Toward a Rational Toward a Rational Regulatory Policy for Regulatory Policy for Development of Drugs to Development of Drugs to Treat Diabetes Mellitus Treat Diabetes Mellitus Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical companies Clinical Trials: AstraZeneca, Eli Lilly, Takeda, Sankyo, Sanofi-Aventis, Roche, and Pfizer. Companies are directed to pay any honoraria, speaking or consulting fees directly to charity so that neither income nor
Transcript
Toward a Rational Regulatory Policy Toward a Rational Regulatory Policy for Development of Drugs to Treat for Development of Drugs to Treat
Diabetes MellitusDiabetes Mellitus
Toward a Rational Regulatory Policy Toward a Rational Regulatory Policy for Development of Drugs to Treat for Development of Drugs to Treat
Diabetes MellitusDiabetes Mellitus
Steven E. Nissen MDChairman, Department of Cardiovascular Medicine
Cleveland Clinic
Steven E. Nissen MDChairman, Department of Cardiovascular Medicine
Cleveland Clinic
Disclosure
Consulting: Many pharmaceutical companies
Clinical Trials: AstraZeneca, Eli Lilly, Takeda, Sankyo, Sanofi-Aventis, Roche, and Pfizer. Companies are directed to pay any honoraria, speaking orconsulting fees directly to charity so that neither income nor tax deduction is received.
Why are We Here?Why are We Here?Why are We Here?Why are We Here?
• The ACCORD trial demonstrated that a drug The ACCORD trial demonstrated that a drug regimen designed to lower blood glucose is regimen designed to lower blood glucose is capable capable of increasing mortality in diabetic patients.of increasing mortality in diabetic patients.
• Multiple rosiglitazone meta-analyses of CV Multiple rosiglitazone meta-analyses of CV outcomes showed improved glycemic control, but an outcomes showed improved glycemic control, but an increase in myocardial ischemic events.increase in myocardial ischemic events.
• Many agents to treat diabetes have failed duringMany agents to treat diabetes have failed duringdevelopment, some to cardiotoxicity.development, some to cardiotoxicity.
• No robust cardiovascular outcomes data existNo robust cardiovascular outcomes data existfor any current diabetes therapies.for any current diabetes therapies.
• In the absence of randomized CV outcomes trials, In the absence of randomized CV outcomes trials, we are left with unsatisfactory methods to assess we are left with unsatisfactory methods to assess benefit and risk. benefit and risk.
• These include meta-analyses or These include meta-analyses or post hoc post hoc data data “dredging” of randomized trials not designed to “dredging” of randomized trials not designed to determine the benefits or risks of determine the benefits or risks of specific specific therapies.therapies.
• This was particularly evident at the recent ADAThis was particularly evident at the recent ADAmeeting with attempts to determine the sourcemeeting with attempts to determine the sourceof the excess mortality in ACCORD.of the excess mortality in ACCORD.
• No amount of “torturing” of the data will enable riskNo amount of “torturing” of the data will enable riskassessment when specific drugs usage notassessment when specific drugs usage notrandomized.randomized.
ACCORDACCORDACCORDACCORD
Drug Class or NameIntensive Therapy
Standard Therapy
Repaglinide 50.2% 17.7%
Rosiglitazone 91.7% 58.3%
Insulin 77.3% 55.4%
glucosidase inhibitor 23.2% 5.3%
Bottom line: A regimen in which more patients received repaglinide, rosiglitazone, insulin and/or an glucosidase inhibitor showed increased mortality risk.
More than 50 years after the initial More than 50 years after the initial introduction of oral anti-diabetic drugs….introduction of oral anti-diabetic drugs….
More than 50 years after the initial More than 50 years after the initial introduction of oral anti-diabetic drugs….introduction of oral anti-diabetic drugs….
Although cardiovascular disease is the cause of death in 75% of diabetics, there exist no
Level of Evidence: Comparative Level of Evidence: Comparative Effectiveness Trials of Diabetes DrugsEffectiveness Trials of Diabetes Drugs
Level of Evidence: Comparative Level of Evidence: Comparative Effectiveness Trials of Diabetes DrugsEffectiveness Trials of Diabetes Drugs
Outcome Level of Evidence
All cause mortality Low to very low
CV disease mortality Low to very low
Nonfatal MI or stroke Low to very low
Peripheral vascular disease Low to very low
Microvascular outcomes Low to very low
The Knowledge GapThe Knowledge GapThe Knowledge GapThe Knowledge Gap
The absence of information on macrovascular effects of diabetes therapies is the unfortunate consequence of current regulatory policy that
emphasizes the importance of glucose lowering, not health outcomes, as a therapeutic goal.
This Approach Has Created a New DisorderThis Approach Has Created a New DisorderThis Approach Has Created a New DisorderThis Approach Has Created a New Disorder
Glucocentricity
The irrational belief that lowering blood sugar using virtually any pharmacological means will produce a
reliable reduction in adverse outcomes
glu-co-cen-tricity |ˈgloōkō senˈtrisitēnoun
Consequences of a “Glucocentric” Consequences of a “Glucocentric” Regulatory Approach to Diabetes DrugsRegulatory Approach to Diabetes Drugs
Consequences of a “Glucocentric” Consequences of a “Glucocentric” Regulatory Approach to Diabetes DrugsRegulatory Approach to Diabetes Drugs
• Pre-approval studies focus on demonstratingPre-approval studies focus on demonstratingmaximal glucose lowering effects.maximal glucose lowering effects.
• Patients are selected with relatively high HbA1cPatients are selected with relatively high HbA1clevels to enhance apparent “efficacy.”levels to enhance apparent “efficacy.”
• Studies seek “bragging” rights- “my drug lowersStudies seek “bragging” rights- “my drug lowersblood sugar more than your drug.”blood sugar more than your drug.”
• Patients at high CV risk are deliberately avoided.Patients at high CV risk are deliberately avoided.Why take a chance of an adverse safety signal?Why take a chance of an adverse safety signal?
Consequences of a “Glucocentric” Consequences of a “Glucocentric” Regulatory Approach to Diabetes DrugsRegulatory Approach to Diabetes Drugs
Consequences of a “Glucocentric” Consequences of a “Glucocentric” Regulatory Approach to Diabetes DrugsRegulatory Approach to Diabetes Drugs
• When safety signals arise, physicians stampede When safety signals arise, physicians stampede to the newest diabetes therapies (for which we to the newest diabetes therapies (for which we know the least about safety).know the least about safety).
• Example: After the rosiglitazone concernsExample: After the rosiglitazone concernsemerged, the fastest growing diabetes class isemerged, the fastest growing diabetes class isa new class, a DPP-IV inhibitor (sitagliptin).a new class, a DPP-IV inhibitor (sitagliptin).
• However, this agent has limited glucose lowering However, this agent has limited glucose lowering
efficacy (about half the effect of establishedefficacy (about half the effect of establishedtherapies) and virtually no long-term safety data. therapies) and virtually no long-term safety data.
The Principal DilemmaThe Principal DilemmaThe Principal DilemmaThe Principal Dilemma
How do we balance the need to bring new diabetes agents to patients in a timely fashion.
vs.
The need for more robust outcome datathat inform physicians of how
to use these drugs safely and effectively
Requiring a large CV outcomes trial prior to approval is undesirable, because this approach
would delay new diabetes therapies by 5-7 years.
Proposal: A Rational Approach to Proposal: A Rational Approach to Approval of New Diabetes DrugsApproval of New Diabetes DrugsProposal: A Rational Approach to Proposal: A Rational Approach to Approval of New Diabetes DrugsApproval of New Diabetes Drugs
A Compromise with Two ComponentsA Compromise with Two ComponentsA Compromise with Two ComponentsA Compromise with Two Components
A pre-approval set of clinical trials designedto rule out a high level of CV risk.
A large randomized outcomes trial that must be underway at the time of approval.
Pre-Approval Development ProgramPre-Approval Development ProgramPre-Approval Development ProgramPre-Approval Development Program
• Pre-approval trials of sufficient size andPre-approval trials of sufficient size andduration to rule out a HR of 2.0 for MACEduration to rule out a HR of 2.0 for MACE(upper 95% confidence interval). (upper 95% confidence interval).
• Required: Pre-specified pooling of CVRequired: Pre-specified pooling of CVoutcomes in all trials with adjudication by anoutcomes in all trials with adjudication by anindependent clinical endpoints committee.independent clinical endpoints committee.
• Useful: At least one study in patients at highUseful: At least one study in patients at highCV risk, perhaps 1000 patients for 1-2 years.CV risk, perhaps 1000 patients for 1-2 years.
MACE = major adverse CV events including death, MI, stroke, and hospitalization for revascularization
87 Events to Exclude Upper 95% CI of 2.087 Events to Exclude Upper 95% CI of 2.087 Events to Exclude Upper 95% CI of 2.087 Events to Exclude Upper 95% CI of 2.0
Active Control
43 44
48 39
35 52
53 34
1.23
0.67
1.56
0.4 0.5 2.01.51.0
Control betterActive better
2.50.67
0.98
Implications of This Regulatory ApproachImplications of This Regulatory ApproachImplications of This Regulatory ApproachImplications of This Regulatory Approach
• Positives:Positives:
– Encourages sponsors to include patientsEncourages sponsors to include patientswith higher levels of cardiovascular risk.with higher levels of cardiovascular risk.
– Provides more reliable pre-approval dataProvides more reliable pre-approval databy adjudication of CV events for pooled trialsby adjudication of CV events for pooled trials
• Negatives:Negatives:
– Modestly slows development programs,Modestly slows development programs,thereby delaying introduction of newthereby delaying introduction of newdiabetes medications by 6-12 monthsdiabetes medications by 6-12 months
Step II in Approval: An AdequatelyStep II in Approval: An AdequatelyPowered Cardiovascular Outcomes TrialPowered Cardiovascular Outcomes Trial
Step II in Approval: An AdequatelyStep II in Approval: An AdequatelyPowered Cardiovascular Outcomes TrialPowered Cardiovascular Outcomes Trial
• Assuming no evidence for excess CV risk (upperAssuming no evidence for excess CV risk (upper95% CI of HR <2.0), a new diabetes drug would be95% CI of HR <2.0), a new diabetes drug would beapprovable based on glucose-lowering efficacy…approvable based on glucose-lowering efficacy…
• If an adequately-powered ongoing CV outcomes trialIf an adequately-powered ongoing CV outcomes trialis underway (already enrolling patients).is underway (already enrolling patients).
• This outcomes study should also address any otherThis outcomes study should also address any otherongoing safety issues (renal, fractures, skin)ongoing safety issues (renal, fractures, skin)
• This policy is a compromise designed to balanceThis policy is a compromise designed to balancespeedy approval with the need to promptly obtainspeedy approval with the need to promptly obtainevidence of benefit (or risk).evidence of benefit (or risk).
Ongoing CV Study at Time of ApprovalOngoing CV Study at Time of ApprovalOngoing CV Study at Time of ApprovalOngoing CV Study at Time of Approval
MACE rate control group
12% reduction
15% reduction
18% reduction
Approximate sample size per treatment group
11% NA 6000 4000
13% 7500 5000 3500
15% 7000 4500 3000
17% 6000 4000 <3000
MACE Endpoint: Death, MI, stroke or ACS hospitalizationalpha=0.05 (two tailed) and 80% power
19901990-1994†-1994†
19951995-1999†-1999†
Total Total pendingpending
(9/30/2005)*(9/30/2005)*
Number of new drugsNumber of new drugswith a Phase IVwith a Phase IVcommitmentcommitment
8888 107107 12311231
Number of Phase IVNumber of Phase IVcommitments completedcommitments completed 1111 00 172172
Promises Not Kept: Phase IV CommitmentsPromises Not Kept: Phase IV CommitmentsPromises Not Kept: Phase IV CommitmentsPromises Not Kept: Phase IV Commitments
Quality of Cardiovascular Quality of Cardiovascular Outcomes Trial: A Critical IssueOutcomes Trial: A Critical Issue
Quality of Cardiovascular Quality of Cardiovascular Outcomes Trial: A Critical IssueOutcomes Trial: A Critical Issue
Characteristic ACCORD ADVANCE
History of macrovascular disease
35% 32%
Statins 88% 47%
Aspirin 76% 56%
ACE Inhibitor 71% Not reported
Those who cannot remember the past are condemned to repeat it.
George Santayana, a Spanish-born American author in 1905
Dual PPARs: A Promising ApproachDual PPARs: A Promising ApproachDual PPARs: A Promising ApproachDual PPARs: A Promising Approach
• Both hyperlipidemia and insulin resistance appear to promote atherosclerosis in diabetics.
• Accordingly, pharmaceutical companies have sought to develop dual and PPAR agonists combining:
• Fibrate-like effects, raising HDL and lowering triglycerides
The first dual PPAR to reachthis stage of the approval process
Muraglitazar Development ProgramMuraglitazar Development ProgramMuraglitazar Development ProgramMuraglitazar Development ProgramCV 168006CV 168006104 weeks104 weeks
The Panel Meeting September 5, 2005The Panel Meeting September 5, 2005The Panel Meeting September 5, 2005The Panel Meeting September 5, 2005
• Although there appears to be an higher incidenceAlthough there appears to be an higher incidenceof major adverse cardiovascular events, the of major adverse cardiovascular events, the sponsor argues there there is:sponsor argues there there is:
• ““Lack of biologic plausibility for CV risk with Lack of biologic plausibility for CV risk with muraglitazar based on”:muraglitazar based on”:
Beneficial effects on markers of CV riskBeneficial effects on markers of CV risk
Broad diversity among reported CV eventsBroad diversity among reported CV events
No increase in CV events with increasing doseNo increase in CV events with increasing dose
Absence of off-target CV toxicity in non-clinicalAbsence of off-target CV toxicity in non-clinicalor clinical studiesor clinical studies
The panel votes 8:1 to approve muraglitazar as monotherapy and 7:2 to
approve use with metformin.
They vote 7:2 against approval in combination with sulfonylureas, requesting
more data.
Six Weeks after the Advisory PanelSix Weeks after the Advisory PanelSix Weeks after the Advisory PanelSix Weeks after the Advisory Panel
Individual Components of CompositeIndividual Components of CompositeIndividual Components of CompositeIndividual Components of Composite
EndpointMuran (%)
Controlsn (%)
RR95%CI
pvalue
All cause mortality16/2374(0.67)
3/1351(0.22%)
3.05 0.89-10.47 0.08
CV death8/2374(0.34%)
1/1351(0.07%)
4.57 0.57-36.53 0.15
Fatal or nonfatal MI15/2374(0.63%)
9/1351(0.30%)
2.14 0.71-6.46 0.18
Fatal or nonfatal stroke9/2374(0.38%)
2/1351(0.15%)
2.57 0.55-11.89 0.23
Fatal or nonfatal TIA5/2374(0.21%)
1/1351(0.07%)
2.85 0.33-24.4 0.34
Adjudicated CHF13/2374(0.55%)
1/1351(0.07%)
7.43 0.97-56.83 0.053
Commonly Used CV Composite EndpointsCommonly Used CV Composite EndpointsCommonly Used CV Composite EndpointsCommonly Used CV Composite Endpoints
EndpointMuran (%)
Controlsn (%)
RR95%CI
pvalue
All cause mortalityor nonfatal MI
27/2374(1.14%)
7/1351(0.52%)
2.21 0.96-5.08 0.06
CV death or nonfatal MI19/2374(0.80%)
5/1351(0.37%)
2.17 0.81-5.83 0.12
All cause mortalityplus nonfatal MI or stroke
35/2374(1.47%)
9/1351(0.67%)
2.23 1.07-4.66 0.03
CV death+ nonfatal MI or Stroke
27/2374(1.14%)
7/1351(0.52%)
2.21 0.96-5.08 0.06
All causemortality+nonfatal MI,stroke, TIA, or CHF
• The FDA issues an “approvable” letter requesting additional CV safety data.
• After ongoing extension trials confirm the CV hazard, all development of the drug halted.
• However, a risky agent came close to approval.
• A clear standard requiring an upper CI <2.0for the HR for CV events would have precluded the necessity for an advisory panel.
The slippery slope of surrogate endpoints The slippery slope of surrogate endpoints in diabetes drug developmentin diabetes drug development
The slippery slope of surrogate endpoints The slippery slope of surrogate endpoints in diabetes drug developmentin diabetes drug development
• Ezetimibe was approved to treatEzetimibe was approved to treathyperlipidemia on the basis of a reductionhyperlipidemia on the basis of a reductionin LDL-C averaging 16-18%in LDL-C averaging 16-18%
• What should we do with a diabetes drugWhat should we do with a diabetes drugthat lowers blood sugar (HbA1c by 1.1%),that lowers blood sugar (HbA1c by 1.1%),but increases LDL-C by 16-18%?but increases LDL-C by 16-18%?
If a 16-18% reduction in LDL-C is sufficient to demonstrate benefit, what inference should we draw
when a drug increases LDL-C by a comparable amount?
If a 16-18% reduction in LDL-C is sufficient to demonstrate benefit, what inference should we draw
when a drug increases LDL-C by a comparable amount?
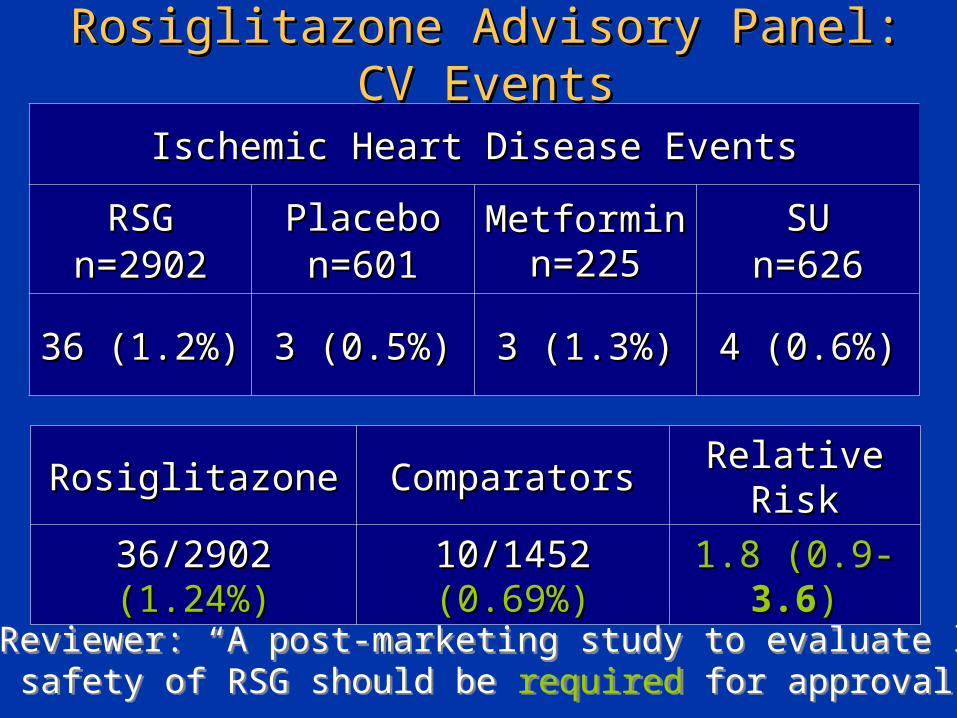
FDA Reviewer: “A post-marketing study to evaluate long-term safety of RSG should be required for approval.”FDA Reviewer: “A post-marketing study to evaluate long-term safety of RSG should be required for approval.”
What Happened to Mandated SafetyWhat Happened to Mandated SafetyStudy of Rosiglitazone? The Adopt TrialStudy of Rosiglitazone? The Adopt Trial
What Happened to Mandated SafetyWhat Happened to Mandated SafetyStudy of Rosiglitazone? The Adopt TrialStudy of Rosiglitazone? The Adopt Trial
• Not a safety study, a “marketing” study, designedNot a safety study, a “marketing” study, designedto show greater durability of glucose loweringto show greater durability of glucose loweringwith rosiglitazone.with rosiglitazone.
• Cardiovascular events collected in a haphazardCardiovascular events collected in a haphazardfashion (not adjudicated!)fashion (not adjudicated!)
• Because of the LDL-raising effect of rosiglitazone,Because of the LDL-raising effect of rosiglitazone,more patients received statins (p<0.01).more patients received statins (p<0.01).
• HR 1.33 for myocardial infacrtion (0.80-2.21).HR 1.33 for myocardial infacrtion (0.80-2.21).The pre-approval signal never goes away!The pre-approval signal never goes away!
• Many small, short term “marketing” studies to Many small, short term “marketing” studies to show glycemia reduction in various populations.show glycemia reduction in various populations.
• No well-designed randomized trials to measureNo well-designed randomized trials to measurehealth outcomes (RECORD underpowered).health outcomes (RECORD underpowered).
• By 2007, 42 trials were completed with 14,237By 2007, 42 trials were completed with 14,237patients.patients.
• FDA analysis in July 2007: Odds ratio forFDA analysis in July 2007: Odds ratio formyocardial ischemia 1.4 (95% CI 1.1-1.8)myocardial ischemia 1.4 (95% CI 1.1-1.8)
• The pre-approval signal never goes away!The pre-approval signal never goes away!
Rosiglitazone in RetrospectRosiglitazone in RetrospectRosiglitazone in RetrospectRosiglitazone in Retrospect
• If an upper CI <2.0 for the HR for CV events If an upper CI <2.0 for the HR for CV events had been required for approval in 1999, had been required for approval in 1999, rosigltazone would not have been approved rosigltazone would not have been approved without more safety data.without more safety data.
• If a large, well-powered outcomes trial had If a large, well-powered outcomes trial had been mandated in 199, we would not have to been mandated in 199, we would not have to wait until 2014 (15 years after approval) to wait until 2014 (15 years after approval) to determine if this drug is safe or not.determine if this drug is safe or not.
PPARs: a Special CasePPARs: a Special CasePPARs: a Special CasePPARs: a Special Case
• At least 50 IND’s filed following last approvalAt least 50 IND’s filed following last approvalof a TZD, nearly all terminated due to toxicity.of a TZD, nearly all terminated due to toxicity.
• Toxicities observed in animals are also evident Toxicities observed in animals are also evident clinically - cardiac, skeletal muscle, renal, bone clinically - cardiac, skeletal muscle, renal, bone marrow. (El Hage)marrow. (El Hage)
• Most development programs terminated withoutMost development programs terminated withoutany publication of the toxicities encountered.any publication of the toxicities encountered.
• PPARs all activate different genes and must bePPARs all activate different genes and must beconsidered individually- this is NOT a “drugconsidered individually- this is NOT a “drugclass” class”
• At least 50 IND’s filed following last approvalAt least 50 IND’s filed following last approvalof a TZD, nearly all terminated due to toxicity.of a TZD, nearly all terminated due to toxicity.
• Toxicities observed in animals are also evident Toxicities observed in animals are also evident clinically - cardiac, skeletal muscle, renal, bone clinically - cardiac, skeletal muscle, renal, bone marrow. (El Hage)marrow. (El Hage)
• Most development programs terminated withoutMost development programs terminated withoutany publication of the toxicities encountered.any publication of the toxicities encountered.
• PPARs all activate different genes and must bePPARs all activate different genes and must beconsidered individually- this is NOT a “drugconsidered individually- this is NOT a “drugclass” class”
Bioinformatics. 2004 Nov 22;20(17):3108-27. Epub 2004 Jun 24.
Gene Expression with PPAR Gene Expression with PPAR AgentsAgentsGene Expression with PPAR Gene Expression with PPAR AgentsAgents
TroglitazoneRosiglitazone
Pioglitazone
23135
12
Pooled TZDs
10
12
26
5
2
02
Matrixmetalloproteinase
Diabetes, Glycemia and CV DiseaseDiabetes, Glycemia and CV DiseaseDiabetes, Glycemia and CV DiseaseDiabetes, Glycemia and CV Disease
• The goal of merely lowering blood glucose levelsThe goal of merely lowering blood glucose levelsin diabetes is too simplistic. We must reduce the in diabetes is too simplistic. We must reduce the complications of diabetes, including CV disease.complications of diabetes, including CV disease.
• With respect to CV disease it appears importantWith respect to CV disease it appears importanthow how you lower blood sugar as well as you lower blood sugar as well as how muchhow much..
• Diabetes drugs, even within the same “class” may Diabetes drugs, even within the same “class” may yield dramatically different CV outcomes.yield dramatically different CV outcomes.
• Clinical outcomes trials comparing alternative Clinical outcomes trials comparing alternative diabetes therapies are essential to determine the diabetes therapies are essential to determine the optimal approach to prevent CV morbidity-mortality. optimal approach to prevent CV morbidity-mortality.
Two Components: A new paradigm for Two Components: A new paradigm for Diabetes Drug developmentDiabetes Drug development
Two Components: A new paradigm for Two Components: A new paradigm for Diabetes Drug developmentDiabetes Drug development
• Sufficient pre-approval data to exclude a Sufficient pre-approval data to exclude a excess hazard of CV events (an upper CI excess hazard of CV events (an upper CI for the hazard ratio not to exceed 2.0.for the hazard ratio not to exceed 2.0.
• A robust post-approval outcome programA robust post-approval outcome programto provide data in a timely fashion (anto provide data in a timely fashion (anongoing outcomes trial at the time of ongoing outcomes trial at the time of approval)approval)