Page 1
8/05/2015
1
Catarina Ang FRANZCOG 20 May 2011
Dr W. Catarina Ang MBBS DSHR (UK) DUE AFSA (France) Dip Epid FRANZCOG MBS MRepMed
Gynaecology Advanced Laparoscopy Infertility
Head of Gynaecology Unit 1, Royal Women’s Hospital
affil Cabrini & Epworth Hospitals, City Fertility Centre Catarina Ang FRANZCOG
New & old procedures for symptomatic fibroids
Myosure for SM fibroids
MRgFUS and UAE for conservative management of fibroids
Malignancy & fibroids – recent controversies & surgical
management
Anything new in pelvic pain/dysmenorrhoea?
Dienogest for endometriosis
The endometriosis assessment scan
Catarina Ang FRANZCOG
Common – 1 in 2
Benign growths of muscle cells in uterus
Different manifestations
asymptomatic
HMB
Pressure sx, pain
↓ fertility
Prolonged PVB (hypermenorrhoea) ↑ with endometritis
frequent histologically
IMB by ulcerating through endometrial lining / distorting cavity & causing congestion of surrounding
Rarely, may prolapse through cervix resulting in profuse bleeding
Catarina Ang FRANZCOG
Catarina Ang FRANZCOG
First reported 1976 (Neuwirth and Amin) monopolar current & 32% dextran 70
1987 Hallez Also converted urologic
resectoscope
0 scope, 1.5% glycine
Evolved into standard
surgical procedure, several
techniques Excision of intramural component by
slicing
‘Cold loop’ myomectomy
Complete excision of fibroid by two-step
procedure
‘Enucleation in toto’
‘hydromassage’
Catarina Ang FRANZCOG
• 0 - Fibroids totally in cavity
• I - sessile with <50%
intramural extension i.e. More
than 50% in cavity
• II – sessile with >50%
intramural extension i.e. Less
than 50% in cavity Wamsteker K, 1993
Page 2
8/05/2015
2
Catarina Ang FRANZCOG
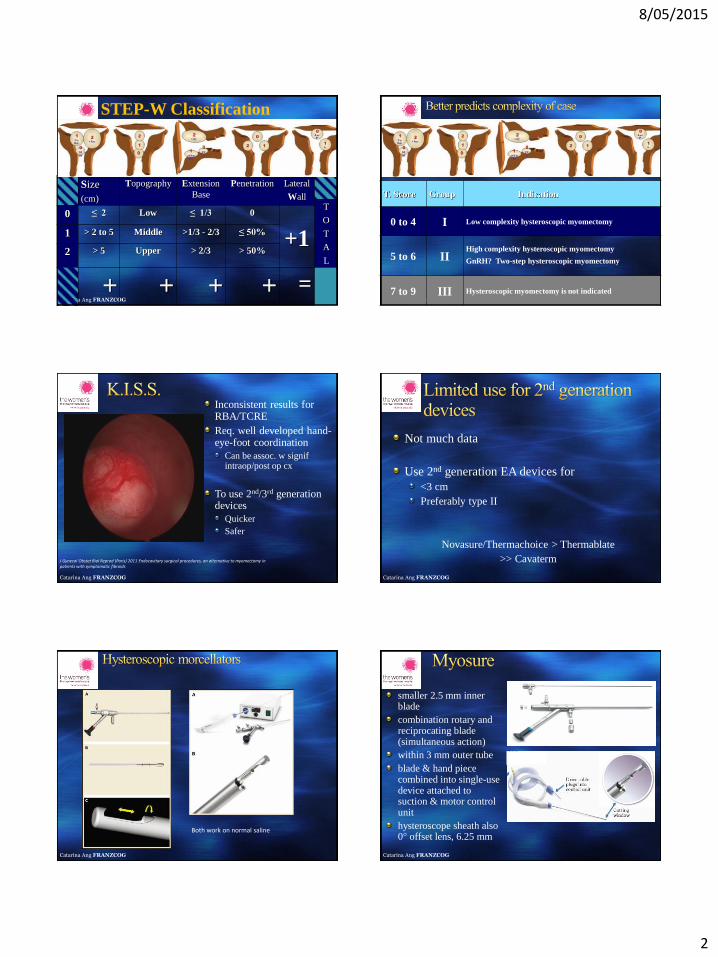
STEP-W Classification
Size
(cm)
Topography Extension
Base
Penetration Lateral
Wall T
O
T
A
L
0 ≤ 2 Low ≤ 1/3 0
+1 1 > 2 to 5 Middle >1/3 - 2/3 ≤ 50%
2 > 5 Upper > 2/3 > 50%
= Catarina Ang FRANZCOG
T. Score Group Indication
0 to 4 I Low complexity hysteroscopic myomectomy
5 to 6 II High complexity hysteroscopic myomectomy GnRH? Two-step hysteroscopic myomectomy
7 to 9 III Hysteroscopic myomectomy is not indicated
Catarina Ang FRANZCOG
Inconsistent results for RBA/TCRE
Req. well developed hand-eye-foot coordination
Can be assoc. w signif intraop/post op cx
To use 2nd/3rd generation devices
Quicker
Safer
J Gynecol Obstet Biol Reprod (Paris) 2011 Endocavitary surgical procedures, an alternative to myomectomy in patients with symptomatic fibroids
Catarina Ang FRANZCOG
Not much data
Use 2nd generation EA devices for
<3 cm
Preferably type II
Novasure/Thermachoice > Thermablate
>> Cavaterm
Catarina Ang FRANZCOG
Both work on normal saline
Catarina Ang FRANZCOG
smaller 2.5 mm inner blade
combination rotary and reciprocating blade (simultaneous action)
within 3 mm outer tube
blade & hand piece combined into single-use device attached to suction & motor control unit
hysteroscope sheath also 0° offset lens, 6.25 mm
Page 3
8/05/2015
3
Catarina Ang FRANZCOG Catarina Ang FRANZCOG http://www.thewomens.org.au/uploads/downloads/HealthProfessionals/CSD/Imaging/MRgFUS_for_Uterine_Fib
roid_Treatment.pdf
Catarina Ang FRANZCOG
How does it work? MRI to locate the fibroids
direct, high-intensity ultrasound energy to destroy fibroid tissue
+ve less invasive than hysterectomy & myomectomy
Which carries a <1% chance of unplanned hysterectomy
with faster recovery
-ve Not suitable for all e.g. Haemodynamic compromise, abdominal scars
Risks inc burns, nerve injury, fibroid migration, pain
Takes time for fibroid to decrease in size (months)
Not permanent
Uncertainty re subsequent fertility / evolving technology
Catarina Ang FRANZCOG
NPV ratio
92%
54.4c
c
15.7c
c
71% volume & 75% symptom reduction at 24 months
SSS-QOL:
62.5
SSS-QOL:
15.6
57 sonications
Acknowledgements to Dr A Dobrotwir
Catarina Ang FRANZCOG
17 pregnancies
13 live births
4 NVD, 7 elective LUSCS, 2 emerg LUSCS
1 miscarriage
3 ongoing
Baby Neroli
Fertility Enhancement
– 9 successful pregnancies
– 10 live births
– Mean age 38yo
– Mean time to conception 9 months
– Mean birth weight 2.9 kg
– Mean gestational age 38 weeks
Acknowledgements to Dr A Dobrotwir Catarina Ang FRANZCOG
good improvement >85% sx of menstrual loss
– mean dominant fibroid volume ↓ 30-46%
min invasive qv surgery for LOS, ADLs
“angiogram”
overnight stay
Fibroid may regrow
Page 4
8/05/2015
4
Catarina Ang FRANZCOG Acknowledgements to Dr J Druce & Cabrini Radiology Catarina Ang FRANZCOG
good improvement >85% sx of menstrual loss
– mean dominant fibroid volume ↓ 30-46%
min invasive qv surgery for LOS, ADLs
but assoc. with ↑ minor post procedural cx – vaginal discharge
– post puncture haematoma
– post embolization syndrome (pain, fever, nausea, vomiting)
– ↑ # unscheduled visits
– ↑ readmission rates
– ↑FSH levels post UAE ?ovarian dysfunction
Catarina Ang FRANZCOG Catarina Ang FRANZCOG
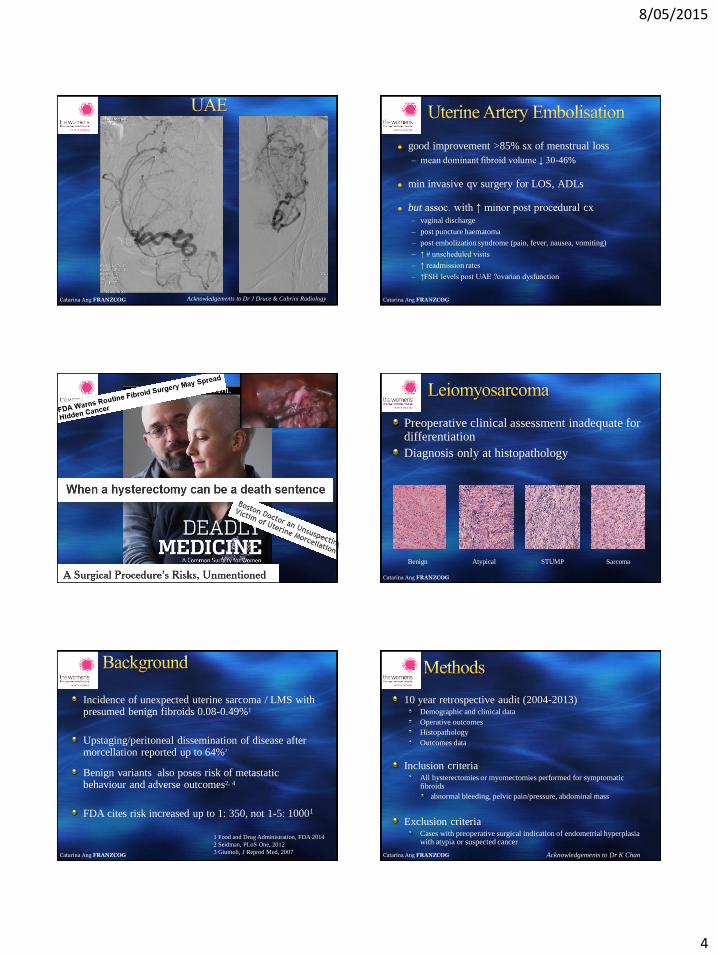
Preoperative clinical assessment inadequate for differentiation
Diagnosis only at histopathology
Benign Atypical STUMP Sarcoma
Catarina Ang FRANZCOG
Incidence of unexpected uterine sarcoma / LMS with presumed benign fibroids 0.08-0.49%1
Upstaging/peritoneal dissemination of disease after morcellation reported up to 64%2
Benign variants also poses risk of metastatic behaviour and adverse outcomes2, 4
FDA cites risk increased up to 1: 350, not 1-5: 10001
1 Food and Drug Administration, FDA 2014
2 Seidman, PLoS One, 2012
3 Giuntoli, J Reprod Med, 2007 Catarina Ang FRANZCOG
10 year retrospective audit (2004-2013) Demographic and clinical data
Operative outcomes
Histopathology
Outcomes data
Inclusion criteria All hysterectomies or myomectomies performed for symptomatic fibroids
abnormal bleeding, pelvic pain/pressure, abdominal mass
Exclusion criteria Cases with preoperative surgical indication of endometrial hyperplasia with atypia or suspected cancer
Acknowledgements to Dr K Chan
Page 5
8/05/2015
5
Catarina Ang FRANZCOG
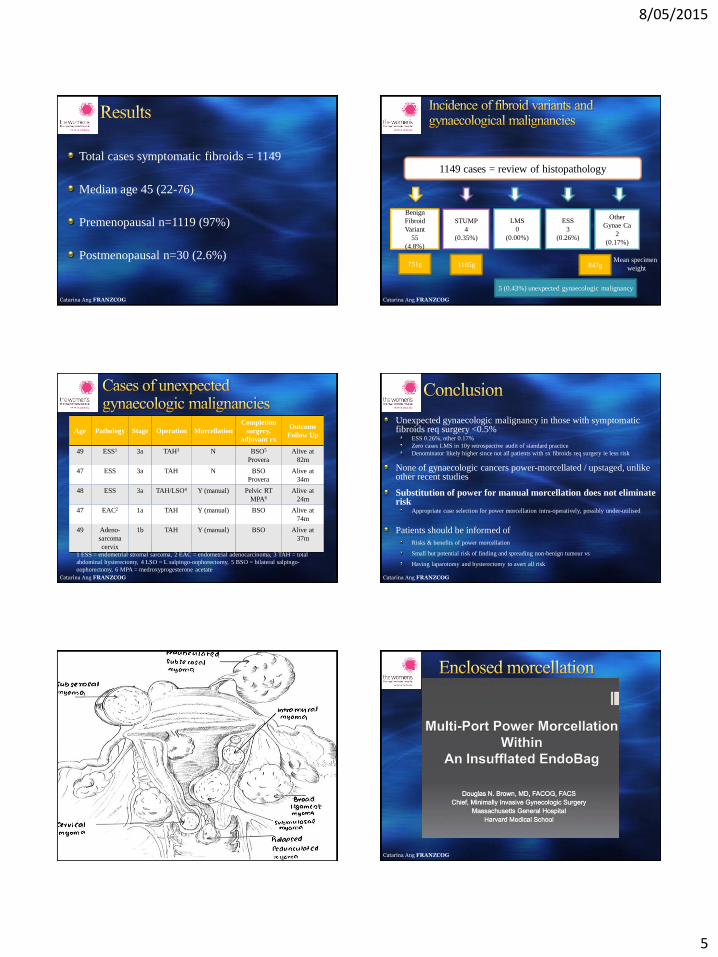
Total cases symptomatic fibroids = 1149
Median age 45 (22-76)
Premenopausal n=1119 (97%)
Postmenopausal n=30 (2.6%)
Catarina Ang FRANZCOG
1149 cases = review of histopathology
5 (0.43%) unexpected gynaecologic malignancy
Benign
Fibroid
Variant
55
(4.8%)
STUMP
4
(0.35%)
LMS
0
(0.00%)
ESS
3
(0.26%)
Other
Gynae Ca
2
(0.17%)
751g 1185g 847g Mean specimen
weight
Catarina Ang FRANZCOG
Age Pathology Stage Operation Morcellation
Completion
surgery,
adjuvant rx
Outcome
Follow Up
49 ESS1 3a TAH3 N
BSO5
Provera
Alive at
82m
47 ESS 3a TAH N
BSO
Provera
Alive at
34m
48 ESS 3a TAH/LSO4
Y (manual)
Pelvic RT
MPA6
Alive at
24m
47 EAC2 1a TAH Y (manual) BSO Alive at
74m
49 Adeno-
sarcoma
cervix
1b TAH Y (manual) BSO Alive at
37m
1 ESS = endometrial stromal sarcoma, 2 EAC = endometrial adenocarcinoma, 3 TAH = total
abdominal hysterectomy, 4 LSO = L salpingo-oophorectomy, 5 BSO = bilateral salpingo-
oophorectomy, 6 MPA = medroxyprogesterone acetate
Catarina Ang FRANZCOG
Unexpected gynaecologic malignancy in those with symptomatic fibroids req surgery <0.5%
ESS 0.26%, other 0.17%
Zero cases LMS in 10y retrospective audit of standard practice
Denominator likely higher since not all patients with sx fibroids req surgery ie less risk
None of gynaecologic cancers power-morcellated / upstaged, unlike other recent studies
Substitution of power for manual morcellation does not eliminate risk
Appropriate case selection for power morcellation intra-operatively, possibly under-utilised
Patients should be informed of
Risks & benefits of power morcellation
Small but potential risk of finding and spreading non-benign tumour vs
Having laparotomy and hysterectomy to avert all risk
Catarina Ang FRANZCOG 20 May 2011 Catarina Ang FRANZCOG
Page 6
8/05/2015
6
Catarina Ang FRANZCOG Catarina Ang FRANZCOG
Catarina Ang FRANZCOG
2010 TGA approved
Selective progestogen receptor agonist combining NET and other progestogen properties with less side effects eg hyperandrogenic, BTB
pain (65 w), continuing 24 w post cessation factors PGE2, IL6, IL8, NGF, VEGF
dysmen, pre-menstrual pain, dyspareunia, CPP
Moderate ovarian activity
Equivalent at least to GnRH analogues
Favourable safety and tolerability profile, <5% cessation
Reduction of endometriotic lesions
Catarina Ang FRANZCOG
No research into contraceptive efficacy
More costly qv COC Or other progestogens, GnRH analogues
Does not assist endometriosis-associated infertility
<5% cessation fr ADRs, most commonly abnormal bleeding (improves if persist)
headache
breast discomfort,
depressed mood
acne
1998 Eur J Endocrinol Effects of dienogest, a synthetic steroid, on experimental endometriosis in rats.
2010 IJGO A dose-ranging study to determine the efficacy and safety of 1, 2, and 4mg of dienogest daily for endometriosis.
2010 EJOGRB Dienogest in treatment of endometriosis-associated pelvic pain: a 12-week, randomized, double-blind, placebo-controlled study
2010 HR Dienogest is as effective as leuprolide acetate in treating the painful symptoms of endometriosis: 24-week, randomized, multicentre,
open-label trial.
Catarina Ang FRANZCOG
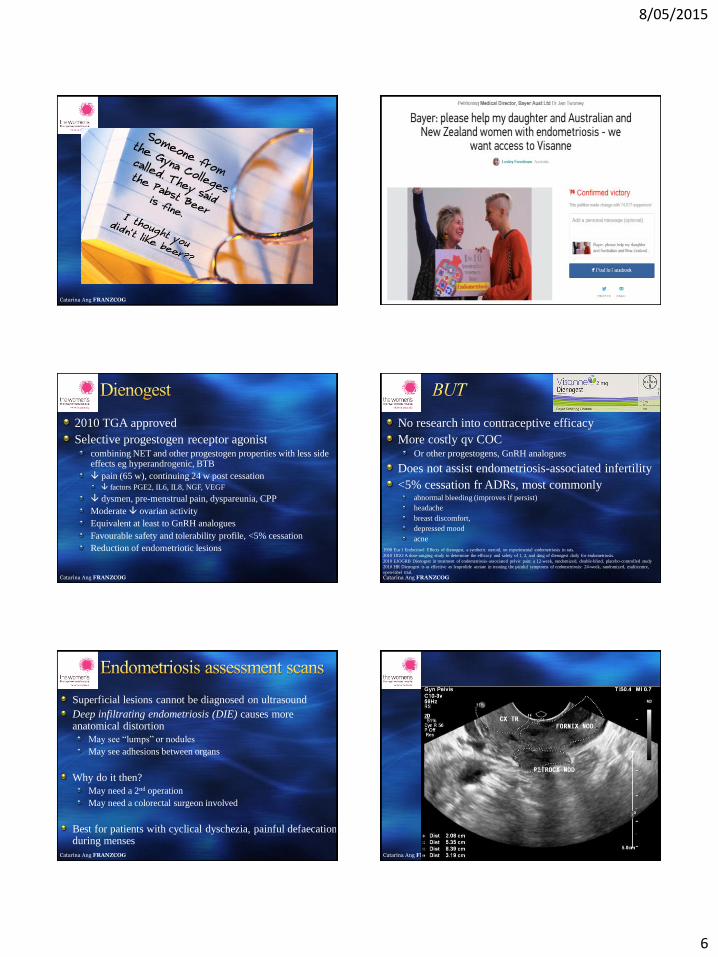
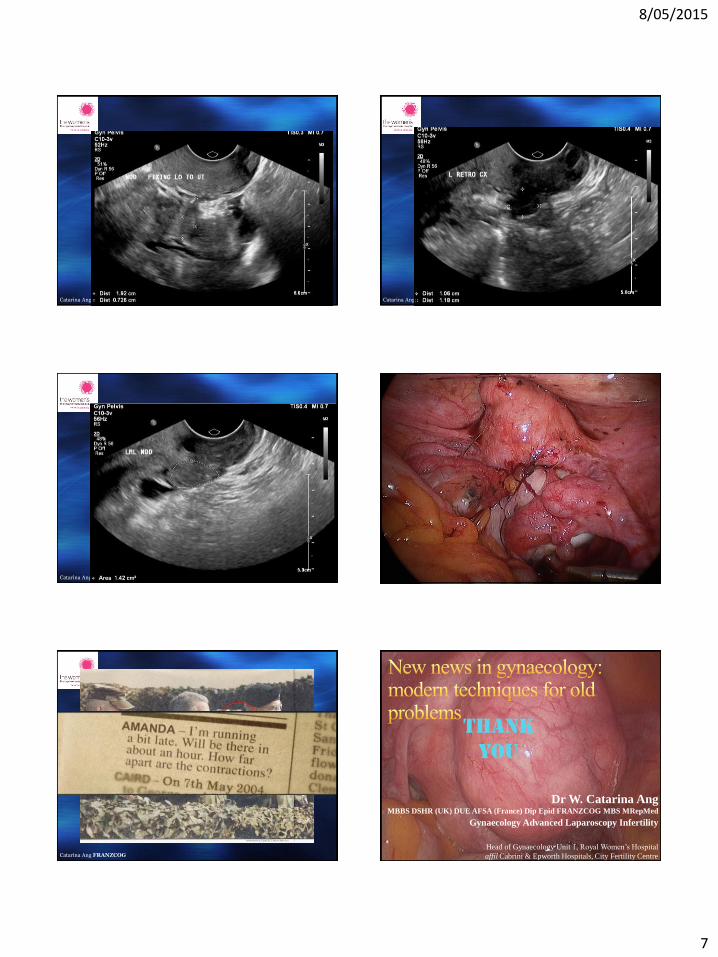
Superficial lesions cannot be diagnosed on ultrasound
Deep infiltrating endometriosis (DIE) causes more anatomical distortion
May see “lumps” or nodules
May see adhesions between organs
Why do it then?
May need a 2nd operation
May need a colorectal surgeon involved
Best for patients with cyclical dyschezia, painful defaecation during menses
Catarina Ang FRANZCOG 20 May 2011
Page 7
8/05/2015
7
Catarina Ang FRANZCOG 20 May 2011 Catarina Ang FRANZCOG 20 May 2011
Catarina Ang FRANZCOG 20 May 2011 Catarina Ang FRANZCOG
Catarina Ang FRANZCOG Catarina Ang FRANZCOG 20 May 2011
Dr W. Catarina Ang MBBS DSHR (UK) DUE AFSA (France) Dip Epid FRANZCOG MBS MRepMed
Gynaecology Advanced Laparoscopy Infertility
Head of Gynaecology Unit 1, Royal Women’s Hospital
affil Cabrini & Epworth Hospitals, City Fertility Centre
Thank
you