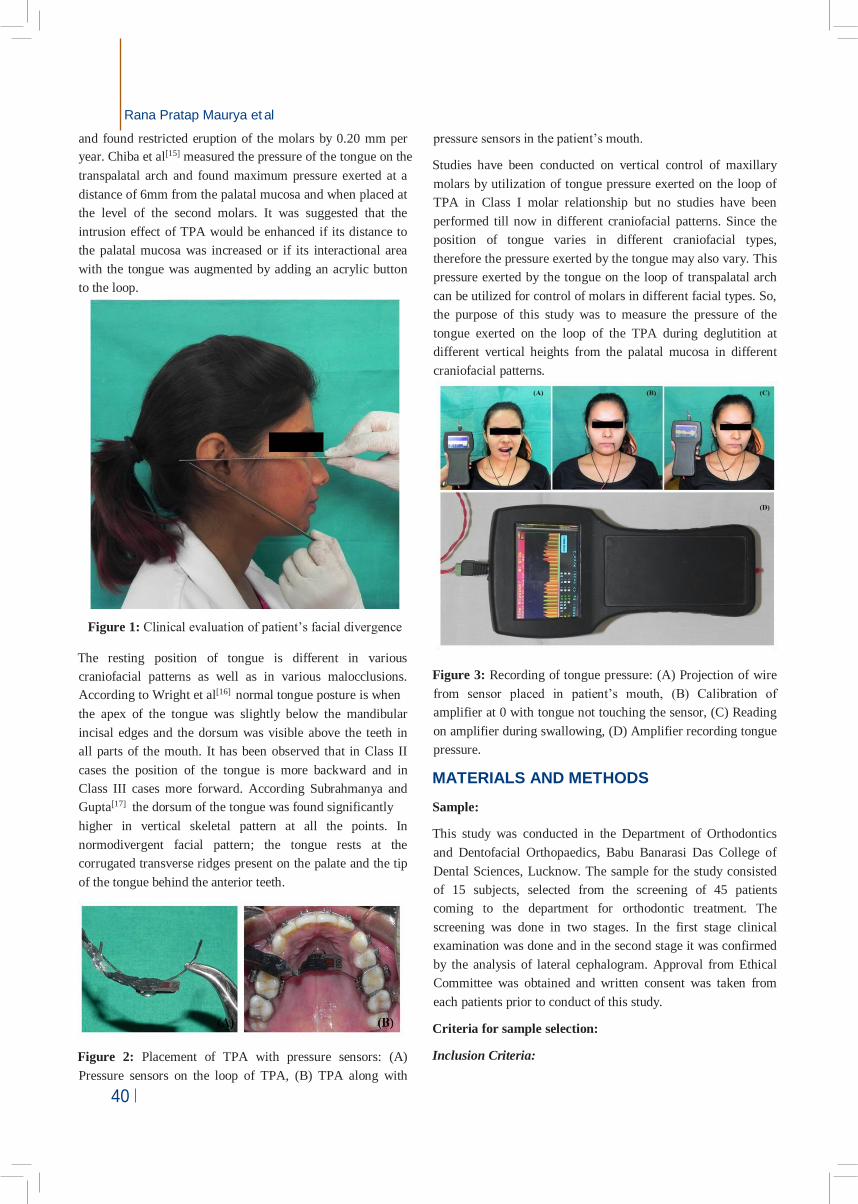
39 Journal of Contemporary Orthodontics, Jan-March 2020;4(1):39-45 To cite: Sugandha Namrata Massey, Rana Pratap Maurya, Tripti Tikku, Akhil Agarwal, Kamna Srivastava, Karunesh Tiwari Tongue Pressure Exerted On the Loop of Transpalatal Arch in Different Craniofacial Patterns J Contemp Orthod 2020;4(1): 39-9. Received on: 20-01-2020 Accepted on: 13-02-2020 Source of Support: Nil Conflict of Interest: None Tongue Pressure Exerted On the Loop of Transpalatal Arch in Different Craniofacial Patterns 1 Sugandha Namrata Massey, 2 Rana Pratap Maurya, 3 Tripti Tikku, 4 Akhil Agarwal, 5 Kamna Srivastava, 6 Karunesh Tiwari 1 Ex-Post-Graduate Student, 2 Reader, 3 Professor and Head of Department, 4 Ex-Reader, 5 Reader, 6 Assistant Professor 1-5 Department of Orthodontics and Dentofacial Orthodontics 6 Department of Physics , Babu Banarasi Das University Lucknow, U.P. India 1-5 Babu Banarasi Das College of Dental Sciences, Babu Banarasi Das University Lucknow, U.P. India ABSTRACT Objective: To evaluate the tongue pressure exerted on the loop of transpalatal arch in different craniofacial patterns at different heights from the palatal mucosa. Material and Method: 15 subjects were divided into three groups according to Schudy’s facial divergence angle as: Group I (Normodivergent), Group II (Hypodivergent) and Group III (Hyperdivergent). TPA was fabricated and placed at 2mm, 4mm and 6mm heights from the palatal mucosa in each subjects and tongue pressure was measured during swallowing using pressure sensors placed on the loop of TPA. The data obtained were recorded and subjected to statistical analysis. Result: On intergroup comparison, maximum tongue pressure was found in Group III followed by Group I and Group II and the difference was statistically significant (p<0.001). When comparison was done at different heights tongue pressure was found highest at 6mm followed by 4mm and 2mm in each group and difference was statistically significant (p<0.001). Conclusion: The maximum tongue pressure was observed in Hyperdivergent and minimum in Hypodivergent craniofacial pattern. It increases as the distance of the TPA from the palatal mucosa increases in all craniofacial patterns. Keyword: Hyperdivergent; Hypodivergent; Normodivergent; Transpalatal Arch, Tongue pressure. INTRODUCTION Tongue posture and functions are of interest in regard to their relationship to the malocclusions. The tongue affects the dentition, alveolar bone and other supporting structures during function as well as at rest. Tongue pressure during swallowing has been found to be several times higher than the lip or cheek pressures [1] Graber reported the average frequency of deglutition to be once a minute between meals and nine times a minute during eating .[2] Even during sleep the swallowing act is performed at infrequent intervals. The average frequency of deglutition is between 1,600-2,400 times a day .[3,4] Due to this high frequency of deglutition the tongue pressure exerted is quite high and this pressure experienced per deglutition can be utilized in correction of malocclusions. Investigators have measured the tongue pressure in order to incorporate its useful effects in correction of various malocclusions. Christiansen et al .[5] evaluated the average force of the resting tongue as 0.8 gm (pressure = 0.039 g/mm 2 ) when measured with a 4.9 mm diameter sensor. Winders 6 and Kydd et al. 7 stated that the tongue pressure during deglutition ranges from 41-709 g/cm 2 (0.40-6.95 N/cm 2 ) and 37-240 g/cm 2 (0.36-2.35 N/cm 2 ) respectively. Transpalatal arches (TPA) are routinely used in orthodontic treatment in both the permanent and mixed dentition. It can be used to stabilize or reinforce the anchorage, or activated to produce various types of tooth movement including derotation of unilateral or bilateral rotated molars, correction of molar crossbites, asymmetric or symmetric distalization of molars, buccal or lingual root torque and molar intrusion .[8-11] TPA along with headgear can also be given to correct the Class II malocclusion in young adults with vertical growth pattern .[8] Hata 12 investigated tongue forces imparted to the palatal bar and their control on vertical maxillary growth. Kazuhiro [13] et al measured tongue pressure during swallowing and found superiority of tongue pressure production at the antero-median part of hard palate. Wise et al [14] studied the effects of a normal transpalatal arch on vertical control of the maxillary first molars Original Article
Transcript
39 Journal of Contemporary Orthodontics, Jan-March 2020;4(1):39-45
To cite: Sugandha
Namrata Massey, Rana
Pratap Maurya, Tripti
Tikku, Akhil Agarwal,
Kamna Srivastava,
Karunesh Tiwari
Tongue Pressure Exerted On
the Loop of Transpalatal
Arch in Different Craniofacial
Patterns
J Contemp Orthod 2020;4(1):
39-9.
Received on:
20-01-2020
Accepted on:
13-02-2020
Source of Support: Nil
Conflict of Interest: None
Tongue Pressure Exerted On the Loop of Transpalatal Arch
1Ex-Post-Graduate Student, 2Reader, 3 Professor and Head of Department, 4Ex-Reader, 5Reader, 6Assistant
Professor
1-5Department of Orthodontics and Dentofacial Orthodontics
6Department of Physics , Babu Banarasi Das University Lucknow, U.P. India
1-5Babu Banarasi Das College of Dental Sciences, Babu Banarasi Das University Lucknow, U.P. India
ABSTRACT
Objective: To evaluate the tongue pressure exerted on the loop of transpalatal arch in different craniofacial patterns at different heights from the palatal mucosa.
Material and Method: 15 subjects were divided into three groups according to Schudy’s facial divergence angle as: Group I (Normodivergent), Group II (Hypodivergent) and Group III (Hyperdivergent). TPA was fabricated and placed at 2mm, 4mm and 6mm heights from the palatal mucosa in each subjects and tongue pressure was measured during swallowing using pressure sensors placed on the loop of TPA. The data obtained were recorded and subjected to statistical analysis.
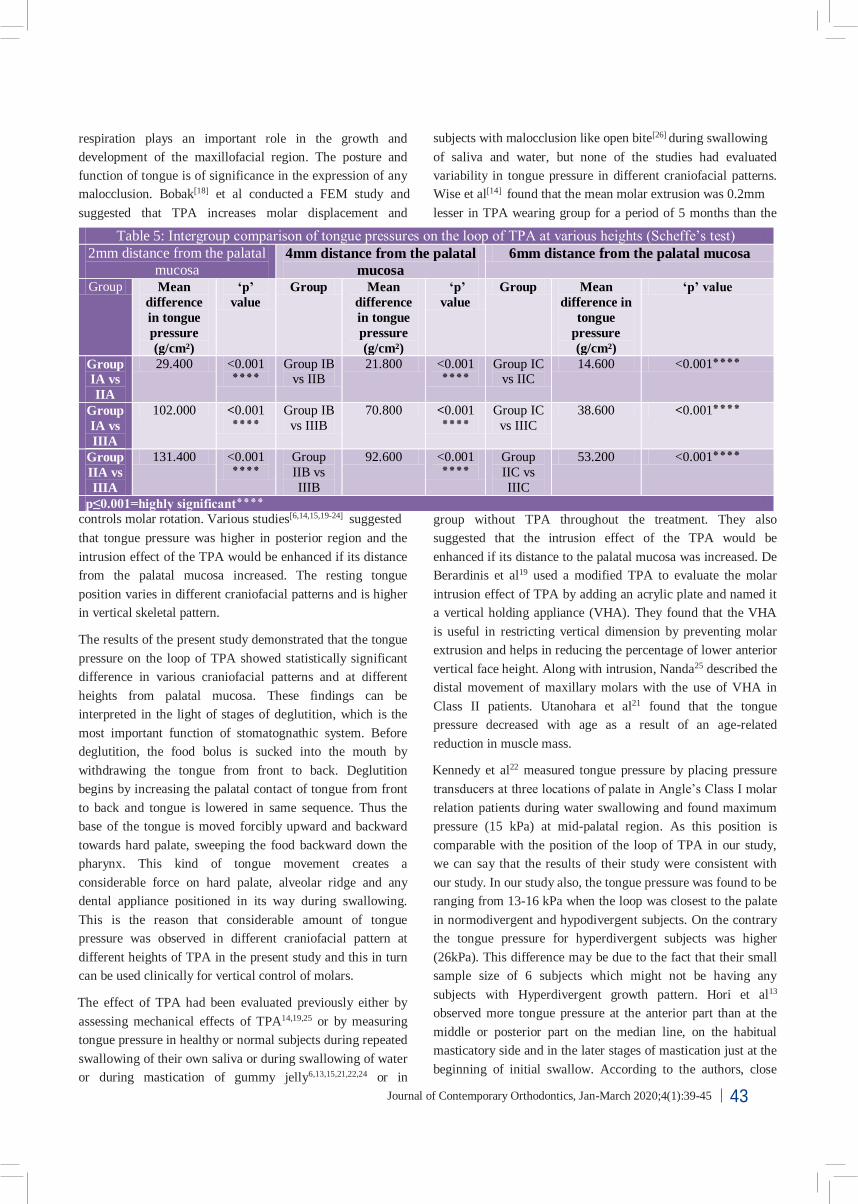
Result: On intergroup comparison, maximum tongue pressure was found in Group III followed by Group I and Group II and the difference was statistically significant (p<0.001). When comparison was done at different heights tongue pressure was found highest at 6mm followed by 4mm and 2mm in each group and difference was statistically significant (p<0.001).
Conclusion: The maximum tongue pressure was observed in Hyperdivergent and minimum in Hypodivergent craniofacial pattern. It increases as the distance of the TPA from the palatal mucosa increases in all craniofacial patterns.