASTER’S RESEARCH PROJECT 16

Gettysburg 1863Interior of a hospital tent during the Civil War of United States. A differently arose in warm, still weather, when tents are difficult to ventilate.
17 H21

2015 MASTER’S RESEARCH PROJECT 18

London 1891The Prince and Princess of Wales visiting a small patient in the Evelina Hospital, 1891. Published in The Illustrated Paper, 28 November 1891, reproduced here courtesy of The Wellcome Library
19 H21

Philadelphia 1925Operating Room scene at the Philadelphia General Hospital, photo-graphed in 1925.
2015 MASTER’S RESEARCH PROJECT 20

Bougainville Island 1943In an underground surgery room, behind the front lines on Bougainville, an American Army doctor operates on a U.S. soldier wounded by a Japanese sniper.” December 13, 1943.
21 H21

Schenectady 1955Bottles are sterilized and filled with baby formula in Ellis Hospital’s formula room, Schenectady, New York State, United States, 1955.
2015 MASTER’S RESEARCH PROJECT 22

Chernobyl 1990Young children rest in a hospital ward in Syekovo, a village near the Cher-nobyl nuclear plant, four years after the blast. 21 April 1990.
23 H21

Chengdu 2005In the southwest of China, Sichuan University represents one of the larg-est academic institutions in the world with over 90,000 students on cam-pus. There are approximately 3,000 medical students on the Health Sci-ence Campus.
2015 MASTER’S RESEARCH PROJECT 24

Fukushima 2011After the enormous tsunami in Japan, a handout photograph made avail-able by the Japanese Red Cross on 13 March 2011 shows that every available space is being used, providing areas for people to sleep, receive treatment, support relatives.
25 H21
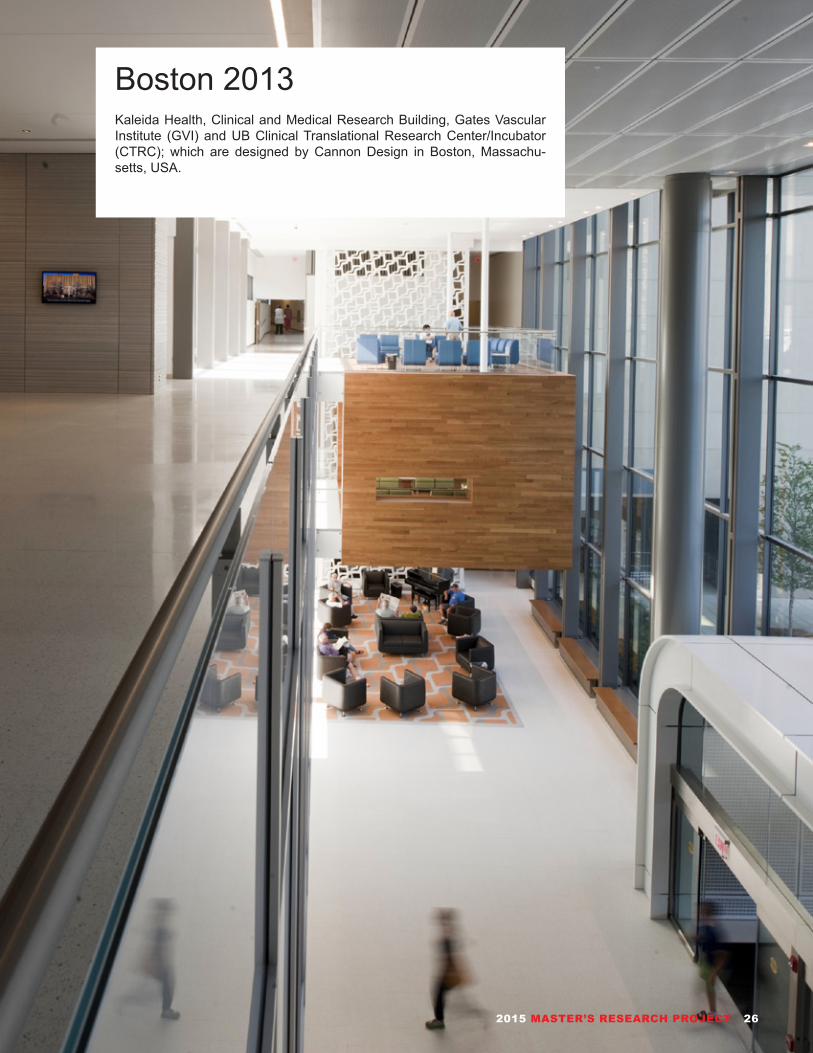
Boston 2013Kaleida Health, Clinical and Medical Research Building, Gates Vascular Institute (GVI) and UB Clinical Translational Research Center/Incubator (CTRC); which are designed by Cannon Design in Boston, Massachu-setts, USA.
2015 MASTER’S RESEARCH PROJECT 26
04ForegroundINTRODUCTION
This project consists of four parts, which together aim to evoke a sustainable and green design for the next generation hospital, which each part itself has been in-trigued by the very basic thought of hospital and hospitalizing in different epochs and aspects.
Part 01 gives a brief historical ichnography of hospitals through ten canonical ex-amples since ancient Greek to present. This part, whose title is inspired by Peter Eisenman’s book - Ten Canonical Buildings. This part intends to open a critical and through view of the way people were thinking about the space for the sick people, and successful findings, and the inspiration it seeks for future in hospitalizing phe-nomena.
Part 02 reviews contemporary problems of healthcare industry primarily in the United States, intending to combine the research results of management science into healthcare sphere and to provoke how a healthcare facilities in future can be managed and constructed.
Part 03 includes a context study page in function and design of the existing Univer-sity of Florida Shands Complex and a guideline page of the accreditation systems of sustainable healthcare buildings. It also considers the possible future applica-tion of the concepts discussed, with a practical design project of Cardiovascular Center in UF Health Shands at University of Florida.
Part 04 contains the sustainable healthcare architecture strategem associated with the design proposal of UF Health Cardiovascular Center, which are concerned with hospital design trends of today and particularly with the evaluation of a scien-tifically contemporary standards for green buildings.
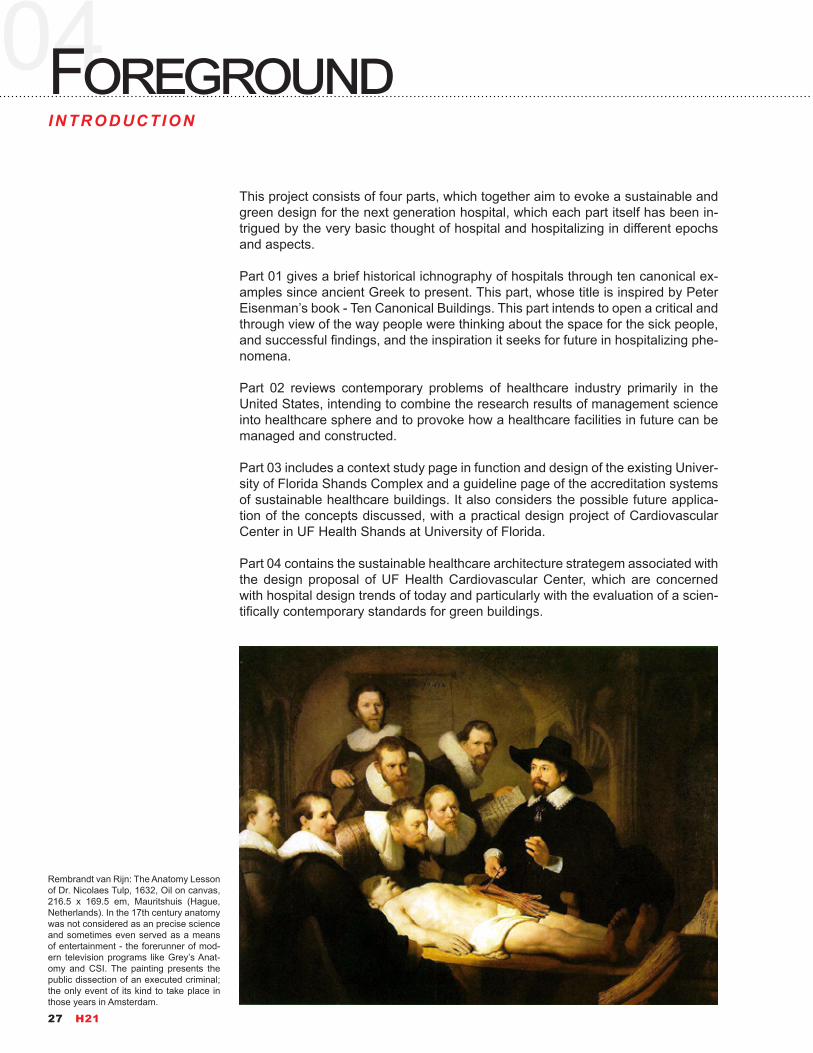
Rembrandt van Rijn: The Anatomy Lesson of Dr. Nicolaes Tulp, 1632, Oil on canvas, 216.5 x 169.5 em, Mauritshuis (Hague, Netherlands). In the 17th century anatomy was not considered as an precise science and sometimes even served as a means of entertainment - the forerunner of mod-ern television programs like Grey’s Anat-omy and CSI. The painting presents the public dissection of an executed criminal; the only event of its kind to take place in those years in Amsterdam.
27 H21
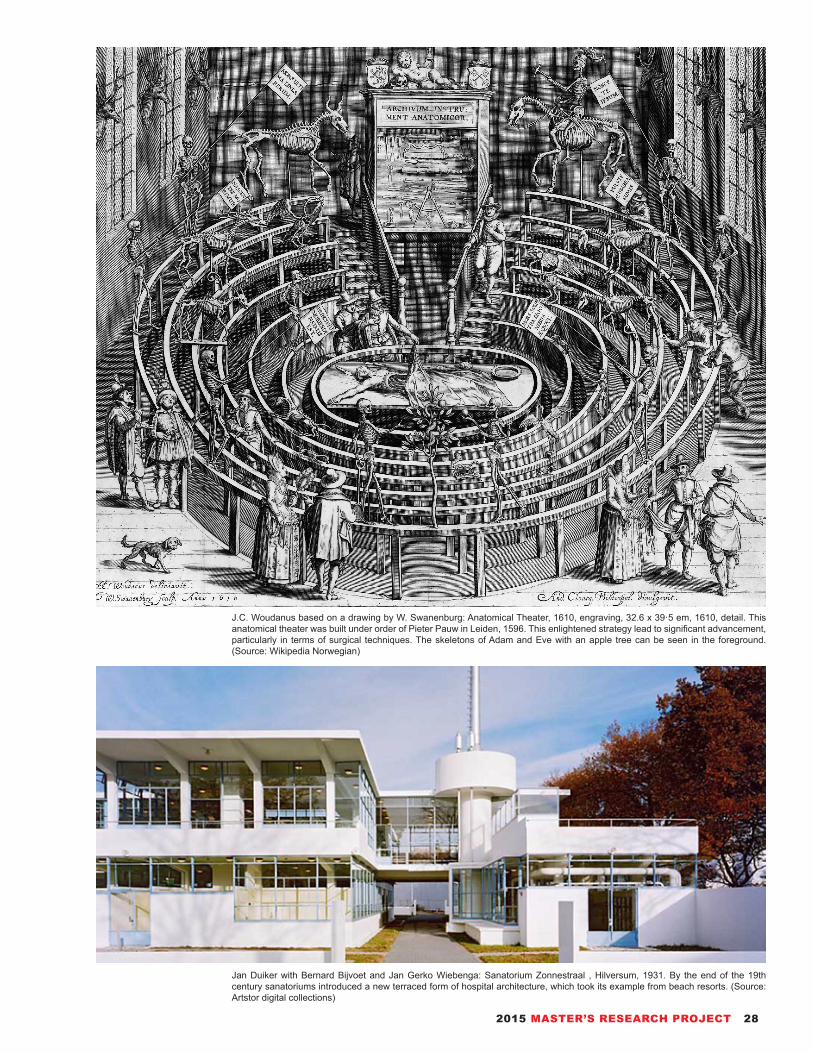
J.C. Woudanus based on a drawing by W. Swanenburg: Anatomical Theater, 1610, engraving, 32.6 x 39·5 em, 1610, detail. This anatomical theater was built under order of Pieter Pauw in Leiden, 1596. This enlightened strategy lead to significant advancement, particularly in terms of surgical techniques. The skeletons of Adam and Eve with an apple tree can be seen in the foreground. (Source: Wikipedia Norwegian)
Jan Duiker with Bernard Bijvoet and Jan Gerko Wiebenga: Sanatorium Zonnestraal , Hilversum, 1931. By the end of the 19th century sanatoriums introduced a new terraced form of hospital architecture, which took its example from beach resorts. (Source: Artstor digital collections)
2015 MASTER’S RESEARCH PROJECT 28

05EvolutionHISTORY
Hospitals are the oldest type of architecture as well as the newest type of architec-ture. The hospital or place of care for the sick has certainly its own evolution from ancient times to the modern. Being a descendant of almshouses, poorhouses, correctional facilities, and welfare centers, in many instances run by the church, the administrative line of the hospital shifts through eras. As requirements of these crucial facilities have grown, public authorities and companies have taken over the running of these care centers. But the ultimate goal remains, which is the attention to cure ill people as a vital component particularly.
The history of hospitals has stretched over 2500 years. This project has collected, illustrated, examined, criticized many historical examples. In the first part, a chro-nology of ten canonical hospitals tells the story of healthcare buildings as it nests within the history of humans: temples dedicated to the healer-god Asclepius in an-cient Greece, known as Asclepieia; to medieval monastery and infirmary at Cluny in France; to St Thomas’s and Guy’s Hospital in London in the Age of Enlighten-ment; to Hotel-Dieu de Paris rebuilding project; to Johns Hopkins Hospital in Balti-more as the sign of rising healthcare industry in new continent; to Paimio Sanato-rium designed by Alvar Aalto as the milestone of modernism; to Beaujon Hospital at Clichy near Paris being the mega-structure of rising medical departments; to the hospital ship of USS Mercy in World War Two which was built to meet intense needs; to Yale-New Haven Hospital as the classical model of post-war hospital design; to Lunder Building of Massachusetts General Hospital which is recognized by AIA in National Healthcare Design Awards in 2012.
On the other hand, with good reason, hospital is new in this time. After a long rela-tion with religion, in the mid 19th century, hospitals and the medical profession be-came more professionalized, with a reorganization of hospital management along more bureaucratic and administrative lines. That is the reason why in the Lunder Building project of Massachusetts General Hospital, the title was acclaimed as Building for the Third Century (B3C); indeed, modern hospital has existed for no more than two hundred years.
The distinction is observed between what we have defined derived and designed historic hospital plans. Designed hospitals were those in which an attempt was made to plan for the function of nursing care. In derived hospitals, the buildings were originally taken from châteaus, estates, monasteries, palaces, prisons, bar-racks, or they were consciously constructed in current architectural forms for any one of them. In a spirit of public civilizing, to be certain, but also with the aspiration of providing a lasting monument to the beneficence of the charitable founders, hospitals were required to meet more needs which are embodied in its plan. The success of a ward design depended until relatively recently on how well the build-ing form chosen adapted to nursing purposes. For example, the barracks form seemed to make for a better nursing unit than did a church or monastery.
Spanning from 1750 to 1850, saw the generation of two kinds of institutions: vol-untary hospitals, which were operated by charitable organizations, though com-monly affiliated with some Protestant religious body; and public hospitals, oper-ated by municipal or regional governments and developed from the almshouses
29 H21

Fa Xian, a Chinese Buddhist monk who travelled across India ca. 400 CE, recorded in his travelogue that healthcare for the ill also appeared early in India. -“The heads of the Vaisya (merchant) families in them (all the kingdoms of north India) establish in the cities houses for dispens-ing charity and medicine. All the poor and destitute in the country, orphans, widowers, and childless men, maimed people and cripples, and all who are diseased, go to those houses, and are provided with every kind of help, and doctors examine their diseases. They get the food and medicines which their cases require, and are made to feel at ease; and when they are better, they go away of themselves.”
maintained by many colonial communities. The second phase, which began during the middle nineteenth century and went to its end, witnessed the formation of “par-ticularistic” hospitals funded by religious or ethnic institutions. This period also saw the coming forth of specialized hospitals for women and for treating certain type of diseases. Also in this time, homeopaths and other members of medical sects opened their own specialized hospitals. In the last score of nineteenth century, planning for function took the upper hand. Finally, from 1890 and into the first thrity years of the twentieth century, profit-making hospitals came into operation, funded and run by corporations or by professional physician groups.
2015 MASTER’S RESEARCH PROJECT 30

In the last century, we have been raised to witness the unprecedented events like worldwide population increase, largest conflicts ever (WWI and WWII), second industrial revolution of information technology, of course many medical miracles. Medicine evolved from the relatively ineffectual, harmful and just palliation of ill-ness and injury to a system of effective, positive, life-prolonging intervention. That intervention has increasingly emphasized the component of diagnosis, so that the trend has been toward earlier intervention and, most recently, prevention or, as it is more accurately termed, “wellness.” Today’s medical technology, genetic re-search, keyhole surgery, and drug therapies hold the promise of not merely allay-ing suffering but also of avoiding it altogether-offered we can find a way to pay for the treatments, the diagnostics, and the drugs they present.
The etymology shows hospital that the linguistic root of the Latin word “hospes” is the same as those of hotel, hostel, hospitable, and hospitality. This meaning should connote the qualities expressed in the names the U.S. Navy has tradition-ally marked to hospital ships: comfort, hope, mercy. Contradictorily, there was a time that a response to hospitals means discomfort and anxiety. It is reasonable. In the days before antibiotic drugs and X-ray machines, before clean surgery room and anesthesia, hospitals were indeed places to be despised. Individuals gener-ally went to a hospital only because they could afford nothing better, like private physician or home treatment. And if a person did go to a hospital, it was very likely that he or she would not leave it alive.
William Simpson (artist, 1823–1899) E. Walker (lithographer, lifespan unknown, working for Day & Son), One of the wards of the hospital at Scutari, 1856, Lithograph, 28 x 44 cm, Library of Congress. Selimiye Barracks (Turkish: Selimiye Kışlası), also known as Scutari Barracks, is a Turkish army barracks located in the Üsküdar district on the Asian part of Istanbul, Turkey. During the Crimean War (1854-1856), the barracks were allocated to the British Army, which was on the way from Brit-ain to the Crimea. On November 4, 1854, Florence Nightingale arrived in Scutari with 38 volunteer nurses. This is a ward of the hospital at Scutari where Florence Nightingale worked and helped to restructure the modern hospital.
31 H21

New Columbia University Medical Building, designed by Diller Scofidio + Renfro. 2012Columbia University has been at the forefront of medical education for more than two centuries, as it was the first medical school in the United States to award the M.D. degree in 1770. Now, the Columbia University Medical Center (CUMC) has announced plans for a new, state-of-the-art medical and graduate education building that reflects how they believe medicine is and should be taught, learned and practiced in the 21st century.
2015 MASTER’S RESEARCH PROJECT 32

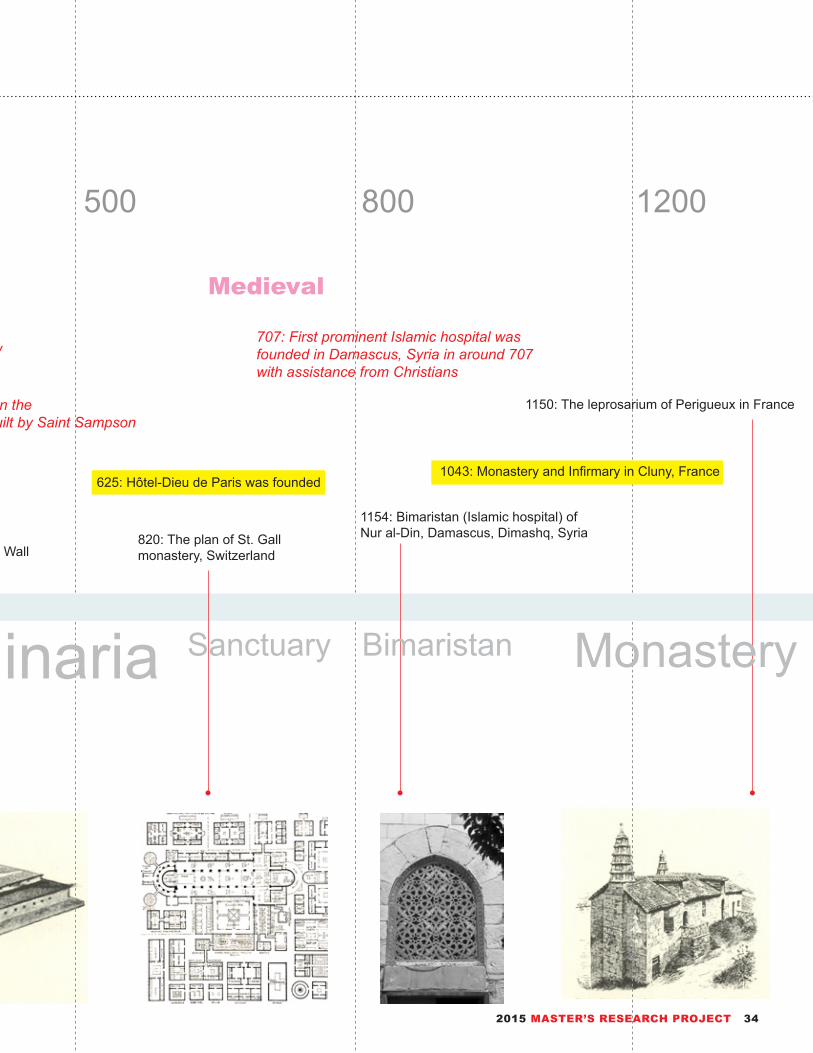
Temple Valetudinaria Sanctuary MonasteryOrigin Asclepieion Bimaristan
350 B.C.E.: Temples dedicated to the healer-god Asclepius, known as Asclepieia in ancient Greece 625: Hôtel-Dieu de Paris was founded
1043: Monastery and Infirmary in Cluny, France
400 B.C.E.: The record in his travelogue by Fa Xian is one of the earliest accounts of a civic hospital system anywhere in the world
1154: Bimaristan (Islamic hospital) of Nur al-Din, Damascus, Dimashq, Syria820: The plan of St. Gall
monastery, Switzerland55: Roman Valetudinarium (Military Hospital) in England (first century CE), as a part of Hadrian’s Wall
1150: The leprosarium of Perigueux in France
100: First public restroom - latrines, or necessaria, appeared in Asklepieion in now Turkey
325: Earliest hospitals in theRoman Empire were built by Saint Sampson the Hospitable
707: First prominent Islamic hospital was founded in Damascus, Syria in around 707 with assistance from Christians
400 C.E.: First description of a civic hospital system anywhere in the world
Classical Medieval
0 500 800 1200300 B.C.E.500 B.C.E.
06TrackALMANAC
33 H21
Temple Valetudinaria Sanctuary MonasteryOrigin Asclepieion Bimaristan
350 B.C.E.: Temples dedicated to the healer-god Asclepius, known as Asclepieia in ancient Greece 625: Hôtel-Dieu de Paris was founded
1043: Monastery and Infirmary in Cluny, France
400 B.C.E.: The record in his travelogue by Fa Xian is one of the earliest accounts of a civic hospital system anywhere in the world
1154: Bimaristan (Islamic hospital) of Nur al-Din, Damascus, Dimashq, Syria820: The plan of St. Gall
monastery, Switzerland55: Roman Valetudinarium (Military Hospital) in England (first century CE), as a part of Hadrian’s Wall
1150: The leprosarium of Perigueux in France
100: First public restroom - latrines, or necessaria, appeared in Asklepieion in now Turkey
325: Earliest hospitals in theRoman Empire were built by Saint Sampson the Hospitable
707: First prominent Islamic hospital was founded in Damascus, Syria in around 707 with assistance from Christians
400 C.E.: First description of a civic hospital system anywhere in the world
Classical Medieval
0 500 800 1200300 B.C.E.500 B.C.E.
2015 MASTER’S RESEARCH PROJECT 34

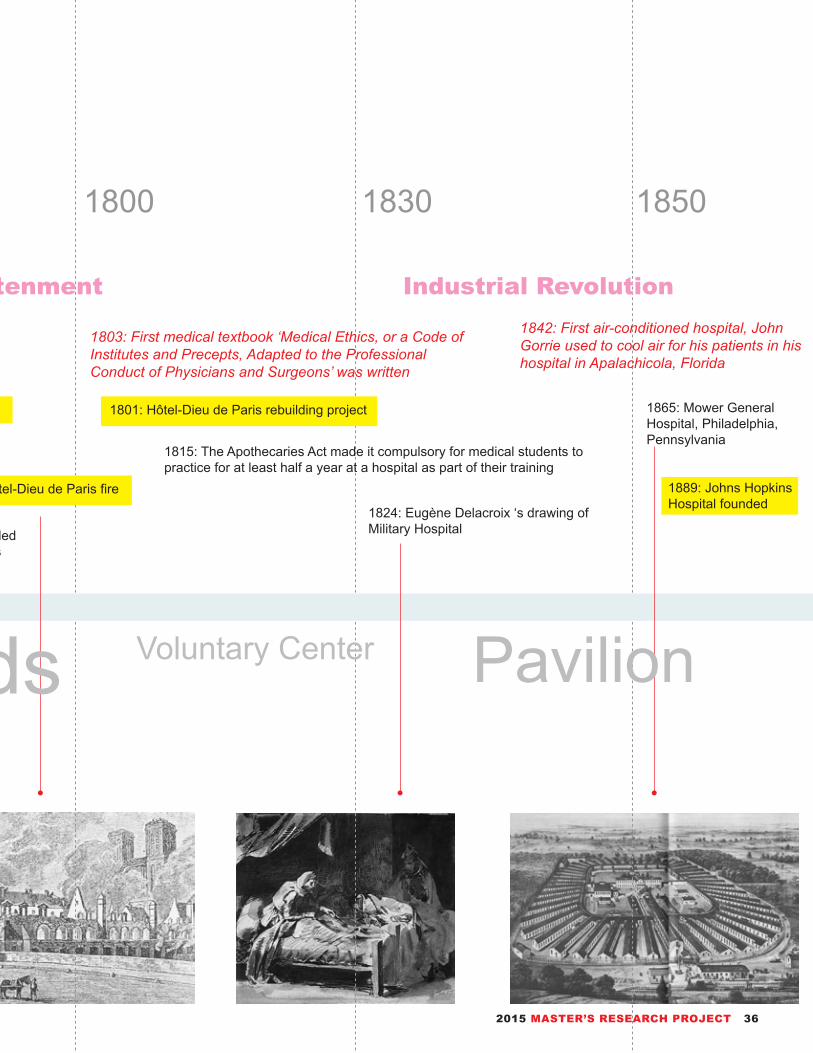
Open Hall Wards PavilionHôtel-Dieu Voluntary Center
1772: Hôtel-Dieu de Paris fire
1801: Hôtel-Dieu de Paris rebuilding project
1889: Johns Hopkins Hospital founded
1721: St Thomas' and Guy's hospitals founded 1865: Mower General Hospital, Philadelphia, Pennsylvania
1824: Eugène Delacroix ‘s drawing of Military Hospital1721: St Thomas' and Guy's hospitals was founded
by Thomas Guy, a publisher of unlicensed Bibles
1500: Episodes from the Life of a Bishop-Saint, by the Master of Saint Giles, showing the Gothic buildings of the Hotel Dieu at right.
1155: Kirkstall Abbey, England. Drain of the dormitory necessarium were built near water
1815: The Apothecaries Act made it compulsory for medical students to practice for at least half a year at a hospital as part of their training
1502: First hospital founded in the Americas - Hospital San Nicolás de Bari, in Dominican Republic
1842: First air-conditioned hospital, John Gorrie used to cool air for his patients in his hospital in Apalachicola, Florida
1803: First medical textbook ‘Medical Ethics, or a Code of Institutes and Precepts, Adapted to the Professional Conduct of Physicians and Surgeons’ was written
Renaissance Enlightenment Industrial Revolution
1700 1800 1830 185015001300
35 H21
Open Hall Wards PavilionHôtel-Dieu Voluntary Center
1772: Hôtel-Dieu de Paris fire
1801: Hôtel-Dieu de Paris rebuilding project
1889: Johns Hopkins Hospital founded
1721: St Thomas' and Guy's hospitals founded 1865: Mower General Hospital, Philadelphia, Pennsylvania
1824: Eugène Delacroix ‘s drawing of Military Hospital1721: St Thomas' and Guy's hospitals was founded
by Thomas Guy, a publisher of unlicensed Bibles
1500: Episodes from the Life of a Bishop-Saint, by the Master of Saint Giles, showing the Gothic buildings of the Hotel Dieu at right.
1155: Kirkstall Abbey, England. Drain of the dormitory necessarium were built near water
1815: The Apothecaries Act made it compulsory for medical students to practice for at least half a year at a hospital as part of their training
1502: First hospital founded in the Americas - Hospital San Nicolás de Bari, in Dominican Republic
1842: First air-conditioned hospital, John Gorrie used to cool air for his patients in his hospital in Apalachicola, Florida
1803: First medical textbook ‘Medical Ethics, or a Code of Institutes and Precepts, Adapted to the Professional Conduct of Physicians and Surgeons’ was written
Renaissance Enlightenment Industrial Revolution
1700 1800 1830 185015001300
2015 MASTER’S RESEARCH PROJECT 36

Radiology EscalationAntibioticsSkyscraper Modernism
1889: Johns Hopkins Hospital was founded, now it is regarded as one of the world's greatest hospitals
1932: Paimio Sanatorium designed by Finnish architect Alvar Aalto was completed
1944: USS Mercy (AH-8) was a Comfort-class hospital ship laid down under Maritime Commission
1884: Civil and Military Hospital, Montpellier, France, the transverse section shows the intake of fresh air
1950: Veterans Hospital in Brooklyn opened, which is designed by Skid-more, Owings & Merrill 1935: Beaujon Hospital located in Clichy, Paris opened
1931: Sanatorium Zonnestraal, was designed by Jan Duiker and is an example of the Nieuwe Bouwenit, it was built as a tuberculosis sanatorium
1895: First X-Ray Image, Wilhelm Conrad Röntgen accidentally discovered an image cast from his cathode ray generator
1945: First country to make the penicillin available for civilian use was Australia after World War II
1860: First official nurses’ training programme, theNightingale School for Nurses was opened
WWIIWWIModern Post-war
1920 1940 1945 19501900
37 H21

Radiology EscalationAntibioticsSkyscraper Modernism
1889: Johns Hopkins Hospital was founded, now it is regarded as one of the world's greatest hospitals
1932: Paimio Sanatorium designed by Finnish architect Alvar Aalto was completed
1944: USS Mercy (AH-8) was a Comfort-class hospital ship laid down under Maritime Commission
1884: Civil and Military Hospital, Montpellier, France, the transverse section shows the intake of fresh air
1950: Veterans Hospital in Brooklyn opened, which is designed by Skid-more, Owings & Merrill 1935: Beaujon Hospital located in Clichy, Paris opened
1931: Sanatorium Zonnestraal, was designed by Jan Duiker and is an example of the Nieuwe Bouwenit, it was built as a tuberculosis sanatorium
1895: First X-Ray Image, Wilhelm Conrad Röntgen accidentally discovered an image cast from his cathode ray generator
1945: First country to make the penicillin available for civilian use was Australia after World War II
1860: First official nurses’ training programme, theNightingale School for Nurses was opened
WWIIWWIModern Post-war
1920 1940 1945 19501900
2015 MASTER’S RESEARCH PROJECT 38

Information Energy DirectionEfficiency Sustainable Evidence
1965: Yale–New Haven Hospital was named as the result of a more formal agreement with the Yale School of Medicine
1951: Massachusetts General Hospital Research Laboratory constructed, and linked by corridor to the 1821 Bulfinch Building
2008: B3C - Building for the Third Century, of Massa-chusetts General Hospital commenced, marking a sustainable and green design for the future
2011: Pacific coast of Tōhoku earthquake near Japan opens a new challenge of mas-sive healthcare by information technology
1993: Hospital for Sick Children in Toronto of Canada, designed by Zeidler Roberts Partnership
1990: Shanghai's Number 1 Maternity hospi-tal, China, the intense population increase questions the existing hospital management
1979: Hospital: House of Hope, Houses of Birth, Houses of No Return drawn by Raimund Abraham
1978: First test tube baby were conceived by IVF, and born in Oldham General Hospital, Greater Manchester, UK
1996: First mammal, Dolly, cloned from an adult somatic cell using the process of nuclear transfer
1953: The structure of the DNA molecule was described by James Watson and Francis Crick at Cambridge University
Cold War GlobalizationSecond Industrial Revolution
1970 1990 2000 20111960
39 H21

Information Energy DirectionEfficiency Sustainable Evidence
1965: Yale–New Haven Hospital was named as the result of a more formal agreement with the Yale School of Medicine
1951: Massachusetts General Hospital Research Laboratory constructed, and linked by corridor to the 1821 Bulfinch Building
2008: B3C - Building for the Third Century, of Massa-chusetts General Hospital commenced, marking a sustainable and green design for the future
2011: Pacific coast of Tōhoku earthquake near Japan opens a new challenge of mas-sive healthcare by information technology
1993: Hospital for Sick Children in Toronto of Canada, designed by Zeidler Roberts Partnership
1990: Shanghai's Number 1 Maternity hospi-tal, China, the intense population increase questions the existing hospital management
1979: Hospital: House of Hope, Houses of Birth, Houses of No Return drawn by Raimund Abraham
1978: First test tube baby were conceived by IVF, and born in Oldham General Hospital, Greater Manchester, UK
1996: First mammal, Dolly, cloned from an adult somatic cell using the process of nuclear transfer
1953: The structure of the DNA molecule was described by James Watson and Francis Crick at Cambridge University
Cold War GlobalizationSecond Industrial Revolution
1970 1990 2000 20111960
2015 MASTER’S RESEARCH PROJECT 40

07ScopeSTATIST ICS
Hospital Bed Density (Hospital beds per 1,000 people)
In Monaco and Japan which are miles ahead in Hospital Beds Density, 1,000 people have 16.5 beds in hospital.
41 H21
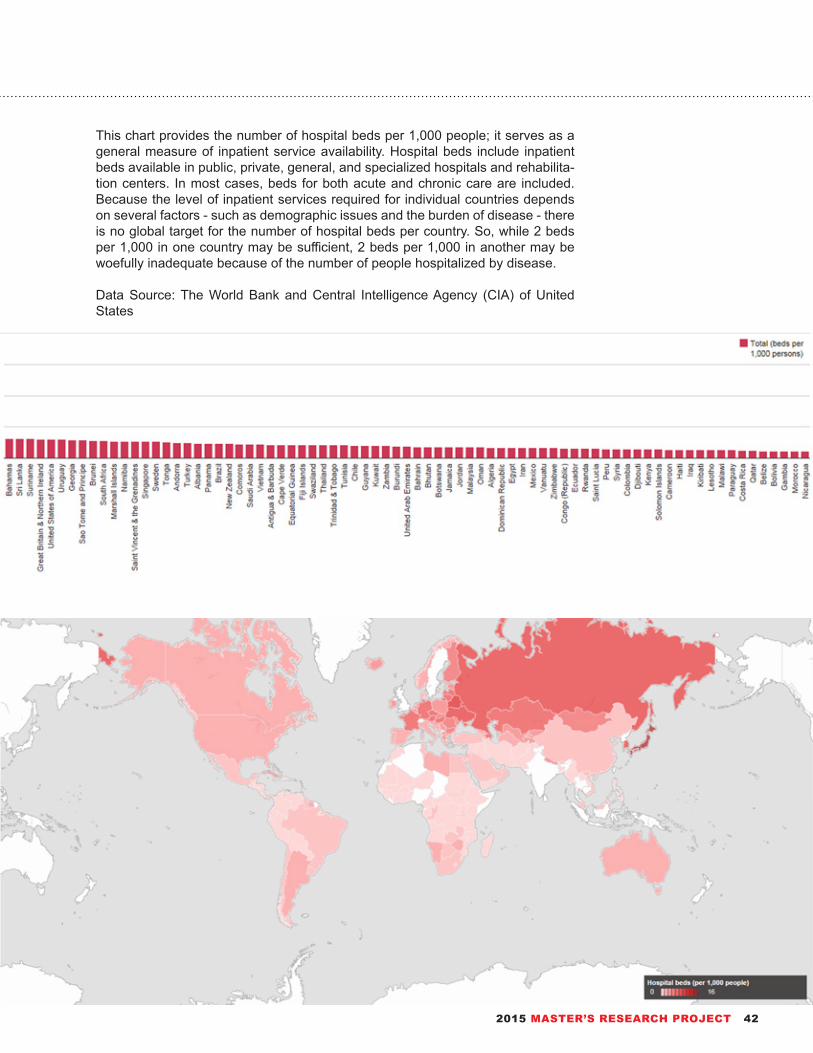
This chart provides the number of hospital beds per 1,000 people; it serves as a general measure of inpatient service availability. Hospital beds include inpatient beds available in public, private, general, and specialized hospitals and rehabilita-tion centers. In most cases, beds for both acute and chronic care are included. Because the level of inpatient services required for individual countries depends on several factors - such as demographic issues and the burden of disease - there is no global target for the number of hospital beds per country. So, while 2 beds per 1,000 in one country may be sufficient, 2 beds per 1,000 in another may be woefully inadequate because of the number of people hospitalized by disease.
Data Source: The World Bank and Central Intelligence Agency (CIA) of United States
2015 MASTER’S RESEARCH PROJECT 42
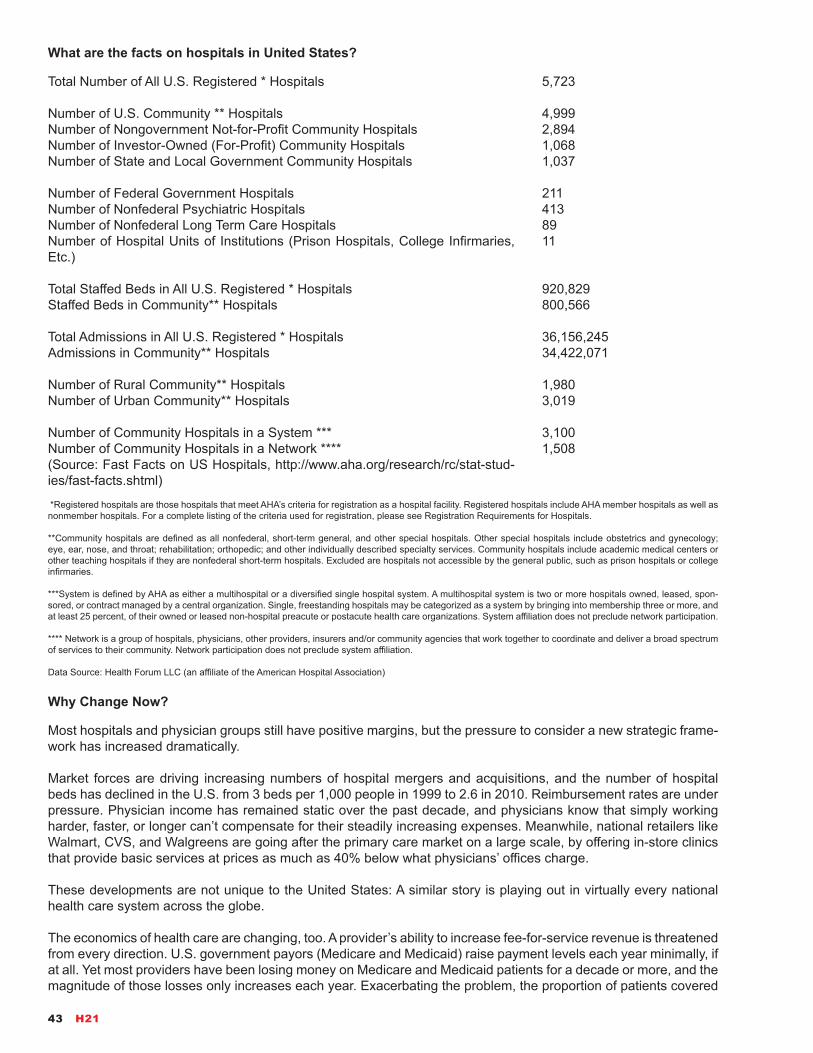
Total Number of All U.S. Registered * Hospitals
Number of U.S. Community ** HospitalsNumber of Nongovernment Not-for-Profit Community HospitalsNumber of Investor-Owned (For-Profit) Community HospitalsNumber of State and Local Government Community Hospitals
Number of Federal Government HospitalsNumber of Nonfederal Psychiatric Hospitals Number of Nonfederal Long Term Care HospitalsNumber of Hospital Units of Institutions (Prison Hospitals, College Infirmaries, Etc.)
Total Staffed Beds in All U.S. Registered * HospitalsStaffed Beds in Community** Hospitals
Total Admissions in All U.S. Registered * HospitalsAdmissions in Community** Hospitals
Number of Rural Community** HospitalsNumber of Urban Community** Hospitals
Number of Community Hospitals in a System ***Number of Community Hospitals in a Network ****(Source: Fast Facts on US Hospitals, http://www.aha.org/research/rc/stat-stud-ies/fast-facts.shtml)
5,723
4,999 2,894 1,068 1,037
211 4138911
920,829 800,566
36,156,245 34,422,071
1,980 3,019
3,1001,508
What are the facts on hospitals in United States?
*Registered hospitals are those hospitals that meet AHA’s criteria for registration as a hospital facility. Registered hospitals include AHA member hospitals as well as nonmember hospitals. For a complete listing of the criteria used for registration, please see Registration Requirements for Hospitals.
**Community hospitals are defined as all nonfederal, short-term general, and other special hospitals. Other special hospitals include obstetrics and gynecology; eye, ear, nose, and throat; rehabilitation; orthopedic; and other individually described specialty services. Community hospitals include academic medical centers or other teaching hospitals if they are nonfederal short-term hospitals. Excluded are hospitals not accessible by the general public, such as prison hospitals or college infirmaries.
***System is defined by AHA as either a multihospital or a diversified single hospital system. A multihospital system is two or more hospitals owned, leased, spon-sored, or contract managed by a central organization. Single, freestanding hospitals may be categorized as a system by bringing into membership three or more, and at least 25 percent, of their owned or leased non-hospital preacute or postacute health care organizations. System affiliation does not preclude network participation.
**** Network is a group of hospitals, physicians, other providers, insurers and/or community agencies that work together to coordinate and deliver a broad spectrum of services to their community. Network participation does not preclude system affiliation.
Data Source: Health Forum LLC (an affiliate of the American Hospital Association)
Why Change Now?
Most hospitals and physician groups still have positive margins, but the pressure to consider a new strategic frame-work has increased dramatically.
Market forces are driving increasing numbers of hospital mergers and acquisitions, and the number of hospital beds has declined in the U.S. from 3 beds per 1,000 people in 1999 to 2.6 in 2010. Reimbursement rates are under pressure. Physician income has remained static over the past decade, and physicians know that simply working harder, faster, or longer can’t compensate for their steadily increasing expenses. Meanwhile, national retailers like Walmart, CVS, and Walgreens are going after the primary care market on a large scale, by offering in-store clinics that provide basic services at prices as much as 40% below what physicians’ offices charge.
These developments are not unique to the United States: A similar story is playing out in virtually every national health care system across the globe.
The economics of health care are changing, too. A provider’s ability to increase fee-for-service revenue is threatened from every direction. U.S. government payors (Medicare and Medicaid) raise payment levels each year minimally, if at all. Yet most providers have been losing money on Medicare and Medicaid patients for a decade or more, and the magnitude of those losses only increases each year. Exacerbating the problem, the proportion of patients covered
43 H21

Health expenditure, public and private, as a share of GDP, OECD countries, 2012 or latest year
=
Expenses for all U.S. hospitals Gross domestic product (GDP) of the Republic of Turkey
How does the United States compare?
Health spending accounted for 16.9% of GDP in the United States in 2012 - the highest share among OECD coun-tries and more than 7½ percentage points above the OECD average of 9.3%. In contrast to most OECD countries, health spending in the United States is split evenly between public and private sources. In 2012, 48% of health spending in the United States was publicly financed, well below the average of 72% in OECD countries.
by government programs is growing: Medicaid will expand substantially in many states in 2014, as the Affordable Care Act is implemented, and the aging of the population will increase the percentage of Medicare patients for years beyond that. Reimbursement for these patients will continue to be pressured by tight federal and state government budgets. National Institutes of Health research cuts will make matters even worse for academic medical centers.
In the past, providers would cover losses from Medicare and Medicaid and from uninsured populations by demand-ing higher payment rates from commercial insurance plans—often winning increases of 8% to 10% per year. Those days are over. Employers are looking for decreases in their health care costs, and they’re getting them by engag-ing in price negotiations, reducing benefits, raising deductibles, and expanding “narrowed network” products that direct patients to providers that accept lower rates or prove better outcomes. A program recently introduced by the California Public Employees’ Retirement System (CalPERS) and Anthem Blue Cross, for example, requires many employees seeking a hip or knee replacement to use only hospitals that have agreed to a bundled fee for the pro-cedure—or to pay the difference if they choose a higher-priced provider outside the network.
The intensifying pressure from employers and insurers for transparent pricing is already beginning to force provid-ers to explain—or eliminate—hard-to-justify price variations. In our state, Massachusetts, the price for a brain MRI ranges from $625 to $1,650. And prices can vary by more than 50% for the same procedure in the same hospital, depending on the patient’s insurer and the insurance product.
Patients will be asked to pay more and more. The percentage of the population in high-deductible health plans is now well into double digits, and it is rising. Many employees in these plans are increasingly unwilling or are simply unable to pay historical charges, and providers incur losses or bad publicity, or both, as they try to collect on the debts.(Direct Citation Source: The Strategy That Will Fix Health Care by Michael E. Porter and Thomas H. Lee, https://hbr.org/2013/10/the-strategy-that-will-fix-health-care/)
2015 MASTER’S RESEARCH PROJECT 44

0
100
200
300
400
500
600
Sour
ce E
UI (
kBtu
/ft
2 ) PM Median Source EUI
National Median Source EUI
Some building types excluded due to inadequate data and/or EUI values beyond this range
Median Source EUI
08CrisisCHALLENGES AND D ILEMMAS
Hospitals - No.2 Energy Intensive Building
Energy use intensity (EUI) varies widely among buildings. One of the key contrib-uting factors is building activity. Supermarkets have relatively high EUI due to re-frigeration loads, while warehouses, with less equipment and fewer workers, tend to have low EUI. The median EUIs in Portfolio Manager are similar to the median EUIs derived from the Department of Energy’s nationally representative Commer-cial Building Energy Consumption Survey (CBECS), which forms the basis of most of the ENERGY STAR energy performance scales. These scales produce a 1-to-100 peer group comparison, accounting for differences in climate and business activities.
“Health care is a terminal illness for America’s governments and businesses. We are in big trouble.”“Perhaps most discouraging of all, however, is that there is no credible map of the terrain ahead that reformers agree upon and trust.”- Clayton Christensen, in the book of The Innovator’s Prescription.
Each median represents the value in the middle of a distribution, but the full range of energy use within each property type can be much larger, as shown in the figure below for School, Office, and Hospital. Hospitals have the highest median of these three, and also the largest range. The EUI values for Office and School are less widely distributed.
What is Source Energy?Source energy is the amount of raw fuel required to operate your building. In addi-tion to what you use onsite, source energy includes losses from generation, transmis-sion, and distribution of energy. Source energy enables the most complete and equitable energy assessment.
45 H21

0%
5%
10%
15%
20%
25%
Perc
ent o
f Bui
ldin
gs
Source EUI (kBtu/ft 2)
School
O�ce
Hospital
Range of Source EUI
Data Source: Energy StarENERGY STAR is a U.S. Environmental Protection Agency (EPA) voluntary pro-gram that helps businesses and individu-als save money and protect our climate through superior energy efficiency.
References1. Thompson, John D., and Grace Goldin. 1975. The hospital: a social and architectural history. New Haven: Yale University Press.
2. Christensen, Clayton M., Jerome H. Grossman, and Jason Hwang. 2009. The innovator’s prescription: a disruptive solution for health care. New York: McGraw-Hill.
3. Nickl-Weller, Christine, and Hans Nickl. 2013. Hospital architecture. [Salenstein, Switzerland]: Braun.
4. Miller, Richard L., Earl S. Swensson, and J. Todd Robinson. 2012. Hospital and healthcare facility design. New York: W.W Norton & Co.
5. “History of hospitals,” last modified February 6, 2015, http://en.wikipedia.org/wiki/History_of_hospitals
6. “Timeline of medicine and medical technology,” last modified February 3, 2015, http://en.wikipedia.org/wiki/Timeline_of_medicine_and_medical_technology
7. “What is energy use intensity (EUI)?” last modified February 6, 2015, http://www.energystar.gov/buildings/facility-owners-and-managers/existing-buildings/use-portfolio-manager/understand-metrics/what-energy
8. “History of Public Hospitals in the United States,” last modified February 6, 2015, http://essentialhospitals.org/about-americas-essential-hospitals/history-of-public-hospitals-in-the-united-states/
9. “History of Hospitals,” last modified February 6, 2015, http://www.nursing.upenn.edu/nhhc/Pages/History%20of%20Hospitals.aspx
10. “Hospital,” last modified February 6, 2015, http://en.wikipedia.org/wiki/Hospital
11. “Hospital beds (per 1,000 people),” last modified January 9, 2012, http://data.worldbank.org/indicator/SH.MED.BEDS.ZS/countries/1W?display=default
12. “Fast Facts on US Hospitals,” last modified March 11, 2014, http://www.aha.org/research/rc/stat-studies/fast-facts.shtml
13. “Health Costs: How the U.S. Compares With Other Countries,” last modified October 20, 2012, http://www.pbs.org/newshour/rundown/health-costs-how-the-us-compares-with-other-countries/
2015 MASTER’S RESEARCH PROJECT 46
“When we are tired, we are attacked by ideas we conquered long ago.”
Friedrich Nietzsche,The Will to Power, 1880
PART 147 H21

09Examples10 CANONICAL HOSPITALS
The ten hospitals chosen for discussion were impor-tant, or in some means, making it better. Each hospital examined in general or in some details does represent the way people were thinking about the Space for the sick at that time and that place.
The method of “cutting history” applied in this part were developed from Peter Eisenman’s didactic and unorth-odox notion in the book of Ten Canonical Buildings. In many instances beyond the ten, other examples from different regions might serve as well but the ten are chosen because reliable information about them was relatively easy to come by, because they could intrigue the design of next generation hospital by certain as-pects, because they place the positive attention closer to Michel Foucault’s idea of “effective history”, “bias”, “misinterpretation” than to the eternal value of the art of canonical edifices.
Illness is anxiety provoking. It is exactly those quali-ties of serene, relaxing and reliability that should be evoked by the space of healthcare facilities. In this sense, Rodney M. Coe concludes of the “meaning of hospitalization” in his Sociology of Medicine (1970) still hits the core, even forty years later:
“Many... attributes of illness may be carried over to the hospital situation and, perhaps, even exaggerated by some features of the hospital. In the first place, the hospital is a strange environment for most people. It has different sounds and smells than the environ-ments to which most of us are accustomed. There is a sort of “air of emergency” about the place as doctors, nurses, and other uniformed personnel move rapidly
from one place to another... (There is also) the threat-ened disruption of normal roles-particularly separation from the family and from the work role”.
“The onset of illness is... an intensely personal mat-ter calling for personalized or supportive responses from the personal community in the form of expressed concern and succorant behavior. Under ordinary cir-cumstances, this would likely be the type of response elicited from family members and friends. When the sick person is removed from the home setting and ad-mitted to the hospital, he is not only deprived of these primary-oriented responses, but also exposed to a se-ries of interactions with others which are characterized as objective and impersonal. They may range from the somewhat bureaucratic, officious behavior of admit-ting clerks and other administrative personnel to the professional scientific aplomb of nurses and examin-ing physicians”.
These cross-era hospitals exhibited in this part dem-onstrate a diverse understanding of the places of healing. Through instances, this observation therefore facilitates a panoramic comparison between the vari-ous projects: How will the ideologies steer the shifts of hospital architecture? What positions did or does hospital architecture occupy in past and today? What factors that enable architects to tackle the challenges facing influential aspects? How did hospital planning satisfy the growing needs and demands of the users? Those questions make an attempt to trace the canoni-cal moments in the development of hospitals.
2015 MASTER’S RESEARCH PROJECT 48

10TempleGREEK ASKLEPIE IALocation: Epidauros, ancient GreeceFounding Year: 350 B.C.E.
Greek Asklepieia (sing. Asclepieion) were places for inpatient nursing, includ-ing bed rest, medication, bath, treatments, diet, and exercise, and a number of floor plans of the large halls were discovered in which patients gathered to dream their dreams. The plan on right shows the double hall for dreamer-patients at the Asklepieion of Athens, founded fifth century B.C. The rooms were 24 feet deep by 108 and 96 feet long and completely closed on three sides and opening to the south with a row of columns,the typical form of a Greek stoa (portico)-oriented to the sun. At that time, the whole part of treatment is whatever a patient dreamed that the god Asklepios told him to do. The architectural forms of thus gathering space for the sick may affect later building, in this sense determining the layout of large medical wards. Asklepieia naturally did not lack latrines, or necesaria as they were aptly called in the Middle Ages, which can be considered as the prototype of public bathrooms in Europe.
The retaining wall on the 1st terrace of the Asklepie-ion photographed from the southeast corner, with statue fragments ornamenting the grounds.
49 H21
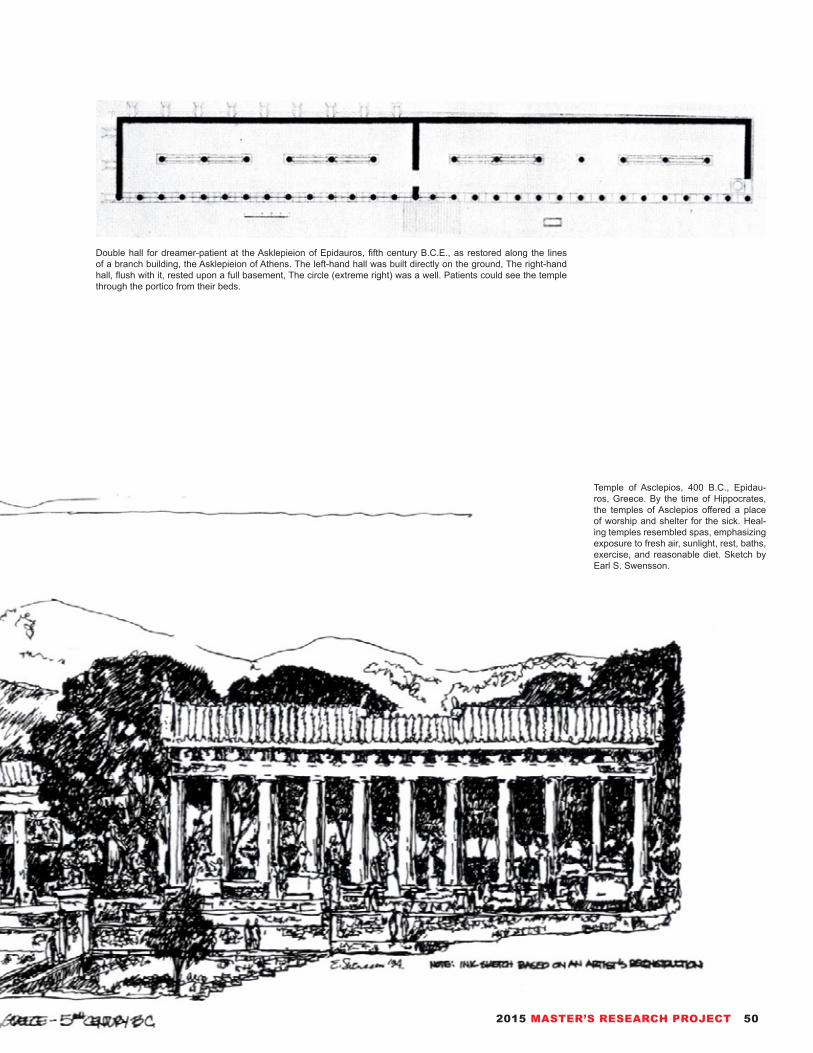
Double hall for dreamer-patient at the Asklepieion of Epidauros, fifth century B.C.E., as restored along the lines of a branch building, the Asklepieion of Athens. The left-hand hall was built directly on the ground, The right-hand hall, flush with it, rested upon a full basement, The circle (extreme right) was a well. Patients could see the temple through the portico from their beds.
Temple of Asclepios, 400 B.C., Epidau-ros, Greece. By the time of Hippocrates, the temples of Asclepios offered a place of worship and shelter for the sick. Heal-ing temples resembled spas, emphasizing exposure to fresh air, sunlight, rest, baths, exercise, and reasonable diet. Sketch by Earl S. Swensson.
2015 MASTER’S RESEARCH PROJECT 50

11SanctuaryINF IRMARY OF MONASTERY IN CLUNYLocation: Cluny, FranceConstruction Completed Year: 1050Replacement Year: 1750
Cluny monastery around 1157, as resorted by Kenneth J. Conant, (a) Infirmaries of St. Hugh (longitudinal section) and Peter the Venerable (long side); (b) infirmary of Peter the Venerable: left, cross section with (A) privy seat and (B) drain; right; western elevation.
Bird’s eye view of the entire mon-astery with (A) infirmary of Peter the Venerable; (A1) its necessa-rium; (B) infirmary of St. Hugh; (B1) its necessarium.
In the monastery at Cluny the infirmary evolved from a long building subdivided into four rooms into a grand open hall, a dominant form of ward construction under religious until the eighteenth century. Increased size of important rooms reflects a growing security and prosperity after the chaos and destruction of the Medieval Ages. The restored ground plan shows the inner structure of this infirmary: the latrines, the four rooms (23’ x 27’), and the mandatum (kitchen) for special foods, which have been brought together in one structure. This monastery were built near water, and streams were diverted to feed the fountains and flush the sewers. The relatioriship between privy seat and sewer shows particularly well in cross section of the infirmary.
51 H21
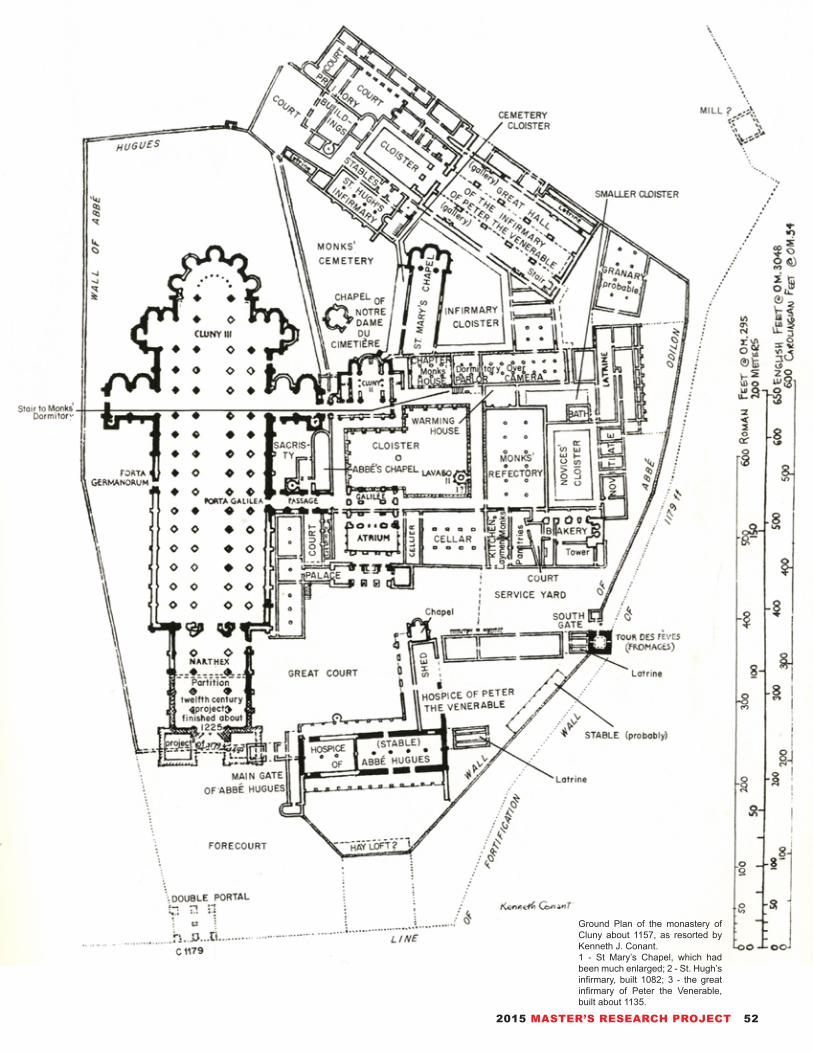
Ground Plan of the monastery of Cluny about 1157, as resorted by Kenneth J. Conant.1 - St Mary’s Chapel, which had been much enlarged; 2 - St. Hugh’s infirmary, built 1082; 3 - the great infirmary of Peter the Venerable, built about 1135.
2015 MASTER’S RESEARCH PROJECT 52
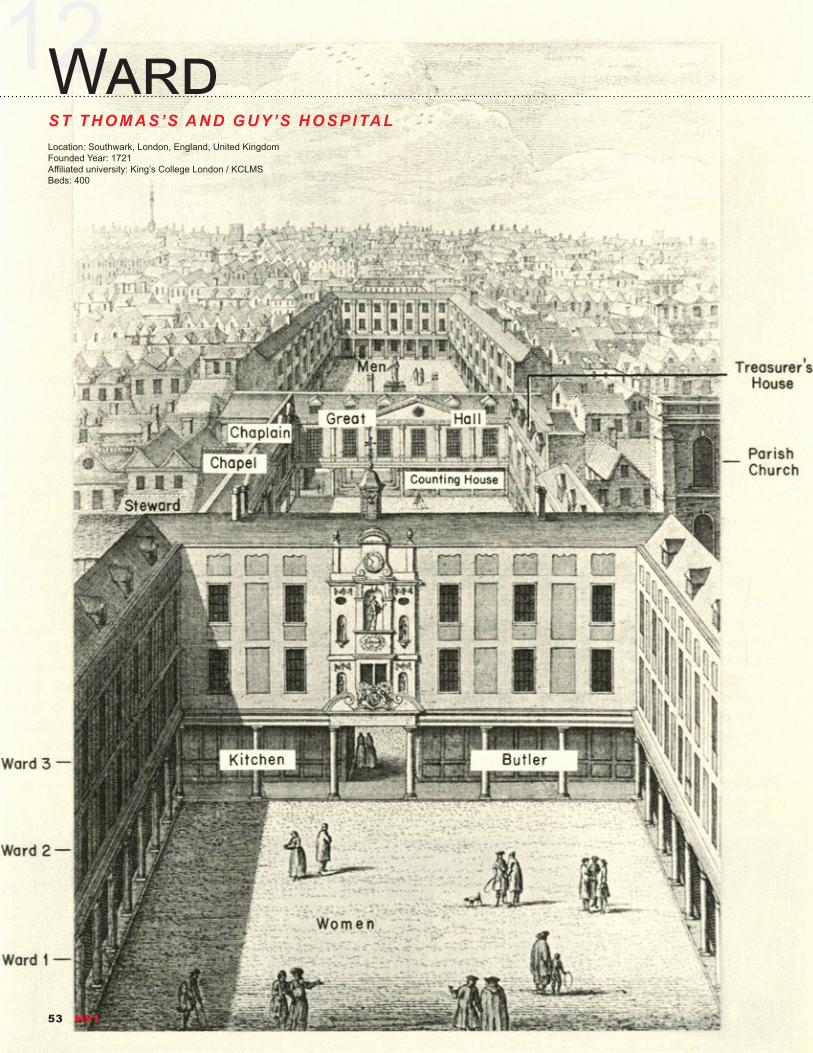
12WardST THOMAS’S AND GUY’S HOSPITALLocation: Southwark, London, England, United KingdomFounded Year: 1721Affiliated university: King’s College London / KCLMSBeds: 400
53 H21
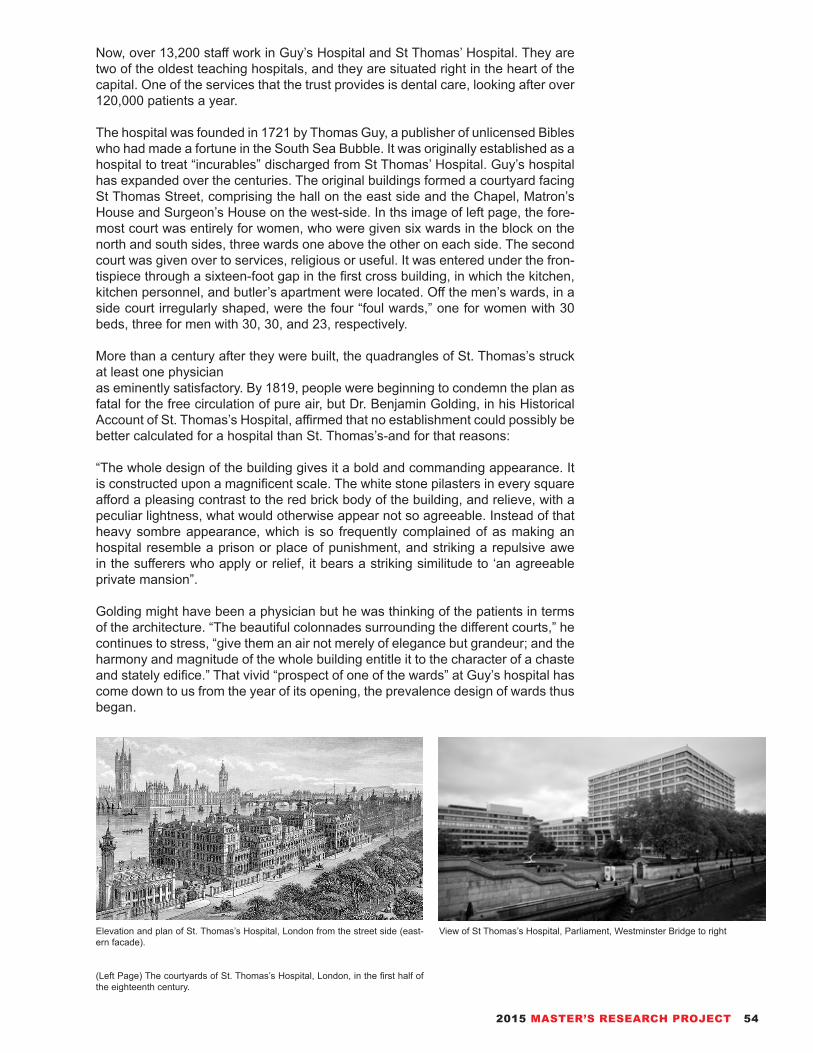
View of St Thomas’s Hospital, Parliament, Westminster Bridge to rightElevation and plan of St. Thomas’s Hospital, London from the street side (east-ern facade).
(Left Page) The courtyards of St. Thomas’s Hospital, London, in the first half of the eighteenth century.
Now, over 13,200 staff work in Guy’s Hospital and St Thomas’ Hospital. They are two of the oldest teaching hospitals, and they are situated right in the heart of the capital. One of the services that the trust provides is dental care, looking after over 120,000 patients a year.
The hospital was founded in 1721 by Thomas Guy, a publisher of unlicensed Bibles who had made a fortune in the South Sea Bubble. It was originally established as a hospital to treat “incurables” discharged from St Thomas’ Hospital. Guy’s hospital has expanded over the centuries. The original buildings formed a courtyard facing St Thomas Street, comprising the hall on the east side and the Chapel, Matron’s House and Surgeon’s House on the west-side. In ths image of left page, the fore-most court was entirely for women, who were given six wards in the block on the north and south sides, three wards one above the other on each side. The second court was given over to services, religious or useful. It was entered under the fron-tispiece through a sixteen-foot gap in the first cross building, in which the kitchen, kitchen personnel, and butler’s apartment were located. Off the men’s wards, in a side court irregularly shaped, were the four “foul wards,” one for women with 30 beds, three for men with 30, 30, and 23, respectively.
More than a century after they were built, the quadrangles of St. Thomas’s struck at least one physicianas eminently satisfactory. By 1819, people were beginning to condemn the plan as fatal for the free circulation of pure air, but Dr. Benjamin Golding, in his Historical Account of St. Thomas’s Hospital, affirmed that no establishment could possibly be better calculated for a hospital than St. Thomas’s-and for that reasons:
“The whole design of the building gives it a bold and commanding appearance. It is constructed upon a magnificent scale. The white stone pilasters in every square afford a pleasing contrast to the red brick body of the building, and relieve, with a peculiar lightness, what would otherwise appear not so agreeable. Instead of that heavy sombre appearance, which is so frequently complained of as making an hospital resemble a prison or place of punishment, and striking a repulsive awe in the sufferers who apply or relief, it bears a striking similitude to ‘an agreeable private mansion”.
Golding might have been a physician but he was thinking of the patients in terms of the architecture. “The beautiful colonnades surrounding the different courts,” he continues to stress, “give them an air not merely of elegance but grandeur; and the harmony and magnitude of the whole building entitle it to the character of a chaste and stately edifice.” That vivid “prospect of one of the wards” at Guy’s hospital has come down to us from the year of its opening, the prevalence design of wards thus began.
2015 MASTER’S RESEARCH PROJECT 54

13PavilionHÔTEL-D IEU DE PARISLocation: Paris, FranceFounded Year: 651Latest Rebuilding: 1877Beds: 349
Plan of the Hôtel-Dieu de Paris by Poyet, end of the eighteenth century, showing its relation to the Siene and the Cathedral of Notre Dame.
Plan of bed areas on the ground floor of the Hôtel-Dieu de Paris before the fire of 1772. All courts are numberd 13.
A comprehensive view of the Hôtel-Dieu de Paris, from the Turgot plan of Paris, 1739.
Wards of the derived hospital plans mentioned in the prior chapter might have been rendered more sanitary by careful supervision, but they were not designed primarily to serve sanitary purposes. The Pavilion, however, when used for wards is embodied with a sanitary code in a building. Pavilion in this sense means an open ward, but of limited extent; ventilated on both long sides by windows, on both short sides by doors; connected to a corridor that serves similar pavilions, but self-contained with its own service rooms. This type of ward came into use in the middle of the nineteenth century and the last examples are just vanishing in late tewntieth century. For more than a hundred years the pavilion was the dominant ward form.
55 H21
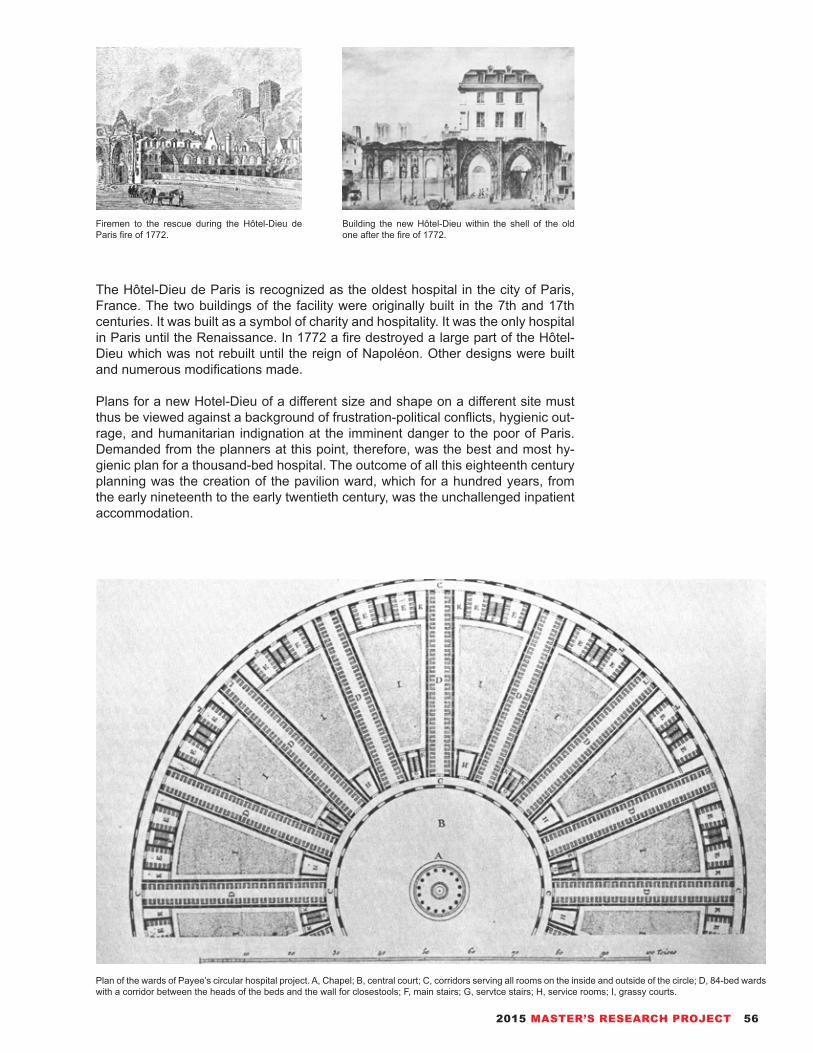
Firemen to the rescue during the Hôtel-Dieu de Paris fire of 1772.
Building the new Hôtel-Dieu within the shell of the old one after the fire of 1772.
Plan of the wards of Payee’s circular hospital project. A, Chapel; B, central court; C, corridors serving all rooms on the inside and outside of the circle; D, 84-bed wards with a corridor between the heads of the beds and the wall for closestools; F, main stairs; G, servtce stairs; H, service rooms; I, grassy courts.
The Hôtel-Dieu de Paris is recognized as the oldest hospital in the city of Paris, France. The two buildings of the facility were originally built in the 7th and 17th centuries. It was built as a symbol of charity and hospitality. It was the only hospital in Paris until the Renaissance. In 1772 a fire destroyed a large part of the Hôtel-Dieu which was not rebuilt until the reign of Napoléon. Other designs were built and numerous modifications made.
Plans for a new Hotel-Dieu of a different size and shape on a different site must thus be viewed against a background of frustration-political conflicts, hygienic out-rage, and humanitarian indignation at the imminent danger to the poor of Paris. Demanded from the planners at this point, therefore, was the best and most hy-gienic plan for a thousand-bed hospital. The outcome of all this eighteenth century planning was the creation of the pavilion ward, which for a hundred years, from the early nineteenth to the early twentieth century, was the unchallenged inpatient accommodation.
2015 MASTER’S RESEARCH PROJECT 56

14SkyscraperJOHNS HOPKINS HOSPITALLocation: 600 N. Wolfe St, Baltimore, Maryland, United States Founded Year: 1889Beds: 1059
First plan fro Johns Hopkins Hospital, 1876 Drawing of Johns Hopkins Hospital, 1900
In American civil war, barracks saved lives. Tents prevented the spread of infec-tion. The military solution for hospital building seemed the most workable one at all. Then how it can work in permanent structures. Block hospitals and pavilions in Europe were liable to become infected and dangerous. At this juncture the city of Baltimore was offered a university and a hospital. It was founded using money from a bequest by philanthropist Johns Hopkins. The Johns Hopkins Hospital and the Johns Hopkins School of Medicine are the founding institutions of modern Ameri-can medicine and are the birthplace of numerous traditions including rounds, resi-dents and housestaff. Many medical specialties were formed at the Johns Hopkins Hospital, including neurosurgery, cardiac surgery, pediatrics and child psychiatry.
The plan were nothing if not symmetrical: an administration building in the center of the facade with an apothecary building behind it; the two pay wards, one for women and one for men, to either side of the facade; a square kitchen behind them to the left balancing the square nurses’ home behind them to the right; and running back into the lot on either side an octagon ward, three common wards, and an isolating ward. To remove foul air from the ward two series of outlets were used. Both are clearly visible in the view of the ward interior (image on upper right) and that of the longitudinal section (image on lower right). The three-layered cor-ridor connected the pavilions; its open sun deck was at the level of the wards. The absence of elevators was a deliberate choice. Patients were carried upstairs from the covered corridor at ground level on stretchers, and the stairs from below did not emerge in the ward itself but at a covered section of the open corridor.
At this time, Johns Hopkins represents the bridge between pavilions to high rise buildings. Nineteenth-century scientific advances, real breakthroughs to under-standing the causes of disease, were not fully understood in their time and only in the twentieth century were they translated into changes in hospital design.
57 H21

Johns Hopkins Hospital interior, common ward(Source: Johns Hopkins Nursing)
Longitudinal section north and south, common ward Johns Hopkins Hospital began one of the nation’s largest hospital construction proj-ects: the Sheikh Zayed Cardiovascular and Critical Care Tower and The Charlotte R. Bloomberg Children’s Center in 2008 (Source: (a) biotic design studio)
2015 MASTER’S RESEARCH PROJECT 58

15ModernismPAIMIO SANATORIUMLocation: Paimio, Finland ProperConstruction Completed Year: 1932Architect: Alvar Aalto
Main Entrance of Paimio Sanatorium
59 H21

Paimio Sanatorium is a former tuberculosis sanatorium in Paimio, Finland Proper, designed by Finnish architect Alvar Aalto. The building was completed in 1932, and soon after received critical acclaim both in Finland and abroad. The building served exclusively as a tuberculosis sanatorium until the early 1960s, when it was converted into a general hospital. Today the building is part of the Turku University Hospital. The sanatorium was nominated to become a UNESCO World Heritage Site.
Aalto’s starting point for the design of the sanatorium was to make the building itself a contributor to the healing process. He liked to call the building a “medical instrument”. For instance, particular attention was paid to the design of the patient bedrooms: these generally held two patients, each with his or her own cupboard and washbasin. Aalto designed special non-splash basins, so that the patient would not disturb the other while washing. The patients spent many hours lying down, and thus Aalto placed the lamps in the room out of the patients line of vision and painted the ceiling a relaxing dark green so as to avoid glare. Each patient had their own specially designed cupboard, fixed to the wall and off the floor so as to aid in cleaning beneath it.
In the early years the only known “cure” for tuberculosis was complete rest in an environment with clean air and sunshine. Thus on each floor of the building, at the end of the patient bedroom wing, were sunning balconies, where weak pa-tients could be pulled out in their beds. Healthier patients could go and lie on the sun deck on the very top floor of the building. As the patients spent a long time—typically several years—in the sanatorium, there was a distinct community atmosphere among both staff and patients; something which Aalto had taken into account in his designs, with various communal facilities, a chapel, as well as staff housing, and even specially laid out promenade routes through the surrounding forest landscape. In the 1950s the disease could be partly dealt with by surgery and thus a surgery wing, also designed by Aalto, was added. Soon after, antibiot-ics saw the virtual end of the disease, and the number of patients was reduced dramatically and the building was converted into a general hospital.
Corridor near Main Laboratories Top Garden for Rehabilitation
2015 MASTER’S RESEARCH PROJECT 60
16ComplexityBEAUJON HOSPITAL AT CL ICHYLocation: Clichy, Paris, France Founded Year: 1935 Architect: Jean Walter
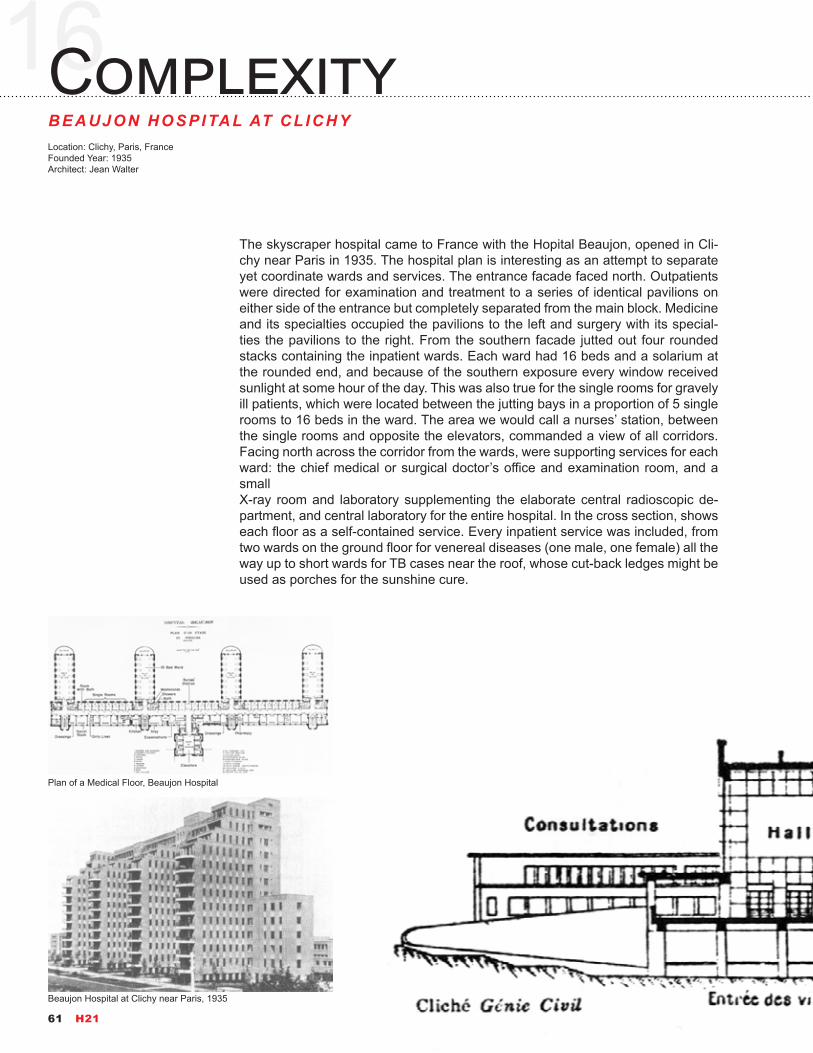
Plan of a Medical Floor, Beaujon Hospital
Beaujon Hospital at Clichy near Paris, 1935
The skyscraper hospital came to France with the Hopital Beaujon, opened in Cli-chy near Paris in 1935. The hospital plan is interesting as an attempt to separate yet coordinate wards and services. The entrance facade faced north. Outpatients were directed for examination and treatment to a series of identical pavilions on either side of the entrance but completely separated from the main block. Medicine and its specialties occupied the pavilions to the left and surgery with its special-ties the pavilions to the right. From the southern facade jutted out four rounded stacks containing the inpatient wards. Each ward had 16 beds and a solarium at the rounded end, and because of the southern exposure every window received sunlight at some hour of the day. This was also true for the single rooms for gravely ill patients, which were located between the jutting bays in a proportion of 5 single rooms to 16 beds in the ward. The area we would call a nurses’ station, between the single rooms and opposite the elevators, commanded a view of all corridors. Facing north across the corridor from the wards, were supporting services for each ward: the chief medical or surgical doctor’s office and examination room, and a smallX-ray room and laboratory supplementing the elaborate central radioscopic de-partment, and central laboratory for the entire hospital. In the cross section, shows each floor as a self-contained service. Every inpatient service was included, from two wards on the ground floor for venereal diseases (one male, one female) all the way up to short wards for TB cases near the roof, whose cut-back ledges might be used as porches for the sunshine cure.
61 H21

Longitudinal section of service floors and facade of one ward bay, Beaujon Hospital. From left to right: consultation rooms; visitors’ entrance (under the auditorium); stairs and elevators; the services, taking up one or more floors: maternity; surgery; medicine; eye, ear, nose, and throat; tuberculosis.
2015 MASTER’S RESEARCH PROJECT 62

17MobilityUSS MERCY AH-8Builder: Consolidated Steel Corporation, Wilmington, Los Angeles, CaliforniaLaunched Year: 25 March 1943Decommissioned Year: 17 May 1946Capacity: 400 patients
USS Mercy, a 11,250 ton (limiting displacement) hospital ship, was built under Maritime Commission contract at Wilmington, California, as a freighter. She was acquired by the Navy when launched in March 1943, and converted to a hospital ship at San Pedro, California. The new ship was commissioned in August 1944, and began a voyage to the south Pacific at the end of that month. In October she went to the Philippines to evacuate casualties of the invasion of Leyte and the Battle of Leyte Gulf, and continued this work well into the next year. During April and May 1945 Mercy transported casualties from Okinawa to the Marianas. She then returned to the Philippines for more evacuation missions and, for nearly two months beginning in mid-June, was station hospital ship in Manila Bay. Following Japan’s decision to surrender in August 1945, Mercy carried a hospital unit to Ko-rea for occupation service. She returned to the United States in November 1945 and made a final round-trip voyage to the central Pacific between early February and early April 1946.
USS Mercy (AH-8) Photos(Source: Department of the Navy--Naval History and Heritage Command)
63 H21

2015 MASTER’S RESEARCH PROJECT 64
18EfficiencyYALE-NEW HAVEN HOSPITALLocation: New Haven, Connecticut, United StatesFounded Year: 1826Affiliation Year: 1965Beds: 1541
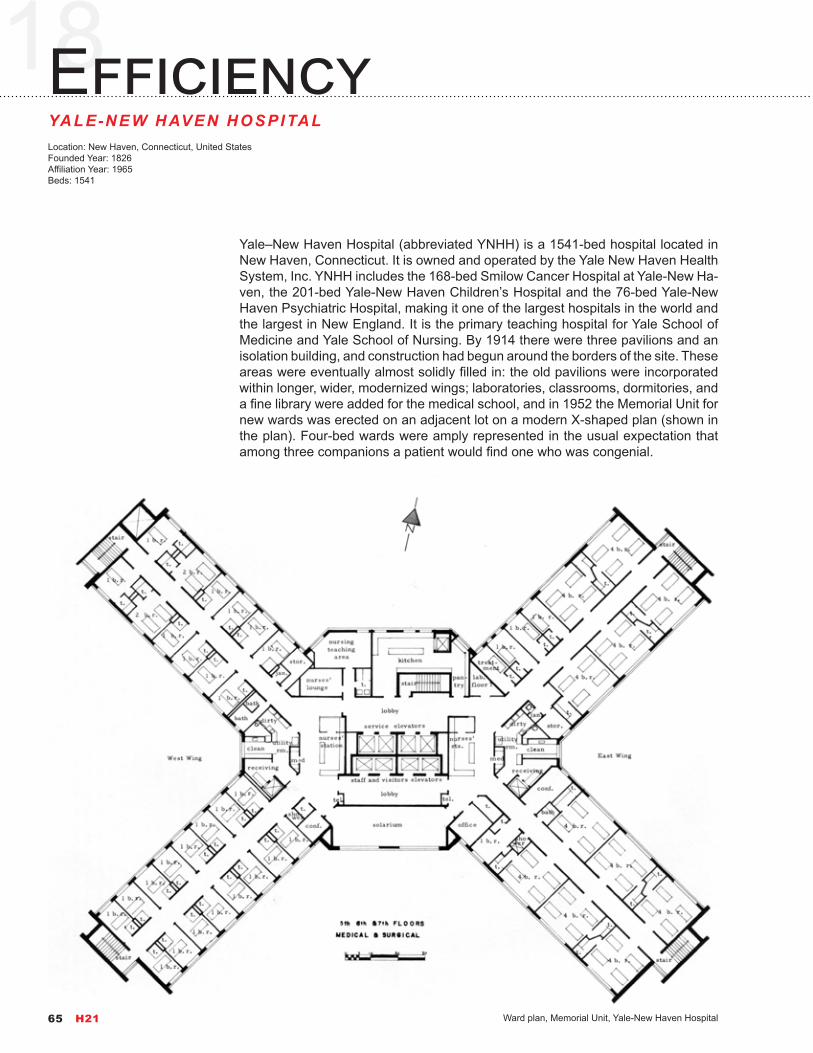
Ward plan, Memorial Unit, Yale-New Haven Hospital
Yale–New Haven Hospital (abbreviated YNHH) is a 1541-bed hospital located in New Haven, Connecticut. It is owned and operated by the Yale New Haven Health System, Inc. YNHH includes the 168-bed Smilow Cancer Hospital at Yale-New Ha-ven, the 201-bed Yale-New Haven Children’s Hospital and the 76-bed Yale-New Haven Psychiatric Hospital, making it one of the largest hospitals in the world and the largest in New England. It is the primary teaching hospital for Yale School of Medicine and Yale School of Nursing. By 1914 there were three pavilions and an isolation building, and construction had begun around the borders of the site. These areas were eventually almost solidly filled in: the old pavilions were incorporated within longer, wider, modernized wings; laboratories, classrooms, dormitories, and a fine library were added for the medical school, and in 1952 the Memorial Unit for new wards was erected on an adjacent lot on a modern X-shaped plan (shown in the plan). Four-bed wards were amply represented in the usual expectation that among three companions a patient would find one who was congenial.
65 H21

West wing of New Haven Hospital (1873) as seen in 1913 from the lawn in front of the original columned structure
Memorial Unit, Yale-New Haven Hospital, New Haven, Connecticut, 1974, as completed with the addition of two new stories.
2015 MASTER’S RESEARCH PROJECT 66
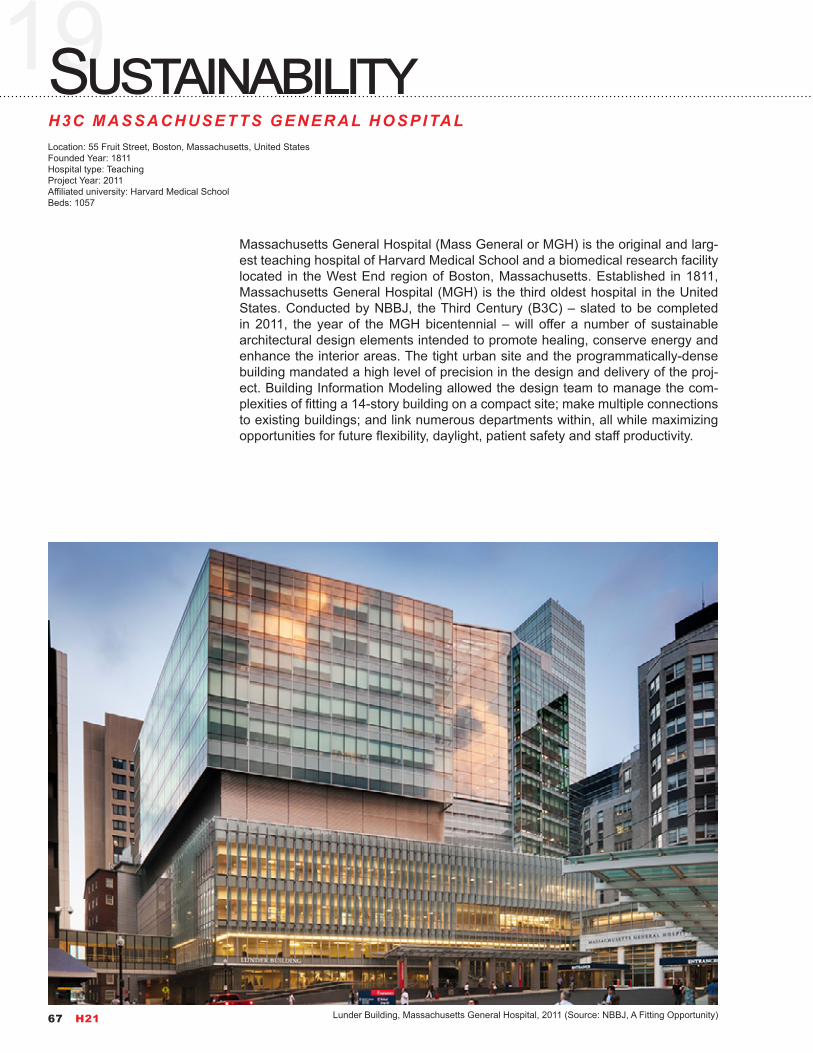
19SustainabilityH3C MASSACHUSETTS GENERAL HOSPITALLocation: 55 Fruit Street, Boston, Massachusetts, United StatesFounded Year: 1811Hospital type: TeachingProject Year: 2011Affiliated university: Harvard Medical SchoolBeds: 1057
Lunder Building, Massachusetts General Hospital, 2011 (Source: NBBJ, A Fitting Opportunity)
Massachusetts General Hospital (Mass General or MGH) is the original and larg-est teaching hospital of Harvard Medical School and a biomedical research facility located in the West End region of Boston, Massachusetts. Established in 1811, Massachusetts General Hospital (MGH) is the third oldest hospital in the United States. Conducted by NBBJ, the Third Century (B3C) – slated to be completed in 2011, the year of the MGH bicentennial – will offer a number of sustainable architectural design elements intended to promote healing, conserve energy and enhance the interior areas. The tight urban site and the programmatically-dense building mandated a high level of precision in the design and delivery of the proj-ect. Building Information Modeling allowed the design team to manage the com-plexities of fitting a 14-story building on a compact site; make multiple connections to existing buildings; and link numerous departments within, all while maximizing opportunities for future flexibility, daylight, patient safety and staff productivity.
67 H21

Lunder Building program
Urban connection
First Patient Tower floor plate design
First Patient Tower volumetric design
Urban Response
Lunder Building floor diagrams to maximize the number of patient beds per floor while minimizing travel distances for staff (Source: NBBJ, A Fitting Opportunity, http://www.nbbj.com/work/massachusetts-general-hospital-lunder-building/)
2015 MASTER’S RESEARCH PROJECT 68

Final Patient Tower Floor Plate Design, H3C, 2011
Lunder Building Views, Massachusetts General Hospital, 2011(Source: NBBJ, A Fitting Opportunity, http://www.nbbj.com/work/massachusetts-general-hospital-lunder-building/)
69 H21

The B3C includes an indoor atrium and lots of natural light. Healing through nature is a philosophy that integrates elements of the outdoors into the healing environ-ment. With this perspective, architects designed each of the 150 patient rooms with large windows that will feature cascading sunlight. A number of rooms will have views of either an 1,800-square-foot atrium garden or the scenic Charles River. Located on the building’s sixth floor, the atrium garden which will include 12-foot hanging plants, bamboo trees and a variety of groundcover vegetation – also will be visible from many of the building’s family and staff lounges and consultation rooms. More than 21,000 square feet of green garden will cover the B3C roofs, providing neighboring buildings with a view of the seasonally changing plants and helping to increase oxygen in the surrounding areas. The roof plants will be drought-tolerant and require no irrigation; all of the necessary water for the plantings will come from rain and condensation collected from the building’s cool-ing system.
Renewable materials such as recycled rubber flooring and bamboo walls will be used throughout the B3C interior. Rubber floors will help to cushion footsteps and reduce noise, and the bamboo panels, which are sustainably harvested, will pro-mote a natural and warm connection to nature.
Up to 75 percent of demolished materials from the Clinics, Vincent Burnham Ken-nedy and Tilton buildings – which previously stood on the site – and construction debris are expected to be diverted from disposal at landfills and used to generate recycled materials. Plans also include using up to 60 percent renewable energy sources for the building’s power.
Lunder Building Main Entrance, Massachusetts General Hospital, 2011(Source: NBBJ, A Fitting Opportunity, http://www.nbbj.com/work/massa-chusetts-general-hospital-lunder-building/)
2015 MASTER’S RESEARCH PROJECT 70
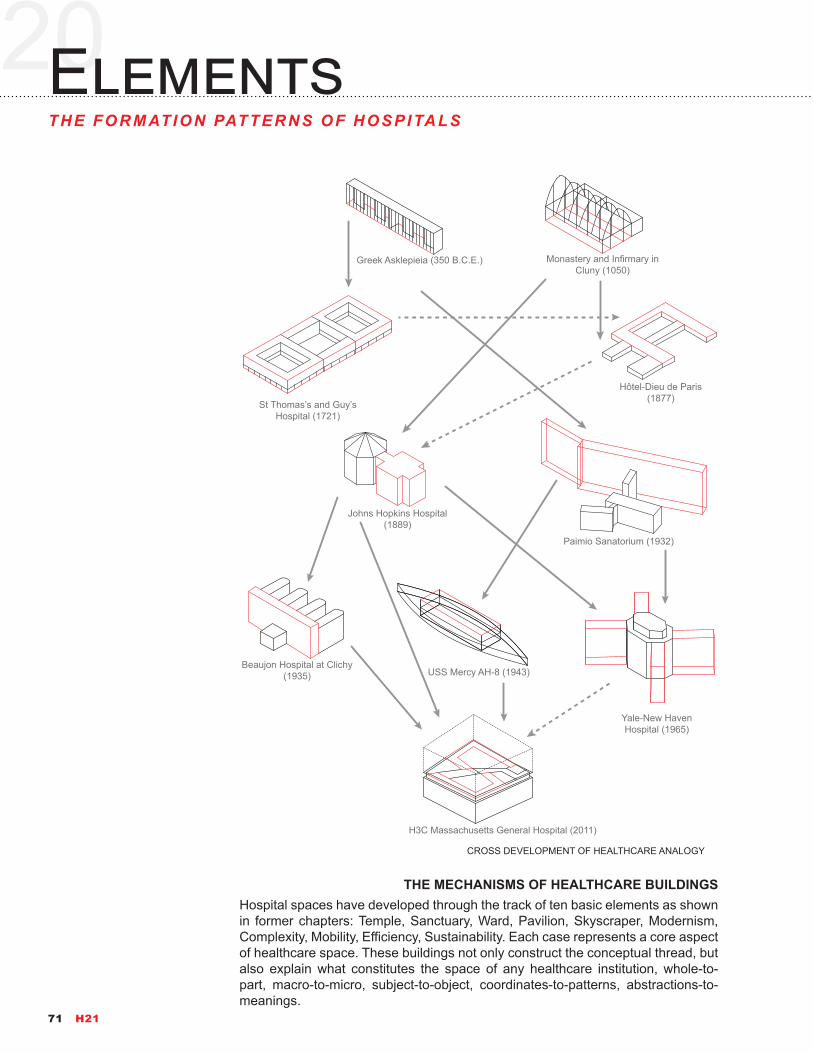
20ElementsTHE FORMATION PATTERNS OF HOSPITALS
Hospital spaces have developed through the track of ten basic elements as shown in former chapters: Temple, Sanctuary, Ward, Pavilion, Skyscraper, Modernism, Complexity, Mobility, Efficiency, Sustainability. Each case represents a core aspect of healthcare space. These buildings not only construct the conceptual thread, but also explain what constitutes the space of any healthcare institution, whole-to-part, macro-to-micro, subject-to-object, coordinates-to-patterns, abstractions-to-meanings.
CROSS DEVELOPMENT OF HEALTHCARE ANALOGY
Greek Asklepieia (350 B.C.E.)
Hôtel-Dieu de Paris (1877)
Johns Hopkins Hospital (1889)
Paimio Sanatorium (1932)
Beaujon Hospital at Clichy (1935) USS Mercy AH-8 (1943)
Yale-New Haven Hospital (1965)
H3C Massachusetts General Hospital (2011)
St Thomas’s and Guy’s Hospital (1721)
Monastery and Infirmary in Cluny (1050)
THE MECHANISMS OF HEALTHCARE BUILDINGS
71 H21

GREEK ASKLEPIEIA (350 B.C.E.)
HÔTEL-DIEU DE PARIS (651)ST THOMAS’S HOSPITAL (1721)
INFIRMARY OF MONASTERY IN CLUNY (1050)
Orientation(Direct Sunlight)
Treatment(Spatial Division of patients and resources)
Beds(Inpatient Placing)
Latrines or Necesaria(Sanitation Facilitating)
Supporting(Storage and Mandatum-Kitchen)
Wards(Male and Female inpatient units separated)
Pavilion(Longitudinal arrangement on behalf of natural air)
Corridor(Rational connection between pavilions)
Pharmacies(Pharmaceutic Supporting)
Control(Visiting group are controlled by main entrance)
Lobby(Supporting and welcoming)
Zoning(Walled organization for the sicks)
Division(Dividing of a great hall)
Galleries(Basic circulation spaces)
Hall(An integrated program in infirmary)Temple
(Modular System established by the temple)
2015 MASTER’S RESEARCH PROJECT 72
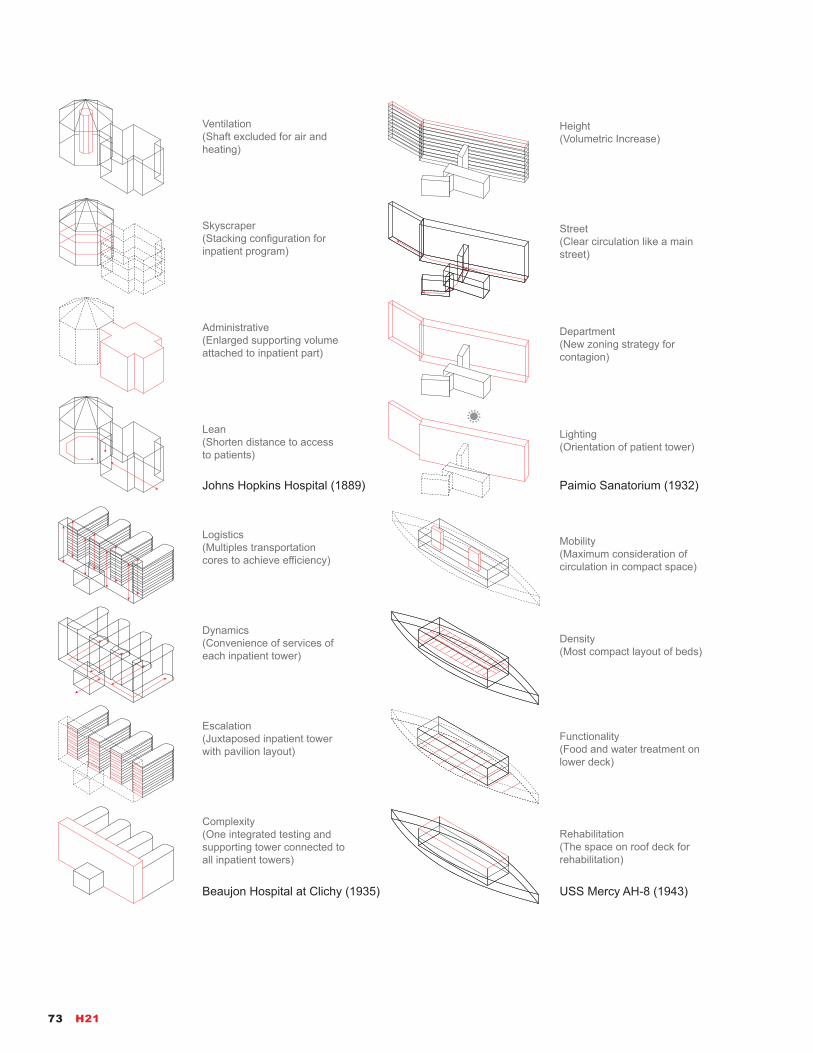
Johns Hopkins Hospital (1889) Paimio Sanatorium (1932)
Beaujon Hospital at Clichy (1935) USS Mercy AH-8 (1943)
Ventilation(Shaft excluded for air and heating)
Height(Volumetric Increase)
Street(Clear circulation like a main street)
Department(New zoning strategy for contagion)
Lighting(Orientation of patient tower)
Skyscraper(Stacking configuration for inpatient program)
Administrative(Enlarged supporting volume attached to inpatient part)
Lean(Shorten distance to access to patients)
Logistics(Multiples transportation cores to achieve efficiency)
Dynamics(Convenience of services of each inpatient tower)
Rehabilitation(The space on roof deck for rehabilitation)
Density(Most compact layout of beds)
Functionality(Food and water treatment on lower deck)
Mobility(Maximum consideration of circulation in compact space)
Complexity(One integrated testing and supporting tower connected to all inpatient towers)
Escalation(Juxtaposed inpatient tower with pavilion layout)
73 H21

Yale-New Haven Hospital (1965) H3C Massachusetts General Hospital (2011)
Core(Rearranged tower core for mechanical, ventilation, and services)
Opportunities(Massing reflects the five-story bed tower is separated from the procedural floors below)
Convenience(Maximizing the number of patient beds per floor)
Efficiency(Minimizing travel distances for medical staff)
Greenness(Atrium garden is visible from many of the building's lounges and consultation rooms)
Accessibility(Modernized wings are connected to the consolidated core)
Incorporation(Old pavilions incorporated in longer and wider towers)
Technology(Laboratories and medical facilities are located in the heart of the X-shape)
References
1. “50 Largest Hospitals in America,” last modified October 26, 2010, http://www.beckershospitalreview.com/lists/50-largest-hospitals-in-america.html
2. Thompson, John D., and Grace Goldin. 1975. The hospital: a social and architectural history. New Haven: Yale University Press.
3. Christensen, Clayton M., Jerome H. Grossman, and Jason Hwang. 2009. The innovator’s prescription: a disruptive solution for health care. New York: McGraw-Hill.
4. Nickl-Weller, Christine, and Hans Nickl. 2013. Hospital architecture. [Salenstein, Switzerland]: Braun.
5. Miller, Richard L., Earl S. Swensson, and J. Todd Robinson. 2012. Hospital and healthcare facility design. New York: W.W Norton & Co.
6. “History of hospitals,” last modified February 6, 2015, http://en.wikipedia.org/wiki/History_of_hospitals
7. “Guy’s Hospital,” last modified January 19, 2015, http://en.wikipedia.org/wiki/Guy%27s_Hospital
8. “Hôtel-Dieu de Paris,” November 28, 2014, http://en.wikipedia.org/wiki/H%C3%B4tel-Dieu_de_Paris
9. “Johns Hopkins Hospital,” December 20, 2014, http://en.wikipedia.org/wiki/Johns_Hopkins_Hospital
10. “A Fitting Opportunity,” January 20, 2012, http://www.nbbj.com/work/massachusetts-general-hospital-lunder-building/
11. “Massachusetts General Hospital”, January 15, 2015, http://en.wikipedia.org/wiki/Massachusetts_General_Hospital
12. “Outboard Profiles of Maritime Commission Vessels,” May 01, 2007, http://drawings.usmaritimecommission.de/drawings_c1.htm
13. “Paimio Sanatorium,” November 30, 2014, http://en.wikipedia.org/wiki/Paimio_Sanatorium
14. “St Thomas’ Hospital,” January 20, 2015, http://en.wikipedia.org/wiki/St_Thomas%27_Hospital
15. “USS Mercy (AH-8)”, July 7, 2013, http://en.wikipedia.org/wiki/USS_Mercy_(AH-8)
16. “Yale–New Haven Hospital,” November 25, 2014, http://en.wikipedia.org/wiki/Yale%E2%80%93New_Haven_Hospital
17. “Building for the Third Century: A sustainable and green design for the future,” Aug 15, 2008, http://www.massgeneral.org/about/newsarticle.aspx?id=1281
2015 MASTER’S RESEARCH PROJECT 74

“I believe in being an innovator.”
Walt DisneyWalt before Mickey: Disney’s early years, 1919-1928
PART 275 H21

21
10 Largest Hospitals in America:
1. New York-Presbyterian Hospital/Weill Cornell Medical Center (New York City) — 2,236. New York-Presbyterian/Weill Cornell is a major non-profit teaching hospital that offers a variety of services, including a renowned can-cer program. The facility admits 48,000 emergency room patients every year and performs 38,500 inpatient and 39,400 outpatient surgeries, as well as 13,700 births. Emergency care is provided 24 hours a day, seven days a week to adults and children in the level I trauma center, psychiatric emergency re-ceiving center and burn center for the city of New York. The hospital also features a high-risk neonatal transport service, where the hospital serves as an emergency transfer, receiving and stabilization center.
2. Florida Hospital Orlando (Fla.) — 1,972. Florida Hospital Orlando is a non-profit acute-care community hospital that serves over 32,000 inpatients and 53,000 outpatients annually. Serving as a major tertiary facility for much of the southeastern part of the United States, the hospital is part of the Florida Hospital system, a group of private hospitals operated by Adventist Health System. It contains nationally renowned institutes for cardiology, diabetes, orthopedics and neuroscience. The hospital was founded in 1908 by leaders of the Adventist Church.
3. Jackson Memorial Hospital (Miami) — 1,756. Jackson Memorial Hospital is a non-profit tertiary teaching hospital that first opened in 1918. The hospital works in conjunction with the University of Miami Miller School of Medicine to offer a wide variety of services, educational programs, a space for clinical research and health-related community services. The hospital is well-known for its Ryder Trauma Center, the only adult and pediatric level I trauma center in the Miami-Dade area. It also features a 66-bed neonatal intensive care unit, the largest unit in the state, and is the only Florida hospital to perform every kind of organ transplant.
4. University of Pittsburgh (Pa.) Medical Center Presbyterian — 1,602. Founded in 1893, University of Pittsburgh Medical Center Presbyterian is a non-profit adult medical-surgical referral hospital with a strong emphasis on research. Closely connected to the University of Pittsburgh School of Medi-cine, the hospital is a recognized leader in cardiology and cardiothoracic sur-gery, trauma services, neurosurgery and organ transplantation. The hospital handles over 30,000 emergency room admissions every year and performs 26,800 inpatient and 23,600 outpatient surgeries. UPMC Presbyterian is also designed as a level I regional resource trauma center. The hospital is divided into two buildings — UPMC Presbyterian and UPMC Montefiore — that are linked by a bridge.
5. Methodist Hospital (Indianapolis) — 1,450. Methodist Hospital, which is part of Clarian Health, is the largest hospital in Indiana with one of the largest
DisruptionBUSINESS MODEL ON CHANGING
Almost everyone in United States wants to reform healthcare to better care at lower cost. Healthcare in 2013 accounted for 16.9% of GDP of United States. In health care, the age of usual business is over. Around the world continents, every health care system is com-bating against rising costs and uneven quality despite the hard work of well-educated, well-motivated clini-cians. Health care providers and policy makers have tried countless incremental fixes—reducing errors, minimizing fraud, enforcing practice guidelines, mak-ing patients better “consumers,” implementing elec-tronic medical records—but none have had much im-pact. The problems facing the healthcare industry is a great deal. Therefore, we may start with the following list of largest hospitals in United States.
critical care departments and the largest neuroscience critical care unit in the country. The hospital also implemented the first and largest comprehensive intensive care patient electronic monitoring system in Central Indiana. As a hospital with one of the largest emergency departments in the country, almost 97,000 patients came through Methodist’s ED in 2008. One-hundred-thirty beds are dedicated to the critical care unit. The hospital has established itself as a leader in the community by launching outreach initiatives, including the Indiana Poison Center, Indiana Mothers’ Milk Bank and ThinkFirst Shaken Baby Program.
6. Montefiore Medical Center – Moses Division Hospital (Bronx, New York) — 1,427. Non-profit Moses Division Hospital offers a variety of services to New York residents and beyond, including cardiac surgery, radiation therapy, joint replacement, spine surgery, Medicare-certified organ transplantation and hy-perbaric medicine. Moses is a major teaching hospital with a teaching cancer program and is actively involved as a major participant in Accreditation Coun-cil for Graduate Medical Education-accredited specialty and subspecialty pro-grams. The hospital handles 73,400 emergency room admissions every year as well as 337,200 outpatient visits and 17,500 inpatient surgeries.
7. Methodist Hospital (San Antonio) — 1,414. Methodist Hospital in San Anto-nio is a 1,414-bed hospital that includes flagship Methodist Hospital, Method-ist Children’s Hospital of South Texas, the Metropolitan Methodist Hospital, the Methodist Specialty and Transplant Hospital and Northeast Methodist Hospital. The hospital was founded in 1963 and is part of Methodist Health-care. The hospital is a regional referral center with 2,500 employees and is used by more than 2,000 physicians associated with the Methodist Health-care System. The facility is located in the South Texas Medical Center and is San Antonio’s largest private hospital as well as the largest provider of healthcare to rural communities in South Texas.
8. Baptist Medical Center (San Antonio) — 1,402. Located in downtown San Antonio, non-profit Baptist Medical Center is part of Baptist Health System and provides complete care for its patients and includes an accredited chest pain center, a wound healing center with state-of-the-art hyperbaric chambers and 18 operating rooms equipped with the latest technology. Baptist employs 5,083 staff members and performs around 21,000 inpatient surgeries and 21,400 outpatient surgeries a year as well as 87,400 outpatient visits. The hospital has embraced the move to private patient rooms by providing every new mother and child with a private patient room.
9. Orlando (Fla.) Regional Medical Center — 1,367. Orlando Regional Medi-cal Center, which is part of Orlando Health and located in downtown Orlando, specializes in trauma, critical care, emergency care, cardiology, orthopedics and neurosciences. ORMC, which is a non-profit institution, is one of Florida’s six major teaching hospitals and Orlando Health’s flagship medical center. It also contains central Florida’s only level I trauma center and provides treatment for memory disorder, epilepsy, brain injury and other rehabilitation needs. As one of Florida’s six major teaching hospitals, ORMC offers gradu-ate medical education in several specialties, including emergency medicine, OB/GYN, orthopedics, pediatrics and general surgery.
10. Methodist University Hospital (Memphis, Tenn.) — 1,273. Methodist Uni-versity Hospital is the largest, most comprehensive hospital in the Method-ist Healthcare system. Located in the heart of the Memphis Medical Center, this non-profit organization receives an estimated 38,400 emergency room admissions every year and performs 16,400 inpatient and 18,500 outpatient surgeries. It also serves as the major academic campus for the University of Tennessee Health Science Center. The hospital includes a neuroscience institute that provides cutting-edge services such as minimally invasive spine surgery, image guided surgery, neurocritical care and PET imaging. The hos-pital also features a level IV epilepsy center and a transplant institute known for its success with kidney, liver and pancreas transplants.
Data Source: Becker’s Hospital Review, 2011
2015 MASTER’S RESEARCH PROJECT 76

ELEMENTS OF DISRUPTIVE INNOVATION
1Sophisticated
Technology thatSimplifies
Regulations andStandards that
FacilitateChange
2Low-cost
InnovativeBusiness Model
3Economically
Coherent ValueNetwork
1ORGANIZE INTO
INTEGRATEDPRACTICE UNITS
(IPUs)
5EXPAND
EXCELLENTSERVICES ACROSS
GEOGRAPHY
4INTEGRATE
CARE DELIVERYACROSS SEPARATE
FACILITIES
3MOVE TO BUNDLED
PAYMENTS FORCARE CYCLES
2MEASURE
OUTCOMES ANDCOSTS FOR EVERY
PATIENT
ENABLING INFORMATION TECHNOLOGY PLATFORM
22RealityTHE INNOVATOR’S PRESCRIPT ION
In 1970 the cost of healthcare in the United States accounted for about 7 percent of gross domestic product. In 2007 it accounted for 16 percent of America’s GDP and it is still climbing. By estimating, the rising cost of Medicare within that bud-get will crowd out all other spending except defense within 20 years. The book of The Innovator’s Prescription presents a path map to the dramatic innovations in healthcare delivery, costs, and policy the public can expect in the next decades. Is it possible to make U.S. health care affordable? Professor Christensen, Dr. Gross-man and Dr. Hwang laid out a start. The core purpose of this book is to show how to make it affordable — less costly and of better quality.
The problems confronting the healthcare industry merely are not unique. The prod-ucts and services provided in every factory line, at their outset, are so complicated and expensive that only the wealthy had access to them, and only experts can provide and use them. Like air planes, photography, telephones, automobiles in their first decades, it is the same with healthcare. However, those industries have been transformed and making the products and services so much more affordable and accessible that a much larger population of people could purchase and use them. In the book, this agent of transformation have been termed as disruptive in-novation. It consists of three elements.
1. Technological Enabler: sophisticated technology whose purpose is to simplify, it routinizes the solution to problems that previously required intuitive experimen-tation in unstructured processes to resolve. 2. Business Model Innovation: con-structing profitable delivery these simplified solutions to customers in ways that make them affordable, convenient and accessible. 3. Value Network: a commercial infrastructure whose coherent companies have consistently disruptive, universally reinforcing business models.
77 H21
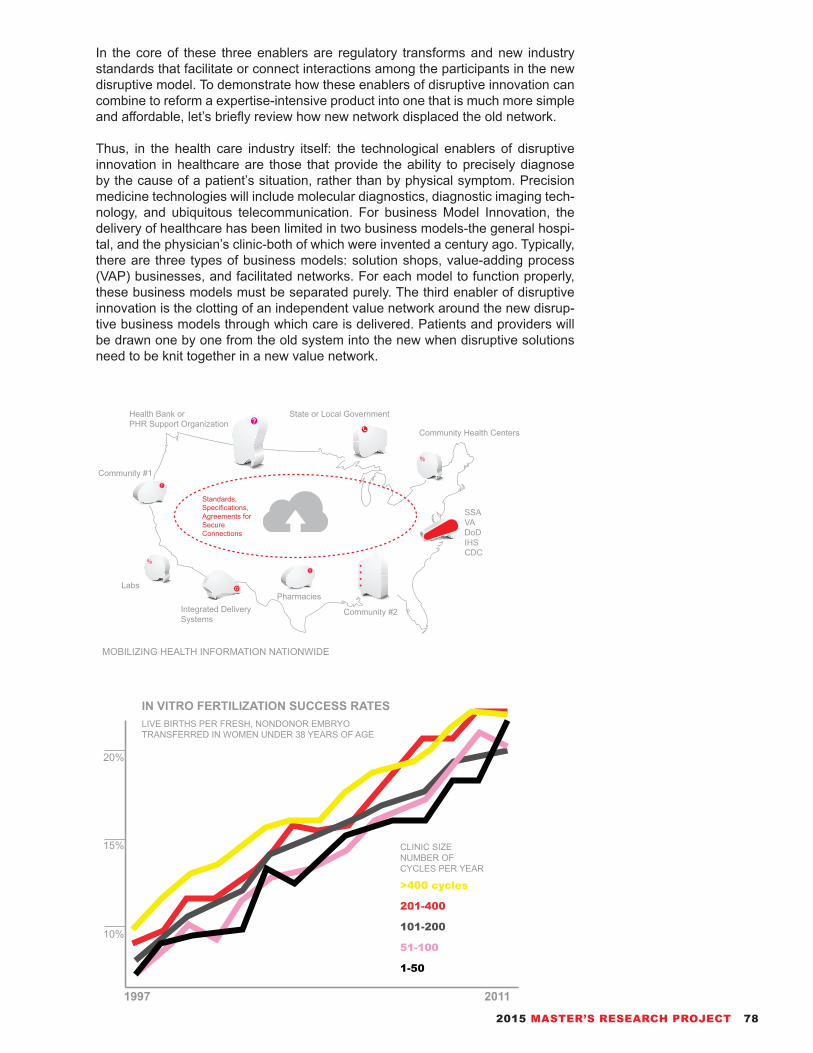
MOBILIZING HEALTH INFORMATION NATIONWIDE
Community #1
Community #2
PharmaciesIntegrated Delivery Systems
Labs
Health Bank orPHR Support Organization
State or Local Government
Community Health Centers
SSAVADoDIHSCDC
Standards,Specifications,Agreements for Secure Connections
20%
LIVE BIRTHS PER FRESH, NONDONOR EMBRYO TRANSFERRED IN WOMEN UNDER 38 YEARS OF AGE
CLINIC SIZE NUMBER OF CYCLES PER YEAR
15%
10%
>400 cycles
201-400
101-200
51-100
1-50
1997 2011
IN VITRO FERTILIZATION SUCCESS RATES
In the core of these three enablers are regulatory transforms and new industry standards that facilitate or connect interactions among the participants in the new disruptive model. To demonstrate how these enablers of disruptive innovation can combine to reform a expertise-intensive product into one that is much more simple and affordable, let’s briefly review how new network displaced the old network.
Thus, in the health care industry itself: the technological enablers of disruptive innovation in healthcare are those that provide the ability to precisely diagnose by the cause of a patient’s situation, rather than by physical symptom. Precision medicine technologies will include molecular diagnostics, diagnostic imaging tech-nology, and ubiquitous telecommunication. For business Model Innovation, the delivery of healthcare has been limited in two business models-the general hospi-tal, and the physician’s clinic-both of which were invented a century ago. Typically, there are three types of business models: solution shops, value-adding process (VAP) businesses, and facilitated networks. For each model to function properly, these business models must be separated purely. The third enabler of disruptive innovation is the clotting of an independent value network around the new disrup-tive business models through which care is delivered. Patients and providers will be drawn one by one from the old system into the new when disruptive solutions need to be knit together in a new value network.
2015 MASTER’S RESEARCH PROJECT 78

Non-consumers
time
time
Disruptive InnovationsMake products simpler and more affordable
Performance improvement that customers can utilize
Pace of performance improvement that companies provide
Sustaining Innovationswhether incremental or radical, make good products better
Performance
Different
Measure
of
Performance
Model of Disruptive InnovationNon-consumers Model of Existing Industry
time
time
least demanding customers
most demanding customers
New Market DisruptionCompete against non-consumption
Low-end DistributionAddressing over-served customers with a low cost business model
Sustaining TechnologyBringing a better product information into an established market
Performance
Different
Measure
of
Performance
23BusinessTHE INNOVATOR’S HEALTHCARE INDUSTRY
Three of the enablers can be concluded as the changes in the infrastructure around healthcare, these comprise the best map we can draw of the terrain of reform ahead.- Reforming the reimbursement system,- Role of information technology in the disruption of health care,- IT and facilitated networks,- Evolution of Patient Health Records,- The Future of the Pharmaceutical and Medical Devices Industries,- Medical Devices and Diagnostic Equipment,- Changes in Medical Education,- The Impact of Regulation on Disruption Innovation in Health Care.
The disruptive innovation theory indicates the process by which complicated, expensive products and services are transformed into affordable products. The theory of comparing the existing and innovative models construct are depicted in left figures. The solid line is assigned the pace of improvement of products and services that corporations provide to their customers as they introduce newer and better products over time. In the meantime, the dotted lines represents the rate of performance progression that customers are able to utilize. As the intersect-ing trajectories of the solid and dotted lines suggest, customer’s needs in a given market application which tends to be relatively stable over time. Additionally, the initial products and services in the original “plane of competition” at the back are typically complicated.
79 H21

How Healthcare Become More Costy (Plugging new technologies into old business model has caused health care costs to rise rather than fall)
Imaging Services
Clinical Research and Training
Data Collection and Warehousing Surgical Suites
Laboratory Services
Specialty Care
RegulationsLicensure and AccreditationCultural ResistanceReimbursement
Lower Continuous cascade of disruption in health care
patient’s homes
time
outpatient clinics
doctor’s offices
General Hospitals
Value-adding process hospitals
Solution shop hospitals
Complexity
of
Diagnosis
and
Treatment
Although hospitals have existed since early classic, the concept of the hospital as we know it today had not begun to form until the eighteenth century in Europe. The solution shop activities within a hospital are typically those involved in diag-nosing patients’ issues. This requires centralized laboratories filled with the most top-advanced instruments to analyze blood and tissue samples, and radiology de-partments with the most sophisticated imaging technologies, such as computer-ized tomography (CT) scanners, magnetic resonance imaging (MRI) machines, and positron emission tomographic (PET) imagers. The typical general hospital’s solution shop is set up to handle any disorder in any part or system within the body. Value-adding process activities consist of the other business model in a general hospital. Their value proposition resolves the second of the jobs that will be done that was noted earlier-to fix problems after certain diagnoses have been made. When the same hospital are seeking to fulfill these two very different value propo-sitions, the consequence for two types of business models creates extraordinary internal discrepancy. The resources and the essential feature of the processes inherent in the two business models are different.
The charts on right depicts the ongoing cascade of disruptions that will be required in order for healthcare to continue to become more affordable and accessible, without compromising too much on quality. Firstly, general hospitals need to create hospitals-within-hospitals, or others must build new institutions that will be focused exclusively on solution shop or value-adding process business models. The solu-tion shops can integrate efficiently for the practice of intuitive medicine, while the value-adding process hospitals can efficiently integrate the steps in their proce-dures. Then new technology must be brought to large group ambulatory clinics, so we can begin doing in that settings the brief of the procedures that can only be done in hospitals today. Those clinics then need to become increasingly capable of doing ever more complicated procedures, drawing into that settings more and more of the activities that have historically been done in hospitals. To realize dis-ruption, drug and medical device manufacturers should focus their technology and product development efforts on bringing the location and the ability to provide care toward the front of this diagram. If today’s hospitals start out focused hospitals to disrupt themselves, the evolution can be positively promising.
2015 MASTER’S RESEARCH PROJECT 80

A New Ecosystem of Disruptive Business Models of Healthcare
Work-site ClinicsMobile Care Services
Wireless Health Devices
Home MonitoringRetail ClinicsHome Visits
Medical Homes and Care HomesServices While Traveling Abroad
Hospital at home
Automated Kiosks
Telehealth/ e-visits
Wellness Programs
Telecommunications
Information Management and Decision-making Tools
Precision Medicine
24ProgressionTHE INNOVATOR’S HOSPITAL DESIGN
Though the institutions of healthcare have been happening for less than two hun-dred years, this artifact has its own history, its own traditions, and its own dogmas. As what has been discussed in the previous page, the disruptive model in health-care will result in the moving down-market of general hospitals and moving up-market of clinic and doctor’s offices. Therefore, a large group of ambulatory clinics can begin doing in that setting the simplest of the procedures that can only be done in hospitals today. And small groups and individual doctors’ offices can begin doing the simplest of things that today require a large ambulatory clinic. Business model innovation, in the form of disruption, is the propelling mechanism by which substantial improvements in the quality and cost of healthcare can be achieved. Thus, the economic division of healthcare industry can be based on three methods solution shops (fee for service), value-adding process business (fee for outcome), facilitated user networks (fee for membership, advertising).
81 H21

References
1. Christensen, Clayton M. 1997. The innovator’s dilemma when new technologies cause great firms to fail. Boston, Mass: Harvard Business School Press.
2. Christensen, Clayton M., Jerome H. Grossman, and Jason Hwang. 2009. The innovator’s prescription: a disruptive solution for health care. New York: McGraw-Hill.
3. “The Strategy That Will Fix Health Care,” October 1, 2013, https://hbr.org/2013/10/the-strategy-that-will-fix-health-care/
4. “Health Information Technologies,” January 1, 2010, http://www.tatrc.org/ports_healthInfo.html
5. “YLMIT Lab Next Generation of Hospital,” December 15, 2013, https://ylmitlab.wordpress.com/
6. Miller, Richard L., Earl S. Swensson, and J. Todd Robinson. 2012. Hospital and healthcare facility design. New York: W.W Norton & Co.
01
03 02
Hospital ls become focused solution shops, practicing intuitive medicine. Focused value-adding
process hospitals & clinics provide procedures after definitive diagnosis.
Facilitated networks take dominant role in the care of many chronic diseases.
SOLUTION SHOPS(Fee for service)- Consulting firms- High-end law firms- R&D organizations- Diagnostic activities of hospitals
VALUE-ADDING PROCESS BUSINESSES(Fee for outcome)- Retailing- Manufacturing- Food Services- Medical Procedures
FACILITATED USER NETWORKS(Fee for Membership, Advertising)- eBay- Insurance- Education- Telecommunications- D-Life (for diabetes patients & families)
THREE TYPES OF BUSINESS MODELS OF FUTURE HEALTHCARE FACILITIES
2015 MASTER’S RESEARCH PROJECT 82

“The world as we have created it is a process of our thinking. It can-not be changed without changing our thinking.”
Albert EinsteinIdeas and Opinions, 1954
PART 383 H21

25
Beginning with an outline of the context introduction and ongoing accreditation systems for healthcare fa-cilities, this part is the original foundation of this re-search project - presenting the design process of UF Health Cardiovascular Hospital in detail. The emerg-ing thoughts challenge the conventions because ev-erything can always be improved upon. Things that are innovative are appealing. Even if eventually they are apart from the ultimate solution, they will have ful-filled a role in making everyone think things in a differ-ent way.
Modern architecture is an intrinsically contradictory profession. The building actions intersect with a huge range of related/unrelated domains, in meanwhile to build is so complex that it requires extreme focus and concentration on the simple idea to plot the whole proj-ect. This property is shown so clearly in especially a healthcare project like the one we will discuss in this part. Therefore, the crucial conclusion which must be drawn out through this design process is to meet particularly high quality requirements in a healthcare institution.
However, the aim is not only to display the design project, but rather to provoke further thought and con-versations. Which trends in healthcare buildings are evident, which developments are acceptable and how should these be embodied in terms of future challeng-es and changes? And finally: an evaluation of these trends allows the design process to draw a conclusion regarding the paradigms shown in terms of questions like: what functions better and what will or develop further in the future . However dynamic, diverse and radical the various ideas to planning and this health-care facility may be, the project presented in this part targets onto a high degree of quality consciousness, which, in the essence, legitimates the strict demands placed on this space of architecture.
In 2013, University of Florida Health officials an-nounced to plan to build a new specialty tower that will house neuromedicine and cardiovascular hospitals to accommodate anticipated growth in several areas. “We’re experiencing increasing demands for our ser-vices, and our hospitals have maintained such high patient volumes that we frequently are functioning at full capacity,” said David S. Guzick, M.D., Ph.D., UF
ProcessPRACTICAL SYNTHESIS OF ADVANCEMENTS
senior vice president for health affairs and president of UF Health. “As a trusted regional and statewide health care resource, we have a responsibility to ensure our facilities can assist us in providing the best possible outcomes while providing the best possible patient ex-perience. These plans will help us meet our patient and community needs.”
The new specialty tower will be located on UF Health’s south campus, just east of Archer Road near the visi-tor parking lot for the UF Health Shands Cancer Hos-pital, and will likely feature about 240 beds. “The new specialty hospital tower will allow us to better address the needs of patients with cardiovascular and neu-rological issues, much like we are providing care to cancer patients with great success at the UF Health Shands Cancer Hospital,” said Timothy M. Goldfarb, CEO of UF Health Shands. “Expanding these nation-ally recognized medical programs will allow us to offer specialized care to more patients.”
In this part, the main aim is to provoke thought and inspire excitement based on this scenario, to pro-mote future demands and expectations of high-quality healthcare architecture and to further develop innova-tive visions.
2015 MASTER’S RESEARCH PROJECT 84

26ThesisMAKING TWENTY-F IRST CENTURY HOSPITAL
In different business models, there are three types: solution shops, value-add-ing process (VAP) businesses, and facilitated networks. As how the healthcare institutions started, the two dominant provider institutions in health care-general hospitals and physicians’ practices-emerged authentically as solution shops. But over a century they have mixed in value-adding process and facilitated network activities in the spectrum of services as well. Nowadays, the health-care system has trapped many disruption-enabling technologies in high-cost institutions that have conflated three business models in the same building. The first step of in-novation must separate different business models into separate institutions whose processes, resources, and profit models are corresponded to the level of precision by which the disease is understood. Solution shops are supposed to become fo-cused so they could deliver and price the services of intuitive medicine accurately. Focused value-adding process hospitals need to absorb those procedures that general hospitals have presently performed after definitive diagnosis. And facilitat-ed networks need to be fostered to manage the care of many behavior-dependent chronic diseases. Solution shops and VAP hospitals can be created as hospitals-within-hospitals if done correctly. The reason why this segregation of business models must happen from the outset of disruption is that it will enable accurate assessments of value, costs, pricing, and profit for each type of business.
EXISTING VALUE NETWORK
85 H21

To achieve to deconstruction of health care institutions into the two different busi-ness models: solution shops and value-adding process activities. This can be done by creating hospitals-within-a hospital, or by building distinct facilities. In ei-ther case, the work done within each business model must be organized distinctly, and their cost accounting and pricing systems must be separated and assembled in ways appropriate to each. The biggest and best medical centers will be able to bifurcate themselves. Smaller hospitals, nonetheless, will need to focus on be-coming solution shops or value-adding process hospitals, or simply expect to be integrated through disruption. The reason why this division is such a essential first step of this innovation is that there are two different jobs-to-be-done. To visualize how this process happens in the next generation healthcare institutions, two differ-ent diagrams of value networks can indicate the attempt.
Data
Finance
Contracting DISRUPTIVE VALUE NETWORK
2015 MASTER’S RESEARCH PROJECT 86

27PracticeUF HEALTH SHANDS CARDIOVASCULAR HOSPITAL
All the study which has been done through the path of this master’s research project did not show a clear vision of the how it will look like for a “hospital for twenty-first century”, but even revealed a number of new question marks. One guiding principle which has been discovered is that healthcare building follows the medical technology and medical situations of that time. This proposal for the new cardiovascular hospital in UF Health South Campus, serving as an integrated component in the entire complex, seeks to preserve the good of existing medical architectural features while opening the future of hospital machine.
According to a World Bank analysis, cardiovascular diseases are the leading cause of deaths on the human society globally. To accommodate anticipated growth of need in thus area, this project intends to propose to build a new specialty hospital that will house cardiovascular services of UF Health Shands Hospital, by taking the preemptive step of the next generation hospital paradigm further.
The design for the new Cardiovascular Center employs the thoughts which has been discussed in previous chapters regarding the H21 (hospital for twenty-first century). Through use of new, more contemporary design methodology of Build-ing Information Modeling, the designer is able to manage programmatically-dense building with a high level of precision in the design and delivery of the project.
The new specialty center is to consolidate and align their cardiac services in an integrated facility that will improve physician collaboration, efficiency, and patient therapy. It will be located on the hospital’s south campus on Archer Road and connect to the existing UF Health Shands Cancer Hospital, providing inpatient and outpatient care to patients with heart and vascular conditions. The program includes private patient beds, ORs (state-of-the-art operating rooms), ICU (inten-sive care unit beds), CCU (coronary care unit), clinic exam procedure rooms, di-agnostic testing and imaging, preoperative and postoperative and PACU (post-anesthesia care unit) areas, multidisciplinary outpatient clinics, catheterization lab facilities, cardiac rehabilitation, hybrid operating rooms, and intraoperative MRI (magnetic resonance imaging).
The center will also contain amenities and resources with a convenient parking garage with 600 spaces to accommodate patients and families. When entering by road or walkway, the central circular park welcomes all to the tranquil environment within the building. Spaces for families such as family zones in the patient room, sleep couches, and technology access will allow extended stays. To engage fami-lies with patient care and recovery actively, educational center with study resourc-es for family care and welcoming wait spaces with views to the scenic landscape will also be included in the center.
Connection link the existing Cancer Hospital to the new hospital at the second level and frame an inviting gateway to the south campus. Those connections play a critical role for ease of facility and logistical access, patient transport to servic-es elsewhere on campus and materials flow. Site landscape facilities will include natural water features and gardens which can be viewed from a number of rooms, retreat spaces for patients and families, and gathering and event space for com-munity health fairs and public wellness events.
87 H21

The Cardiovascular Hospital will include an indoor atrium and abundant natural light. Located on the building’s ground floor and fifth floor, the gardens will include trees and a variety of groundcover vegetation that will be visible from many of the units and staff lounges and consultation rooms. A green garden will cover the roofs, and those plants will be drought-tolerant and require no irrigation; all of the necessary water for the plantings will come from rain harvesting and condensation collected from the building’s cooling towers.
Due to being open 24 hours a day and meeting strict interior environmental re-quirements, hospitals are notorious in energy conservation, making LEED certi-fication or other green building criteria very difficult. One preliminary task to sus-tainable practices is the recycling of most construction waste during the building’s construction schedule, as well as the use of renewable materials such as recycled rubber flooring and wood walls; rubber floors will help to cushion footsteps and reduce noise, and the wood panels, which are sustainably recollected locally in Florida neighbors, will promote a natural and warm connection to nature. Elec-tricity conservation stratagem include sun shading, high-efficiency air handlers, low-E windows, low-energy light fixtures, and cascading daylighting; the project is targeting on that more than 80 percent of interior spaces receive natural light. Use of low-emitting adhesives, sealants, carpets, and paints throughout the facility preserves air quality, while low-flow plumbing fixtures reduce water consumption.
University of Florida Health (UF Health) is a medical network associated with the University of Florida. It includes two academic hospitals – UF Health Shands Hospital in Gainesville and UF Health Jacksonville in Jacksonville – and several other hospitals and facilities in North Flor-ida. The network was named to the U.S. News & World Report’s 2007 list of the na-tion’s top 50 hospitals.
2015 MASTER’S RESEARCH PROJECT 88

89 H21

BIRD’S VIEW FROM THE NORTHEAST CORNER OF SOUTH CAMPUS
2015 MASTER’S RESEARCH PROJECT 90

| (UPPER) SKETCH OF THE VIEW ON ARCHER ROAD| (UPPER IN RIGHT PAGE) SKETCH OF THE VIEW OF THE PUBLIC GARDEN| (LOWER IN RIGHT PAGE) SKETCH OF VIEW OF SOUTH LAKE NEAR THE CANCER HOSPITAL
91 H21

2015 MASTER’S RESEARCH PROJECT 92

Located on the south campus of University of Florida, the new Cardiovascular Center is potentially connected with other facilities of UF Health system including UF Health Shands Hospital, UF Health Shands Cancer Hospital and UF Health Shands Children’s Hospital. The adjacency are
mostly open landscape, however for the future expandability of the entire complex, the useful space is relatively constraint.
SITE CONDITIONS
The Cardiovascular Center provides a series entrances to improve the connectivity of the other parts of the campus. At the west side close to the Cancer Hospital, an accessible bridge is added to the Cardiovascular Hospital. The east end as the extension of the main spine of the value-adding
process wing opens to the main garages. At the central garden of the Cardiovascular Hospital, the passage is preserved for the purpose of the expansion of other facilities in the site.
CONNECTIVITY AND EXPANDABILITY
UF Health Shands Cancer Hospital
Medical Clinics Tower
Specialty Hospital
Parking Structure
93 H21

Daylighting of the interior spaces are applied based on whether it is needed for that type of room. More than eighty percent of the rooms are proposed to have natural lighting through the means of orientation and openings on facade. The Cardiovascular Hospital will enhance daylight and
views to green areas and plants that has a healing effect on bed lying patients.
DAYLIGHTING AND VISIBILITY
The building program consists of two wings that houses a bifurcated array of the solution shop program and the value-adding program. All programs are organized as the combination of linear and the traditional grid through the buildings. The linear array of programs gives clarity of
circulation and efficient logistics. The grid-matrix provides the intimacy of the complex functions.
FUNCTIONALITY
UF Health Shands Cancer Hospital
Wing of Solution Shop Wing of Value-Adding ProcessUF Health Shands Children’s Hospital
UF Health Shands Hospital
2015 MASTER’S RESEARCH PROJECT 94

The institution program consists of four parts: solution shops, value-adding process, supporting, community connection. The question emerge of how to allow for maximum flexibility and efficiency while still preserving the functionality and autonomy of individual artifacts.
PROGRAMS
Café1450 SF
Conference Center
2025 SF
Gift Shop1360 SF
Patient Management
Center3000 SF
Sterile Processing
Receiving Dock3600 SF Vestibule
2000 SF
Locker Room3000 SF
Locker Room3600 SF
Kitchen3000 SF
Bed Support3000 SF
Administrative Offices
4200 SF
Roof Garden3000 SF
Mechanical21000 SF
Mechanical21000 SF
Central Processing Department15000 SF
SOLUTION SHOP
VALUE-ADDING PROCESS
SUPPORTING COMMUNITY CONNECTION
Family Center3500 SF
Outpatient Echocardiography
6000 SF
Outpatient Clinics Center
6000 SF
Shands Pavilion6000 SF
Emergency Department10000 SF
Cardiovascular Clinics
11000 SF
Operation Theaters8000 SF
Intermediate Beds15000 SF
CDU2000 SF
SpecimenCollection3000 SF
MRI OR3000 SF
OR Supports3000 SF
PACUs5000 SF
CCUs5000 SF
ICUs5000 SF
Imaging CT3925 SF
Electro-physiology Rooms
2750 SF
Advanced Molecular Diagnostics Center
3000 SF
Diagnostic Units12000 SF
CDSS center6000 SF
UF Precision Medicine Hub
23000 SF
Cardiac Stress Test
2100 SF
SPECT1250 SF
PET1250 SF
95 H21

It is proposed of “hospitals in a hospital” in the Cardiovascular Center that will allow this advanced medical center to bifurcate itself rather than to stick on the existing commingling model of solution shop and value-adding process. Two identities composed of two services - fee for service and fee for outcome.
(BUILDING WING A) (BUILDING WING B)
PROGRAMMING RELATIONS
Café1450 SF
Conference Center
2025 SFGift Shop1360 SF
Patient Management
Center3000 SF
Sterile Processing
Receiving Dock3600 SFVestibule
2000 SF
Locker Room3000 SF
Locker Room3600 SF
Kitchen3000 SF
Bed Support3000 SF
Administrative Offices
4200 SFRoof Garden3000 SF
Mechanical21000 SF
Mechanical21000 SF
Central Processing Department15000 SF
SOLUTION SHOPS VALUE-ADDING PROCESS
Family Center3500 SF
Outpatient Echocardiography
6000 SF
Outpatient Clinics Center
6000 SF
Shands Pavilion6000 SF
Emergency Department10000 SF
Cardiovascular Clinics
11000 SF
Operation Theaters8000 SF
Intermediate Beds15000 SF
CDU2000 SF
SpecimenCollection3000 SF
MRI OR3000 SF
OR Supports3000 SF
PACUs5000 SF
CCUs5000 SF
ICU5000 SF
Imaging CT3925 SF
Electrophysiology Rooms
2750 SF
Advanced Molecular Diagnostics Center
3000 SF
Diagnostic Units12000 SF
CDSS Center6000 SF
UF Precision Medicine Hub
23000 SF
Cardiac Stress Test
2100 SF
SPECT1250 SF
PET1250 SF
2015 MASTER’S RESEARCH PROJECT 96

(Building Wing of Solution Shop)
(Public Access from the Central Garden)
(Imaging Programs Support the Value-Adding Process)
(Advanced Medical Programs Fused Together)
(Sky Lit Space Organizes the Framework)
(Hanging Extrusions Enhancing the Interior)
(Interchangeable Spaces for Future Technology)
(Bridges across Two Wing Provide Connections)
INCORPORATION
ACCESSIBILITY
SUPPORT
CONSOLIDATION
LIGHTING
FLEXIBILITY
DYNAMICS
INTER-BRIDGING
SPATIAL STRATAGEM OF SOLUTION SHOP WING
97 H21

(Reunited Value-Adding Process Wing in Paradigm)
(Main Street Providing Clear Logistics and Circulation)
(Efficient Division Strategy through a Matrical Grid)
(Sub-divisions with Matrical Relations Spatially)
(Outpatient Programs Linked to Parking Facility)
(Service Floor Accommodation Located in Middle)
(Facing Green Areas and Daylighting for Nursing Units)
(Shortest Distance to ORs and Support Programs)
OPPORTUNITIES
CLARITY
DIVISION
MATRIX
CONVENIENCE
SERVICE
ORIENTATION
PROXIMITY
SPATIAL STRATAGEM OF VALUE-ADDING PROCESS WING
2015 MASTER’S RESEARCH PROJECT 98
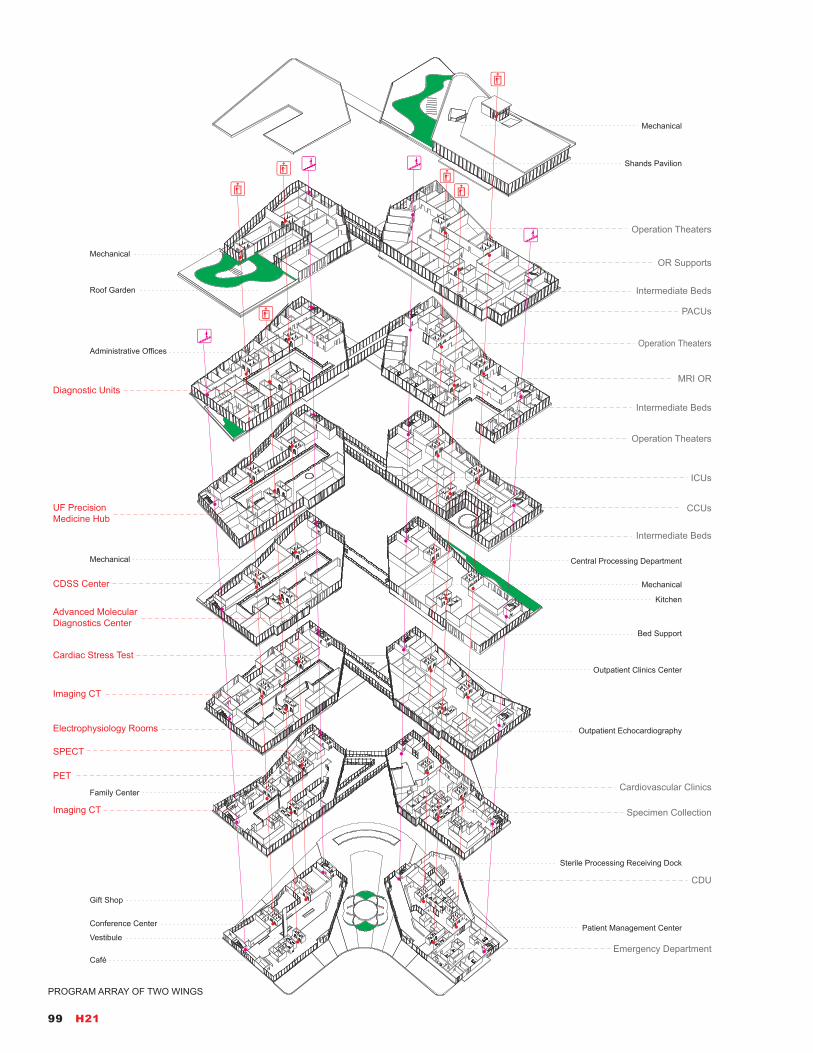
Café
Conference Center
Gift Shop
Patient Management Center
Sterile Processing Receiving Dock
Vestibule
Kitchen
Bed Support
Administrative Offices
Roof Garden
Mechanical
Mechanical
Mechanical
Central Processing Department
Family Center
Outpatient Echocardiography
Outpatient Clinics Center
Shands Pavilion
Mechanical
PACUs
Operation Theaters
Operation Theaters
MRI OR
Emergency Department
Cardiovascular Clinics
Intermediate Beds
Intermediate Beds
Intermediate Beds
CDU
Specimen Collection
OR Supports
CCUs
ICUs
Operation Theaters
PET
SPECT
Cardiac Stress Test
Electrophysiology Rooms
Imaging CT
Imaging CT
Advanced Molecular Diagnostics Center
CDSS Center
UF Precision Medicine Hub
Diagnostic Units
PROGRAM ARRAY OF TWO WINGS
99 H21
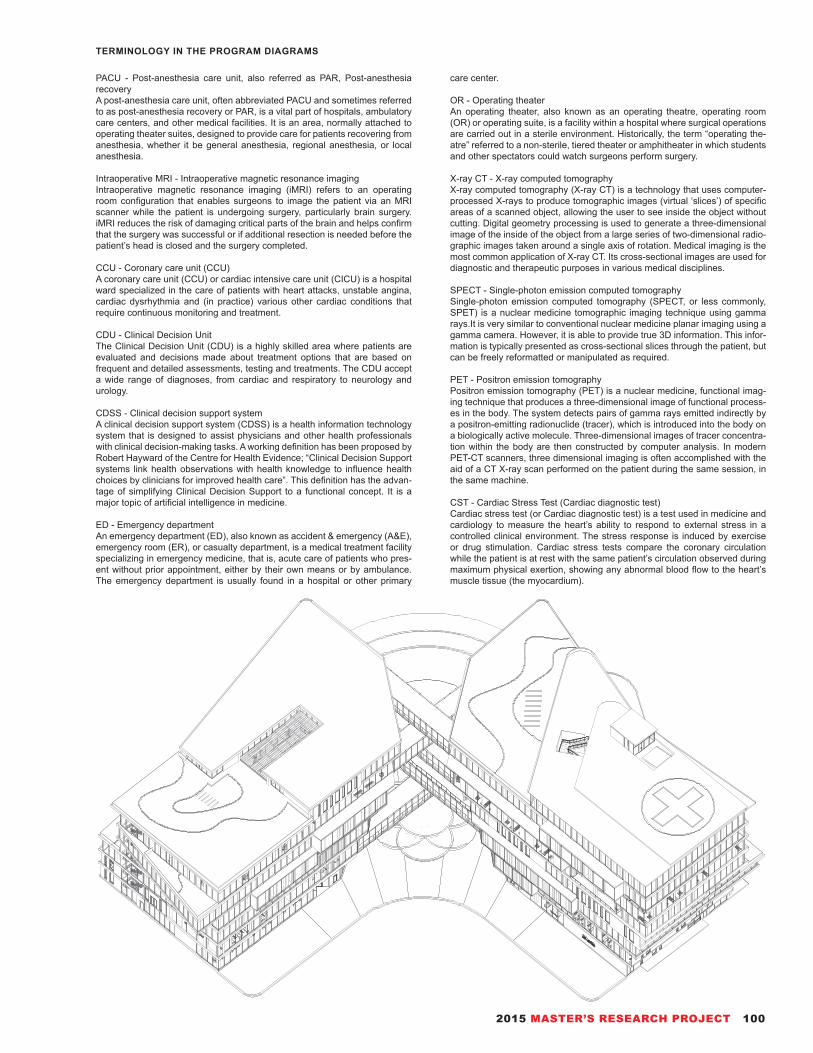
PACU - Post-anesthesia care unit, also referred as PAR, Post-anesthesia recoveryA post-anesthesia care unit, often abbreviated PACU and sometimes referred to as post-anesthesia recovery or PAR, is a vital part of hospitals, ambulatory care centers, and other medical facilities. It is an area, normally attached to operating theater suites, designed to provide care for patients recovering from anesthesia, whether it be general anesthesia, regional anesthesia, or local anesthesia.
Intraoperative MRI - Intraoperative magnetic resonance imagingIntraoperative magnetic resonance imaging (iMRI) refers to an operating room configuration that enables surgeons to image the patient via an MRI scanner while the patient is undergoing surgery, particularly brain surgery. iMRI reduces the risk of damaging critical parts of the brain and helps confirm that the surgery was successful or if additional resection is needed before the patient’s head is closed and the surgery completed.
CCU - Coronary care unit (CCU)A coronary care unit (CCU) or cardiac intensive care unit (CICU) is a hospital ward specialized in the care of patients with heart attacks, unstable angina, cardiac dysrhythmia and (in practice) various other cardiac conditions that require continuous monitoring and treatment.
CDU - Clinical Decision UnitThe Clinical Decision Unit (CDU) is a highly skilled area where patients are evaluated and decisions made about treatment options that are based on frequent and detailed assessments, testing and treatments. The CDU accept a wide range of diagnoses, from cardiac and respiratory to neurology and urology.
CDSS - Clinical decision support systemA clinical decision support system (CDSS) is a health information technology system that is designed to assist physicians and other health professionals with clinical decision-making tasks. A working definition has been proposed by Robert Hayward of the Centre for Health Evidence; “Clinical Decision Support systems link health observations with health knowledge to influence health choices by clinicians for improved health care”. This definition has the advan-tage of simplifying Clinical Decision Support to a functional concept. It is a major topic of artificial intelligence in medicine.
ED - Emergency departmentAn emergency department (ED), also known as accident & emergency (A&E), emergency room (ER), or casualty department, is a medical treatment facility specializing in emergency medicine, that is, acute care of patients who pres-ent without prior appointment, either by their own means or by ambulance. The emergency department is usually found in a hospital or other primary
care center.
OR - Operating theaterAn operating theater, also known as an operating theatre, operating room (OR) or operating suite, is a facility within a hospital where surgical operations are carried out in a sterile environment. Historically, the term “operating the-atre” referred to a non-sterile, tiered theater or amphitheater in which students and other spectators could watch surgeons perform surgery.
X-ray CT - X-ray computed tomographyX-ray computed tomography (X-ray CT) is a technology that uses computer-processed X-rays to produce tomographic images (virtual ‘slices’) of specific areas of a scanned object, allowing the user to see inside the object without cutting. Digital geometry processing is used to generate a three-dimensional image of the inside of the object from a large series of two-dimensional radio-graphic images taken around a single axis of rotation. Medical imaging is the most common application of X-ray CT. Its cross-sectional images are used for diagnostic and therapeutic purposes in various medical disciplines.
SPECT - Single-photon emission computed tomographySingle-photon emission computed tomography (SPECT, or less commonly, SPET) is a nuclear medicine tomographic imaging technique using gamma rays.It is very similar to conventional nuclear medicine planar imaging using a gamma camera. However, it is able to provide true 3D information. This infor-mation is typically presented as cross-sectional slices through the patient, but can be freely reformatted or manipulated as required.
PET - Positron emission tomographyPositron emission tomography (PET) is a nuclear medicine, functional imag-ing technique that produces a three-dimensional image of functional process-es in the body. The system detects pairs of gamma rays emitted indirectly by a positron-emitting radionuclide (tracer), which is introduced into the body on a biologically active molecule. Three-dimensional images of tracer concentra-tion within the body are then constructed by computer analysis. In modern PET-CT scanners, three dimensional imaging is often accomplished with the aid of a CT X-ray scan performed on the patient during the same session, in the same machine.
CST - Cardiac Stress Test (Cardiac diagnostic test)Cardiac stress test (or Cardiac diagnostic test) is a test used in medicine and cardiology to measure the heart’s ability to respond to external stress in a controlled clinical environment. The stress response is induced by exercise or drug stimulation. Cardiac stress tests compare the coronary circulation while the patient is at rest with the same patient’s circulation observed during maximum physical exertion, showing any abnormal blood flow to the heart’s muscle tissue (the myocardium).
TERMINOLOGY IN THE PROGRAM DIAGRAMS
2015 MASTER’S RESEARCH PROJECT 100

SITE PLAN
101 H21

2015 MASTER’S RESEARCH PROJECT 102

103 H21

VIEW FROM THE NORTHEAST CORNER ON ARCHER ROAD
2015 MASTER’S RESEARCH PROJECT 104

105 H21

BIRD’S VIEW OF THE SOUTH SIDE OF THE SITE OF THE CARDIOVASCULAR HOSPITAL
2015 MASTER’S RESEARCH PROJECT 106

107 H21

| (UPPER FACING PAGE) VIEW FROM THE WEST SIDE THROUGH ARCHER ROAD| (LOWER) VIEW FROM THE NORTHEAST CORNER ON WALDO ROAD GREENWAY-DEPOT AVENUE RAIL-TRAIL
2015 MASTER’S RESEARCH PROJECT 108
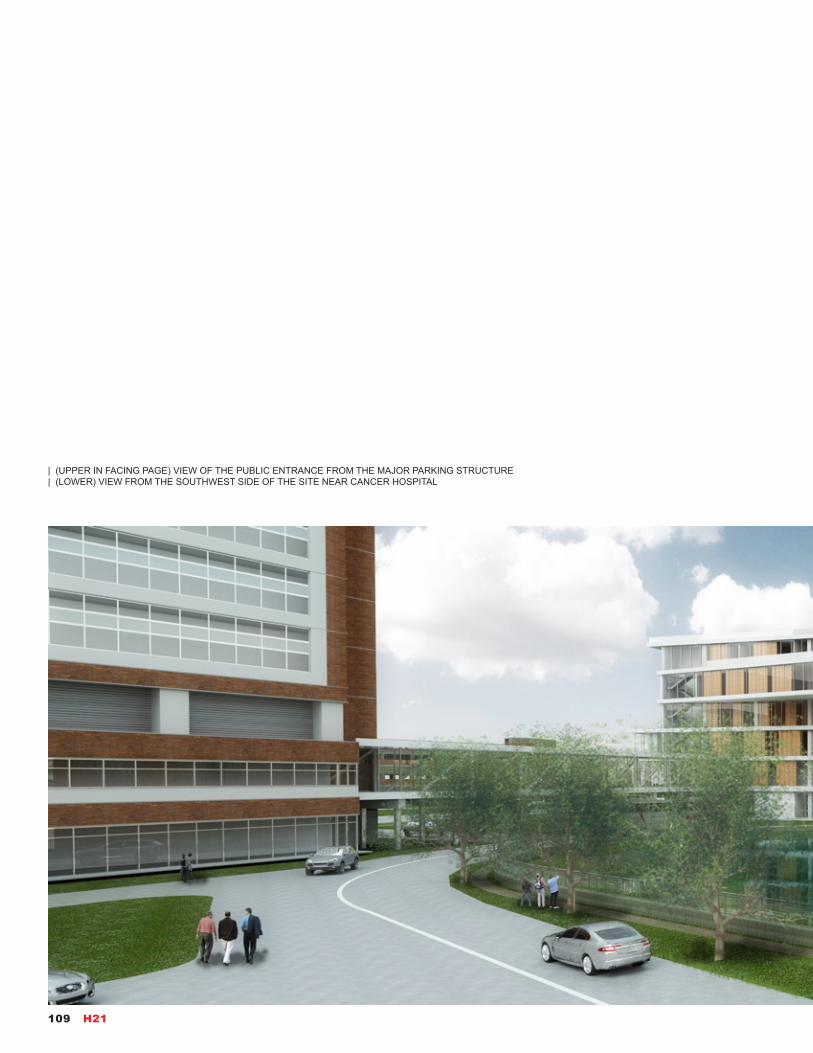
| (UPPER IN FACING PAGE) VIEW OF THE PUBLIC ENTRANCE FROM THE MAJOR PARKING STRUCTURE| (LOWER) VIEW FROM THE SOUTHWEST SIDE OF THE SITE NEAR CANCER HOSPITAL
109 H21

2015 MASTER’S RESEARCH PROJECT 110

VIEW OF THE PUBLIC ENTRANCE OF THE CARDIOVASCULAR HOSPITAL
111 H21

2015 MASTER’S RESEARCH PROJECT 112

113 H21
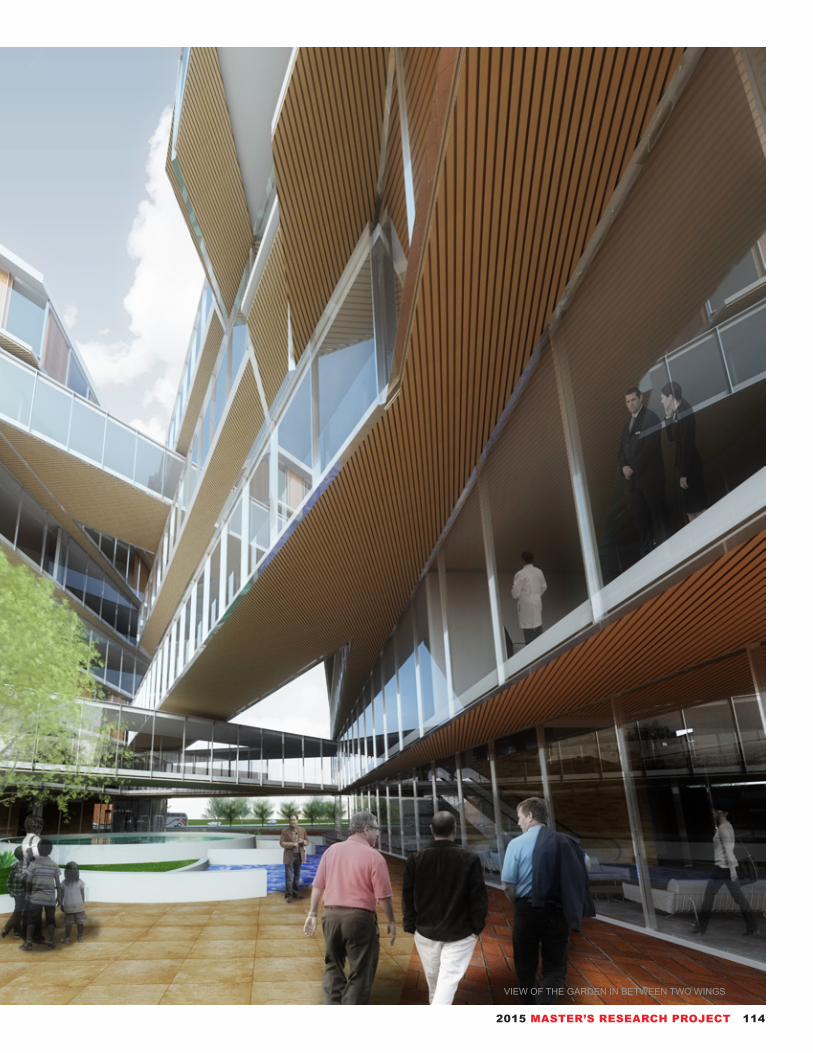
VIEW OF THE GARDEN IN BETWEEN TWO WINGS
2015 MASTER’S RESEARCH PROJECT 114

| (UPPER) VIEW OF INTER-BRIDGES FROM FORTH LEVEL| (RIGHT PAGE) VIEW OF THE CENTRAL SPINE OF SOLUTION SHOP WING
115 H21

2015 MASTER’S RESEARCH PROJECT 116

117 H21

VIEW FROM IMAGING DEPARTMENT
2015 MASTER’S RESEARCH PROJECT 118

LONGITUDINAL SECTION OF SOLUTION SHOP WING
AXONOMETRIC SECTION OF SOLUTION SHOP WING
119 H21

AXONOMETRIC SECTION OF VALUE-ADDING PROCESS WING
2015 MASTER’S RESEARCH PROJECT 120

GROUND LEVEL PLAN
121 H21

2015 MASTER’S RESEARCH PROJECT 122

SECOND LEVEL PLAN
123 H21

2015 MASTER’S RESEARCH PROJECT 124

SIXTH LEVEL PLAN
125 H21

2015 MASTER’S RESEARCH PROJECT 126

127 H21

VIEW FROM THE DIAGNOSTIC UNITS
2015 MASTER’S RESEARCH PROJECT 128

VIEW FROM THE SOUTHWEST CORNER NEAR CANCER HOSPITAL
VIEW FROM THE LOBBY OF VALUE-ADDING WING
129 H21

References1. “UF Health announces expansion plans,” last modified Aug 27, 2013, https://ufhealth.org/news/2013/uf-health-announces-expansion-plans.
2. “New UF Health Specialty Hospital Tower,” last modified September 24th, 2014, http://cardiology.medicine.ufl.edu/2014/09/24/new-uf-health-specialty-hospital-tower/.
3. Christensen, Clayton M. 1997. The innovator’s dilemma when new technologies cause great firms to fail. Boston, Mass: Harvard Business School Press.
4. Christensen, Clayton M., Jerome H. Grossman, and Jason Hwang. 2009. The innovator’s prescription: a disruptive solution for health care. New York: McGraw-Hill.
GROUND LEVEL AXONOMETRIC DIAGRAM
SECOND LEVEL AXONOMETRIC DIAGRAM
SIXTH LEVEL AXONOMETRIC DIAGRAM
2015 MASTER’S RESEARCH PROJECT 130
“I think our task now is to rethink how we ‘assume’ design conditions, rather than reviewing the conditions, we need to start by questioning the way we relate to nature.”
Toyo Ito“The fragile state of things”, 2011
PART 4131 H21

28
When it comes to healthcare, any writing regarding the paradigms can be a tricky task, particularly in an arena where the politics are unstable, the solutions are diffi-cult, and the economics is dispiriting. In the healthcare field, changes have been occurring so fast for so long that what seem a dramatic change often appear in days to set new game rules. All of these changes sig-nify the needs to regulate the designs of healthcare fa-cilities to stay fluid and flexible and include paradigms for future use, paradigms that differ from the way we think our designs today.
Many of the changes that occurred in the past rose to the profound level of what we call paradigms as we discussed in the first part of ten canonical hospitals. And for the same reason, this project has been led to produce this part to assume or anticipate paradigms that are essential to seeing ahead and getting beyond. In the wider social and technological landscape of which healthcare industry, a number of profound and interrelated paradigm changes which are active and governing the building design extensively should be observed:
• From Youth to Longevity. The percentage of citi-zens over age seventy keeps soaring, especially for those developed countries. Ironically, as people live longer, the healthcare system can become impacted with greater pressure due to this situation. But it has also emerged a range of facilities designed for varying needs of the independent elderly.
• From Healing to Health. Contemporary medicine is undergoing a drastic shift from remediation (the pure art of healing) to health-an art of health maintenance. The new paradigm has potentially affected hospital ar-chitecture from reviewing to preemptive assumption.
• From Speciality to Universalness. Nowadays it is happening is to look on the whole of the healthcare en-vironment. The idea, backed by much research, is that a pleasant, stress-free environment, both architectural and surrounding landscape, helps heal the patients. Color, finishes, indirect lighting, fine furniture, natural daylighting.
• From Responding to Preventing. It can no longer suffice for a hospital administrator, healthcare policy-maker, or architect to recognize a certain need and try to figure out how to respond to it. Human needs are by their nature dynamic, contemporary technology has accelerated that dynamism. Hospitals designed for human beings must emulate that dynamism by preventing the problems.
• From Categorization to Mutuality. From a larger view, traditional healthcare emphasizes fragmentation rath-er than a mutual system. The current paradigm shift in healthcare places the entire population within a healthcare system. The hospital or healthcare facility must learn to serve those in the community who cur-rently require treatment as well as those healthy popu-lation who may benefit from wellness services. Archi-tects will be asked upon to plan facilities that provide for extensive community outreach and that overcome the stereotype of the hospital as an isolated castle.
• From Congregation to Integration. Boosted by Infor-mation Technology, it is no longer necessary to gath-er personnel and equipment into a single building or complex. The technology now sustains for deep inte-gration of treatment among any number of healthcare professionals. Data, services, finance can be dissemi-nated globally. On the basic level, designing a hospital will involve accommodating those advance.
In addition to catch up with other major paradigm shifts, hospital planners and designers also need to recognize the following changes:• From Management to Relationship.• From Passive Receiver to Active Receiver.• From Institutional to Residential.• From Inpatient to Ambulatory Care.• From Freestanding to Regional.• From Urgent Care to Primary Care.• From Nursing Center to Subacute Center.
AssumptionEMPHASIS ON NEW PARADIGMS IN TWENTY-F IRST CENTURY
2015 MASTER’S RESEARCH PROJECT 132
29StrategemCHANGING NEEDS, CHANGING D IRECTIONS
Not just in terms of an era’s zeitgeist, but in terms of changing paradigms: models, patterns, tool-sets of assumptions about a field, profession, or society that explain and guide our thinking and behavior, several needs influence or promise to impact hospital and healthcare design. The quality and the safety of healthcare facili-ties have always been the paramount of what design concerns, but these days heightened consideration is being taken to measuring the caliber of needs and to promote the results. The landscape of all aspects of healthcare is changing. Hos-pital and other healthcare facility design is now moving toward evidenced-based and green design to make hospitals more sustainable businesses as well as build-ings, healthier places to visit. Following items consider the new design directions shaped by the changes in the needs of this time for healthcare.
• FlexibilityAbove all, flexible. Because of its size, multimillion-dollar building program and complexity, healthcare design is needed for flexibility is further intensification by the technological nature of the healthcare industry. Not only should facilities adapt to changing patient populations and changing patient needs, but they should also anticipate the physical demands new technologies would make. Hospitals and healthcare facilities make more strict demands on electrical/mechanical systems, thus, present harder challenges to achieving flexible design.
The traditional “racetrack” corridor pattern does have a certain flexibility, in that it can often be added to and modified with some purposes. However, it is an often inefficient and uncomfortable layout. As the decedent, circular plan alternatives to the racetrack recognized in popularity in the 1970s and were often welcomed by providing nursing service, who shortened distance and could more effectively attend to patients’ needs. In real use, the circular plan is less flexible than even the racetrack plan, due to the requirement of double nursing stations and staffing needs.
Beyond this obtaining in productivity and efficiency, flexibility is not only important for patient well-being but also crucial to any industry operating in a competitive market. To offer a great flexibility, in the design proposal of this project, the various modules that can be configured and reconfigured as needed allows a potential flexibility. But still, the solution to keep both functionality and dynamics is under exploration.
• ExpandabilityExpandability consideration should begin at the planning stage, however it usu-ally does not end at that point, nor even after construction phase is complete. In a global vision, most healthcare facilities are built based on a certain masterplan, but by essence, hospitals are always engaged in a dynamic change, a process
133 H21

that is part of what medical conditions may ask for. The strategy which is the most relevant to ensuring the ongoing expandability of the design is the participation of the users. For example, in the practical scenario of this project, the cardiovascu-lar hospital is merely a step in the expansion of the whole system. We may say “growth”, since in an environment as dynamic as that of the hospital or healthcare facilities, the constructing is never really complete. In today’s healthcare environ-ment, a completed project is, truly, an expandable project designed for, and con-sidered for, the expansion of the whole system. In sum, a project in which the expanding possibility built-in represents the greatest chance of enduring.
• Vertical IntegrationAssociated with the flexibility, vertical integration (redesign and rethinking the tra-ditional departmental zoning of the hospital) is primarily to maximize caregiver contact with patients and to promote continuity of different kinds of services for each patient from admission to discharge. Like the experiment which is initiated in the design proposal of this project, in vertically integrated hospitals, the multiplicity of departments is reduced to only a few integrated areas of services/responsibility, like supporting, services for fee, and services for outcome (patient care).
What is outlined down there suggests some design implications of vertical integra-tion for programs grouping and indicates how facilities, equipment, and staff may be effectively shared across what once were the isolated of traditional depart-ments:Supporting (entry area, registration processes, medical records, office, information services, administration, staff lounge, human resources);Services for Fee (pharmacy, laboratory, support center, materials management, education, diagnostic services);Services for Outcome (emergency services and combined ICU/CCU, recovery, obstetrics, surgery, physical therapy, inpatient medical, physicians’ offices).
Acute-Care Center of the Future. Per-spective. Upon entering the registration area (the small building at the driveway in the foreground), patients present their personal data card containing all the infor-mation needed for check-in. An attendant directs the patients to the appropriate de-partment. Patient room; occupy the pe-riphery of the building. Ancillary areas are located in the core. The sloped area at the front of the facility houses shafts for the transport of supplies; mechanical, electri-cal, and plumbing lines; and staff circula-tion. Supplies are received at the base of the sloped area, and then distributed as needed. The building is organized verti-cally by department—one floor for cardiol-ogy, one for neurology, etc. Floors can be reconfigured as needed. Sketch by Earl S. Swensson. (Source: Earl Swensson As-sociates, Inc.)
2015 MASTER’S RESEARCH PROJECT 134
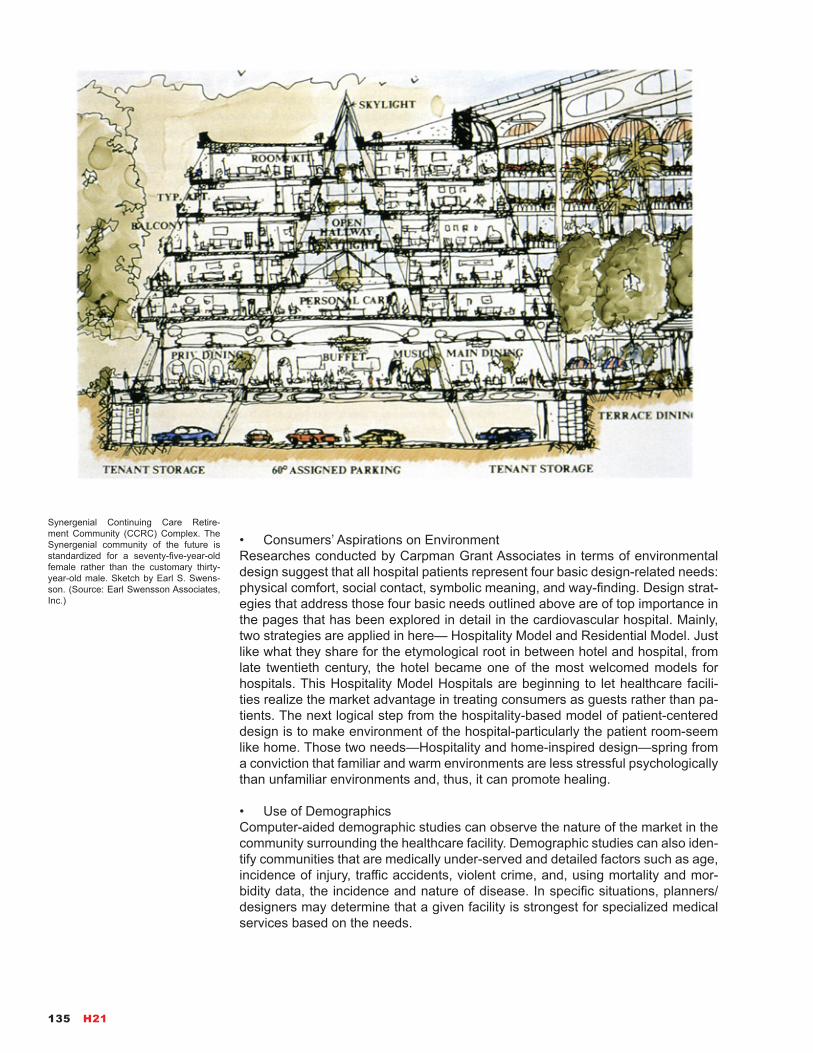
• Consumers’ Aspirations on EnvironmentResearches conducted by Carpman Grant Associates in terms of environmental design suggest that all hospital patients represent four basic design-related needs: physical comfort, social contact, symbolic meaning, and way-finding. Design strat-egies that address those four basic needs outlined above are of top importance in the pages that has been explored in detail in the cardiovascular hospital. Mainly, two strategies are applied in here— Hospitality Model and Residential Model. Just like what they share for the etymological root in between hotel and hospital, from late twentieth century, the hotel became one of the most welcomed models for hospitals. This Hospitality Model Hospitals are beginning to let healthcare facili-ties realize the market advantage in treating consumers as guests rather than pa-tients. The next logical step from the hospitality-based model of patient-centered design is to make environment of the hospital-particularly the patient room-seem like home. Those two needs—Hospitality and home-inspired design—spring from a conviction that familiar and warm environments are less stressful psychologically than unfamiliar environments and, thus, it can promote healing.
• Use of DemographicsComputer-aided demographic studies can observe the nature of the market in the community surrounding the healthcare facility. Demographic studies can also iden-tify communities that are medically under-served and detailed factors such as age, incidence of injury, traffic accidents, violent crime, and, using mortality and mor-bidity data, the incidence and nature of disease. In specific situations, planners/designers may determine that a given facility is strongest for specialized medical services based on the needs.
Synergenial Continuing Care Retire-ment Community (CCRC) Complex. The Synergenial community of the future is standardized for a seventy-five-year-old female rather than the customary thirty-year-old male. Sketch by Earl S. Swens-son. (Source: Earl Swensson Associates, Inc.)
135 H21

• Aging PopulationCertain market trend of aging population is obvious. Demographically, the popu-lation of America is aging, for other developed countries, the situations are the same. With important implications for the healthcare market and for the design of healthcare and many other facilities, aging community is especially important in healthcare related design. In large part from federal legislation in the form of the Americans with Disabilities Act, new building codes stem that architects should be standardizing public facilities for the ideal of a seventy-year-old woman. Guidelines for extensive use of health and hospital facilities include: using large, clear letters for signs; avoiding lighting the backgrounds of signs; providing higher illumination levels and diminishing glare; avoiding uneven lighting; designing acoustically op-timal environments that incorporate sound-absorbing materials; acuity of hearing tends to diminish with age, and some persons have difficulty distinguishing speech from background noise; providing ample seating, with chair arms that assist in sit-ting and rising; so on so forth.
• Business ThinkingThe core idea of economics is to make choices. In the new market-driven health-care climate, all of those involved in planning, designing, and allocating resources for hospitals and healthcare facilities must become compatible in the thinking of business if they are to be chosen. The matters of business used to require sim-ply the considerations in terms of dollars and cents but now requires expressing oneself in terms of cost-effectiveness. Consumers have already learned to differ-entiate cost and quality and, formally or informally, evaluate the services that they choose by applying this equation: Value= Cost+ Quality. Along with this comes a questioning of “life at any cost”, thus, the mission at any level is to vary degrees defined as delivering value to market. And that process requires a deeper thinking of what it has been just scratched the surface in the part 02 of the business model.
• Green DesignThe major movement toward “green” design is certificate human-centered archi-tecture to meet certain standards for environmentally sustainable construction. LEED-certified buildings use key resources more efficiently than conventional buildings simply built to code. In return, it can be compiled a list of the benefits of following a LEED strategy, ranging from improved air and water quality to re-duced solid waste, all of which benefit the building’s users and community at large scale. In some cases, LEED-certified buildings can cost more to design and con-struct, partially because sustainable construction principles call for better building products. However, just like a lot of things “green,” hospitals can prove its worth over time in lower operational costs and increased employee productivity, and the increased marketability as a truly healthier machine for health-keeping, which a hospital, perhaps above all other buildings, should strive to reach.
2015 MASTER’S RESEARCH PROJECT 136

30PossibilitiesF INDINGS AND CONCLUSION FROM H21
At the beginning of this book, it has been mentioned that it was an devastating earthquake that made me decide to establish architecture as my life’s career. One lesson that I learned from that tragedy is that when all the people find themselves faced with a great threat that may take their lives, the appeal about making build-ings from everyone is relevantly unitary —to make something, or anything, to pro-tect lives in tranquility. For me, this concept drives all the decisions as an architec-tural designer, especially in the designing of public buildings—and it has driven me to research into healthcare field in this book.
To protect the health of humanity and civilization in tranquility is the mission of both the physicians and architects. It is in reality that both of those professions are facing the changes in how to shape the future by design of the whole thing. Throughout this project, it have strived to balance on the delineating future and a practical design proposal for those ideas concerning with hospitals and healthcare facilities which are currently building or currently planning. In this final page, it will take an extended view and attempt to profile the trends and developments likely to shape healthcare and, therefore, the practice of healthcare architecture. The discussion naturally boils down to three broad areas: (1) possibilities of trends of medical technology, (2) how architecture practice will facilitate the healthcare de-velopments, (3) further thoughts from the design proposal in H21.
Through the reading for this project, it is noticed that numerous historians who study medical history regard all the healthcare prior to the 1930s as the Dark Ages. Until the emergency of antibiotic drugs, doctors could really seize a little chance to win the combat against diseases. Although the counterattack of HIV, Ebola, Mar-burg virus, Lassa fever, Legionnaire’s disease, hantavirus, hepatitis C, anthrax, West Nile virus place a great pressure on the defense line, new technology and new discoveries at least are advancing. Two megatrends will continue to shape the future of medicine: biology medicine now addresses the causes of disease, and noninvasive treatments and minimally invasive procedures will continue to exten-sively replace surgery. They are happening in the form of Genomics, Nanotechnol-ogy, Pharmacology, Treatment Modalities, Robotic Surgery, Decentralized Care and Self-Care, A Caveat. These trends of technology has freed healthcare from the bed-centered hospital and they may embody certain extensions into future. In this project, based on the bifurcation of the solution shop and value-adding pro-cess, those implications above are represented in some programs like precision medicine hub and CDSS center.
Designers of future healthcare facilities will probably be quested to create a total healthcare solutions for the whole community, especially as a larger percentage of the elder population. Such facilities as solution machines for communities may be-come as pervasive in this century as the sprawling of planned suburban communi-ties was in post-World War II period. The key concept in this process is flexibility. The concept of flexibility extends beyond what the architect designs to provide a range of services, or a template. This change may make architects be active dur-ing the entire lifespan of the facility. In this sense, architects will serve as caregiv-ers, practitioners of medicine, and members of the patient-care team. But there is more profound dimensions of this new role. The future of healthcare architecture
137 H21

are being driven by three traditional antagonists: technology, economics and hu-manity. They may lead all things to paradox. But there is always a belief that is instilled in this whole project, that the heart of the future of hospital and healthcare facility design will remain as simple as before. Just as what we went through in the ten canonical hospitals in Greek, India, medieval Europe, after the technology has run through a long and meandering path, the healthcare may back to the very concept similar to those temples.
The hope of this book, especially with its emphasis on chronological cases, cur-rent situations, business models, a practical design proposal, and observations of trends and changing needs is to demonstrate that these aspects can not be exclusive in our study. Instead, the basic principles of good healthcare design are synonymous, thus, to use the ideas of the origin, the future, the solution for now as a basis for design in our projects-from benchmark placement to the interior elements-will lead the process forward. In sum, whatever directions or paradigms the healthcare facilities design of the future may take, it will include an ultimate hope of what we have been long preserving—we are capable to make it better of the environment around us. By that meaning, H21 has been a gripping experience to visualize the assumptions.
References
1. Miller, Richard L., Earl S. Swensson, and J. Todd Robinson. 2012. Hospital and healthcare facility design. New York: W.W Norton & Co.
2. Guenther, Robin, and Gail Vittori. 2008. Sustainable healthcare architecture. Hoboken, N.J.: John Wiley & Sons.
3. Grunden, Naida, and Charles Hagood. 2012. Lean-led hospital design: creating the efficient hospital of the future. Boca Raton: Taylor & Francis/CRC.
4. Cama, Rosalyn. 2009. Evidence-based healthcare design. Hoboken, N.J.: John Wiley & Sons.
Further Thoughts from the H21. Sketched by the Author. As a vision cast into the future, the car-diovascular hospital ought to be perceived as the total solution machine for cardio-vascular diseases. On north side of the site located the solution shop wing, this building is to provide all the components concerning diagnosis. In this wing, the structure is designed for advanced infor-mation storage and processing. For the other part, the value-adding process wing is designed for achieving the checking-in and treatment in seconds. Upon entering the registration area, patients can check-in based on their own digital record. Clin-ics and ORs are built for maximum flex-ibility. Patient rooms occupy the prime orientation of the building for daylighting. The back part houses shafts for the trans-port of supplies. Mechanical, electrical, plumbing lines, and staff circulation are structured at the concentrated cores for convenience. The zoning in both vertically and horizontally embodies the needs for the new era of medical practice.
2015 MASTER’S RESEARCH PROJECT 138
31LinksBIBL IOGRAPHY
AIA Academy of Architecture for Health, and Facilities Guidelines Institute. 2006. Guidelines for design and construction of health care facilities. Washington, DC: American Institute of Architects.
Boekel, Andrea. 2008. Architecture for healthcare. Vic-toria: Images Pub. Group.
Bostridge, Mark. 2008. Florence Nightingale: the mak-ing of an icon. New York: Farrar, Straus and Giroux.
Brockliss, Lawrence, and Colin Jones. 1997. “The Hospital in the Enlightenment,” in The Medical World of Early Modern France. Oxford: Oxford University Press.
Bowers, Barbara S. 2007. The medieval hospital and medical practice. Aldershot, England: Ashgate.
Bruegmann, Robert. 1978. Architecture of the hospital: 1770-1870, design and technology. Thesis--University of Pennsylvania.
Cama, Rosalyn. 2009. Evidence-based healthcare de-sign. Hoboken, N.J.: John Wiley & Sons.
Chaney, Edward. 1998. The evolution of the grand tour: Anglo-Italian cultural relations since the Renais-sance. London: Frank Cass.
Chaney, Edward. 2000. ”’Philanthropy in Italy’: English Observations on Italian Hospitals 1545-1789”, in: The Evolution of the Grand Tour: Anglo-Italian Cultural Re-lations since the Renaissance, 2nd edition. London, Routledge.
Christensen, Clayton M., Jerome H. Grossman, and Jason Hwang. 2009. The innovator’s prescription: a disruptive solution for health care. New York: McGraw-Hill.
Chung, C. J., Inaba, J., Koolhaas, R., Leong, S. T., & Cha, T.-W. (2001). Harvard Design School guide to shopping. Koln, Taschen.
Coe, Rodney M. 1978. Sociology of medicine. New York: McGraw-Hill.
D’Antonio, Patricia. 2010. American nursing: a history of knowledge, authority, and the meaning of work. Bal-timore: Johns Hopkins University Press.
Eisenman, Peter, and Ariane Lourie Harrison. 2008. Ten canonical buildings 1950-2000. New York: Rizzoli.
Fischer, Joachim. 2006. Medical design. Cologne: Daab.
Goldin, Grace. 1994. Work of Mercy: A Picture History of Hospitals. Boston Mills Press.
Granshaw, Lindsay Patricia, and Roy Porter. 1989. The Hospital in history. London: Routledge.
Grunden, Naida, and Charles Hagood. 2012. Lean-led hospital design: creating the efficient hospital of the future. Boca Raton: Taylor & Francis/CRC.
Guenther, Robin, and Gail Vittori. 2008. Sustainable healthcare architecture. Hoboken, N.J.: John Wiley & Sons.
Harrison, Mark, Margaret Jones, and Helen M. Sweet. 2009. From western medicine to global medicine: the hospital beyond the West. New Delhi: Orient Black-Swan.
Henderson, John, Peregrine Horden, and Alessandro Pastore. 2007. The impact of hospitals, 300-2000. Ox-ford: Peter Lang.
Henderson, John. 2006. The Renaissance hospital: healing the body and healing the soul. New Haven: Yale University Press.
Horden, Peregrine. 2008. Hospitals and healing from antiquity to the later Middle Ages. Aldershot, Hamp-shire, Great Britain: Ashgate Variorum.
James, Paul, and Tony Noakes. 1994. Hospital archi-tecture. [New York]: Longman.
James, W. Paul, and William Tatton-Brown. 1986. Hospitals: design and development. London: Architec-tural Press.
139 H21

Jones, Colin. 1989. The charitable imperative: hospi-tals and nursing in ancien régime and revolutionary France. London: Routledge.
Koolhaas, Rem, Hans Ulrich Obrist, Kayoko Ota, and James Westcott. 2011. Project Japan: metabolism talks--. Koln: TASCHEN GmbH.
Lewenson, Sandra, and Eleanor Krohn Herrmann. 2008. Capturing nursing history: a guide to historical methods in research. New York: Springer Pub.
Marberry, Sara O. 1997. Healthcare design. New York: Wiley.
McGrew, Roderick E., and Margaret P. McGrew. 1985. Encyclopedia of medical history. New York: McGraw-Hill.
Medical facilities: new concepts in architecture & de-sign = Gendai kenchiku shusei : iryo shisetsu. 1994. Tokyo, Japan: Meisei Publications.
Miller, Richard L., Earl S. Swensson, and J. Todd Rob-inson. 2012. Hospital and healthcare facility design. New York: W.W Norton & Co.
Nickl-Weller, Christine, and Hans Nickl. 2013. Hospital architecture. [Salenstein, Switzerland]: Braun.
Porter, David R. 1982. Hospital architecture: guide-lines for design and renovation. Ann Arbor, Mich: AU-PHA Press.
Porterfield, Amanda. 2005. Healing in the history of Christianity. Oxford: Oxford University Press.
Rashid, Rushdi, and Regis Morelon. 1996. Encyclo-pedia of the history of Arabic science. London: Rout-ledge.
Risse, Guenter B. 1999. Mending bodies, saving souls: a history of hospitals. New York: Oxford Univer-sity Press.
Redstone, Louis G. 1978. Hospitals and health care facilities. New York: McGraw-Hill.
Scheutz, Martin. 2008. Europaisches Spitalwesen: in-stitutionelle Fürsorge in Mittelalter und früher Neuzeit = Hospitals and institutional care in medieval and early modern Europe. Wien: R. Oldenbourg Verlag.
Stavrianos, Leften Stavros. 1982. The world since 1500: a global history. Englewood Cliffs, N.J.: Pren-tice-Hall.
Stavrianos, Leften Stavros. 1982. The world to 1500: a global history. Englewood Cliffs, N.J.: Prentice-Hall.
Terry, Neville. 1994. The Royal Vic: the story of Mon-treal’s Royal Victoria Hospital, 1894-1994. Montreal, Quebec: McGill-Queen’s University Press.
Thompson, John D., and Grace Goldin. 1975. The hospital: a social and architectural history. New Ha-ven: Yale University Press.
Wall, Barbra Mann. 2011. American Catholic hospi-tals: a century of changing markets and missions. New Brunswick, N.J.: Rutgers Univ. Press.
Winkel, Steven R., David S. Collins, and Steven P. Ju-roszek. 2007. Building codes illustrated for healthcare facilities: a guide to understanding the 2006 Interna-tional building code for healthcare facilities. Hoboken, N.J.: Wiley.
2015 MASTER’S RESEARCH PROJECT 140

32CreditsList of Illustrations
All reasonable efforts to secure permissions for the visual material reproduced herein have been made by the author of each page. The author apologize to anyone who has not been informed.
The notations indicate the page of where the image is located. This list is sorted according to the pages in this book.
Manifesto9: Asklepieion at Epidauros. From Leon’s Massage Board. https://bleon1.wordpress.com/.
11: Vercovicium. From HISTORIA PARA NO DORMIR. http://historiaparano-dormiranhell.blogspot.com/2014/06/122-dc-el-muro-de-adriano-2-parte.html.
13: Interior of the Hotel-Dieu of St. Jean in Angers in the nineteenth century. From A Verdier and F. Cattois, Architecture civile et domestique, Paris: Librai-rie archeologique de Vor Didron, 1857, 2: 101.
15: Johannes Beerblock’s oil painting View of the Sick Ward of St. John’s Hospital (Bruges), 1778. Reproduced with the joint permission of the Insrirur Royal du Parrimoine Arrisrique, Brussels, and Commissie van Openbare Ondersrand, Bruges.
17: Interior of a hospital tent before Petersburg Field Hospital, sketch by A. McCullum. From the Healy Collection, Library, the New York Academy of Medicine.
19: The Prince and Princess of Wales visiting a small patient in the Evelina Hospital, 1891. Published in The Illustrated Paper, 28 November 1891. From The Wellcome Library.
20: Operation Room Scene at the Philadelphia General Hospital, 1925. From Penn Nursing Science, University of Pennsylvania School of Nursing.
21: “In an underground surgery room, behind the front lines on Bougainville, an American Army doctor operates on a U.S. soldier wounded by a Japanese sniper.” December 13, 1943. 111-SC-187247. From National Archives, Pic-tures of World War II.
22: Behind the Scenes at Ellis Hospital, 1955. From Ellis Hospital Collection.
23: Chernobyl power plant in pictures: 25 years since the world’s worst nucle-ar accident. From the Anorack, http://www.anorak.co.uk/.
24: Hospital Lobby and Triage. From International Emergency Medicine Elec-tive, http://www.utoledo.edu/med/gme/em/International%20Global%20Emer-gency%20Medicine%20Elective.html.
25: A hospital view after a powerful earthquake hit Japan on 11 March 2011. From Japanese Red Cross, EPA/Toshiharu Kato, http://www.vosizneias.com/78398/2011/03/13/tokyo-japan-earthquake-2011-devastating-photos-of-the-wreckage/.
26: Kaleida Health, Clinical and Medical Research Building. From Canon De-sign.
Foreground27: The Anatomy Lesson of Dr. Nicolaes Tulp. From Mauritshuis (Hague, Netherlands).
28: J.C. Woudanus based on a drawing by W. Swanenburg: Anatomical The-ater. From Wikipedia Norwegian, http://en.wikipedia.org/wiki/Norwegian.
28: Sanatorium Zonnestraal , Hilversum. From Artstor Digital Collections.
Evolution30: Fa Hien at the ruins of Ashoka palace. From Hutchinson’s story of the nations, London.
30: Travels of Faxian (Record of the Buddhist Countries). From Faxian zhuan.
31: One of the wards of the hospital at Scutari. From Library of Congress.
32: Diller Scofidio + Renfro Unveils New Columbia University Medical Building . From Columbia University Medical Center (CUMC)
Scope41: Meeting of thousands of people. From FreeStockPhotos, http://www.free-stockphotos.name/wallpaper/130/meeting-of-thousands-of-people-images-photography.html.
42: Hospital Bed Density (Hospital beds per 1,000 people). From The World Bank.
44: View in an Operation Theater. From John Hopkins Hospital.
44: Flag of Turkey. From Turkish Historical Society, Turkish Flag Law (Türk Bayrağı Kanunu), Law nr. 2893 of 22 September 1983.
Crisis45: Typical EUI values. From ENERGY STAR (a U.S. Environmental Protec-tion Agency).
46: Range of Source EUI. From ENERGY STAR (a U.S. Environmental Pro-tection Agency).
Temple49: Kos and the Ancient Asklepieion. From Bike Classical, bikeclassical.blogspot.com/2013/09/kos-and-ancient-asklepieion.html.
49: Temple of Asclepios. From Earl S. Swensson.
50: Hall for dreamer-patients, Asklepieion of Epidauros, fifth century B.C. From Alfonse Defrasse and Henri Lechat, Epidaure. Paris: May and Motteroz, 1895, p. 131.
Sanctuary51: Elevations and bird’s eye view of Cluny monastery about 115 7, as re-stored by Kenneth J. Conant. Courtesy Medieval Academy of America. Pho-tos Ufford and Nedzweski.
52: Ground plan of Cluny monastery about 115 7, as restored by Kenneth J. Conant. Courtesy Medieval Academy of America. Photo Ufford and Nedz-weski.
Ward53: St. Thomas’s Hospital, London, engraving by William H~nry Toms (171 7-1 750). From the Library of the Wellcome Instirute for the History of Med!Cme, London, by courtesy of the Wellcome Trustees.
54: Elevation and plan of St. Thomas’s Hospital. From Westminster Bridge - WHERE THAMES SMOOTH WATERS GLIDE, http://thames.me.uk/s00130.htm.
54: View of St Thomas’s Hospital, Parliament, Westminster Bridge to right. From Britain from Above, http://www.britainfromabove.org.uk/.
Pavilion55: The Hotel-Dieu of Paris on the Turgot plan, 1739. From C. Toilet, Les edifices hospitaliers, fig. 66.
55: Plan of the Hotel-Dieu of Paris by Poyer, end of eighteenth century. From C. Toilet, Les edifices hospitaliers depuis leur origine jusqu’a nos jours, Paris, 1892, fig. 233.
55: Plan of bed areas at the Hotel-Dieu of Paris before the fire of 1772. From C. Toilet, Les edifices hospitaliers, fig. 71.
141 H21

56: Firemen to the rescue during the Hotel-Dieu fire of 1772. From Maurice Dogny, Histoire de l’Hopital Saint-Louis, Paris, ].-B. Bailliere, 1911, fig. 15.
56: Rebuilding the Hotel-Dieu of Paris. From Raymond Escholier, Les vieux hopitaux franfais: Hotel-Dieu, Lyons: Ciba, 1938, p. 25.
56: Plan of the wards of Poyer’s circular hospital project. From Toilet, Les edifices hospitaliers, fig. 23 5.
Skyscraper57: Final plan for Johns Hopkins Hospital (by Billings, 1876). From Ochsner and Sturm, The Organization . .. of Hospitals, p. 476.
57: Terrific Drawing of Johns Hopkins Hospital. From Ghosts of Baltimore.
58: Johns Hopkins Hospital interior. From Johns Hopkins Nursing, http://mag-azine.nursing.jhu.edu/2011/11/defining-moments-11/.
58: Longitudinal section, common ward, Johns Hopkins Hospital. From Bill-ings, Description, pl. 23.
58: Johns Hopkins Hospital night view. From (a) biotic design studio.
Modernism59: Main Entrance of Paimio Sanatorium. From The Building Blurb, Mar 25 2012, https://thebuildingblurb.wordpress.com/2012/03/25/paimio-sanatori-um/.
60: Corridor near Main Laboratories. From The Building Blurb, Mar 25 2012, https://thebuildingblurb.wordpress.com/2012/03/25/paimio-sanatorium/.
60: Top Garden for Rehabilitation. From The Building Blurb, Mar 25 2012, https://thebuildingblurb.wordpress.com/2012/03/25/paimio-sanatorium/.
Complexity61: Plan of a medical floor, Beaujon Hospital. From Louis Mourier and Albert Chenevier, Le Nouvel Hopital Beaujon de Paris, Administration Generale de l’Assistance Publique a Paris, 1935, courtesy M. Candille, director.
61: Elevation, Beaujon Hospital, Clichy, France (1935). From Pierre Vallery-Radot, Nos hopitaux Parisiens, un siecle d’histoire hospitaliere de Louis-Philippe jusqu’a nos jours (1837-1949), Paris: Editions Paul Dupont, 1948, p. 17 5.
62: Longitudinal section of the services and facade of a ward bay, Beaujon Hospital. From Mourier and Chenevier, Le Nouvel Hopital Beaujon de Paris, Administration Generale de l’Assistance Publique a Paris, courtesy M. Can-dille, director.
Mobility63: US Mercy Photos. From DEPARTMENT OF THE NAVY—AVAL HISTORY AND HERITAGE COMMAND.
Efficiency65: Ward plan, Memorial Unit, Yale-New Haven Hospital. From Yale-New Ha-ven Hospital.
66: West wing of New Haven Hospital. From Yale-New Haven Hospital.
66: Memorial Unit, Yale-New Haven Hospital, 1974. Photo by Stuart Langer;courtesy Yale-New Haven Hospital.
Sustainability67: All Photos and diagrams of Lunder Building, Massachusetts General Hos-pital. From NBBJ, A Fitting Opportunity, http://www.nbbj.com/work/massachu-setts-general-hospital-lunder-building/.
Reality
77: The cover of the The Innovator’s Prescription: A Disruptive Solution for Health Care. From Amazon.com, http://www.amazon.com/The-Innovators-Prescription-Disruptive-Solution/dp/0071592083.
Process88: Bird’s view of UF Health Shands Hospital. From UF Health Podcasts.
Strategem134: Acute-Care Center of the Future. From Earl Swensson Associates, Inc..
135: Synergenial Continuing Care Retirement Community (CCRC) Complex. From Earl Swensson Associates, Inc..
2015 MASTER’S RESEARCH PROJECT 142

Dominic Feng
Master of Architecture candidateUniversity of Florida, Gainesville, Florida, USAE-mail: [email protected]: (+1)352-665-1117
Thanks for Reviewing.

















