Page 1
1
1
The Patient Worn Enhanced Protection Face Shield for Flexible Endoscopy 2
3
Running title: Enhanced protection face shield (EPFS) to be worn by the patient during 4 endoscopy 5
6
Jack B Anon MD* Ear Nose and Throat Specialists of Northwestern Pennsylvania 7 Erie, PA 8 Carter Denne DO UPMC Hamot Erie, PA 9 Darcy Rees Design Engineer ASPEUS Erie, PA 10
Corresponding Author: 11 Jack B Anon MD FACS 12 1645 W 8th St Erie PA 16505 13 (814)864 9994 [email protected] 14
15
FUNDING: None 16
CONFLICTS OF INTEREST: 17
Jack B Anon : co-owner Aspeus Medical 18
Darcy Rees : co-owner Aspeus Medical 19
Carter Denne: None 20
CONTRIBUTIONS: 21
Jack B Anon- study design, conception of device, manuscript writing 22
Darcy Rees- device design engineering, study design, manuscript editing and review 23
Carter Denne- device design modification, editing of manuscript 24
25
26
27
28
29
KEYWORDS: Covid-19, Flexible endoscopy, aerosolization, face shield, 30
Complete Manuscript Click here to access/download;CompleteManuscript;OTOLHNSver3.docx
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 2
2
Abstract 31
32
OBJECTIVES: The primary objective of this study was to compare the protection 33
afforded by a standard face shield design to a new enhanced design in a controlled 34
setting. 35
36
METHODS: This study was exempted from review by IRB waiver. A flexible fiberoptic 37
endoscopy was placed through stellate openings in the standard face shield and the 38
enhance face shield. A series of simulated coughs were created with bursts of 39
fluorescein dye through an atomizer tip placed within the test subject’s mouth. 40
Ultraviolet lighting illuminated the test area and areas of dye splatter were noted. 41
42
RESULTS: Fluorescein dye is easily aerosolized along the lateral inferior aspect of a 43
standard shield with significant contamination of the surrounds. The enhanced face 44
shield maintained a barrier to the aerosolized dye. 45
46
DISCUSSION Face shields, rather than face masks, should be considered as a 47
preferred alternative for the public and healthcare professionals (HCPs) alike as they 48
address many of the personal protection (PPE) concerns especially during the Covid-19 49
pandemic. Otolaryngologists are at high risk from aerosol generating procedures such 50
as flexible fiberoptic endoscopy even when wearing PPE’s. Here we describe a uniquely 51
designed face shield to be worn by the patient as another layer of protection for the 52
environment and medical personnel. 53
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 3
3
54
IMPLICATIONS FOR PRACTICE: During the course of a flexible fiberoptic endoscopy, 55
medical personnel are safely isolated from potential infectious particles with a newly 56
designed face shield. 57
58
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 4
4
INTRODUCTION: 59
The Covid-19 (SARS-CoV-2) pandemic has dramatically changed the overall practice of 60
medicine. Currently there is no immunogenic vaccine available and medical therapies 61
are just being explored, making the prevention of infection by SARS-CoV-2 of greatest 62
concern. It is recognized that universal use of face coverings in hospitals and in the 63
community interrupts the transmission of SARS-CoV-2, but concerns about availability, 64
cost, ease of use, comfort, and risks of autoinfection have prevented the healthcare 65
authorities from recommending universal personal protection equipment (PPE) 66
practices.1,2 However, it has been suggested that a face shields, rather than face 67
masks, should be considered as a preferred alternative for the public and healthcare 68
professionals (HCPs) alike as they address all of these concerns.1,2 69
70
During the Wuhan outbreak, otolaryngologists had the highest rates of nosocomial 71
spread, and anecdotal reports from around the globe appear to support the Chinese 72
experience.3-5 It has been suggested that the contact with the upper respiratory mucosa 73
of patients and the high viral load in the upper respiratory tract of SARS-CoV-2 patients 74
could be responsible for exposing otolaryngologists at higher rates than other HCPs.3,5 75
An area of particular concern are aerosol-generating procedures, such as the 76
performance of flexible fiberoptic laryngoscopy (FFL), and there are currently no formal 77
guidelines to reduce the risk of SARS-CoV-2 virus transmission during these 78
procedures.4,3 Additionally, PPE such as masks and gowns can protect the clinician but 79
the examination room environment may be contaminated for hours.4,5 80
81
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 5
5
To address this need, we have developed the enhanced protection face shield (EPFS) 82
to be worn by the patient during these procedures. The EPFS is a unique tool that was 83
designed to be worn by the patient during an FFL to address the issues of HCP 84
protection during the procedure and reduce environmental contamination. The EPFS 85
closes the superior opening with a foam strip and limits the lateral opening with an 86
increased horizontal dimension and a strong curve design. The containment is 87
increased further by the inferior opening that is sealed by the addition a lower shelf. 88
Access to the patient’s nose for endoscope placement is accomplished by the 89
placement of a stellate flexible cut opening(s) in the shield at the level of a typical 90
nostril. Here, we demonstrate the ability of the EPFS to protect the HCP and the clinical 91
environment from patient splatter during an FFL procedure. 92
93
MATERIALS AND METHODS: 94
This study is a proof of concept. The Allegheny Health Systems IRB review board 95
granted a waiver for review based on study design. The EPFS is a die cut sheet of 96
0.012-inch anti fog coated amorphous-polyethylene terephalate (APET) thermal plastic 97
measuring 11 ft by 13 ft in its final form. Further cuts are created along the inferior 98
lateral aspect along with the creation of a dual tab locking system (Figure 1). Two 99
stellate openings are also die cut anteriorly approximating the position of a patient’s 100
nostrils. These openings provide for passage of a rigid or flexible endoscope without 101
violating the shield’s protection. Foam padding attaches along the superior rim of the 102
plastic. Adjustable straps at the top and bottom allow the shield to be fit comfortably. 103
The EPFS is normally stored flat. The integral tabs- when locked into place before use- 104
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 6
6
form a lower posterior facing ledge. This conformation effectively isolates the lower and 105
lateral edges from the surrounds. (Figure 2) 106
107
The efficacy of the EPFS was evaluated in a controlled setting. A “cough” was simulated 108
with the mucosal atomization device (MAD©, Teleflex, Morrisville, NC) attached to 109
intravenous tubing connected to a 20 mL syringe filled with fluorescein dye was placed 110
into the mouth and held at the level of the lips by the teeth (Figure 3). The MAD© tip 111
faced anteriorly and atomizes fluids into a fine mist of particles 30-100 microns in size. 112
An off-the-shelf APET plastic control face shield 0.012 in thickness and 9 in length x 10 113
in wide attached to a plastic head band was used as a comparator. A stellate cut was 114
also made at the mid portion of this shield for access. The face shields were 115
sequentially placed on the test subject by a medical assistant and a 3 mm fiberoptic 116
endoscope (aScope 4 RhinoLaryngo Slim, AMBU INC, Columbia, MD) was placed 117
through the stellate opening as would occur in an actual endoscopy. For each test, the 118
“cough” consisted of applications of approximately 5-7 mL each of fluorescein dye 119
pushed through the system. Precise localization of the dye of was performed by the 120
activation of fluorescence via a floodlight 100-watt LED UV source emitting at the range 121
of 380-420 nm. Video and high resolution still photography was recorded with two 122
cameras Sony A7iii with Sony FE 28mm F/2 Camera and a Sony A6500 with Tamron 123
28-75mm F/2.8. (See supplemental video) 124
125
RESULTS 126
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 7
7
Following the test on the standard shield, there is visible fluorescein dye splatter on a 127
number of regions of the face mask (Figure 4). The fluorescein dye was scattered along 128
the side and lower parts of the plastic. More importantly, a field of fluorescein spray was 129
noted across a significant part of the subject’s white shirt. When the EPFS was tested in 130
an identical manner, the fluorescein was captured by the closed lower lateral and 131
inferior part of the shield’s shelf (Figure 5). No fluorescein was observed on the 132
subject’s clothing. The EPFS contained the contaminants within the confines of the 133
closed space around the subject’s face and protected the examining personnel. Close 134
surveillance with the UV light further showed there was no disruption of the shield’s 135
barrier by the endoscope passing through the stellate opening. 136
137
DISCUSSION 138
The aggressive protection of medical personnel, patients, and the community have 139
become issues of paramount importance since the SARS-CoV-2 pandemic revealed 140
flaws in current PPE practices and products.1-3 Most procedural considerations from 141
various groups recommend postponing all procedures that are elective or not 142
imminently necessary.3-5 This begs the question of how many important, non-SARS-143
CoV-2 diagnoses could be missed or misdiagnosed and how many patients may 144
experience delayed treatment due to SARS-CoV-2.3-5 It is essential that physicians are 145
able to get back to day-to-day patient care while maintaining the health and safety for 146
themselves, other HCPs, and patients.2-5 We believe this could be accomplished with 147
other practical PPE options. 148
149
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 8
8
There are currently no formal guidelines on the best method of reducing the risk of 150
SARS-CoV-2 transmission during routine use of FFL by otolaryngologists, which has 151
lead our group and others to consider the development of alternative PPE options so 152
that these sensitive procedures can continue.3 Here we have demonstrated that when 153
the subject is wearing the EPFS, the larger droplets of a simulated cough are captured 154
by the shield’s shelf and not spread beyond the shield’s borders or onto the subject’s 155
clothing. We further showed that there was no disruption of the shield’s barrier by the 156
endoscope passing through the stellate opening. Taken together, these data suggest 157
that the EPFS when worn by the patient during FFL procedures may provide additional 158
protection for the clinician and the clinical environment. 159
160
LIMITATIONS OF THE STUDY 161
The bioaerosol cloud produced from speaking, coughing or sneezing is a complicated 162
system. This multiphase cloud contains particle of gas, liquids and solids. Face shields 163
disrupt the flow pattern from the point source oral cavity and our dye study shows the 164
directional change will lead to a predominant inferior and lateral stream. The MAD© 165
device lower limit of droplet production is 30 mm and droplets <30 mm are not able to 166
be produced or visualized in our study. Droplets <10 mm have flow patterns similar to 167
that of air flow and are capable of escaping from around the face shield. Similarly, we 168
were constrained by the lack of the availability of laser particle analysis systems and an 169
ability to visualize all particles within the bioaerosol cloud produced by a patient. Our 170
study only gives an overview of larger droplets and further studies are planned to 171
assess the movements of smaller droplets in relation to the shield. Finally, at this time, 172
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 9
9
all examination rooms that are exposed to patients without (and maybe even with) 173
masks should be considered contaminated. We recommend that appropriate cleaning of 174
these rooms be performed. 175
176
CONCLUSIONS 177
Overall, the multifaceted utility of the EPFS combined with the low cost of $5.00 per unit 178
appears to satisfy some of the many concerns raised by the SARS-CoV-2 outbreak 179
including protection, cost-effectiveness, and supply-chain issues. 180
181
182
183
184
185
186
187
188
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 10
10
References: 189
190
1. Perencevich EN, Diekema DJ, Edmond MB. Moving Personal Protective 191
Equipment Into the Community: Face Shields and Containment of COVID-19. 192
JAMA. 2020. 193
2. Advani S, Smith B, Lewis S, Anderson DJ, Sexton DJ. Universal Masking in 194
Hospitals in the COVID-19 era: Is it Time to consider Shielding? Infection Control 195
& Hospital Epidemiology. 2020:1-9. 196
3. Vukkadala N, Qian ZJ, Holsinger FC, Patel ZM, Rosenthal E. COVID-19 and the 197
Otolaryngologist: Preliminary Evidence-Based Review. The Laryngoscope. 2020. 198
4. Chan JYK, Wong EWY, Lam W. Practical Aspects of Otolaryngologic Clinical 199
Services During the 2019 Novel Coronavirus Epidemic: An Experience in Hong 200
Kong. JAMA Otolaryngology–Head & Neck Surgery. 2020. 201
5. Givi B, Schiff BA, Chinn SB, et al. Safety Recommendations for Evaluation and 202
Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA 203
Otolaryngology–Head & Neck Surgery. 2020. 204
205
206
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 11
11
Figures: 207
1 The enhanced face shield demonstrating the design and the tab closure system 208
2 The stellate opening allows passage of the flexible endoscope. Note the MAD © 209
nozzle between the lips 210
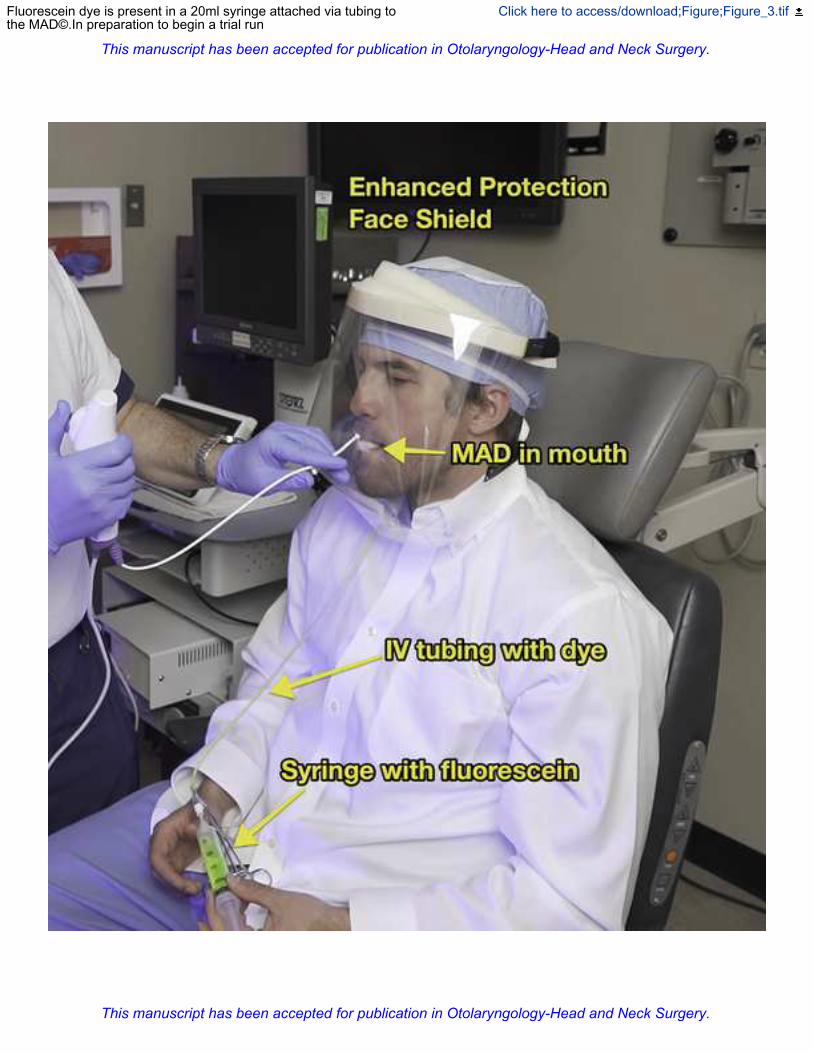
3 Fluorescein dye is present in a 20ml syringe attached via tubing to the MAD©.In 211
preparation to begin a trial run 212
4 A standard face shield revealing fluorescent dye has been atomized onto the shield 213
and beyond its boundaries 214
5 From within the enhanced shield, dye is present scattered anteriorly, laterally and 215
inferiorly. There is no encroachment through the shield’s barrier, even at the stellate 216
opening. 217
SUPPLEMENTAL VIDEO; Demonstrates the fluorescein dye study in live demo 218
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 12
The enhanced face shield demonstrating the design and the tab closure system Click here to access/download;Figure;Image_1.tif
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 13
The stellate opening allows passage of the flexible endoscope. Note the MAD © nozzlebetween the lips
Click here to access/download;Figure;Figure_2.tif
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 14
Fluorescein dye is present in a 20ml syringe attached via tubing tothe MAD©.In preparation to begin a trial run
Click here to access/download;Figure;Figure_3.tif
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 15
A standard face shield revealing fluorescent dye has been atomized onto the shieldand beyond its boundaries
Click here to access/download;Figure;Figure_4.tif
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 16
From within the enhanced shield, dye is present scattered anteriorly, laterally andinferiorly. There is no encroachment through the shield’s barrier, even at the stellate
Click here to access/download;Figure;Figure_5.tif
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 17
video
Click here to access/downloadVideo Clip
Dr. Anon Face Shield 1_compressed.mp4
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
Page 18
Institutional Review Board
FWA: 000015120
1-844-577-4621
May 8, 2020 To Whom It May Concern: The project using face shield to limit Ear Nose and Throat professional from COVID-19 would not require review from an IRB as it is not considered to be human subject research. Research is a systematic investigation, including research development, testing and evaluation, designed to develop or contribute to generalizable knowledge. As this project was to show feasibility of a device, no generalizable knowledge would be obtained. The IRB does not consider the project to be human subject research and would not be required to review this project. If you have any questions, please feel free to contact me. Sincerely,
Dawnmarie DeFazio, CIP, CHSP Director, Clinical Research and Regulatory Affairs Vice Chair, AHN Institutional Review Board
IRB Approval/Exemption
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.
This manuscript has been accepted for publication in Otolaryngology-Head and Neck Surgery.