Page 1
To view an archived recording of this presentation please click the following link: http://pho.adobeconnect.com/p86z3rm8kfb/ Please scroll down this file to view a copy of the slides from the session.
Page 2
PublicHealthOntario.ca
Helpful tips when viewing the recording:
• The default presentation format includes showing the “event index”. To close the events index, please click on the following icon and hit “close”
• If you prefer to view the presentation in full screen mode, please click on the following icon in the top right hand corner of the share screen
Page 4
Using gut microbes as therapy
for C.difficile infection
and beyond Emma Allen-Vercoe
University of Guelph
PHO Rounds Microbiology
October 8th 2015
Page 5
Presenter disclosure
• Faculty: Emma Allen-Vercoe
• Name of the commercial interest:
Nubiyota LLC
• Nature of the relationship: Co-founder
and scientific advisor
NuBiyota Better ecosystem, better health
Page 6
Only very few microbes are pathogens In fact, human health depends on microbiota health
We are the vessels for our microbial passengers
https://www.broadinstitute.org/files/news/images/2012/gevers_cover_nature.png
Page 7
There are more bacteria living in your gut
than there are people on the planet…
Gut: 200-500
bacterial
species
Also Archaea as
well as yeasts &
other
microscopic
eukaryotes
Page 8
Everyone is different
Gut microbial ecosystems are highly variable in
composition and abundance profiles between people
http://farm9.staticflickr.com
Page 9
How do we acquire
our microbes?
Toh & Allen-Vercoe, MEHD Feb 2015
Page 10
How do we acquire
our microbes?
Toh & Allen-Vercoe, MEHD Feb 2015
Page 11
What do our gut microbes do for us?
Metabolic
• Fermentation of non-digestible substrates
• Production of vitamins, SCFA
• Removal of toxins, carcinogens
• Differentiation of IECs
Structural
• Intestinal villi and crypts
• Tight junctions
• sIgA production
• Mucus secretion
Protective
• Colonization resistance
• Innate and adaptive
immunity
• Inflammatory cytokine
oversight
Competition
for sites and
nutrients
Immune
system and
barrier
function
Antimicrobial
secretion Energy
After Cryan et al.
Page 12
We exist with our microbes in a delicate
state of equilibrium
http://eco-chick.com/2008/10/1621/still-rock-n-roll-the-balanced-stone-art-of-shane-hart/
Page 13
Maintaining the equilibrium
High diversity of species:
•Healthy ecosystem
•Balance
•Functional redundancy
•Resistance to disease
Low diversity of species:
•Sick ecosystem
•Imbalance
•Functional disability
•Susceptibility to disease
Page 14
‘Extinction events’ may impact health • Hygiene hypothesis
– We are preventing proper colonization by being too clean
• Missing microbiota hypothesis – Blaser & Falkow Nature Reviews Microbiology 2009
– We are disturbing proper colonization across generations through e.g. antibiotic use, poor diet, over-sanitary lifestyle
• Antimicrobial use (especially in early childhood) may be particularly problematic
• Highly refined Western-style diet exacerbates the problem further
http://www.medicaldrugeffects.com/save-environment/
http
://paren
ting1
.kno
ji.com
/paren
tal-examp
le-in-d
rug-p
reventio
n/
http
://cast-science.b
logsp
ot.ca
Page 15
• Several studies have shown:
– Gut microbiota changes significantly with
antibiotic use
– Takes a long time afterwards to return to
baseline
– Sometimes does not return to baseline at all
– Repeated ‘hits’ cause vast changes from
which the ecosystem does not recover
Looft et al., PNAS 2012; Robinson & Young Gut Microbes. 2010; Jakobsson et al. PLoS One. 2010;
Antonopoulos et al., Infect Immun. 2009; Dethlefsen et al. PLoS Biol. 2008.
Page 16
• Lack of microbial
diversity
• Loss of
‘keystone’
species
• Overgrowth of
opportunistic
pathogens
• Poor diet/lifestyle
• Drug interactions
DISEASE
“Dysbiosis”
• How do we look inside the black box?
• How do we study it?
Page 17
Examples of diseases associated with
reduced gut microbiota diversity (published research)
Infant colic
Neonatal necrotizing enterocolitis
Obesity
Inflammatory bowel diseases
Clostridium difficile infection
Eczema Colorectal cancer
Allergic asthma Celiac disease
Autism
Irritable Bowel Syndrome
Page 18
• The Good
• Lactic Acid Bacteria
(LAB)
– E.g. Bifidobacterium
and Lactobacillus spp.
• Butyrate-producing
bacteria
– E.g. Faecalibacterium
prausnitzii, Roseburia
spp.
• The Bad
• Opportunistic
pathogens
– E.g. E.coli,
Pseudomonas
aeruginosa,
Clostridium difficile,
Bacteroides fragilis
• Sulfate-reducing
bacteria
– E.g. Desulfovibrio spp.
The Ugly: it really is not that clear-cut
What’s inside the black box?
Page 19
Some microbes are like bad teenagers in a
subway station…
In a crowded
environment they tend to
behave well
When the crowds are gone,
they tend to start behaving
in antisocial ways
Wikimedia commons images
Page 20
C.difficile:
a ‘bad teenager’
Normal colon
Non-spore-forming anaerobes predominate;
C.difficile absent or numbers low
Antibiotics
-clindamycin
-cephalosporins
-ampicillin
Vancomycin or
metronidazole
Symptoms abate
Cessation of therapy
Return to normal
Reduction in major
genera of anaerobes:
C.difficile grows
to high numbers
C. Carlucci, A-V lab, 2012
Production of
exotoxins A and B
Diarrhea
Ulceration
of colon
Death Wikimedia commons
Page 21
So, C.difficile is a pathogen that
needs to be destroyed!
• We need to throw our best chemical
weapons at it to rid ourselves of the
scourge!
• …NO, this is NOT the best strategy
http://forums.bistudio.com/showthread.php?98772-Grenade-Throwing-Animation
Page 22
We simply need to
repopulate the subway
…but how do we do that?
Page 23
The human gut microbiota is
a complex microbial
ecosystem
http://www.sciencephoto.com
Its function and behaviour
is best studied as a whole
Page 24
Microbes in a microbiology lab… •Almost always exist on their own as part of a
pure culture
•Usually have to adapt to survive this way
•Are often grown logarithmically
•Are usually given access to rich nutrient
sources
Microbes in nature… •Almost always exist as part of microbial
communities
•Benefit from their microbial friends (& host)
•Rarely grow logarithmically
•Rarely have access to rich nutrient
sources
Page 25
…thus, chemostats
can be used to
emulate the human
colonic environment
The human colon is a type of
chemostat…
How do we study the black box?
Page 26
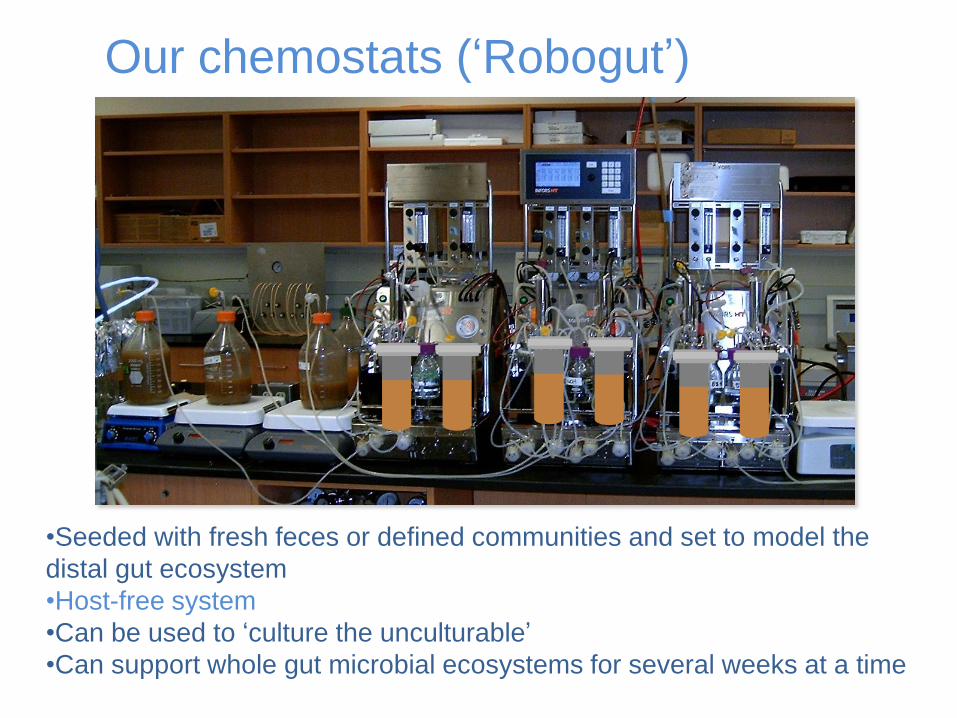
Our chemostats (‘Robogut’)
•Seeded with fresh feces or defined communities and set to model the
distal gut ecosystem
•Host-free system
•Can be used to ‘culture the unculturable’
•Can support whole gut microbial ecosystems for several weeks at a time
Page 27
Microbes ‘talk’ each other using
small molecules
Wikimedia commons images
Many of these small molecules are also absorbed by the host
Page 28
“Liquid gold”
Allows us to eavesdrop on microbial conversations
Page 29
Patterns of perturbation differ between donors Different
people’s
microbiota
responds to
antibiotic
disturbance in
different ways
Kathleen Schroeter and Julie McDonald
Page 30
‘Defined’ microbial ecosystems
• As well as studying fecal ecosystems, we can culture diversity from fecal samples
• Reconstitute into defined ‘experimental’ ecosystems
– Strain composition is known • Genomes, transcriptomes, metabolomes etc. known or
measureable
• Strain composition can be easily (and cleanly) altered
• We can look at deliberate changes in composition and how they affect ecosystem function
Page 31
Defined communities from ulcerative colitis patients
UC1
UC3
Rifaximin treatment
effects vary
according to
community
Kaitlyn Oliphant
Page 32
Yen et al., Journal of
Proteome Research,
2015
1H NMR profiling of
liquid gold
‘Liquid gold’ derived
from different donors
produces metabolic
profiles unique to the
respective hosts
Marc
Aucoin, U
Waterloo
Sandi Yen
Page 33
•Results in cure of the
patient in >90% of cases
•Rapid resolution of CDI
•Only rare recurrence of
disease
•Fresh homogenate instilled
into patient within a few hrs
of preparation •Rectal enema
•Colonoscopy
•Nasoduodenal tube
•“Poop pills”
Back to CDI… FMT: one way to put the people back on the
subway platform…
Page 34
But not without risk…
Known
• Potential to transmit
infection
• Risks of procedure
• Colonoscopy and
associated sedation
Unknown • Changes in
microbiome that increase risk of other diseases (e.g., IBD, cancer, obesity, etc)
• Risk of acquiring new pathogens or infection
• Development of autoimmune disorders
Long-term risks: UNKNOWN
Page 35
Case report: sudden and
unexpected weight gain after FMT
Sciencedaily.com
Alang and
Kelly, 2014
Page 36
What if we could create ‘synthetic stool’ to
treat CDI?
Page 37
Good idea – why hasn’t anyone
done this before?
• They have! Early studies used small number
of gut microbial isolates to treat CDI
– Tvede & Rask Madsen, Lancet 1989
• Fell out of favour with increased antibiotic use
• Difficult to do – most gut anaerobes
(erroneously) thought to be ‘unculturable’
• Prior lack of understanding of the importance
of the gut microbiota to health
Page 38
Steps to MET
1. Find a healthy donor
2. Use chemostat to isolate microbial diversity
3. Characterize, curate and preserve isolates
4. Test for, and remove, undesirable
components
Antibiotic resistance, presence of virulence genes,
toxicity, etc.
5. Assemble, test and optimize ecosystem Determine optimal growth conditions/scalability
Page 39
“RePOOPulate” • Acidaminococcus intestinalis
• Bacteroides ovatus
• Bifidobacterium adolescentis (x2)
• Bifidobacterium longum (x2)
• Collinsella aerofasciens
• Dorea longicatena (x2)
• Escherichia coli
• Eubacterium eligens
• Eubacterium limosum
• Eubacterium rectale (x4)
• Eubacterium ventriosum
• Faecalibacterium prausnitzii
• Lactobacillus casei
• Lactobacillus paracasei
• Parabacteroides distasonis
• Raoultella sp.
• Roseburia faecalis
• Roseburia intestinalis
• Ruminococcus torques (x2)
• Streptococcus mitis
• Likely novel species (x5)
• Likely novel genus & species (x1)
(Closest species by full-length 16S alignment)
Page 40
“RePOOPulate” • Acidaminococcus intestinalis
• Bacteroides ovatus
• Bifidobacterium adolescentis (x2)
• Bifidobacterium longum (x2)
• Collinsella aerofasciens
• Dorea longicatena (x2)
• Escherichia coli
• Eubacterium eligens
• Eubacterium limosum
• Eubacterium rectale (x4)
• Eubacterium ventriosum
• Faecalibacterium prausnitzii
• Lactobacillus casei
• Lactobacillus paracasei
• Parabacteroides distasonis
• Raoultella sp.
• Roseburia faecalis
• Roseburia intestinalis
• Ruminococcus torques (x2)
• Streptococcus mitis
• Likely novel species (x5)
• Likely novel genus & species (x1)
Lachnospiraceae and Ruminococcaceae family species (Generally lacking in CDI, IBD)
Page 41
RePOOPulate proof-of-principle trial
• 2 elderly ladies with severe, recurrent C.diff infections were treated (April and June 2011)
• RePOOPulate made fresh at Guelph, driven to KGH, and administered via colonoscopy
– 1 dose, 100mLs
• Both patients recovered within 2 days and have remained C.diff-free ever since (despite numerous subsequent antibiotic exposures)
Page 43
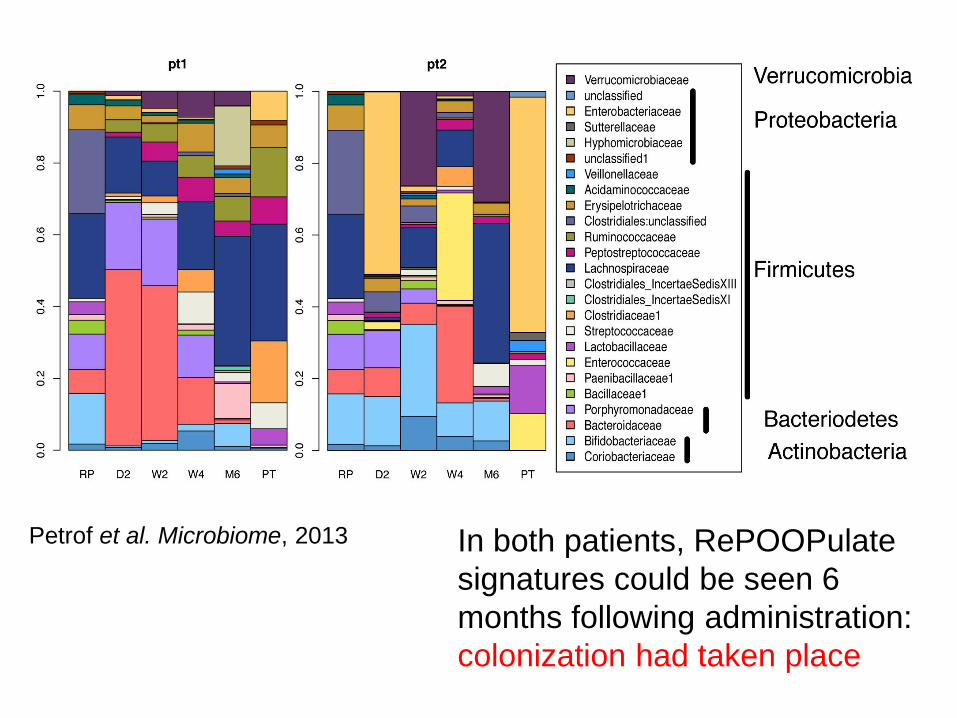
Petrof et al. Microbiome, 2013 In both patients, RePOOPulate
signatures could be seen 6
months following administration:
colonization had taken place
Page 44
Why only n=2? • Trial temporarily stopped by Health
Canada
– Is RePOOPulate/MET1 a probiotic or a biologic drug?
• Health Canada (& FDA): should be considered as a biologic
– Potentially easier to regulate than fecal bacteriotherapy
– But so far, no guidelines for us!
From Health Canada Guidelines for FMT
Page 45
Where we currently are with MET
• Developing MET1+ as well as other METs
from a range of healthy donors
• Creating a QC pipeline
– Based on metagenomics,
metabolomics/metabonomics and other
proprietary measures
• Scale up and stabilization of product
– For encapsulation and simple, oral delivery
– Sounds easy, but it isn’t!
• Gearing up for new clinical trial
Page 46
The challenges
• What’s the definition of a healthy gut microbiota? – Defining species content is likely not enough
• What determines success or failure of engraftment? – And how can we modulate this?
• What are the long-term risks? – (Much easier to measure with a defined MET)
• Can the MET approach be applied for other disease indications?
Page 47
Do we need to match patient to
ecosystem?
Consider different people’s bodies as different
models of car Consider the gut microbiota as an engine
Wikimedia commons images
Page 48
Maybe we should just replace the faulty part of the engine
Birchall et al. in prep
…Ushering in the era of personalized medicine
Page 49
I foresee a time when… • People will regularly have a
microbiome check-up
• Antibiotic use will be minimal and personalized to reduce risk of microbiota damage
• Microbial Ecosystem Therapeutics will enter mainstream medicine
• “Symbiontology” will become a new medical specialty
– A merger of Gastroenterology, microbial ecology, nutrition science, and many other disciplines
Page 50
Acknowledgements EA-V lab members
Christian Ambrose
Erin Bolte
Christian Carlucci
Kyla Cochrane
Michelle Daigneault
Kaitlyn Oliphant
Rafael Peixoto
Kathleen Schroeter
Mariia Taguer
Mike Toh
Sandi Yen
And alumni
Eric Brown
Ian Brown
Julie McDonald
Queen’s U
Elaine Petrof
Adriana Breen
Curtis Noordhof
KGH clinical staff
Western U
Greg Gloor
Jean Macklaim
U Waterloo
Marc Aucoin
NuBiyota Better ecosystem, better health
Page 51
I found the problem, Mr. Smith. Instead of
probiotics, you have been taking amateur biotics.