Tracheostomy Audit: Factors affecting tracheostomy outcome in critically ill patients Dr Carren Teh Dr Lye Meng Hon Dr Megalah a/p Selvamani Dr Sobani Bin Din Dr Fadzilah Ismail Improving post tracheostomy complication rates in Hospital Sungai Buloh 1
Transcript
1
Tracheostomy Audit: Factors affecting tracheostomy outcome in
critically ill patients
Dr Carren Teh Dr Lye Meng Hon
Dr Megalah a/p Selvamani
Dr Sobani Bin Din Dr Fadzilah Ismail
Improving post tracheostomy
complication rates in Hospital Sungai Buloh
2
OUTLINE OF PROBLEM
3
• 20 May 2006 – commencement of service• 3 sub-units : ENT, Audiology dan Speech and swallowing therapy
Problems Identification
1. High post tracheostomy complication rate2. Synechia post nasal operations3. High incidence of hearing impairment not
detected at birth
4
5
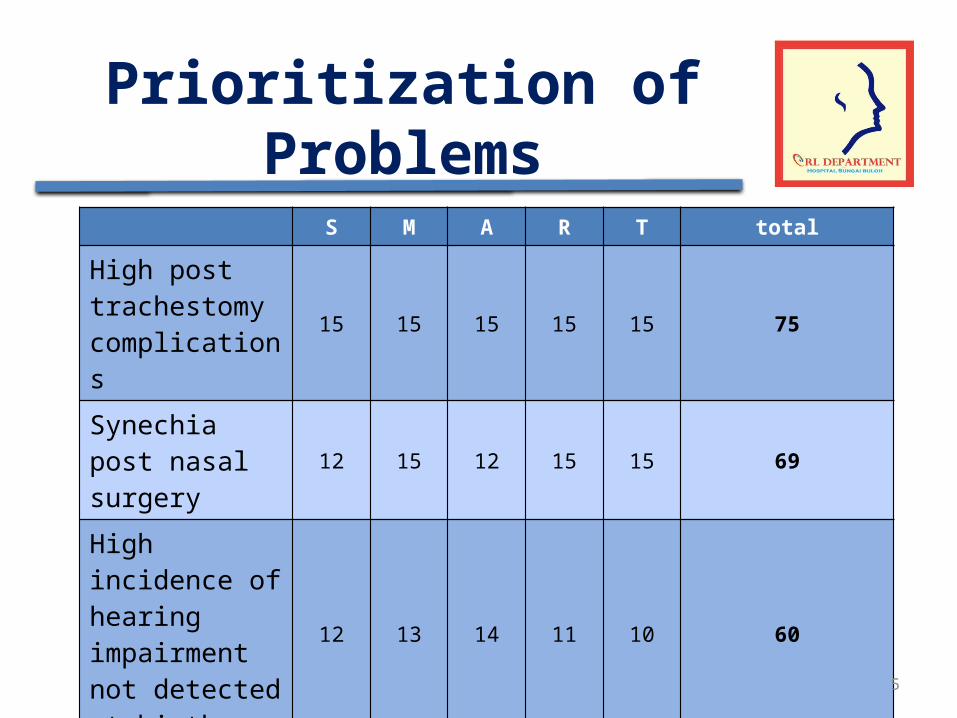
Prioritization of ProblemsS M A R T total
High post trachestomy complications
15 15 15 15 15 75
Synechia post nasal surgery 12 15 12 15 15 69
High incidence of hearing impairment not detected at birth
12 13 14 11 10 60
6
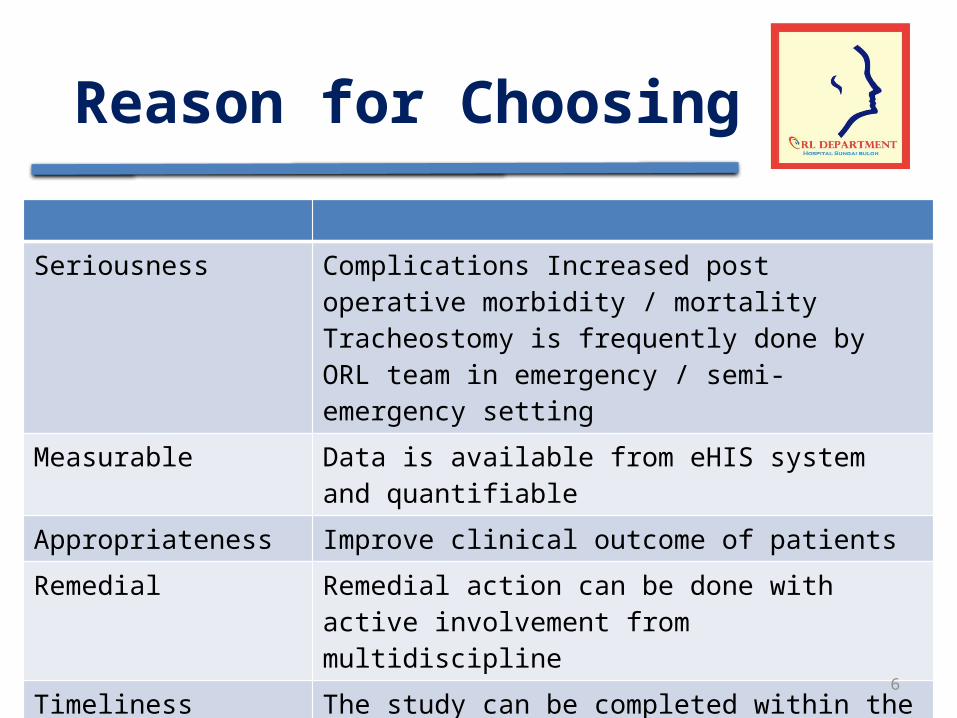
Reason for Choosing
Seriousness Complications Increased post operative morbidity / mortalityTracheostomy is frequently done by ORL team in emergency / semi-emergency setting
Measurable Data is available from eHIS system and quantifiable
Appropriateness Improve clinical outcome of patients
Remedial Remedial action can be done with active involvement from multidiscipline
Timeliness The study can be completed within the short period of time
7
Reasons for Rejection
• Synechia post nasal surgery– Less severe complication– Infrequent number of cases
• High incidence of hearing impairment not detected at birth– Remedial measures require increase in resources
(beyond control of department)– High risk screening program already in place
2008 2009 2010 2011 2012 2013 20140
20
40
60
80
100
120
140
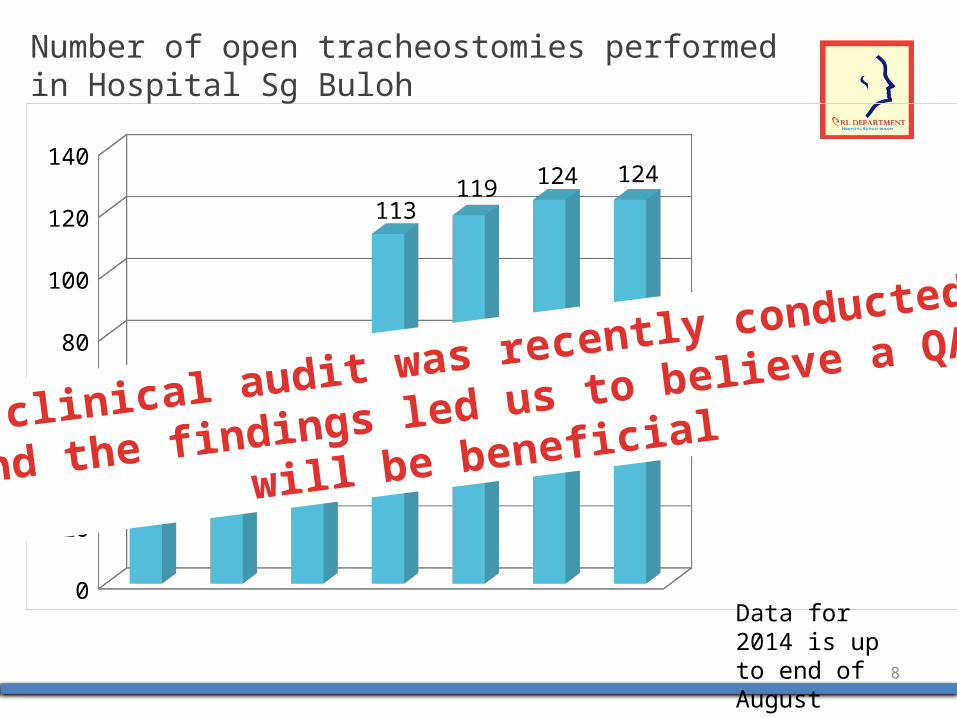
41
65 64
113119 124 124
Number of open tracheostomies performed in Hospital Sg Buloh
Data for 2014 is up to end of August
A clinical audit was recently conducted
and the findings led us to believe a QA
will be beneficial
8
9
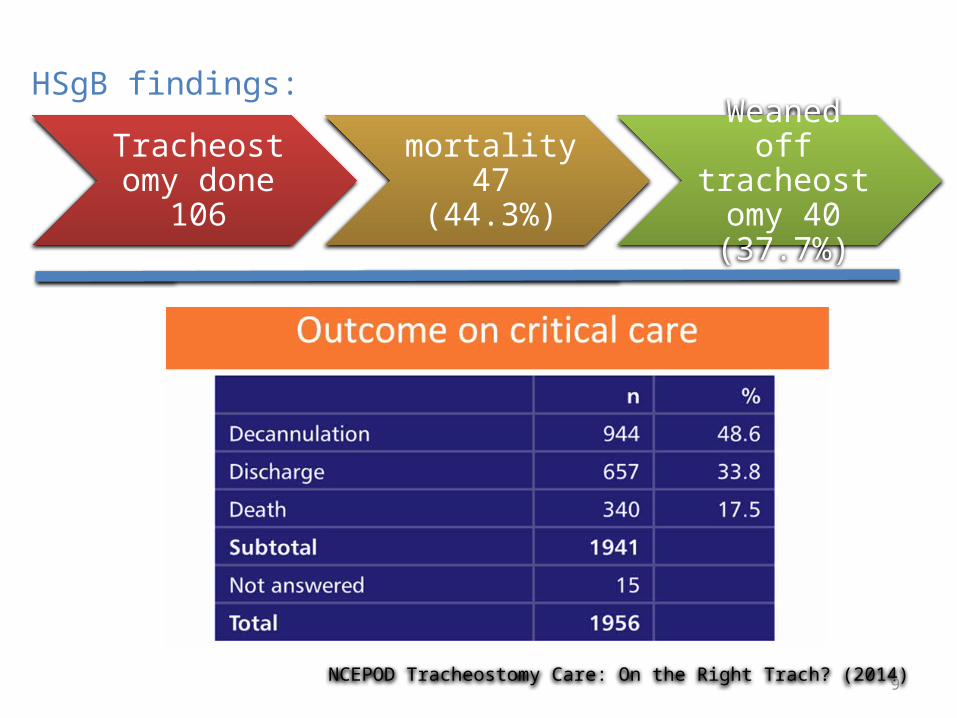
Tracheostomy done 106
mortality 47 (44.3%)
Weaned off tracheostomy
40 (37.7%)
NCEPOD Tracheostomy Care: On the Right Trach? (2014)
HSgB findings:
10
Mortality rates
Overall 30 day mortality rate is 15-25%
AE Kejner, Castellanos PF, Rosenthal EL, MT Hawn. All-Cause Mortality after Tracheostomy at a Tertiary Care Hospital over 10- Month period. ORL-
Head and Neck Surg. 2012; 146 (6): 918-22
11
• Factors significantly improving survival– Indian race– Absence of co-morbidities– Normal platelet values
• Factors significantly improving success of weaning– Presence of co-morbidities
• Factors giving rise to failure of weaning– Duration of intubation less than 7 days
POSSIBLE KEY MEASURES FOR IMPROVEMENT
NOT PRACTICAL!
12
Complication rates
Tracheostomy-related complications were reported for 6.3% and most common complication was bleeding
D Young, DA Harrison, B Cuthberson, Effect of Early vs Late Tracheostomy Placement on Survival
in Patients Receiving Mechanical Ventilation The TracMan Randomized Trial. JAMA. 2013;309(20):2121-2129
HSgB Post operative complication : 10.4%
13
Complication rates
• The 6% rate of major or serious insertion complications – major bleeding, posterior tracheal wall injury, pneumothorax and death
• The majority (5% overall rate) of the major insertion complications were related to bleeding
AJ Glossop, TC Meekings, SP Hutchinson, SJ Webber Complications following tracheostomy insertion in critically ill patients – experience from a large teaching hospital. JICS The Intensive Care Society 2011 Volume 12, Number
4, October 2011
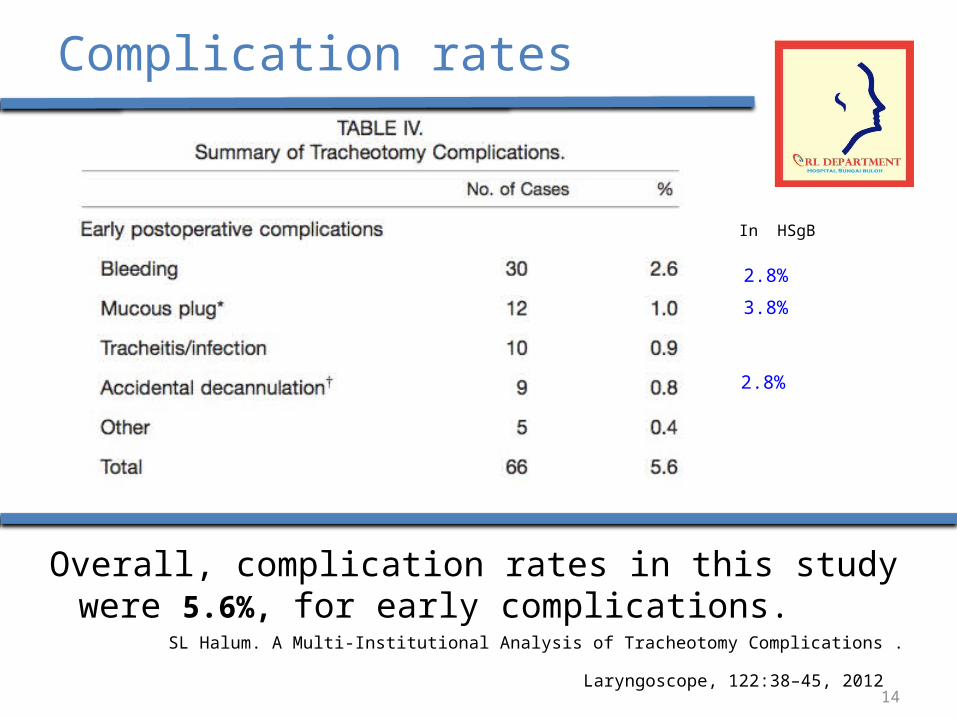
Complication rates
Overall, complication rates in this study were 5.6%, for early complications.
SL Halum. A Multi-Institutional Analysis of Tracheotomy Complications . Laryngoscope, 122:38–45, 2012
2.8%
3.8%
2.8%
In HSgB
14
15
Improving post tracheostomy complication rates in Hospital
Sungai Buloh
16
Nursing Care
Excellent nursing care is the cornerstone for reducing the morbidity and postoperative complications of tracheostomy.
B Huffman, H Emam, M Stevens. Tracheostomy with emphasis on perioperative nursing care. Journal of Nursing Education and Practice, 2014,
Vol. 4(3). 13-19
17
STANDARDIZED TRAINING
A standardized education module for tracheostomy care teaching resulted in significant increases in provider knowledge and confidence.
JC Yelverton, JH Nguyen, W Wan, MC Kenerson, TA Schuman. Effectiveness of a standardized education process for tracheostomy care. Laryngoscope 2014
Jul 8. Epub 2014 Jul 8.
18
Problem Statement
• What: high post trachestomy complication rate• Who: critically ill patients, healthcare providers,
family members• When: pre-, intra- and post-op• Why: to improve patient outcome• How: proper pre-op preparation, improving post
operative nursing care, provide adequate training
19
Goal
• To reduce post tracheostomy complication rates.
• To reduce mortality rate of post tracheostomy patients.
20
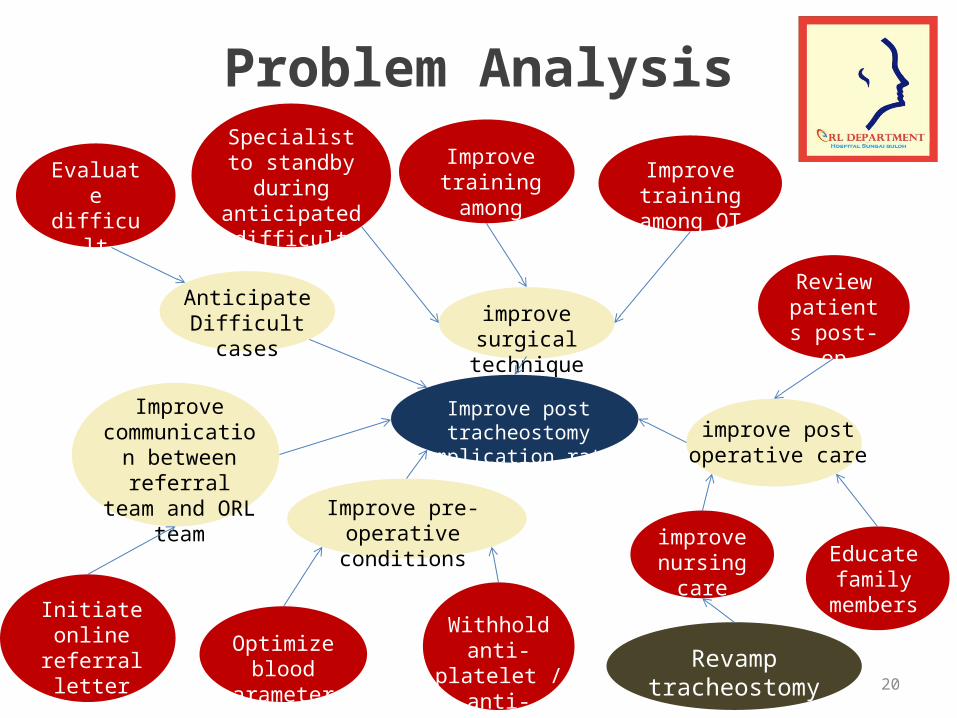
Improve post tracheostomy complication rates
improve surgical technique
Improve training among surgeons Improve training
among OT staff
Anticipate Difficult cases
Optimize blood parameters
Evaluate difficult
anatomy
Improve pre-operative conditions
Withhold anti-platelet / anti-
coagulant
improve post operative care
improve nursing care Educate
family members
Problem AnalysisSpecialist to
standby during anticipated
difficult cases
Review patients post-op
Improve communication
between referral team and ORL
team
Revamp tracheostomy care course
Initiate online referral letter with checklist
21
Study Objectives
General objective:• To reduce the percentage of post tracheostomy
complication in Hospital Sungai Buloh
Specific objectives:• To identify contributing factors• To formulate intervention strategies• To carry out remedial action efficiently
22
Key Measures For Improvement
23
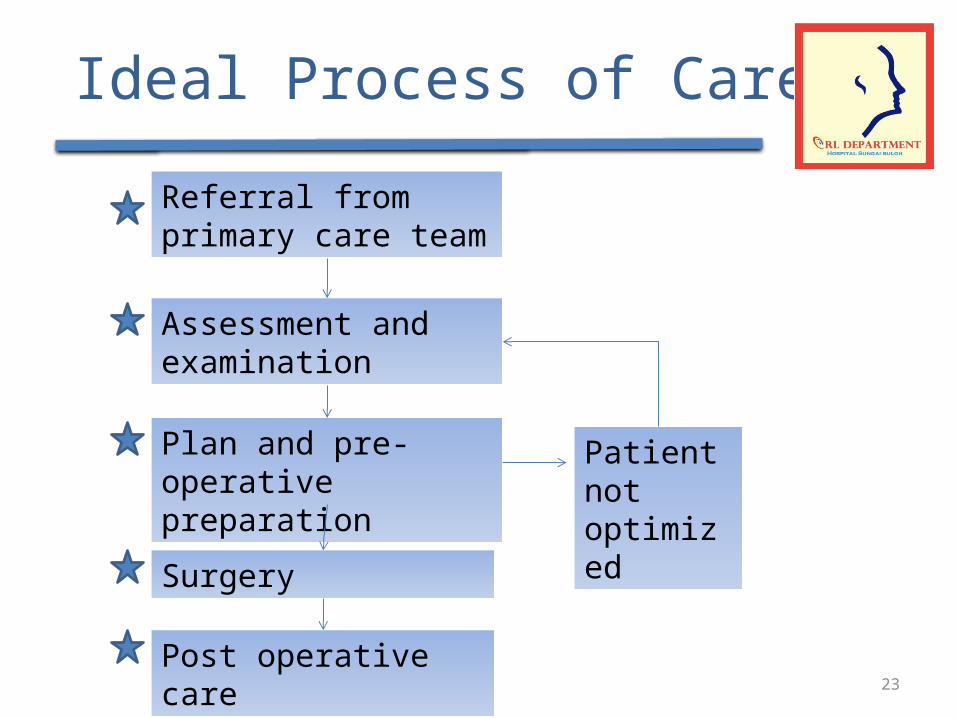
Ideal Process of Care
Referral from primary care team
Assessment and examination
Plan and pre-operative preparation
Patient not optimized
Surgery
Post operative care
24
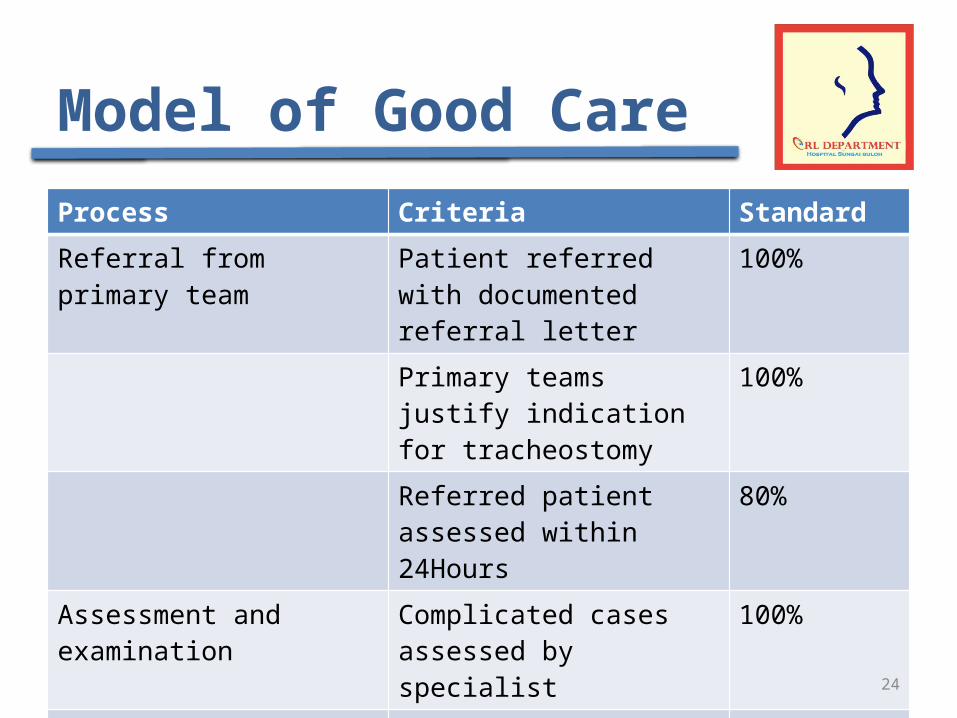
Model of Good CareProcess Criteria StandardReferral from primary team Patient referred with
documented referral letter100%
Primary teams justify indication for tracheostomy
100%
Referred patient assessed within 24Hours
80%
Assessment and examination Complicated cases assessed by specialist
100%
All patients with anterior neck swelling to undergo USG -neck
100%
Results of lab tests and previous results are ready
100%
25
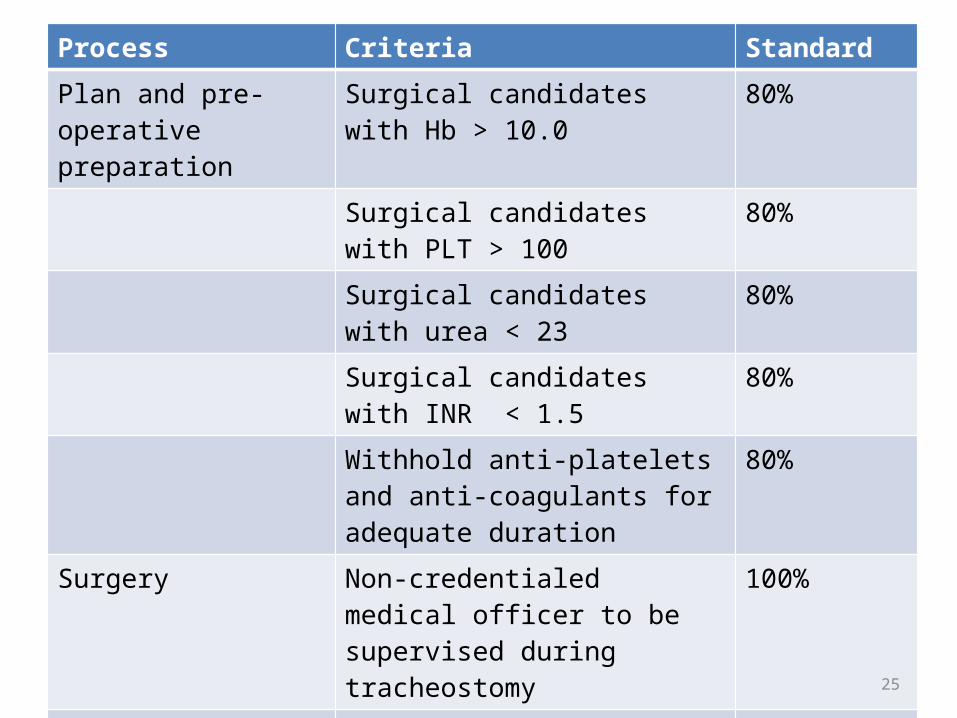
Process Criteria StandardPlan and pre-operative preparation
Surgical candidates with Hb > 10.0 80%
Surgical candidates with PLT > 100 80%Surgical candidates with urea < 23 80%Surgical candidates with INR < 1.5 80%Withhold anti-platelets and anti-coagulants for adequate duration
80%
Surgery Non-credentialed medical officer to be supervised during tracheostomy
100%
Specialist to standby during anticipated difficult tracheostomy
100%
Post operative care Post –op assessment by surgeon on post op Day 1
100%
ORL medical officer to review patient during trachy tube first change
100%
26
Indicator and Standard
• Indicator:= number of patients with post tracheosotmy complications total number of patients undergoing tracheostomy
• Standards:– Post tracheostomy early complications: 5.6%
x 100
SL Halum. A Multi-Institutional Analysis of Tracheotomy Complications . Laryngoscope, 122:38–45, 2012
27
PROCESS OF GATHERING INFORMATION
28
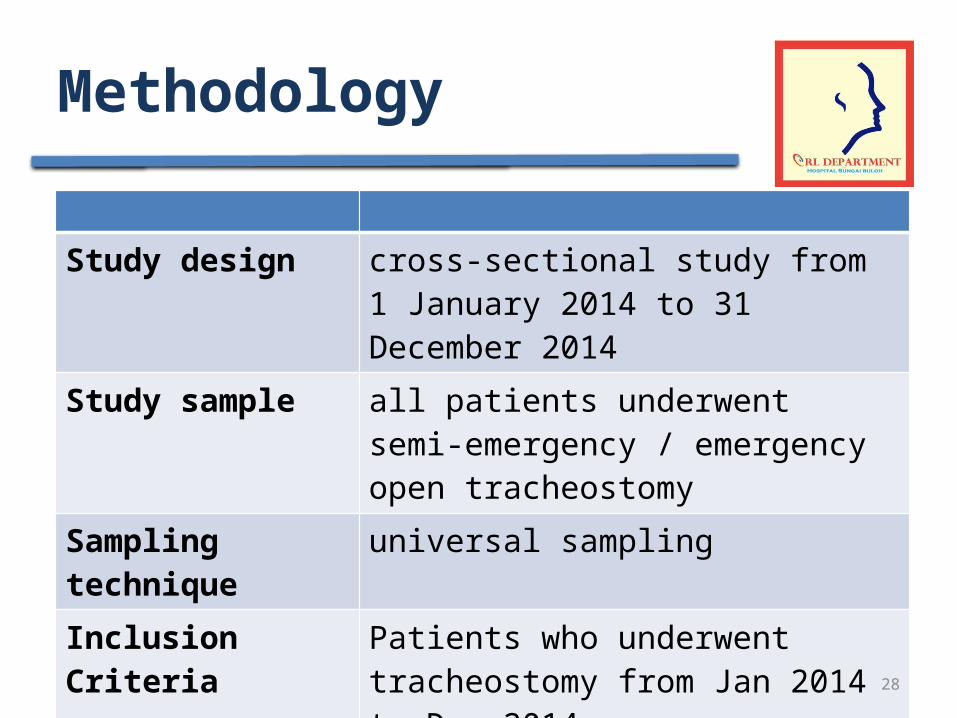
Methodology
Study design cross-sectional study from 1 January 2014 to 31 December 2014
Study sample all patients underwent semi-emergency / emergency open tracheostomy
Sampling technique universal samplingInclusion Criteria Patients who underwent tracheostomy
from Jan 2014 to Dec 2014
Exclusion Criteria ENT CasesElective CasesIncomplete data
29
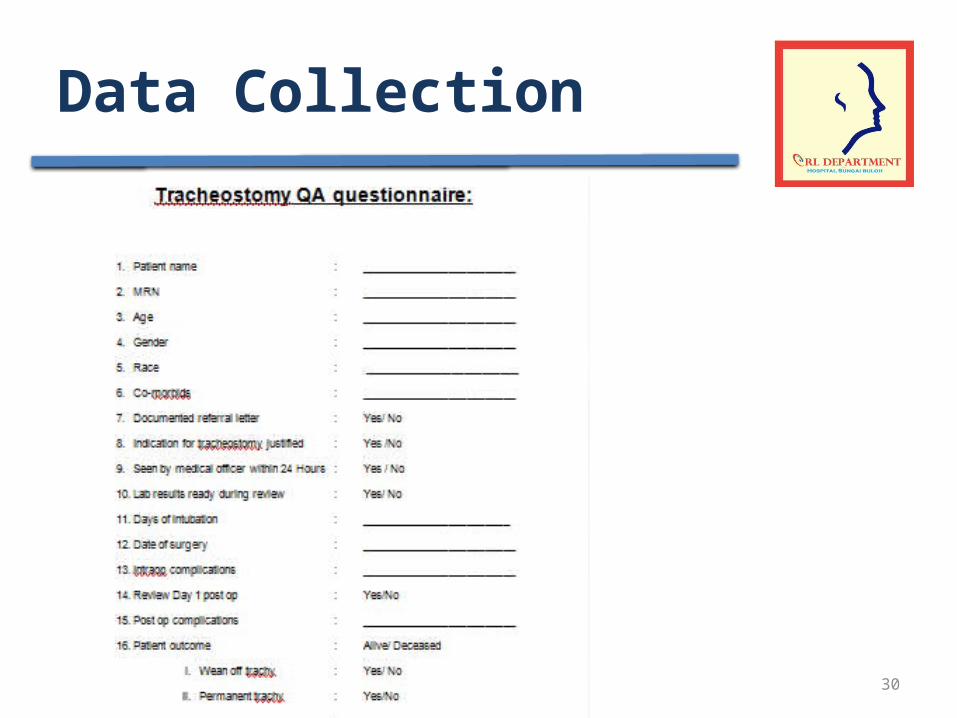
Data Collection Method
• Duration of study– Verification Study: 2 weeks– Remedial measures : 3 months– First phase study: 1 month
• Instrument– IT recorded sources (eHIS)– Checklist with data tabulation
• Data analysis– SPSS / Excel
30
Data Collection
31
Strategies
• To initiate a new online referral letter form in eHIS which incorporates a checklist– Valid indication for tracheostomy.– Lastest blood investigation .
• To revamp tracheostomy care courses / workshop – Tracheostomy care courses for health care