Total distalization of the maxillary arch in a patient with skeletal Class II malocclusion Yoon Jeong Choi, a Jong-Suk Lee, b Jung-Yul Cha, c and Young-Chel Park d Seoul, Korea In nongrowing patients with skeletal Class II malocclusion, premolar extraction or maxillary molar distalization can be used as camouflage treatment. Orthodontic miniscrew implants are widely used for this purpose because they do not produce undesirable reciprocal effects and do not depend on the patient’s cooperation. This article reports on max- illary molar distalization by using miniscrew implants to correct a Class II problem. The main considerations of molar distalization treatment with miniscrew implants are discussed. (Am J Orthod Dentofacial Orthop 2011;139:823-33) T he treatment options for nongrowing skeletal Class II patients include camouflage treatment and surgi- cal correction. In a skeletal Class II patient having a short vertical dimension with no transverse discrep- ancies, it has been reported that an increase in the vertical dimension by orthognathic surgery or molar extrusion is unstable after a long-term follow up. 1-3 Therefore, if there is minimal skeletal discrepancy, a camouflage approach maintaining the vertical dimension after extraction would be an appropriate treatment alternative for stable treatment results. In camouflage treatment, the premolars are extracted to relieve crowding, correct protrusion, and establish proper occlusion. Creating space by stripping and correc- tion of the Class II molar relationship with maxillary molar distalization would be an alternative treatment. Distaliza- tion of maxillary molars can be accomplished by using a pendulum appliance, a distal jet, or a headgear. 4-6 Recently, miniscrew implants and miniplates have become widely used to treat Class II problems. 7-12 In this case report, miniscrew implants were used to distalize the maxillary molars, relieve the crowding, and establish a Class I molar relationship. DIAGNOSIS AND ETIOLOGY The patient was a 21-year old man with a chief com- plaint of dental crowding. The pretreatment facial pho- tographs showed protrusion of both upper and lower lips, a deep mentolabial fold, and mandibular asymmetry around the chin area. This was the result of trauma when he was 6 years old (Figs 1 and 2). In the frontal cephalogram, the chin was deviated to the left side, and an asymmetric mandibular lower border was observed. The lateral cephalometric analysis showed a Class II skeletal pattern with a low mandibular plane angle (Fig 3, Table). The IMPA angle of 117.5 reflected a compensatory proclination of the mandibular incisors, although it was measured from the most labially posi- tioned tooth, which was the left central incisor. The up- per and lower lips were protrusive by 4.1 and 8.0 mm, respectively, from the esthetic line. The panoramic radio- graph showed that both maxillary third molars were fully erupted, and the periodontal state was generally good. Molar relationships were Class II on both sides. The max- illary midline was 3.0 mm to the right of the facial mid- line, because of the ectopic right canine. The mandibular midline was 1.5 mm to the left of the facial midline with moderate anterior crowding. Overbite was 3.0 mm, and overjet was 2.5 mm. The Bolton tooth-ratio analysis (sum of incisors, 4:3.08; anterior ratio, 80.4%; overall ratio, 92.9%) indicated that the mandibular teeth were generally larger than the maxillary teeth. Based on these findings, the patient was diagnosed as skeletal Class II Division 1 with a hypodivergent profile and facial asymmetry. a Clincial assistant professor, Department of Orthodontics, Oral Science Research Center, Institute of Craniofacial Deformity, College of Dentistry, Yonsei University, Seoul, Korea. b Private practice, Seoul, Korea. c Assistant professor, Department of Orthodontics, Oral Science Research Center, Institute of Craniofacial Deformity, College of Dentistry, Yonsei University, Seoul, Korea. d Professor, Brain Korea 21 project, Department of Orthodontics, Oral Science Re- search Center, Institute of Craniofacial Deformity, College of Dentistry, Yonsei University, Seoul, Korea. The authors report no commercial, proprietary, or financial interest in the products or companies described in this article. Supported by a grant from the Institute of Craniofacial Deformity. Reprint requests to: Young-Chel Park, Department of Orthodontics, College of Dentistry, Yonsei University, 134 Sinchon-dong Seodaemun-gu, Seoul 120-749, Korea; e-mail, [email protected]. Submitted, June 2009; revised and accepted, July 2009. 0889-5406/$36.00 Copyright Ó 2011 by the American Association of Orthodontists. doi:10.1016/j.ajodo.2009.07.026 823 CASE REPORT
Transcript
CASE REPORT
Total distalization of the maxillary arch ina patient with skeletal Class II malocclusion
Yoon Jeong Choi,a Jong-Suk Lee,b Jung-Yul Cha,c and Young-Chel Parkd
In nongrowing patients with skeletal Class II malocclusion, premolar extraction or maxillary molar distalization can beused as camouflage treatment. Orthodonticminiscrew implants are widely used for this purpose because they do notproduce undesirable reciprocal effects and do not depend on the patient’s cooperation. This article reports on max-illary molar distalization by using miniscrew implants to correct a Class II problem. The main considerations of molardistalization treatment with miniscrew implants are discussed. (Am J Orthod Dentofacial Orthop 2011;139:823-33)
The treatment options for nongrowing skeletal ClassII patients include camouflage treatment and surgi-cal correction. In a skeletal Class II patient having
a short vertical dimension with no transverse discrep-ancies, it has been reported that an increase in the verticaldimension by orthognathic surgery or molar extrusion isunstable after a long-term follow up.1-3 Therefore, ifthere is minimal skeletal discrepancy, a camouflageapproach maintaining the vertical dimension afterextraction would be an appropriate treatment alternativefor stable treatment results.
In camouflage treatment, the premolars are extractedto relieve crowding, correct protrusion, and establishproper occlusion. Creating space by stripping and correc-tion of the Class II molar relationship with maxillary molardistalization would be an alternative treatment. Distaliza-tion of maxillary molars can be accomplished by usinga pendulum appliance, a distal jet, or a headgear.4-6
Recently, miniscrew implants and miniplates havebecome widely used to treat Class II problems.7-12
ial assistant professor, Department of Orthodontics, Oral Science Researchr, Institute of Craniofacial Deformity, College of Dentistry, Yonseirsity, Seoul, Korea.te practice, Seoul, Korea.tant professor, Department of Orthodontics, Oral Science Research Center,te of Craniofacial Deformity, College of Dentistry, Yonsei University, Seoul,.ssor, Brain Korea 21 project, Department of Orthodontics, Oral Science Re-Center, Institute of Craniofacial Deformity, College of Dentistry, Yonsei
rsity, Seoul, Korea.uthors report no commercial, proprietary, or financial interest in the productspanies described in this article.rted by a grant from the Institute of Craniofacial Deformity.t requests to: Young-Chel Park, Department of Orthodontics, College oftry, Yonsei University, 134 Sinchon-dong Seodaemun-gu, Seoul 120-749,; e-mail, [email protected], June 2009; revised and accepted, July 2009.5406/$36.00ight � 2011 by the American Association of Orthodontists..1016/j.ajodo.2009.07.026
In this case report, miniscrew implants were used todistalize the maxillary molars, relieve the crowding,and establish a Class I molar relationship.
DIAGNOSIS AND ETIOLOGY
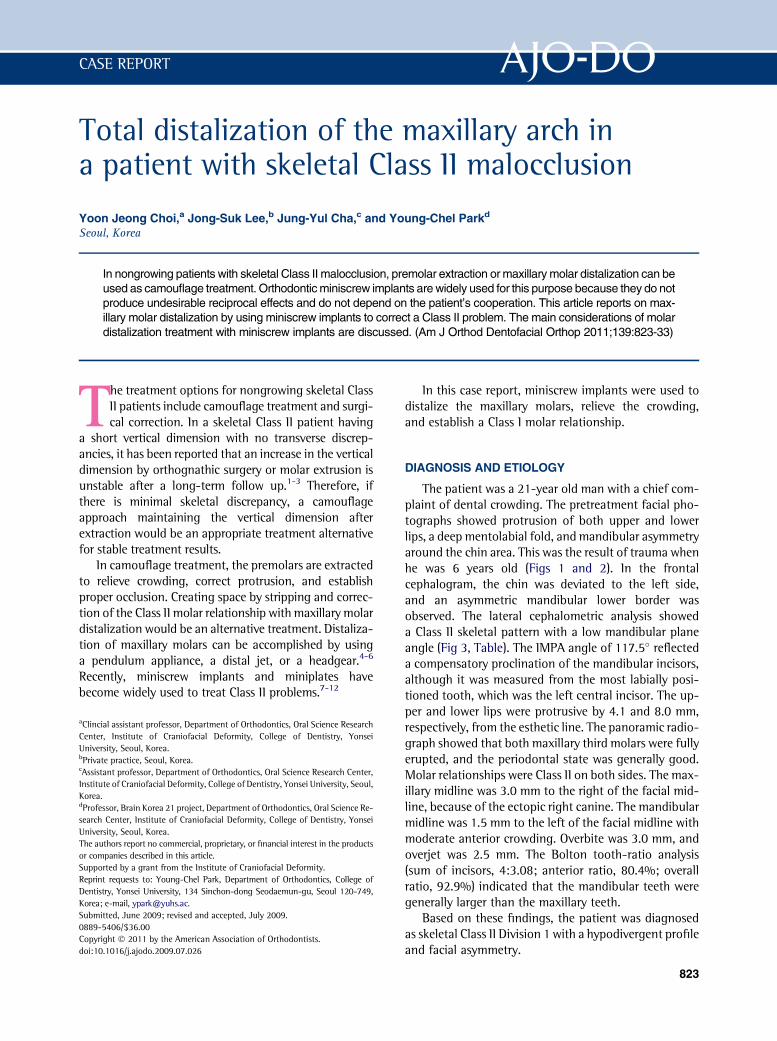
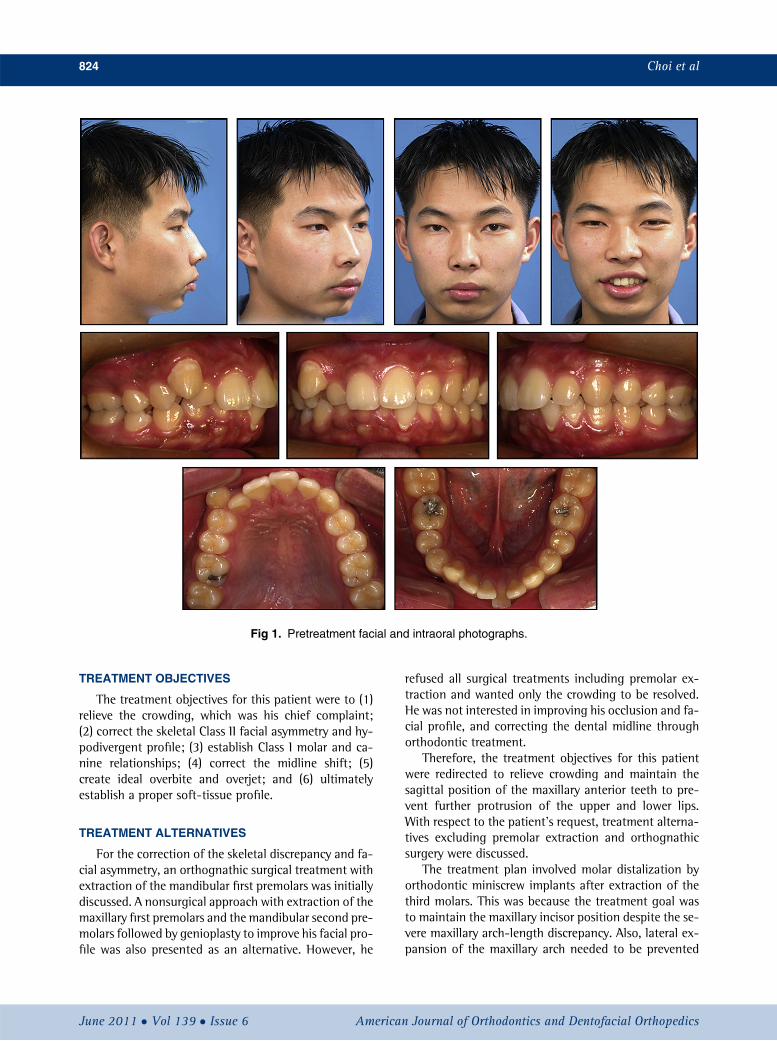
The patient was a 21-year old man with a chief com-plaint of dental crowding. The pretreatment facial pho-tographs showed protrusion of both upper and lowerlips, a deep mentolabial fold, andmandibular asymmetryaround the chin area. This was the result of trauma whenhe was 6 years old (Figs 1 and 2). In the frontalcephalogram, the chin was deviated to the left side,and an asymmetric mandibular lower border wasobserved. The lateral cephalometric analysis showeda Class II skeletal pattern with a low mandibular planeangle (Fig 3, Table). The IMPA angle of 117.5� reflecteda compensatory proclination of the mandibular incisors,although it was measured from the most labially posi-tioned tooth, which was the left central incisor. The up-per and lower lips were protrusive by 4.1 and 8.0 mm,respectively, from the esthetic line. The panoramic radio-graph showed that both maxillary third molars were fullyerupted, and the periodontal state was generally good.Molar relationships were Class II on both sides. The max-illary midline was 3.0 mm to the right of the facial mid-line, because of the ectopic right canine. The mandibularmidline was 1.5 mm to the left of the facial midline withmoderate anterior crowding. Overbite was 3.0 mm, andoverjet was 2.5 mm. The Bolton tooth-ratio analysis(sum of incisors, 4:3.08; anterior ratio, 80.4%; overallratio, 92.9%) indicated that the mandibular teeth weregenerally larger than the maxillary teeth.
Based on these findings, the patient was diagnosedas skeletal Class II Division 1 with a hypodivergent profileand facial asymmetry.
Fig 1. Pretreatment facial and intraoral photographs.
824 Choi et al
TREATMENT OBJECTIVES
The treatment objectives for this patient were to (1)relieve the crowding, which was his chief complaint;(2) correct the skeletal Class II facial asymmetry and hy-podivergent profile; (3) establish Class I molar and ca-nine relationships; (4) correct the midline shift; (5)create ideal overbite and overjet; and (6) ultimatelyestablish a proper soft-tissue profile.
TREATMENT ALTERNATIVES
For the correction of the skeletal discrepancy and fa-cial asymmetry, an orthognathic surgical treatment withextraction of the mandibular first premolars was initiallydiscussed. A nonsurgical approach with extraction of themaxillary first premolars and the mandibular second pre-molars followed by genioplasty to improve his facial pro-file was also presented as an alternative. However, he
June 2011 � Vol 139 � Issue 6 American
refused all surgical treatments including premolar ex-traction and wanted only the crowding to be resolved.He was not interested in improving his occlusion and fa-cial profile, and correcting the dental midline throughorthodontic treatment.
Therefore, the treatment objectives for this patientwere redirected to relieve crowding and maintain thesagittal position of the maxillary anterior teeth to pre-vent further protrusion of the upper and lower lips.With respect to the patient’s request, treatment alterna-tives excluding premolar extraction and orthognathicsurgery were discussed.
The treatment plan involved molar distalization byorthodontic miniscrew implants after extraction of thethird molars. This was because the treatment goal wasto maintain the maxillary incisor position despite the se-vere maxillary arch-length discrepancy. Also, lateral ex-pansion of the maxillary arch needed to be prevented
Journal of Orthodontics and Dentofacial Orthopedics
Fig 2. Pretreatment dental casts.
Fig 3. Pretreatment lateral and frontal cephalograms and panoramic radiograph.
Choi et al 825
American Journal of Orthodontics and Dentofacial Orthopedics June 2011 � Vol 139 � Issue 6
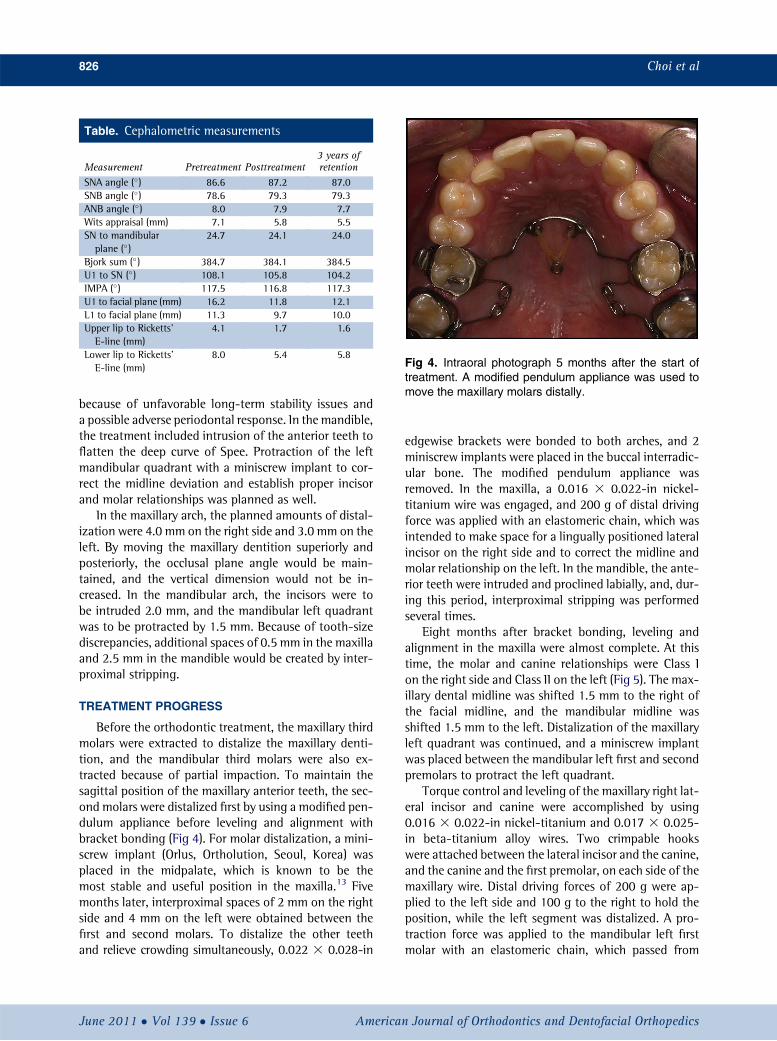
Fig 4. Intraoral photograph 5 months after the start oftreatment. A modified pendulum appliance was used tomove the maxillary molars distally.
Table. Cephalometric measurements
Measurement Pretreatment Posttreatment3 years ofretention
Bjork sum (�) 384.7 384.1 384.5U1 to SN (�) 108.1 105.8 104.2IMPA (�) 117.5 116.8 117.3U1 to facial plane (mm) 16.2 11.8 12.1L1 to facial plane (mm) 11.3 9.7 10.0Upper lip to Ricketts’E-line (mm)
4.1 1.7 1.6
Lower lip to Ricketts’E-line (mm)
8.0 5.4 5.8
826 Choi et al
because of unfavorable long-term stability issues anda possible adverse periodontal response. In the mandible,the treatment included intrusion of the anterior teeth toflatten the deep curve of Spee. Protraction of the leftmandibular quadrant with a miniscrew implant to cor-rect the midline deviation and establish proper incisorand molar relationships was planned as well.
In the maxillary arch, the planned amounts of distal-ization were 4.0 mm on the right side and 3.0 mm on theleft. By moving the maxillary dentition superiorly andposteriorly, the occlusal plane angle would be main-tained, and the vertical dimension would not be in-creased. In the mandibular arch, the incisors were tobe intruded 2.0 mm, and the mandibular left quadrantwas to be protracted by 1.5 mm. Because of tooth-sizediscrepancies, additional spaces of 0.5 mm in the maxillaand 2.5 mm in the mandible would be created by inter-proximal stripping.
TREATMENT PROGRESS
Before the orthodontic treatment, the maxillary thirdmolars were extracted to distalize the maxillary denti-tion, and the mandibular third molars were also ex-tracted because of partial impaction. To maintain thesagittal position of the maxillary anterior teeth, the sec-ond molars were distalized first by using a modified pen-dulum appliance before leveling and alignment withbracket bonding (Fig 4). For molar distalization, a mini-screw implant (Orlus, Ortholution, Seoul, Korea) wasplaced in the midpalate, which is known to be themost stable and useful position in the maxilla.13 Fivemonths later, interproximal spaces of 2 mm on the rightside and 4 mm on the left were obtained between thefirst and second molars. To distalize the other teethand relieve crowding simultaneously, 0.022 3 0.028-in
June 2011 � Vol 139 � Issue 6 American
edgewise brackets were bonded to both arches, and 2miniscrew implants were placed in the buccal interradic-ular bone. The modified pendulum appliance wasremoved. In the maxilla, a 0.016 3 0.022-in nickel-titanium wire was engaged, and 200 g of distal drivingforce was applied with an elastomeric chain, which wasintended to make space for a lingually positioned lateralincisor on the right side and to correct the midline andmolar relationship on the left. In the mandible, the ante-rior teeth were intruded and proclined labially, and, dur-ing this period, interproximal stripping was performedseveral times.
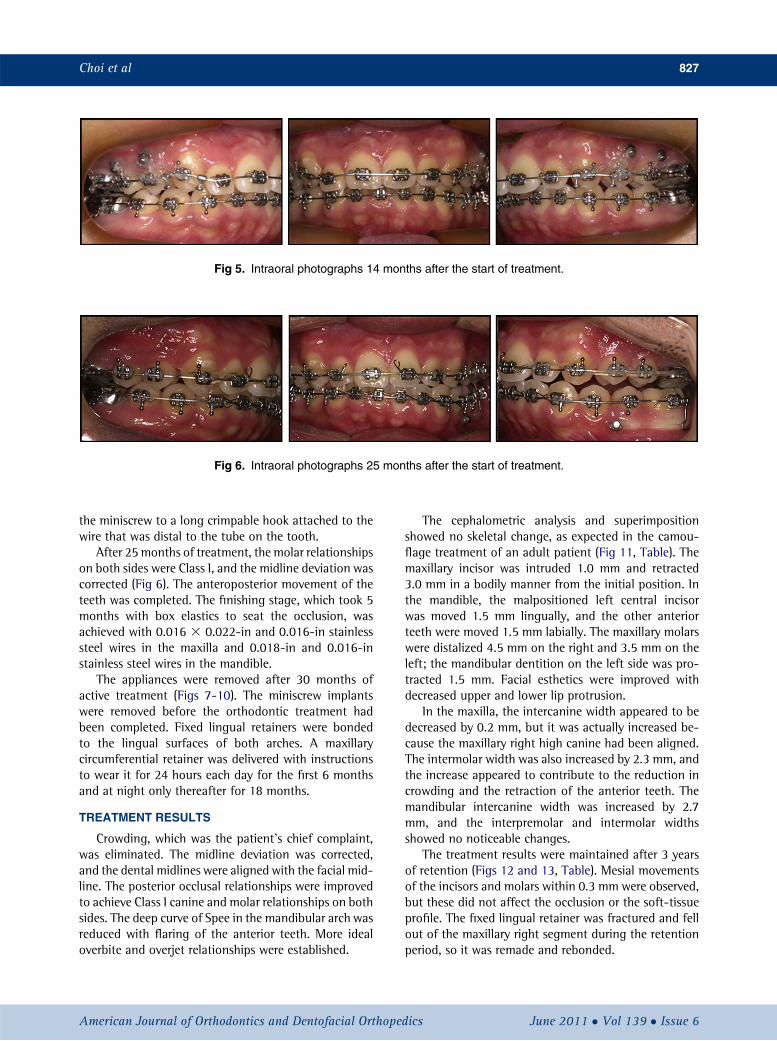
Eight months after bracket bonding, leveling andalignment in the maxilla were almost complete. At thistime, the molar and canine relationships were Class Ion the right side and Class II on the left (Fig 5). The max-illary dental midline was shifted 1.5 mm to the right ofthe facial midline, and the mandibular midline wasshifted 1.5 mm to the left. Distalization of the maxillaryleft quadrant was continued, and a miniscrew implantwas placed between the mandibular left first and secondpremolars to protract the left quadrant.
Torque control and leveling of the maxillary right lat-eral incisor and canine were accomplished by using0.016 3 0.022-in nickel-titanium and 0.017 3 0.025-in beta-titanium alloy wires. Two crimpable hookswere attached between the lateral incisor and the canine,and the canine and the first premolar, on each side of themaxillary wire. Distal driving forces of 200 g were ap-plied to the left side and 100 g to the right to hold theposition, while the left segment was distalized. A pro-traction force was applied to the mandibular left firstmolar with an elastomeric chain, which passed from
Journal of Orthodontics and Dentofacial Orthopedics
Fig 5. Intraoral photographs 14 months after the start of treatment.
Fig 6. Intraoral photographs 25 months after the start of treatment.
Choi et al 827
the miniscrew to a long crimpable hook attached to thewire that was distal to the tube on the tooth.
After 25months of treatment, the molar relationshipson both sides were Class I, and the midline deviation wascorrected (Fig 6). The anteroposterior movement of theteeth was completed. The finishing stage, which took 5months with box elastics to seat the occlusion, wasachieved with 0.016 3 0.022-in and 0.016-in stainlesssteel wires in the maxilla and 0.018-in and 0.016-instainless steel wires in the mandible.
The appliances were removed after 30 months ofactive treatment (Figs 7-10). The miniscrew implantswere removed before the orthodontic treatment hadbeen completed. Fixed lingual retainers were bondedto the lingual surfaces of both arches. A maxillarycircumferential retainer was delivered with instructionsto wear it for 24 hours each day for the first 6 monthsand at night only thereafter for 18 months.
TREATMENT RESULTS
Crowding, which was the patient’s chief complaint,was eliminated. The midline deviation was corrected,and the dental midlines were aligned with the facial mid-line. The posterior occlusal relationships were improvedto achieve Class I canine and molar relationships on bothsides. The deep curve of Spee in the mandibular arch wasreduced with flaring of the anterior teeth. More idealoverbite and overjet relationships were established.
American Journal of Orthodontics and Dentofacial Orthoped
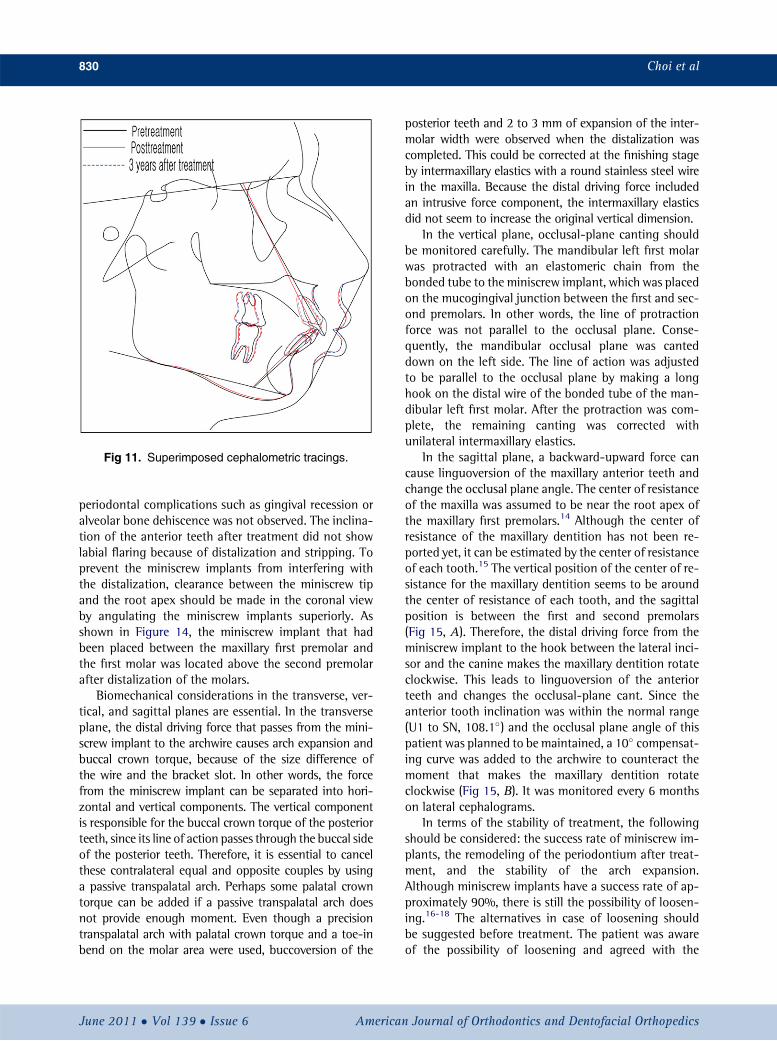
The cephalometric analysis and superimpositionshowed no skeletal change, as expected in the camou-flage treatment of an adult patient (Fig 11, Table). Themaxillary incisor was intruded 1.0 mm and retracted3.0 mm in a bodily manner from the initial position. Inthe mandible, the malpositioned left central incisorwas moved 1.5 mm lingually, and the other anteriorteeth were moved 1.5 mm labially. The maxillary molarswere distalized 4.5 mm on the right and 3.5 mm on theleft; the mandibular dentition on the left side was pro-tracted 1.5 mm. Facial esthetics were improved withdecreased upper and lower lip protrusion.
In the maxilla, the intercanine width appeared to bedecreased by 0.2 mm, but it was actually increased be-cause the maxillary right high canine had been aligned.The intermolar width was also increased by 2.3 mm, andthe increase appeared to contribute to the reduction incrowding and the retraction of the anterior teeth. Themandibular intercanine width was increased by 2.7mm, and the interpremolar and intermolar widthsshowed no noticeable changes.
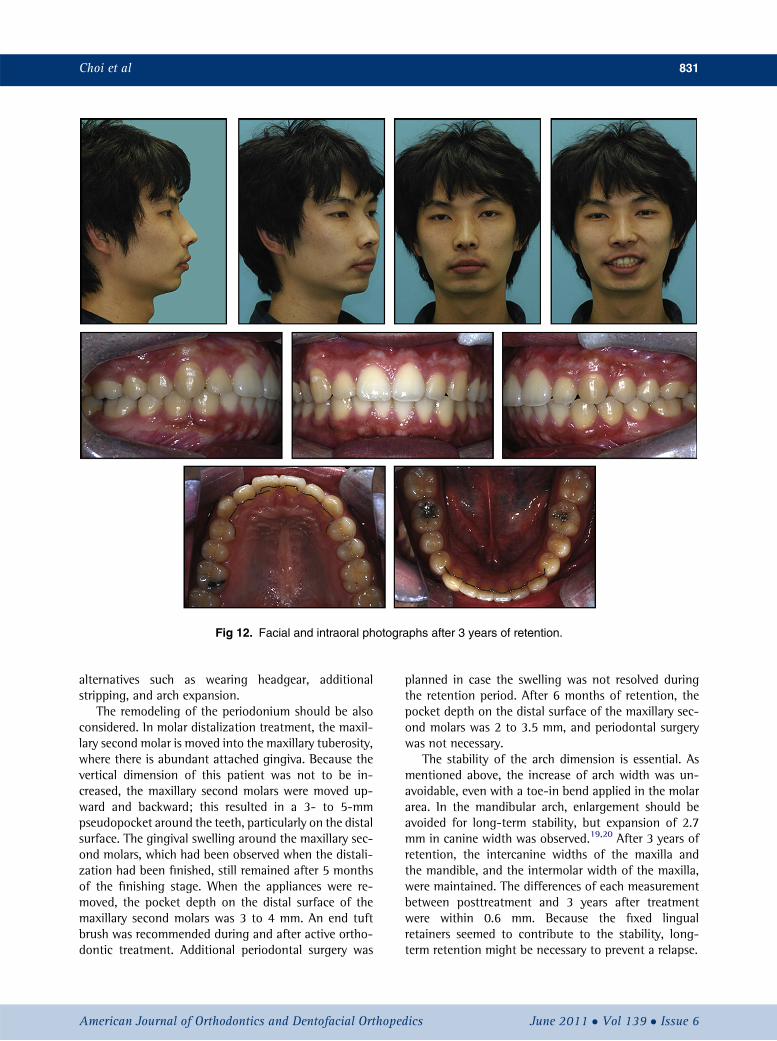
The treatment results were maintained after 3 yearsof retention (Figs 12 and 13, Table). Mesial movementsof the incisors and molars within 0.3 mm were observed,but these did not affect the occlusion or the soft-tissueprofile. The fixed lingual retainer was fractured and fellout of the maxillary right segment during the retentionperiod, so it was remade and rebonded.
ics June 2011 � Vol 139 � Issue 6
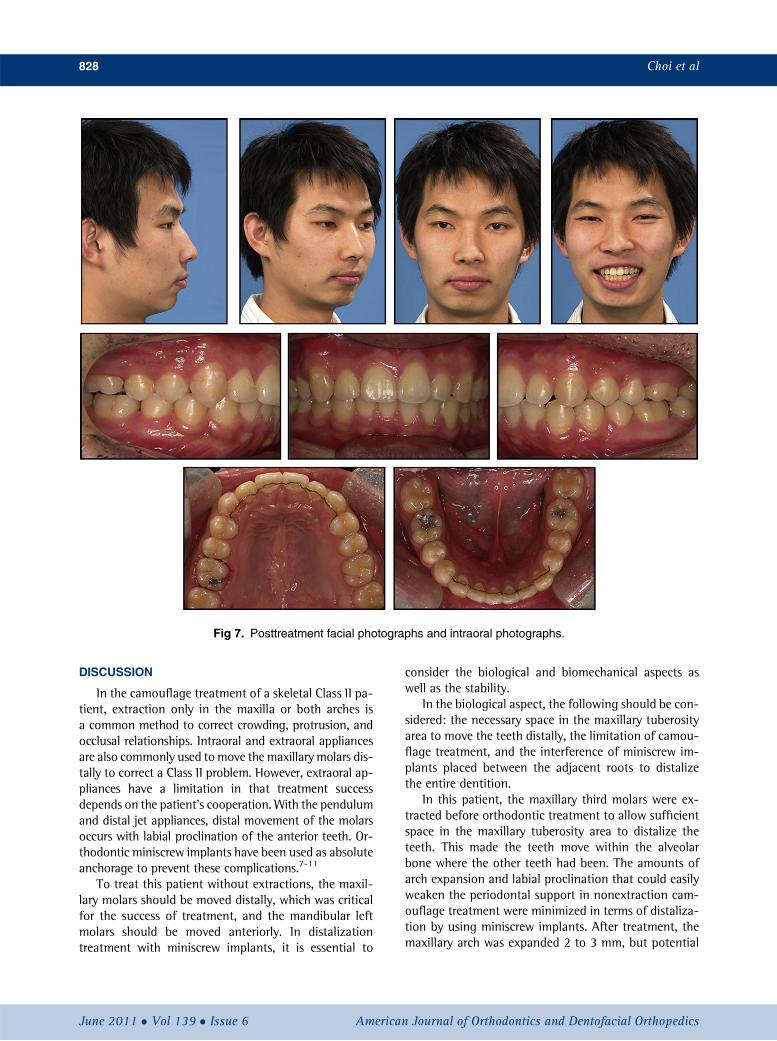
Fig 7. Posttreatment facial photographs and intraoral photographs.
828 Choi et al
DISCUSSION
In the camouflage treatment of a skeletal Class II pa-tient, extraction only in the maxilla or both arches isa common method to correct crowding, protrusion, andocclusal relationships. Intraoral and extraoral appliancesare also commonly used tomove the maxillary molars dis-tally to correct a Class II problem. However, extraoral ap-pliances have a limitation in that treatment successdepends on the patient’s cooperation. With the pendulumand distal jet appliances, distal movement of the molarsoccurs with labial proclination of the anterior teeth. Or-thodontic miniscrew implants have been used as absoluteanchorage to prevent these complications.7-11
To treat this patient without extractions, the maxil-lary molars should be moved distally, which was criticalfor the success of treatment, and the mandibular leftmolars should be moved anteriorly. In distalizationtreatment with miniscrew implants, it is essential to
June 2011 � Vol 139 � Issue 6 American
consider the biological and biomechanical aspects aswell as the stability.
In the biological aspect, the following should be con-sidered: the necessary space in the maxillary tuberosityarea to move the teeth distally, the limitation of camou-flage treatment, and the interference of miniscrew im-plants placed between the adjacent roots to distalizethe entire dentition.
In this patient, the maxillary third molars were ex-tracted before orthodontic treatment to allow sufficientspace in the maxillary tuberosity area to distalize theteeth. This made the teeth move within the alveolarbone where the other teeth had been. The amounts ofarch expansion and labial proclination that could easilyweaken the periodontal support in nonextraction cam-ouflage treatment were minimized in terms of distaliza-tion by using miniscrew implants. After treatment, themaxillary arch was expanded 2 to 3 mm, but potential
Journal of Orthodontics and Dentofacial Orthopedics
Fig 8. Posttreatment dental casts.
Fig 9. Lateral cephalogram and panoramic radiograph.Fig 10. Frontal cephalogram 2 months before removingthe appliance.
Choi et al 829
American Journal of Orthodontics and Dentofacial Orthopedics June 2011 � Vol 139 � Issue 6
Fig 11. Superimposed cephalometric tracings.
830 Choi et al
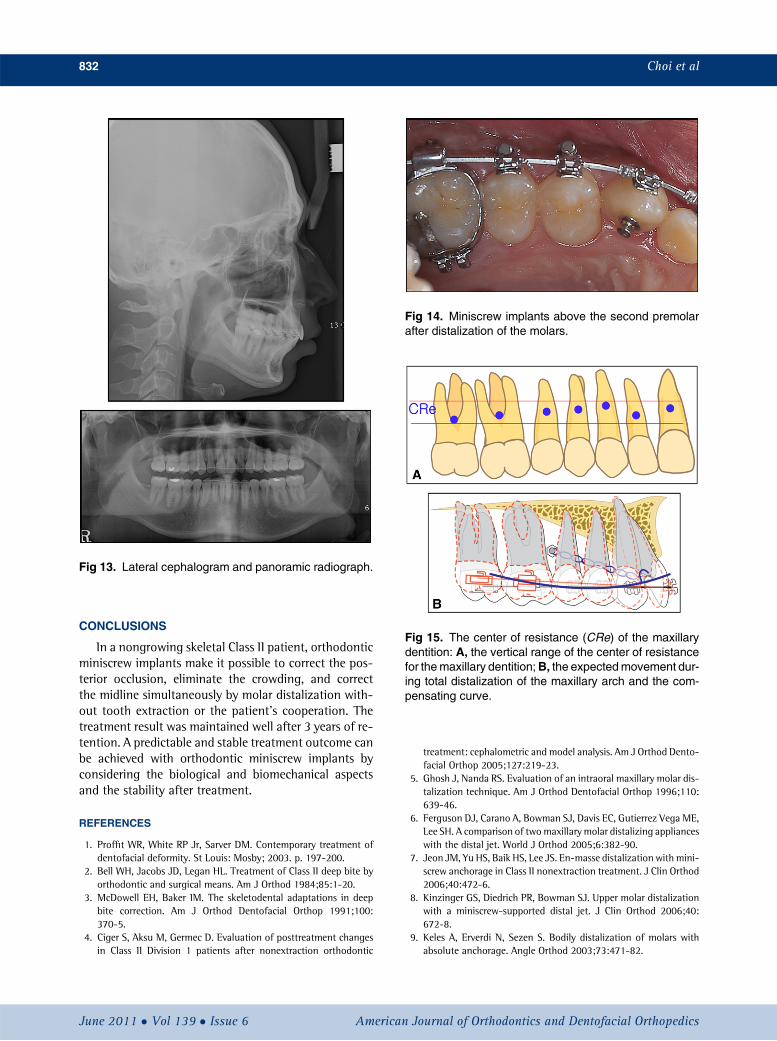
periodontal complications such as gingival recession oralveolar bone dehiscence was not observed. The inclina-tion of the anterior teeth after treatment did not showlabial flaring because of distalization and stripping. Toprevent the miniscrew implants from interfering withthe distalization, clearance between the miniscrew tipand the root apex should be made in the coronal viewby angulating the miniscrew implants superiorly. Asshown in Figure 14, the miniscrew implant that hadbeen placed between the maxillary first premolar andthe first molar was located above the second premolarafter distalization of the molars.
Biomechanical considerations in the transverse, ver-tical, and sagittal planes are essential. In the transverseplane, the distal driving force that passes from the mini-screw implant to the archwire causes arch expansion andbuccal crown torque, because of the size difference ofthe wire and the bracket slot. In other words, the forcefrom the miniscrew implant can be separated into hori-zontal and vertical components. The vertical componentis responsible for the buccal crown torque of the posteriorteeth, since its line of action passes through the buccal sideof the posterior teeth. Therefore, it is essential to cancelthese contralateral equal and opposite couples by usinga passive transpalatal arch. Perhaps some palatal crowntorque can be added if a passive transpalatal arch doesnot provide enough moment. Even though a precisiontranspalatal arch with palatal crown torque and a toe-inbend on the molar area were used, buccoversion of the
June 2011 � Vol 139 � Issue 6 American
posterior teeth and 2 to 3 mm of expansion of the inter-molar width were observed when the distalization wascompleted. This could be corrected at the finishing stageby intermaxillary elastics with a round stainless steel wirein the maxilla. Because the distal driving force includedan intrusive force component, the intermaxillary elasticsdid not seem to increase the original vertical dimension.
In the vertical plane, occlusal-plane canting shouldbe monitored carefully. The mandibular left first molarwas protracted with an elastomeric chain from thebonded tube to the miniscrew implant, which was placedon the mucogingival junction between the first and sec-ond premolars. In other words, the line of protractionforce was not parallel to the occlusal plane. Conse-quently, the mandibular occlusal plane was canteddown on the left side. The line of action was adjustedto be parallel to the occlusal plane by making a longhook on the distal wire of the bonded tube of the man-dibular left first molar. After the protraction was com-plete, the remaining canting was corrected withunilateral intermaxillary elastics.
In the sagittal plane, a backward-upward force cancause linguoversion of the maxillary anterior teeth andchange the occlusal plane angle. The center of resistanceof the maxilla was assumed to be near the root apex ofthe maxillary first premolars.14 Although the center ofresistance of the maxillary dentition has not been re-ported yet, it can be estimated by the center of resistanceof each tooth.15 The vertical position of the center of re-sistance for the maxillary dentition seems to be aroundthe center of resistance of each tooth, and the sagittalposition is between the first and second premolars(Fig 15, A). Therefore, the distal driving force from theminiscrew implant to the hook between the lateral inci-sor and the canine makes the maxillary dentition rotateclockwise. This leads to linguoversion of the anteriorteeth and changes the occlusal-plane cant. Since theanterior tooth inclination was within the normal range(U1 to SN, 108.1�) and the occlusal plane angle of thispatient was planned to be maintained, a 10� compensat-ing curve was added to the archwire to counteract themoment that makes the maxillary dentition rotateclockwise (Fig 15, B). It was monitored every 6 monthson lateral cephalograms.
In terms of the stability of treatment, the followingshould be considered: the success rate of miniscrew im-plants, the remodeling of the periodontium after treat-ment, and the stability of the arch expansion.Although miniscrew implants have a success rate of ap-proximately 90%, there is still the possibility of loosen-ing.16-18 The alternatives in case of loosening shouldbe suggested before treatment. The patient was awareof the possibility of loosening and agreed with the
Journal of Orthodontics and Dentofacial Orthopedics
Fig 12. Facial and intraoral photographs after 3 years of retention.
Choi et al 831
alternatives such as wearing headgear, additionalstripping, and arch expansion.
The remodeling of the periodonium should be alsoconsidered. In molar distalization treatment, the maxil-lary second molar is moved into the maxillary tuberosity,where there is abundant attached gingiva. Because thevertical dimension of this patient was not to be in-creased, the maxillary second molars were moved up-ward and backward; this resulted in a 3- to 5-mmpseudopocket around the teeth, particularly on the distalsurface. The gingival swelling around the maxillary sec-ond molars, which had been observed when the distali-zation had been finished, still remained after 5 monthsof the finishing stage. When the appliances were re-moved, the pocket depth on the distal surface of themaxillary second molars was 3 to 4 mm. An end tuftbrush was recommended during and after active ortho-dontic treatment. Additional periodontal surgery was
American Journal of Orthodontics and Dentofacial Orthoped
planned in case the swelling was not resolved duringthe retention period. After 6 months of retention, thepocket depth on the distal surface of the maxillary sec-ond molars was 2 to 3.5 mm, and periodontal surgerywas not necessary.
The stability of the arch dimension is essential. Asmentioned above, the increase of arch width was un-avoidable, even with a toe-in bend applied in the molararea. In the mandibular arch, enlargement should beavoided for long-term stability, but expansion of 2.7mm in canine width was observed.19,20 After 3 years ofretention, the intercanine widths of the maxilla andthe mandible, and the intermolar width of the maxilla,were maintained. The differences of each measurementbetween posttreatment and 3 years after treatmentwere within 0.6 mm. Because the fixed lingualretainers seemed to contribute to the stability, long-term retention might be necessary to prevent a relapse.
ics June 2011 � Vol 139 � Issue 6
Fig 13. Lateral cephalogram and panoramic radiograph.
Fig 14. Miniscrew implants above the second premolarafter distalization of the molars.
Fig 15. The center of resistance (CRe) of the maxillarydentition: A, the vertical range of the center of resistancefor themaxillary dentition;B, the expectedmovement dur-ing total distalization of the maxillary arch and the com-pensating curve.
832 Choi et al
CONCLUSIONS
In a nongrowing skeletal Class II patient, orthodonticminiscrew implants make it possible to correct the pos-terior occlusion, eliminate the crowding, and correctthe midline simultaneously by molar distalization with-out tooth extraction or the patient’s cooperation. Thetreatment result was maintained well after 3 years of re-tention. A predictable and stable treatment outcome canbe achieved with orthodontic miniscrew implants byconsidering the biological and biomechanical aspectsand the stability after treatment.
REFERENCES
1. Proffit WR, White RP Jr, Sarver DM. Contemporary treatment ofdentofacial deformity. St Louis: Mosby; 2003. p. 197-200.
2. Bell WH, Jacobs JD, Legan HL. Treatment of Class II deep bite byorthodontic and surgical means. Am J Orthod 1984;85:1-20.
3. McDowell EH, Baker IM. The skeletodental adaptations in deepbite correction. Am J Orthod Dentofacial Orthop 1991;100:370-5.
4. Ciger S, Aksu M, Germec D. Evaluation of posttreatment changesin Class II Division 1 patients after nonextraction orthodontic
June 2011 � Vol 139 � Issue 6 American
treatment: cephalometric and model analysis. Am J Orthod Dento-facial Orthop 2005;127:219-23.
5. Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar dis-talization technique. Am J Orthod Dentofacial Orthop 1996;110:639-46.
6. Ferguson DJ, Carano A, Bowman SJ, Davis EC, Gutierrez Vega ME,Lee SH. A comparison of twomaxillary molar distalizing applianceswith the distal jet. World J Orthod 2005;6:382-90.
7. Jeon JM, Yu HS, Baik HS, Lee JS. En-masse distalization with mini-screw anchorage in Class II nonextraction treatment. J Clin Orthod2006;40:472-6.
9. Keles A, Erverdi N, Sezen S. Bodily distalization of molars withabsolute anchorage. Angle Orthod 2003;73:471-82.
Journal of Orthodontics and Dentofacial Orthopedics
Choi et al 833
10. Kyung SH, Hong SG, Park YC. Distalization of maxillary molarswith a midpalatal miniscrew. J Clin Orthod 2003;37:22-6.
11. Kim SH, Lee KB, Chung KR, Nelson G, Kim TW. Severe bimaxillaryprotrusion with adult periodontitis treated by corticotomy andcompression osteogenesis. Korean J Orthod 2009;39:54-65.
12. Kim SJ, Chun YS, Jung SH, Park SH. Three dimensional analysis oftooth movement using different types of maxillary molar distaliza-tion appliances. Korean J Orthod 2008;38:376-87.
13. Kim HJ, Yun HS, Park HD, Kim DH, Park YC. Soft-tissue andcortical-bone thickness at orthodontic implant sites. Am J OrthodDentofacial Orthop 2006;130:177-82.
15. Poppe M, Bourauel C, J€ager A. Determination of the elasticityparameters of the human periodontal ligament and the locationof the center of resistance of single-rooted teeth: a study of
American Journal of Orthodontics and Dentofacial Orthoped
autopsy specimens and their conversion into finite elementmodels. J Orofac Orthop 2002;63:358-70.
16. Kuroda S, Sugawara Y, Deguchi T, KyungHM, Takano-Yamamoto T.Clinical use of miniscrew implants as orthodontic anchorage: successrates and postoperative discomfort. Am J Orthod Dentofacial Orthop2007;131:9-15.
17. Crismani AG, Bernhart T, Schwarz K, Celar AG, Bantleon HP,Watzek G. Ninety percent success in palatal implants loaded 1week after placement: a clinical evaluation by resonance frequencyanalysis. Clin Oral Implants Res 2006;17:445-50.
18. Park HS, Lee SK, Kwon OW. Group distal movement of teeth usingmicroscrew implant anchorage. Angle Orthod 2005;75:602-9.