22
2005 2005 2005 2005 2005 Tobacco Prevention and Control in North Dakota A Status Report of Leading Indicators
20052005200520052005
Tobacco Prevention andControl in North DakotaA Status Report ofLeading Indicators


Tobacco Prevention andControl in North Dakota
A Status Report ofLeading Indicators
John HoeJohn HoeJohn HoeJohn HoeJohn Hoevvvvven,en,en,en,en,Governor of North Dakota
TTTTTerrerrerrerrerry Dwy Dwy Dwy Dwy Dwelle, M.D., M.Pelle, M.D., M.Pelle, M.D., M.Pelle, M.D., M.Pelle, M.D., M.P.H.T.H.T.H.T.H.T.H.T.M..M..M..M..M.State Health Officer
KKKKKaralee Hararalee Hararalee Hararalee Hararalee Harperperperperper, M.M., L.A, M.M., L.A, M.M., L.A, M.M., L.A, M.M., L.A.C..C..C..C..C.Director, Division of Tobacco Prevention and Control
11111

Prepared by:Leana A. Bouffard, Ph.D.Lisa R. Muftic, A.B.D.Dave A. HohnDepartment of Criminal Justice and Political ScienceNorth Dakota State University
Kathleen Mangskau, R.D.H., M.P.A.Former Director, Division of Tobacco Prevention and ControlNorth Dakota Department of Health
Designed by:Cameo SkagerCommunications ConsultantNorth Dakota Department of Health
Acknowledgements:The Division of Tobacco Prevention and Control would like to thank the many individualsand groups who are committed to tobacco control in North Dakota and who contributed tothe progress and achievement of tobacco prevention goals in the state. These groups includelocal programs in communities and schools, local youth groups leading tobacco preventionefforts in their communities, and partner agencies and organizations across the state.
Special thanks to Clint Boots, data analyst for the Division of Tobacco Prevention andControl, for his assistance in data collection and verification.
This publication was supported with funding from the North Dakota Community HealthGrant Program and Cooperative Agreement U58/CCU822794-03 from the U.S. Centersfor Disease Control and Prevention’s Office on Smoking and Health.
22222

Tobacco use remains the number-one preventable cause of premature death and disease inNorth Dakota and the nation. Tobacco-related diseases kill 874 North Dakotans each year. Inaddition to the human toll, tobacco use imposes a significant financial burden on the state.Smoking costs the state $372 million annually in direct medical expenditures and lostproductivity.
In partnership with local health agencies, tribes and communityorganizations, North Dakota has made tremendous gains against tobaccouse. The prevalence of smoking has decreased. The vast majority of peoplein the state are protected from secondhand smoke in public places andplaces of employment, and programs to assist tobacco users in quitting areavailable across North Dakota. We have made significant progress inreducing tobacco use since 2001, when the North Dakota Department ofHealth launched a statewide tobacco control effort funded through theCommunity Health Grant Program. Tobacco prevention and control effortsin the state are working and making a difference.
Tobacco control work in North Dakota is not finished. Far too many youthand adults continue to smoke. Nearly one in five of our youth and adults are current smokers.Other forms of tobacco including spit tobacco and cigars are also areas of concern. We havevisions of new social norms – healthier babies, tobacco-free youth, smoke-free air and fewerpremature deaths from heart disease, cancer, stroke and chronic lung disease. We have a visionof North Dakotans who see quality of life as a measurement of success.
Our overall success in improving the health status of North Dakotans depends greatly oncontinuing to achieve reductions in the rates of tobacco use among both adults and youngpeople. The challenges are great. Tobacco companies have more than doubled their marketingand promotional expenditures in North Dakota since the 1998 Master Settlement Agreementwith states. The tobacco industry spends more than $32 million a year in North Dakotapromoting its products and creating new tobacco users. If the current youth smoking trendscontinue, another 36,000 youth are projected to start smoking and more than 11,000 youthcould die prematurely from smoking. These figures underscore the need for intensified andcomprehensive tobacco control efforts in the state.
To succeed, programs must be maintained at the community level with adequate and sustainedfunding and must address the needs of North Dakotans of all ages and racial, cultural andethnic backgrounds. We have a great opportunity to build upon our current programs to furtherprevent and reduce tobacco use in our state and build a healthier North Dakota.
Terry Dwelle, M.D., M.P.H.T.M.State Health Officer
33333
Reducing Tobacco Use: Making Significant Strides

Clint BootsDivision of Tobacco Prevention and ControlNorth Dakota Department of Health
Dr. Leana BouffardNorth Dakota State University
Josh DerrCancer Information ServiceMayo Clinic Cancer Center
Rich FennoFargo Cass Public Health
Favian KennedyNorth Plains Tobacco Prevention ProjectTribal Chairman’s Health Board
Dr. Ralph KilzerNorth Dakota State Senator
Marlys KnellNorth Dakota Cancer Registry
44444
Tobacco Prevention DataAdvisory Committee Members
Kathleen MangskauDivision of Tobacco Prevention and ControlNorth Dakota Department of Health
Kathy MoumDivision of Chronic DiseaseNorth Dakota Department of Health
Dr. Nicholas NeumannUniversity of North DakotaSchool of Medicine & Health Services
Dr. Stephen PickardMedical EpidemiologistNorth Dakota Department of Health
Clara Sue PriceNorth Dakota State Representative
Dr. Nancy Vogeltanz-HolmCenter for Health Promotion andTranslation ResearchUniversity of North DakotaSchool of Medicine & Health Sciences
55555
Program Funding
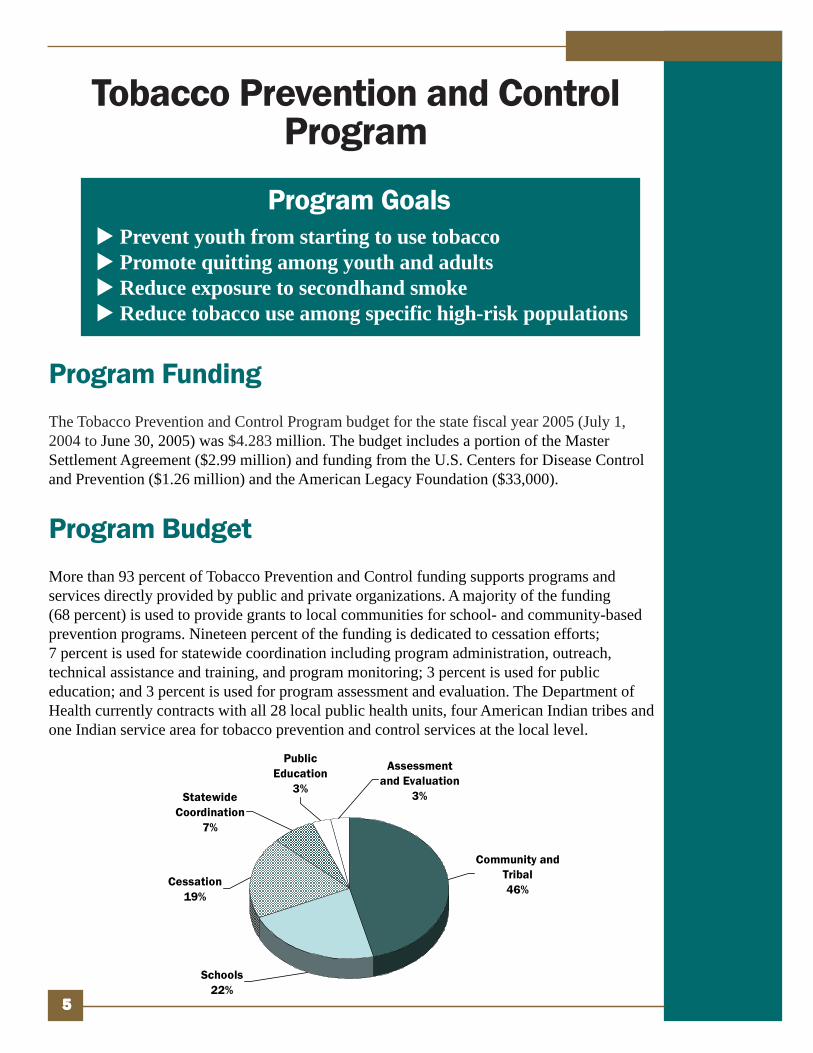
The Tobacco Prevention and Control Program budget for the state fiscal year 2005 (July 1,2004 to June 30, 2005) was $4.283 million. The budget includes a portion of the MasterSettlement Agreement ($2.99 million) and funding from the U.S. Centers for Disease Controland Prevention ($1.26 million) and the American Legacy Foundation ($33,000).
Program Budget
More than 93 percent of Tobacco Prevention and Control funding supports programs andservices directly provided by public and private organizations. A majority of the funding(68 percent) is used to provide grants to local communities for school- and community-basedprevention programs. Nineteen percent of the funding is dedicated to cessation efforts;7 percent is used for statewide coordination including program administration, outreach,technical assistance and training, and program monitoring; 3 percent is used for publiceducation; and 3 percent is used for program assessment and evaluation. The Department ofHealth currently contracts with all 28 local public health units, four American Indian tribes andone Indian service area for tobacco prevention and control services at the local level.
Tobacco Prevention and ControlProgram
Prevent youth from starting to use tobaccoPromote quitting among youth and adultsReduce exposure to secondhand smokeReduce tobacco use among specific high-risk populations
Program Goals
Public Education
3%Statewide
Coordination7%
Assessment and Evaluation
3%
Cessation19%
Community and Tribal46%
Schools22%

The North Dakota Department of Health is working to build a comprehensive approach topreventing and reducing tobacco use in the state. Following the U.S. Centers for DiseaseControl and Prevention model, North Dakota’s plan is to achieve its goals through anintegrated approach where each component reinforces the other.
66666
Current Efforts
Community-BasedPrograms
Local Public Health Unit-BasedProgramsAll 28 local public health units receivefunding to support community-basedprograms and coalitions serving NorthDakota’s 53 counties. Local coalitionsand networks create work plans that fitlocal needs and opportunities to reduceyouth access to tobacco; create tobacco-free schools, workplaces and publicplaces; and link tobacco users tocessation programs and services.
Local programs continued to educatebusiness owners and the public about thehealth consequences of tobacco use andthe dangers of exposure to secondhandsmoke. During fiscal year 2005, manybusinesses implemented voluntarysmoke-free policies. Fargo, West Fargo,Grafton and Grand Forks passed smoke-free ordinances to protect a majority oftheir workers and the public fromsecondhand smoke in public places andplaces of employment.
Tribal-Based ProgramsAmerican Indians have a tobacco-use ratethat is twice as high as the state average.All four tribes and one Indian service areareceive funds to implement tobaccoprevention programs. Their efforts aredesigned to decrease tobacco use byAmericanIndianswhilerespectingthe sacreduse oftobacco intheir culture.
Tribalprogramscontinuedtheir tobaccopreventionpubliceducation efforts. An increasing number oftribal businesses implemented smoke-freepolicies, and there is a growing interest incessation services. In the first year ofoperation, nearly 5 percent of the NorthDakota Tobacco Quitline callers wereAmerican Indian.

77777
Public education campaigns:• Create and sustain public
awareness.• Promote tobacco-use cessation.• Decrease the likelihood of
initiation of tobacco use amongyoung people.
• Can have far reaching impactson social and behavior changein a population.
• Can be used to target high-riskand hard-to-reach populations.
• Counter pro-tobaccoinfluences.
Why Public EducationCampaigns Are Important
Comprehensive School-Based Programs
During the current biennium, all 28 localpublic health units received funding toimplement comprehensive tobaccoprevention programs in schools.
Students benefit from proven effectivetobacco prevention curricula; specialresources and training for teachers; schoolpolicies that aim to eliminate the use oftobacco in school buildings, on groundsand at school events; and cessationsupport for students and staff.
Research has shown that school-basedprograms are effective when combinedwith other program components that arereinforced by adults and the communityenvironment.
During fiscal year 2005, evidenced-basedtobacco prevention curricula reached27,664 students. Eighty-eight schooldistricts implemented tobacco-free schoolgrounds policies covering 80,838 students.Sustained activity and support at the locallevel are critical to ensure that all studentsare taught about the dangers of tobaccouse and offered assistance in quitting.Tobacco-free policies model tobacco-freelifestyles that students should emulate.
Statewide PublicEducation Campaign
Local public health units partnered todevelop a public education campaign toincrease public awareness of the dangersof secondhand smoke.
Local public health units providemonthly press releases in communities toinform the public about the latesttobacco-related health information andtobacco prevention research. The NorthDakota Department of Healthimplemented a campaign to inform thepublic about the new North DakotaTobacco Quitline and the servicesoffered.

A tobacco cessation quitline:• Provides convenient, readily
available, anonymous, freeaccess to information aboutquitting tobacco use.
• Provides motivation to helptobacco users quit.
• Provides support to tobaccousers who have recently quitand need encouragement toprevent relapse.
• Can be used to target high-risk populations.
• Provides a resource forinformation about othertobacco cessation programsand makes referrals.
Why a Tobacco CessationQuitline Is Important
88888
Statewide Leadershipand Coordination
The Tobacco Prevention and ControlProgram is complex and engages a widevariety of partners and activities. Thestate program provides training, techni-cal assistance and consultation to localprograms. Program activities and con-tracts are carefully monitored to ensureeffective implementation and use ofresources. Coordination among thevarious program components is essentialto achieve maximum benefits andaccountability.
Program Evaluation
Program outcomes are measured using awide variety of sources including theYouth Risk Behavior Survey, YouthTobacco Survey, Behavioral Risk FactorSurveillance System, Pregnancy RiskAssessment and Monitoring System,birth and death certificates, tax revenueand consumption data, and specificresearch projects. This informationguides the development and revision ofprogram services to ensure effective useof resources.
North Dakota’s tobacco preventionprogram is working. Results for keyindicators are provided on pages9 through 16 of this report.
Cessation Programs
Local public health units use a portion oftheir funding to develop cessation programsand services for youth and adults and trainhealth-care providers in effective cessationapproaches. City/county and state employeecessation programs continue to be offered.
During fiscal year 2005, the North DakotaTobacco Quitline was launched, providingfree, confidential cessation counseling toany resident interested in quitting. Morethan 2,300 individuals called the quitlineduring that period. The six-month quit ratefor quitline callers was 39 percent. Anadditional 965 individuals receivedcessation services through local cessationprograms.

Program Successes
Youth Smoking – The percentage of youth in grades ninethrough 12 who are current smokers has significantly declinedfrom 41 percent in 1999 to 22 percent in 2005. That means there are8,700 fewer youth smoking.
Youth Smokeless Tobacco – The percentage of youth in gradesnine through 12 who are current smokeless tobacco users hasdeclined from 15 percent in 1999 to 11 percent in 2005. That meansthere are 2,200 fewer youth using smokeless tobacco.
Adult Smoking – The percentage of current adult smokers 18and older has declined from 23 percent in 2000 to 20 percent in2005. That means there are 15,000 fewer adults smoking.
Money Saved – An estimated $52 million in tobacco-related direct medicalexpenditures and lost productivity costs are saved each year as a result of the reducednumber of adults smoking.
Health-Care Costs – An estimated $121 million in futuretobacco-related health-care costs has already been saved by thereduced number of youth using tobacco.
Cessation – Cessation programs are conducted in 67 locations in 45 counties. In fiscalyear 2005, nearly 1,000 individuals enrolled in these local cessation programs and tried toquit using tobacco. In addition, more than 2,300 people called the North Dakota TobaccoQuitline, seeking assistance with quitting tobacco use.
North Dakota continues to make progress in reducing tobacco use and preventing youthfrom becoming addicted. Monitoring and evaluation of program efforts show that weare making a difference – despite the fact that the tobacco industry spends more than$32 million per year marketing its products in the state. The commitment to evidence-based tobacco prevention and cessation is reducing tobacco use among youth and adults,saving lives and saving money.
99999

North Dakota’s Tobacco Prevention and Control Program has made greatprogress working with its partners in local communities, schools and tribes, andit is time to build on that momentum. The job is far from finished and the workis challenging. Thousands of teens in North Dakota continue to start usingtobacco every year and hundreds of adults die from it.
To produce lasting results, a sustained comprehensive approach is necessary.Continuing to invest in proven tobacco prevention strategies will help futuregenerations in North Dakota live long and healthy lives. Achieving this goalwill require ongoing collaboration among state decision makers, public healthofficials, business leaders and community members. Working together will helpto save lives and money and reduce the health and economic consequences oftobacco use in North Dakota.
1111100000
The Work Ahead

Leading Tobacco Indicators
1111111111
The Burden of Tobacco○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Source: SAMMEC, 1999 and 2001
Each year, smokingkills 874 NorthDakotans.
Secondhand smokekills 80 to 140North Dakotanseach year.
Mortality
Economic Costs
Smoking costsNorth Dakota $372million annually.- $193 million in
direct medicalexpenditures
- $179 million inlost productivity
Source: SAMMEC, 1998 and 2001

Age of Initiation
Youth Smokeless Tobacco Use
11.210.313.215.1
01020304050
1999 2001 2003 2005
Year
Perc
enta
ge
1111122222
Youth Tobacco Use
Between 1999 and 2005, the useof smokeless tobacco productsamong North Dakota youthdecreased from 15.1 percent to11.2 percent.
Goal: 5 percent by 2010
The percentage of individualswho smoked their first wholecigarette before the age of 13decreased from 43.7 percent in2001 to 38.6 percent in 2005(asked of those who ever triedsmoking).
Goal: 34 percent by 2008
Cigarettes
Smokeless Tobacco
Age of Initiation
The percentage of North Dakotayouth who currently smokecigarettes significantly decreasedfrom 40.6 percent in 1999 to22.1 percent in 2005.
Goal: 22 percent by 2010
Youth Cigarette Use
40.630.2
22.1
35.3
01020304050
1999 2001 2003 2005Year
Perc
enta
ge
Source: YRBS (grades 9-12)
Smoked Cigarettes Before Age 13
36.7 38.643.7
020406080
100
2001 2003 2005
Year
Per
cent
age
Source: YRBS (grades 9-12)
Source: YRBS (grades 9-12)
GOGOGOGOGOALALALALAL
MET!MET!MET!MET!MET!

1111133333
Adult Tobacco UseCigarettes
Smokeless Tobacco
The percentage of North Dakotaadults currently smoking hasremained relatively stable.However, since 2000 there hasbeen a steady decline.
Goal: 19 percent by 2010
Despite a decline in 1998, thepercentage of North Dakota adultswho use smokeless tobaccoproducts has remained relativelystable.
Goal: 4 percent by 2010
Adult Smokeless Tobacco Use
5.14.05.0
01020304050
1996 1998 2003
Year
Perc
enta
ge
Source: BRFSS
Adult Cigarette Use
20.119.820.521.522.123.3
22.2
01020304050
1999 2000 2001 2002 2003 2004 2005
Year
Perc
enta
ge
Source: BRFSS

Cigarette Consumption
1111144444
Cessation AttemptsAdult Quit Attempts
Youth Quit Attempts
Cigarettes Sold
The percentage of North Dakotaadult current smokers who haveattempted to quit has remainedrelatively stable.
Goal: 55 percent by 2008
Note: Due to the small numberof respondents in this category,three-year rolling averages wereused.
The percentage of North Dakotayouth current smokers who haveattempted to quit has increasedin the past two years.
Goal: 63 percent by 2008
There has been a steady descreasein the number of cigarettes packssold, except for a slight increasebetween 2003 and 2005.
Youth Quit Attempts
57.9 57.8 65.1
020406080
100
2001 2003 2005
Year
Perc
enta
ge
Adult Quit Attempts
48.245.1 46.2 49.0 50.1 50.1 49.3 50.2 49.7
020406080
100
1994
-96
1995
-97
1996
-98
1997
-99
1998
-00
1999
-01
2000
-02
2001
-03
2002
-04
Year
Perc
enta
ge
Source: BRFSS
Total Number of Cigarettes Sold
886831
8841,0101,019 963
0
500
1,000
1995 1997 1999 2001 2003 2005Year
Num
ber (
in m
illion
s)
Source: North Dakota Tax Department
Source: YRBS (grades 9-12)
GOGOGOGOGOALALALALAL
MET!MET!MET!MET!MET!
Note: The increase in packssold between 2003 and 2005may be due to cross-border salesto Minnesota residents avoidinghigher tax rates in their homestate.

1111155555
Tobacco-Related Disparities
Smoking Rates in North Dakota
7.4
19.9
28.3
21.7
18.4
24.4
26.1
19.0
22.0
19.3
26.3
59.5
NA
NA
0 10 20 30 40 50 60 70
65+ years
45-64 years
25-44 years
18-24 years
> 12 years Education (20+ years)
12 years Education (20+ years)
< 12 years Education (20+ years)
Women
Men
White
Hispanic
Asian/Pacific Islander
Native American/Alaska Native
African American
PercentageSource: BRFSS 2002-2003
Research shows that state tobacco prevention programs must be broad-based andcomprehensive to be effective. A review of the data shows that tobacco use among somepopulation groups is higher than for the general population. These groups also often haveless access to health care and other resources. The result is a health disparity or adisproportionate occurrence of tobacco-related death and disease.
Tobacco-related health disparities are influenced by many factors, including the socio-economic status, geographic location, race and ethnicity, gender, sexual orientation, ordisability of a population. The history, cultural beliefs and country of origin of manypopulations also can affect their tobacco-use rates. Reducing tobacco use in high-risk groupsis one of four central goals of the Tobacco Prevention and Control Program.
In 2005, the Division of Tobacco Prevention and Control applied for a grant from the U.S.Centers for Disease Control and Prevention, Office on Smoking and Health, to develop aplan to address tobacco-related disparities. The division received the grant and work on theplan began in July of 2005. The planning grant will allow the Division of TobaccoPrevention and Control to take a broader look at tobacco-related disparities in the state anddevelop strategies to address them.
Note: Estimates for racial/ethnic groups are based on combined 2002 and 2003 data.
Youth Access to Tobacco
1111166666
Attitudes TowardsSmoke-Free
Environments
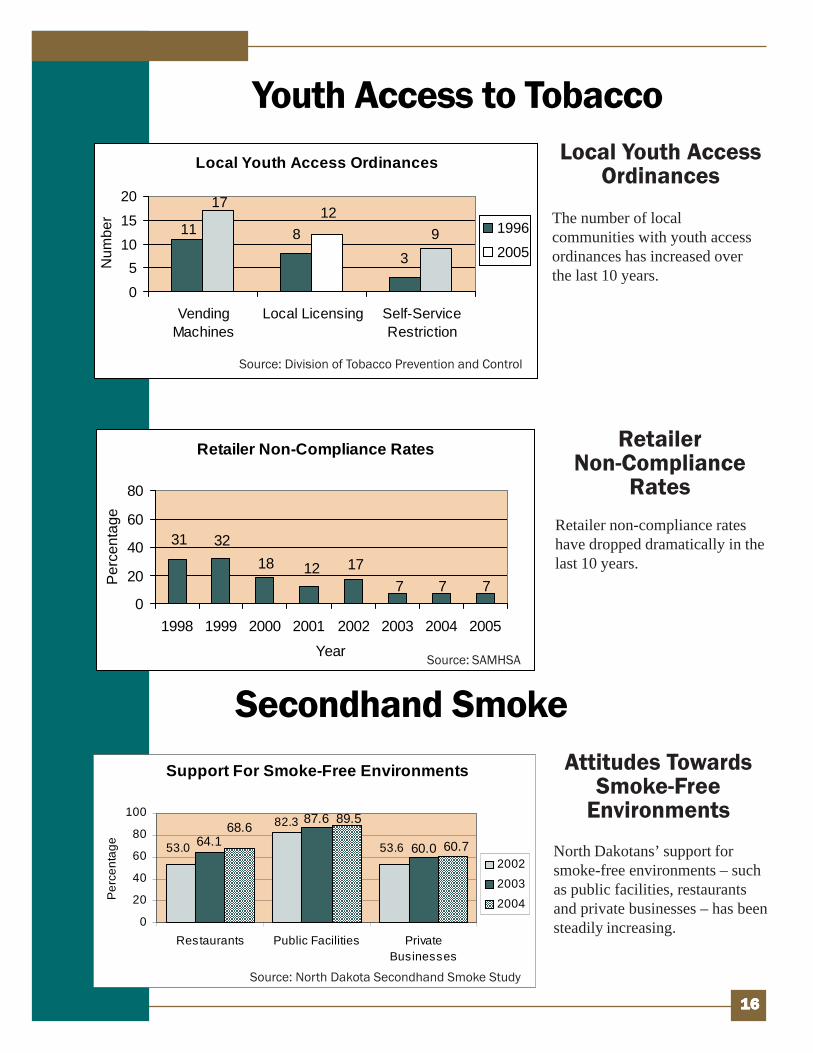
Support For Smoke-Free Environments
53.0
82.3
53.664.1
87.6
60.068.6
89.5
60.7
0
20
40
60
80
100
Restaurants Public Facilities PrivateBusinesses
Per
cent
age
2002
2003
2004
Secondhand Smoke
Source: North Dakota Secondhand Smoke Study
North Dakotans’ support forsmoke-free environments – suchas public facilities, restaurantsand private businesses – has beensteadily increasing.
Local Youth AccessOrdinances
RetailerNon-Compliance
Rates
The number of localcommunities with youth accessordinances has increased overthe last 10 years.
Retailer non-compliance rateshave dropped dramatically in thelast 10 years.
Local Youth Access Ordinances
93
81112
17
0
51015
20
VendingMachines
Local Licensing Self-ServiceRestriction
Num
ber
1996
2005
Source: Division of Tobacco Prevention and Control
Retailer Non-Compliance Rates
127 77
17183231
0
20
40
60
80
1998 1999 2000 2001 2002 2003 2004 2005
Year
Per
cent
age
Source: SAMHSA

1111177777
Smoke-Free Policies
Local Smoke-Free Ordinances2001:
Minot – Minot’s ordinance eliminated smoking in restaurants unless they wereseparately enclosed and ventilated.
2004:Fargo – The Fargo ordinance eliminated smoking in all public, indoor workplacesexcept truck stops and enclosed bars that do not admit people younger than 21.
West Fargo – West Fargo’s ordinance eliminated smoking in all workplaces andpublic places except those establishments that as of August 1, 2004, hold a city liquorlicense and do not admit people younger than 21.
2005:Grafton – Grafton’s ordinance eliminated smoking in all public places and work-places except bars and restaurants with separate, enclosed bars.
Grand Forks – The Grand Forks ordinance eliminated smoking in all publicplaces and workplaces except those establishments that hold a certain class of alcohollicense and do not admit people younger than 21. The ordinance also extends the smokingrestriction to outdoor areas of restaurants and requires that “no smoking” signs be posted.
In 2005, the North DakotaLegislative Assembly passedsmoke-free legislation makingmost workplaces and publicplaces smoke-free. The smoke-free law went into effectAugust 1, 2005.
A Statewide Smoke-Free Law

Data Sources
1111188888
Behavioral Risk Factor Surveillance System (BRFSS)The Behavioral Risk Factor Surveillance System (BRFSS) is the world’s largesttelephone survey. The BRFSS is a state-based, random-digit-dialed telephone survey ofthe noninstitutionalized civilian population 18 and older. It is designed to monitor theprevalence of the major behavioral risks among adults associated with prematuremorbidity and mortality. Information from the survey is used to improve the health of theAmerican people.
North Dakota Secondhand Smoke StudyThe North Dakota Secondhand Smoke Study assesses the impact of the statewidesecondhand smoke public education campaign. It is used to obtain information to refineplans and strategies targeting reduction of North Dakota residents’ exposure tosecondhand smoke. Statewide random sample interviews are conducted with 1,200 adultsbetween the ages of 18 and 54.
North Dakota Tax Department Annual Statement of CollectionsEvery year, the North Dakota Tax Department publishes a report containing the annualstatement of collections related to cigarette and tobacco tax collected in the state.
Smoking-Attributable Mortality, Morbidity and Economic Costs(SAMMEC)
SAMMEC provides an online database that allows users to estimate the adverse healthoutcomes and disease impact of smoking on adults and children. The Adult SAMMECapplication provides users the ability to estimate the number of annual deaths, yearsof potential life lost, medical expenditures and productivity losses among adults dueto smoking.
Substance Abuse and Mental Health Services Administration (SAMHSA)SAMHSA’s Center for Substance Abuse Prevention oversees implementation of theSynar amendment which requires that states have laws prohibiting the sale of tobacco toindividuals younger than 18. States must provide an annual report on the progress beingmade in the area of youth access to tobacco products.
Youth Risk Behavior Survey (YRBS)The YRBS, developed in 1990, monitors priority health risk behaviors, includingtobacco use, that contribute markedly to the leading causes of death, disability andsocial problems among youth and adults in the United States. The survey is administeredto students in grades seven through 12 every other year in a random sample of NorthDakota schools. Statistics used in this report are based on survey results from gradesnine through 12.


FFFFFor more infor more infor more infor more infor more information, contact:ormation, contact:ormation, contact:ormation, contact:ormation, contact:Division of Tobacco Prevention and ControlNorth Dakota Department of Health600 E. Boulevard Ave., Dept. 301Bismarck, N.D. 58505-0200Phone: 701.328.3138or 800.280.5512 (toll-free)www.ndhealth.gov/tobacco

















