19
The time to act: Optimising patient care Gavin Giovannoni Queen Mary University of London, UK
| Date post: | 21-Jan-2017 |
| Category: |
Health & Medicine |
| Upload: | gavin-giovannoni |
| View: | 2,630 times |
| Download: | 0 times |

The time to act: Optimising patient careGavin GiovannoniQueen Mary University of London, UK

Who should take responsibility?
• The person with MS?
• The HCP or neurologist?
• The healthcare system?
• The regulators?
• Society?
HCP, healthcare practitioner; MS, multiple sclerosis.
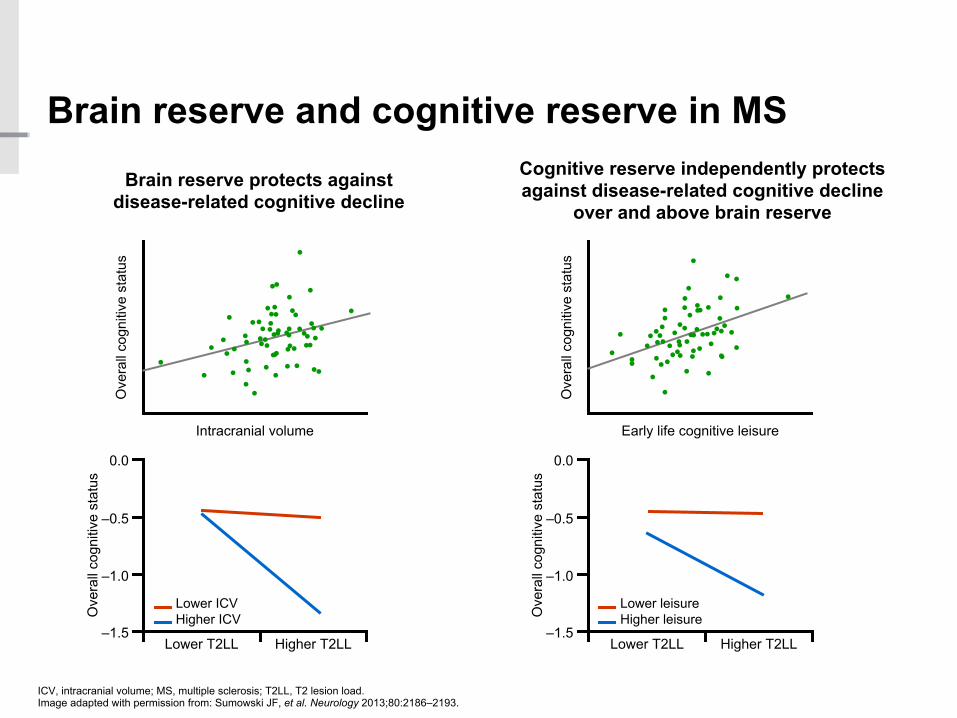
Brain reserve and cognitive reserve in MS
ICV, intracranial volume; MS, multiple sclerosis; T2LL, T2 lesion load. Image adapted with permission from: Sumowski JF, et al. Neurology 2013;80:2186–2193.
Brain reserve protects against disease-related cognitive decline
Cognitive reserve independently protects against disease-related cognitive decline
over and above brain reserve
Intracranial volume
Ove
rall
cogn
itive
sta
tus
Early life cognitive leisure
Ove
rall
cogn
itive
sta
tus
Lower T2LL
Ove
rall
cogn
itive
sta
tus
0.0
‒0.5
‒1.0
‒1.5
Ove
rall
cogn
itive
sta
tus
0.0
‒0.5
‒1.0
‒1.5Higher T2LL
Lower leisureHigher leisure
Lower ICVHigher ICV
Lower T2LL Higher T2LL
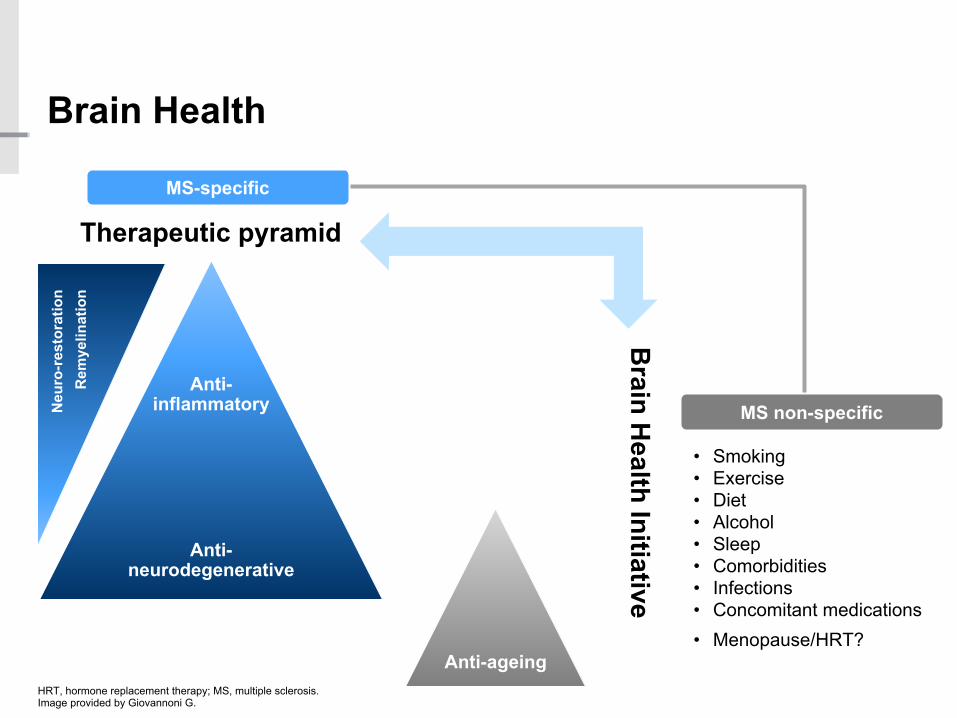
MS non-specific
Brain Health
HRT, hormone replacement therapy; MS, multiple sclerosis.Image provided by Giovannoni G.
Therapeutic pyramid
Brain H
ealth Initiative
• Smoking• Exercise• Diet• Alcohol• Sleep• Comorbidities• Infections• Concomitant medications• Menopause/HRT?
MS-specific
Anti-inflammatory
Anti-neurodegenerative
Rem
yelin
atio
nN
euro
-res
tora
tion
Anti-ageing
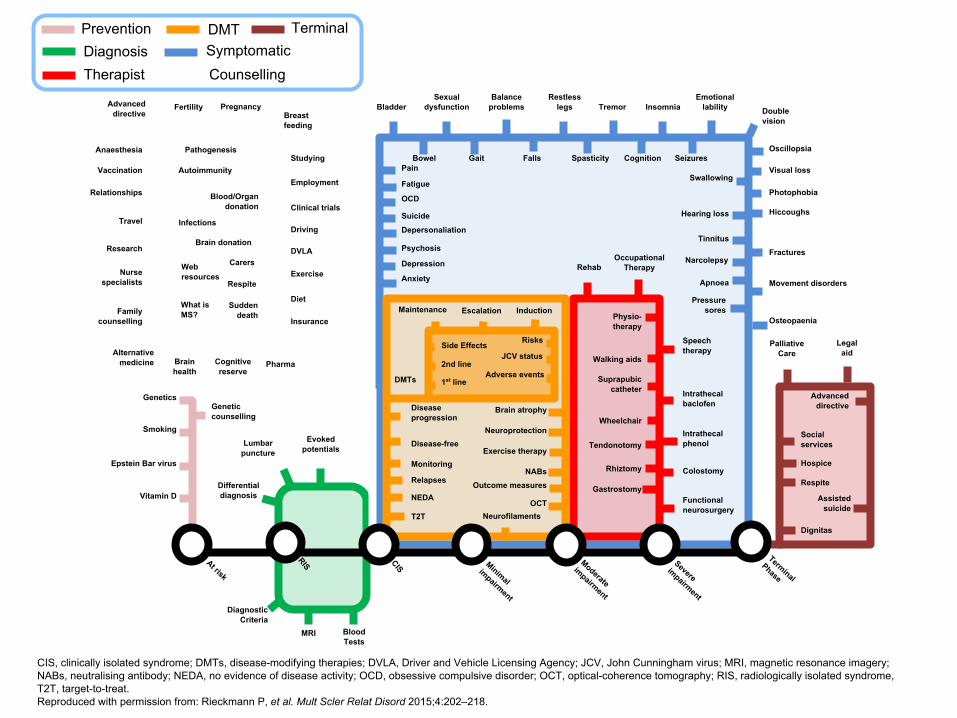
PreventionDiagnosis
DMTSymptomatic
Therapist
Terminal
Counselling
Epstein Bar virus
Genetics
Vitamin D
Smoking
Risks
Adverse events
Differentialdiagnosis
At risk
RIS CIS Minimal impairment
Moderateimpairment
Severeimpairment
Terminal
Phase
MRI
Evokedpotentials
Lumbar puncture
BloodTests
DiagnosticCriteria
Cognition
Depression
Fatigue
Bladder
Bowel
Sexual dysfunction Tremor
PainSwallowing
SpasticityFalls
Balance problems Insomnia
Restless legsFertility
Clinical trials
Gait
Pressuresores
Oscillopsia
Emotionallability
Seizures
Gastrostomy
Rehab
Suprapubiccatheter Intrathecal
baclofen
Physio-therapy
Speech therapy
OccupationalTherapy
Functional neurosurgery
Colostomy
Tendonotomy
Studying
EmploymentRelationships
Travel
Vaccination
Anxiety
Driving
Nurse specialists
Family counselling
Relapses
1st line
2nd line
Maintenance Escalation Induction
Monitoring
Disease-free
Disease progression
DMTs
Side Effects
Advanced directive
Exercise
Diet
Alternativemedicine
PregnancyBreastfeeding
Research
Insurance
Visual loss
PalliativeCare
Assistedsuicide
Socialservices
Legalaid
Genetic counselling
Intrathecalphenol
Fractures
Movement disorders
Osteopaenia
Brain atrophy
Hearing loss
Tinnitus
Photophobia
Hiccoughs
DVLA
Neuroprotection
Psychosis
Depersonaliation
Brainhealth
Cognitivereserve
Sudden death
Suicide
OCD
Narcolepsy
Apnoea
Carers
Respite
Hospice
Respite
Dignitas
Advanced directive
Rhiztomy
Wheelchair
Walking aids
Blood/Organdonation
Brain donation
Exercise therapy
NABs
Autoimmunity
Infections
Outcome measures
Webresources
Pathogenesis
Doublevision
What isMS?
NEDA
T2TOCT
Neurofilaments
JCV statusPharma
Anaesthesia
CIS, clinically isolated syndrome; DMTs, disease-modifying therapies; DVLA, Driver and Vehicle Licensing Agency; JCV, John Cunningham virus; MRI, magnetic resonance imagery; NABs, neutralising antibody; NEDA, no evidence of disease activity; OCD, obsessive compulsive disorder; OCT, optical-coherence tomography; RIS, radiologically isolated syndrome, T2T, target-to-treat.Reproduced with permission from: Rieckmann P, et al. Mult Scler Relat Disord 2015;4:202–218.
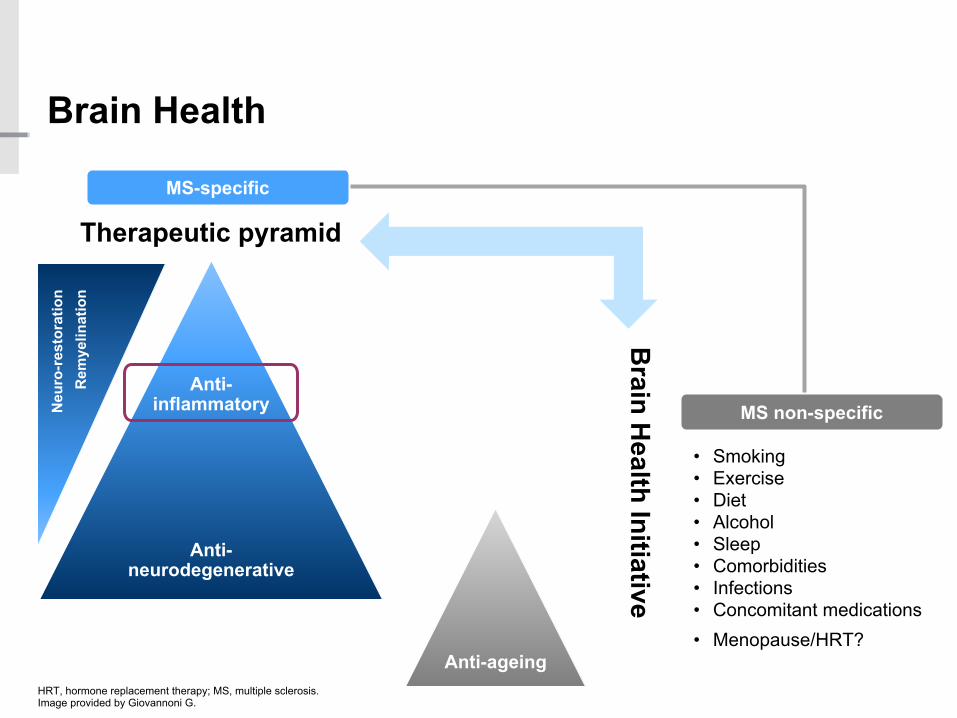
MS non-specific
Brain Health
HRT, hormone replacement therapy; MS, multiple sclerosis.Image provided by Giovannoni G.
Therapeutic pyramid
Brain H
ealth Initiative
• Smoking• Exercise• Diet• Alcohol• Sleep• Comorbidities• Infections• Concomitant medications• Menopause/HRT?
MS-specific
Anti-inflammatory
Anti-neurodegenerative
Anti-ageing
Rem
yelin
atio
nN
euro
-res
tora
tion
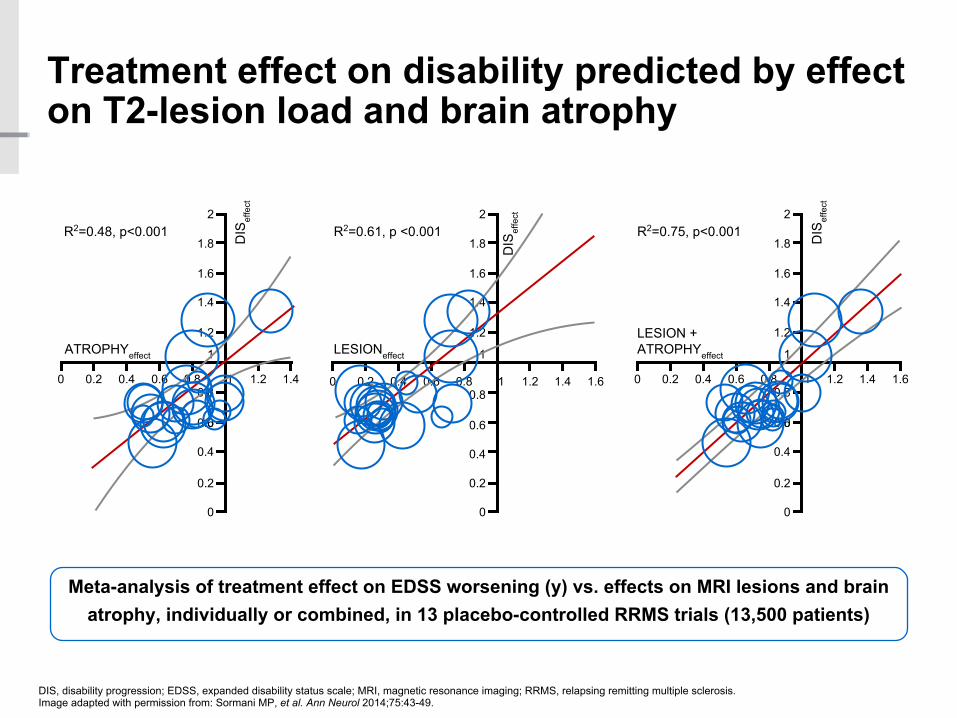
Treatment effect on disability predicted by effect on T2-lesion load and brain atrophy
DIS, disability progression; EDSS, expanded disability status scale; MRI, magnetic resonance imaging; RRMS, relapsing remitting multiple sclerosis.Image adapted with permission from: Sormani MP, et al. Ann Neurol 2014;75:43-49.
Meta-analysis of treatment effect on EDSS worsening (y) vs. effects on MRI lesions and brain atrophy, individually or combined, in 13 placebo-controlled RRMS trials (13,500 patients)
0 0.2 0.4 0.6 0.8 1 1.2 1.4
0
0.2
0.4
00.6
0.8
1
1.2
1.4
1.6
1.8
2
ATROPHYeffect
DIS
effe
ct
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
LESIONeffect
R2=0.61, p <0.001
DIS
effe
ct
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6
0
0.2
0.4
00.6
0.8
1
1.2
1.4
1.6
1.8
2
LESION + ATROPHYeffect
R2=0.75, p<0.001 DIS
effe
ct
R2=0.48, p<0.001

Rapid adoption of innovations is“biggest unmet need of all”
Adapted from: Rogers EM, Diffusion of Innovations. New York, Free Press of Glencoe 1962.
Laggards
Late adopters
Majority adopters
Early adopters
~30% tipping point
Innovators
Time0%
50%
100%
Per
cent
age
of ta
rget
pop
ulat
ion
who
ado
pt

Large disparities exist in access to DMTs
DMT, disease-modifying therapy; MS, multiple sclerosis.Image provided by Giobannoni G. 1. Hollingworth S et al. J Clin Neurosci 2014;21:2083–2087; 2. World Bank, 2015. http://data.worldbank.org/indicator/SP.POP.TOTL. Accessed 27 May 2016;3. MSIF, 2013. http://www.atlasofms.org Accessed 27 May 2016; 4. Wilsdon T, et al. 2013. http://crai.com/sites/default/files/publications/CRA-Biogen-Access-to-MS-Treatment-Final-Report.pdf, Accessed 27 May 2016.
0 20 40 60 80 100
Newer DMTEstablished DMTNo DMT
All people with MS (%)
All data are from 2013
4
4
4
4
4
4
4
4
44
4
4
4
1–3
Established DMTsDMTs approved for relapsing forms of MS during the 1990s and reformulations or generic versions of these substances
Newer DMTsDMTs approved for relapsing forms of MS that have a different mechanism of action from established DMTs
Perf
orm
ance
Time
Old
New
Newer
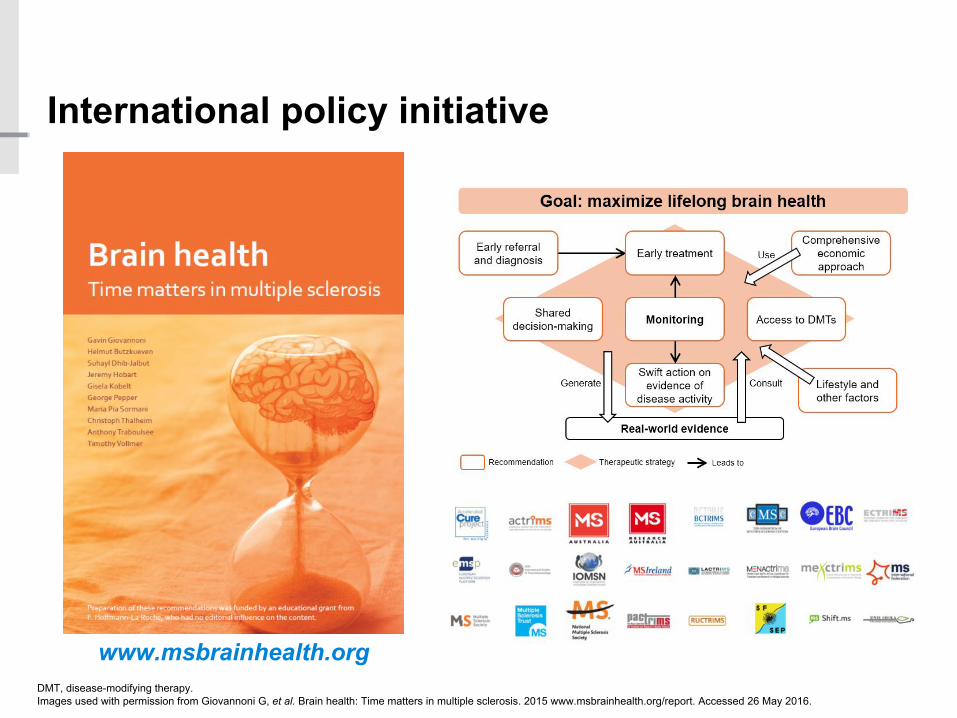
www.msbrainhealth.org
International policy initiative
DMT, disease-modifying therapy. Images used with permission from Giovannoni G, et al. Brain health: Time matters in multiple sclerosis. 2015 www.msbrainhealth.org/report. Accessed 26 May 2016.
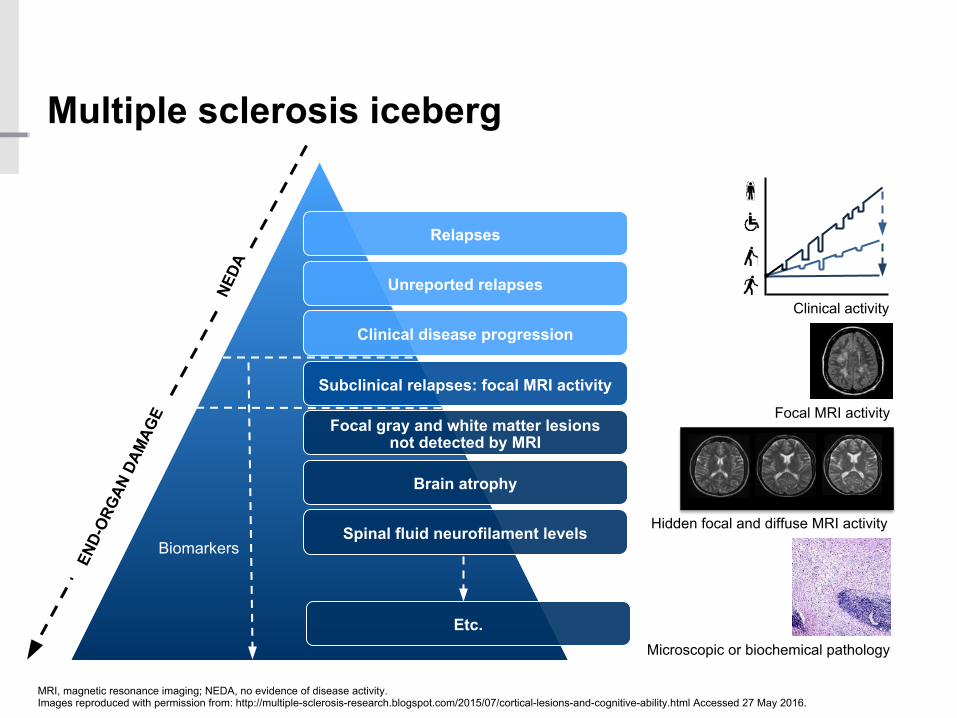
Relapses
Unreported relapses
Clinical disease progression
Subclinical relapses: focal MRI activity
Focal gray and white matter lesions not detected by MRI
Brain atrophy
Spinal fluid neurofilament levels
Etc.
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
Biomarkers
NEDA
END-
ORG
AN D
AMAG
E
Multiple sclerosis iceberg
MRI, magnetic resonance imaging; NEDA, no evidence of disease activity. Images reproduced with permission from: http://multiple-sclerosis-research.blogspot.com/2015/07/cortical-lesions-and-cognitive-ability.html Accessed 27 May 2016.
Stroke or brain attack: ‘time really is brain’
Passive Active
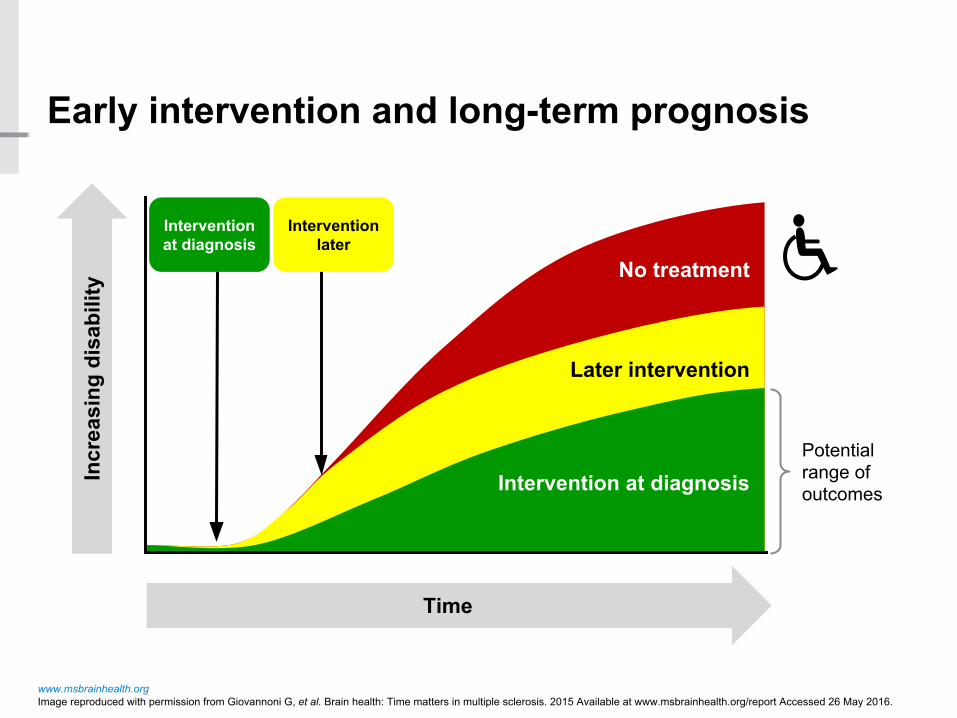
Early intervention and long-term prognosis
www.msbrainhealth.orgImage reproduced with permission from Giovannoni G, et al. Brain health: Time matters in multiple sclerosis. 2015 Available at www.msbrainhealth.org/report Accessed 26 May 2016.
Incr
easi
ng d
isab
ility
Time
Intervention at diagnosis
Intervention later
Potentialrange ofoutcomes
No treatment
Later intervention
Intervention at diagnosis

Barts-MS: 2016 Brain Health Challenge
Treat-2-Target
Lifestyle
Comorbidities
Wellness 2016Brain Health
Challenge
Barts-MS
Barts-MS: 2016 Brain Health Challenge
MS, multiple sclerosis; NEDA, no evidence of disease activity ,
• Prognosis• Active MS• Treatment• Re-baselining• Monitoring• NEDA
Treat-2-Target
Lifestyle
Comorbidities
Wellness
Barts-MS: 2016 Brain Health Challenge
• Diet & supplements• Exercise• Smoking• Alcohol• Sleep• Stress
Treat-2-Target
Lifestyle
Comorbidities
Wellness
Barts-MS: 2016 Brain Health Challenge
• Obesity• Hypertension• Glucose• Cholesterol• Smoking• Sleep disorders• Infections• Falls• Depression & anxiety• Concomitant medications
Treat-2-Target
Lifestyle
Comorbidities
Wellness
Barts-MS: 2016 Brain Health Challenge
• Intellectual• Emotional• Physical• Social• Spiritual• Occupational• Environmental
Treat-2-Target
Lifestyle
Comorbidities
Wellness

“Our vision is to create a better future for people with MS and their families”

















