They Did What on the Same Day? The Hematology Laboratory at The Johns Hopkins Hospital, Baltimore went live with a new LIS, new hematology analyzers and a new hematology middleware. The Johns Hopkins Hospital’s Hematology Laboratory has been auto-validating results for the last 15 years, achieving an auto-validation rate of ~90% on the 1600 to 1900 CBCs they run per day, including the samples from pediatrics and oncology. When they recently decided to move from a homegrown to a vendor-based LIS system, they realized that they would need a middleware program to handle hematology’s 140+ rules. The challenge for many clinical labs around the country is to put custom hematology rules into LIS software, because most LIS platforms cannot handle the number of rules and triggers required by hematology labs. But this needn’t be a deterrent for implementing hematology auto-validation if one uses a middleware specifically designed for this purpose. Sysmex’s WAM™ program is such a system.
The implementation of two new software systems simultaneously (WAM and LIS) at the Johns Hopkins Hematology Laboratory was successful and a key contributor to the success was constant communication between the lab’s team and the Sysmex implementation team. Sysmex assigns a dedicated project manager who keeps track of all the details, so lab teams don’t have to worry about things getting lost in the shuffle.
President’s Message “Sysmex XN-3000, this is East Liverpool City Hospital, you are cleared to land.”
Let’s talk about customer service. There’s a famous story from back in the day of a diagnostics rep that learned a client needed a mononucleosis kit. So, he hired a small plane and flew the kit to a remote location in the Northwest. It must have been an interesting discussion about delivering solutions to customer needs with his District Manager after that one.
We all know stories about how medical technologists have done some extraordinary things for their patients. I’d like to tell you a more recent story about what Sysmex was able to do to get a new Sysmex XN-3000 Automated Hematology Analyzer in place for a client. At Liverpool East City Hospital in Ohio, the hospital doorways and elevators are too small for lab analyzers to get through. So, the delivery of the XN-3000 to the City of East Liverpool in Ohio was made by air through a roof-top trap door. But the opening for this maneuver had about the same spare room as a typical passenger has on a regional jet. It took only an hour after three crane lifts. We have some photos on page 4.
These stories remind me of a famous and favorite quote of Henry Ford. “A manufacturer is not through with his customer when the sale is completed. He has then only started with his customer.”
All of these stories have a common theme: Customer Service. I believe Sysmex is able to deliver not only unique products themselves, but the customized service and technical support needed for quality results and improved efficiency.
I also think we listen to the client better than any diagnostics company in the market. In fact, the entire XN product line was created based on client input and the feedback from the market has been overwhelmingly positive thus far.
In the course of our work, we also found ways to systemize the laboratory’s sample handling of EDTA tubes by designing high throughput automation solutions that can automate virtually all laboratory tests that require an EDTA sample. This has led to the integration of instruments that can handle slide making/staining, tube sorting
(continued on page 2) (continued on page 2)
Johns Hopkins Hospital, located in Baltimore, Maryland.
2
and archiving and even HbA1c requests right on the hematology line. This is another solution that we have been able to deliver.
To me this confirms that keeping our focus on you, the client, is the only way to conduct our business. Therefore, we will continue to listen to the clinical laboratory professionals who deliver hundreds of thousands of diagnostic tests daily to our nation’s physicians. This approach enables us to anticipate change, respond with agility, and most importantly, to deliver. Not all manufacturers can say this.
So we thank you, our clients, who have inspired our innovation and enabled us to deliver revolutionary, best-in-class product offerings. This is evidenced by external recognition, such as our Company’s recent Confirmit Ace Award, which recognized our excellence in using client feedback to improve business results. It’s evidenced by our company’s president in Kobe, Japan who arranged his business trip to North America to coincide with a client’s ribbon cutting ceremony to celebrate the go live of their new Sysmex HST automated hematology solution.
In a recent meeting of industry business leaders, I listened for three days as they discussed profitability, return on assets and investments, metrics, segmentation and market share. Certainly, these are important. But noticeable by their absence was any mention of their clients and their clients’ needs or how their companies would meet these needs.
That’s how Sysmex is different.
I am reminded of another comment that Henry Ford once made, “It is not the employer who pays (my) wages—he only handles the money. It is the product and customer who pay the wages.” This philosophy is our philosophy.
Sincerely,
John Kershaw President & CEO Sysmex America, Inc.
This communication extended to include cooperation between Sysmex and the LIS vendor, who would get on the phone together for problem solving sessions. Sysmex considers this a key factor to going live with two new software programs at the same time and finishing the implementation in just eight weeks.
As an additional aid to laboratories, Sysmex’s implementation program provides comprehensive guidelines to labs around the country. Sysmex documentation provides labs and IS departments what needs to be tested and how the testing should be done. Sysmex will work with the lab at every step, instead of leaving the technologists and IS departments to figure it out on their own. When a question concerning the new LIS system arose, Sysmex got on the phone with the LIS vendor to discuss what needed to be done so the go live was smooth. Participating in WAM training and understanding how WAM works can help with brainstorming and bringing some creativity to the problem solving process. Being able to talk things through with the Sysmex staff on site and being able to access other people at Sysmex helped the lab and IS teams identify where they needed to make changes.
Checklist for SuccessBased on experience, the Sysmex implementation team recommends the following for laboratories that intend to implement auto-validation with middleware:
Constant communication with the vendor. Sysmex provides a dedicated Project Manager and a Technical Integration Specialist who are on site much of the time and who get hands-on for some of the data-heavy work. “Sysmex can help because they understand the LIS portion of the project as well as WAM,” said Tracey Kelvington, Sr. Project Manager, Sysmex America. “We will sit down with you for a lot of the labor-intensive work that includes wet and dry rule testing.”
Enough people assigned to the project. If there isn’t enough staff assigned to the project, it will fail. Sysmex was fortunate to have four staff members, including a supervisor, on the internal team. The key is to have enough people on the team so that they can focus on the project until completion and the project will progress more quickly.
(continued from page 1)
2
Tracey Kelvington Sr. Product Manager,
Sysmex America
(continued from page 1)
3
People with the ability to think out of the box. Sysmex believes you will need to come up with new ways to create rules if the old way does not work. You don’t have to be an IT person to understand how the system works. Together the lab team and Sysmex can figure out a way to make WAM do what is needed. Identify a person who can think that way about rules and you will avoid getting stuck.
Make sure the lab director is onboard. If the team presents a way to do something that is different than what was done in the past, show how it will work, and ask for management approval.
Get staff buy-in. This is especially true if the laboratory hasn’t auto-validated before. Make sure the hematology staff are always informed about what is going on with the project and is involved throughout the process.
Don’t implement old rules. Think through the clinical needs for rules as well as the workflow needs. For example, a low platelet delta check rule might need to be different than a normal platelet delta check. Challenge the need for using old rules from 20 years ago e.g., doctors wanting to see a diff on any WBC below 2,000. Is that rule still needed given your patient population and your analyzer performance? If you don’t change your mindset about auto-validation, your review rate is going to reflect this.
Choose a Middleware Designed for HematologyFor laboratories looking toward new hematology middleware, the following can provide a quick start:
1. Have a clear understanding of the software’s capabilities.
2. Understand your workflow in detail.
3. Understand what you, your management and your clinicians want to accomplish with the middleware.
4. If you have never done auto-validation, seek out colleagues in other hospitals and ask how they do it.
5. Understand your rules and have confidence in them.
SummaryMoving to auto-validation can be uncomfortable at first, according to Kelvington. Technologists are used to seeing results before they leave the lab and reporting out results without a human eye on them can cause anxiety. One way successful teams look at auto-validation is that the lab staff is going to be looking at the patient samples that really need their attention. This can improve turnaround time and the quality of the work the lab is reporting. This translates into a less stressful environment, better managed workloads and more staff confidence. Once done, both the laboratory staff and patients benefit.
The XP-300 is built on the same award-winning design concept utilized in the company’s new Sysmex XN-Series™ – Silent Design®. Silent Design is a human-centered approach that simplifies analyzer operation and the user interface based on careful study of laboratory processes, the relationship between the operator and the analyzer, and how people work.
4
As a Sysmex Network Communications Systems (SNCS) compatible hematology analyzer, labs with the new XP-300 can participate in the Sysmex Insight™ Quality Control Program. Insight is Sysmex’s web-based inter-laboratory quality assessment program designed to facilitate evaluation of hematology analyzer performance. Insight eliminates manual steps and meets lab requirements to document, review and maintain history for peer comparison analyzer data by uploading quality control data. This enables the laboratory to review streamlined and comprehensive reports with statistical and graphical presentation of analyzer performance anytime from anywhere.
XP-300 customers also will benefit from implementation support, on-site training and access to the Sysmex Customer Resource Center. Although the marketing and sales activity of the KX-21N will cease in June, Sysmex America will continue to provide service and support.
For more information about the new Sysmex XP-300 Automated Hematology Analyzer, contact your local sales representative or the Sysmex Website at www.sysmex.com/us.
New Sysmex XP-300™: A Big Update for Smaller Labs
Retirement Planned for the KX-21N™ Two Sysmex analyzers, the KX-21N™ and the pocH-100i™, have served small hospitals, clinics and office-based laboratories well. Now, Sysmex has taken the user friendly software of the pocH-100i and combined it with a modified version of the reliable KX-21N hardware to create a new analyzer, the XP-300™ Automated Hematology Analyzer.
According to Susan Behnke, Product Manager, Hematology, Sysmex America, the KX-21N is known for its outstanding reliability and simple operation, and the pocH-100i, which will continue to be available, is known for its intuitive software and very small footprint. “Now Sysmex has combined the best attributes of the two analyzers with the convenience of a color touch panel for ease-of-use operation and standard barcode capability,” said Behnke.
The XP-300 is scheduled to launch in June. It offers a CBC with a three-part differential [%/# LYM, MXD (monos, eos, basos) and Neutrophil]. This differential, like the X-Series and XN-Series analyzers, gives an Absolute Neutrophil Count (ANC). The maximum throughput is 60 samples per hour with a data storage capacity up to 40,000 complete sample results with histograms. “One of the most time-saving features of the XP-300 is barcode scanning, which allows for the digital input of 51 quality control TARGET and LIMIT parameters. Previously, these had to be manually keyed into the KX-21N system,” she added.
Susan Behnke Product Manager,
Hematology, Sysmex America
“Sysmex XN-3000, this is East Liverpool Hospital. You are cleared to land.”The doorways were too small and so were the elevators. So, the delivery of the new XN-3000 Compact Automation System to the East Liverpool City Hospital in Ohio was made by air. For those that fly a good bit, it was like threading a 747 onto the flight deck of an aircraft carrier. Amazingly, it took only 1-1/2 hours and three “air” lifts from the time the delivery truck arrived until the system was in the laboratory.
As evidenced by this unusual installation, no challenge is too great for the dedicated implementation teams at Sysmex. Meeting each customer’s unique installation needs is our mission.
LiftoffAn XN-3000 wagon and a slide-maker stainer.
Level FlightXN-3000, you have traffic at 12 o’clock.
LandingGetting the new components to the lab required they fit through a trap door on the roof.
5
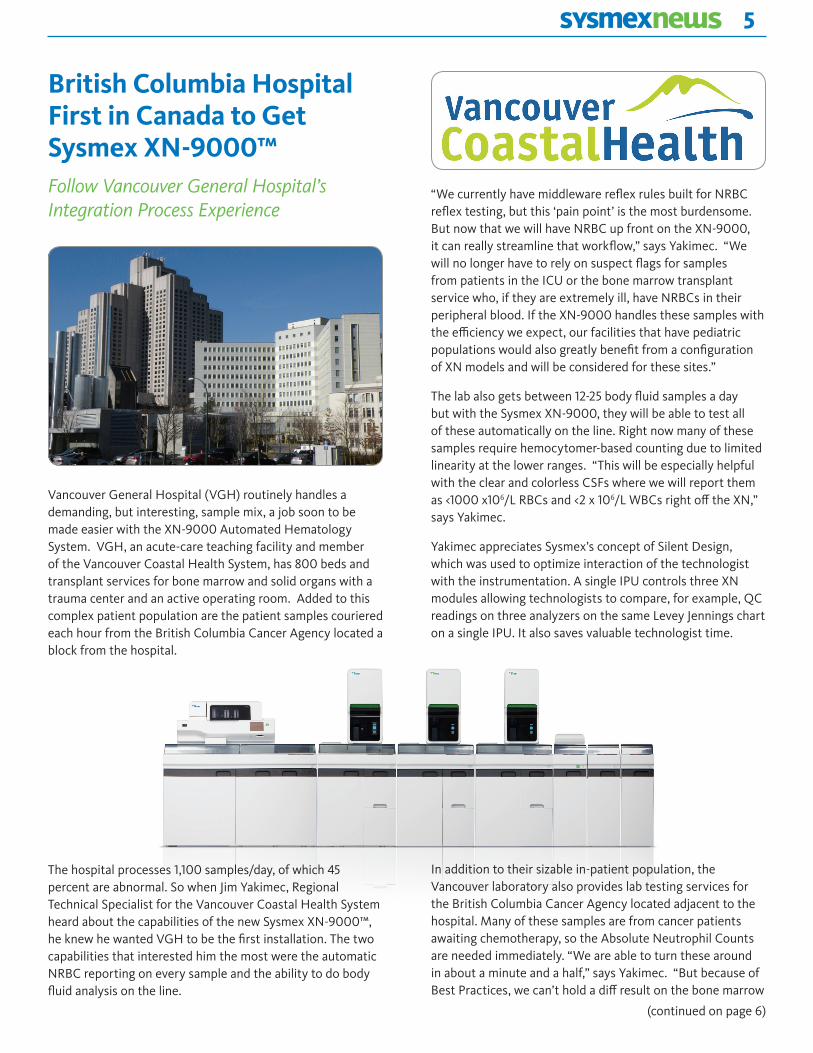
British Columbia Hospital First in Canada to Get Sysmex XN-9000™Follow Vancouver General Hospital’s Integration Process Experience
Vancouver General Hospital (VGH) routinely handles a demanding, but interesting, sample mix, a job soon to be made easier with the XN-9000 Automated Hematology System. VGH, an acute-care teaching facility and member of the Vancouver Coastal Health System, has 800 beds and transplant services for bone marrow and solid organs with a trauma center and an active operating room. Added to this complex patient population are the patient samples couriered each hour from the British Columbia Cancer Agency located a block from the hospital.
The hospital processes 1,100 samples/day, of which 45 percent are abnormal. So when Jim Yakimec, Regional Technical Specialist for the Vancouver Coastal Health System heard about the capabilities of the new Sysmex XN-9000™, he knew he wanted VGH to be the first installation. The two capabilities that interested him the most were the automatic NRBC reporting on every sample and the ability to do body fluid analysis on the line.
“We currently have middleware reflex rules built for NRBC reflex testing, but this ‘pain point’ is the most burdensome. But now that we will have NRBC up front on the XN-9000, it can really streamline that workflow,” says Yakimec. “We will no longer have to rely on suspect flags for samples from patients in the ICU or the bone marrow transplant service who, if they are extremely ill, have NRBCs in their peripheral blood. If the XN-9000 handles these samples with the efficiency we expect, our facilities that have pediatric populations would also greatly benefit from a configuration of XN models and will be considered for these sites.”
The lab also gets between 12-25 body fluid samples a day but with the Sysmex XN-9000, they will be able to test all of these automatically on the line. Right now many of these samples require hemocytomer-based counting due to limited linearity at the lower ranges. “This will be especially helpful with the clear and colorless CSFs where we will report them as <1000 x106/L RBCs and <2 x 106/L WBCs right off the XN,” says Yakimec.
Yakimec appreciates Sysmex’s concept of Silent Design, which was used to optimize interaction of the technologist with the instrumentation. A single IPU controls three XN modules allowing technologists to compare, for example, QC readings on three analyzers on the same Levey Jennings chart on a single IPU. It also saves valuable technologist time.
(continued on page 6)
In addition to their sizable in-patient population, the Vancouver laboratory also provides lab testing services for the British Columbia Cancer Agency located adjacent to the hospital. Many of these samples are from cancer patients awaiting chemotherapy, so the Absolute Neutrophil Counts are needed immediately. “We are able to turn these around in about a minute and a half,” says Yakimec. “But because of Best Practices, we can’t hold a diff result on the bone marrow
6
The new Sysmex XN-Series: an Equal Opportunity AnalyzerWhat if you never have to choose between hematology analyzers with different capabilities and different throughputs again? What if you could eliminate worries about your workload, your abnormal or complicated patient populations, body fluid samples, bench space, or level of automation?
The new XN-Series analyzers from Sysmex are equalizing hematology laboratories on a global scale. This is because Sysmex has developed the first truly universal hematology analytical module, the XN-10™, that provides every laboratory with CBC and differential, including analysis of immature cell forms from all three cell lines: WBC, RBC and Platelets. It even automates body fluid cell counts, including a 2-part differential, on serous, spinal and synovial fluids. The smallest in the series is the XN-1000 and comprises a single XN-10 module on a dedicated sampler. All XN-Series configurations have identical reagents, QC software and analytical capabilities, making the XN-Series a truly scalable series of analyzers.
The Sysmex XN-Series also heralds the end of the era when labs had dissimilar back-up analyzers, replacing it with the functionality of “co-primary” analyzers. This new approach allows laboratories to balance workloads across two identical
analyzers, the XN-2000™. With expanded reporting capability, on-board rules for reflex and re-run testing and the availability of advanced clinical parameters resident on each of the analytical modules of the XN-2000, specimens no longer need to be routed to one analyzer or another. Labs can also make dramatic improvements to turnaround times since reflex testing and re-runs are handled automatically by onboard rules. The total workload can now be accomplished in a compact space, quickly and easily.
or cancer services. So we have implemented a new test called a preliminary neutrophil count, which we can release with just that one parameter through the middleware.”
Yakimec is already impressed with his current differential review rate of 11 percent to 13 percent. “If our population were primarily normal samples, we would be able to reduce this substantially,” he says. The hospital has been using Sysmex’s Immature Granulocyte (IG) parameter since 2007 to reduce unnecessary slide reviews even with this challenging patient mix. “We would never consider an analyzer without this capability,” says Yakimec. VGH has been reporting Immature Reticulocyte Fraction (IRF) since February 2012, and are currently doing a study with the renal transplant unit on RET-He (hemoglobin content of reticulocytes).
The chain of events after the hospital’s XN-9000 acquisition unfolded at lightning speed post system delivery on March 18, 2013. Installation and two weeks of training were completed within weeks of acquisition. Currently, validation studies are underway. Yakimec even managed to squeeze in a Grand Rounds for the hospital’s residents and physicians to ensure they too were aware of the new technology and the benefits it will afford them in the diagnosis and treatment of their patients.
The subjects explored across two Ground Rounds presentations included: cell classification technology; platelet counting improvements leading to fewer repeats, extended linearity capabilities; the new NRBC capability shown with a DVT case study and review of conditions in which NRBCs may appear in the peripheral blood; the outcome implications for adults in the ICU showing NRBCs in peripheral blood; body fluids analysis.
Based on what has been accomplished to date, the staff at VGH expect a fast and sure go live.
Jim Yakimec, Technical Support, Hematology Laboratory, Vancouver Coastal Health, left, and Kin Cheng, recently retired, together worked with Sysmex Canada to bring the new Sysmex XN-9000 AutomatedHematology System to Vancouver General Hospital (VGH). VGH, a 800-bed acute-care teaching facility and member of the Vancouver Coastal Health System, is the first hospital to install the new XN-Series automated hematology system.
(continued from page 5)
7
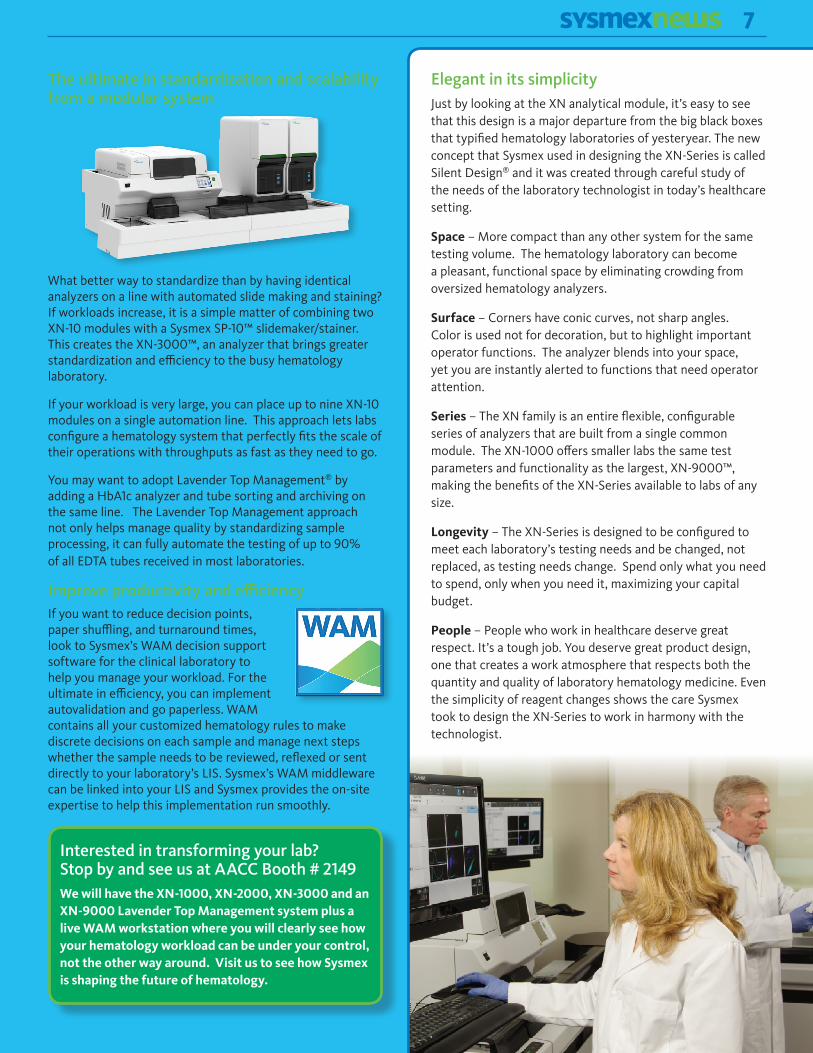
The ultimate in standardization and scalability from a modular system
What better way to standardize than by having identical analyzers on a line with automated slide making and staining? If workloads increase, it is a simple matter of combining two XN-10 modules with a Sysmex SP-10™ slidemaker/stainer. This creates the XN-3000™, an analyzer that brings greater standardization and efficiency to the busy hematology laboratory.
If your workload is very large, you can place up to nine XN-10 modules on a single automation line. This approach lets labs configure a hematology system that perfectly fits the scale of their operations with throughputs as fast as they need to go.
You may want to adopt Lavender Top Management® by adding a HbA1c analyzer and tube sorting and archiving on the same line. The Lavender Top Management approach not only helps manage quality by standardizing sample processing, it can fully automate the testing of up to 90% of all EDTA tubes received in most laboratories.
Improve productivity and efficiencyIf you want to reduce decision points, paper shuffling, and turnaround times, look to Sysmex’s WAM decision support software for the clinical laboratory to help you manage your workload. For the ultimate in efficiency, you can implement autovalidation and go paperless. WAM contains all your customized hematology rules to make discrete decisions on each sample and manage next steps whether the sample needs to be reviewed, reflexed or sent directly to your laboratory’s LIS. Sysmex’s WAM middleware can be linked into your LIS and Sysmex provides the on-site expertise to help this implementation run smoothly.
Elegant in its simplicityJust by looking at the XN analytical module, it’s easy to see that this design is a major departure from the big black boxes that typified hematology laboratories of yesteryear. The new concept that Sysmex used in designing the XN-Series is called Silent Design® and it was created through careful study of the needs of the laboratory technologist in today’s healthcare setting.
Space – More compact than any other system for the same testing volume. The hematology laboratory can become a pleasant, functional space by eliminating crowding from oversized hematology analyzers.
Surface – Corners have conic curves, not sharp angles. Color is used not for decoration, but to highlight important operator functions. The analyzer blends into your space, yet you are instantly alerted to functions that need operator attention.
Series – The XN family is an entire flexible, configurable series of analyzers that are built from a single common module. The XN-1000 offers smaller labs the same test parameters and functionality as the largest, XN-9000™, making the benefits of the XN-Series available to labs of any size.
Longevity – The XN-Series is designed to be configured to meet each laboratory’s testing needs and be changed, not replaced, as testing needs change. Spend only what you need to spend, only when you need it, maximizing your capital budget.
People – People who work in healthcare deserve great respect. It’s a tough job. You deserve great product design, one that creates a work atmosphere that respects both the quantity and quality of laboratory hematology medicine. Even the simplicity of reagent changes shows the care Sysmex took to design the XN-Series to work in harmony with the technologist.
Interested in transforming your lab? Stop by and see us at AACC Booth # 2149We will have the XN-1000, XN-2000, XN-3000 and an XN-9000 Lavender Top Management system plus a live WAM workstation where you will clearly see how your hematology workload can be under your control, not the other way around. Visit us to see how Sysmex is shaping the future of hematology.
8
Coming Soon: Sysmex leverages system data to optimize maintenance and improve laboratory productivity
Evidence-Based Maintenance Principles to Drive Reliability DecisionsAt Sysmex, we are constantly looking at ways to improve the amount of time an analyzer is ready for patient testing so our laboratory customers can focus on what’s most important…high quality patient care.
With that in mind, Sysmex is replacing our traditional maintenance program with a new Service Maintenance Program. This new program uses evidence-based principles instead of the standard post-call checklist. Using analyzer evidence improves reliability decisions and maximizes productivity of the lab.
With our support technology and a connection to Sysmex Network Communications System (SNCS™), the new service program applies evidence-based principles to perform critical maintenance functions that are regulatory-required, facilitate quality results and represent excellent laboratory practice for all Sysmex customers.
Using a proprietary Evidence-Based Maintenance (EBM) analytics tool, Sysmex evaluates key pieces of data to guide our trained Field Service Representatives (FSRs) to customize maintenance decisions for every analyzer. The data include visual inspection, time since the last service visit, analyzer alarms, Quality Control trending, historical databases such as Insight™ and part replacement histories, cycle counts, and predictive rules.
Evidence-based principles are widely used in the medical community. This new process is unique to Sysmex. It is significantly different compared to other service providers in that Sysmex is looking for “evidence” of the need for maintenance and uses extensive analytics in determining required maintenance activities. The EBM tool assures consistency and documentation of the maintenance activities performed.
Evidence-based maintenance activities are performed during every scheduled and unscheduled service visits by a FSR. The maintenance portion takes approximately 10 to 20 minutes, and some of this time is offset by replacing the post-call checklist.
Upon completion of the Service Maintenance activities, customers receive a comprehensive Certificate of Completion that can be used for reporting to accrediting agencies. The certificate lists the maintenance activities completed by the FSR and the resulting verification of analyzer performance.
These service maintenance enhancements reduce non-productive analyzer time. They do not require Sysmex customers to change operating procedures, and all required maintenance is completed annually as specified in the service contract. This program is included with no additional fees for analyzers that are SNCS connected with an active service contract. Without an SNCS connection, FSRs simply use the traditional maintenance checklist.
Sysmex makes the most reliable hematology analyzers*. We use technology to keep them ready to perform.
*According IMV Service Trak™ 2012.
FOR EVALUATION PURPOSES ONLYSysmex Service Maintenance Certificate
Analyzer Verification Status:Analyzed all levels of the customer's QC. All parameters of all levels were within manufacturer's assay range and within the customer's established range. Instrument was also returned to normal operating mode.
FSR Comments: Cleaned drain filters for WBC reaction unit and RBC reaction chamber
Component SubComponent Action FSR Notes
RBC Unit Filter CLEANEDReaction Unit Filter CLEANEDReaction Unit Reaction Unit assy CLEANEDReagent Chambers Trap chamber CLEANEDReagent Chambers Tubing CLEANEDSampler Unit Internal Barcode Reader CLEANEDSampler Unit Sampler Unit Assy CLEANEDSheath Syringe Unit Sheath Syringe Unit Assy CLEANEDSheath Syringe Unit Worm gear LUBRICATEDWaste Chambers Chamber CLEANEDWhole Blood Syringe Unit Motor CLEANEDWhole Blood Syringe Unit Syringe assy CLEANED
Page: 1 Generated: 4/9/2013 12:13:19 PM
Hospital
9
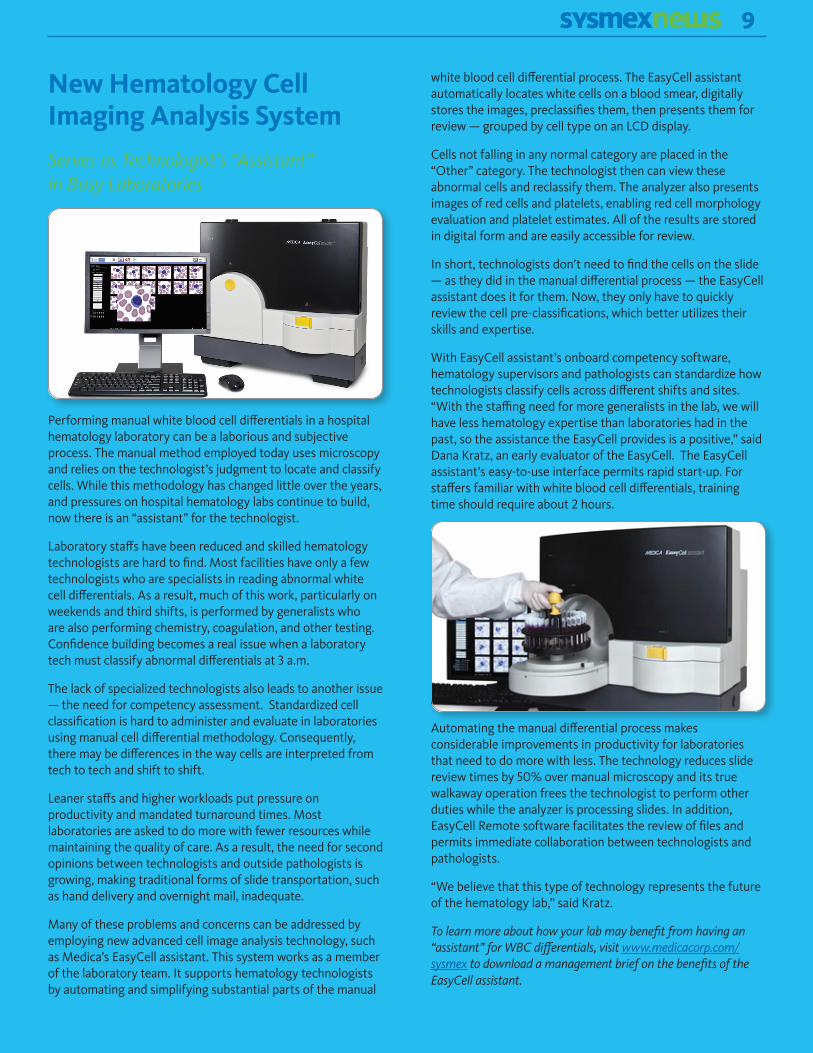
New Hematology Cell Imaging Analysis System
Serves as Technologist’s “Assistant” in Busy Laboratories
Performing manual white blood cell differentials in a hospital hematology laboratory can be a laborious and subjective process. The manual method employed today uses microscopy and relies on the technologist’s judgment to locate and classify cells. While this methodology has changed little over the years, and pressures on hospital hematology labs continue to build, now there is an “assistant” for the technologist.
Laboratory staffs have been reduced and skilled hematology technologists are hard to find. Most facilities have only a few technologists who are specialists in reading abnormal white cell differentials. As a result, much of this work, particularly on weekends and third shifts, is performed by generalists who are also performing chemistry, coagulation, and other testing. Confidence building becomes a real issue when a laboratory tech must classify abnormal differentials at 3 a.m.
The lack of specialized technologists also leads to another issue — the need for competency assessment. Standardized cell classification is hard to administer and evaluate in laboratories using manual cell differential methodology. Consequently, there may be differences in the way cells are interpreted from tech to tech and shift to shift.
Leaner staffs and higher workloads put pressure on productivity and mandated turnaround times. Most laboratories are asked to do more with fewer resources while maintaining the quality of care. As a result, the need for second opinions between technologists and outside pathologists is growing, making traditional forms of slide transportation, such as hand delivery and overnight mail, inadequate.
Many of these problems and concerns can be addressed by employing new advanced cell image analysis technology, such as Medica’s EasyCell assistant. This system works as a member of the laboratory team. It supports hematology technologists by automating and simplifying substantial parts of the manual
white blood cell differential process. The EasyCell assistant automatically locates white cells on a blood smear, digitally stores the images, preclassifies them, then presents them for review — grouped by cell type on an LCD display.
Cells not falling in any normal category are placed in the “Other” category. The technologist then can view these abnormal cells and reclassify them. The analyzer also presents images of red cells and platelets, enabling red cell morphology evaluation and platelet estimates. All of the results are stored in digital form and are easily accessible for review.
In short, technologists don’t need to find the cells on the slide — as they did in the manual differential process — the EasyCell assistant does it for them. Now, they only have to quickly review the cell pre-classifications, which better utilizes their skills and expertise.
With EasyCell assistant’s onboard competency software, hematology supervisors and pathologists can standardize how technologists classify cells across different shifts and sites. “With the staffing need for more generalists in the lab, we will have less hematology expertise than laboratories had in the past, so the assistance the EasyCell provides is a positive,” said Dana Kratz, an early evaluator of the EasyCell. The EasyCell assistant’s easy-to-use interface permits rapid start-up. For staffers familiar with white blood cell differentials, training time should require about 2 hours.
Automating the manual differential process makes considerable improvements in productivity for laboratories that need to do more with less. The technology reduces slide review times by 50% over manual microscopy and its true walkaway operation frees the technologist to perform other duties while the analyzer is processing slides. In addition, EasyCell Remote software facilitates the review of files and permits immediate collaboration between technologists and pathologists.
“We believe that this type of technology represents the future of the hematology lab,” said Kratz.
To learn more about how your lab may benefit from having an “assistant” for WBC differentials, visit www.medicacorp.com/sysmex to download a management brief on the benefits of the EasyCell assistant.
10
Qualifying Automated Urine Sediment Analysis for Clinical Use
Part two of a series on urinalysisComparing a new automated urinalysis method to a traditional manual method often poses unique challenges which can be overcome with a better understanding of the statistical tools used in urinalysis. Many new analyzers in the laboratory can be easily compared to previous methods because automated analyzers typically measure values in quantitative units and have low total error, which
facilitate a direct method comparison. However, when it comes to validating a new way to perform urinalysis, challenges arise that are not often encountered in other diagnostic fields. Examination of formed element method results and their sources of error is key to understanding the statistical challenges encountered to automating manual sediment analysis. A discussion of the statistical tools used in urinalysis method implementation, both strip chemistry and formed element analysis, can also shed light on this otherwise complex undertaking.
Traditional Manual Sediment AnalysisMany factors outside the control of the technologist can influence the accuracy of visual urine sediment analysis. The manual method traditionally requires review of 10 high-powered fields (hpf), the equivalent of 2 µl of unspun urine, which may or may not capture all clinically significant elements. The typical imprecision in the manual method at clinical decision levels can easily change a normal result to an abnormal result. For example, one slide may show 1-3 RBC/hpf, which is normal according to the American Urological Association’s best practice guidelines, while another slide prepared on the same sample may show 4-6 RBC/hpf, which is abnormal and may trigger follow-up by the clinician.
Many factors contribute to the total error inherent in manual sediment analysis. Counting cells in low concentrations results in high Coefficients of Variation (%CV), which increase mathematically when lower volumes of sample are examined; one microliter of analyzed sample is associated with 60% CVs, but when anayzing 10 µl, the %CV drops to 18%.
On cover-slipped samples, any or all of the following distribution errors may occur:
• Formed elements may settle on different focal planes.
• Elements may have a non-random distribution so some rare formed elements may not be observed.
• In abnormal samples with a high concentration of formed elements, the elements may adhere to one another, to mucous or migrate to the edges of the slide1.
The lack of stain can also impact the imprecision of visual methods. When stain is not used, it can be difficult to discriminate between look-alike cells, e.g., RBC vs. non-budding yeast. On the other hand, non-specific stains can color the background and may obscure some formed elements such as RBCs or ghost cells1.
Automated Sediment Analysis
Sysmex’s UF-1000i™ analyzes unspun urine, thereby eliminating the variables associated with centrifugation, re-suspension and decanting. The use of fluorescent flow technology with hydrodynamic focusing and selective cell lysing allows for better separation of cells to improve the classification and enumeration of formed elements. The UF is also able to analyze a significantly higher volume of each sample than can be done by visual methods, helping to
Leslie Williams MT (ASCP), Urinalysis
Product Manager, Sysmex America
11
(continued on page 12)
ensure highly accurate and precise results. The UF measures approximately 9 µl of sample and up to 80,000 particles can be analyzed and classified for every sample, reducing the risk of missing a rare but clinically significant formed element. Classification is further enhanced through the use of specific dyes and stains that highlight the RNA , the nucleus and other internal components of the cells.
ISLH Reference MethodTo resolve the discrepancies that are routinely uncovered when comparing manual and automated urine sediment methods, the scientific community developed a reference method that can be used by any clinical laboratory.
The ISLH reference method is recommended to evaluate urinalysis methods, including new automated methods, or to arbitrate discrepancies between methods. This is a hemocytometer- based quantitative method in which a measured amount of sample is used and elements are counted on a grid. A Fuchs Rosenthal chamber, with a 0.2 mm height, is used to allow even the larger formed elements to occupy the space between the slide and the coverslip. The chamber count has a lower total error because variables are controlled or eliminated; for example the method is performed on a sample that has not been centrifuged, re-suspended or decanted. This method is not used on a routine basis because it is very time consuming but does have the advantage of having no calibration or reagent bias and is considered a definitive comparison of non-equivalent methods or calibrated systems.
Interpreting Correlation Studies between Semi-quantitative and Quantitative MethodsInterpreting the correlation results between a semi-quantitative manual method and a numeric, automated urinalysis method can be daunting, as there are no “traditional” statistics such as correlation coefficient, Y-intercept, slope or bias to guide the reviewer. Instead, concordance charts are used. There are two types of charts used for this type of comparison.
Figure 1 shows a concordance chart, which is often used when comparing methods for formed element analysis. This chart compares a predicate (current) method, called the reference, against the test (new) method to be evaluated based on what the laboratory has determined to be the normal value for the parameter. The boxes in the chart display the concordance, or agreement between the methods, as well as the discordance, or disagreement. In the example in Figure 1, a total of 138 samples were tested by both methods.
Figure 1
Negative Reference (Normal)
Positive Reference (Abnormal)
Total
Negative Test (Normal
72 7 79
Positive Test (Abnormal)
31 28 59
Total 103 35 138 The reference method and the test method agreed on 72 normal samples; this is the negative concordance between the methods. The two methods also agreed on 28 abnormal samples; this is the positive concordance between the methods. However, there is also some discordance; the reference method produced an abnormal result for 7 samples, while the test method resulted normal. Likewise, the test method produced abnormal results for 31 samples, but the reference method was normal.
The discordant results require some attention, but what do they really mean? A review of the raw data for these discordant results may prove helpful, especially if the discordant results are borderline normal. There are two statistics that are used with this type of comparison, as shown in Figure 2 below, and while not as common as regression statistics they can provide some help when reviewing concordance data.
Figure 2
McNemar’s test for Symmetry
Test < Reference 7 (5.1%)
Test > Reference 31 (22.5%)
Symmetry test FAILS p < 0.001
Cohen’s Kappa 40.70%
The McNemar’s test for symmetry is a test for bias – does one method produce consistently higher results? Ideally, the discordant results should be equally distributed, but if the percentage of test < reference is higher or lower than the percentage of test > reference, the symmetry test fails. However, when trying to compare two different technologies or semi-qualitative methods, some asymmetry is to be expected. For example, the UF is often discordant with the manual sediment method because cell recovery is typically higher on the UF. This is due to the loss of cells when the sample is centrifuged and decanted, and so discordance is expected from the known differences in sample handling by the two methods.
12
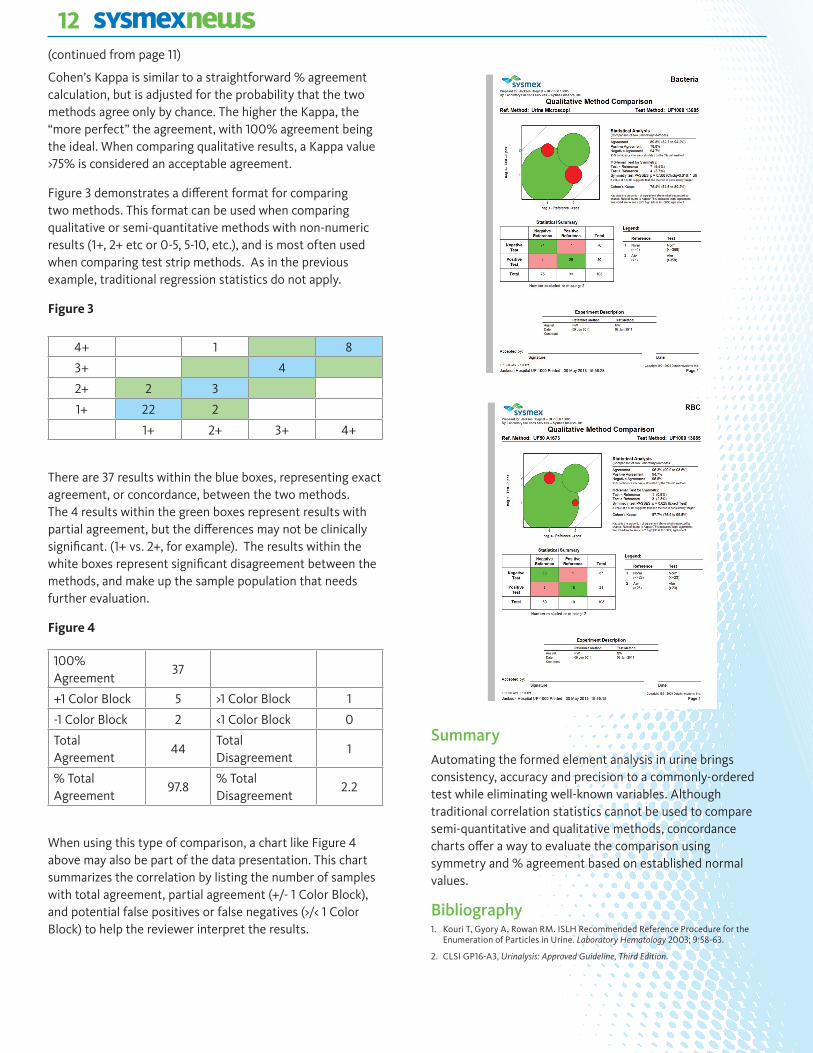
Cohen’s Kappa is similar to a straightforward % agreement calculation, but is adjusted for the probability that the two methods agree only by chance. The higher the Kappa, the “more perfect” the agreement, with 100% agreement being the ideal. When comparing qualitative results, a Kappa value >75% is considered an acceptable agreement.
Figure 3 demonstrates a different format for comparing two methods. This format can be used when comparing qualitative or semi-quantitative methods with non-numeric results (1+, 2+ etc or 0-5, 5-10, etc.), and is most often used when comparing test strip methods. As in the previous example, traditional regression statistics do not apply.
Figure 3
4+ 1 8
3+ 4
2+ 2 3
1+ 22 2
1+ 2+ 3+ 4+
There are 37 results within the blue boxes, representing exact agreement, or concordance, between the two methods. The 4 results within the green boxes represent results with partial agreement, but the differences may not be clinically significant. (1+ vs. 2+, for example). The results within the white boxes represent significant disagreement between the methods, and make up the sample population that needs further evaluation.
Figure 4
100% Agreement
37
+1 Color Block 5 >1 Color Block 1
-1 Color Block 2 <1 Color Block 0
Total Agreement
44Total Disagreement
1
% Total Agreement
97.8% Total Disagreement
2.2
When using this type of comparison, a chart like Figure 4 above may also be part of the data presentation. This chart summarizes the correlation by listing the number of samples with total agreement, partial agreement (+/- 1 Color Block), and potential false positives or false negatives (>/< 1 Color Block) to help the reviewer interpret the results.
SummaryAutomating the formed element analysis in urine brings consistency, accuracy and precision to a commonly-ordered test while eliminating well-known variables. Although traditional correlation statistics cannot be used to compare semi-quantitative and qualitative methods, concordance charts offer a way to evaluate the comparison using symmetry and % agreement based on established normal values.
Bibliography1. Kouri T, Gyory A, Rowan RM. ISLH Recommended Reference Procedure for the
Enumeration of Particles in Urine. Laboratory Hematology 2003; 9:58-63.
2. CLSI GP16-A3, Urinalysis: Approved Guideline, Third Edition.
(continued from page 11)
13
Alan D. Michelson MD, Professor of Pediatrics and Professor of Medicine, Harvard Medical School, Director, Center for Platelet Research Studies, Boston Children’s Hospital/Dana-Farber Cancer Institute, Boston, MA, discussed “The Clinical Utility of the Immature Platelet Fraction.” This session explored the use of the Immature Platelet Fraction (IPF) to assess the thrombocytopenia of immune thrombocytopenia vs. acute leukemia. The response of IPF to thrombopoietin mimetics was discussed, as well as the application of IPF in research studies of acute coronary syndromes and dopidogrel therapy.
Frelinger AL, III, Barnard MR, Fox ML, Michelson AD. The Platelet Activity After Clopidogrel Termination (PACT) study. Circ Cardiovasc Interv 2010 Oct;3(5):442-9.
Alan D. Michelson, MD Professor of Pediatrics
and Professor of Medicine, Harvard Medical School
Marjorie L. Zucker, MD, former Assoc. Professor of Pathology, Kansas University Medical Center, Kansas City, KS, provided a lecture on “Mechanism of Thrombocytopenia in Chronic Hepatitis C as Evaluated by the Immature Platelet Fraction.” This lecture explored the use of the immature platelet fraction (IPF) in the evaluation of thrombocytopenia by the physician and discussed the role of thrombopoietin levels in thrombocytopenia associated with Hepatitis C.
Zucker ML, Hagedorn CH, Murphy CA, Stanley S, Reid KJ, Skikne BS. Mechanism of thrombocytopenia in chronic hepatitis C as evaluated by the immature platelet fraction. Int J Lab Hematol 2012 Oct;34(5):525-32.
Marjorie L. Zucker, MD Former Assoc. Professor
of Pathology, Kansas University Medical Center
The ISLH is a must-attend event on the calendar for hematology laboratorians. Founded in 1992 by an international group of laboratory professionals in order to chart new directions for laboratory hematology, the group now has over 800 members in over 50 countries and conducts annual scientific meetings in the US, Europe and Asia. The ISLH has been instrumental in standards and guidelines development in laboratory hematology and has also expanded its repertoire of disciplines to cater for the growing needs of laboratory hematologists.
Michael H. A. Roehrl, MD Director, UHN Program in
BioSpecimen Sciences
A presentation by Michael H. A. Roehrl, MD, PhD, Associate Professor, University of Toronto, Director, UHN Program in BioSpecimen Sciences, Toronto, Canada, focused on “The Sysmex Immature Granulocyte Marker: Reference Ranges and Clinical Use in Outpatient Settings.” This lecture explored how precise normal outpatient IG reference ranges are established, which is a prerequisite for clinically meaningful interpretation of the parameter.
Roehrl MH, Lantz D, Sylvester C, Wang JY. Age-dependent reference ranges for automated assessment of immature granulocytes and clinical significance in an outpatient setting. Arch Pathol Lab Med 2011 Apr;135(4):471-7.
(continued on page 14)
Sysmex-At-A-GlanceSysmex America
Immature Cell Indices in the Spotlight at 2013 ISLH Sysmex Scientific WorkshopSysmex marked its presence at the ISLH 2013, the XXVIth International Symposium on Technological Innovations in Laboratory Hematology in Toronto, Canada with a Sysmex-sponsored Scientific Workshop focused on immature cell indices featuring internationally renowned physicians in the field. This year’s event put the spotlight on the clinical utility of two immature cell indices. The automated Immature Granulocyte count and the Immature Platelet Fraction. These are becoming increasingly important and can provide useful information about the pathophysiologic mechanism of hematopoiesis to the clinician to help guide and justify treatment decisions.
14
“Dog’s Best Friend” – Best-in-Class Hematology Analyzers
Did you know that Sysmex provides state-of-the-art hematology testing for our beloved pets? Like humans, our pets sometime require blood tests that enable their veterinarians to better diagnose and provide treatment options.
The Sysmex XT-2000iV™ Automated Hematology Analyzer is specifically designed for animal diagnostics and offers the same reliability and accuracy for which
the Sysmex brand is known. It uses the same state-of-the-art fluorescent flow cytometry technology and advanced cell-counting methods used in Sysmex hematology analyzers for human testing, according to Elizabeth Wiet, Scientific and Medical Affairs Manager, Sysmex America.
Now the Sysmex XT-2000iV is available to all animal diagnostic markets through a new Sysmex three-year distribution agreement with IDEXX Laboratories. Sysmex, in turn, is responsible for installation, customer training, technical service and ongoing customer support for the product at the customer site. IDEXX is responsible for veterinary application support to the customer. The XT-2000iV and IDEXX’s Sysmex-manufactured IDEXX ProCyte Dx® Hematology Analyzer enables veterinarians nationwide to provide advanced medical care while improving staff efficiency.
IDEXX Laboratories, Inc. is a leader in pet healthcare innovation, serving practicing veterinarians around the world with a broad range of diagnostic and information technology-based products and services.
(Sysmex-At-A-Glance continued from page 13)
Sysmex America, Inc. has been awarded 3 new contracts from Premier in the categories of hematology (both Premier and Ascend) and urinalysis. The effective date of all contracts is August 1, 2013 - July 31, 2016. Premier announced the contract awards to their membership on May 6. This is Sysmex’s 6th consecutive hematology contract with Premier and the 2nd Ascend and Urinalysis contracts. Sysmex has been awarded the Premier Pinnacle Award for supplier quality for 6 years.
Sysmex America Earns ISO-RecertificationSysmex America in Lincolnshire, IL and Sysmex Reagents America have successfully achieved recertification for our Environmental Management System as defined by ISO 14001.
Some of Sysmex’s environmental success stories that have contributed to this recertification include the following:
• The Virtual Training Studio has reduced CO2 by eliminating flights to and from Chicago and taxi / limo rides to and from the airport equating to 82,000 carbon units – this is in addition to minimizing the disruptions to our customers’ lab staff;
• Standard CELLPACK replacements with our concentrated CELLPACK C by our customers have eliminated an average of 12,288 kg of CO2 per year;
• The addition of our Reno, NV Distribution Center has reduced Greenhouse Gas / CO2 emissions associated with reagent distribution by 21.4% - this in addition to better serving our west coast customers.
The above efforts, coupled with Sysmex Corporation’s Global Eco-Vision 2020 Plan, have earned the Company’s 77th overall ranking among the top 100 Most Sustainable Companies in the World based on a Company’s performance metrics including environmental objectives.
To find out how your efforts are reducing Greenhouse gases / CO2 footprint, visit the U.S. Environmental Protection Agency calculator at http://www.epa.gov/cleanenergy/energy-resources/calculator.html#results.
To be eligible for a 2013 Confirmit ACE Award, Confirmit clients must have conducted one or more ongoing surveys to assess customer satisfaction, employee satisfaction, or partner satisfaction between October 1, 2011 and September 30, 2012. In addition, applicants must know that they achieve consistently high scores for customer satisfaction, among other eligibility requirements. Sysmex won awards in the Technical Assistance Center (TAC), Field Service and Customer Service categories.
15
Outstanding Achievement in Customer Excellence – ACE AwardThe Technical Assistance Center, Field Service and Customer Service at Sysmex America have been awarded the Confirmit ACE (Achievement in Customer Excellence) Award. This award recognizes Sysmex for demonstrating rigorous application of customer feedback management practices resulting in outstanding achievements in customer satisfaction. This is the second consecutive year Sysmex has received this prestigious accolade.
“Complete customer satisfaction is a top priority at Sysmex,” said Naomi Jones, Marketing Research Manager, Sysmex America. “We poll customers each week to consistently drive quality improvements and outstanding service. Our excellence in the application of these feedback processes is demonstrated by a close-to-perfect mean score within
each of three ongoing Sysmex Customer Service Excellence Surveys conducted last year, which has earned Sysmex this distinct honor.”
According to Pam Ballard, Director of Technical Customer Support, Sysmex America, “At Sysmex, we continually recognize our associates for being effective in addressing our customer’s needs. The processes we have in place allow us to act quickly on trend and service opportunities and change our internal process to consistently deliver a positive customer experience.”
(Sysmex-At-A-Glance continued on page 16))
Naomi Jones Marketing Research
Manager, Sysmex America
Pam Ballard Director of Technical Customer Support,
Sysmex America
16(Sysmex-At-A-Glance continued from page 15)
Sysmex America and Customers Earn 2013 Honor Roll Placement as Caring CompaniesIn March, the Center for Companies That Care announced its 2013 Honor Roll. It’s no surprise that a number of healthcare organizations, including some of Sysmex America’s customers, earned placement on this year’s national list for their outstanding workplace practices and active community involvement. It’s the fifth consecutive year that the Center has recognized Sysmex America for the same.
Many healthcare organizations are leaders in quality healthcare, social initiatives and community services. For example, healthcare companies were among the first to embrace diversity hiring and training initiatives, to provide support for working mothers, and to establish support groups and social media channels for patients and care provider benefit. Bottom line, healthcare organizations are committed to their employees and to the communities in which these professionals serve. Sysmex America is proud to be among this elite group of companies that care.
According to Karen Stoneman, Vice President of Human Resources, Sysmex America, “Our corporate philosophy, The Sysmex Way, recognizes the need to develop and respect the individuality of our employees and to provide a workplace where they can realize their full potential. In doing so, we enable them to provide our customers with unmatched quality, advanced technologies and superior
support while serving as a responsible member of society.”
Center for Companies That Care is a national, not-for-profit organization dedicated to social sustainability by engaging employers in improving the lives of employees, families, and communities. For more information about the Center, visit www.companies-that-care.org.
Karen Stoneman Vice President of
Human Resources, Sysmex America
Sysmex Canada
CML Healthcare Celebrates Milestone – Goes Live with Nation’s Largest Automated Hematology SystemCML Healthcare, Inc., a leading community-based provider of laboratory and medical imaging services in Ontario and British Columbia, has acquired and fully implemented the Sysmex HST-N™ Total Hematology Automation System, making it Canada’s largest installation to date. According to CML’s President and Chief Executive Officer Thomas Wellner, the system was “…installed on time, and on budget.”
“We are very pleased with the smooth installation process at CML’s central laboratory,” said Carl Rocha, General Manager, Sysmex Canada. “Our focus is to provide hematology solutions that help clinical laboratories improve their operations. We are proud to have accomplished this installation for CML in a timely manner.”
CML’s installation is in line with the Company’s strategy of implementing infrastructure improvements at the central laboratory and improving efficiency by leveraging technology. Sysmex’s hematology solutions will provide CML with the benefits of enhanced clinical opportunities, increased capacity, improved operational efficiencies and decreased operating costs. Using barcode technology, the Sysmex hematology system enables CML to process 12,000 – 15,000 blood counts daily.
Officials from CML Healthcare, Inc., Mississauga, Ontario, Sysmex Canada
and Sysmex Corporation, Kobe, Japan, recently unveiled CML’s new automated
hematology system at the Company’s Canadian headquarters. On hand to
participate in a ribbon cutting ceremony was Chairman and CEO of Sysmex
Corporation, Kobe, Japan, Mr. Hisashi Ietsugu, center. Also present were
CML’s Senior Vice President of Laboratory Services and Integration Wendy
Gilmour and Thomas Wellner, President and Chief Executive Officer.
Sysmex Latin America & the Caribbean
Sysmex Latin America and the Caribbean Website Gets News Look, Ease-of-Use Navigation
Sysmex Latin America and the Caribbean has launched a new website that features an updated design and functionality that makes it easier for customers, partners and distributors to access information about Sysmex products and services. Website information, available in Portuguese and Spanish languages, also provides access to educational resources, relevant distributor information, career opportunities, and key contact information. To learn more about Sysmex Latin America and the Caribbean, visit the subsidiary’s new website at https://www.sysmex.com/la.
Scientific Sessions Spotlight Sysmex Advanced Clinical Parameters Sysmex Latin America and the Caribbean joined forces with its distributor in Mexico to support scientific update sessions as part of the CONAQUIC (National Federation of Clinical Chemists in Mexico) event called, “Integrating medical area with the clinical laboratory.” Presentations by Sysmex Application Specialists Elsa Sanchez and Jessica Ovalle featured a range of topics including Sysmex advanced clinical parameters and what the doctors need to know from the clinical laboratory. More than 250 healthcare professionals attended the continuing education meetings.
17
Lab Week WinnerDr. Holly McDaniel, MD, a pathologist with Clin-Path Associates, is the Laboratory Medical Director at Banner Estrella Medical Center (BEMC) in Phoenix Arizona, submitted this article for the lab week contest. BEMC is part of the Banner System which manages 23 acute-care hospitals, as well as other health services in seven states. In Arizona, the Lab Techs and Pathologists work together as
Laboratory Sciences of Arizona (LSA) and Pathology Specialists of Arizona (PSA) to provide excellent laboratory services to the Banner patients, physicians and hospitals.
I am such a fan of Sysmex. As soon as I heard about the new parameters, Immature Granulocytes, Reticulocyte Hemoglobin, and Immature Platelet Fraction, I met with my CMO to discuss the impact that these new tests could have on patient care. The Banner Arizona Hospitals would be first to implement during 2011-2012. In the future, we expect all of the Banner Hospitals to implement the Sysmex hematology platform and report the Advanced Clinical Parameters (ACPs).
Implementation of the Sysmex XE-5000 in nine large hospitals was fairly easy. You would think getting so many analyzers up and running in multiple hospitals, would be impossible to do in seven months. Especially, when we had CAP inspections in the middle of
the implementation process! But we have outstanding laboratory technologists and the Sysmex team supported us every step of the way. It was “bam, bam, bam,” starting in December 2011 and finished up in May 2012. We’ve been extremely happy with the whole process.
The first step was implementing the analyzers in the Banner Arizona Hospital Laboratories. The next step is utilizing them to improve patient care. Education is key. Prior to implementation at my hospital, I gave presentations to each department to give them an overview of the ACPs. Handouts, memos and table toppers were also used to get the word out. Now that we are up and running, there are interpretive messages to help our end-user, clinicians, nursing, pharmacists etc., better understand these parameters. For example, the IG message states that” the IG count includes metas, myelos, pros. Bands are not included in the IG count. They are included with the neutrophil count.”
I’m a huge fan of the Immature Granulocyte (IG) count. I can see a clear cut left shift of truly significant cells – metamyelocytes, myelocytes and promyelocytes – with the IG. We now define a left shift as an absolute IG count of > 0.1 x103/uL. This is a small number of rare, but significant cells in the blood.
Let’s compare the automated IG with the manual differential. A patient with an absolute IG count of 0.2 x103/µL, meets our definition for a left shift. If the WBC count was 20 x103/µL, this means the analyzer found 320 cells out of 32,000 cells that have cellular features (cell membrane characteristics, cytoplasmic granularity, nuclear material, etc.) meeting criteria for an immature granulocyte (metamyelocyte, myelocyte or promyelocyte). Since the manual differential only counts 100 cells, to have the same result of 0.2 x103µL immature granulocytes, one immature granulocyte needs to be identified. However, the manual differential is limited by uneven distribution of cells on the slide and subjectivity of the person making the decision. If zero metamyelocytes, myelocytes or promyelocytes are identified by manual review, then the IG = 0.0 x103/µL, if two are seen the IG = 0.4 x103/µL. For a physician reviewing the CBC results, one cell on the manual differential can make the difference between no suspicion of infection versus suspicion of infection.
Looking back, I would like to make it clear to our staff that Neutrophils should be broken down into two groups, the Mature Neutrophils and the Immature Granulocytes.
1. Mature Neutrophils consist of segmented neutrophils and bands. The mature Neutrophil Count is the same as the Absolute Neutrophil Count (ANC).
2. Immature Granulocytes consist of metamyelocytes, myelocytes and promyelocytes. Previous hematology analyzers could not identify or quantify immature granulocytes, so the manual differential was the only way to identify cells less mature than segmented neutrophils.
18
Dr. Holly McDaniel, MD Medical Director at Banner
Estrella Medical Center
Two seminal articles written about the ITR (Manroe, 19791 and Schelonka 19942) give different reference values with ≤ 0.16 in one study (Zero-24 hours after birth) and 0.05-0.27 in the other (4 hours after birth). Both studies had one person performing the manual differentials, so neither study reflects the real world experience where more than one lab tech would be performing manual differentials.
An ITR of 0.2 has often been cited in the literature as the cut off for determining negative or positive probability a neonate has an infection. But, because the band count comes from the subjective, imprecise manual differential, the ITR is not reproducible. So now that we have an analyzer that can identify and quantify the immature granulocytes, wouldn’t the IG count be better than the ITR?
To me, the answer is Yes! Hands down, the automated IG is better than the ITR.
Other important parameters with our new hematology analyzer include the Immature Platelet Fraction (IPF) and the Reticulocyte Hemoglobin Content (RET-He). It’s not just a CBC.
My hospital has been live on Sysmex for almost a year now. For any lab that is in the process of implementing the ACPs, I would recommend learning about the tests as much as possible and educating administration, clinicians, informatics, pharmacy, etc., as early as possible. Find out if any committees or workgroups at your hospital or in your system are working on care pathways, quality improvements or other projects that where the ACPs could be useful. The parameters directly relate to infection/sepsis and anemia management, all of which are on hospital administration’s radar.
References:1. Manroe, Barbara L. et al. The neonatal blood count in health and disease. I.
Reference values for neutrophlic cells. Journal of Pediatrics, vol 95, No. 1, 1979 pp 89-98.
2. Schelonka, Capt. Robert L. et al. Peripheral leukocytes count and leukocyte indexes in healthy newborn term infants. Journal of Pediatrics, vol 125, Number 4, 1994, pp 603-606.
Dr. McDaniel and team having fun in the laboratory.
I am on a crusade to “BAN the BANDS”! Unfortunately this is more difficult than first anticipated. The band count is enmeshed in the medical literature as part of the criteria to help identify when a patient has a significant bacterial infection (SBI) or is septic. The neonatologists are hanging on tightly to the band count, as it is part of their equation for the Immature to Total Neutrophil Ratio (ITR).
20
SPRING 2013
Sysmex America, Inc. 577 Aptakisic Road Lincolnshire, IL 60069