Thoracic and Thoracic and Abdominal Trauma Abdominal Trauma Bartholomew J Tortella Bartholomew J Tortella MTS, MD, MBA, FACS, FCCM MTS, MD, MBA, FACS, FCCM through the kindness of through the kindness of James Eakins, MD James Eakins, MD Hahnemann Wolforth Trauma Hahnemann Wolforth Trauma Center Center
Transcript
Thoracic and Thoracic and Abdominal TraumaAbdominal Trauma
• Decreased breath soundsDecreased breath sounds• Decreased pulse-oxDecreased pulse-ox• Shortness of breathShortness of breath• CrepitusCrepitus• Subcutaneous airSubcutaneous air• High index of suspicion based on High index of suspicion based on
• By definition, there is no hemodynamic By definition, there is no hemodynamic compromise with a simple pneumothoraxcompromise with a simple pneumothorax
• Treat respiratory distress symptomaticallyTreat respiratory distress symptomatically• Chest tube to definitively treat Chest tube to definitively treat
pneumothoraxpneumothorax
Tension PneumothoraxTension Pneumothorax
• Air under tension in Air under tension in pleural space between pleural space between lung and chest walllung and chest wall
• Increased thoracic Increased thoracic pressure interferes with pressure interferes with venous return to the venous return to the heart, therefore heart, therefore decreasing cardiac decreasing cardiac outputoutput
• aka “sucking chest wound”aka “sucking chest wound”• Defect in chest wallDefect in chest wall• Air follows path of least resistance and Air follows path of least resistance and
goes through hole in chest wall rather than goes through hole in chest wall rather than through airway into lungsthrough airway into lungs
• Patient unable to ventilatePatient unable to ventilate• Requires a defect of about 2/3 diameter of Requires a defect of about 2/3 diameter of
tracheatrachea
Diagnosis – Open PneumothoraxDiagnosis – Open Pneumothorax
• Visible defect in chest wallVisible defect in chest wall• Air audibly moves in and outAir audibly moves in and out
Massive hemothoraxMassive hemothorax
• Massive bleeding into pleural spaceMassive bleeding into pleural space• Sources include lung, heart, great vesselsSources include lung, heart, great vessels
• Signs and symptoms of massive Signs and symptoms of massive hemorrhagehemorrhage TachycardiaTachycardia HypotensionHypotension ShockShock
• Decreased breath soundsDecreased breath sounds• Dullness to percussionDullness to percussion• Can be obvious with penetrating but hard Can be obvious with penetrating but hard
to diagnose in blunt traumato diagnose in blunt trauma
– need to stop the – need to stop the bleedingbleeding
Cardiac TamponadeCardiac Tamponade
• Buildup of blood in pericardial sacBuildup of blood in pericardial sac• Compresses heart and impairs venous Compresses heart and impairs venous
return to the heartreturn to the heart• Decreased cardiac outputDecreased cardiac output• Therefore – hypotension and deathTherefore – hypotension and death
• Not always present and conditions / Not always present and conditions / environment frequently difficultenvironment frequently difficult
• Index of suspicion must be highIndex of suspicion must be high
Treatment - TamponadeTreatment - Tamponade
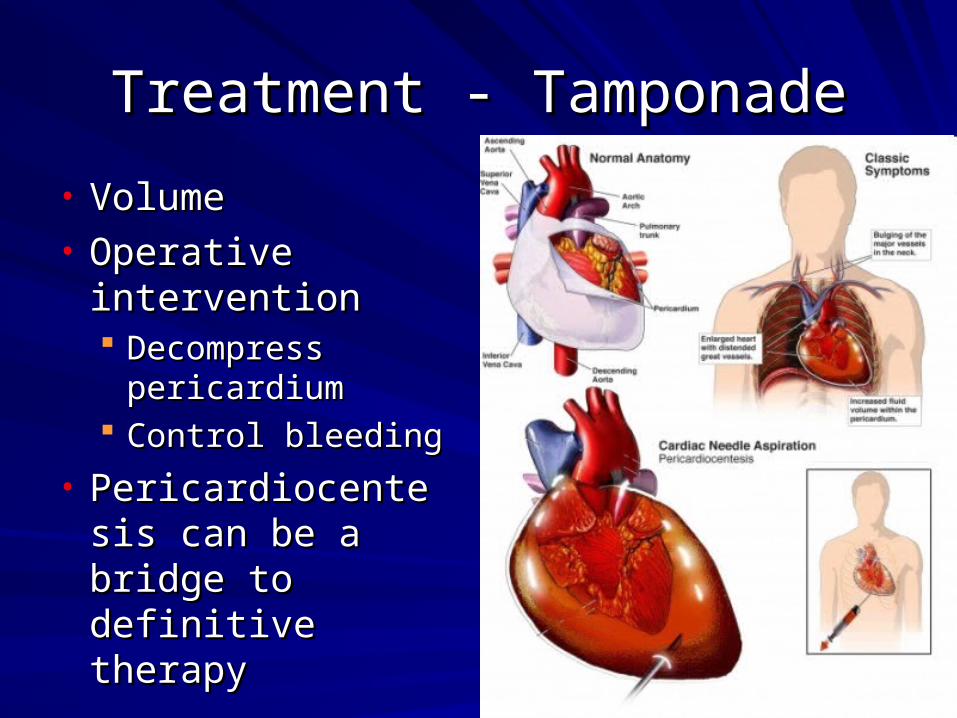
• VolumeVolume• Operative Operative
interventionintervention Decompress Decompress
pericardiumpericardium Control bleedingControl bleeding
• Pericardiocentesis Pericardiocentesis can be a bridge to can be a bridge to definitive therapydefinitive therapy
Flail ChestFlail Chest• Definition – 3 or more ribs broken in 2 placesDefinition – 3 or more ribs broken in 2 places
Flail ChestFlail Chest
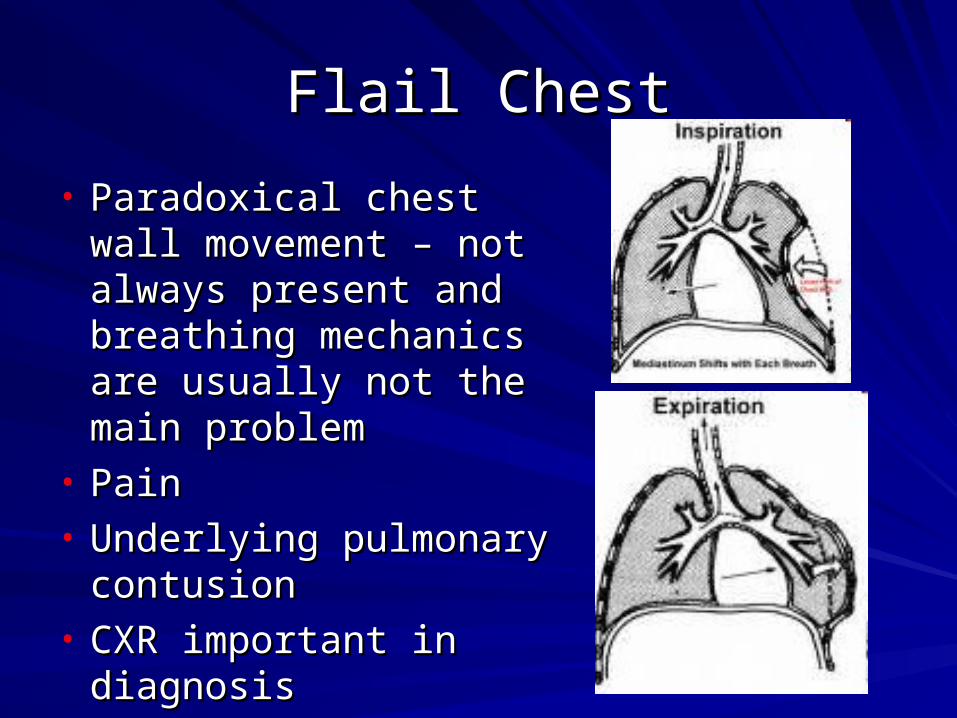
• Paradoxical chest wall Paradoxical chest wall movement – not always movement – not always present and breathing present and breathing mechanics are usually mechanics are usually not the main problemnot the main problem
contusioncontusion• CXR important in CXR important in
diagnosisdiagnosis
Treatment – Flail chestTreatment – Flail chest
• Pain ControlPain Control• Treat respiratory distress symptomaticallyTreat respiratory distress symptomatically• Intubation because of the pulmonary Intubation because of the pulmonary
problems, not the rib fracturesproblems, not the rib fractures• Taping: NEVER!!!!Taping: NEVER!!!!
ConclusionConclusion
• Many life-threatening injuries possible with Many life-threatening injuries possible with thoracic traumathoracic trauma
• ABC’s remain the sameABC’s remain the same• Prompt diagnosis and treatment is the keyPrompt diagnosis and treatment is the key
• The injuries are the same but the workup The injuries are the same but the workup depends on mechanism and depends on mechanism and hemodynamicshemodynamics
IntroductionIntroduction
• ABC’sABC’s• AnatomyAnatomy• EvaluationEvaluation• Indications for surgeryIndications for surgery
Initial EvaluationInitial Evaluation
• AirwayAirway• BreathingBreathing• CirculationCirculation• Evaluation of the abdomen can become Evaluation of the abdomen can become
important as early as “C”important as early as “C”
• The most important factor in the The most important factor in the evaluation of patients with evaluation of patients with abdominal trauma is to determine abdominal trauma is to determine
who needs an operationwho needs an operation..
• There are two general indications for There are two general indications for abdominal surgeryabdominal surgery BleedingBleeding Hollow viscus injuryHollow viscus injury
• It is only necessary to determine that one It is only necessary to determine that one of the two exists, not the specific organ of the two exists, not the specific organ involved.involved.
• AdvantagesAdvantages Very specificVery specific Very sensitiveVery sensitive Good visualization of Good visualization of
retroperitoneumretroperitoneum
• DisadvantagesDisadvantages TimeTime Need for travelNeed for travel
Algorithm for Blunt TraumaAlgorithm for Blunt Trauma
• If unstable, need to evaluate quickly for If unstable, need to evaluate quickly for intra-abdominal bleeding using U/S or DPLintra-abdominal bleeding using U/S or DPL If positive, then surgeryIf positive, then surgery If negative, then evaluate for other bleeding If negative, then evaluate for other bleeding
sources and obtain CT Scan when more sources and obtain CT Scan when more stablestable
• If stable, CT Scan is the test of choiceIf stable, CT Scan is the test of choice
Penetrating TraumaPenetrating Trauma
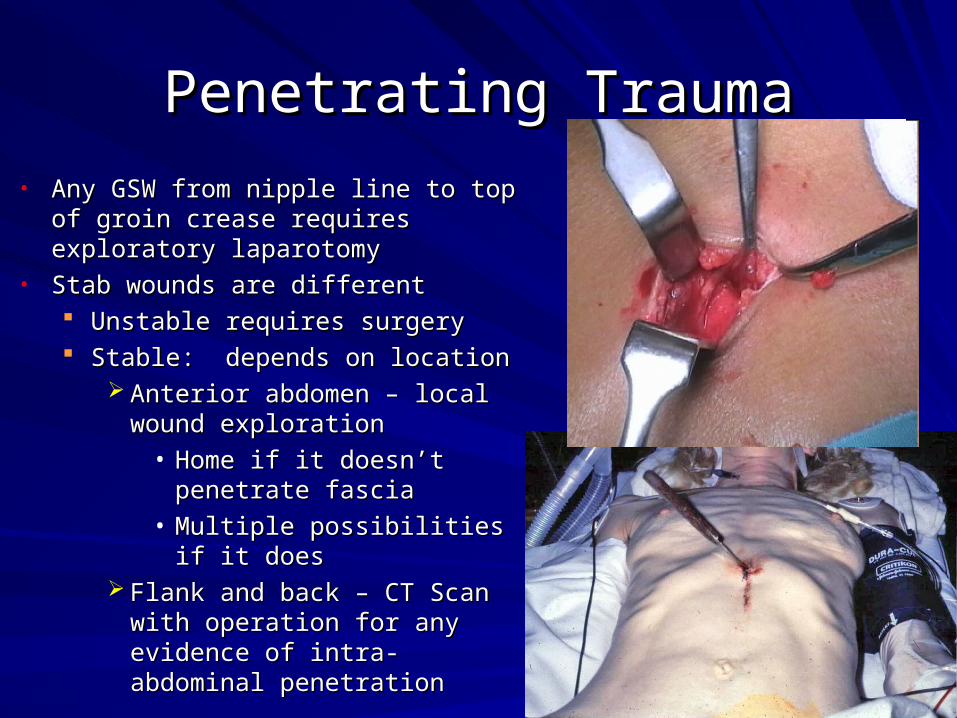
• Any GSW from nipple line to top of Any GSW from nipple line to top of groin crease requires exploratory groin crease requires exploratory laparotomylaparotomy
• Stab wounds are differentStab wounds are different Unstable requires surgeryUnstable requires surgery Stable: depends on locationStable: depends on location
Anterior abdomen – local wound Anterior abdomen – local wound explorationexploration
• Home if it doesn’t penetrate Home if it doesn’t penetrate fasciafascia
• Multiple possibilities if it Multiple possibilities if it doesdoes
Flank and back – CT Scan with Flank and back – CT Scan with operation for any evidence of operation for any evidence of intra-abdominal penetrationintra-abdominal penetration
Indications for surgeryIndications for surgery
• Any GSWAny GSW• Unstable SWUnstable SW• SW that penetrates anterior fascia or evidence SW that penetrates anterior fascia or evidence
of abdominal penetration on CT Scanof abdominal penetration on CT Scan• Unstable blunt trauma with intra-abdominal fluid Unstable blunt trauma with intra-abdominal fluid
by U/S or DPLby U/S or DPL• Stable blunt trauma with positive CT ScanStable blunt trauma with positive CT Scan
Free airFree air Free fluid without solid organ injuryFree fluid without solid organ injury Suspicion for significant retroperitoneal injurySuspicion for significant retroperitoneal injury
ConclusionConclusion
• ABC’s always come firstABC’s always come first• Not necessary to determine specific injury, Not necessary to determine specific injury,
only whether an operation is neededonly whether an operation is needed• Specific evaluation depends on patient Specific evaluation depends on patient