Traditional Medical Beliefs and the Impact of Hygiene Instruction Daniel Bennett Syed Ali Asjad Naqvi Wolf-Peter Schmidt March 21, 2014 Abstract Many people throughout the world believe in traditional, unscientific causes of disease. These beliefs may undermine public health efforts such as hygiene campaigns, which invoke the germ theory of disease. We evaluate a novel program that tries to increase the salience of hygiene instruction by showing participants live microbes from their environment under a microscope. We find that this program has a larger effect on hygiene knowledge, hygiene behavior, and respondent and child health than instruction alone. However, we also show (consistent with Bayesian learning) that only non-believers in traditional medicine respond to the intervention. This pattern suggests that traditional beliefs contribute to the communicable disease burden in developing countries. Finally, we show that pre-existing behavioral constraints limit the program’s impact on hygiene, illustrating a key limitation of instructional interventions. Daniel Bennett: University of Chicago, [email protected]; Asjad Naqvi: Vienna University of Economics and Business, [email protected]; Wolf-Peter Schmidt: London School of Hygiene and Tropical Medicine, [email protected]. We received helpful feedback from Dan Black, Jeff Grogger, and Edward Higgins.
Transcript
Traditional Medical Beliefs and theImpact of Hygiene Instruction
Daniel Bennett Syed Ali Asjad Naqvi Wolf-Peter Schmidt
March 21, 2014
Abstract
Many people throughout the world believe in traditional, unscientific causes ofdisease. These beliefs may undermine public health efforts such as hygiene campaigns,which invoke the germ theory of disease. We evaluate a novel program that triesto increase the salience of hygiene instruction by showing participants live microbesfrom their environment under a microscope. We find that this program has a largereffect on hygiene knowledge, hygiene behavior, and respondent and child health thaninstruction alone. However, we also show (consistent with Bayesian learning) that onlynon-believers in traditional medicine respond to the intervention. This pattern suggeststhat traditional beliefs contribute to the communicable disease burden in developingcountries. Finally, we show that pre-existing behavioral constraints limit the program’simpact on hygiene, illustrating a key limitation of instructional interventions.
Daniel Bennett: University of Chicago, [email protected]; Asjad Naqvi: Vienna University ofEconomics and Business, [email protected]; Wolf-Peter Schmidt: London School of Hygiene and TropicalMedicine, [email protected]. We received helpful feedback from Dan Black, Jeff Grogger,and Edward Higgins.
1 Introduction
Traditional medical beliefs are common throughout the world. Traditional medicine accounts
for 30-50 percent medical consumption in China, and up to 80 percent of consumption in
parts of Sub-Saharan Africa (WHO 2003). In South Asia, which is the focus of this study,
many people subscribe to Unani medicine, in which illnesses arise through imbalance between
humorally “hot” and “cold” elements (Anwar et al. 2012, Karmakar et al. 2012). Hakims,
who provide Unani medical care, are active in markets throughout the region (Banerjee et
al. 2004, Das and Hammer 2005).
Traditional medical beliefs may contribute to the global disease burden by discourag-
ing healthy behavior. Traditional health practices potentially crowd out modern practices
if these inputs are substitutes in the health production function or the household budget
constraint. Unani beliefs are a particular threat to the adoption of modern hygiene and san-
itation practices, which call upon the germ theory of disease. In the Unani system, eating
too much food or eating foods that are humorally hot leads to diarrhea (Nielsen et al. 2003).
A belief that humoral imbalances cause infection reduces the impetus to was hands and
maintain latrines. Traditional and modern practices sometimes clash more directly. Oral
rehydration (including breast milk) is the consensus treatment for infant diarrhea. However
Unani medicine recommends withholding breast milk from infants with diarrhea because
working in the fields makes a woman’s breast milk hot (Mull and Mull 1988).1
Microbe Literacy is a novel hygiene program that tries to make hygiene messages salient
to people with traditional medical beliefs. Despite the policy importance of hygiene instruc-
tion, policymakers have struggled to communicate hygiene messages effectively (Fewtrell et
al. 2005, Monte et al. 1997). Microbe Literacy facilitators use microscopes to show partici-
pants the microbes that are present in everyday substances from their environment, such as
standing water and buffalo dung. For many participants, who are mostly poor and illiterate,
1As another example, some traditional healers in Sub-Saharan Africa advocate ritual bloodletting as atreatment for AIDS (Hrdy 1987).
1
the demonstration is the first time they have conceived of microscopic life. Instructors begin
by using magnifying glasses to demonstrate the concept of magnification. Then participants
take turns looking through a microscope while others observe on a closed-circuit television.
In a follow-up infection prevention workshop, instructors lead a discussion of hygiene best
practices, such as hand washing, latrine usage, and food safety.
We evaluate this program through a cluster-randomized trial. We offered Microbe Lit-
eracy to female participants in existing government-sponsored adult literacy classes (ALCs)
in southern Punjab Province, Pakistan. ALC students tend to be socioeconomically disad-
vantaged and lack formal schooling. The experiment includes three arms, which respectively
received the full program, only the infection prevention workshop, and no programming.
This design allows us to measure the impact of the program both absolutely and relative
to conventional hygiene instruction. We measure knowledge through several factual hygiene
questions, and gauge hygiene behavior by directly observing the personal appearance of the
respondent and her children. We also elicit the prevalence of diarrhea, fever, and cough for
the respondent and her young children.
Microbe Literacy significantly improves hygiene knowledge and behavior. The program
increases hygiene knowledge by 0.37 standard deviations (14 percent) and improves the
personal appearance of respondents by 0.29 standard deviations (8 percent). The program
has a larger effect on respondent hygiene than child hygiene, and it does not affect household
sanitation outcomes such as open defecation, which the participant does not directly control.
Microbe Literacy does not significantly reduce diarrhea, but reduces fever and cough by 44-46
percent for the respondent and by 19-34 percent for children younger than five. It generally
has a larger effect than standard hygiene instruction, although the difference is not always
significant.
To explore how traditional beliefs mediate the effect of the program, we aggregate several
indicators of adherence to traditional medicine into a traditional belief index (TBI). These
variables focus on beliefs in aspects of the hot/cold theory of disease and hypothetical and
2
actual utilization of hakims. We find that people without strong traditional beliefs learn
the most from the program. The effect on knowledge is small and insignificant for strong
adherents to traditional medicine, but is over four times larger and highly significant for
people without traditional beliefs. The result is robust if we control for the interaction
between treatment and 19 demographic and economic characteristics, which minimizes the
concern that the TBI proxies for socioeconomic status. This finding is consistent with a
Bayesian learning model in which traditional medicine adherents have more precise prior
beliefs. It also suggests that the program does not successfully reach people with strong
traditional beliefs.
Hygiene knowledge only changes behavior if recipients can overcome practical constraints
on behavior change. Hygiene is potentially inconvenient and expensive. Young women in
culturally conservative households may have little bargaining power over hygiene inputs.
We assess the relevance of these constraints by constructing a hygiene propensity score that
incorporates constraints based on economic circumstances, the lack of female empowerment,
and the physical environment.2 By interacting treatment with the propensity score and the
TBI, we show that the program primarily improves hygiene for people who are unconstrained
and do not hold traditional beliefs. We consider the relative importance of economic, social,
and practical constraints by creating separate propensity scores by category. Economic and
social factors appear to limit the impact on hygiene more than practical factors.
This study makes three primary contributions. We establish experimentally that a
program to increase the salience of hygiene instruction improves learning, behavior change,
and health. Existing public health studies of hygiene instruction, which have mixed results
(Davis et al. 2011, Beau De Rochars et al. 2011), do not formally examine why programs
may or may not be effective. Secondly, we show that traditional beliefs limit the acquisition
2Economic variables include housing characteristics, food deprivation, and education. Social variablesmeasure the patriarchal orientation of the household, include whether the respondent needs permission tohave female friends, whether she is a decision maker regarding the schooling of children, and whether sheinteracts with people outside of the village. Practical variables include water supply and latrine characteristicsand the presence of animals.
3
of hygiene knowledge through the program. This result suggests that traditional beliefs
contribute to the global burden of disease by discouraging health behaviors. Little or no
economic research assesses the health implications of traditional beliefs, which are ubiquitous
in both rich and poor countries. Finally, we show that economic and social factors limit the
program’s impact on behavior. To improve health, informational interventions must first
improve knowledge and behavior. The lengthy causal chain may make hygiene instruction
less cost effective than more expensive sanitation and water supply projects that directly
affect behavior and health.
We proceed in Section 2 describes the context, the setting, and the intervention. Section
3 describes our empirical strategy, including the randomization and data collection. Section
4 presents results, and Section 5 concludes.
2 Context
We conducted this study in rural parts of four districts in southern Punjab Province, Pak-
istan. Although this region produces abundant wheat and cotton, residents are relatively
poor because of the unequal land distribution. The population is predominantly Sunni Mus-
lim, although people belong to several sects. Communities are culturally conservative and
practice Purdah, which limits the interaction of women outside of the village.
The National Commission for Human Development (NCHD) regularly conducts adult
literacy classes throughout the country. Classes are gender-segregated and typically take
place in the home of an affluent member of the village. The classes are free to participants,
include around 25 people per class, and aim to establish basic literacy and numeracy. Classes
meet for 90 minutes per day, six days a week, for six months. The median age for participants
in our sample is 25, with ages ranging from 15 to 60. Because more affluent people seek
formal schooling, ALC participants are generally poorer than average.
Many people in rural Pakistan hold traditional beliefs about the causes of illness. Some
of these beliefs derive from Unani medicine, which emphasizes humoral “hot” and “cold”
4
states (Mull and Mull 1988). A person achieves health through balance between hot and
cold states, which do not correspond to physical temperature. Foods and activities have hot
and cold properties. Because diarrhea is a symptom of excess heat in the body, a person
with diarrhea should avoid other heat sources and consume cold foods. A mother’s hot or
cold status is believed to influence the quality of her breast milk. Working in the field makes
a mother’s breast milk hot and less suitable as a food source. People also perceive that
consuming too much food may lead to diarrhea. Nielsen et al. (2003) find that “when eating
too much, the food could not circulate properly in the stomach, resulting in incomplete
digestion and diarrhea.” In our sample, 93 percent of respondents believe that eating hot
foods is a cause of diarrhea.
People seek care from both traditional and Western health care providers, including con-
currently for the same illness (Hunte and Sultana 1992). Traditional medicine practitioners
known as hakims advocate Unani, herbal, and Ayurvedic remedies. A common treatment is
a taveez, or amulet, which is inscribed with religious sayings. People can seek Western health
care from both public and private clinics, as well as from lady health workers (LHWs), who
travel from village to village. Anwar et al. (2012) argue that people distrust public health
care providers in Pakistan because the standards of care in the public system are so poor.
The high cost and lack of access to Western care also encourages people to seek traditional
medical treatments. 41 percent of respondents in our sample trust hakims “ a good amount”
or “a great deal.”
2.1 Description of the Intervention
Microbe Literacy (ML) is a novel hygiene-education program developed by the South Asia
Fund for Health and Education (SAFHE), an international non-profit organization. The
ML curriculum incorporates a microscope demonstration and an infection privation work-
shop, each of which requires 90 minutes of class time. Facilitators begin the microscope
demonstration by using magnifying glasses to illustrate the concept of magnification. Next
5
they explain that a microscope allows someone to see small things with even more powerful
magnification. Each workshop uses one microscope, which is connected to a monitor so that
everyone can see at once. Facilitators create slides using nearby substances likely to contain
microbes, such as standing water, buffalo dung, and spoiled food.
The infection prevention (IP) workshop takes place approximately one week after the
microscope demonstration. Instructors teach participants about the different ways that
communicable diseases can be transmitted. Participants learn good hygiene and sanitation
practices, including hand washing with soap, proper food handling and storage, and water
purification. They learn to avoid open defecation and garbage disposal and to maintain a
clean cooking area. Participants learn to treat diarrhea through oral rehydration. This cur-
riculum captures the essential components of hygiene education as it is practiced elsewhere.
Field reports suggest that the intervention leaves a strong impression on participants.
One facilitator describes a microscope workshop: “It was amazing for women to see the bac-
teria on the slides which had been sampled from their homes. Women were very astonished
to know how much bacteria live around them. They expressed that they will be careful to
avoid microbes for themselves and for their children.” A facilitator described an infection
prevention workshop: “Women said that they get sick every week, but now they will take
preventative measures and they are hopeful they will never get sick.”
Ahmad et al. (2012) conducted a pilot study of Microbe Literacy in the Swat Valley of
Pakistan. The authors report that baseline diarrhea prevalence is 52 percent among children
under age 5, which is 50 percent higher than in our sample. In this study, ML reduces
diarrhea by 65 percent and respiratory illness by 76 percent. The study employs a pre-post
methodology, which means that seasonal variation in disease conditions may confound the
results.
6
2.2 Data and Sampling Methodology
We collaborated with the NCHD to implement a randomized evaluation of Microbe Literacy
in the spring of 2013. The NCHD operated 605 ALCs for women in the districts of Rahim
Yar Khan, Muzaffargarh, Bahawalnagar, and Lodhran during this period. We selected 210
adult literacy classes and concentrated on Lodhran and Rahim Yar Khan districts. We
enrolled all eligible ALC participants who were present in class for the baseline survey and
excluded participants under age 15. Surveyors conducted interviews in respondents’ homes
to avoid interference from other classmates.
The survey instrument measures the respondent’s demographic and economic charac-
teristics, health, knowledge of disease pathways, and adherence to traditional medicine. We
measure knowledge by asking respondents whether they agree or disagree with four state-
ments: “Untreated water is safe to drink”, “I can tell if my hands are dirty just by looking
at them”, ”It is safe to eat food that has been touched by flies”, and “The worst thing diar-
rhea can do is make my child uncomfortable.” The correct answer to all of these questions
is “false”, so that respondents cannot answer correctly simply by agreeing with surveyors.
Over 50 percent of respondents believe that they can directly observe whether their hands
are dirty, and over 80 percent believe that diarrhea is not a serious health risk for children.
We sum the correct responses to create a knowledge score. Respondents correctly answer
around two out of four questions correctly in the baseline.
We measure hygiene by directly observing the personal appearance of the respondent
and her children. Surveyors measured this outcome on a three-point Likert scale, which we
standardized by providing an example image for each possible response, which we show in
Appendix Figure 1. This approach avoids relying self-reports, which are unreliable for a
socially-desirable behavior such as hygiene. Appendix Table 1 shows that personal appear-
ance is strongly correlated with other hygiene and sanitation outcomes that are available in
the baseline survey. We also show results for the presence of open defecation and garbage and
the cleanliness of the cooking area, which reflect household rather than individual behavior.
7
We measure health by eliciting the incidence of diarrhea, fever, and cough for the re-
spondent and her three youngest children within the past two weeks.3 We limit the child
sample to children younger than five because young children are the most susceptible to
diarrhea and for consistency with other data sources. This limitation does not have an
important effect on our estimates. Improved hygiene may also reduce fever and cough in-
cidence. Cough indicates upper respiratory infection, while fever is the symptom of several
illnesses, including diarrheal infections. As Schmidt et al. (2011) note, diarrhea is measured
with error because respondents have varying interpretations of what constitutes diarrhea.
Fever and cough arguably contain less measurement error because the interpretation of these
symptoms is less idiosyncratic. For respondents, baseline diarrhea, cough, and fever are 13
percent, 26 percent, and 17 percent respectively. For their children younger than five, these
incidences are 34 percent, 36 percent, and 24 percent.
We conducted a follow-up survey in August and September 2013, around 14 weeks
after the intervention. The follow-up questionnaire closely resembles the baseline question-
naire but does not include some socioeconomic variables that would be unlikely to vary
over the timespan. The follow-up occurred immediately after Ramadan, during the rainy
season. Incidence of diarrhea is lower during this period. Seasonality may also affect re-
sponses to hygiene knowledge questions because some respondents may have answers that
are seasonally-specific. For instance, respondents may believe that hand contamination is
more visible during the dry season than during the rainy season.
To examine how traditional beliefs mediate the impact of the program, we develop a
traditional belief index using several baseline indicators. These variables include whether the
3Following the recommendation of Schmidt et al. (2010) and Schmidt et al. (2011), we elicit diarrhea overboth one-week and two-week horizons. The one-week horizon reduces measurement error due to lack of recall,while the two-week horizon is easier to compare to other data sources. To assess whether surveyor promptingaffected our responses, we administered two versions of the diarrhea question to random subsamples ofrespondents. In the prompted version, the surveyor provided the definition of diarrhea as three loose stoolswithin 24 hours before asking if the respondent or her children had experienced diarrhea. In the unpromptedversion, the surveyor asked if the respondent or her children had experienced any illness and only recordedresponses matching the definition of diarrhea. This distinction did not lead to meaningful differences indiarrhea prevalence.
8
respondent believes that (1) eating hot foods causes diarrhea, (2) eating cold foods causes
diarrhea, (3) withholding foods and liquids is an effective treatment for diarrhea, (4) with-
holding breast milk is an effective treatment for diarrhea, and (5) other home remedies are
effective treatments for diarrhea. We also include whether the respondent (6) has consulted
a hakim within the past three months, (7) would consult a hakim if her child was having fits
(seizures), and (8) would consult a hakim if her child was having fainting spells.4 The TBI
is the unweighted sum of these outcomes, and varies from 0 to 8, with a median of 3. Figure
1 shows the frequency distribution of the TBI. As an alternative, we also define the TBI as
the first principal component of these variables.
Adherence to traditional beliefs is correlated with socioeconomic status. Appendix Table
2 shows how key variables in our analysis differ for people with above-median and below-
median values of the TBI. Non-believers in traditional medicine are younger, more literate,
and somewhat less religious. They live in somewhat nicer housing and they are more likely
to have animals. These respondents and their children have lower incidence of diarrhea,
fever, and cough, although the causal relationship between these variables is ambiguous.
Interactions with the TBI may capture these socioeconomic and health differences rather
than traditional beliefs per say. As a robustness test to address this concern, regressions with
TBI interactions also control for the interaction of treatment with all of the demographic
and economic variables in this table.
3 Empirical Approach
3.1 Study Design
Our study incorporates three treatment arms. The Microbe Literacy (ML) arm received
both the microscope demonstration and the infection prevention workshop. The Infection
Prevention (IP) arm received only the infection prevention workshop. The Control arm
4We elicited the hypothetical responses to fits and fainting spells because these morbidities have vaguecauses and have both traditional and Western explanations.
9
received no hygiene education through the program. Before randomizing, we groups ALCs
into 110 geographic clusters, which we defined so that all clusters were at least 1 kilometer
apart. Based on this limitation, control ALCs are a median of 3 kilometers from the nearest
ALC in the ML arm. We stratified by grouping clusters into three diarrhea prevalence
categories and four districts, which led to a total of 12 cells containing an average of 17.5
ALCs.
Geographic proximity creates the possibility that information from the treatment may
reach control respondents. In practice, treatment contamination does not appear to be a
serious concern. The practice of Purdah severely limits the ability of females to interact with
people outside of their village. In our baseline survey, 69 percent of respondents had not
spoken to anyone outside of their village and 62 percent had not traveled outside of their
village in the past seven days. In the follow-up, only 8 percent of control respondents had
heard of an event involving microscopes. Results below do not change if we discard control
respondents who live near the treatment or are aware of the program.
We assess the validity of the randomization by comparing the baseline characteristics
of respondents by treatment status. Table 1 includes 19 demographic and economic char-
acteristics, including age, marital status, religion, assets, and labor supply. The table also
summarizes the knowledge, hygiene, health outcome variables. Columns 1 through 3 report
the baseline mean for each treatment arm. Columns 4 and 5 show p-values for the difference
between the ML and IP arms, and between the ML and C arms respectively.5 5.7 percent of
the mean comparisons in this table are statistically significant at 5 percent, which supports
the validity of the randomization.
Our stratification procedure ensures balance in health variables across treatment arms
but may yield economically meaningful baseline imbalances in other variables.6 The demo-
graphic variables in Table 1 do not vary systematically by treatment arm, however individual
5We obtain p-values by regressing each variable on treatment dummies while controlling for strata dum-mies and clustering by randomization group, which is consistent with our main estimation strategy below.
6Bruhn and McKenzie (2009) argue that rerandomization, which improves balance on all observables,does not increase the validity of the randomization but instead shifts imbalance onto unobservables.
10
variables sometimes show imbalance. Although hygiene behavior and health outcomes are
generally balanced in Table 1, hygiene knowledge is notably imbalanced: ML respondents
answer around 0.2 fewer questions correctly than either IP or control respondents. The
magnitude of this imbalance may make it difficult to identify a treatment effect through a
standard cross-sectional regression.
Our regressions are based on the following specification in which i indexes the respondent
and j indexes the ALC. We estimate this specification using only data from the follow-up
round.
Yij = β1MLj + β2IPj + β3Ybij + Sj + εij (1)
ML and IP are indicators for the Microbe Literacy and Infection Prevention arms. Y bij
is the baseline value of the dependent variable, and Sj is a vector of strata dummies. If
the dependent variable is balanced in the baseline, controlling for Y bij improves precision
by absorbing variation in the dependent variable. We control for strata dummies because
random assignment occurs within strata (Kernan et al. 1999). We cluster standard errors
by randomization group.
As we discuss above, hygiene knowledge happens to be imbalanced across treatment arms
in the baseline. This imbalance interferes with the ability to detect a treatment effect if the
treatment causes arms to achieve greater balance than they had in the baseline. Because
knowledge is initially lower in the ML arm than the control arm, a specification such as
Equation (1) may fail to find a treatment effect since knowledge levels have converged by
the follow-up. We address this concern by estimating the effect on hygiene knowledge as a
difference-in-difference in addition to the specification above.
Yijt = β1POSTt ·MLj + β2POSTt · IPj (2)
+ β3MLj + β4IPj + β5POSTt + Sj + εijt
11
The difference-in-difference nets out the difference in baseline levels and identifies a treatment
effect using the differential change in the outcome.7
We supplement estimates of these specifications with regressions that incorporate inter-
actions with the traditional belief index. A negative coefficient on the interaction between
MLj and TBIij indicates that the impact of ML is weaker for respondents who hold tra-
ditional beliefs. Traditional beliefs are not randomly assigned, and may be correlated with
other factors that mediate the impact of the program. We address the concern that the
TBI may proxy for socioeconomic status by controlling for the interaction of ML and IP
with a long list of socioeconomic characteristics. These characteristics include age, liter-
acy, education, marital status, household size, religious sect, religious adherence (number of
fasting days during the most recent Ramadan; number of prayers per day), house character-
istics, roof characteristics, savings, land, livestock, electricity, refrigerator and mobile phone
ownership, agricultural employment, and female labor force participation.
4 Results
4.1 The Impact of Microbe Literacy
We begin by showing the impact of Microbe Literacy on hygiene knowledge, hygiene behavior,
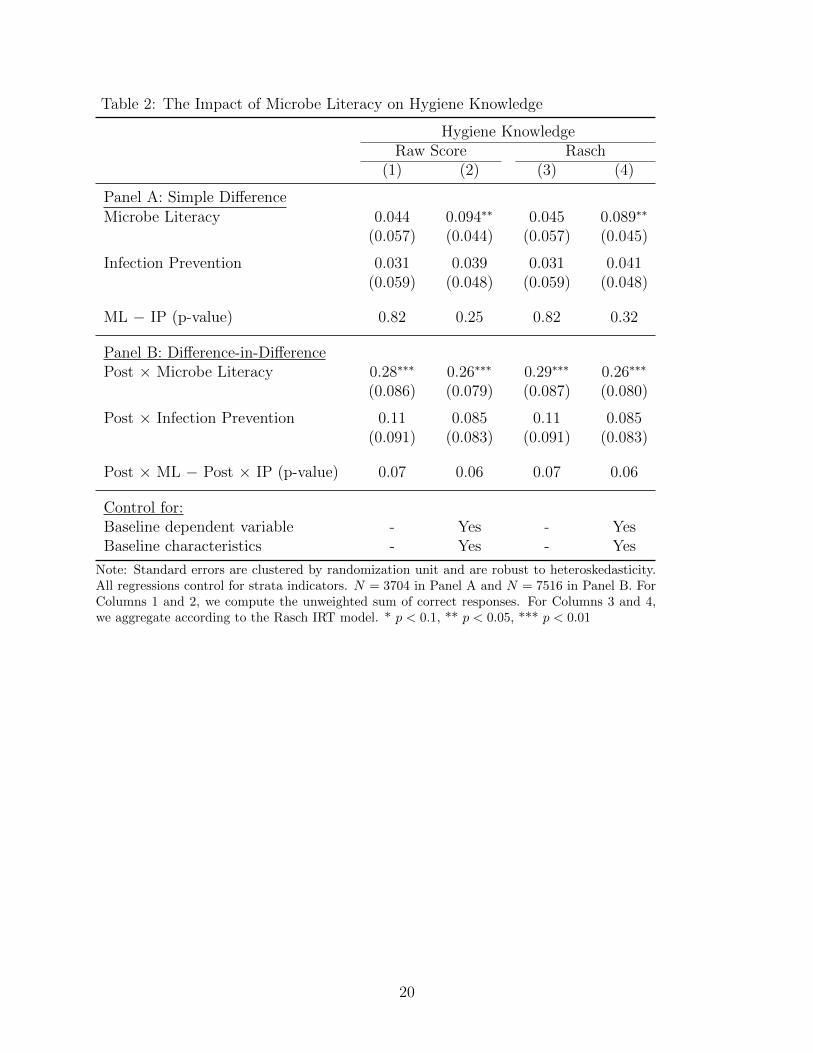
and health. Table 2 shows the effect of Microbe Literacy on hygiene knowledge. Panel A
shows results based on a cross-sectional regression in the follow-up period (Specification 1)
while Panel B shows results based on a difference-in-difference specification. Columns 1 and
2 estimate the impact on the raw knowledge score, which is the unweighted sum of correct
responses. Columns 3 and 4 estimate the impact on the Rasch score, which utilizes item
response theory to weight questions according to their difficulty.
Column 1 of Panel B shows our preferred specification, in which Microbe Literacy im-
7Estimates of equation (2) for hygiene and health and estimates of equation (1) for hygiene knowledgeare available from the authors. Hygiene and health estimates are not sensitive to the choice of specification.Cross-sectional difference regressions for hygiene knowledge show no treatment effect, which is consistentwith convergence of the ML arm after baseline imbalance.
12
proves the knowledge score by 0.28 points. This change is 14 percent improvement over the
baseline level and equals 0.37 standard deviations in the knowledge index. Infection Pre-
vention without the microscope component increases the score by only 0.11 points, which
is statistically different from the impact of ML (p = 0.07). Column 1 of Panel A shows
that estimates are smaller and are insignificant if we use equation (1) to estimate the effect
on knowledge. This finding is consistent with the baseline imbalance for hygiene knowledge
across study arms. Columns 2 and 4 include controls for baseline demographic and economic
characteristics of respondents, as well as the baseline dependent variable. As expected, these
controls slightly increase the precision of the estimates. Panel A estimates become larger and
statistically significant. This pattern arises because controlling for the baseline dependent
variable partially addresses the baseline imbalance in the dependent variable.
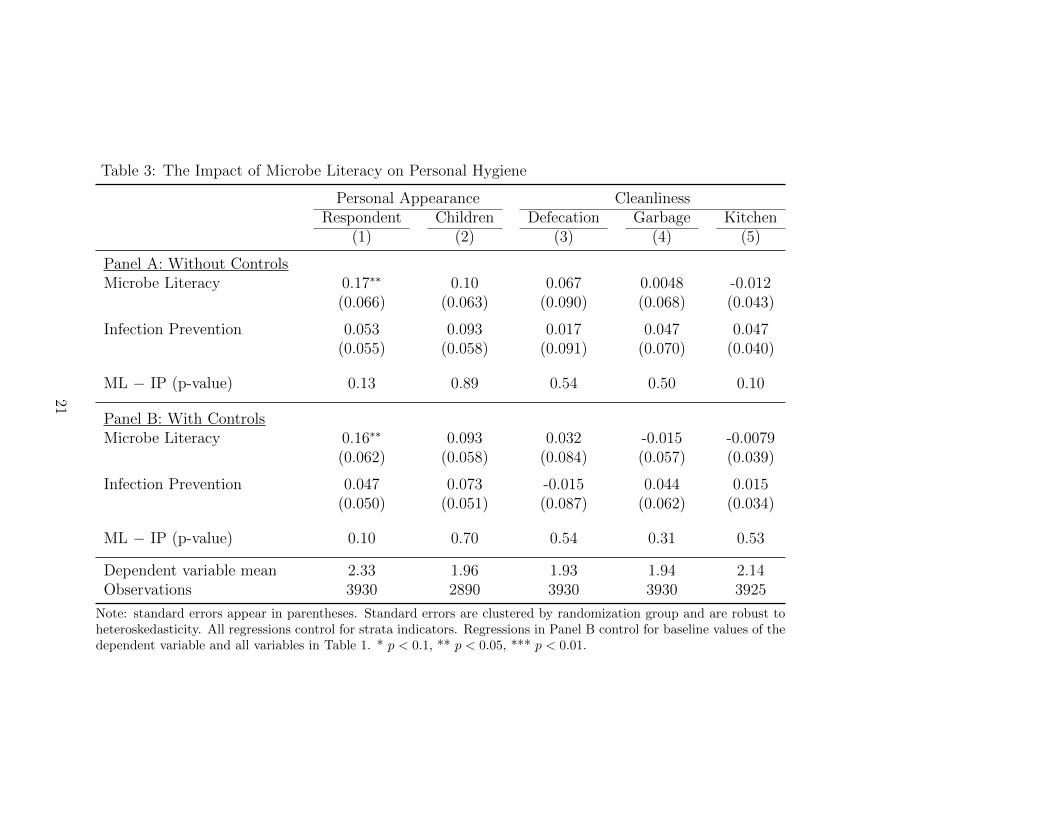
Table 3 estimates the treatment effect on several hygiene outcomes. Panel A shows
estimates that exclude demographic and economic controls, while Panel B shows estimates
that include these controls. Our primary hygiene outcomes are the personal appearance
of the respondent and her children, which appear in Columns 1 and 2. Microbe Literacy
significantly improves the personal appearance of the respondent. The average score increases
by 0.17 points on a three-point scale. This effect is 8 percent of the baseline level and 0.29
standard deviations. The effect is marginally significantly different from the effect of IP, with
a p-value of 0.13 without controls and 0.10 with controls. The estimate for child hygiene is
qualitatively similar but is smaller and not statistically significant.
Columns 3-5 show estimates for other hygiene and sanitation outcomes for the house-
hold. Column 3 shows results for the surveyor observation of the absence of open defecation,
Column 4 shows results for the absence of garbage, and Column 5 shows results for the
cleanliness of the cooking area. These outcomes differ from respondent and child hygiene
in Columns 1 and 2 because they are determined jointly with the household. Whereas
a respondent plausibly has some autonomy over grooming choices that are reflected in her
appearance, other household members also influence the cleanliness or dirtiness of the house-
13
hold environment. The lack of results here is consistent with our hypothesis that important
constraints limit the impact of the program on behavior.
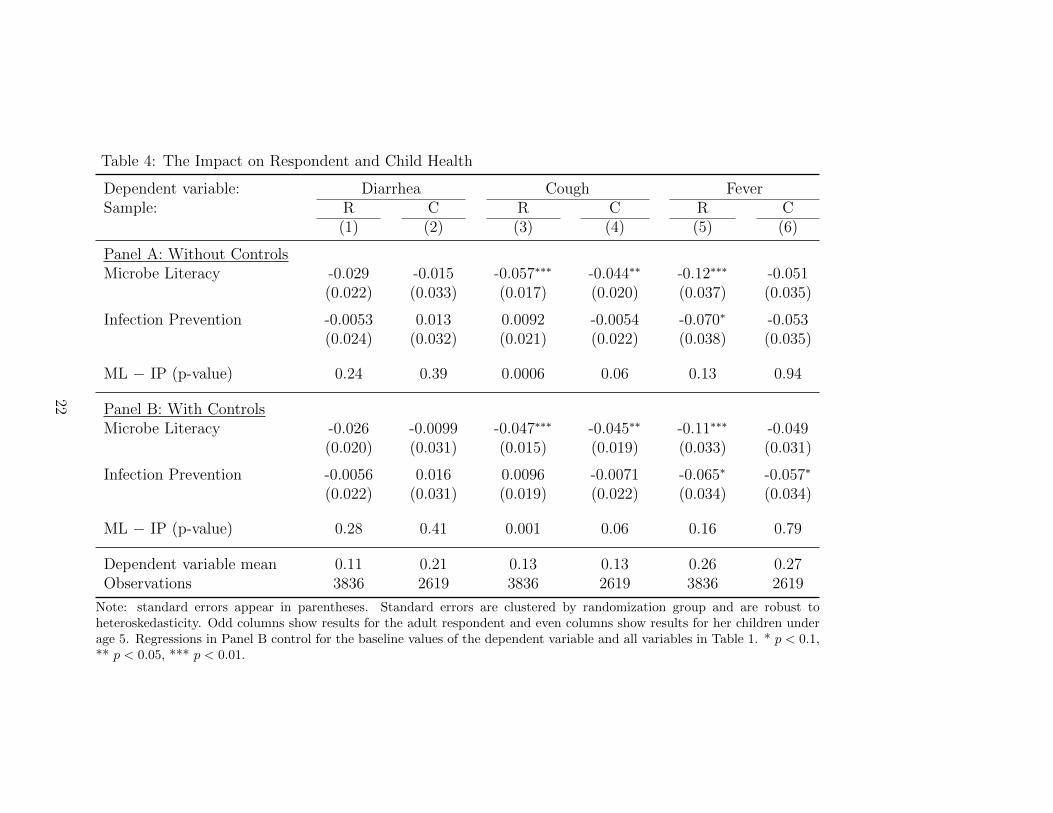
Table 4 shows the impact on diarrhea, cough, and fever based on Equation (1). Odd
columns show results for the respondent and even columns show results for children under
age five. We distinguish between the full sample (Panel A) and the high-diarrhea subsample
(Panel B), which is defined according to the stratification. Columns 1 and 2 do not show
significant treatment effects on diarrhea. ML reduces diarrhea by 26 percent for the respon-
dent and by 7 percent for her children, but these estimates are not significant. Estimates
are larger but remain insignificant for the high-diarrhea subsample.
The remainder of the table shows that ML significantly reduces in incidence of cough
and fever. Cough declines by 5.7 percentage points (44 percent) for the respondent and by
4.4 percentage points (34 percent) for her children. These estimates are nearly twice as large
in the high-diarrhea subsample, which also has higher baseline prevalence of cough. In Panel
A, the effect of ML on cough is significantly larger than the effect of IP. We find similar
estimates for fever. ML reduces incidence of fever by 12 percentage points (46 percent) for
the respondent and by 5.1 percentage points (19 percent, p = 0.15) for her children.
4.2 Traditional Beliefs and the Impact on Hygiene Knowledge
This subsection investigates whether adherence to traditional beliefs medicates the impact of
Microbe Literacy. We modify our primary specifications by interacting treatment with the
baseline traditional belief scores of respondents. The sign of this interaction is theoretically
ambiguous because it depends on how Bayesian learning parameters vary by TBI. However
one possibility is that high-TBI respondents may learn less from the program because they
have more precise prior beliefs, which lead them to discount the information they receive.
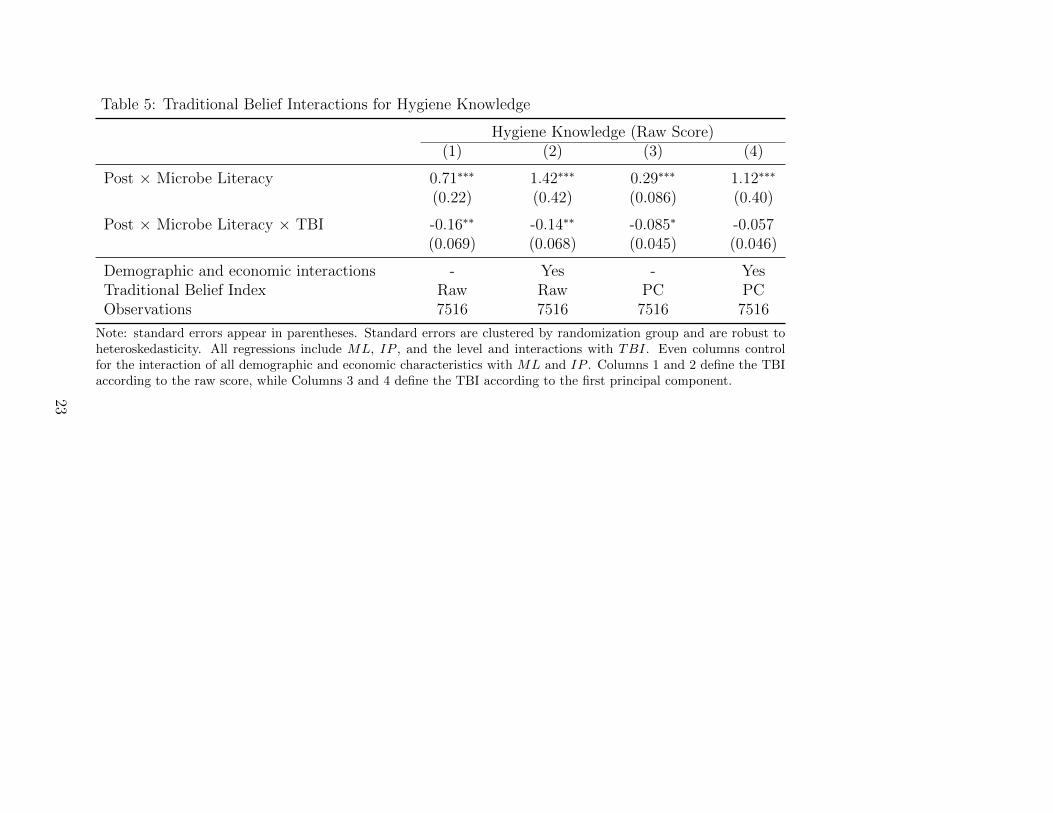
Estimates for the differential impact by TBI on hygiene knowledge appear in Table 5.
Columns 1 and 2 show results based on the raw sum of traditional belief indicators, while
Columns 3 and 4 show results based on the first principal component of these variables.
14
Estimates in Column 1 indicate that someone with a TBI score of 0 increases her score by
0.71 points. Each unit increase in the TBI reduces the impact on the score by 0.16 points.
Although the treatment is randomly assigned in this regression, traditional beliefs are not
randomly assigned, and so omitted variables that are correlated with the TBI may confound
these estimates. In particular, Appendix Table 2 shows that people without traditional
beliefs have higher socioeconomic status. Columns 2 and 4 address this concern by controlling
for the interaction between Post × treatment and all of the demographic and economic
variables reported in Table 1. These controls, which are jointly significant (p < 0.0001),
only slightly attenuate the estimate, which suggests that traditional beliefs do not proxy for
socioeconomic status.
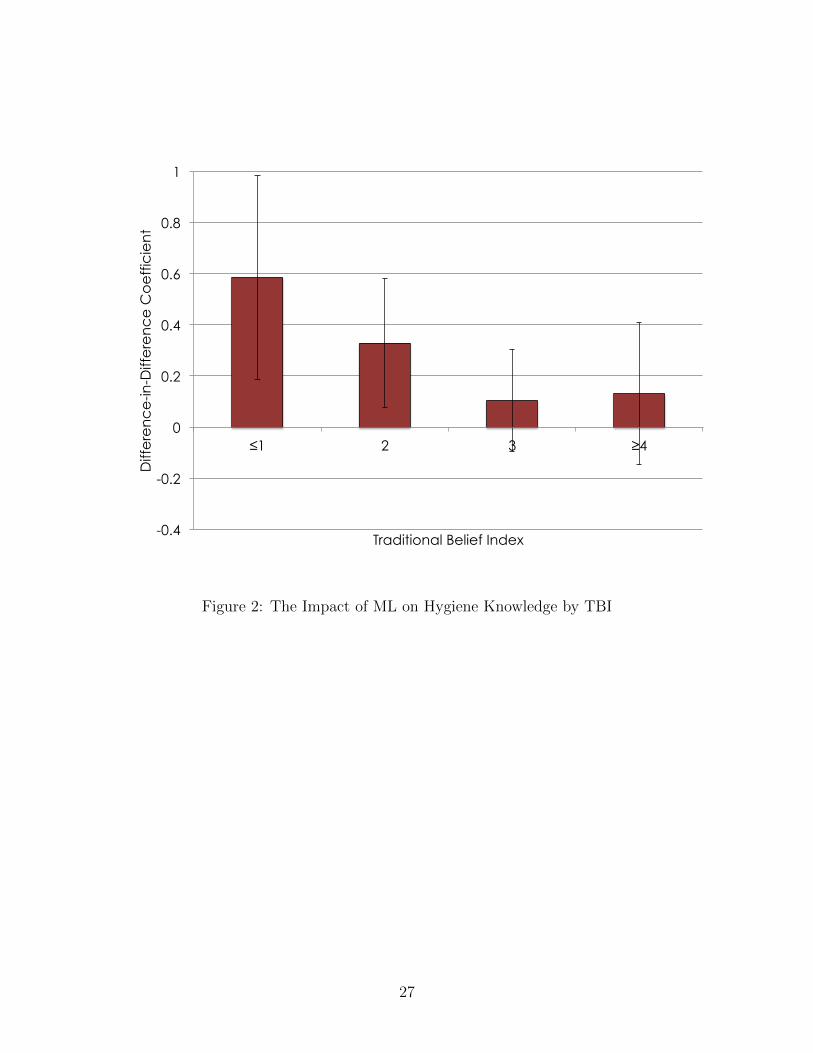
Figure 2 illustrates the differential treatment effects for people who do not hold tradi-
tional beliefs. The figure plots the ML coefficient from separate regressions by TBI value.
ML increases the knowledge scores of people with TBI values of 0 or 1 by 0.59 but increases
the scores of people with TBI values of 4 or more by just 0.13. This result suggests that the
program is unsuccessful in terms of conveying knowledge to people with traditional medical
beliefs.
Estimates for the differential effect by TBI on hygiene and health appear in Table 6.
Odd columns show results for the respondent and even columns show results for her children
younger than five. These estimates are consistent with the findings in Table 5, but they are
weaker and not statistically significant. Respondents with high TBI values improve their
appearance less in response to the program. Their health in terms of fever and cough also
does not fall as much. The insignificance of these results suggests that other factors may also
mediate hygiene and health outcomes, and thereby weaken the impact of the intervention.
We investigate this hypothesis further below.
15
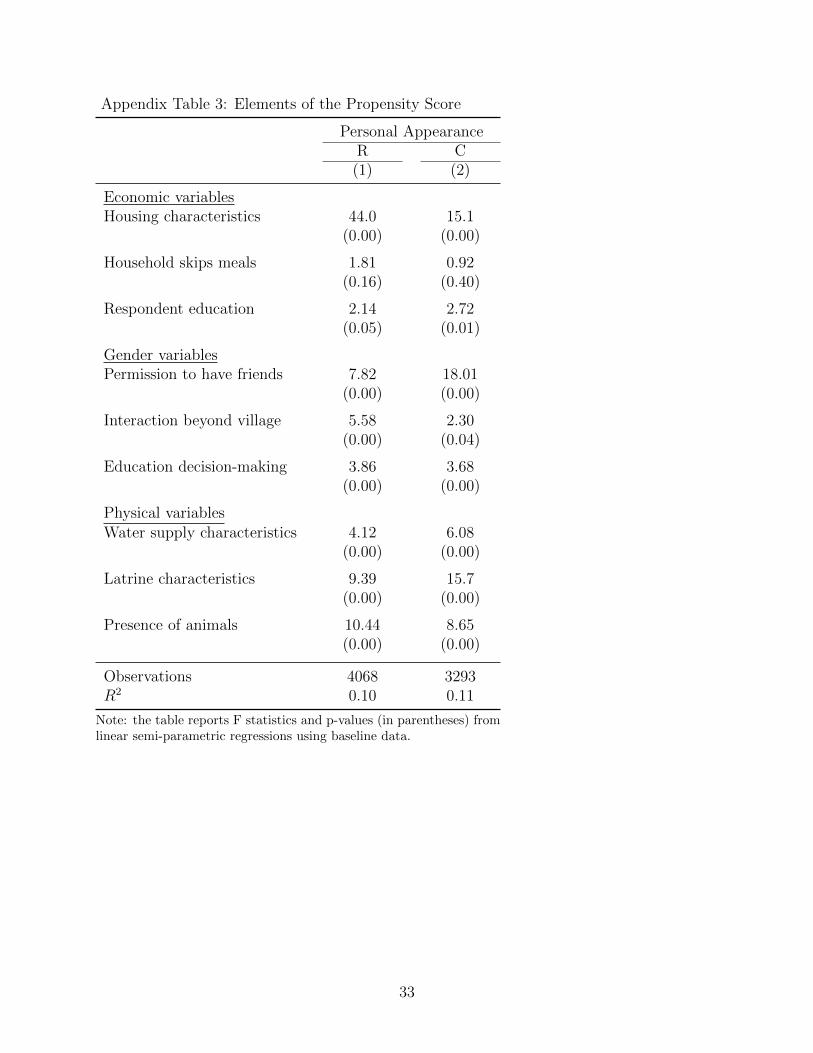
4.3 Propensity Score Interactions
Beahvioral constraints may prevent people from changing behavior in response to new in-
formation. These constraints are multidimensional and may vary individually. We identify
three categories of factors that plausibly influence respondent and child hygiene. We sum-
marize these variables and their contributions to the propensity score in Appendix Table
3. Economic variables include housing characteristics (the type of house and roof), whether
household members skip meals, and the respondent’s education. Gender variables include
whether the respondent needs her husband’s permission to have female friends, whether
she travels or speaks with people outside of her village, and the identity of the household
decision-maker with respect to the education of children. Physical variables include the type
of water supply, the characteristics of the latrine (including where it drains and whether it
is shared), and the presence of several types of domesticated animals.
Because most of these variables are categorical, we regression hygiene on category indi-
cators. The table shows the f-statistics and p-values for these indicators by group. Almost all
of these variables are highly significant. They jointly explain 10 percent of hygiene variation.
Our baseline estimates are based on a propensity score using OLS. However estimates based
on an ordered probit model, which is more appropriate for an ordered dependent variable,
are comparable.
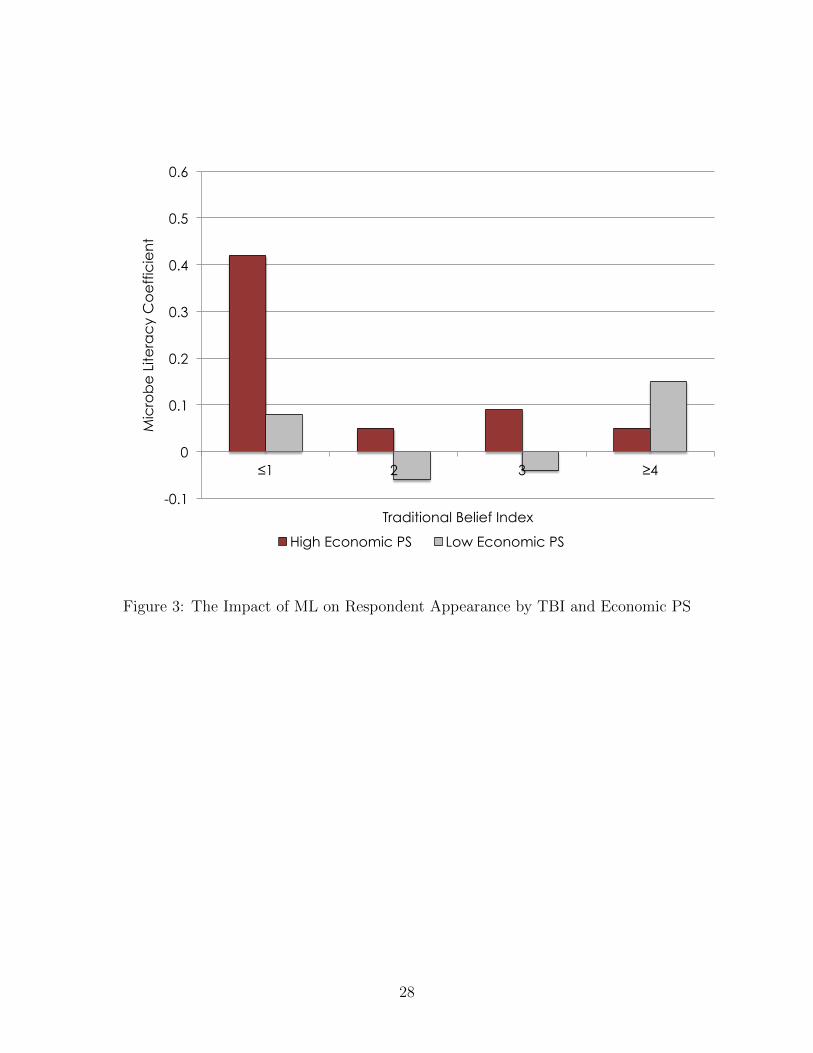
Table 7 shows estimates for the interaction between treatment, the propensity score,
and the TBI. Panel A shows the straight interaction, while Panel B distinguishes between
respondents with TBI values of 0 or 1, and those with TBI values of 2 or more. Columns
1 and 2 show results for the combined propensity score, and indicate that people with
high propensity for good hygiene respond more to treatment, however this effect diminishes
as the traditional belief index increases. Panel B shows the stark result that the entire
treatment effect on hygiene arises for people with traditional belief responses of 0 or 1, which
indicates that the absence of traditional beliefs and the absence of practical constraints are
complementary for behavior change.
16
Columns 3 through 8 distinguish between the categories of constraints. Economic and
(to a lesser extent) gender constraints appear to limit behavior change more than physical
constraints. We illustrate this pattern further in Figures 3, 4, and 5, which plot the responses
for high- and low-propensity respondents with different TBI values. In particular, Figure 3
shows that the hygiene response is concentrated among high-propensity respondents without
traditional beliefs.
5 Conclusion
Hygiene education may have mixed effectiveness as an anti-diarrheal intervention because
people hold traditional beliefs that are not consistent with a pathogenic model of disease
transmission. Microbe Literacy attempts to make hygiene instruction more salient by demon-
strating the existence of microbes to participants. Our estimates generally show that ML has
a larger impact on knowledge, behavior, and health than conventional hygiene education,
although these differences are not always statistically significant. Neither ML or IP has a
significant effect on diarrhea in this study, despite the focus of this intervention on improving
this outcome.
Estimates for the interaction between the program and traditional medical beliefs indi-
cate that these beliefs interfere with learning and behavior change. The lack of significant
treatment effects for adherents to traditional beliefs in Figures 2 and 3 suggest that policy-
makers must take more drastic steps to overcome the bias against hygiene education among
people with traditional beliefs. Our results suggest that the prevalence of traditional medi-
cal beliefs in the developing world may interfere with the adoption of healthy behaviors and
contribute to the tremendous disease burden in poor countries.
Finally, our estimates highlight how practical constraints may prevent behavior change
from learning interventions. Hygiene education is attractive from a policy perspective be-
cause it is inexpensive compared to water supply and sanitary investments. However a
combination of educational and infrastructural investments may be needed to achieve large
17
and sustained health improvements.
18
Table 1: Baseline Characteristics by Treatment Status
Mean P-valueML IP C ML − IP ML − C(1) (2) (3) (4) (5)
Demographic CharacteristicsAge 26.0 27.7 28.1 0.36 0.21Illiterate 0.25 0.24 0.38 0.95 0.04Any schooling 0.28 0.13 0.11 0.15 0.03Married 0.57 0.63 0.63 0.37 0.31Household size 6.6 6.5 6.4 0.86 0.68Barailvi sect 0.78 0.81 0.74 0.78 0.81Hadis sect 0.14 0.16 0.24 0.79 0.35Ramadan fasting days 12.7 14.4 15.4 0.21 0.04Prays at least once per day 0.75 0.73 0.76 0.81 0.95
Note: Standard errors are clustered by randomization unit and are robust to heteroskedasticity.All regressions control for strata indicators. N = 3704 in Panel A and N = 7516 in Panel B. ForColumns 1 and 2, we compute the unweighted sum of correct responses. For Columns 3 and 4,we aggregate according to the Rasch IRT model. * p < 0.1, ** p < 0.05, *** p < 0.01
20
Table 3: The Impact of Microbe Literacy on Personal Hygiene
Personal Appearance CleanlinessRespondent Children Defecation Garbage Kitchen
(1) (2) (3) (4) (5)
Panel A: Without ControlsMicrobe Literacy 0.17∗∗ 0.10 0.067 0.0048 -0.012
Note: standard errors appear in parentheses. Standard errors are clustered by randomization group and are robust toheteroskedasticity. All regressions control for strata indicators. Regressions in Panel B control for baseline values of thedependent variable and all variables in Table 1. * p < 0.1, ** p < 0.05, *** p < 0.01.
21
Table 4: The Impact on Respondent and Child Health
Dependent variable: Diarrhea Cough FeverSample: R C R C R C
Note: standard errors appear in parentheses. Standard errors are clustered by randomization group and are robust toheteroskedasticity. Odd columns show results for the adult respondent and even columns show results for her children underage 5. Regressions in Panel B control for the baseline values of the dependent variable and all variables in Table 1. * p < 0.1,** p < 0.05, *** p < 0.01.
22
Table 5: Traditional Belief Interactions for Hygiene Knowledge
Hygiene Knowledge (Raw Score)(1) (2) (3) (4)
Post × Microbe Literacy 0.71∗∗∗ 1.42∗∗∗ 0.29∗∗∗ 1.12∗∗∗
Demographic and economic interactions - Yes - YesTraditional Belief Index Raw Raw PC PCObservations 7516 7516 7516 7516
Note: standard errors appear in parentheses. Standard errors are clustered by randomization group and are robust toheteroskedasticity. All regressions include ML, IP , and the level and interactions with TBI. Even columns controlfor the interaction of all demographic and economic characteristics with ML and IP . Columns 1 and 2 define the TBIaccording to the raw score, while Columns 3 and 4 define the TBI according to the first principal component.
23
Table 6: Traditional Belief Interactions for Hygiene and Health
Appearance Diarrhea Fever CoughR C R C R C R C(1) (2) (3) (4) (5) (6) (7) (8)
Note: standard errors appear in parentheses. Standard errors are clustered by randomization group and are robust to heteroskedasticity. Thetraditional belief index (TBI) is the unadjusted sum of responses. Odd columns refer to the respondent and even columns refer to the children.
24
Table 7: Propensity Score Interactions for Respondent and Child Hygiene
Dependent variable: Personal Appearance of:R C R C R C R C
Note: standard errors appear in parentheses. Standard errors are clustered by randomization group and are robust to heteroskedasticity. Odd columnsrefer to the respondent and even columns refer to her children.
25
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8
Perc
en
t
Traditional Belief Index
Figure 1: The Frequency Distribution of the Traditional Belief Index
26
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
≤1 2 3 ≥4
Diff
ere
nc
e-in
-Diff
ere
nc
e C
oe
ffic
ien
t
Traditional Belief Index
Figure 2: The Impact of ML on Hygiene Knowledge by TBI
27
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
≤1 2 3 ≥4
Mic
rob
e L
itera
cy
Co
eff
icie
nt
Traditional Belief Index
High Economic PS Low Economic PS
Figure 3: The Impact of ML on Respondent Appearance by TBI and Economic PS
28
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
≤1 2 3 ≥4
Mic
rob
e L
itera
cy
Co
eff
icie
nt
Traditional Belief Index
High Gender PS Low Gender PS
Figure 4: The Impact of ML on Respondent Appearance by TBI and Gender PS
29
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
≤1 2 3 ≥4
Mic
rob
e L
itera
cy
Co
eff
icie
nt
Traditional Belief Index
High Physical PS Low Physical PS
Figure 5: The Impact of ML on Respondent Appearance by TBI and Physical PS
30
Appendix Table 1: The Correlation Between Personal Appearance and Other Hygiene Measures
Absence of Absence of Cleanliness Breastfeeds Hand Rinse Hand RinseDefecation Garbage of Kitchen Exclusively Turbidity E. coli
(1) (2) (3) (4) (5) (6)
Appearance of Respondent 0.32∗∗∗ 0.29∗∗∗ 0.28∗∗∗ 0.038 -0.18∗∗∗ -22.5∗
(0.029) (0.024) (0.017) (0.042) (0.036) (11.5)
Appearance of Children 0.10∗∗∗ 0.048∗∗ 0.20∗∗∗ 0.072∗ -0.12∗∗∗ -9.01(0.029) (0.024) (0.017) (0.042) (0.037) (11.8)
Note: the table reports F statistics and p-values (in parentheses) fromlinear semi-parametric regressions using baseline data.
33
Appendix Figure 1: Photographs Corresponding to Personal Appearance Categories
34
References
Ahmad, Fayyez, Uzair Ahmad, Bilal Aziz, Edward Higgins, Ian King, AsjadNaqvi, and Iqbal Rehman, “Preliminary Results on Use of Microscopes to ReduceRates of Diarrhea and Respiratory Illness in Children Under Five of Non-Literate Par-ents in Swat Valley, Pakistan,” August 2012. Unpublished manuscript.
Anwar, M., J. Green, and P. Norris, “Health-Seeking Behaviour in Pakistan: a Narra-tive Review of the Existing Literature,” Public Health, 2012, 126, 507–517.
Banerjee, Abhijit, Angus Deaton, and Esther Duflo, “Wealth, Health, and HealthServices in Rural Rajasthan,” American Economic Review, May 2004, 94 (2), 326–330.
Beau De Rochars, Valery, Julie Tipret, Molly Patrick, Lara Jacobson, KamilBarbour, David Berendes, Diana Bensyl, Cathie Frazier, Jean Domercant,Roodly Archer, Thierry Roels, Jordan Tappero, and Thomas Handzel,“Knowledge, Attitudes, and Practices Related to Treatment and Prevention of Cholera,Haiti, 2010,” Emerging Infectious Diseases, November 2011, 17 (11), 2158–2161.
Bruhn, Miriam and David McKenzie, “In Pursuit of Balance: Randomization in Prac-tice in Development Field Experiments,” American Economic Journal: Applied Eco-nomics, 2009, 1 (4), 200–232.
Das, Jishnu and Jeffrey Hammer, “Which doctor? Combining Vignettes and itemresponse to measure clinical competence,” Journal of Development Economics, 2005,78, 348–383.
Davis, Jennifer, Amy Pickering, Kirsten Rogers, Simon Mamuya, and AlexandriaBoehm, “The Effects of Informational Interventions on Household Water Management,Hygiene Behaviors, Stored Drinking Water Quality, and Hand Contamination in Peri-Urban Tanzania,” American Journal of Tropical Medicine and Hygiene, February 2011,84 (2), 184–191.
Fewtrell, L, RB Kaufmann, D Kay, W Enanoria, L Haller, and JM Colford,“Water, Sanitation, and Hygiene Interventions to Reduce Diarrhoea in Less DevelopedCountries: a Systematic Review and Meta-Analysis,” Lancet Infectious Diseases, 2005,5 (1), 42–52.
Hrdy, Daniel, “Cultural practices contributing to the transmission of human immunodefi-ciency virus in Africa,” Reviews of Infectious Diseases, 1987, 9 (6), 1109–19.
Hunte, Pamela and Farhat Sultana, “Health-Seeking Behavior and the Meaning ofMedications in Balochistan, Pakistan,” Social Science and Medicine, 1992, 34 (12),1385–1397.
Karmakar, Palash, Muhammad Mazharul Islam, Md. Golam Kibria, Moham-mad Salim Hossain, and Mohammad Mafruhi Sattar, “Prevalence, belief andawareness of preferring traditional health care system in urban and rural people of
35
Noakhali district, Bangladesh,” International Current Pharmaceutical Journal, 2012, 1(9), 229–234.
Kernan, Walter, Catherine Viscoli, Robert Makuch, Lawrence Brass, and RalphHorwitz, “Stratified Randomization for Clinical Trials,” Journal of Clinical Epidemi-ology, January 1999, 52 (1), 19–26.
Monte, Cristina, Ann Ashworth, Marilyn Nations, A. Lima, A. Barreto, andSharon Huttly, “Designing Educational Messages to Improve Weaning Food HygienePractices of Families Living in Poverty,” Social Science and Medicine, 1997, 44 (10),1453–64.
Mull, J. Dennis and Dorothy Mull, “Mothers’ Concepts of Childhood Diarrhea in RuralPakistan: What ORT Program Planners Should Know,” Social Science and Medicine,1988, 27 (1), 53–67.
Nielsen, Melanie, Anneke Hoogvorst, Flemming Konradsen, Muhammed Mu-dasser, and Wim van der Hoek, “Causes of Childhood Diarrhea as Perceived byMothers in the Punjab, Pakistan,” Southeast Asian Journal of Tropical Medicine andPublic Health, June 2003, 34 (2), 343–351.
Schmidt, Wolf-Peter, Benjamin Arnold, Sophie Boisson, Bernd Genser, StephenLuby, Mauricio Barreto, Thomas Clasen, and Sandy Cainrcross, “Epidemiolog-ical Methods in Diarrhoea Studies - an Update,” International Journal of Epidemiology,December 2011, 40 (6), 1678–92.
, Bernd Genser, Mauricio Barreto, Thomas Clasen, Stephen Luby, SandyCainrcross, and Zaid Chalbi, “Sampling Strategies to Measure the Prevalence ofCommon Recurrent Infections in Longitudinal Studies,” Emerging Themes in Epidemi-ology, August 2010, 7 (15), 1–13.
World Health Organization, “Traditional Medicine,” 2003. Fact Sheet No. 134.