Page 1
_____________________________________________________________________ 1
TITLE PAGE
THE PATTERN AND OUTCOME OF TREATMENT OF PLEURAL EFFUSION IN
NATIONAL HOSPITAL ABUJA, NORTH-CENTRAL NIGERIA :
AN EVALUATION OF AETIOLOGY, DIAGNOSIS, TREATMENT AND
OUTCOME OF TREATMENT IN A 1 YEAR PROSPECTIVE
STUDY IN NATIONAL HOSPITAL.
A dissertation submitted to the National Post-Graduate Medical
College of Nigeria(NPMCN) in partial fulfillment of the
requirements for the award of the Fellowship of the
Faculty of Surgery [FMCS].
BY
DR. UGWUANYI UGOCHUKWU CHARLES P.
DEPT. OF SURGERY
NATIONAL HOSPITAL ABUJA.
NOV.2006
Page 2
_____________________________________________________________________ 2
DECLARATION PAGE
“It is hereby declared that this work on Pattern and Outcome
of Treatment of Pleural Effusion in National Hospital Abuja,
done under the direct supervision of Dr.S.A.I. Salawu(FMCS)
is original and has not been presented to any other college
for a fellowship, nor has it been submitted elsewhere for
publication”.
Dr.Ugwuanyi Charles Ugochukwu
ATTESTATION PAGE
I hereby certify that the work on Pattern and Outcome
of Treatment of Pleural Effusion in National Hospital by
Page 3
_____________________________________________________________________ 3
Dr.Ugwuanyi Charles Ugochukwu was carried out under my
supervision.
You may therefore accord it any necessary considerations.
Thank you.
Dr. S.A.I. SALAWU( FMCS, FWACS, FICS)
Chief Consultant Surgeon,
National Hospital Abuja, Nigeria.
TABLE OF CONTENTS.
Title Page i
Declaration ii
Attestation iii
Table of contents iv
Dedication v
Acknowledgement vi
Ethical Clearance vii
Summary/Abstract 1
Introduction 4
Chapter 1-Literature Review 5
Chapter 2-Materials/Method 52
Chapter 3-Results 59
Chapter 4-Discussion/conclusions 79
References 94
Proforma for Analysis 99
Page 4
_____________________________________________________________________ 4
DEDICATION
To Ifeoma, Chommy, Somtoo and Munny.
For being there.
Page 5
_____________________________________________________________________ 5
ACKNOWLEDGEMENTS
I will start by thanking the Almighty God for sound health,
guidance and protection .
My wife, Ifeoma and my children, Chommy, Somtoo and Munny
deserve special thanks for tolerating those long hours
in the office during this work.
The Chief Medical Director of National Hospital Abuja,
Dr. Z.O. Ajuwon, was very encouraging and deserves a special
appreciation.
I am also full of thanks to the Head of Department of
Surgery, National Hospital Abuja , Dr. Y.D. Abubakar
for the departmental support given to this project.
For taking the pains to supervise every stage of
this project I am most grateful to Dr. S.A.I
Salawu, Consultant Surgeon National Hospital Abuja.
Special thanks goes to Prof. Oluwole Adebo, Consultant
Cardiothoracic Surgeon, University College Hospital
Ibadan, Nigeria, for all his useful suggestions.
Page 6
_____________________________________________________________________ 6
Dr. Tony Anigbo, Chief Consultant Neurosurgeon in the
National Hospital, was the major source of inspiration
and deserves more thanks than I can offer.
Former Head of Department of Surgery, National Hospital
Abuja, Prof. P.O. Obekpa whom I regard as my mentor
as a Surgeon was always accessible for advice and
any form of support, and I thank him for that immensely.
All the Resident Doctors in the National Hospital
Abuja, especially in the Surgery Department were very
supportive and I remain thankful to them. Dr(S).Lawal,
Ihekire, Adamu, Udoye, Ekwueme deserve special mention.
Other members of staff of the National Hospital
Abuja, especially in the Nursing, Radiology, Chemical
Pathology, Microbiology, and histopathology ,too numerous
to mention here were very helpful and I remain very
thankful to them.
THE SUMMARY/ABSTRACT
Problem under Study – Pleural Effusion is a common cause
Page 7
_____________________________________________________________________ 7
of morbidity/mortality in our daily clinical practice.
There are several causes of Pleural Effusion. Whereas most
medically related causes require treatment directed
mainly at the primary cause, others require in addition
some form of surgical intervention.
Objective of the Study – To find out the common causes
of surgically important pleural effusion in the
National Hospital Abuja Nigeria, and also the
contemporary methods of diagnosis , therapy and outcome
of such.
Methodology – All cases of Pleural Effusion requiring some
form of surgical intervention , by way of tube
thoracostomy drainage at some point in their management
were sampled over a one year period spanning between
February 2005 to February 2006 in a prospective
fashion. Relevant clinical data including clinical symptoms
and signs, radiological findings, results of pleural
fluid analysis ,primary disease condition, treatments
directed at both the primary pathology as well as the
effusion , the common complications observed during
treatment and the outcome of these treatments recorded
at 6 months re-evaluation were all recorded in a
proforma.
Statistical analysis of data was done with EPI-INFO soft
ware and presented in form of pie charts, bar charts,
histogram and tables.
Results – Of the 86 cases of surgically important
pleural effusion sampled, the commonest presentation was
dyspnoea (100%) and dullness to percussion on the
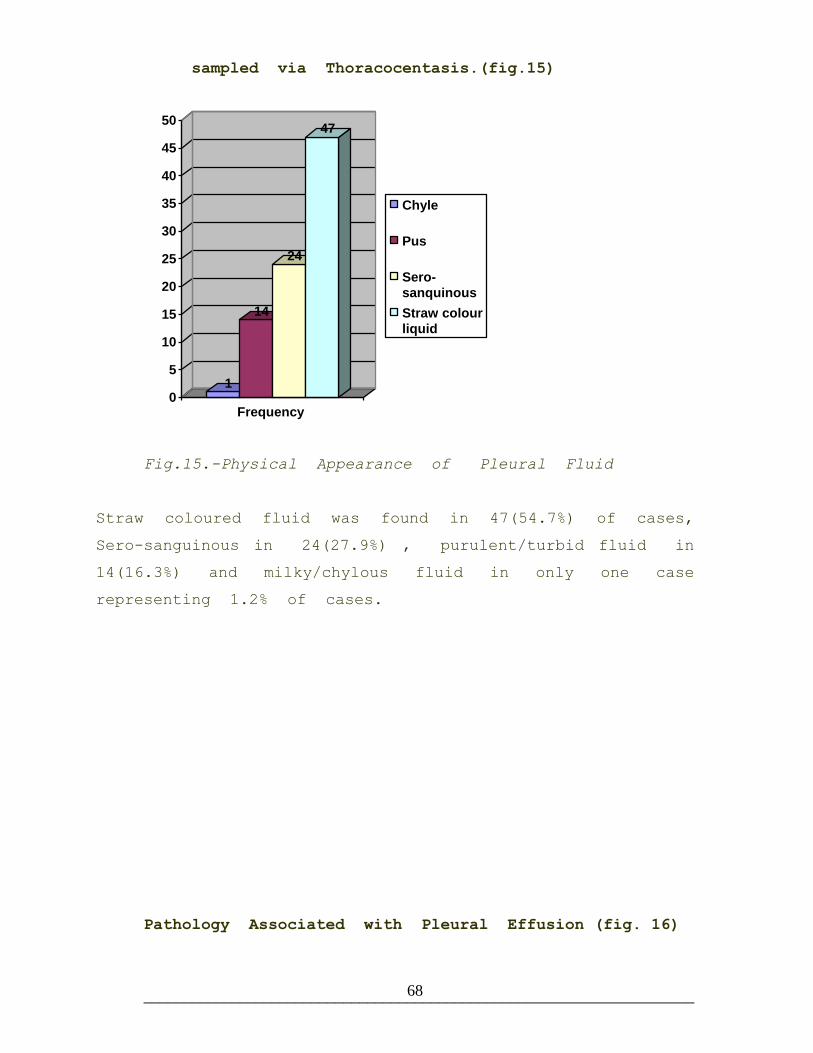
affected hemithorax(100%). Thoracentasis yielded straw
Page 8
_____________________________________________________________________ 8
coloured fluid in (54.7%), sero-sanguinous in (27.9%),
turbid/purulent in (16.3%) and chyle in (1.2%) only. The
commonest radiological feature was the meniscus sign in
addition to the other radiological features of the
primary pathology. Chemistry analysis of the aspirate
confirmed it to be exudative effusion in 100% of cases.
Neoplastic disease was found in 35 cases (40.7%), Pulmonary
tuberculosis in 32 cases (37.2%) and Pneumonia in 19 cases
(22.1%). The commonest cause of malignant effusion was
found to be Breast Carcinoma which was recorded in
65.7% of these. Others were soft tissue sarcoma (11%), lung
carcinoma (11.4%), intra-abdominal carcinoma (8.6%), parotid
carcinoma (2.9%). Most patients had tube thoracostomy
drainage of the effusion in addition to the treatment
of the primary disease condition. Concerning outcome of
treatment, 71% of those with malignant effusion were
dead at 6 months and indeed recorded the worst prognosis
amongst the causes of primary pathology.
The commonest complication observed during treatment was
premature dislodgement of the chest tube.
Discussion/Conclusion – Neoplastic disease was the leading
cause of surgically important pleural effusion from this
study with Breast carcinoma contributing the highest
quota. It also represents the worst prognosis as well above
2/3 of all such cases were dead at 6 months. Para-pneumonic
effusions had the best outcome as 88% of them did not show
any evidence of the disease or any complication arising
there from at 6 months re-evaluation. This may be related to
availability of appropriate antibiotics and early exhibition
of such. Tuberculous effusions had a far better prognosis
than malignant ones, but not as good as the para-
pneumonic ones.
Page 9
_____________________________________________________________________ 9
Application of diagnostic armaments and early diagnosis is
important in the eventual outcome of treatment of pleural
effusions.
INTRODUCTION.
Pleural cavity is that potential space lined by visceral and
parietal pleura and normally contains very little fluid which
is in dynamic equilibrium with the extra-cellular fluid(ECF).
Page 10
_____________________________________________________________________ 10
In certain pathological conditions, this stable dynamic
equilibrium is disrupted leading to the accumulation of fluid
in the pleural space in the form of exudates or transudates.
The diagnosis, treatment and outcome of treatment of Pleural
Fluid Collection in whichever form is determined by the
specific etiologic agent.
The objective of this study was therefore to elucidate the
Pattern of Pleural Effusion commonly encountered in our
Surgical Practice here in the National Hospital, and in
clear terms define the realistic methods of diagnosis and
therapy as well as the outcome of such.
Justification of this study was based on the fact that pleural
effusion and its associated morbidity/mortality often present
a diagnostic and therapeutic challenge in our daily surgical
practice, hence the need for a study in this direction.
Scope-This is a prospective study carried out at the National
Hospital Abuja between February 2005 to February 2006.
Exclusions-All medically related causes of pleural effusions
whose treatments hardly requires any surgical intervention.All
cases of traumatic haemothorax are excluded because alteration
of Staling forces does not really play ay role in its
formation.
Limitations of this study include, patients who decline to
participate for various reasons, relatively high cost of
medical bills which affected prompt compliance to treatment
and follow up in some patients, incessant strike action in
health institutions across the country, occasional
breakdown of vital equipment, missing case notes.
CHAPTER ONE
LITERATURE REVIEW
ANATOMY OF THE PLEURAL CAVITY
EMBRYOLOGY.
At the end of the third week of intra-uterine life, the intra-
Page 11
_____________________________________________________________________ 11
embryonic mesoderm on each side of the midline differentiates
into 3 portions; paraxial, intermediate and lateral.
Intercellular clefts appear in the lateral mesoderm and divide
it into somatic mesoderm and splanchnic layers lining the
body wall and the yolk sac wall respectively .Hence the space
bordered by these layers forms the intra-embryonic coelom
which is initially in wide communication with the extra-
embryonic coelom .But with the cranio-caudal and lateral
folding of the body of the embryo ,this communication is lost
and a large intra-embryonic cavity extending from the thoracic
region down to the pelvic region is formed 1.
The cells of the somatic mesoderm lining the intraembryonic
coelomic cavity become mesothelial and line the outside of
the pleural ,pericardial and peritoneal cavities .Similarly,
the splanchnic mesoderm form mesothelium which line visceral
layer of lungs, heart and abdominal organs. Hence, the
different origins of parietal and visceral pleura.
The septum transversum is a thick plate of mesodermal tissue
which attempts to divide the intra-embryonic coelomic cavity
into thoracic and abdominal regions, though partially, because
it leaves a large pericardio-peritoneal canal on each side2.
When the lungs expand ,the mesoderm of the body wall is split
into a definitive wall of thorax and pleuro-pericardial
membrane which contains the common cardinal vein and phrenic
nerve.With the descent of the heart, the common cardinal veins
shift towards the midline and as a result the pleuro-
pericardial membranes are drawn out like a mesentry, and
finally fuse with each other and with the root of the lungs.
Hence the thoracic cavity is divided into a definitive
pericardial cavity and two pleural cavities, while the pleuro-
pericardial membranes persist as the fibrous pericardium in
adults.
Page 12
_____________________________________________________________________ 12
The pleuro-peritoneal folds which are crescent shaped extend
from the caudal border of the pleural cavities in a medial and
ventral directions and by the seventh week of intra-uterine
life ,fuses with the mesentery of the esophagus ,as well as
the septum transversum. It is at this point that the pleural
cavities are completely separated from the abdominal cavity by
this assembly of tissues from different origin called
diaphragm. Myoblasts originating from the somatic mesoderm of
the leteral and posterior chest wall penetrate the adjacent
pleuro-peritoneal membranes to form the muscular part while
the septum transversum forms the tendinous part.
GROSS ANATOMY.
The Pleural Cavity is a potential space lying between the
chest wall, lungs and mediastinum. It is lined by a two
layered membrane called pleura. The inner Visceral layer
covers the lungs including the fissures ,while the outer
Parietal layer covers the rib cage, diaphragm and mediastinum.
The Visceral pleura is absent at the hilum of the lungs where
pulmonary vessels, bronchi and nerves enter the lung tissue.
The mediastinum separates the pleural cavity into two halves.
The pleural membranes are smooth, glistening, and semi-
transparent. Despite these similarities the two membranes have
unique differences. Visceral pleura contain no pain fibres,
and has a dual blood supply from bronchial and pulmonary
vessels, while the parietal pleura is innervated by the
intercostals nerves with blood supply from systemic
intercostals vessels. The lymphatic drainage of visceral
pleura is to the sub-pleural, intra-bronchial,tracheo-
bronchial lymph nodal chain.
PHYSIOLOGY.
Page 13
_____________________________________________________________________ 13
The pleura produces fluid which act as a lubricant which
provide a frictionless surface between the two pleurae, in
response to changes in lung volumes during respiration. The
normal pleural space contains approximately 1ml of fluid,
representing the balance between hydrostatic and oncotic
pressure in the visceral and parietal pleural vessels on one
hand and lymphatic drainage on the other[fig.1].Disruption of
this balance results in effusions.
Normally there is a continuous circulation of fluid out of the
arterial end of the capillaries into the interstitial
space/third space, then back into the venous end of the
capillaries. In order to maintain this normal circulation of
fluid across the capillary wall, a balance between the two
main forces namely hydrostatic/capillary blood pressure and
plasma oncotic pressure, operate which controls the rate and
direction of fluid movements.
Some fluid and protein enter the lymphatics before eventually
returning to the general circulation ultimately through the
thoracic duct .This may be partly the result of tissue
pressure, and partly due to osmotic attraction of proteins in
the lymphatic system 3.
Venous capillary obstruction or any increase venous pressure
far beyond 10mmHg occur in elevated pulmonary venous pressure
due to congestive cardiac failure for instance, reduces the
quantity of fluid re-absorbed at the venous end of the
capillaries, resulting in pleural fluid accumulation
containing serum protein of less than 3g%, specific gravity of
less than 1016, and LDH usually less than 200IU, features
characteristic of a transudate.
Lymphatic obstruction as in neoplastic infiltration and
Page 14
_____________________________________________________________________ 14
chronic inflammation reduces the clearance of pleural filtrate
protein load along with water and hence produces pleural fluid
collection of high protein content, >3g%,specific
gravity>1016,LDH > 200IU,features in keeping with exudates.
PLEURAL EFFUSION
INTRODUCTION.
Pleural effusion is defined as an abnormal accumulation of any
type of fluid in the pleural space, as a result of the
disruption of the haemo-dynamic equilibrium that exist across
pleural membranes namely hydrothorax, sero-pus, frank pus,
blood, chyle 4.
Pleural effusion is an indicator of a pathologic process that
may be of primary pulmonary origin, related to another organ
/system or to systemic disease. Hence it may occur in the
setting of an acute or chronic disease ,but is not a diagnosis
in itself 5.
The possible mechanisms in the formation of pleural effusions
vary with different aetiologies but usually due to:
a. Altered Permeability of the Pleural Membrane
in inflammatory process, neoplstic disease,
pulmonary embolism.
b. Reduction in intra-vascular oncotic pressure
in hypo-albuminemia ,hepatic cirrhoses, syndrome.
c. Increased Capillary Permeability or Vascular
Disruption as in trauma, neoplastic disease,
inflammatory process, pulmonary infarction,
pancreatitis, uremia.
d. Increased Capillary Hydrostatic Pressure in the
Page 15
_____________________________________________________________________ 15
systemic/pulmonary circulation as in Superior Vena
Cava Obstruction, Congestive Cardiac Failure.
e. Reduction of Intra-Pleural Pressure and inability
Of the lung to expand in atelectasis ,mesothelioma.
f. Reduced Lymphatic Drainage/Complete Lymphatic
Lymphatic Blockade which occur in thoracic duct
obstruction/rupture following malignancy,trauma.
g. Persistent Increase in Pleural Fluid Oncotic
Pressure from an existing pleural effusion causing
accumulation of further fluid.
h. Diffusion of fluid from pulmonary edema across the
visceral pleura.
Epidemiology
The approximate annual incidence pleural effusion in
the United States is 1.3 Million. Congestive Cardiac
Failure[0.5m] , Para-pneumonia[0.3m], Malignancy[0.2m],
Pulmonary Embolism [0.15] , Tuberculous effusion [0.0025]
Internationally, the relative annual incidence of pleural
effusion is estimated at 320/100000 in industrialized
countries .Elsewhere, the distribution and causes depends
on the population such as tuberculous effusions are
common in TB prevalent areas like Sub-Saharan Africa,
with its association with HIV/AIDS prevalence.
Any age can be affected though pleural effusion is commoner in
adults. Sex incidence shows equal distribution in both
sexes, however certain causes have a sex predilection.
About 2/3 of malignant effusions occur in women
Page 16
_____________________________________________________________________ 16
because of association with breast and gynecological
malignancies.6
Yellow nail syndrome is also commoner in females due to
association with systemic lupus erythematosus . It is
associated with other respiratory disorders including
chronic bronchitis, pleural effusion, chronic sinusitis .
A case of Bronchiectasis in association with Yellow
Nail Syndrome was reported in Nigeria 7.
Malignant mesothelioma with effusion is common in
males due to occupational exposure of males to
asbestos.
Sympathetic effusions secondary to pancreatic problems
are commoner in males due to higher alcohol
consumption.
Rheumatoid arthritis is commoner in males, hence its
associated effusion.
CLASSIFICATION
The classification of pleural effusion is based on the
mechanism of fluid formation and pleural fluid chemistry 8.
Generally pleural effusions are classified into Transudate or
Exudate. However ,with some causes ,there exist an overlap.9.
Transudative pleural effusions - Systemic factors that govern
formation of fluid include increased systemic and or pulmonary
capillary hydrostatic pressure(elevated pulmonary capillary
wedge pressure of (10mmHg),decreased colloid osmotic pressure
in the systemic circulation or both. Pleural membranes are
Page 17
_____________________________________________________________________ 17
intact and not involved in the pathogenesis of the fluid
formation .The permeability of the pleural capillaries to
proteins is also normal.
Exudative effusions- Local factors govern the formation of
fluid,and these include altered permeability of pleural
membranes ,increased capillary wall permeability ,vascular
disruption ,partial or complete obstruction of the lymphatic
drainage of the pleural space. Consequently, the protein
content of an exudates is high, usually >3g%.
AETIOLOGY
THE COMMON CAUSES OF EXUDATIVE EFFUSION INCLUDE;
a. Para pneumonic secondary to bacterial, fungal,
parasitic , viral , and atypical organisms like
mycoplasma, legionella, chlamydia, rickettsiae.
b. Malignancy like carcinoma, lymphoma, mesothelio
c Tuberculosis
d. Pulmonary embolism
e. Collagen Vascular disease eg rheumatoid
arthritis, systemic lupus erythematosus,
f. Asbestos related benign inflammatory exudative
pleural effusion.
g. Gastrointestinal Disease conditions causing
sympathetic effusions such as Whipple’s disease,
intra-abdominal abscess ,acute/chronic pancreatitis,
pancreatic pseudocyst.
Page 18
_____________________________________________________________________ 18
h. Trauma-blunt and penetrating injury to the chest
causing haemothorax , chylothorax.
i. Post-Cardiac Injury [Dressler Syndrome], reported
after cardiac surgery, pacemaker insertion,
myocardial infarction, angioplasty, blunt
chest trauma.
j. Esophageal perforation during endoscopy
k. Drug induced primary pleural disease
Eg. nitrofurantoin, dantrolene, methysergide,
bromocriptine, amiodarone, methotrexate, oxprenolol,
practolol, minoxidil, mitomycin.
l. Meig’s Syndrome
m. Sarcoidosis
THE COMMON CAUSES OF TRANSUDATIVE EFFUSION INCLUDE;
a. Congestive Heart Failure
b. Cirrhoses[hepatic hydrothorax]
c. Atelectasis [ which may be secondary to malignancy
or pulmonary embolism]
d. Hypo albuminaemia
e. Nephrotic Syndrome
f. Peritoneal Dialysis
g. Myxedema
h. Constrictive Pericarditis
i. Superior Vena Cava obstruction
SOME CAUSES RESPONSIBLE FOR COMBINED
EXUDATIVE/TRANSUDATIVE PLEURAL EFFUSION INCLUDE:-
Page 19
_____________________________________________________________________ 19
a. Pulmonary embolism
b. Hypothyroidism
c. Diuresed Transudate,
d. Long Standing Transudate
e. Pericardial Disease [inflammatory,constrictive]
f. Atelectasis , amyloidosis, sarcoidosis
Despite the myriad of causes of pleural effusion
enumerated above ,by far the commonest causes include
congestive cardiac failure, pneumonias, tuberculosis,
malignancy, pulmonary embolism.
Other rarer causes of pleural effusion have been reported.
“Thoracic endometriosis was reported in a 34 year old
Ugandan female complaining of recurrent right sided chest
pain, with clinical and radiological evidence of right
sided pleural effusion 15. Subsequent management via CT
chest, chest tube drainage ,and thoracotomy confirmed
endometriosis which responded to the usual hormonal
treatment.
A case of massive hemorrhagic ascites and pleural
effusion caused by endometriosis was also reported in
Lagos , Nigeria. 16.
Pleural deposits from light chain myeloma has been
reported as another cause of pleural effusion 17
PATHOPHYSIOLOGY
Various mediators are involved in the production of
altered permeability and the evolution of pleural
effusion.
Page 20
_____________________________________________________________________ 20
Types of pleural effusion include hydrothorax, chylothorax,
malignant effusion, parapneumonic effusion, empyema etc. In
addition to the pathophysiologic effect of the primary
disease, pleural effusions share a common effect on
the physiological derangements of the pulmomary system.
Pleural effusion produces a restrictive defect that is
correlated with the size of the effusion. Because ,
both the air spaces and the pulmonary circulation
are compressed and because of pulmonary hypoxic
vasoconstriction , there is little shunting and only
mild hypoxaemia. In addition to lung parenchymal
compression, massive effusions pushes the mediastinum
to the contralateral side further compromising the
cardio-pulmonary function. Ventilation-perfusion mismatch
occurs, hence, tachycardia and dyspnoea are the commonest
symptoms. The accumulation of fluid in the alveoli
may occure and that predisposes to irritation of the
alveolar wall resulting in cough which is initially
dry. Tissue devitalization in chronic lung parenchymal
diseases eg pulmonary tuberculosis, malignancies, etc
predisposes the alveolar capillaries to rupture during
cough episodes resulting in occasional haemoptysis.
Pleural inflammation and metastatic deposits cause
pleuritic chest pains which decreases in intensity
as the effusion increases in size.
Removal of a large effusion can result in modest
improvement in lung function, but often, the underlying
cause of the effusion eg malignant effusion, causes
persistent functional abnormalities.
The accumulation of fluid in the hemithorax impairs the normal chest excursion and
Page 21
_____________________________________________________________________ 21
is responsible for the stony dullness to percussion in place of resonant note of a
hemithorax containing a fully expanded lung.
TYPES OF EXUDATIVE PLEURAL EFFUSION:
Chyliform/Pseudochylous Effusion grossly resemble frank
chylothorax .However ,the pathogenesis does not involve the
thoracic duct or indeed any lymphatic drainage system ,and it
does not contain any chylomicrons .It occurs in long standing
(mean 5 years) pleural effusions associated with Rheumatoid
arthritis ,tuberculosis ,paragonimiasis infestation . The
milky white appearance is due to the high lipid levels i.e
cholesterol crystals or lecithin-globulin complexes.10.
Malignant Pleural effusion is usually an exudate and caused
by a neoplastic disease. It accounts for 13-40% all pleural
effusions in the United States. Pleural effusion develops in
nearly 50% of patients with metastatic cancer. The most common
tumours that cause malignant pleural effusion include
adenocarcinomas and other carcinomas of the lungs, breast
cancer, lymphoma, leukaemia, accounting for about 75% of all
malignant pleural effusions .Others include ovarian carcinoma,
stomach cancer ,sarcomas and malignant melanoma. It is
usually caused by a disturbance of the normal Starling
forces regulating the re-absorption of fluid in the
pleural space, via obstruction of mediastinal lymphatics
draining the parietal pleura. Hence tumours that
metastize most frequently to these nodes such as lung
cancer, breast cancer cause most malignant effusions.
Whereas the effusion restricts ventilation, the pleural
deposits of tumour cause pleuritic chest pain.
Lymphangitic pulmonary metastases further worsen pulmonary
function. The primary lesion may also have disseminated
Page 22
_____________________________________________________________________ 22
to other sites such as bone, brain, further debilitating
the patient.
Fig. 1. Chest Radiographs showing massive left sided
pleural effusion and marked mediastinal shift before(A) and
after(B) tube thoracostomy drainage.
Para-pneumonic effusions complicate bacterial pneumonias .In
the United States of America,30-40% of patients with bacterial
pneumonias develop pleural effusion in-spite of their advanced
medicare .It therefore implies that the incidence of this
complication is much higher in underdeveloped third world with
the ravaging malnutrition ,poverty, HIV/AIDS, and poor access
to medicare. Streptococcus Pneumonia has a high predilection
for complications eg bacteremia ,multi-lobar involvement, and
pleural effusion. It is important to understand the
pathophysiology of parapneumonic effusions.It is most often
associated with pneumonia, particularly aspiration events
with anaerobes. But, generally, aerobic infections are
commoner than anaerobic. Similarly, gram- positive aerobic
pneumonic infections is about twice commoner than gram
negative aerobes. Commonly implicated gram positive
aerobes include Stphylococcus aureus and Streptococcus
pneumonia in about 70% of cases11.
Then, the gram negative aerobes which include
Page 23
_____________________________________________________________________ 23
Klebsiella, Pseudomonas, and Haemophilus species. Commonly
encountered anaerobes include Bacteroides and
peptostreptococcus species. Mixed infections do occur
sometimes in which case it is more likely to progress
to empyema . Mycobacterium tuberculosis is the commonest
cause of chronic granulomatous infection/inflammation of
the lung parenchyma and associated lymph nodes.
Following an overwhelmed host defence mechanisms, lung
tissue responds by inflammation, which can produce
tissue necrosis as in S.aureus infection , impair ciliary
action and impede phagocytosis. Inflammation may cause
exudation of fluid into the pleural space. Pleural effusion
evolves in three phases. The initial phase is the
accumulation of small but sterile fluid caused by the
infection contagious to the pleural space. Intersticial
fluid increases during pneumonic process and accumulates
in the pleural space because of increased permeability
of the interstitium as well as exceeded absorptive
capacity of the pleural space. Effusion here is
neutrophilic, with low white cell count and LDH but
normal glucose and Ph. Fortunately many para-pneumonic
effusions do not progress beyond this stage and
resolve as the pneumonia is treated, because antibiotic
penetration of the space is very good. The second
stage occurs if bacteria and polymorphs enter the
pleural space .The inflammatory response causes fibrin
to be deposited along the visceral and parietal pleura
that can lead to loculation. In association with this
is a significant rise in pleural fluid LDH level [.1000],
while the pH [.7.2] and glucose [.60mg/dl] levels fall.
The third stage occurs if the fluid is not drained
as fibroblasts move in organizing the fluid into a
pleural peel, making removal of fluid by a needle
Page 24
_____________________________________________________________________ 24
aspiration impossible. This pleural fluid will encase
or trap the lung permanently, impairing its ability to
function. If it is still infected, it will act as
an abscess .This abscess can drain spontaneously through
the chest wall as empyema neccesitans, or disastrously
into a bronchus forming a life threatening broncho-
pleural fistula. Hence para-pneumonic effusions can be
classified into uncomplicated effusion[exudative stage],
complicated effusion[fibrino-purulent stage], and thoracic
empyema[organization stage].
Chest trama especially penetrating and chest surgery
may also be associated with super-infection in the
pleural space. Infection via haematogenous spread or
direct contact is also possible as in subdiaphragmatic
abscess, ruptured esophagus, mediastinitis, osteomyelitis,
pericarditis, cholangitis.
Tuberculous Pleural Effusion. Mycobacterim tuberculosis is
the commonest cause chronic grnulomatous lung parenchymal
disease,which often is complicated by pleural effusion.
Effusion is usually preceeded by tuberculous pleuritis which
should be suspected in patients with history of exposure to
or mantaux positive findings. Most tuberculous effusions
result from a hypersensitivity reaction o involving the
pleural membrane and capillaries to the mycobacterium rather
than microbial invasion of the pleura, and this is
responsible for the very low yield of acid-fast bacilli in
pleural fluid analysis.
Empyema Thoracis means suppurative fluid collection in the
pleural cavity. In the pediatric age group, para-pneumonic
effusions is the most frequent etiology for empyema 12 .It is
often due to an inflammatory process in adjacent
Page 25
_____________________________________________________________________ 25
structures as occurs in pneumonia ,lung abscess,
,tuberculosis etc .Underlying carcinoma of the bronchus must
be suspected in any
patient over the age of 45 years presenting with pleural
effusion/empyema13. Other causes of empyema thoracis are
ruptured sub-phrenic abscess, ruptured amoebic abscess,
osteomyelitis of the spine/ribs, esophageal perforation, and
unguided instrumentation of the pleural cavity such as
aseptic pleural fluid drainage.
Pathogenesis of empyema involves an initial generalized
pleural infection and thin inflammatory exudates. It
later becomes more localized with the development of
thick pleural adhesions due to fibrin content and
thickening of the pus. The empyema may either resolve
spontaneously , rupture into the lung parenchyma, with
a resultant broncho-pleural fistula, or become chronic
with marked thickening of the pleurae and an
intervening cheesy pus akin to bread and butter
appearance. The resultant effect is restricted chest
movement, crowding of the ribs and concave scoliosis
to the affected side. It has been known that
streptococcal infection produces thin pus whereas
pneumococcus produces thick pus with a high fibrin
content of the inflammatory exudates. But with the
advent of antibiotics being used routinely in most
chest infections ,most empyema are sterile at initial
diagnosis. Indeed the advent of modern chemotherapy has
radically altered the natural history of an empyema
and has abolished the different types of empyema due
to different organisms.14. Empyema thoracis is suspected
by observing a slow rate of symptomatic improvement in
a patients general condition after chest infection and
suspicion is heightened by the typical radiographic
Page 26
_____________________________________________________________________ 26
features. Comfirmation of diagnosis is by aspiration of
pus with a wide bore needle such as 14G. Culture may
not be positive, though not surprising.
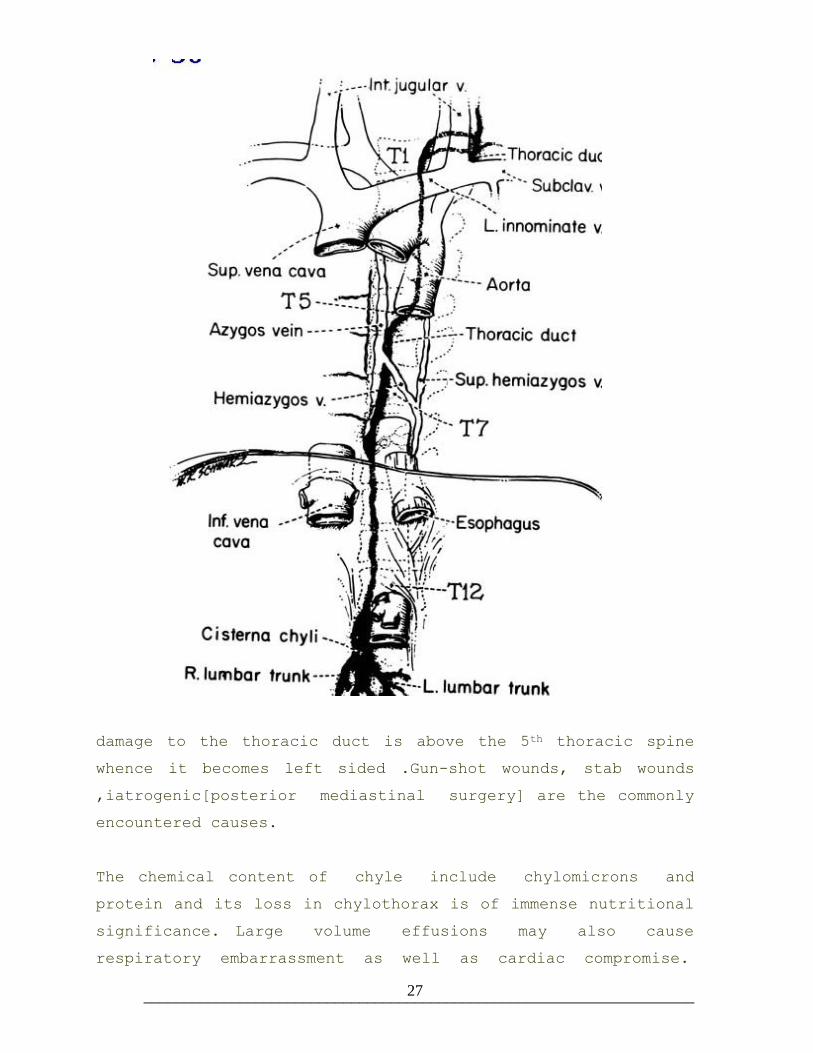
Chylothorax means the accumulation of chyle in the pleural
cavity .It is most commonly caused by trauma or tumor with
rupture of the thoracic duct anywhere along its course[Fig
2]. Chylothorax is usually right sided except if the
Fig.2.-Course of the thoracic duct.
The confluence of the right and left lumbar
lymphatic trunks forms the cisterna chyli which
lies on the anterior body of first lumbar
vertebra. It ascends into the posterior mediastinum to
become the thoracic duct by passing through the
diaphragm at the level of twelfth thoracic
vertebra. The thoracic duct remains on the left side
of the posterior medistinum until it ascends to the
seventh to fifth thoracic vertebra where it crosses
over to the right side where it continues its
journey towards its termination at the root of the
neck in the junction between the right subclavian and
right internal jugular veins. It can therefore be
damaged at any point in this long tortuous pathway.
Page 27
_____________________________________________________________________ 27
damage to the thoracic duct is above the 5th thoracic spine
whence it becomes left sided .Gun-shot wounds, stab wounds
,iatrogenic[posterior mediastinal surgery] are the commonly
encountered causes.
The chemical content of chyle include chylomicrons and
protein and its loss in chylothorax is of immense nutritional
significance. Large volume effusions may also cause
respiratory embarrassment as well as cardiac compromise.
Page 28
_____________________________________________________________________ 28
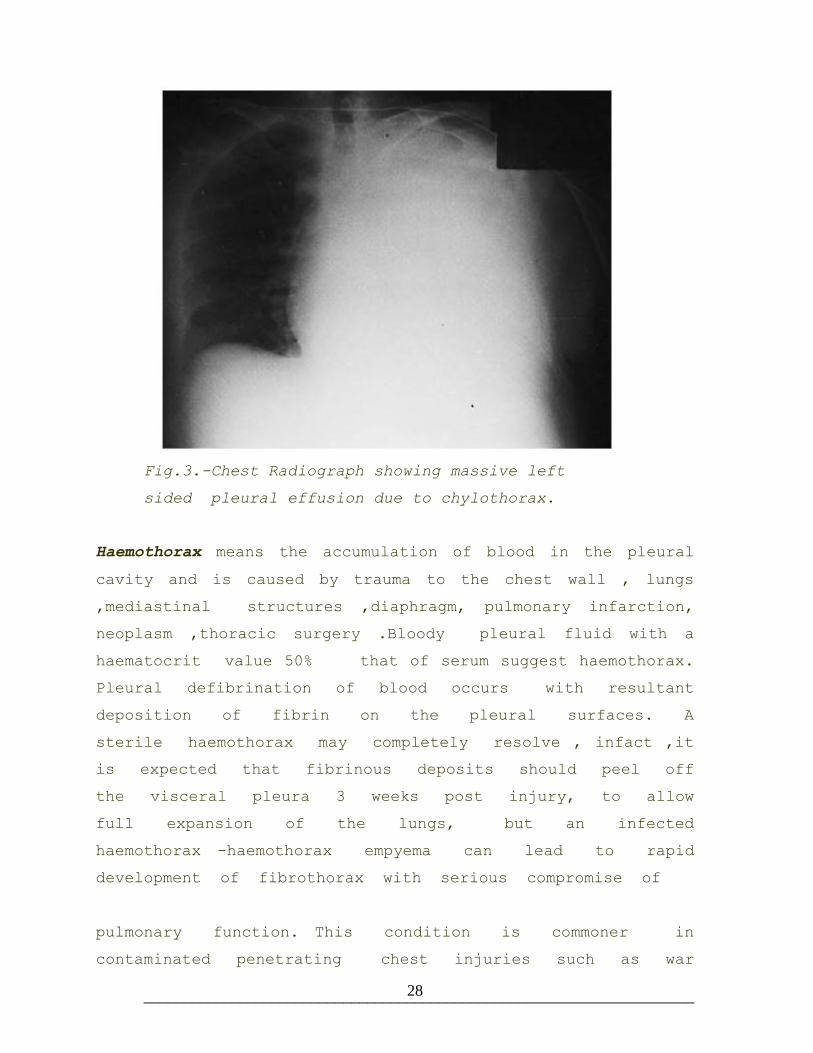
Fig.3.-Chest Radiograph showing massive left
sided pleural effusion due to chylothorax.
Haemothorax means the accumulation of blood in the pleural
cavity and is caused by trauma to the chest wall , lungs
,mediastinal structures ,diaphragm, pulmonary infarction,
neoplasm ,thoracic surgery .Bloody pleural fluid with a
haematocrit value 50% that of serum suggest haemothorax.
Pleural defibrination of blood occurs with resultant
deposition of fibrin on the pleural surfaces. A
sterile haemothorax may completely resolve , infact ,it
is expected that fibrinous deposits should peel off
the visceral pleura 3 weeks post injury, to allow
full expansion of the lungs, but an infected
haemothorax -haemothorax empyema can lead to rapid
development of fibrothorax with serious compromise of
pulmonary function. This condition is commoner in
contaminated penetrating chest injuries such as war
Page 29
_____________________________________________________________________ 29
and gun-shot injuries especially when associated with
underlying lung injury. Conversely, it is less common
following clean stab injuries to the chest, and
expectedly commoner in haemo-pneumothorax than in pure
haemothorax.
Pleural cavity has the capacity to contain large
volumes of fluid /blood. In rapid bleeding into the
pleural cavity, large blood clots may occure, thus
setting the stage for a possible an imprisoning
fibrothorax later . But in slow bleed into the pleural
cavity, blood in the pleural space tends to be
defibrogenated and slow to clot. Hence auto-transfusion
can be practiced by means of a cell saver or
manually collecting the blood in a sterile drainage
system , adequate filtration and re-infusion into the
patient.
Third space loss of blood into the pleural cavity
poses a potential threat to the cardiovascular
stability of the patient, and shock may result. In
addition lung is compressed and medistinum is displaced
to the contralateral hemithorax., further compromising
both the respiratory and cardiac function. The critical
factor in this condition is tissue anoxia therefore
such patients require prompt intervention.
CLINICAL FEATURES OF PLEURAL EFFUSION.
The clinical manifestations of pleural effusion are
variable and often related to the underlying cause ,
however the commonly associated symptoms are dyspnoea ,
cough, chest pain.
Dyspnoea indicates a large effusion but usually not
Page 30
_____________________________________________________________________ 30
less than 500mls. However other factors such as
underlying lung disease, cardiac dysfunction , anaemia
may contribute. It is the most common clinical presentation
of pleural effusion. 18.
Chest Pain is typically described as sharp, biting,
pleuritic. It signifies pleural irritation. It may be
localized to the chest wall or referred to the
ipsilateral shoulder or upper abdomen if diaphragm is
involved in the disease process.The pain diminishes as
the size of the effusion increases.
Cough may be non productive and is due to irritation
of the alveoli by some fluid that may accumulate
therein. It may also be productive and may even be
associated with haemoptysis especially in lung
parenchymal diseases such as tuberculosis , lung
carcinoma .
Fever of acute onset associated with chest pain,
sputum production and leukocytosis which persists after
48 hours of initiation of antibiotic treatment
complicated by dyspnoea and dullness to percussion in
the affected hemithorax is suggestive of a para-
pneumonic effusion
Other signs and symptoms are pointers to the
underlying disease process. Pedal edema , orthopnea,
paroxysmal nocturnal dyspnea ,cough productive of frothy
sputum occure in congestive cardiac failure . Haemoptysis
, night sweats, malaise, low grade fever , weight loss
occure in pulmonary tuberculosis. An acute febrile
episode , purulent sputum , pleuritic chest pain , occure
in aerobic bacterial pneumonias .
Page 31
_____________________________________________________________________ 31
Physical Findings are equally variable but depends on
the volume of the pleural effusion. If the volume of
the effusion is less than 300mls,it may not be
clinically detectable .Otherwise the features are:-
-Elevated body temperature in para-pneumonic
Effusions
-Diminished chest excursion on the affected
hemithorax - Hoover’s sign
-Dullness to percussion on the affected hemithorax.
-Reduced tactile fremitus on the affected
hemithorax.
-Tracheal deviation to the contralateral side
signifies medistinal shift which is observed in
large volume effusions 1000mls. Ipsilateral
deviation may occure in obstruction of a lobar
bronchus by endobronchial tumour or less commonly
a foreign body 18.
-Diminished / inaudible breath sounds
-Pleural friction rub
-Egophony [‘e’ to ‘ a’ changes] at the most
superior aspect of effusion.
Other important physical findings that provide clues to
the cause pleural effusion include anasarca in
nephritic syndrome and hypoproteinemia ; cutanous
Page 32
_____________________________________________________________________ 32
changes in liver diseases; distended neck veins , S3
gallop rhythm in congestive cardiac failure; breast
nodule, intra –abdominal mass , pelvic mass may suggest
malignant effusion.
LABORATORY INVESTIGATIONS.
Pleural fluid analysis – Thoracocentasis is done through
a selected intercostals space with a 23G needle to
sample at least 20mls of pleural fluid.
Fig.4. Thoracocentasis.
The initial step is to examine the physical
characteristics of the sampled fluid as follows:-
a. Bloody Fluids- possible causes include,
-Malignancy
-Chest Trauma
-Pulmonary Embolism
-Tuberculosis
-Infection
-Mesothelioma
Page 33
_____________________________________________________________________ 33
b. Turbid Fluids- possible causes include,
-Increased cellular content as occurs
in inflammatory exudates
-Increased lipid content lipid content
c. Yellow/Whitish Turbid- possible causes include;
-Chyle
-Cholesterol
-Empyema
d. [Chcolate/ anchovy sauce] , found in:-
-Ruptured amebic liver abscess into the
pleural space[hepato-pleural fistula]
e. Black fluid, found in,
Aspergillus involvement of pleura
f. Yellow Green fluid with debris, found in
Rheumatoid pleurisy
g. Highly viscous - suggest, malignant mesothelioma
[hyaluronic acid]
h. Putrid odour- suggests
anaerobic pleural space infection
I Ammonia odour suggests,
Urinothorax
j. Purulent effusion suggest
Para-pneumonic effusion which may progress to
empyema thoracis
Page 34
_____________________________________________________________________ 34
k. Yellow thick metallic sheen found in,
-long standing chyliform effusion.
CHEMICAL ANALYSIS
Initial chemical analysis of the following parameters
is mandatory; serum protein, serum LDH, pleural fluid
protein content, pleural fluid LDH.
TOTAL PROTEIN LEVELS AND DIFFERENTIALS
Pleural fluid is an exudates if one or more of the
following condition is met; ratio of pleural fluid protein
to serum level greater than 0.5 or ratio of pleural
fluid LDH to serum LDH level greater than 0.6, except
in transudative effusions caused by congestive cardiac
failure when the patient had undergone diuretic therapy
for more than 48hrs. This air can be cleared by the
use serum albumin/pleural fluid albumin ratio whereby a
gradient greater than 1.2 suggest exudates while below
1.2 suggest transudate 20.
Light’s criteria further suggests that a pleural fluid
LDH concentration greater than 2/3 of the upper limit
of normal serum reference range is most likely an
exudates.”21. It further states that if only one test
is to be performed , measurement of the total
protein concentration is the most practical in view
of its accuracy and availability.
Glucoselevel. Low levels [<60mg/dl] suggest tuberculosis,
malignancy, parapneumonic effusion, empyema , haemothorax .
LDH level is directly proportional to the degree of
inflammation, and levels greater than 1000iu/l is
Page 35
_____________________________________________________________________ 35
found in parapneumonic effusion, paragonimiasis.
Amylase level. 1000 Somogyi units or pleural/serum amylase
ratio1.1 signifys a sympathetic effusion secondary to
acute pancreatitis pseudopancreatic cyst esophageal
rupture malignancy ruptured ectopic pregnancy. Assay of
pancreatic and salivary isoenzymes helps to further
narrow the diagnosis.
pH estimation , if 7.2 suggest empyema , complicated
parapneumonia , esophageal rupture , malignancy ,
paragonimiasis , tuberculosis. Worthy of note is that
pleural fluid pH is influenced by the level of
acidemia.
Cytologic analysis is strongly recommended for patients
withe a history of undiagnosed effusion, suspected
malignancy, pneumocystis carinii infection, exudative
effusion normal fluid glucose/amylase levels.
Blood Culture is necessary if the pneumonic process is
suspected to be part of a septisemic process.
Gram Staining,culture and sensitivity. Bacilli staining
with Zeil –Neelson stain, Fungal staining with potassium
hydroxide, culturing and sensitivity for aerobic /
anaerobic organisms and fungi are essential if
facilities permit.
Lipid estimation is mandatory when a milky fluid is
encountered. Triglycerides, Cholesterol, and total lipids are
estimated. The presence of chylomicrons in the fluid
confirms chylothorax while its absence in a milky fluid
confirms pseudo-chylothorax.
Page 36
_____________________________________________________________________ 36
Pleural fluid creatinine /serum creatinine is done when
an effusion with an ammoniacal odour is encountered. A
ratio of greater than 1 confirms urinothorax.
Pleural fluid Haematocrit is done if a bloody pleural
fluid is encountered. When compared with serum
haematocrit and found to be greater than 50%
,haemothorax is comfirmed
CELL COUNT AND DIFFERENTIALS
a. Red Blood Cell [RBC] count > 100,000/mm3
suggest trauma, malignancy, pulmonary embolism,
post-surgery.
b. White Blood Cell [WBC] count > 10,000/mm3 suggest
parapneumonia Relative neutrophilia suggest
acute inflammatory process while eosinophilia
Suggest associated pneumothorax, haemothorax,
pulmonary infarction or Parasitic infestation
such as paragonimiasis . Pleural fluid
esinophilia commonly indicate benign disease and
a favourable prognosis when it is present in
any malignant effusion.22. Basophilia of > 10%
though uncommon indicates leukaemic infiltration.
Lymphocytic count in excess of 50% indicates
long standing chronic pleural effusion
particularly malignant disease eg lymphoma , or
tuberculosis, sarcoidosis, chylothorax. Plasma
cells suggest multiple myeloma while macrophages
suggest chronic granulomatous inflammatory
conditions.
Page 37
_____________________________________________________________________ 37
c. Mesothelial cells are commonly exfoliated into
the thin pleural fluid and should not be
confused with malignant cells in view of
their histological similarities, therefore it is
the absence and not the presence that is
significant in conditions where there is
fibrosis or infiltration of the pleural surfaces
as in tuberculous effusion, empyema thoracis.
Note that the reproducibility of these test results
depends on the appropriateness of the sampling bottles.
This is discussed in more details in Chapter 2.
IMAGING STUDIES
Chest Radiograph. - Confirms the effusion as well as
helping to determine the cause of the effusion. Enlarged
cardiac silhoette, underlying lung parenchymal disease,
mediastinal shift etc when present are quite obvious.
The most common radiologic feature of pleural effusion
is the blunting of costophrenic angle and the classical
meniscus sign which occurs in advanced cases. Other
features include:-
-Generalized homogenous opacity below the meniscus
-Diffuse haziness as the fluid extends posteriorly
[ground glass appearance]
-Mediastinal shift Visibility of pulmonary vessels through
the haziness
-Absence of air bronchogram
-Obliteration of diaphragmatic silhouette
Page 38
_____________________________________________________________________ 38
-Reduced visibility of lower lobe vasculature
-Widened minor fissure
-Apical capping
-Hemidiaphragmatic inversion due to weight of fluid
Noteworthy is that the usual upright postero- anterior [P-A]
view or antero-posterior [A-P] view may not show
the lateral costophrenic angle blunting until 250-
500mls of fluid has accumulated, but a lateral view
will show costophrenic angle blunting even with as
little as 175-200mls. Hence the need for additional
views. Decubitus views especially bilateral is very
useful in large effusions as hemi-diaphragmatic
elevation suggest sub-pulmonic effusion, it helps to
exclude a loculated effusion and may equally expose
an underlying pulmonary lesion .Characteristically a
decubitus view shows layering of fluid. 1cm layer
approximates 200mls of fluid 23.Supine view is only
employed in sick patients who are confined in a
recumbent position .
Fig.5.-Chest Radiographs Showing right sided empyema
Page 39
_____________________________________________________________________ 39
cavity and left sided massive pleural effusion.
INTERPRETATION OF RADIOLOGICAL FINDINGS:
Bilateral pleural effusion in the absence of
congestive cardiac failure is commonly caused by
malignancy except for lung and breast carcinoma. Breast
carcinoma associated pleural effusion are typically
ipsilateral to the primary breast carcinoma in 58-70%
of cases, however 20 –26% of cases develop in the
contralateral side, while 10-16% develop bilateral
effusion 24. Other possible causes are nephritic
syndrome , pulmonary embolism , tuberculosis, esophageal
rupture , Meig’s syndrome.
Massive effusions are commonly malignant in 70% of cases.
Other possibilities include congestive cardiac failure ,
tuberculosis , liver cirrhoses , transdiaphragmatic rupture
of huge liver abscess, paragonimiasis, pancreatic
pseudocyst, Meig’s syndrome. Massive effusion is often
accompanied by mediastinal shift. If not or if shifted the
ipsilateral side it suggests narrowing of ipsilateral
mainstream bronchus probably due to carcinoma .It may
also be due to atelectasis, or fixation of the
mediastinum due to fibrosis of chronic inflammation or
tumour infiltration of the mediastinal nodes of
ipsilateral lungs.
The localization of the fluid also provide diagnostic
clues eg isolated right sided effusion occure in
cirrhoses , sub-phrenic/liver abscess, hydatid disease of
the liver, Meig’s syndrome, endometriosis while left
sided effusion points to esophageal rupture pancreatic
disease left sub-phrenic , transdiaphragmatic rupture of
Page 40
_____________________________________________________________________ 40
splenic abscess.
Atypical radiologic presentations include sub pulmonic
effusions typical of nephrotic syndrome.
Fig .6.- Chest RadiographS showing a homogenous opacity
on the right hemithorax(A) and meniscus sign on the right
hemithorax(B)
ULTRASONOGRAPHY-
Can detect as low as 50mls of pleural fluid.
It is rapid and available at bedside
It can identify a loculated / encysted effusion
It can also differentiated pleural fibrosis thickening and
parenchymal consolidation
COMPUTERISED TOMOGRAPHIC SCANNING [C-T SCAN]
Permits simultaneous imaging of the entire pleural
space, lung parenchyma, and mediastinum, as well as
the lesion contained therein, and the anatomical
relationships.
Page 41
_____________________________________________________________________ 41
Fig.7. C-T scan of the chest showing right sided empyema
thoracis.
MAGNETIC RESONANCE IMAGING [MRI]
MRI has a limited role , but it is useful and better
than C-T SCAN in depicting tumour extension to the
chest wall , brachial vessels, subclavian vessels,
vertebral bodies, and spinal canal.
NUCLEAR IMAGING
With gallium labeled leukocytes is occasionally employed
to rule out lung parenchymal infection
CONTRAST ENHANCED STUDY OF ESOPHAGUS
This can be done with the patient in a lateral
decubitus position .A water soluble contrast agent like
hexabrix is preferred for this test and is useful in
investigating for esophageal perforation.
VENTILATION – PERFUSION SCANNING [V-P SCAN]
This test is mandatory if pulmonary embolism is
suspected, but the associated pleural effusion should
first be drained so that it does not affect the
interpretation of the result.
Page 42
_____________________________________________________________________ 42
MANAGEMENT OF PLEURAL EFFUSION
COMMON PROCEDURES;
1. Thoracocentasis- This is the first line and least
invasive of all diagnostic procedures. It may also be
therapeutic and relatively safe. An appropriate sized needle
is placed into the appropriate intercostals space to sample
the fluid.
2. Tube Thoracostomy- The placement of a thoracostomy
into a designated intercostals space usually suffice for
evaluation and treatment of most pleural fluid
collection.
3. Per-cutanous Biopsy- This is a non invasive method
employed to biopsy pleural , lung parenchymal or
mediastinal lesions, with accuracy enhanced by image
guidance.
4. Open Biopsy- Involves at least a mini-thoracotomy such
that a visual assessment of the lesion and the extent
can equally be made.
5. Thoracoscopy/Biopsy-Allows an endoscopic assessment of
pleural cavity and mediastinum and enhances accuracy of
biopsy ,through a minimally invasive approach.
6. Other Ancillary Procedures like bronchoscopy, perfusion
lung scanning, pulmonary arteriography are complementary.
TREATMENT OF PLEURAL EFFUSION
Pre-hospital care- involves recognition of the cardio-
pulmonary instability in such patients and taking
prompt measures aimed at initial resuscitation in
Page 43
_____________________________________________________________________ 43
line with standard principles of basic life
support(BLS), while making prompt arrangements to
evacuate such patients to a well set emergency
department outfit.
Emergency Room Care- Based on the presentation, the
patient is classified into three:-
1. stable patient , not requiring hospital admission
2. stable patient , but requires hospital admission
3. unstable patient, requires immediate intervention
Stable patients include pleural effusion secondary to
viral pleurisy, free fluid thinner than 10mm on a
lateral decubitus , asymptomatic effusion secondary to
medical conditions like Congestive Heart Failure, Renal
Disease, Liver Cirrhoses and also any post surgical
effusion thinner than 10mm. Such patients need no
admission , but must be re-evaluated 2-3 days later
while on medication for the primary disease, and if
the effusion is worsening, thoracocentasis for fluid
analysis is indicated.
Stable patients requiring admission have an effusion
more than 10mm thickness on decubitus view. Such include
parapneumonic effusions with no toxic features, recurrent
effusions with a change in symptomatology. Admission is
for further evaluation via diagnostic thoracocentasis. Para
pneumonic effusions should be promptly treated with
antibiotics because of the tendency to complications
such as empyema thoracis even before any invasive
procedures.
Unstable patients are toxic with cardio- pulmonary
Page 44
_____________________________________________________________________ 44
instability as in life threatening traumatic or medical
conditions, hydropneumothorax, massive effusion with
mediastinal shift, ruptured thoracic duct, esophageal
perforation.
Such patients are made to sit up so as to increase
tidal volume and reduce work of breathing. Then an
immediate diagnostic/therapeutic thoracocentasis is done.
Chest tube placement with tube directed postero-
inferiorly for liquids and superiorly for air. Traumatic
Haemothorax and Empyema Thoracis requires large bore
thoracic catheter size 34-40F.
Radiographs play an essential role in the management
of pleural effusion. However, in very unstable and
severely distressed patients, in the emergency department
thoracocentasis and thoracostomy tube insertion play a
leading role in stabilizing such patients , while
radiographs is reserved for monitoring. Note that
critically distressed patients have been lost in the
radiograph bukky because this simple rule was
neglected.
In view of the possibility of an evolving pathology
especially in chest trauma, a repeat chest radiograph
should be obtained 3-6hrs later.
The need to evaluate the the patient from head to toe
cannot be overemphasized because it helps to address
other life threatening conditions.
When the patient is stabilized, continued management in
the ward involves accurate diagnosis, as per the cause
of the cause and treatments channeled to that. Medical
Page 45
_____________________________________________________________________ 45
cases are referred accordingly, while surgical patients
are managed accordingly.
This research mainly focuses on surgically related
pleural effusion, where procedures like thoracocentasis,
thoracostomy, ribresection , thoracotomy, pleurodesis, are
fairly routine procedures.
The commonest procedure in the management of pleural
effusion are thoracocentasis, tube thoracostomy, and
pleurodesis.
Thoracocentasis can be done in the emergency unit,
consulting room, or in the ward with local anasthetic
infiltration on the appropriate intercostals space.21g
needle is then inserted and directed through the upper
border of the rib of the selected intercostals space
to sample the fluid, which is sent for analysis.
Chest tube is inserted by asking the patient to sit
on a chair , edge of the bed, or lying at 45 degrees
on the bed. Intercostal space , usually the 5th
intercostals space in the mid axillary line is selected
because it can afford an easy and safe access to the
pleural space for the drainage of both liquid and
air. It is infiltrated with 1% xylocaine. Incision is
made through skin, subcutaneous plane, and intercostals
muscles parted, staying very close to the upper border
of the adjacent rib.
Page 46
_____________________________________________________________________ 46
Fig.8. Diagramatic illustration of dissection through an
intercostal space during tube thoracostomy.
On breaching the parietal pleura a gush of fluid is
is noted ,which may require an indwelling thoracic
catheter retained for a couple of days to ensure a
smother and complete drainage and usually connected to
an underwater seal drainage system to eliminate the
leakage of air into the pleural cavity. The area of
skin incision is neatly sutured, purse string placed
and then dressed. Patient may be given some
analgesics and antibiotic. The chest tube is connected
to a closed pleural drainage system which ranges from
simple to the very complex depending on the specific
clinical problem. A sound understanding of the
principles of the chest drainage system by both the
attending physician and nursing staff is of primary
importance and time spent communicating this to the
understanding of the attending nursing staff is well
spent. 25. When little or no continuing air leakage is
expected, and only liquid drainage is expected, a
simple underwater seal drainage system or a rubber
flutter valve with a plastic bag arrangement is
adequate. [fig.9].
Page 47
_____________________________________________________________________ 47
Fig.9. Diagramatic illustration of a patient with right
sided tube-thoracostomy with underwater seal connection.
From Ibadan Nigeria, Adebo et al reported that their
preferred method of chest drainage in traumatic
haemothorax consist of insertion under anaesthesia of
the tubular end of of an Aldon`s Urobag equivalent
to number 34 Argyle chest tube, beveled, multifenestrated
and placed within the 5th or 6th intercostals space in
the mid - axillary line.26. It is also important to
note that some previous study has confirmed the
efficacy of this valved system in the evacuation of
fluid and or air from the pleural space.27. In the
past a two bottle system with the first being a dry
tap provides separate reservoir for collection of
fluid, then the second bottle which contains the
underwater seal specification, but this arrangement
added to the dead space between the pleural space and
the water seal surface. When large air leaks are
expected , large glass bottles with rubber stoppers and
glass tubes have been replaced by compact plastic
Page 48
_____________________________________________________________________ 48
drainage that require less space and are unlikely to
be damaged and may be used as a simple underwater
seal or attached to a vacuum source. The three
compartment system comprises a collection chamber ,
water seal , and vacuum regulator with a long tube
open to the air and extending under the water level.
Pumps with a low air flow capacity should not be used
when large air leaks either continous or intermittent
is expected. The drainage system should function to
prevent ingress of air into the pleural cavity, even
when the vacuum apparatus fails, also the system should
allow egress of large volume of air suddenly, whether
the vacuum system is functioning or not. Needless to
mention , the drainage bottles should be placed at a
level below the chest always even when the patient
being wheeled to other parts of the hospital.
The correct placement and completeness of drainage are
both comfirmed on chest radiographs .Complete re-
expansion of the lungs is an indication for removal
of the chest tube, during which the purse string is
neatly tied to forestall the leakage of air into the
pleural cavity.
Large effusions are drained in aliquots of say
500mls every 4hours,so as to avert the development of
pulmonary edema, a potentially fatal condition that
may complicate drainage of massive effusions in one
swoop Some patients may experience violent cough which
may result in rupture of some fragile blood vessels
in the lung parenchyma such that an initially non
haemorrhagic effusion becomes so and patient may also
develop haemoptysis. A sudden release of pressure in
the chest can also cause a drop blood pressure.28.
Page 49
_____________________________________________________________________ 49
Treatment of Parapneumonic Effusion. For community acquired
pneumonia, a 2nd or 3rd generation cephalosporin and a
macrolide antibiotic is quite effective. In severe
community-acquired pneumonia and hospitalized patients, a
3rd generation cephalosporin with antipseudomonal activity
and a macrolide is preferred. Parenteral route is
preferred and is continued until afebrile for 7-10 days
then continued orally for 1-3 weeks. For uncomplicated
parapneumonic effusions, complete resolution with
antibiotics alone is expected. However, serial physical
examination and radiography may necessitate repeat
thoracentasis if patients condition worsens ,especially
if effusion increases in size or patient remains or
becomes afebrile. For complicated effusion, there is a
variable response to antibiotic alone and since gram
stain is positive, tube thoracostomy is recommended. For
empyema initial management involves tube thoracostomy.
If there is no noticeable improvement following tube
thoracostomy, an ultrasound scan or computerized
tomographic scan of the chest is performed to detect
loculated fluid as well as the position of the tube.
In the presence of multiple loculi, thrombolytic therapy
is administered intrapleurally. The thombolytic agents
must be administered early to be more effective and
studies suggest that treatment group required less
surgical intervention and fewer days of hospital stay
29. Streptokinase and urokinase are equally effective
although streptokinase may lead to sensitization with
production of an antibody response and subsequent
allergic reaction. Loculations in the pleural space
can also be disrupted and pleural space drained
completely via Video-Assisted Thoracoscopy[VATS] or open
Page 50
_____________________________________________________________________ 50
thoracostomy/decortication which also helps to evacuate
any abscess collection.
Open drainage of an abscess cavity via rib resection
is only recommended in patients who are too ill to
tolerate a major decortication surgery. 1 to 3 ribs
overlying the lower part of the empyema cavity is
resected to allow open drainage.
Tuberculous Pleural Effusion usually disappears with prompt
exhibition of standard anti-Koch’s regimen. The aim of anti-
tuberculous chemotherapy include, to cure the patient of the
disease with minimum interference with their living in as
short a time as possible whatever the initial drug
susceptibility of the causative organisms, to prevent death
from active disease or its late effects, to prevent relapse
of the disease and emergence of acquired drug resistance and
finally to protect the community from transmission of the
disease. Properly applied short course chemotherapy is
guaranteed to yield the desired results especially in the
context of control programmes recommended by under the
National Tuberculosis Programme of the World Health
Organization. For associated Pleural effusion, a closed system
needle aspiration helps to relieve associated mild respiratory
distress but situations where there is severe respiratory
distress due to massive pleural effusion and respiratory rate
above 40 cycles per minute, a standard tube thoracostomy
drainage of the pleural space is indicated. Therefore tube
thoracostomy drainage of a tuberculous pleural effusion is
best avoided unless when absolutely indicated to avoid the
risk of empyema necessitants.
Malignant Pleural Effusion tend to be massive and recurrent,
hence presents a therapeutic challenge. Treatment directed at
Page 51
_____________________________________________________________________ 51
the primary mitotic lesion in form of surgery, chemotherapy
and radiotherapy are usually employed early in the disease
management. The appearance of malignant pleural effusion
therefore indicates an advancement of the mitotic lesion in
spite of any previous treatments. Hence, the presence of
malignant effusion is a poor prognostic sign with a mean
survival after diagnosis of 3-11 months in most series
30.
In recurrent pleural effusion there may be need for
pleurodesis. Following complete drainage and re-expansion
of the lungs, and daily chest tube drainage of less
than 100mls, it may just be possible to approximate
the two pleural surfaces in order to forestall further
re- accumulation of fluid. Historically, many chemical
agents have been instilled into the pleural space and
shown to have some effectiveness in controlling
effusions, including tetracycline, oxycycline, minocycline,
bleomycine, cisplatine, doxorubicine, etoposide,
fluorouracil, mitomycine, mitoxanthrone, interferone,
corynebacterium parvum, mepacrine, methylprednisolone, and
talc. 31.
But it appears that talc is a better option
than the rest as suggested by a large single arm
comparative studies and very small randomnized studies
suggest advantages for talc as the sclerosing agent
compared to tetracycline and bleomycine in greater
than 90% and 50% respectively 32. In our practice
tetracycline is more accessible compared to the rest
sclerosing agents. Dissolved in sterile water tetracycline
has shown a good promise as a sclerosing agent for
pleurodesis. ”33.
Page 52
_____________________________________________________________________ 52
TECHNIQUE OF PLEURODESIS
Before removal of the chest tube after drainage, a
reconstituted solution of the chosen agent is injected
into the pleural cavity after which the tube is double
clamped for at least 2 hours, while the patient is
asked to turn from side to side to ensure even
distribution of the agent in the pleural cavity.
Thereafter it is unclamped and may be connected to a
low suction if necessary. Chemical pleurodesis can also
be done via a video-assisted thoracoscopy in the
operating room, under general anaesthesia, during which
the surgeon may access any biopsy 34.
The chest tube is removed when there is both clinical
and radiological indication. Securing nylon suture is
severed, tube pulled out, while the purse string is
tied simultaneously to avoid sucking in air. Air tight
dressing is now applied.
Patient may experience fever and chest pain due to
the inflammatory process in the pleural cavity. Aspirin
tablets are quite helpful should this complication arise.
There are reported cases of failure to pleurodesis
usually due to loculation , inaccurate tube placement,
lung entrapment by visceral peel , all hampering the a
complete drainage of the the pleural cavity. These
factors are more important than the choice of a
sclerosing agent. Surgical decortication has been advocated
for this problem but it is potentially dangerous and
has resulted in broncho-pleural fistula and empyema.
Placement of a pleuro-peritoneal shunt has also been
attempted but it is often complicated by fibrinous
obstruction of the stoma. A pleural spigot has
Page 53
_____________________________________________________________________ 53
recorded some success in fourteen published cases but
the potential complication is infection which may
worsen an already bad situation. Radiation therapy may
be indicated in pleural effusion secondary to lymphoma
though with limited success and also the potential
danger of lung damage.
Malignant pleural effusion are still an unresolved clinical
problem inspite of the above measures. Current trials
with interleukin 2 injected into the pleural space
have been documented. The efficiency of intra-pleural
interleukin 2 has never been related to lesion
location or cancer histotype. This observation
demonstrates that treatment with intra-cavity interleukin
2 avoids repeated accumulation of fluid , not only with
an anti-neoplastic mechanism but mainly inducing
fibrosis process.35.
Treatment of Empyema Thoracis , depends on the stage
in the natural history of the disease.
In Stage 1 Disease[acute stage], the pus is thin and
remains thin. When collected in in a test tube, it
contains less than one third sediment after 24hrs
standing. Treatment here involves aspiration and
instillation of heavy doses of antibiotic done every
2-3 days. Chest tube insertion can also be done, but
patient must also receive systemic antibiotics.
In Stage 2 Disease [sub-acute stage], the pus is thick
with a high fibrin content. On 24hrs standing, the
sediment greater than one third basically due to a
high fibrin content. Chest tube placement may be done
initially especially in an acutely ill patient
Page 54
_____________________________________________________________________ 54
moreso when there is an associated broncho-pleural
fistula, ruptured esophagus, lung abscess. This
procedure is usually temporary because even the widest
bore tube easily gets blocked by fibrin. Decortication
should be offered to fit patients while tube
thoracostomy should
be maintained as long as there is fear of lung
collapse. Rib resection [fig 10] is the preferred
modality of treatment when the pus is thick
especially after a failed aspiration and intercostals
tube drainage. To avoid chronicity, rib resection
drainage must not be delayed too long and it must
be adequate and dependent.
Fig.10 Diagrammatic
illustration of rib
resection drainage
procedure in
empyema thoracis.
In Stage 3
Disease [chronic], there is a marked adhesive fibrin
deposits on both visceral and parietal pleural
surfaces, with some little intervening insipissated pus.
The drainage method employed earlier may have been too
late or grossly inadequate. Decortication is the
procedure of choice at this stage and it involves
the complete removal of the fibrous wall of the
empyema cavity from both the lung, chest wall and
Page 55
_____________________________________________________________________ 55
diaphragm in order to allow the the previously
imprisoned lung to expand and fill up the space
previously occupied by the empyema. This
operation is a major undertaking and should only be
done if the patient was previously fit and the
general condition is still reasonably good and is not
adviced in the elderly.
Other associated or predisposing disease conditions
should equally be treated on their own merits , at
the same time the empyema thoracis is being treated.
Treatment of chylothorax may be conservative initially,
by decompressing the thoracic lymphatics with parenteral
hyper-alimentation or oral medium chain triglycerides
and adequate drainage with intercostals tube. Talc
pleurodesis may be tried after 3-4 weeks. If the above
measures fail, thoracotomy is nessecitated and it is
aimed at ligating the thoracic duct at the site of
leakage, whose identification is facilitated a fatty
meal just prior to surgery.
Pleuro-peritoneal shunts have been used successfully for
refractory chylothorax in infants following surgery for
congenital heart disease.
For adults with malignancies, surgical intervention may
not be effective but in trauma cases, conservative
decompression as outlined above usually suffices and
surgical intervention is usually unnecessary.
The management of haemothorax depends on the rate of
bleeding, volume of blood already lost, associated
haemodynamic derangement, as well as the underlying
Page 56
_____________________________________________________________________ 56
cause. If haemothorax is small [<250mls] and bleeding had
stopped, as evidenced by clinical status, only
observation may suffice. For moderate blood loss [500mls]
a tube thoracostomy with an underwater seal drainage
system is adviced because it allows complete evacuation
of blood from the pleural space as well as ensuring
adequate monitoring of any continued bleed. Serial chest
roentgenogram helps to monitor lung re-expansion. Needle
aspiration is discouraged because of the risk of
introducing infection, but if considered necessary at
any point, all aseptic procedures must be adhered to.
If there is a continued bleeding of volumes
>200mls/hr, or an initial loss of >1500mls of fresh
blood, or presence of massive clots, or clinical signs
of haemodynamic instability, there is an overwhelming
indication for an emergency exploratory thoracotomy with
concomitant vigorous correction of haemodynamic
instability. Because blood in the pleural space tends
to be de-fibrinogenated, and slow to clot, it can be
collected via a sterile drainage system into a sterile
container, filtered and re-infused into the patient.36.
To prevent the the development of an imprisoning
fibrothorax and to gain re-expansion of a lung
compressed by blood clot, early evacuation of clotted
haemothorax and decortication are sometimes recommended .
It is however expected that fibrinous deposits on the
pleural surfaces should peel off 3 weeks post injury,
so as to allow full re-expansion of the lungs.
Page 57
_____________________________________________________________________ 57
CHAPTRE TWO-MATERIALS AND METHOD
OVERVIEW
This was a prospective study involving all patients who
presented to National Hospital Hospital Abuja between February
2005 and February 2006 with pleural effusion requiring some
form of surgical intervention in the course of their
management.
Page 58
_____________________________________________________________________ 58
STUDY CENTRE.
The Department of Surgery, National Hospital Abuja wass the
study center. Is located in the central business district of
the Federal Capital Territory(FCT) Abuja.
FCT is located in the North Central Geo-Political zone of
Nigeria.
National Hospital Abuja was established by Decree 36 of
1999 by the then Military Government.
Its operations has remained under the supervision of
Presidency via the office of the Secretary to the
Federal Government since the current democratic
dispensation.
It was designed to serve as an apex referral hospital
for Nigerians as well as neighboring countries, so
as to stem the tide towards seeking medical treatment
abroad hence its endowment with the state of the art
equipment.
STUDY POPULATION
FCT settlers who are heterogeneous in nature constitute
the bulk of the patients that attend National Hospital
for treatment. The rest were from neighboring states and
countries.
Inclusion Criteria-Only patients with clearly defined clinical
and radiological evidence of pleural effusion who in addition
will benefit from surgical intervention constituted the
study group. Random sampling was done over a period of 1 year
Page 59
_____________________________________________________________________ 59
spanning from February 2005-February 2006.
Exclusion Criteria-Any other patient including those with
pleural effusion with medically related causes. All cases of
traumatic haemothorax whose formation does not depend on the
alteration of starling forces.
Sample Size-A total of 86 cases fulfilled the stipulated
requirements for sampling and were available for sampling
during the study period between February 2005 to February
2006.
Whereas some of these patients presented through the accident
and emergency unit , others were referred from
oncology, Internal Medicine, Pediatrics departments of the
hospital or from neighboring hospitals.
DATA COLLECTION PROCESS
Patients that met the criteria were sampled randomly
during the stipulated study period.
A pre-designed proforma was employed as a tool to
document the relevant demographic ,clinical , radiological,
biochemical, bacteriological, cytological data as well as
treatment modality, outcome of treatment, and complication
of treatment peculiar to any sampled case.
PATIENT HANDLING PROTOCOL
Except in dire emergencies with severe life threatening
respiratory distress, all selected patients were
subjected to thorough history, physical examination and
radiological assessment , followed by consent for
thoracocentasis which yielded the pleural fluid itself,
providing an opportunity to assess its physical
appearance such as purulent/turbid, serosanguinous, straw
coloured, milky etc. Thoracocentasis was done through the
5th intercostals space mid-axillary line under sterile
condition. The sampled fluid was accordingly stored in
their respective ideal containers as follows:
Page 60
_____________________________________________________________________ 60
-Plain tube for protein, LDH, glucose, triglycerides, and
Cholesterol estimation
-Ethylene diamine tetra acetic acid bottle for cell count
and packed cell volume
-Heparin treated blood gas syringe for ph
-Sterile container for Gram stain/culture, acid-fast
bacilli and fungal studies
-50 millilitre heparin treated container for cytology.
Following a successful thoracocentasis, patient’s consent
was further sought and a thoracostomy tube was
inserted through the appropriate intercostal space ,
usually the 5th or 6th space mid-axillary line, and
tightly secured in place with nylon 2 suture, ensuring
that at least all the fenestrations at the thoracic
end of the chest tube were well insinuated into the
pleural cavity. The thoracostomy tube which all along
was double clamped with strong artery forceps to
prevent sucking air into the chest was then connected
to the under-water seal drainage system and the clamps
removed.
Immediate observation of an oscillatory movement of a
column of fluid in the tube indicates a correct
placement of tube in the pleural space. This was
further confirmed by a post- intubation check X-ray of
the chest.
For patients who presented with massive pleural
effusion, the fluid was only allowed to drain in
aliquots of 200-300mls/hr to avoid complications like acute
onset severe cough which may provoke haemoptysis, rebound
pulmonary edema.
CARE OF THE CHEST TUBE
Constant reassurance of the patient was mandatory.
Thoracostomy site wound was inspected regularly and any
Page 61
_____________________________________________________________________ 61
sepsis treated accordingly. Oscillation of fluid column was
checked regularly to ensure that tube remained in-situ
Daily recording of output from the chest tube was
done and when less than 50cc ,indicated that extubation
was due.
Extubation was effected by asking the patient to
inhale maximally and to hold the breath, while the
sutures holding the tube were severed and tube pulled
out quickly and a pre-positioned purse string
tightened to secure an air-tight seal of the chest
wall. A neat dressing was then applied.
LABORATORY METHODS
CHEMISTRY
Electrolyte estimation was by the use of ion-selective
electrode method in an automated machine.
Lipid estimation was done by automated enzymatic colorimetrc
test.
Protein level was estimated by turbimetry/precipitation
or colorimetric method(Biuret’s test)
Microbiology
Initial Gram- Stain, followed by culture in chocolate,
blood and Ma Conkey medium, and then antibiotic
sensitivity.
Acid- Fast Bacilli x3 was done on the sediment of the spun
fluid.
Fungal Test can be done with seaboard agar.
CYTOLOGY
Page 62
_____________________________________________________________________ 62
Pap smear of the spun sediment was made on a
slide and fixed with 90% alcohol, then stained with
Haematoxylene-Eosin solution before reading.
RADIOLOGY
A postero-anterior chest radiograph was usually done and
it often defines the features of the effusion as
well as any associated mediastinal shift/pathology.
Other views may be quite useful in certain circumstances such
as,
Lateral view defines minimal collection (<175cc) in
the costo-phrenic angles, supine views for moribund/bed
confined patient, and decubitus for investigating other
associated pathology in the lung which may have been
masked by the effusion.
Chest radiographs were also used to monitor the
progress of drainage of the effusion.
Computerized Tomographic Scanning and Magnetic Resonance
Imaging are other modalities of investigating chest
pathologies.
SUBSEQUENT PATIENT MANAGEMENT
In most patients, nothing more need be done. However
in some, associated pathology or the outcome of
investigations dictated further treatment such as
pleurodesis for recurrence prone malignant effusion,
decortication for complicated empyema thoracis.
Page 63
_____________________________________________________________________ 63
ETHICAL CONSIDERATIONS
Ethical clearance was sought from the ethical committee of the
National Hospital. Only patients who willfully consented
were included in this study and reserved the right
to withdraw at any stage if they felt so.
An information sheet was given to all subjects stating
all that was required of them and providing opportunity
to clear their doubts, before consent was given.
DATA ANALYSIS-was done using the EPI-INFO statistical soft
ware package and presented in the form of pie charts, bar
charts, histogram and tables.
SAMPLE OF INFORMATION SHEET FOR PATIENTS/RELATIVES
Fluid can accumulate in the space inside the chest called
pleural cavity. This condition is abnormal and in certain
quantity leads to breathlessness and impaired quality of life.
There are various causes such as trauma, tumor, infection
which may be revealed in the course of investigation.
A structured in management has a direct effect on the outcome
of treatment. This study is mostly carried out by the patient
bedside in the wards where they are normally admitted such as
the Surgical, Medical, pediatric wards under strict
supervision.
With your consent, we believe that your enrolment in this
study will benefit not only you but also others with similar
problems. It will also afford us yet another opportunity for
the advancement of surgical research.
We are also quite willing to furnish you with any further
explanations on demand.
Page 64
_____________________________________________________________________ 64
Thank you
Dr.Charles Ugwuanyi
Dept. of Surgery
National Hospital Abuja.
SAMPLE OF CONSENT FORM FOR PATIENTS.
I-----------------------------hereby give consent for
myself/my child to participate in this on pleural effusion.
I have been furnished with the information sheet which has
been fully explained to me. I also understand that that no
additional expenses will be incurred by me as a result of
this study other than the routine expenses associated with my
healthcare and follow-up.
I hereby make this declaration willingly.
Signature of patient/Gourdian Signature of witness
CHAPTER THREE-RESULTS
A total of 86 cases of pleural effusion requiring some
sort of surgical intervention were sampled in this 1
year prospective study spanning February 2005 to
February 2006 in the National Hospital Abuja.
Sex Distribution.[fig 11]
There were 48 males [55.8%] and 38 females [44.2%]
Male: Female ratio is therefore 1.26: 1.
Page 65
_____________________________________________________________________ 65
Fig. 11.- Sex distribution of patients.
Age Distribution [fig 12]
Age range was from 1 year to 80 years.
Peak age was 30 years with a frequency of 9 representing
40.7% of all cases.
Youngest age was 1 year with a frequency of 2
representing 2.3% of all cases sampled.
Oldest patient was 80 years with a frequency of 1
representing 1.2% of cases.
The cluster age incidence was between 17 years and 66
years.
Page 66
_____________________________________________________________________ 66
Fig. 12.- Age distribution of patients.
City of Residence of Patients. (fig 13)
Cases residing within Abuja and environs
constitute 67 [81.7%] of all cases sampled, while
were spread across the other parts of Nigeria.
Fig. 13.- City of residence of patients.
Clinical Presentation of Cases Studied. (fig 14)
Page 67
_____________________________________________________________________ 67
Breathless
ness
Coug
h
Chest
pain
Feve
r
Weight
Loss
86 83 78 42 50
.Fig 14.-Clinical Presentation of Cases Studied.
Breathlessness was present in all the 86 (100%) patients
studied.
Cough was present in 83 (96.5%) of cases.
Chest Pain occurred 78(90.69%) of cases.
Fever was present in 42(48.8%) of cases.
Weight loss was present in 50(58.13%) of cases.
Physical signs in keeping with right sided
pleural effusion was found in 54(62.79%) of
cases while signs of left sided pleural
effusion was found in 28(32.55%) of cases. The
chest signs were bilateral in 49(4.6%) of
cases studied.
Physical Appearance of Pleural Fluid
0
10
20
30
40
50
60
70
80
90
Breathlessness Chest pain Weight Loss
Page 68
_____________________________________________________________________ 68
sampled via Thoracocentasis.(fig.15)
1
14
24
47
0
5
10
15
20
25
30
35
40
45
50
Frequency
Chyle
Pus
Sero-
sanquinous
Straw colour
liquid
Fig.15.-Physical Appearance of Pleural Fluid
Straw coloured fluid was found in 47(54.7%) of cases,
Sero-sanguinous in 24(27.9%) , purulent/turbid fluid in
14(16.3%) and milky/chylous fluid in only one case
representing 1.2% of cases.
Pathology Associated with Pleural Effusion (fig. 16)
Page 69
_____________________________________________________________________ 69
1
Fig.16.-Pathology Associated with Pleural Effusion.
Neoplastic Disease was present in 35(40.72%)
of cases , Pulmonary Tuberculosis in 32(37.2%)
of cases and Pneumonia in 19(22.1%) of cases.
Distribution of malignant causes.(fig. 17)
Fig. 17.-Disstribution of malignant causes of pleural
effusion.
Breast carcinoma made up 23(65.7%) , Intra-abdominal
Page 70
_____________________________________________________________________ 70
malignancy 3 (8.6%) , Lung carcinoma 4(11.4%) , Soft
Tissue Sarcoma 4(11.4%) and Parotid Tumour1(2.9%).
Chemical Analysis of Pleural Effusion.
a. Specific Gravity- ranged from 1016 to 1018
in all cases.(fig. 18)
1016 1017 1018
13 39 340
200
400
600
800
1000
1200
Values and freq.
Specific Gravity No. Of Patients
Datasets
Frequencies of Specific Gravity
Fig. 18.- Specific Gravity Ranges.
b. Protein Content- ranged from 39mg/dl to 72
mg/dl in all the 86 samples.
c. Glucose level- ranged from 21mg/dl to 67mg/dl(Table 1)
Gl
ucose
No. Of
Patients
Pe
rcent
21 4 4.
7%
23 6 7.
0%
24 1 1.
2%
26 1 1.
2%
27 4 4.
7%
28 2 2.
3%
29 1 1.
2%
30 1 1.
2%
Page 71
_____________________________________________________________________ 71
31 8 9.
3%
32 8 9.
3%
34 8 9.
3%
35 1 1.
2%
36 1 1.
2%
37 6 7.
0%
38 2 2.
3%
39 1 1.
2%
41 3 3.
5%
42 6 7.
0%
43 6 7.
0%
44 1 1.
2%
45 4 4.
7%
47 5 5.
8%
51 1 1.
2%
55 1 1.
2%
62 1 1.
2%
63 1 1.
2%
67 2 2.
3%
T
otal 86
1
00.0%
Table 1 Glucose Levels
Page 72
_____________________________________________________________________ 72
d. Triglycerides ranged from 86mg/dl to 300 mg/dl.(Table 2)
T
G
No. of
Patients
Pe
rcent
8
6 1
1.
2%
8
7 2
2.
3%
8
9 1
1.
2%
9
0 1
1.
2%
9
5 4
4.
7%
9
6 1
1.
2%
9
7 1
1.
2%
9
8 15
17
.4%
1
01 4
4.
7%
1
02 12
14
.0%
1
03 5
5.
8%
1
04 5
5.
8%
1
05 3
3.
5%
1
07 1
1.
2%
1
08 2
2.
3%
1
09 3
3.
5%
1
12 2
2.
3%
1
15 1
1.
2%
1
20 1
1.
2%
1
23 13
15
.1%
1
24 1
1.
2%
1
25 2
2.
3%
1
32 1
1.
2%
Page 73
_____________________________________________________________________ 73
1
34 1
1.
2%
1
45 1
1.
2%
1
52 1
1.
2%
3
00 1
1.
2%
T
otal 86
1
00.0%
Table .2.- Triglyceride
Levels in fluid sample
e. Lactate Dehydrogenase (LDH) ranged from 350 iu to
4120iu.(Table.3)
L
DH
No. Of
Patients
Pe
rcent
3
50 1
1.
2%
4
00 3
3.
5%
8
42 1
1.
2%
8
50 1
1.
2%
8
67 1
1.
2%
8
97 1
1.
2%
9
50 1
1.
2%
Page 74
_____________________________________________________________________ 74
9
74 1
1.
2%
9
80 2
2.
3%
9
83 3
3.
5%
9
86 1
1.
2%
1
080 1
1.
2%
1
100 1
1.
2%
1
120 2
2.
3%
1
132 1
1.
2%
1
181 1
1.
2%
1
186 1
1.
2%
1
278 1
1.
2%
1
420 1
1.
2%
1
489 1
1.
2%
1
589 1
1.
2%
Page 75
_____________________________________________________________________ 75
1
789 1
1.
2%
1
816 1
1.
2%
1
823 1
1.
2%
1
830 1
1.
2%
1
848 2
2.
3%
1
856 1
1.
2%
1
875 1
1.
2%
1
880 1
1.
2%
1
934 1
1.
2%
1
974 1
1.
2%
1
980 2
2.
3%
1
984 1
1.
2%
2
085 1
1.
2%
2
102 1
1.
2%
Page 76
_____________________________________________________________________ 76
2
116 1
1.
2%
2
120 1
1.
2%
2
167 1
1.
2%
2
168 2
2.
3%
2
170 1
1.
2%
2
180 4
4.
7%
2
186 1
1.
2%
2
188 1
1.
2%
2
240 2
2.
3%
2
246 1
1.
2%
2
281 1
1.
2%
2
467 1
1.
2%
2
678 1
1.
2%
2
750 1
1.
2%
Page 77
_____________________________________________________________________ 77
2
810 1
1.
2%
2
812 1
1.
2%
2
830 1
1.
2%
2
840 1
1.
2%
2
845 1
1.
2%
2
864 1
1.
2%
2
870 1
1.
2%
2
896 1
1.
2%
3
120 4
4.
7%
3
121 1
1.
2%
3
124 1
1.
2%
3
140 1
1.
2%
3
180 1
1.
2%
3
310 2
2.
3%
Page 78
_____________________________________________________________________ 78
3
320 1
1.
2%
3
340 1
1.
2%
3
380 1
1.
2%
3
720 1
1.
2%
3
812 1
1.
2%
4
120 1
1.
2%
T
otal 86
1
00.0%
Table 3 Lactate Dehydrogenase (LDH) Levels
f. Cholesterol level ranged from 96mg/dl to 188mg/dl.
(Table 4)
Choles
terol
No. Of
Patients
Pe
rcent
96 1 1.
2%
108 1 1.
2%
109 1 1.
2%
110 1 1.
2%
115 1 1.
2%
123 2 2.
3%
124 1 1.
2%
Page 79
_____________________________________________________________________ 79
125 1 1.
2%
127 2 2.
3%
128 2 2.
3%
129 1 1.
2%
130 1 1.
2%
132 1 1.
2%
134 1 1.
2%
135 3 3.
5%
142 1 1.
2%
143 2 2.
3%
145 3 3.
5%
146 3 3.
5%
147 1 1.
2%
149 1 1.
2%
154 6 7.
0%
156 14 16
.3%
160 1 1.
2%
162 1 1.
2%
163 4 4.
7%
164 2 2.
3%
165 2 2.
3%
167 12 14
.0%
168 2 2.
3%
168.9 2 2.
3%
169 1 1.
2%
171 1 1.
2%
173 2 2.
3%
174 2 2.
3%
Page 80
_____________________________________________________________________ 80
178 1 1.
2%
187 1 1.
2%
188 1 1.
2%
Total 86 1
00.0%
Table .4.- Cholesterol Levels
g. Sodium level ranged from 130mg/dl to
140 mg/dl.(Table 5)
Page 81
_____________________________________________________________________ 81
Table .5.- Sodium Levels
h. Potassium level ranged
from 2.9mg/dl to
4.1mg/dl.(Table 6)
N
a+
No. Of
Patients
Pe
rcent
1
30 1
1.
2%
1
31 3
3.
5%
1
32 2
2.
3%
1
35 3
3.
5%
1
36 2
2.
3%
1
37 11
12
.8%
1
38 8
9.
3%
1
39 6
7.
0%
1
40 5
5.
8%
1
41 15
17
.4%
1
42 3
3.
5%
1
43 12
14
.0%
1
45 3
3.
5%
1
47 12
14
.0%
T
otal 86
1
00.0%
Page 82
_____________________________________________________________________ 82
Table.6.-
Potassium
Levels
i. Chloride level ranged from 95mg/dl to
Potassium No. Of Patients Perce
nt
2.9 1 1.2%
3.1 7 8.1%
3.2 3 3.5%
3.4 1 1.2%
3.5 7 8.1%
3.6 1 1.2%
3.7 13 15.1%
3.8 10 11.6%
3.9 10 11.6%
4.1 15 17.4%
4.2 8 9.3%
4.3 4 4.7%
4.4 1 1.2%
4.5 2 2.3%
4.6 1 1.2%
4.7 2 2.3%
Total 86 100.0
%
Page 83
_____________________________________________________________________ 83
114mg/dl.(Table 7)
Fig. 19-Chloride Levels
j. Ph ranged from 7.0 to 7.2 (Fig. 20)
7 7.1 7.212
68
6
010203040506070
Value and
Freq.
pH No. Of Patients
Data set
pH Chart of Patients
fIg.20 Ph range Levels
K. Bicarbonate ranged from 18mg/dl to 25mg/dl.(Table 9)
Page 84
_____________________________________________________________________ 84
Table
.9.-
Bicarbonate Levels
CYTOLOGICAL ANALYSIS OF PLEURAL FLUID.
Of the 35 cases of neoplastic disease associated
pleural effusion, 24(68.6%) did not yield any positive
cytology while 11(31.42%) yielded positive cytology.
ACID FAST BACILLI(AFB) ANALYSIS OF PLEURAL FLUID
Of the 32 cases of Tuberculous effusion, positive
AFB yield was found in Only 2(6.25%) but negative in
30(93.75%) of cases.
White Cell Count- In the tuberculous cases, 24 out of the
32(75%) had relative lymphocytosis while the rest (25%) had
neutrophilia most probably due to secondary infection. All
HCO
3- No. Of Patients
Percen
t
18 5 5.8%
19 19 22.1%
20 23 26.7%
21 17 19.8%
21.
2 1 1.2%
22 19 22.1%
23 1 1.2%
25 1 1.2%
To
tal 86
100.0
%
Page 85
_____________________________________________________________________ 85
(100%)of the cases of para-pneumonic effusions had
neutrophil lymphocytosis
Microscopy Culture and Sensitivity of Pleural Fluid
Of the 19 cases of parapneumonic effusion, 14(73.68%)
yielded negative growth while 5(26.3 %) yielded positive
culture.
CHEST X-RAY FINDINGS
4(4.6%) cases had radiologically confirmed bilateral
pleural effusion of varying degree.
1(1.16%) case had a radiological evidence of right
sided hydro-pneumothorax
28(32.55%) cases had a radiological evidence of left
sided pleural effusion of varying degree.
53(60.22%) cases had radiological evidence of right
sided pleural effusion of varying degree.
62 cases (72.09%) had radiologically confirmed
Mediastinal shift,usually to the opposite side of
the lesion.
TREATMENT OF PLEURAL EFFUSIO IN NATIONAL HOSPITAL. (FIG.V)
Treatment of the primarily associated pathology was initiated
and or consolidated.
Tube- thoracostomy with an underwater seal drainage system, was
offered to 81(94.1%) of all cases.
Page 86
_____________________________________________________________________ 86
Pleurodesis was offered as an additional treatment to 32(37.2%)
of these.
Exploratory Thracotomy was offered to 6 patients
representing 6.9% of all, while
Tube thoracostomy with under-water seal drainage and low
suction was offered to 4 patients (4.65%)only.
OUTCOME OF TREATMENT AT 6 MONTHS EVALUATION
a. Neoplastic Disease Associated Pleural Effusion.
25 cases(71.4%) of malignant effusion progressed to death at
six months check up in-spite of all treatments given.
9 cases (25.7%) had partial recovery and still battling with
the disease at six months.
Only 1 case representing 2.9% of all malignant effusion showed
clinical evidence of complete recovery at six months.
b. Para-Pneumonic Pleural Effusion
16 cases (88.9%) of all para-pneumonic effusions showed
clinical and radiological evidence of complete recovery.
2 cases (11.1%) only showed evidence of partial recovery and
progression to empyema thoracis.
c.Pulmonary Tuberculous Effusion
15 cases (51.7%) of all tuberculous effusion showed both
clinical and radiological evidence of complete recovery at 6
months.
Page 87
_____________________________________________________________________ 87
9 cases (31%) showed partial recovery.
5 cases (17.22%) progressed to further complications culminating
in death.
COMMON COMPLICATIONS OBSERVED IN TREATMENT OF PLEURAL EFFUSION
IN NATIONAL HOSPITAL.
a. Premature Dislodgement of thoracostomy tube was
observed in 29 cases representing 33.72% of all
cases studied.
b. Progression to infection in a previously sterile
fluid was observed in 9 cases(10.4%).
c. Pneumothorax was observed in 8 cases (9.30%).
d. Wound sepsis at the thoracostomy site was
observed in 29 cases (33.7%)
e. Recurrence of effusion was observed in 35
cases (40.7%).
TREATMENT OF COMPLICATIONS
All cases of premature dislodgement of thoracostomy tube
and pneumothorax were treated satisfactorily by proper
re-positioning/ securing of the tube and antibiotic cover.
Wound sepsis was treated by daily wound dressing and
wound swab culture and sensitivity directed antibiotic therapy.
Page 88
_____________________________________________________________________ 88
Recurrent Effusion was treated by repeat tube thoracostomy
in 21(60%) of recurrent cases with additional pleurodesis
in 13(37.1%) of cases. Only one case of recurrence had
thoracotomy and decortication.
Page 89
_____________________________________________________________________ 89
CHAPTER 4-DISCUSSIONS AND CONCLUSIONS
Though males were more affected than females in this
study, certain associated pathologies were commoner in
females , for example, carcinoma of the breast in females
was responsible for 65% of all malignant effusions in
this series.
All age groups were affected but the cluster age
incidence was 17 to 66 years. Very few cases were seen at the
extremes of life.
Most patients (81.7%) involved in this study reside within
Abuja, Nigeria and its environs, which constitute the
major catchments area for National Hospital. The rest
were spread across other parts of Nigeria and beyond.
CLINICAL PRESENTATION
All the 86 patients (100%) sampled, presented with dyspnoea. It
is the most common presentation of pleural effusion as
clearly documented by Abrahamian et al. 18.
Pleural effusion produces a restrictive defect on the
lungs, alveolar sacs, and pulmonary circulation is thus
compromised. Massive effusion further pushes the mediastinum
to the contralateral side . There is also a decreased
ipsilateral lung volume modulated by neurogenic reflexes
from the lungs , all contributing to compromised cardio-
Page 90
_____________________________________________________________________ 90
pulmonary function. The resultant clinical effect of all
these is dyspnoea as well as tachycardia.
It is not likely that an effusion not sufficient to
produce clinically detectable dyspnoea to be surgically
important. About 500mls of pleural fluid is required to
produce clinically detectable dyspnoea. It is important to
note that other associated pathologies both in the lungs
and elsewhere may contribute to dyspnoea.
Cough was the second commonest symptom encountered in
this series, present in 96.5% of cases. It was initially
unproductive ,caused by irritation of the alveolar walls
by some fluid accumulation . In a few cases it later
became productive and infact was associated with
haemoptysis. Studies have shown that this situation
arises in the chronic lung parenchymal diseases such as
pulmonary tuberculosis, malignancies, whereby the
sorrounding alveolar blood vessels are sufficiently
devitalized by this underlying pathology and are rendered
prone to rupture easily especially with violent coughs,
hence precipitating haemoptysis.
Chest pain was recorded in 78% of cases. It was typically
described as sharp, biting, or pleuritic initially. This is
due to pleural irritation caused by inflammation or
malignant deposits around the pleura, and localized to
the ipsilateral chest wall or referred to to the
ipsilateral shoulder if the shoulder is involved.
Weight loss was recorded in a little above half the
cases (58.1%). It is not usually caused by the effusion,
but related to the underlying pathological condition such
Page 91
_____________________________________________________________________ 91
as malignant cachexia of advanced neoplastic disease,
chronic debilitating diseases.
Fever was found in just below half the cases
studied(48.8%), mostly observed in parapneumonic cases,
or secondary to septic instrumentation of the pleural
space in a previously sterile effusion.
The aforementioned symptoms occurred in various combinations
in different patients, in addition to other symptoms directly
related to the primary pathology.
Physical signs elicited on chest examination in keeping
with right pleural effusion was found in 62.8%. These
signs include reduced chest excursion, dullness to
percussion, reduced tactile fremitus, egophony.
The same signs were elicited on the left hemothorax in
32.5% of cases, while in 4.6% of cases they were
bilateral.
Therefore, this study demonstrates that pleural effusion
was commoner in the right hemithorax.
Thoracocentasis which was carried out to sample pleural
fluid in all cases studied yielded straw-coloured fluid
in 54.7% of cases, followed by serosanguinous fluid in
27.9% , pus in 16.3% and milky in 1.2%.
Straw coloured fluid was therefore the commonest, while
chylous fluid was the least common.
Page 92
_____________________________________________________________________ 92
Straw coloured fluids are commonly found in tuberculous
pleural effusions, but can also be found in some
malignant pleural effusions as well as para-pneumonic
effusions and sympathetic effusions.
Serosanguinous fluids are commonly seen in malignant pleural
effusions, but can also be seen in tuberculous pleural
effusion, pulmonary embolism.
Frank haemothorax are usually caused by chest trauma,
blood dyscrasias, but are excluded from this study since
they are not strictly speaking effusions.
Purulent/turbid effusions are almost always diagnostic of
an exudates due to parapneumonic condition, but it can
also be found in other types of effusion following a
septic instrumentation of the pleural space. It may
therefore indicate a progression to empyema thoracis.
Milky effusion is almost always associated with chylothorax,
but in some cases of long standing transudative
effusions, the cholesterol content increases, thus giving
a milky appearance in a condition called pseudochylous
effusion.
No cases of brown/chocolatey fluid suggesting ruptured amebic
abscess, or black fluid suggesting aspergillosis was
encountered in this study.
PLEURAL FLUID ANALYSIS.
The assessment of pleural aspirate was guided to some
extent by the clinical context in which the effusion
Page 93
_____________________________________________________________________ 93
occurred. In most cases the cause of the pleural
effusion was already known at this stage from clinical
and radiological evaluation. However laboratory evaluation
of pleural aspirate may either buttress an already known
diagnosis or provide an inroad into the elucidation of a
pleural effusion whose cause was not already known.
Measurement of total protein and lactate de-hydrogenase
concentrations, microbiologic and cytologic analysis are
among the myriad of tests that can be conducted for
these purposes.
In this study , the total protein concentration of
pleural fluid ranged from 39g/dl to 72g/dl. This was way
above 3g/dl which is generally used as the reference
point for distinguishing exudates from transudates,
though this may result in misclassification in about 15%
of cases. This is where Lights criteria comes in, with
a sensitivity of 99% and specificity of 98%.21. It
employs parameters such as a combination of serum
protein, pleural fluid LDH, serum LDH estimation in
various permutations.
A 1997 meta-analysis of the diagnostic value of tests
used to distinguish transudates from exudates did not
find any test or combination of tests to be clearly
superior.20 Hence the choice of tests is individual
preference, but if choice narrows to one, measurement of
the total protein concentration is the most practical
choice in view of high accuracy and availability.
Page 94
_____________________________________________________________________ 94
Protein level was high due to increased pleural
permeability resulting from complex inflammatory mediators
interacting between the mesothelium whose cells play an
active role in inflammation, phagocytosis, leucocyte
migration, tissue repair, antigen presentation, coagulation
and fibrinolysis and the endothelium. Lymphatic blockade
aqually plays a role especially in malignant effusions.
So, all the samples studied were clearly exudative, and
was therefore not surprising that all pleural fluids
sampled in this study had a high specific gravity which
ranged from 1016 to 1018, due to the high protein
and/or cellular content.
The lactate dehydrogenase levels were also clearly elevated
well above the upper limit of normal in most of the
samples.
Conversely, most of the sampled fluids had relatively low
level of glucose which ranged from 21 to 67mg/dl. This
is in line with findings in tuberculous effusions,
malignant effusions , parapneumonic effusions etc.It is
believed that the high cellular metabolic activity in these
conditions use up the available glucose.
Trigyceride was mostly within normal range except in one
case which recorded 300mg/dl. That was the only case of
chylothorax in this study and was secondary to iatrogenic
rupture of the thoracic duct in a patient that had
decortication for stage 3 empyema thoracis.
Page 95
_____________________________________________________________________ 95
High pleural fluid triglyceride levels is most commonly
caused by rupture of thoracic duct due to tumour ,
trauma , whereby chylous fluid high in chylomicrons and
protein content is lost into the pleural cavity
usually the right. This is of immense nutritional importance,
and such patients sooner tips to severe nutritional
deficiency.
Though the electrolyte picture was found to be similar
to that of serum in most cases, the ph were
slightly acidic .Again this is attributable to an avalanche of
products of anerobic cellular respiration such as lactic acid.
Acidic pleural effusion suggests parapneumonic
effusion/empyema, malignancy, tuberculosis.
The diagnostic yield of cytological analysis in this
study was only 24%. In some other studies it is
generally in the range of 50 to 60 % . It is even
higher in patients with bulky pleural tumour, and a
repeat cytological testing may increase the yield to
more than 70%. Similarly, testing of 3 or more samples
may increase the yield to 90%. The low yield in this
study may be attributed to a number of factors such as
observer dependent error, poor tissue sampling and
handling, inadequate sampling , laboratory limitations.
Out of the 32 cases of pulmonary tuberculosis
encountered in this study, positive pleural fluid acid-
fast bacilli was found in only 2 cases representing
6.25%. This is indeed a very low yield.
Page 96
_____________________________________________________________________ 96
Based on a study by Seibert A.F. et al, where he reviewed
1,738 cases, of pulmonary tuberculosis, between 1968 to
1988,in Mobile, Alabama, 70 cases of tuberculous pleural
effusion were identified. Diagnostic modality used was to
culture mycobacterium in sputum, pleura, or pleural
fluid, backed up with clinical/radiologic features. But
this diagnosis could also be made in the absence of a
positive culture and acid-fast bacilli if the patient
had a lymphocytic exudates in addition to all clinical
and roentgenographic abnormalities, which improved on
anti-tuberculous medications. It is there fore not unusual
not to have a very low yield of acid-fast bacilli in
pleural fluid in cases of tuberculous pleural effusion.
Tuberculous pleuritis should therefore be suspected in
patients with a history of exposure to or mantaux
positive findings and in patients with lymphocytic
effusions, especially if less than 5% mesothelial
cells are detected on diffrential count. Because most
tuberculous effusions probably result from a
hypersensitivity reaction to the mycobacterium, rather
than from microbial invasion of the pleura, acid-fast
bacilli stains of the pleural fluid are rarely
diagnostic (<10% of cases) , and pleural fluid cultures
grow mycobacterium in less than 65% of cases.40.
The combination of histology and culture of pleural
tissue biopsy further increases the diagnostic yield to
90%. This was one major limitation of this study due
to the absence of Abrams pleural biopsy needle.
Adenosine deaminase activity(ADA) whereby a level in
pleural fluid greater than 43u/u, interferon-gamma
Page 97
_____________________________________________________________________ 97
concentration in pleural fluid greater than 140pg/ul all
support tuberculous pleuritis, but since both were not
available for this study, that was another limitation
of this study.
Only 26.3% of the parapneumonic effusions yielded a positive
culture. This is rather not surprising since with the
advent of antibiotics most of these patients have
already been exposed to various antibiotics before
presentation, hence sterilizing the pleural fluid. This is
the same reason why the natural history of empyema
thoracis has been more or less abolished , and very
few cases of empyema complicating parapneumonic are seen
nowadays.
Concerning radiological findings, only 4.6% of cases
studied showed an evidence of bilateral pleural effusion
by way of blunting of costophrenic angles, classical
meniscus sign, and homogenous opacity below the meniscus.
Commonly employed is the P-A view where by a minimum of
250-500mls of fluid must accumulate before the
costophrenic angles could be blunted. Other views such
as A-P , decubitus were not commonly employed in this
study. Bilateral pleural effusion in the absence of
congestive cardiac failure is commonly caused by a
malignancy excluding breast and lung carcinoma. This is
because breast/lung carcinoma associated pleural effusion
are typically ipsilateral to the primary lesion in 58
to 70% of cases, however 20 to 25% of cases develop
an effusion in the contralateral side, while 10 to 16%
develop bilaterally 22. Other causes of bilateral
Page 98
_____________________________________________________________________ 98
pulmonary effusion include pulmonary tuberculosis, Meig’s
syndrome, pancreatic pseudocyst.
Hydropneumothorax was recorded in 1.16% of cases studied. The
most likely cause is a ruptured subpleural bleb in
pulmonary tuberculosis. Other causes include previous chest
intubation, and malpositioned chest tube.
Left sided effusion was recorded in 32.55% of cases
while right sided effusions was found in 53%. Hence
right sided effusions were far commoner in this series.
Certain pathologies have a predeletion to a specific
sided effusion , for example, whereas esophageal rupture,
trans-diaphragmatic rupture of splenic abscess produce a
left sided effusion, sub-phrenic and liver abscess ,
hydatid disease will rupture into the right pleural
space. None of these cases were however encountered in this
study.
Mediastinal shift was recorded in 72% of cases, usually
to the contralateral side, and mainly observed in
massive effusions. But in some cases, either no shift
is observed or an ipsilateral shift may even be
observed. This occurs if there if there is narrowing of
ipsilateral mainstream bronchus, which can be caused by
carcinoma, atelectasis, fixation of the mediastinum due
to fibrosis of chronic inflammation or tumour
infiltration of the mediastinal nodes of ipsilateral
lungs,
The pathologic condition responsible for pleural effusion
in each case was nearly always identified following
Page 99
_____________________________________________________________________ 99
structured application of clinical methods via history,
physical examination , laboratory and radiological
evaluation.
Neoplastic disease was identified in 40.7% of all cases
studied, followed by pulmonary tuberculosis in 37.2% and
pneumonia in 22.1% of all cases. This showed that
malignant pleural effusions was almost twice commoner
than para-pneumonic pleural effusion. Further analysis of
the causes of malignant pleural effusions showed that
breast carcinoma was responsible for 65% ,about 2/3 of
all cases of malignant effusion , while the rest
encountered including, lungs, intra-abdominal, soft tissue
sarcoma and parotid carcinoma constituted the rest 1/3.fig
16.
All the medical causes of pleural effusion such as
congestive cardiac failure as well as traumatic
haemothorax were excluded from this study. Other surgical
causes of pleural effusion were not encountered in this
study, probably due to their rarity in this environment.
Treatment directed at the primarily associated pathology
was either initiated and/or consolidated.
In most tuberculous and parapneumonic pleural effusions,
the aim of surgical intervention via chest intubation is
to alleviate life threatening cardio-respiratory
insufficiency while allowing adequate time for the
chemotherapeutic agents to act towards curing the
patient.
Page 100
_____________________________________________________________________ 100
This contrasts sharply with the situation in malignant
effusion.To improve the quality of life of the patient,
the least invasive, least morbid, and least costly therapy
should be employed in managing malignant effusions. This
is because most of these patients have limited survival.
Hospitalization should be minimized, so that patients are
not unnecessarily removed from the family.
In this study, 94% of all cases had tube thoracostomy
and underwater seal drainage , while an additional low
suction was applied in 4.6% cases, the aim of which
was to encourage completeness of drainage. 37% of these
case required further pleurodesis which is aimed at
discouraging fluid re-accumulation, a situation which
applied mostly in malignant pleural effusions. The
diagnosis of a malignant pleural effusion signifies a
poor prognosis because it is usually a manifest of far
advanced disease. In a meta-analysis of 417 patients with
malignant effusion, the survival period was 4 months.
Hence treatment should not be heroic but directed at
alleviating and improving the quality of life as much
as possible. Exploratory thoracotomy was offered to only
6.9% of patients , indicated only in cases that required
decortication.
The outcome of treatment in malignant pleural effusion
was uniformly fatal as up to 71% were dead at 6
months of diagnosis, while 25% were seriously battling
the disease at 6 months check-up, despite all treatment
modalities. Only one case (2.9%) showed a clinical
evidence of absence of disease at 6 months check-up.
This high mortality/morbidity seen in malignant effusions
Page 101
_____________________________________________________________________ 101
comfirms Heffner .J.E. et al position that the diagnosis of
malignant pleural effusion signifies a poor prognosis
because it is usually a manifest of a far advanced
disease, with a median survival of 4 months.
Conversely, 51.7% of tuberculous pleural effusions showed
both clinical and radiological evidence of complete
recovery at 6 months check-up, while 31% were still
battling the disease and 17.2% had progressed to further
complication and death in-spite of all treatment. It was
however not clear if the co-morbid conditions which was
found in some of these cases contributed to this
mortality, but this is outside the scope of this
study, and indeed is worth futher researching into.
88% of the parapneumonic cases recovered completely,
while 11% had partial recovery at 6 months check.
Some of the latter indeed progressed to empyema
thoracis. This high rate of complete recovery and very
low rate of progression to empyema thoracis can be
attributed to availability and early exhibition of
antibiotics.
This study therefore confirmed that parapneumonic effusions
had the best outcome , followed by tuberculous and
malignant ones having an abysmally low outcome.
Common complications observed in the course of treatment
include premature dislodgement of chest tube which was
observed in 33.72% of all cases intubated. Closely
related to that is pneumothorax which was observed in
9.3% of all cases. This complication was directly
Page 102
_____________________________________________________________________ 102
related to poor surgical technique even as some patients
have been blamed for pulling on the tube. Treatment was
directed to improving surgical technique by employing the
appropriately trained personnel and ensuring that tube is
positioned or repositioned and tightly secured with
appropriate sutures. Contamination and infection of a
previously sterile pleural effusion was observed in 10.4%
of cases while wound sepsis around the thoracostomy
site was observed in 33.7% of cases. Both were directly
related to non adherence to strict aseptic technique
during the procedure of chest tube insertion, especially
during emergencies. Treatment here was by preventive
measures and the use of appropriate antibiotics.
Recurrent effusion was recorded in 40.7% of cases
especially in malignant and tuberculous pleural effusions.
In malignant pleural effusions, recurrence is due to
persistent and indeed the progression of the primary
disease in spite of the exhibition of multimodality
treatment especially in advanced/metastatic diseases. In
tuberculous pleural effusion it is mainly due to
persistence of infection following drug resistance and/or
non-compliance to medication. It may also be related to
advanced disease state. Treatment of recurrence was by
repeat chest intubation and pleurodesis for malignant
effusions . In tuberculous cases, repeat chest drainage,
review of anti-koch’s medication were the hallmarks of
treatment. Exploratory thoracotomy and/ decortication were
indicated in very few cases.
In conclusion, this study was able to expose the common
causes of pleural effusion requiring surgical intervention in
National Hospital Abuja. The diagnostic armaments and
Page 103
_____________________________________________________________________ 103
their uses , treatment modalities and limitations , the
outcome of treatment as it applies to the different
diseases and the common complications of treatment
observed were equally exposed, hence providing a platform
for improvement in the management of patients suffering
from this disease.
Page 104
_____________________________________________________________________ 104
REFERENCES
1. Jan Langman, Formation of body cavities and
Serous Membrane; Medical Embryology, Fourth
Edition, Page 144. 1984.
2. Jan Langman, Formation of Diaphragm and Thoracic
Cavity; Medical Embryology, Fourth Edition, Page
144. 1984.
3. Bhattachariya S.K., Surgical Physiology of
Rate and Directionof Fluid Movements; ShortCases
in Surgery, Fourth Edition, Page191, 1978.
4. Anyanwu C.H., Pleural Effusions, Thoracic
Surgery; Principles and Practice of Surgery and
Pathology in the Tropics, Third Edition, Page 427
5. Friedrick M.A., Pleural Effusion; e-medicine,
http://www.e-medicine.com/emerg/topic462.htm,
page 6 of 32.
6. Ibid.
7. Adegboye V.O., Ladipo J.K., Adebo O.A., Yellow
Page 105
_____________________________________________________________________ 105
Nail Syndrome and Bronchiectasis; Nigerian
Journal of Surgical Research, Volume 4, No 3,
2002, page 115 – 118.
8. Anyanwu C.H., Thoracic Surgery , Principles and
Practice of Surgery and Pathology in the Tropics,
Third Edition, Page 427.
9. Abrahamian F.M., Pleural Effusion; e-medicine,
http://www.e-medicine.com/emerg/topic462.htm.
Page 6 of 32.
10. Ibid.
11. John.A.H., Parapneumonic effusions in pediatrics,
http://www.pediatrics uchicago.edu/chiefs/am
report/parapneumonic effusion-files/slide
0006.htm.
12. Alkrinawi .S. Respiratory Infection in
Children;emedicine,http://www.ipeg.org/guidelines
/empyema.ht.ml.
13. Kussabe R.B.,Rare Causses of Pleural Effusion:
African Health Science,2001 (2) : 97-98.
14. Raymond.H., Michael .B., Empyema: Essentialss of
Thoracic Surgery: page 105,1996.
15. Kusabe .R.B., Rare Causes of Pleural Effusion:
African Health Science, 2001 (2) 97-98.
Page 106
_____________________________________________________________________ 106
16. Lesi O.A., Kehinde M.O., Massive Haemorrhagic
Pleural Effusion-an unusual presentation of
endometriosis, Nigerian Medical Practitioner,
volume 44 (1) 2003, 22-44.
17. Basssey . J.A, Graham .A. Gould, Pleural
Deposits from Light Chain Myeloma- an unusual
cause of pleural effusion: Archives of Ibadan
Medicine, volume3 (2) 2002, 64-65.
18. Abrahamian.F.M.,PleuralEffusion
e-medicine,http://www.emedicine.com/emerg/
topic462.htm.Page15 of 32.
19. Robbins.J.,Pleural Effusion,e-medicine,
http://www.e-medicine.com/med/topic 1843 html.
20. Abrahamian .F.M.,Pleural Effusion,
e-medicine,http://www.e-medicine.com/emerg/topic
462. htm. Page 15 of 32.
21. Rafel.S. et al., Management of Pleural effusion,
http://www.medscape.com/viewarticle/535594
22. Abrahamian.F.M.,PleuralEffusion,
e-medicine,http://www.e-medicine.com/emerg/topic
462.htm.page 15 of 32.
23. Ibid
24. Robbins Jeffery,Pleural Effusion,
Page 107
_____________________________________________________________________ 107
e-medicine,http://www.e-medicine.com/emerg.
PAGE 3 of 18.
25. Heimlich,H.J., Valve Drainage of Pleural Cavity;
Diseases of the Chest. 53:282,1968.
26. Oluwole Adebo,The Value of Chest Intubation In
The Initial Management of Chest Trauma In a
Developing Country; African Journal of Trauma;
May 2004 – Nov 2004, Vol 2(no 2-4) .page 76-79.
27. Adegboye V.O, Adebo O.A, Ossinowo .O., Brimmo:
Closed Chest Drainage Without an Underwater
Seal. African Journal of Medical Sciences 1996,
25 (4) 353-5.
28. Cancer Bacup- Management of Pleural Effusion,
http://www.cancerbacup.org.uk/resources support.
29. Snow.J.A.Parapneumoniceffusions in children.
http://pediatrics uchicago.edu/chief/AM
report/parapneumonic effusion
30. Indu,D,Aprim, YY; Surgery on CD Rom, Johnson and
Johnson Professional Export. African Health Care
[email protected] .
31. Walker RPB,Voughan LM, Sahn SA, chemical
pleurodesis for malignant pleural effusions.
Annals of Internal Medicine 120(1): 56-64;1994.
32. Hartman DL, Gaither J.M, Kesler K.A et al.
Page 108
_____________________________________________________________________ 108
Comparison of insufflated Talc under
laparoscopic guidance with standard tetracycline
and bleomycin for control of malignant pleural
effusion .Journal of Thoracic and CardioVascular
Surgery,105(4):743-748,1993.
33. Ezeome E.R. et al. Use of tetracycline
capsules for pleurodesis in breast cancer
patients with malignant pleural effusion.Journal
of College of Medicine, University of Nigeria
Nsukka,2005:9(2) :82-84 .Published in African
Journal On Line (AJOL).
34. Carolyn Clary-Macy,Chemical pleurodesis for
pleural effusion, UCSF, Thoracic Surgery http:
//www.cancersupportivecare.com/pleural
html.pg2/2. 2005.
35. Arigoni C ,Tisi E, Ballabio D, Cassina E
et al.Neoplastic Pleural Effusion.
Our Therapeutic Progress . page 5/13
http:// www.chirurgia
thoracica.org/pleuri-effusion-maligne-htm.
36. Jacobs L.M, Hsieh J.W.,A Clinical Review
Of auto-transfusion and its role In trauma,
Journal of American Medical Association
251:3283,1984.
Page 109
_____________________________________________________________________ 109
Proforma for Analysis
(A) Bio-data
Name
Age
Sex
Hospital No.
Tribe
Town / City of Residence
Occupation
Marital Status
(B) Presenting Complaints
YES NO
Breathless
Cough
Chest Pain
Fever
Wt Loss
Others
Page 110
_____________________________________________________________________ 110
(C) Associated Pathology
Present Absent
Neoplastic disease
Tuberculosis (PTB)
Pneumonia
Connective Tissue
Disease
Recurrence
Others (Pls specify)
D. Type of Neoplastic Disease
Present Absent
Breast CA
Lungs CA
Soft Tissue Sarcoma
Intra Abdominal Malignancy
Parotid CA
Others.
E. Findings on Physical Examination
Parameters present Absent
Pallor
Cynosis
Features of respiratory distress e.g., RR,
Flaring of alar nasi, sweating etc
Trachea Deviation
Increased Chest Excursion
Decreased Chest Excursion
Increase Percussion Note
Decreased Percussion Note
Normal air entry
Any Added sounds
Abnormal Heart sound
Distended Neck Veins
Page 111
_____________________________________________________________________ 111
F. Investigative findings
Pleural Fluid Collection – Physical Characteristics
Yes No
Air -
Liquid: - blood:
- Straw colored
liquid
- Pus
- Chyle
- Clear Liquid
- Sero - Sanguinous
G. Pleural Fluid Aspirate Analysis
Chemistry Control Level
Specific Gravity
- glu
- Prot
- LDH
- Serum LDH
- P. LDH/S.LDH
- PH
- TG
Cholesterol
TG / cholesterol
Na+
- Cl-
- K+
-HCo3-
Transudate
Exudate
Microbiology
Present
Absent
- AFB
- MCS
- Pus Cell
- Fungal
Cytology
Present
Absent
- WBC
- RBC
- Malignant Cells
Page 112
_____________________________________________________________________ 112
H. Radiological Findings
Chest X-ray – PA View <25% 25-50% >50%
Normal Study
(R) Hydrothorax
(L) Hydrothorax
Bilateral Hydrothorax
(R) Pneumothorax
(L) Pneumothorax
Bilaterial Pneumothorax
Hydropneumothorax
Mediastinal shift
CT - chest
State Findings (If any, pls) Yes
No
I. Treatment Modality
Yes No
- Observation
(Serial chest X-ray)
- Needle Aspiration
- Tube thoracostomy +
Under – Water Seal Drainage
- Tube Thoracostomy +
Under – Water Seal Drainage + Low
Suction
- Rib – resection + Eloesser Window
- Thoracotomy (Exploratory)
- Pleurodesis
- Decortication
- Pneumonectomy
- Pleuro – peritoneal shunt
- Video thoracoscopy with debridement of
pleural
Instillation of streptokinase
Others (Pls. specify)
J. Treatment of Other Concomitant disease Condition
Please specify Yes ……… Or No ………….
Page 113
_____________________________________________________________________ 113
K. Outcome of Treatment
Complete Recovery Complication
Pneumonia
Pulmonary tuberculosis
Neoplastic Diseases
Constrictive Pericaditis
Chronic Liver Disease
Congestive Cardiac
Failure
Chest Trauma
Connective tissue
Disease
Others (pls. specify)
L. COMMON COMPLICATION OBSERVED
Present Absent
Premature Dislodgement of Tube
Pneumothorax of Tube
Wound Sepsis E.g., Meleny’s
Gangrene
Progressive Empyema Thoracis
Recurrence
M. Treatment of Recurrence
Yes No.
Needle Aspiration
Tube Thoracostomy
Eleasar Window
Pleurodesis
Decortication